Embed Size (px)
Citation preview

Sepsis is defined as the body’s reaction to infection that results in a dysregulated, life-threatening immune response causing organs to fail (Rhodes et al., 2017; Singer et al., 2016). Sepsis can be triggered by any infection but is most commonly the result of infections of the lungs, urinary tract, abdomen, skin, soft tissue, bones or joints (UK Sepsis Trust, 2019). Sepsis is a time-critical condition: if detected and treated early, the clinical outcome is good; if left unchecked, the patient can quickly develop septic shock, a subset of sepsis that causes multi-organ failure (UK Sepsis Trust, 2019). Septic shock encompasses circulatory, cellular and metabolic dysfunction, and has a high risk of mortality (Rhodes et al., 2017).
A study in 2017 estimated that there were 48.9 million cases of sepsis worldwide and 11 million deaths annually (Rudd et al., 2020). World Sepsis Day, held on 13 September every year, aims to increase global awareness of this poorly understood condition. In May 2017, the World Health Assembly, the decision-making arm of the World Health Organization, made sepsis a global health priority and adopted a resolution to prevent, diagnose, manage and improve sepsis outcomes (Global Sepsis Alliance, 2017).
In the UK, 52,000 deaths are attributable to sepsis every year—more than prostate, bowel and breast cancer combined—with a cost of at least £1.5 billion to the NHS (UK Sepsis Trust, 2019). An estimated 65,000 patients survive sepsis each year but can be left with long-term complications, such as cognitive dysfunction, amputation and irreversible
damage to the lungs, kidneys and heart, as well as post-traumatic stress disorder, often linked to their prolonged stay in intensive care units (NCEPOD, 2015).
Sepsis is a clinical priority in the UK. Political and healthcare organisations have increased the focus on better care and outcomes for patients with sepsis (NHS England, 2015). In the UK, many NHS trusts have implemented local and regional initiatives to improve outcomes for patients, including the use of sepsis pathways.
The National Confidential Enquiry into Patient Outcome and Death (NCEPOD, 2015) recommends introducing a clinical lead for sepsis to champion best practice, take responsibility for the clinical governance of sepsis management and liaise with staff responsible for antimicrobial stewardship in their hospital. NICE (2017) has published guidelines and recommendations on the recognition, diagnosis and early management of sepsis. Numerous reports have highlighted failings in the identification of sepsis and promoted best practice relating to the assessment and timely initiation of treatment for sepsis (Mothers and Babies: Reducing Risk through Audits and Confidential Enquiries Across the UK [MBRRACE-UK], 2020; NCEPOD, 2015; Parliamentary and Health Service Ombudsman, 2013).
This procedure explains the pathophysiology of sepsis, its possible causes and vulnerable patient groups.
Page 1 of 4
Management ofMedical Emergencies
Adults
Sepsis Part 1: Possible causes and high-risk groupsClaire Walker, Lecturer, University of Liverpool
©2021 Clinical Skills Limited. All rights reserved
Do not undertake or attempt any procedure unless you are, or have supervision from, a properly trained, experienced and competent person.Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution.
[PIC: sepsis cascade / loss of fluid from blood vessels into interstitial space due to vasodilation/vessel leakage]
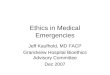
The pathogenesis of sepsis is complex and is characterised by an exaggerated inflammatory response throughout the body. This response involves the immune system and the coagulation cascade (Hunt, 2019; UK Sepsis Trust, 2019). This systemic inflammatory response triggers the immune system to release large amounts of leukocytes (white blood cells) and chemicals such as chemokines and other cytokines, and coagulation factors (Ward & Levy, 2017). These substances cause blood vessels to vasodilate and leak resulting in a fall in blood pressure and tissue hypoperfusion. These changes lead to increased oxygen demand, acidosis and ischaemia at the cellular level (McClelland & Moxon, 2014).
Pathophysiology of sepsis
CW says add the liver and bladder as well and outline them in red
Close up this space to normal style SK 240821
• Coagulopathy • Fibrinolysis• Local immune response
LeukocytesErythrocytes Platelets
• Microvascular thrombosis
Fibrin
Vasodilation
Local infection Inflammation Sepsis Septic shock
Thrombus
Vessel leakage
• Hypovolaemia• Acidosis• Ischaemia/tissue hypoxia• Acute organ dysfunction

Management ofMedical Emergencies
Adults
Sepsis Part 1: Possible causes and high-risk groups Page 2
Page 2 of 4
Do not undertake or attempt any procedure unless you are, or have supervision from, a properly trained, experienced and competent person.Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution.
