Embed Size (px)
Citation preview

Decreasing Trends in Mean HbA1cAre Not Associated WithIncreasing Rates of SevereHypoglycemia in Children: ALongitudinal Analysis of TwoContemporary Population-BasedPediatric Type 1 DiabetesRegistries From Australia andGermany/Austria Between1995 and 2016Diabetes Care 2019;42:1630–1636 | https://doi.org/10.2337/dc18-2448
OBJECTIVE
To investigate temporal trends in glycemic control and severe hypoglycemia ratesfor pediatric patientswith type 1diabetes from1995 to 2016by analyzing data fromthe longitudinal, prospective, population-based German/Austrian (Diabetes Pa-tient History Documentation [DPV]) and Western Australian (Western AustralianChildren’s Diabetes Database [WACDD]) diabetes registries.
RESEARCH DESIGN AND METHODS
Patients diagnosed with type 1 diabetes aged <15 years were identified from theDPV (N = 59,883) and WACDD (N = 2,595) registries and data extracted for all clinicvisits occurring between 1995 and 2016, inclusive. Mean HbA1c and severehypoglycemia (self-reported loss of consciousness/convulsion) rates were calcu-lated per 100 patient-years.
RESULTS
Between 1995 and 2016, the annual mean HbA1c decreased from 8.3 to 7.8% in theDPV cohort and from 9.2 to 8.3% in the WACDD cohort. Over the same period, thesevere hypoglycemia rate decreased by an annual average of 2% (relative risk 0.983[95% CI 0.981, 0.986]) in the DPV cohort and 6% (relative risk 0.935 [95% CI 0.934,0.937]) in the WACDD cohort. Concomitant decreasing trends in both HbA1c andsevere hypoglycemia rates were observed in boys and girls, all age-groups, andinjection therapy/pump regimen groups.
CONCLUSIONS
Over the past two decades, there have been concurrent improvements in HbA1c
and decreasing severe hypoglycemia rates in two contemporary, longitudinal,population-based pediatric cohorts of type 1 diabetes. Translation of these datainto clinical practice and patient education may reduce fear of hypoglycemia andenable better glycemic control.
1Telethon Kids Institute, University of WesternAustralia, Perth, Western Australia, Australia2Central Institution for Biomedical Engineering,Institute of Epidemiology and Medical Biometry,University of Ulm, Ulm, Germany3German Center for Diabetes Research,Munchen-Neuherberg, Germany4Department of Diabetes and Endocrinology,Perth Children’s Hospital, Perth, Western Aus-tralia, Australia5Department of Pediatrics, Medical University ofInnsbruck, Innsbruck, Austria6Division of Endocrinology and Diabetes, Med-ical Faculty, RWTH Aachen University, Aachen,Germany
Corresponding author: Aveni Haynes, [email protected]
Received 28 November 2018 and accepted 28May 2019
A.H. and J.M.H. are joint first authors.
E.A.D. and R.W.H. are joint senior authors.
© 2019 by the American Diabetes Association.Readers may use this article as long as the workis properly cited, the use is educational and notfor profit, and the work is not altered. More infor-mation is available at http://www.diabetesjournals.org/content/license.
