Embed Size (px)
Citation preview

ADVANCES IN INSULINJanet B. McGill, MD

Grants to Washington University: NIH, Helmsley Trust, Dexcom, Novartis, Medtronic, NovoNordisk, Sanofi
Consultant: Aegerion, Culinary Arts, Gilead, NovoNordisk, Sanofi
Speaker: Aegerion, Dexcom, Janssen, Mannkind
Slides are from many sources: Thanks to Drs. Philip Home, Bruce Bode, Guillermo Umpierrez, Garry Tobin

Fred Sanger determined
sequence in 1955 received
Nobel Prize in 1958
Fredrick Banting and John James
Richard Macleod Nobel Prize in 1923
Early Timeline for Insulin Development

Early, modest reporting…
• Banting and Best made public their report on the
effectiveness of pancreatic extracts in the treatment of
diabetic dogs on November 14, 1921. The report (later
published in J Lab Clin Med 7:251–266, 1922) stated,
"...it is very obvious that the results of our experimental
work, as reported in this paper do not at present justify
the therapeutic administration of degenerated gland
extracts to cases of diabetes mellitus in the clinic."
Allen FN, letter to NEJM, 1977

• “A hope for life
which they
hardly dared to
anticipate”
• Dr. Elliott P.
Joslin May 1922
Major RH. JAMA 1923;80:1597.
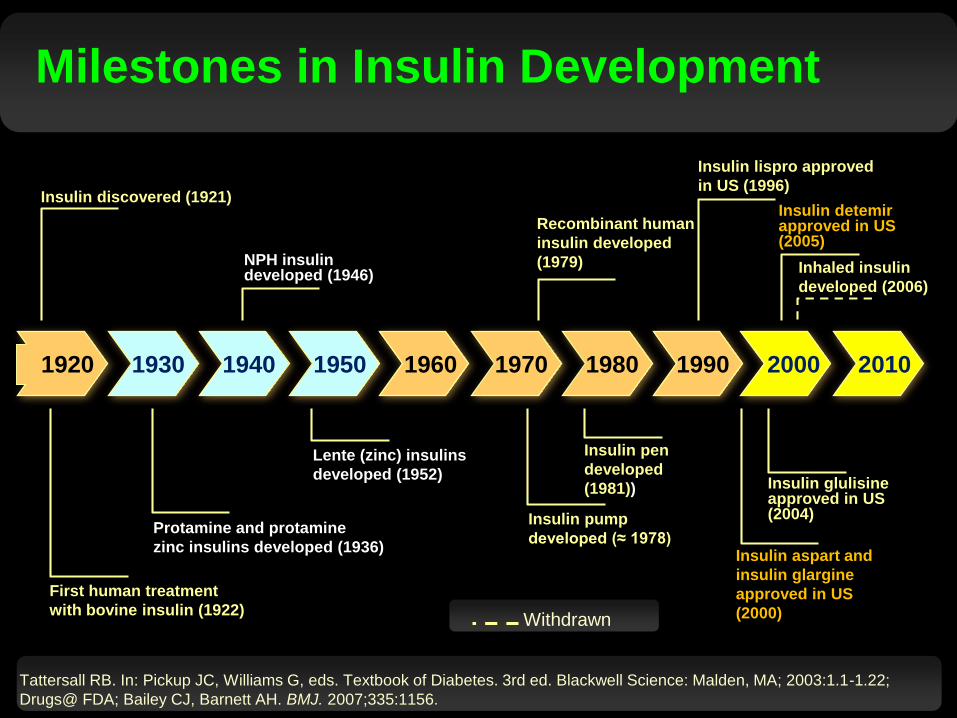
Milestones in Insulin Development
Withdrawn
Tattersall RB. In: Pickup JC, Williams G, eds. Textbook of Diabetes. 3rd ed. Blackwell Science: Malden, MA; 2003:1.1-1.22;
Drugs@ FDA; Bailey CJ, Barnett AH. BMJ. 2007;335:1156.
1920 1930 1940 1960 1970 1980 2000 201019901950
Insulin discovered (1921)
First human treatment
with bovine insulin (1922)
Protamine and protamine
zinc insulins developed (1936)
NPH insulin developed (1946)
Lente (zinc) insulins
developed (1952)
Recombinant human
insulin developed
(1979)
Insulin pump
developed (≈ 1978)
Insulin pen
developed
(1981))
Insulin lispro approved
in US (1996)
Insulin aspart and
insulin glargine
approved in US
(2000)
Insulin glulisine approved in US(2004)
Insulin detemir approved in US(2005)
Inhaled insulin
developed (2006)

Insulin Development Continues
Information from multiple sources: JMcGill
Continuous glucose monitoring + insulin pump
Techno
sphere
Inhaled
insulin
Ultra
long
acting
Ultra
short
acting
Smart
insulin
Closed
Loop
Systems
Biosimilar
insulin
Approved Degludec, FiAsp
approved????? Hybrid Closed
Loop systems are
available

Challenges with
extraction included
managing the pH,
additives, avoiding
other peptides,
maintaining consistent
concentration.

Renovated Connaught Laboratory supplied all of Canada’s insulin until 1927
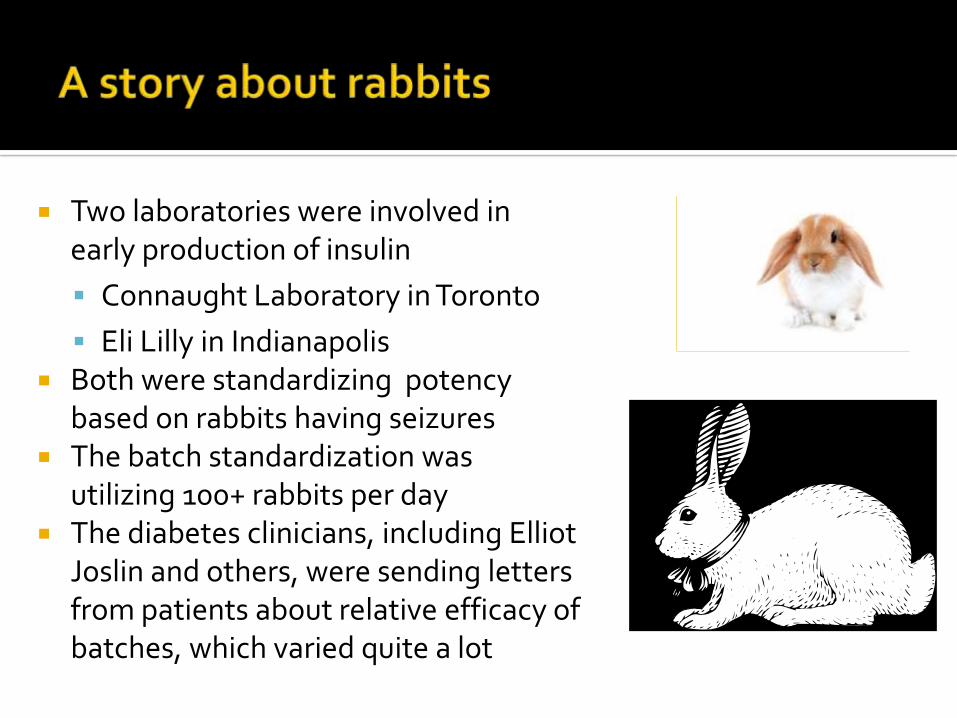
Two laboratories were involved in early production of insulin
▪ Connaught Laboratory in Toronto
▪ Eli Lilly in Indianapolis Both were standardizing potency
based on rabbits having seizures The batch standardization was
utilizing 100+ rabbits per day The diabetes clinicians, including Elliot
Joslin and others, were sending letters from patients about relative efficacy of batches, which varied quite a lot