Source: http://health-fts.blogspot.com/2012/01/neonatal-sepsis.html
ADD Endocarditis pointing to the heart
Meningitis
Pneumonia
Endocarditis
Bloodstream infection
Gall bladder infection (cholecystitis)
Urinary tract infectionUrinary catheter-related infection
Abdominal causes, e.g., appendicitis, burst ulcer, perforated bowel
Intravascular catheter-related infection
Diarrhoeal disease
Wound from trauma or surgery
Septic arthritis/osteomyelitis
Skin/soft tissue infection,e.g., cellulitis, infected leg ulcer
Infected cut or bite
Signs of sepsis in children A child who is unwell with a fever (or who has had a fever in the last 24 hours) or low temperature, and who has any of the following symptoms, requires urgent medical attention (UK Sepsis Trust, 2019):• Tachypnoea;• A convulsion;• Skin that looks mottled, cyanotic, or pale;• A rash that does not fade when you press it;• Very lethargic or difficult to wake;• Feels abnormally cold to touch.
If a child shows any of the following symptoms, “think sepsis” (NHS Inform, 2020; UK Sepsis Trust, 2019):• Temperature over 38°C in babies under 3 months, or
over 39°C in babies aged 3–6 months;• Low temperature (below 36°C: check three times in a
10-minute period);• Respiratory distress;• Unable to say more than a few words at once (in older
children who normally talk);• Not passed urine or had a wet nappy for 12 hours;• Not feeding (child under 5 years);• Not drinking for more than 8 hours (when awake);• Repeated vomiting in child under 5 years;• Vomit is bile-stained (green), bloody or black;• Fontanelle on a baby's head is bulging;• Eyes look “sunken”;• Child cannot be encouraged to show interest in
anything;• Baby is floppy;• Weak, “whining” or continuous crying in a younger
child;• Confusion in an older child;• Not responding or very irritable;• Stiff neck, especially when trying to look up and down.
Signs of sepsis in adults (UK SepsisTrust, 2019)
• Slurred speech or confusion;• Extreme shivering or muscle pain, or fever;• Passing no urine (in a day);• Severe breathlessness;• It feels like you are going to die; and• Skin mottled or discoloured.
Some common causes of sepsis

EXP: 10 - 2017
LOT: A21LA356
Infanrix hexa 6
EXP:
10
LOT: A21LA356
Infanrix hexa 6
Recognising sepsis
Vulnerable groups: (a) Children and babies
Adults
Sepsis Part 1: Possible causes and high-risk groups Page 3
Page 3 of 4
Do not undertake or attempt any procedure unless you are, or have supervision from, a properly trained, experienced and competent person.Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution.
Anyone can be affected by sepsis, and it remains unclear why some people who get an infection develop sepsis and others do not. People are more likely to develop sepsis after a viral illness, such as a cold, or a minor injury (UK Sepsis Trust, 2019). Evidence suggests that early recognition of sepsis can be improved. The very young, the very old, patients who are immunosuppressed and pregnant women are at particular risk (NHS England, 2015).
In 2017, an estimated 20.3 million children under 5 years, and 4.9 million children and adolescents aged 5–19 years, had sepsis worldwide; of those under 5 years, an estimated 2.9 million died as a result (Rudd et al., 2020). Children often present with atypical or vague signs and symptoms, which can lead to delayed or inappropriate treatment (UK Sepsis Trust, 2019). The immune system of a child is not the same as that of an adult, and the immune system does not reach full maturity until adolescence. Neonates are most compromised as their immune system is poor and their immune response is less reactive to pathogens (Randolph & McCulloh, 2014).
The UK vaccination programme has contributed to the prevention of sepsis. Childhood vaccinations against Haemophilus influenzae type B, meningococcal serogroups B and C and pneumococcal infection have both protected the vaccinated children and reduced the circulation of these organisms in the wider community (PHE, 2020; NHS England, 2015).
Due to existing comorbidities, reduced immunity, limited function and the effects of aging, older people are particularly vulnerable to developing sepsis (Nasa et al., 2012), in particular from respiratory and urinary tract infections (UTIs) (NCEPOD, 2015). Liver disease and malnutrition increase the risk of developing sepsis (Martin et al., 2017; Yan et al., 2014; Foreman et al., 2003).
The influenza and pneumococcal vaccine programme can help to prevent some cases of pneumonia, and taking preventative measures, such as ensuring adequate nutrition and hydration and effective management of incontinence, can help reduce the chance of UTIs (NHS England, 2015).