Aveni Haynes,1 Julia M. Hermann,2,3
Helen Clapin,4 Sabine E. Hofer,5
Beate Karges,6 Timothy W. Jones,1,4
Elizabeth A. Davis,1,4 and
Reinhard W. Holl,2,3 for the WACDD and
DPV registries
1630 Diabetes Care Volume 42, September 2019
CLINCARE/ED
UCATION/N
UTR
ITION/PSYCHOSO
CIAL

The landmark Diabetes Control and Com-plications Trial (DCCT) demonstrated theeffect of good glycemic control in min-imizing the risk for diabetes-relatedcomplications (1–3). However, a majoradverse finding of the DCCT was an in-verse association between the risk ofsevere hypoglycemia (SH) and lowerglycemia, with patients treated inten-sively experiencing a threefold higherSH rate compared with those receivingconventional treatment (4). Followingpublication of these findings, individualswith type 1 diabetes and their clinicianshave faced the challenge of loweringglycemic targets against the increasedrisk of SH, which is not only potentiallyfatal but also associated with longer-termconsequences itself (5–9).Over the past two decades, consider-
able advances have been made in di-abetes therapies and technologies (10).In conjunction with these technologicaladvances and newer insulins, changes inpatient education over the past decadesinclude the use of multidisciplinaryteams, education of families and groups,the use of carbohydrate counting, andspecific education on hypoglycemiaawareness. These changes in usual di-abetes care have affected both glycemiccontrol and the risk of SH (11–15).Both population- and single diabetes
clinic–based studies in several countrieshave examined the association betweenglycemic control and SH rates over recentdecades. The majority of these have re-ported improvements in metabolic controlwithout a concomitant increase in SH rates(16–21). Such longitudinal observations sug-gest that the inverse association previouslyreported from the DCCT has weakened in
contemporary cohorts of children andadolescents diagnosed with type 1 diabe-tes and that the use of modern diabetestherapies and technologies may enablelower glycemic targets to be achieved,without increasing the incidence of SH(22). This paradigm shift in the contem-porary relationship between glycemiccontrol and risk of hypoglycemia hasthe potential to remove barriers suchas fear of hypoglycemia for parents,but requires a change in education andclinical practice for health care profes-sionals. However, confirming the changein risk of hypoglycemia with lower HbA1cin more than one cohort using the samestudy design and longitudinal data isnecessary before translation of thesenew data begins.
Recently, a cross-sectional study of chil-dren and adolescents diagnosed withtype 1 diabetes aged,15 years attendingdiabetes clinics during 2011 to 2012, iden-tified from the Diabetes Patient HistoryDocumentation (DPV), Western AustralianChildren’s Diabetes Database (WACDD),and T1D Exchange Clinic (T1DX) registries,found no association between contem-porary rates of SH and mean HbA1c (23).Longitudinal data on glycemic control andSH events are routinely collected at threemonthly clinic visits attended by patients inGermany/Austria and Western Australiafrom the time of diagnosis until the ageof 18 years. Therefore, this study aimed tofurther examine the relationship betweenglycemic control and SH in these twopopulation-based pediatric cohorts oftype 1 diabetes, undertaking a retrospec-tive longitudinal analysis of these data anddetermining the temporal trends between1995 and 2016.
RESEARCH DESIGN AND METHODS
Study PopulationThe study population was all children andadolescents diagnosed with type 1 di-abetes aged ,15 years identified fromthe DPV database in Germany and Aus-tria and the WACDD in Western Australia.The DPV, established in 1995, and theWACDD, established in 1987, are bothprospective, longitudinal, population-basedregistries that have been previously de-scribed in detail and have estimated case-ascertainment rates of 80% and .99%,respectively (24,25). Data obtained viaclinicians during routine, quarterly di-abetes clinic visits are recorded in theDPV and WACDD, including HbA1c andthe number of self-reported episodes ofSH since the last visit. As most patientsin both of these populations attenddiabetes clinics approximately every3 months, this minimizes the risk ofrecall bias for self-reported SH events(26).
Record Selection CriteriaData for eligible cases were extracted forall clinic visits between 1 January 1995and 31 December 2016, inclusive. Re-cords for data analysis were restrictedto patients aged ,18 years with a du-ration of diabetes $12 months.
Definition of SHSH was defined according to currentInternational Society for Pediatric andAdolescent Diabetes guidelines as a hy-poglycemic episode resulting in loss ofconsciousness and/or seizure (27). Thesum of SH events and observation timewas calculated for each patient andcalendar year.
Table 1—Demographic and clinical characteristics of study participants by source registry
DPV WACDD
Total cases (N) 59,883 2,595
Total observation time (patient-years) 296,179 16,063
Boys (%) 52 51
Mean age at diagnosis 6 SD (years) 8.0 6 3.8 8.1 6 3.9
Mean number of visits/year 6 SD (N) 3.7 6 1.8 3.3 6 0.8
Mean follow-up time 6 SD (years) 4.3 6 3.5 5.4 6 3.7
Mean HbA1c 6 SD (%) 8.0 6 1.4 8.4 6 1.2
Mean HbA1c (mmol/mol) 64 68
Median HbA1c (IQR) (%) 7.8 (7.1–8.7) 8.2 (7.5–9.0)
Median HbA1c (IQR) (mmol/mol) 62 (54–72) 66 (58–75)
SH rate per 100 patient-years (95% CI)* 4.0 (3.9, 4.1) 10.0 (9.1, 10.9)
Annual percent change in mean SH rate; RR (95% CI)* 22%; 0.983 (0.981, 0.986), P , 0.001 26%; 0.935 (0.934, 0.937), P , 0.001
*Poisson regression estimate.