Tailored treatment options for patients with impaired renal function7
Improvement in glycemic control1
Minimization of the risk of hypoglycemia2
Glycemic control without weight gain3,4
Treatment regimens that provide a comprehensive approach to CV risk factor reduction4-6
Better treatment adherence8
CV, cardiovascular
1. Liebl A et al. Diabetologia 2002;45:S23-8; 2. Cryer PE. Diabetes 2008;57:3169-76; 3. Fonseca V et al. Diabetes Care 2013;36:2162-8;
4. Goldenberg RM. Can J Diabetes 2011;35:518-27; 5. International Diabetes Federation. Global Guideline for Type 2 Diabetes:
http://www.idf.org/global-guideline-type-2-diabetes-2012, accessed 1/30/13; 6. Inzucchi SE et al. Diabetes Care 2012;35:1364-79;
7. Cavanaugh KL. Clin Diabetes 2007;25:90-7; 8. Delamater AM. Clin Diabetes 2006;24:71-7

Insulin PK/PD properties have high intra and inter-individual variability
“Rapid acting” insulins have been slower than expected, and last longer than food absorption
“Long acting” insulins have differing PK and PD properties, provide dosing flexibility.
Insulin is not administered in isolation: patient physiology also changes, and dose requirements can vary by up to 100% day to day*
Insulin regimens are challenging for many patients
*Unpublished data, Beta Bionic closed loop program

Modifications that
stabilize the
hexamers
prolong the
duration of action
Modifications that
destabilize the
hexamers shorten
the onset and
duration of action
Insulin is stored within the beta cells as a hexameric complex. After secretion, the
zinc ion disassociates and the insulin is then broken down to individual monomers
which are then active on the receptor.

PK/PD
• Regular insulin has a short duration of action1
• Protamine and zinc formulations delayed onset and extended the duration of action1
• Absorption varied by injection site2
Administration
• Zinc, lente, and ultralente insulins were injected once or twice a day1,3
Efficacy/Hypoglycemia
• Zinc insulin may have been less effective than regular insulin1
• Concerns about immunogenicity of animal insulins
1. Tattersall RB. In: Pickup JC, Williams G. Textbook of Diabetes. 3rd ed.
Malden, MA: Blackwell Science Ltd; 2003:1.1-1.22.
2. Richter B, Neises G. Cochrane Database Syst Rev. 2005;(1):CD003816.
3. Tunbridge FK, et al. Diabet Med. 1989;6:496-501.
Animal insulins transformed an acute,
fatal disease into a manageable
chronic disease1
1920 1930 1940 1960 1970 1980 2000 201019901950 2020
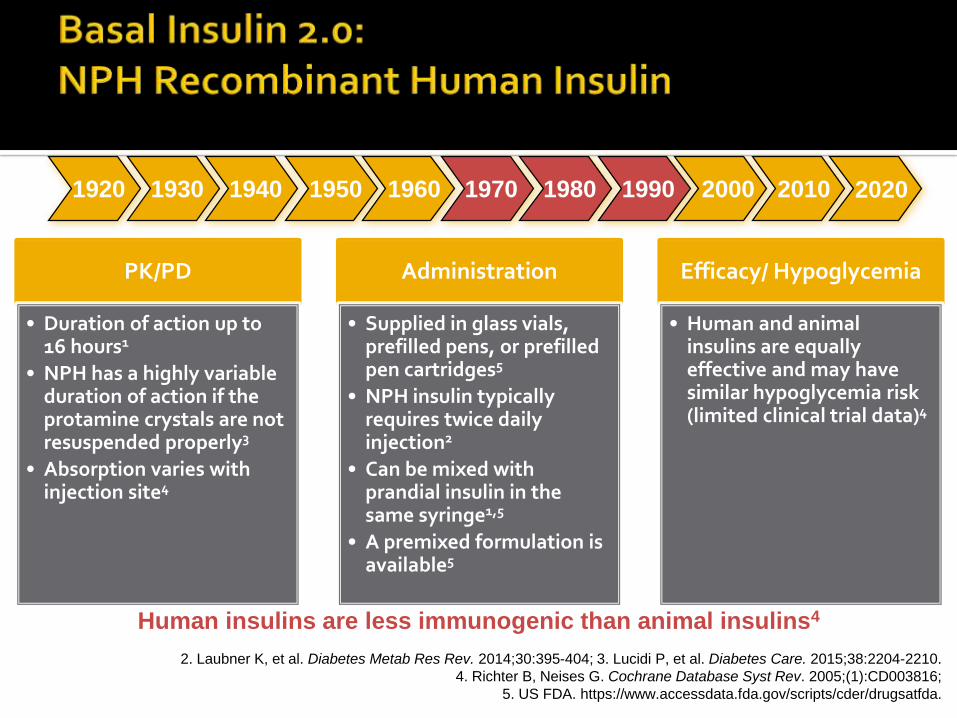
PK/PD
• Duration of action up to 16 hours1
• NPH has a highly variable duration of action if the protamine crystals are not resuspended properly3
• Absorption varies with injection site4
Administration
• Supplied in glass vials, prefilled pens, or prefilled pen cartridges5
• NPH insulin typically requires twice daily injection2
• Can be mixed with prandial insulin in the same syringe1,5
• A premixed formulation is available5
Efficacy/ Hypoglycemia
• Human and animal insulins are equally effective and may have similar hypoglycemia risk (limited clinical trial data)4
1. Skyler JS. In: Lebovitz HE, ed. Therapy for Diabetes Mellitus and Related Disorders. 4th ed.
Alexandria, VA: American Diabetes Association; 2004:207-223.
2. Laubner K, et al. Diabetes Metab Res Rev. 2014;30:395-404; 3. Lucidi P, et al. Diabetes Care. 2015;38:2204-2210.
4. Richter B, Neises G. Cochrane Database Syst Rev. 2005;(1):CD003816;
5. US FDA. https://www.accessdata.fda.gov/scripts/cder/drugsatfda.
Human insulins are less immunogenic than animal insulins4
1920 1930 1940 1960 1970 1980 2000 201019901950 2020