(b) Older patients
Ensuring that childhood vaccinations are kept up to date will help protect children against sepsis. When giving childhood vaccinations, follow local policy regarding personal protective equipment
Some vaccination programmes for older people reduce the risk of infections that can result in sepsis. When giving vaccinations, follow local policy regarding personal protective equipment
Management ofMedical Emergencies

RUNNING ALERT ALARM
Fluid Flow to Patient
Options Primary Piggyback
Press Primary or Piggyback
MainDisplay
VolumeHistory
AlarmSilence
BackLight
Rate Vol
7 8 9
4 5 6
1 2 3
0
STOPOpen
CLR
ONOFFCHARGE
START
ADULT RMHRate
mL/hr
300
Air Detected
VolumeRemaining
300
TimeRemaining 1:00 hr min
HOLD
LIFT
5F
5Fr
IF YOU’RE FE
VERISH OR SHIVERING
AND FEELIN
G REALLY UNWELL
Sepsis i
s a po
tential
ly life
threat
ening
conditi
on, trig
gered
by infe
ction
It’s ha
rd to s
pot, bu
t it kill
s 44,0
00 peo
ple
a year
in the
UK
It can
be eas
y to tre
at if ca
ught ea
rly. Th
e
charity
needs
fundin
g to tra
in
the pu
blic an
d the h
ealthc
are co
mmunity
on how
to spo
t sepsi
s more
quick
ly
IT’S A SIMPLE
QUESTION,
BUT IT C
OULD SAV
E LIVESNHS
JUST ASK “COULD
IT BE
SEPSI
S?” THE UK
SEPSIS
TRUST
www.sepsi
strust.o
rg
(d) People who are immunosuppressed
People who are immunosuppressed are at risk of neutropenic sepsis which has the potential to be rapidly fatal (UK Sepsis Trust, 2019). Patients may be immunosuppressed due to radiotherapy, chemotherapy, long-term steroid therapy or anti-rejection drugs following organ transplant, autoimmune conditions, diabetes or vascular disease. Prevention and treatment of sepsis can be challenging in patients with a poor immune response to infection (Kalil & Opal, 2015).
The bone marrow continuously produces white blood cells called neutrophils, which help to provide immunity, but chemotherapy suppresses this function and prevents these white blood cells from maturing. As a result, their number in the bloodstream decreases; this is called neutropenia (Vioral & Wentley, 2015). Cancer patients receiving chemotherapy are therefore prone to neutropenic sepsis, which is a significant cause of cancer treatment-related mortality (Ford & Marshall, 2014). Patients who are on long-term immunosuppressant therapy likewise require regular monitoring of their white blood cell counts.
Advise vulnerable patients about relevant immunisations. For example, offer the pneumococcal vaccine to patients with respiratory conditions, such as chronic obstructive pulmonary disease. Give information to patients and carers about how to recognise the signs and symptoms of sepsis and what to do if they feel unwell. The UK Sepsis Trust has excellent resources for patients: https://sepsistrust.org/
Adults
Sepsis Part 1: Possible causes and high-risk groups Page 4
Page 4 of 4
Do not undertake or attempt any procedure unless you are, or have supervision from, a properly trained, experienced and competent person.Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution.
This is for immunosuppressed patients
Move blue type to the vulnerable groups pageShow bald patient who has had chemo, nurse taking temperature, with blanket round them because they are cold
Maternal infection leading to sepsis is an important and preventable cause of mortality and severe morbidity. Global estimates suggest that direct (obstetric) infections are the third most common cause of maternal mortality in low-to-middle income countries due to a lack of affordable healthcare (WHO, 2020a; 2020b).
During pregnancy, significant physiological changes occur that make pregnant women more vulnerable. Vasodilation of arterial and venous smooth muscle occurs to accommodate the increase in blood volume (see insets), making pregnant women vulnerable to dyspnoea, palpitations, tiredness and pulmonary oedema. Changes to respiratory physiology increase the respiratory rate.
Changes to the coagulation of the blood, increased body weight and a reduction in cardiorespiratory reserve increase complications during infection (Joseph et al., 2009).
The ureters can become obstructed by the expanding uterus leading to urinary stasis and increasing the incidence of urinary tract infections.
Measure pulse, temperature, respiratory rate and blood pressure in any pregnant woman who presents feeling unwell. Preventing influenza during pregnancy is important and pregnant women are offered influenza immunisation for this reason (NHS England, 2015). Likewise, pregnant women are encouraged to become vaccinated against COVID-19 (RCOG, 2021)
Vasodilation in pregnancy
Cross-section through normal blood vessel
(c) Pregnancy
Management ofMedical Emergencies