care.diabetesjournals.org Haynes and Associates 1631

Glycemic ControlIndividual mean and median HbA1c werecalculated for each calendar year offollow-up using all available HbA1c valuesfor those individual contributing obser-vations for that year.
CovariatesData were also extracted for age, sex,duration of diabetes, and insulin treat-ment regimen. For each calendar year,patients were categorized into groupsaccording to age at the last visit in thecalendar year (,6 years, 6 to ,13years, and 13 to ,18 years), durationof diabetes (2 to #5 years and .5years), and treatment regimen (injec-tions or continuous subcutaneous in-sulin infusion).
Statistical AnalysesFor each patient included in the study,the mean annual HbA1c, total number ofSH events, and total observation time
were calculated for each calendar year ofthe study period. To calculate the SH rateper category, the total number of SHevents of patients within the categorywas used as the numerator and theirsummed total observation time used asthe denominator. The resulting rate wasthen multiplied by 100 to provide the SHrate per 100 patient-years. Similarly, theannual mean HbA1c for each categorywas estimated as the mean of individualmean HbA1c for all patients in that cat-egory and calendar year.
Longitudinal trends in mean HbA1c andSH rates were analyzed using negativebinomial regression to account for over-dispersion of SH events (28). As indi-viduals could contribute to multiplecalendar years in the trend analysis,a random intercept for patient wasincluded in the regression models.Dependent on the category being ana-lyzed, trend analysis included adjust-ment for sex, age-group, duration of
diabetes group, and insulin regimen, asappropriate.
A two-tailed P value ,0.05 was con-sidered statistically significant, with theTukey-Kramer method for correction ofP values applied for multiple compari-sons. All analyses were performed usingSAS version 9.4 (SAS Institute, Cary, NC).
EthicsThe study was performed according tothe principles of the Declaration of Hel-sinki for medical research and approvedby the ethics committees of each registrycenter, as well as the local institutionalreview boards of participating centers.
Role of Funding SourceThe DPV registry is supported by theGerman Center for Diabetes Research(grant 82DZ01402). This funding sourcedid not have any involvement in the studydesign, analysis, interpretation of studyfindings, or manuscript preparation.
RESULTS
A total of 59,883 and 2,595 cases from theDPV andWACDD registries, respectively,were included in the study, contributinga total observation time of 312,222patient-years from 1 January 1995 to 31December 2016 (Table 1). Demographiccharacteristics were similar for the studycohorts from both registries, with justover 50% of cases being boys (52% in DPVand 51% in WACDD) and a mean age atdiagnosis of 8 years (Table 1). The meanduration of study follow-up was 4.3 and5.4 years, with patients attending anaverage of 3.7 and 3.3 clinic visits peryear, in the DPV and WACDD studycohorts, respectively (Table 1). The over-all mean unadjusted HbA1c for the wholestudy period was 8.01% (95% CI 7.99,8.02) for the DPV cohort and 8.35% (95%CI 8.31, 8.40) for theWACDD cohort (P,0.001). The overall unadjusted SH rate forthe whole study period was 4.0 (95% CI3.9, 4.1) per 100 patient-years for theDPV cohort compared with 10.0 (95% CI9.1, 10.9) per 100 patient-years in theWACDD cohort (Table 1).
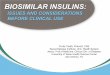
Temporal Trends in Annual MeanHbA1c and SH RateWhen analyzed over the study period, asignificant decreasing trend was ob-served in both mean HbA1c and SHrate for both cohorts (Fig. 1). From1995 to 2016, themeanHbA1c decreased
Figure 1—Mean HbA1c (%) and SH rate (per 100 patient-years) by calendar year from 1995 to2016 for study participants in the DPV and WACDD diabetes registries. Dashed line indicates meanHbA1c (%) with 95% CI; solid line indicates SH rate (per 100 patient-years) with 95% CI.