PK/PD
• Duration of action up to 24 hours1
Administration
• Supplied in glass vials, prefilled pens, or pen cartridges3
• Typically requires 1-2 injections/day2
• No premixed insulins including a long-acting basal insulin are approved3,4,a
Efficacy/ Hypoglycemia
• Equivalent efficacy as human insulin5
• Trend toward less nocturnal hypoglycemia than human insulin5
a Aspart 70/30, lispro 50/50, and lispro 75/25 have
components that are intermediate-acting insulin analogues.5
1. Disorders. 4th Skyler JS. In: Lebovitz HE, ed. Therapy for Diabetes Mellitus
2. Laubner K, et al. Diabetes Metab Res Rev. 2014;30:395-404.
3. US FDA. https://www.accessdata.fda.gov/scripts/cder/drugsatfda.
4. Cengiz E, et al. Diabetes Care. 2012;35:690-692.
5. Singh SR, et al. CMAJ. 2009;180:385-397.
The absorption of analogue insulins does not vary with the injection site1
1920 1930 1940 1960 1970 1980 2000 201019901950 2020

PK/PD
• Duration of action up to 42 hours1-3
Administration
• Supplied and administered in prefilled pens with disposable needles3
• 1 premixed formulation is approved3
Efficacy/Hypoglycemia
• Equivalent efficacy as long-acting basal analogues4,5
• Potentially less hypoglycemia than long-acting basal analogues4-6
1. Becker RH, et al. Diabetes Obes Metab. 2015;17:261-267.2. Haahr H, Heise T. Clin Pharmacokinet. 2014;53:787-800.3. US FDA. https://www.accessdata.fda.gov/scripts/cder/drugsatfda.4. Freemantle N, et al. BMJ Open. 2016;6:e009421.
5. Heller S, et al. Diabet Med. 2016;33:478-487.
6. Garber AJ. Diabetes Obes Metab. 2014;16:483-491.
7. Meneghini L, et al. Diabetes Care. 2013;36:858-864.
8. Riddle MC, et al. Diabetes Technol Ther. 2016 Feb 3.
[Epub ahead of print].
Ultralong-acting insulins are more forgiving of variations in the time intervals
between injections and have less variability within and between
patients than long-acting basal analogues6-8
1920 1930 1940 1960 1970 1980 2000 201019901950 2020

Insulin degludec injected
Insulin Degludec1,2
• Dihexamers (69 kDa) form soluble
multihexamers after injection
• Multihexamers (> 5000 kDa)
disassemble slowly
• Monomers are released rapidly
after hexamers disassemble 1. Jonassen I, et al. Pharm Res. 2012;29:2104-2114.
2. Haahr H, Heise T. Clin Pharmacokinet. 2014;53:787-800.
3. http://www.google.com/patents/US20120122774.
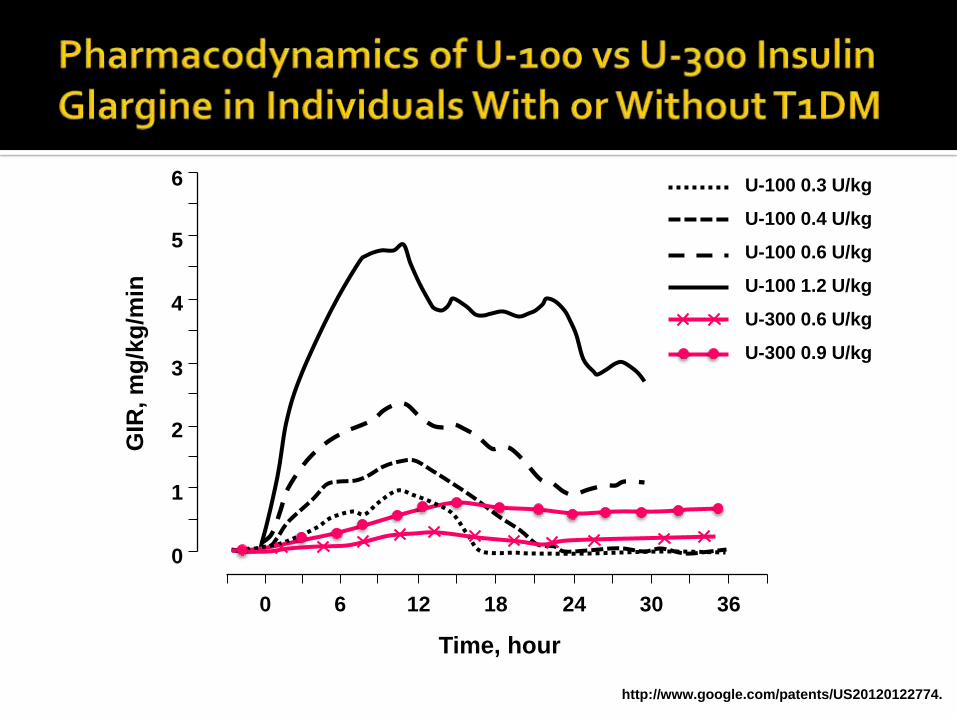
U-300 Insulin Glargine3
• Same amino acid substitutions as
U-100 insulin glargine
• Higher concentration = smaller
injection volume
• Surprising and unexpected
differences in exposure and
activity for U-300 vs U-100 glargine
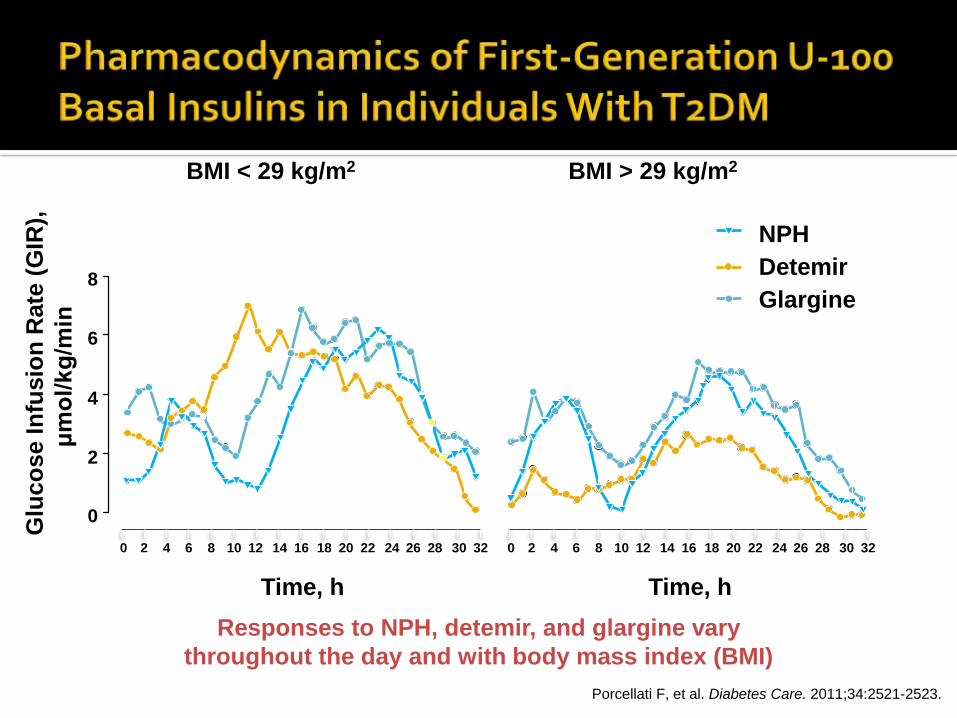
Porcellati F, et al. Diabetes Care. 2011;34:2521-2523.
Responses to NPH, detemir, and glargine vary
throughout the day and with body mass index (BMI)
Glu
co
se In
fus
ion
Rate
(G
IR),
μm
ol/
kg
/min
BMI < 29 kg/m2 BMI > 29 kg/m2
0
Time, h
2 4 6 8 12 14 20 22 26 28 321816 24 3010
0
2
4
6
8
0
Time, h
2 4 6 8 12 14 20 22 26 28 321816 24 3010
NPH
Detemir
Glargine