1632 Concurrent Improvements in HbA1c and SH Rates Diabetes Care Volume 42, September 2019

from 8.3 to 7.8% in the DPV cohort andfrom 9.2 to 8.3% in the WACDD cohort. Inconjunction with the decreasing trend inHbA1c, a statistically significant decreas-ing trend was observed in the SH rates inboth cohorts. After adjusting for sex, age-group, and diabetes duration group, themean annual SH rate decreased by anaverage of 2% (relative risk [RR] 0.983[95%CI 0.981, 0.986];P,0.001) per yearover the study period in the DPV cohortand 6% (RR 0.935 [95% CI 0.934, 0.937];P , 0.001) per year in the WACDD cohort(Fig. 1).When examined by sex (Fig. 2) or age-
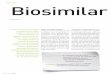
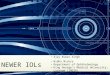
group (Fig. 3), similar decreasing trendsin both the annual mean HbA1c and SHrates were observed in all subgroups.Due to the small number of SH events inpatients aged ,6 years in the WACDDcohort, this age-group was excluded inthe analyses stratified by age-group forthis cohort (Fig. 3).To further examine the relationship
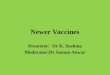
between HbA1c and SH over time, recordswere categorized into four time pe-riods (1995–2001, 2002–2006, 2007–2011,and 2012–2016) and the mean adjustedSH rate for each time period and HbA1cgroup was estimated using negative bi-nomial regression as described previously.
For both the DPV and WACDD cohorts, adecrease in the estimated marginal meanSH rate was observed in each HbA1c groupfor each successive time period (Fig. 4).
CONCLUSIONS
This study reports decreasing trends inmean HbA1c and SH rates having oc-curred simultaneously over the past20 years in two independent, population-based pediatric cohorts with type 1 di-abetes receiving usual care in differentparts of the world. This observation is incontrast to findings reported by the DCCTin the late 1990s, in which decreasingHbA1c levels were associated with a sig-nificant increased risk of SH (4). Morerecently, a longitudinal follow-up studyof the DCCT/Epidemiology of DiabetesInterventions and Complications (EDIC)cohort reported a continued 13–15% in-creased risk of SH for every 10% decreasein HbA1c during EDIC (12).
However, several other studies, notablyin pediatric patients with type 1 diabetes,have reported changes in the relationshipbetween HbA1c and SH rates over the pastfew decades. In 2004, a Western Aus-tralian study reported improvements inHbA1c having occurred over the previousdecade without a concurrent increase in
SH (16). In 2007, a U.S.-based study an-alyzing two small type 1 diabetes cohortsidentified from the same single pediat-ric diabetes clinic 5 years apart reportedthat intensification of diabetes manage-ment during the 5 years between thetwo cohorts studied had resulted notonly in lowered HbA1c, but also in areduction of SH rates (17).More recently,in Denmark, lowering of HbA1c at thepopulation level was reported to haveoccurred without a corresponding in-crease or change in SH rates (19,20).Consistent with this, analysis of DPVshowed that compared with the period1995–2003, in 2004–2012, low HbA1cwas a minor risk factor for SH in this co-hort (21). A cross-sectional analysis of pe-diatric patients attending diabetes clinicsbetween 2011 and 2012 identified fromthe U.S. T1D Exchange Clinic, DPV, andWACDD registries found no associationbetween HbA1c and SH rates in thesepediatric cohorts of type 1 diabetes (23).
Concurrent decreasing trends in HbA1cand SH rates have been reported in in-dependent studies of theWACDD (29,30)and DPV (18,31) pediatric type 1 diabetescohorts over the past decades. The DPVand WACDD cohorts represent pediatrictype 1 diabetes cohorts receiving usual
Figure 2—Mean HbA1c (%) and SH rate (per 100 patient-years) by calendar year from 1995 to 2016 for study participants in the DPV and WACDDdiabetes registries by sex. Dashed line indicates mean HbA1c (%) with 95% CI; solid line indicates SH rate (per 100 patient-years) with 95% CI.
care.diabetesjournals.org Haynes and Associates 1633

care in developed nations on separatecontinents, with different models of di-abetes care and national governmentfunding for diabetes-related technolo-gies. For example, Western Australia has acentralized model of care with pediatricpatients diagnosed with diabetes man-aged at a single center in one tertiarypediatric hospital. All patients are there-fore managed according to the sameclinical protocol by the same multidisci-plinary team, which includes diabeteseducators. Data from the DPV relateto patients treated at multiple centers,by different diabetes specialists and
multidisciplinary teams, with potentialvariation in their models of clinical care.In addition, unlike Germany/Austria, al-though Australia has a national publichealth service, access to medical devicessuch as insulin pumps and continuousglucose monitoring is not necessarilyavailable to patients free of charge,meaning there may be some disparity inaccess to latest technologies by patientsocioeconomic status. Therefore, thisinternational collaborative study was un-dertaken to analyze the longitudinal dataavailable from these two separate, in-dependent diabetes registries together.
This study reports that over the pastseveral decades, there has been an over-all decrease in mean HbA1c in both ofthese independent pediatric type 1 di-abetes cohorts, without a correspondingincrease in SH rates. Of interest, themean HbA1c and SH rates observed inthe DPV cohort were lower than thoseobserved in theWACDD across the studyperiod. In addition, the pattern of declinein mean HbA1c in the WACDD cohortappears steeper in the earlier part of thestudy period followed by a more grad-ual and stable decline thereafter. Im-portantly, this is not explained by any
Figure 3—Mean HbA1c (%) and SH rate (per 100 patient-years) by calendar year from 1995 to 2016 for study participants in the DPV and WACDD diabetesregistries by age-group. Dashed line indicates mean HbA1c (%) with 95% CI; solid line indicates SH rate (per 100 patient-years) with 95% CI.
1634 Concurrent Improvements in HbA1c and SH Rates Diabetes Care Volume 42, September 2019

differences in data collection or complete-ness during the study period time, as theWACDD was established in 1987 and waswell established by 1995 when this studyperiod commenced. The observationaldata analyzed in this study were not setup to infer any causal relationships be-tween specific changes in diabetesmanagement/therapies and ensuingchanges in HbA1c and/or severe hypoglyce-mic risk over time, including any associa-tions that could account for the change inslope of decline observed in theWACDD.The concurrent decreasing trends in
HbA1c and SH rates observed in thislongitudinal study of two independentcohorts provide strong evidence thatthe relationship between HbA1c and SHrates has changed in developed countries(19,21,23) where modern diabetes ther-apies and technology are being used totreat pediatric patients with type 1diabetes by health professionals inwell-developed pediatric diabetes careprograms. Advances in diabetes therapiesand technologies over the past decadesincluding insulin analogs, pump therapy,continuous glucose monitoring, andpatient/carer education, together with in-creasing clinical experience in the use ofthese diabetes management tools, arelikely to have resulted in reduction inHbA1c without an increase in SH rates(10,13,32,33). Importantly, reduced SHrates over time were observed in allHbA1c groups, including the lowest HbA1cgroup, in both of the cohorts analyzed inthis study.The strengths of this study are its use
of data from prospective, population-
based diabetes registries with highcase ascertainment levels of .90% forthe DPV and .99.9% for the WACDD withconsistent data collection from routineclinical visits attended throughout thestudy period for all participants. Thecompleteness of these population-basedregistries minimizes the risk of selectionbias, enabling an accurate analysis to beundertaken with results that are gener-alizable to all children and adolescentsdiagnosed with type 1 diabetes in thesepopulations. Furthermore, both the DPVand WACDD are well-established longi-tudinal registries with data on SH eventssystematically and routinely collected atdiabetes clinic visits for.20 years. Mostpatients in both of these cohorts at-tended clinic visits every 3 months, whichminimizes the risk of recall bias for self-reported SH events in this study. Animportant strength of this report isthat the data provide information onoutcomes over an extended 22-yeartime period in population-based samplesfrom the real world, in contrast to datafrom clinical trials in which limitationsto interpreting changes in hypoglycemiarates include potential biases from par-ticipant selection and trial effects.