a Glucose clamp study in patients with T2DM (n = 49).b Glucose clamp study in patients with T2DM (n = 16).
1. Heise T, et al. Diabetes Obes Metab. 2012;14:944-950.
2. Heise T, et al. Diabetes. 2012;61(suppl 1):A91 [abstract 349-OR].
U-100 Formulation1,a U-200 Formulation2,b
GIR
, m
g/k
g/m
in
0
2
3
4
5
1
160 4 8 12 20 24
Time, hours
0.8 U/kg
0.4 U/kg
0.6 U/kg
GIR
, m
g/k
g/m
in0
2
3
4
5
1
160 4 8 12 20 24
Time, hours
0.6 U/kg
GIR
, m
g/k
g/m
in
5
4
3
2
1
0
6
Time, hour
0 6 12 18 24 30 36
http://www.google.com/patents/US20120122774.
U-100 0.3 U/kg
U-100 0.4 U/kg
U-100 0.6 U/kg
U-100 1.2 U/kg
U-300 0.6 U/kg
U-300 0.9 U/kg

Symptomatic and cognitive responses to induced hypoglycemia were similar for DEG and GLAR
Moderately greater counterregulatory response with DEG, but recovery times (BG ≥ 70 mg/dL) were similar
a Volunteers with T1DM, N = 28. Koehler G, et al. Diabetologia. 2014;57:40-49.

a Insulin dosed at 0.6 U/kg in individuals with T1DM. Heise T, et al. Expert Opin Drug Metab Toxicol. 2015;11:1193-1201.

Each generation of basal insulin has offered incremental advances in safety and convenience over the previous generation
Ultralong-acting basal insulins are notable for their:▪ Very long duration of action (> 24 hours)
▪ Flatter pharmacodynamic profiles
▪ Consistent pharmacodynamic action
▪ Throughout the day
▪ On different days
▪ In different patients
Recovery time from hypoglycemia is similar for degludec and U-100 glargine U-300 glargine is metabolized in the same manner as U-100 glargine

1. Owens DR. Diabetes Technol Ther. 2013;15:776-785; 2. Drugs@FDA. http://www.accessdata.fda.gov/Scripts/cder/DrugsatFDA. Accessed October 11, 2015;
3. American Diabetes Association. Diabetes Care. 2016;39(suppl 1):S1-S112; 4. Garber AJ, et al. Endocr Pract. 2016;22:84-113; 5. Hirsch IB, et al. Diabetes. 2015;64(suppl 1):A100 [abstract 385-OR]; 6. Lebovitz HE. Diabetes Rev. 1999;7:139-153.
At diagnosis1
• Benefit especially likely in:
– Treatment-naive individuals with hyperglycemic
symptoms and A1C > 8.5%
– Latent autoimmune diabetes in adults (LADA)
In combination with non-insulin
agents2-5
• Addition to ≥ 2 antihyperglycemic agents when
glycemic control is not at target
• Combinations reduce glycemic variability compared
with insulin-only regimens
In long-duration disease3,6
• Loss of β-cell function is inevitable as T2DM
progresses
• Can be used in any patient (including those with
comorbidities that preclude the use of other agents)

a Meta-analysis of 3 clinical trials in T1DM and T2DM.b P < .05.c Meta-analysis of individuals requiring > 60 U/d TDD in 5 clinical trials in T1DM and T2DM.
Ritzel R, et al. Diabetes Obes Metab. 2015;17:859-867.
Rodbard HW, et al. Endocr Pract. 2014;20:285-292.
ΔA1C, % Nocturnal hypo, EPY
Weight, kg Insulin dose,U/kg/d
DEG –1.2 0.09-1.00 103.3 ± 18.3 0.98 ± 0.36
U-100 GLAR –1.3 0.00-1.60 101.1 ± 17.1 0.92 ± 0.31
RR:
0.48b
ΔA1C, % Severe hypo, % ΔWeight, kg Insulin dose,U/kg/d
U-300 GLAR –1.02 2.3 0.51b 0.85
U-100 GLAR –1.02 2.6 0.79 0.76
U-300 Glargine vs U-100 Glarginea
Degludec vs U-100 Glarginec

U-300 Glargine Degludec
1. Heise T, et al. J Diabetes. 2016;8:132-138.
2. Becker RH, et al. Diabetes Care. 2015;38:637-643.
Steinstraesser A, et al. Diabetes Obes Metab. 2014;16:873-876.
For ultralong-acting insulins, exposure increases over the first days of treatment, then plateaus1
Absorption and elimination equilibrate and no further increase in serum insulin concentration occurs1
Steady state is mostly achieved in:
• 2-3 days for degludec1
• 3-4 days U-300 glargine2
A 57 yo man has been treated with metformin plus MDI for the past 18 years. His fasting C-peptide is 1.6X LLN. Anti-GAD Ab are positive at a very low titer. HbA1c is 6.6%.
Trial of U-300 glargine plus a GLP1-RA plus SGLT2 inhibitor in addition to metformin.
His usual dose of U-100 glargine is 65 units; starting dose of U-300 glargine is 70 units.
A B C D E F
0% 0% 0% 0% 0% 0%

Follow-up visit
▪ “This new insulin does not work as well. I have been increasing the dose with no benefit”
His self-titrated dose is now 140 units daily plus metformin, GLP1-RA and SGLT2 inhibitor.
My response: you have reached the plateau effect, go back to 70 units.
A B C D E F
0% 0% 0% 0% 0% 0%
The major advantage to basal analogue insulin is:
A. Lower cost
B. Flatter profile
C. Better glucose control
A B C
2.56%
66.67%
30.77%

Trial ♦ Randomized, open-label, parallel, 24-week, multicenter, treat-to-target trial
Patient population ♦ N=756
♦ Overweight with inadequate glycemic control (HbA1c >7.5%)
♦ On ≤2 oral agents
Treatment arms ♦ Bedtime glargine or NPH once daily, titrated to a target FBG ≤5.5 mmol/L (<100 mg/dL)
Outcome measures ♦ FBG
♦ HbA1c
♦ Hypoglycemia
♦ % patients reaching HbA1c ≤7% without documented nocturnal hypoglycemia (primary outcome)
♦ Change in body weight and insulin dose
Riddle MC et al. Diabetes Care 2003;26:3080-6
Dose titration weekly +8 units to -4 units depending on FPG. Subsequent studies
have used +2 units every 2 days or +1 unit daily with similar results.
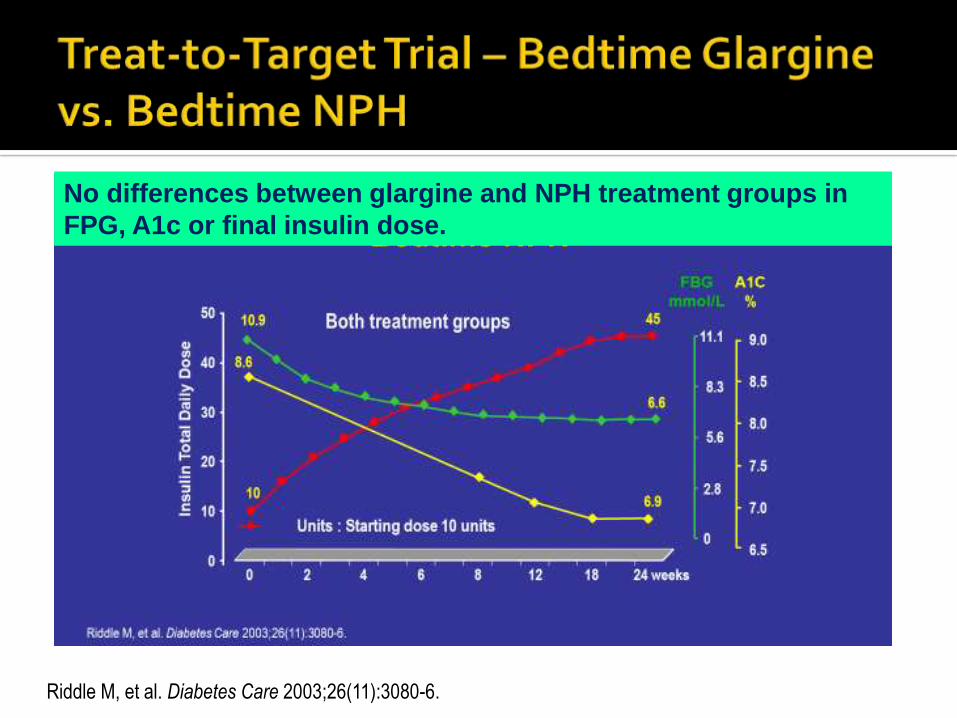
No differences between glargine and NPH treatment groups in
FPG, A1c or final insulin dose.
Riddle M, et al. Diabetes Care 2003;26(11):3080-6.

♦ Significantly lower rates of hypoglycemia, particularly nocturnal hypoglycemia, were seen with insulin glargine compared to NPH; however this may not justify the use of insulin glargine in resource-challenged settings, particularly in T2D patients
Riddle MC et al. Diabetes Care 2003;26:3080-6
Hypoglycemic events/patient-year
NPH (N=389)
Glargine (N=367) p-value
Relative Risk Reduction
Overall hypoglycemia
All symptomatic events 17.7 13.9 .02 21%
Confirmed events ≤4.0 mmol/L 12.9 9.2 <.005 29%
Confirmed events ≤3.1 mmol/L 5.1 3.0 <.003 41%
Nocturnal hypoglycemia
All reported events 6.9 4.0 <.001 42%
Confirmed events ≤4.0 mmol/L 5.5 3.1 <.001 44%
Confirmed events ≤3.1 mmol/L 2.5 1.3 <.002 48%
Copyright © 2016 Eli Lilly and
Company

A 71 yo retired chemistry professor comes to the office for an opinion. She has mild diabetes and takes metformin. She also has sicca syndrome, dry eyes and mouth and a poorly defined rheumatologic condition.
Her A1c is 5.9%, but she reports having high glucoses and leg cramps after hiking. Glucoses can be high after meals and coffee in particular.

Testing shows that her anti-GAD65 Ab is strongly positive, and her C-peptide is low, ~1.3X the LLN for the assay
I recommend insulin, which the patient does not want to start.
6 months later, she complains of worsening leg cramps. She agrees to start insulin,4 units of basal glargine, and her leg cramps resolve.

Although >75% of patients receiving insulin therapy have been reported to have suboptimal glycemic control,1,2 intensifying insulin therapy is often delayed3
aDefined as HbA1c ≥7.5%bNumber of patients included in the analysis: bolus insulin, n=569; premixed insulin, n=24
1. Penfornis A et al. Diabetes Metab 2011;37:440-5
2. Kostev K et al. Diabetes Metab Syndr Obes 2015;8:45-8
3. Khunti K et al. Diabetes Obes Metab 2016;18:401-9
Khunti et al, 20163
(N=11,696) n (%)
Median Time to Insulin
Intensification From
First HbA1c ≥7.5% (years)
HbA1c at Insulin
Intensification
(%, mean ± SD)
Patients eligible for
intensificationa 6072 (51.9) 3.7 NA
Patients who had their
treatment intensified1879 (30.9) 3.7 NA
Bolus insulin 881 (46.9) NA 9.3 ± 1.44b
Premixed insulin 810 (43.1) NA 9.6 ± 1.09b
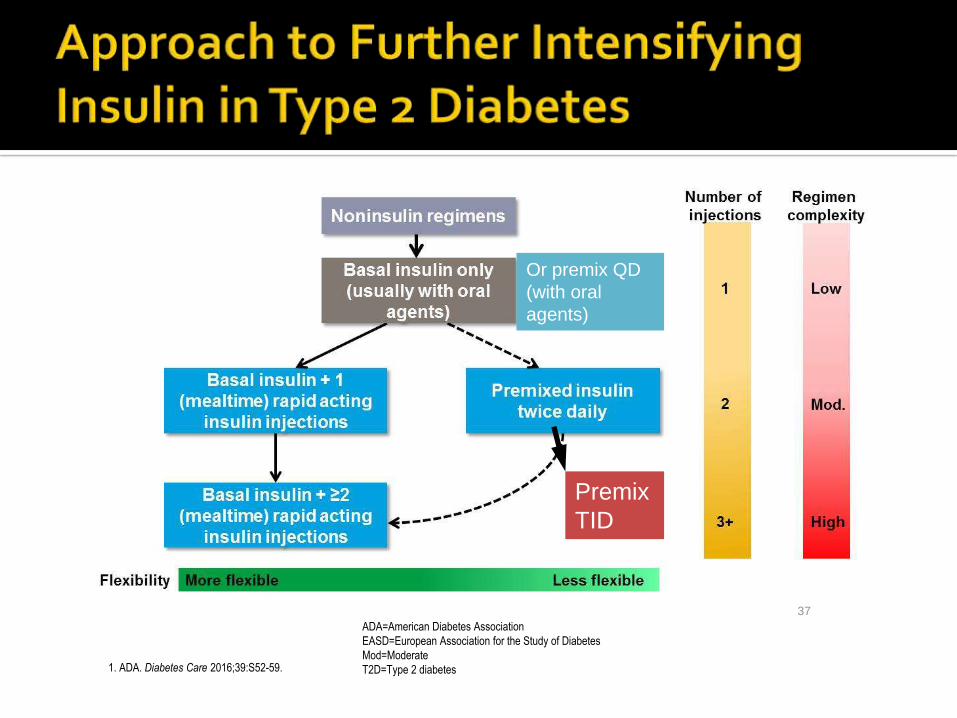
37
1. ADA. Diabetes Care 2016;39:S52-59.
ADA=American Diabetes Association
EASD=European Association for the Study of Diabetes
Mod=Moderate
T2D=Type 2 diabetes
Or premix QD
(with oral
agents)
Premix
TID

Basal insulin
• Always the first step1,2
Prandial dose
(basal + 1 [“basal-plus”])
• Add doses only if goals are unmet on simpler regimen1-8
Prandial dose
(basal + 2 [basal-bolus])
• Add doses per meal size or PPG level3,4
Prandial dose (basal + 3
[basal-bolus])
1. ADA. Diabetes Care. 2016;39(suppl 1):S1-S112; 2. Garber AJ, et al. Endocr Pract. 2016;22:84-113; 3. Bergenstal RM, et al. Diabetes Care. 2008;31:1305-1310; 4. Meneghini L, et al. Endocr Pract. 2011;17:727-736; 5. Davidson MB, et al. Endocr Pract. 2011;17:395-403; 6. Riddle MC, et al. Diabetes Obes Metab. 2014;16:396-402; 7. Rodbard HW, et al. Lancet Diabetes Endocrinol. 2014;2:30-37; 8. Raccah D, et al. Diabetes Metab.
2012;38:507-514.
Step 1
Step 2
Step 3
Step 4
Add GLP1 RA +/- SGLT2i

Long-acting basal insulins have been evaluated in 3 trials
of stepwise addition of prandial insulin doses1-3
After a basal run-in, about half of participants were
unable to reach A1C < 7% with basal insulin only1-3
There was no consistent pattern for the number of
prandial injections needed to reach A1C < 7%1-3
For basal + 3 prandial injections reached through
stepwise intensification, the proportion with A1C < 7%
exceeded 50% in only 1 trial3
(range: 18%2 to 63%3)
Diminishing A1C reductions were observed with each
additional injection1-3
Hypoglycemia and body weight generally increased
with each additional injection1-3
.
1. Meneghini L, et al. Endocr Pract. 2011;17:727-736; 2. Raccah D, et al.
Diabetes Metab. 2012;38:507-514; 3. Rodbard HW, et al. Lancet Diabetes
Endocrinol. 2014;2:30-37.

1. Fulcher GR, et al. Diabetes Care. 2014;37:2084-2090;
2. Rodbard HW, et al. Diabetes Obes Metab. 2016;18:274-280;
3. Garber AJ, et al. Lancet. 2012;379:1498-1507;
4. Drugs@FDA. http://www.accessdata.fda.gov/Scripts/cder/DrugsatFDA.
5. Riddle MC, et al. Diabetes Care. 2014;37:2755-2762.
a A1C < 7% without hypoglycemia in last 12 wk: 21.8% IDegAsp BID
vs 14.9% BIAsp 30 BID, P < .05; BL A1C 8.3-8.4%; b BL A1C 8.3%; c
BL A1C 8.3%-8.4%; d BL A1C 7.7%, no hypoglycemia or weight data
reported; e BL A1C 8.0%, no hypoglycemia or weight data reported; f
BL A1C 8.2%.
1,a 3,c 4,d2,b 4,e 5,f
• Statistically significant reductions in hypoglycemia in many trials (overall1,3;
nocturnal1,3; severe1,2); numerical reductions in all trials (overall and nocturnal1-3,5)
• Equivalent or lower weight gain with ultralong-acting basal insulin1-3,5
Premixed insulin trials Basal-bolus insulin trials
A 54 yo man comes to my office for diabetes management. He reports that he “takes” pre-mixed human 70/30 insulin, 35 units in the morning and 25 units in the evening. He is 77 kg, and has had ESRD for 6 months, receives hemodialysis 3 days per week. HbA1c is 8.7%
Question: Do you take all of this insulin?
Answer: sometimes.
More history: those were his pre-dialysis doses. A few weeks prior to the visit he took both injections, had a severe hypoglycemic reaction, fell and incurred a sub-dural hematoma.

My recommendation:
▪ Start linagliptin
▪ Basal insulin, 0.3 units/kg (20 units) on non-dialysis days, 0.2 units/kg (16 units) on dialysis days
Follow-up: No lows, glucoses are acceptable, A1c is 7.3%

The fast acting insulin Lispro reverses the penultimate proline
and lysine near the carboxyl terminus and weakens the
interaction 200 fold compared to standard human insulin. Insulin
Aspart changes one of the amino acids to a charged structure in
the same region with similar results- Proline is substituted with an
Aspartic acid residue.

The critical nature of the detailed chemical structure of insulin
Human
insulin Asn
Cys
TyrAsn
GluLeuGlnTyrLeuSer
Ile
Cys
Ser
Thr
Cys
CysGln
GluVal
Ile Gly
ProLys
Thr
Tyr
Phe
Phe
Gly
Glu
Arg
GlyCys
LeuValLeuAla Tyr
LeuGluVal
His
Cys
GlySer
Leu
His
Val
Gln
Asn
Phe
S
S S
S
S
S
Thr
Asn
Cys
TyrAsn
GluLeuGlnTyrLeuSer
Ile
Cys
Ser
Thr
Cys
CysGln
GluVal
Ile Gly
ProLys
Thr
Tyr
Phe
Phe
Gly
Glu
Arg
GlyCys
LeuValLeuAla Tyr
LeuGluVal
Asp
Cys
GlySer
Leu
His
Val
Gln
Asn
Phe
S
S S
S
S
S
Thr
Asn
Cys
TyrAsn
GluLeuGlnTyrLeuSer
Ile
Cys
Ser
Thr
Cys
CysGln
GluVal
Ile Gly
AspLys
Thr
Tyr
Phe
Phe
Gly
Glu
Arg
GlyCys
LeuValLeuAla Tyr
LeuGluVal
His
Cys
GlySer
Leu
His
Val
Gln
Asn
Phe
S
S S
S
S
S
Thr
Insulin
aspart
Insulin
B10-Asp
2x insulin receptor binding
2x metabolic activity in vitro
1/10 th receptor dissociation rate
6x IGF-1 receptor binding
10x mitogenicity (SAOS cells)
Mammary tumours in rats
Kurtzhals et al, Diabetes, 2000
Hansen et al, Diabetologia, 2011

Katzung BG. Basic and Clinical Pharmacology. 10th ed. 2007
Note that the y-axis is dose dependent and may not be comparable between short- and long-acting insulins
NPH, neutral protamine Hagedorn
>24-hr basal Degludec
U-300
glargine
Degludec

The Diabetes Control and Complications Trial Research Group. Diabetes 1997;46:271-86
HbA1c, glycosylated hemoglobin; T2DM, type 2 diabetes mellitus

1. UKPDS Group. Lancet 1998;352:837-53; 2. ADVANCE Collaborative Group. N Engl J Med 2008;358:2560-72; 3. Action to Control
Cardiovascular Risk in Diabetes Study Group. N Engl J Med 2008;358:2545-59; 4. Duckworth W et al. N Engl J Med 2009;360:129-39
aIntensive glycemic control was defined differently in these trials; bhypoglycemia requiring any assistance in glucose-lowering trials
Conv, conventional therapy; Gly, glibenclamide; HbA1c, glycosylated hemoglobin; HR, hazard ratio; Int, intensive therapy; Std, standard therapy;
T2DM, type 2 diabetes mellitus; UKPDS, United Kingdom Prospective Diabetes Study; VADT, Veterans Affairs Diabetes Trial



*p<0.05. Error bars: ± standard error (mean). The conversion factor between mmol/L and mg/dL is 0.0555. PPG increment changes from baselines were analysed using a linear model.CI, confidence interval; ETD, estimated treatment difference; PG, plasma glucose; PPG, postprandial glucose.1. Russell-Jones D et al. Diabetes Care 2017;40:943–950; 2. Mathieu C et al. Diabetologia 2017;60(Suppl 1):S314.
1-h ETD: −0.91 mmol/L (95% CI: −1.40; −0.43)*
2-h ETD: −0.42 mmol/L (95% CI: −1.11; 0.27)
PG
(mg/d
L)
Bolus dose
0.1 U/kg Time (min)
60 120 180 2400
1-h ETD: –1.18 mmol/L (95%CI: –1.65; –0.71)*
2-h ETD: –0.67 mmol/L (95%CI: 1.29; –0.04)*
Bolus dose
0.1 U/kg Time (min)
PG
(m
mo
l/L) PG
(mg/d
L) P
G (
mm
ol/L)
Faster aspart
(mealtime)
IAsp
(mealtime)
60 120 180 2400
0
1
2
3
4
5
6
7
0
1
2
3
4
5
6
7
0
18
36
54
72
90
108
126
0
18
36
54
72
90
108
126
* *
*
Week 52Week 26
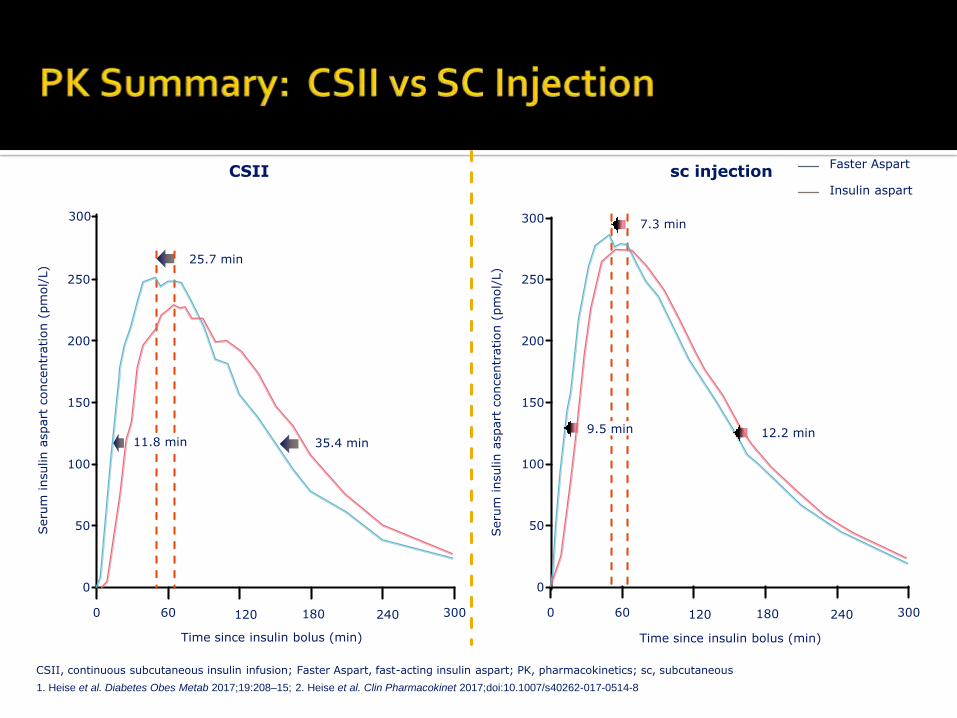
CSII sc injection
50
0
150
100
200
0
Seru
m insulin a
spart
concentr
ation (
pm
ol/
L)
250
300
Time since insulin bolus (min)
60 120 180 240
25.7 min
11.8 min 35.4 min9.5 min
7.3 min
12.2 min
50
0
150
100
200
0
Seru
m insulin a
spart
concentr
ation (
pm
ol/
L)
250
300
Time since insulin bolus (min)
60 120 180 240
300300
CSII, continuous subcutaneous insulin infusion; Faster Aspart, fast-acting insulin aspart; PK, pharmacokinetics; sc, subcutaneous
1. Heise et al. Diabetes Obes Metab 2017;19:208–15; 2. Heise et al. Clin Pharmacokinet 2017;doi:10.1007/s40262-017-0514-8
Faster Aspart
Insulin aspart

Boss. J Diabetes Sci Tech 2012; 6:773-9
The area under the curve
for both the insulin and the
GIR are not the same! The
Peak GIR is similar but
occurs earlier at 45
minutes versus 120
minutes
Higher dose of
technosphere insulin may
be required to manage
PPG

The pharmacokinetic (PK)/ (PD) profiles
for orally inhaled technosphere (TI) 8
units relative to subcutaneously
administered insulin lispro 8 units from a
study in 12 patients with type 1 diabetes.
Data are baseline-corrected serum
insulin concentrations after
administration of TI insulin or
subcutaneous insulin lispro and GIR
rates.
The glucose infusion rate utilizing a
glucose clamp is clearly different again
with the peak occurring at 53 minutes
versus 120 minutes with the RAA insulin
lispro.
Insulin lispro (8 units)
Afrezza® (8 units)
Insu
lin (m
U/m
L)
Time (minutes)
Baseline-corrected serum insulin concentrations and GIR after administration of technosphere
or subcutaneous insulin lispro in type 1 diabetes patients (N=12)
Data from Package insert Afreeza
.
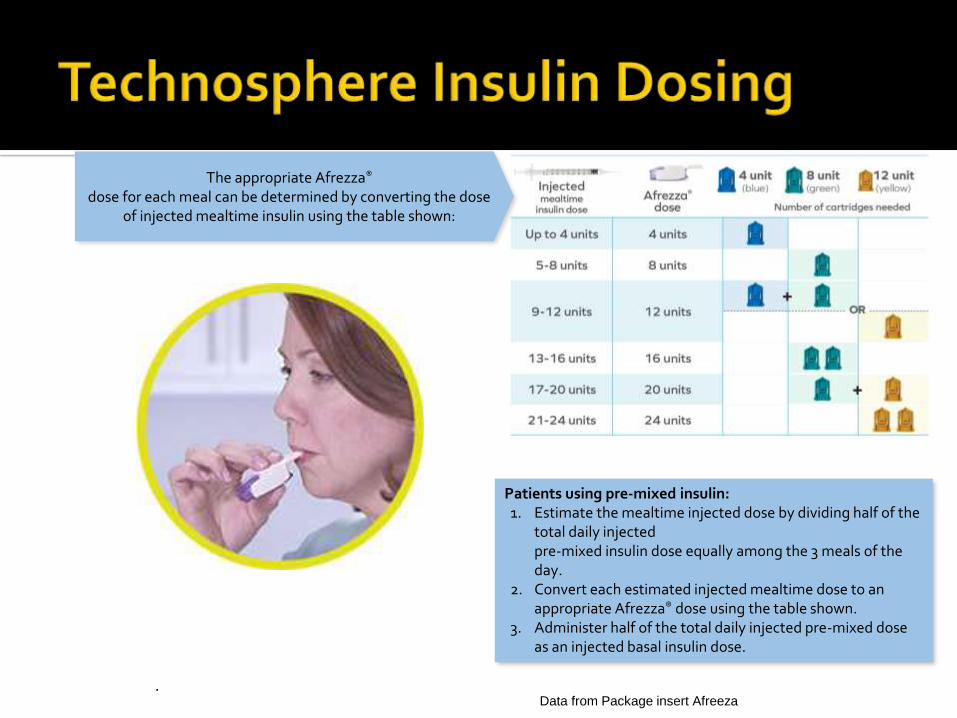
The appropriate Afrezza®
dose for each meal can be determined by converting the dose of injected mealtime insulin using the table shown:
Patients using pre-mixed insulin: 1. Estimate the mealtime injected dose by dividing half of the
total daily injected pre-mixed insulin dose equally among the 3 meals of the day.
2. Convert each estimated injected mealtime dose to an appropriate Afrezza® dose using the table shown.
3. Administer half of the total daily injected pre-mixed dose as an injected basal insulin dose.
Data from Package insert Afreeza

A 43 yo man who works as an auto mechanic says that he cannot test his glucose or take insulin during the day because his hands are too dirty. He also is wary of increasing his basal insulin because of hypoglycemia. His A1c is 8.7%.
I recommend inhaled insulin and a continuous glucose monitor, which he obtains. His A1c drops to 7.3% without hypoglycemia, and with less effort.

Dance website 56

Rapid acting insulin analogues have provided
A. Mealtime insulin coverage
B. More flexibility with dosing
C. Perfect glucose control
D. A and B
A B C D
7.08%10.62%
3.54%
78.76%

• Generally
reserved for
patients taking
>200 units daily
• Dose is 1:1
• Given bid or tid
• Reduces volume,
injections and
may improve
compliance

A 53 yo woman comes to me for a second opinion. She has had diabetes for 12 years, and is now treated with metformin, a GLP1 RA, an SGLT2 inhibitor and insulin through an insulin pump. She weighs 92 kg and takes 230 units of insulin.
On examination, she has thin extremities and central obesity
Her A1c is 6.8%, she is very compliant.
Should I consider U-500 insulin?

My recommendations:▪ Lower the carbohydrates in your diet to <150 grams to
start, then <100 grams▪ Lower calories to <1200▪ Exercise▪ Consider bariatric surgery
9 months later: ▪ Weight loss of 12 kg▪ Insulin dose is down to 68 units, A1c is 6.5%▪ Pump is stopped and one injection of basal insulin is
started.

12 wk study in patients with uncontrolled HbA1c values on MET or MET + SU (MET was continued; SU was stopped)
Human 70/30 was given 30 minutes before supper; BiAsp 70/30 10 minutes before supper; and NPH was given at bedtime
At endpoint, there was no difference in HbA1c (-1.1 to 1.3%) between the treatment groups
Kilo C et al. J Diabetes Complications 2003
Analog BiAsp 70/30, 70% NPL (like NPH); 30% rapid-acting aspart; NPH, neutral
protamine Hagedorn intermediate-acting; MET, metformin; SU, sulfonylurea

188 patients randomized to either treat-ment with a third oral agent (SU+MET+ TZD) vs starting human 70/30 BID (0.75 units/kg/day 2/3 AM 1/3 PM 30 min AC)
Titration was +10% to appropriate dose every other day based on 2-3 self-monitored PG values measured per day
Endpoint 70/30 dose was 63+26 units/day
Comparative cost was 1/3 less with the 70/30 insulin
Schwartz S et al. Diabetes Care 2003;26:2238-43

♦ Two observational studies showed similar glycemic control with premix and basal-bolus insulin regimens
▪ TREAT: In this 24-month observational study mean change in HbA1c from baseline was -2.6% for premix and -2.7% for basal-bolus1
▪ CREDIT: In this 4-year observational study mean change in HbA1c from baseline was -2.1% for premix and -1.9% for basal-bolus 2
♦ Two meta-analyses of RCTs demonstrated similar efficacy and hypoglycemia rates between premix and basal-bolus regimens for reducing HbA1c in patients initiating3,4 and intensifying4 insulin therapy
CREDIT=Cardiovascular Risk Evaluation in people with type 2 Diabetes on Insulin Therapy; RCT=randomized controlled trials;
TREAT=TREATment factors and costs associated with insulin therapy in patients with type 2 diabetes
1. Oguz A et al. Curr Med Res Opin 2013;29:911-202. Home PD et al. Diabetes Res Clin Pract 2015:108:350-9
3. Wang C et al. Diabet Med 2015;32:585-944. Giugliano D et al. Endocrine 2016;51:417-28

Insulin Update: What’s wrong with insulin and how will new products
and technology fix it?
Insulin is too expensive
• Enter generic insulin, “biosimilar” insulins
• Human insulin
Long-acting insulins do not act long enough
• Degludec
• Glargine U-300
Short-actin insulins are not rapid enough
• Technosphere, inhaled insulin
• Rapid acting aspart and faster lispro (in development)

Insulin Update: What’s wrong with insulin and how will new products
and technology fix it?
Too many units need to be given
• U-500 human R
• U-300 insulin glargine
• U-200 degludec
• U-200 insulin lispro
Insulin causes hypoglycemia
• Smart insulin (not currently in development)
• Closed loop and dual chambered pumps
• Continuous glucose monitoring
• Improved glucagon

Rege NK et. al. Curr opinion Endocrinol Diabetes Obesity 2017, 24: 267-78
Cartoon representation of derivatization of the insulin molecule in glucose-responsive insulin (GRI)
technology. The insulin hormone comprises two polypeptide chains that are designated ‘A’ and ‘B’ and
are connected by two disulfide linkages spanning residues A7 and B7 and A20 and B19. (a) Sites that
have been modified in molecular GRI development have been highlighted in colors corresponding to GRI
systems illustrated in boxes.
Smart insulin

Advances in insulin structure and biochemistry have improved diabetes therapy for persons with both T1DM and T2DM.
Biosimilar insulins are now available, though cost reductions are yet to be realized in all areas.
New routes of delivery and insulin delivery devices, including closed loop systems, mimic normal physiology safely.
Smart insulin remains a concept.
Heat stable insulin
Improved management systems for impaired patients
Non-injection administration systems
Improved access to any insulin, monitoring supplies and education. This requires political support.

THANK YOU
Questions?