It is important to note that our studyfindings relate to population-level HbA1cand SH rates and cannot account forindividual-level variation in significantrisk factors (e.g., history of previoussevere hypoglycemic event, impairedhypoglycemic awareness, and residualb-cell function), which help determinethe most appropriate clinical manage-ment goals for each patient. Although the
requirement for individualized glycemictargets remains unquestioned, this studyprovides further strong support for therevision of the historical dogma thatlower glycemic targets are associatedwith an increased risk of SH. This willrequire a shift in the clinical approach ofhealth care professionals and educationaimed at reducing the fear of hypogly-cemia for patients and their carers. Untilthis happens, the commonly held beliefthat increased rates of SH occur withlowering HbA1c is likely to impede effortsto increase the number of children andadolescents with type 1 diabetes reach-ing optimal glycemic targets and diabetes-related outcomes (7,9,33–35).
Funding. The DPV registry is supported by theGerman Center for Diabetes Research (grant82DZ01402).Duality of Interest. T.W.J. has received hono-raria for speaking and advisory board member-ship from Eli Lilly and Company, Novo Nordisk,Sanofi, and Medtronic. No other potential con-flicts of interest relevant to this article werereported.
There was no involvement by the fundingsources acknowledged in this study in any aspectof the study design, data collection, data analysisand interpretation, or writing of or decision topublish this manuscript.Author Contributions. A.H. conducted theliterature search, interpretation of data analysis,synthesis of results, and compilation of tables andfigures and wrote the manuscript, incorporatingfeedback and comments from all coauthors.J.M.H. was responsible for data aggregationand data management, conducted the dataanalysis, assisted with interpretation of theresults, and reviewed the tables, figures, andmanuscript. H.C., S.E.H., B.K., and T.W.J. reviewedthe results, tables, and figures and contributed to
Figure 4—Mean HbA1c (%) and estimated marginal mean SH rate (per 100 patient-years) adjusted for sex, age-group at diagnosis, and diabetesduration, by time period, for study participants in the DPV and WACDD. White bar with dots is 1991–2001; striped bar is 2002–2006; dark gray is2007–2011; and light gray is 2012–2016.
care.diabetesjournals.org Haynes and Associates 1635

the manuscript. E.A.D. and R.W.H. were jointsenior authors for this manuscript and contrib-uted to study design, reviewed the literaturesearch, results, tables, and figures, and contrib-uted to the manuscript. E.A.D. and R.W.H. arethe guarantors of this work and, as such, hadfull access to all of the data in the study andtake responsibility for the integrity of the dataand the accuracy of the data analysis.
References1. NathanDM,GenuthS, Lachin J, etal.;DiabetesControl and Complications Trial Research Group.The effect of intensive treatment of diabeteson the development and progression of long-term complications in insulin-dependent diabetesmellitus. N Engl J Med 1993;329:977–9862. Nathan DM; DCCT/EDIC Research Group.The Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions andComplications study at 30 years: overview. Di-abetes Care 2014;37:9–163. Lachin JM, Bebu I, Bergenstal RM, et al.; DCCT/EDIC Research Group. Association of glycemic var-iability in type 1 diabetes with progression of mi-crovascular outcomes in the Diabetes Control andComplications Trial. Diabetes Care 2017;40:777–7834. The Diabetes Control and Complications TrialResearch Group. Hypoglycemia in the DiabetesControl and Complications Trial. Diabetes 1997;46:271–2865. Cryer PE. The barrier of hypoglycemia indiabetes. Diabetes 2008;57:3169–31766. Seaquist ER, Anderson J, Childs B, et al.Hypoglycemia and diabetes: a report of a work-group of the American Diabetes Association andthe Endocrine Society. Diabetes Care 2013;36:1384–13957. Cryer PE. Glycemic goals in diabetes: trade-offbetween glycemic control and iatrogenic hypo-glycemia. Diabetes 2014;63:2188–21958. Frier BM. Hypoglycaemia in diabetes mellitus:epidemiology and clinical implications. Nat RevEndocrinol 2014;10:711–7229. McNeilly AD, McCrimmon RJ. The Scylla andCharybdis of glucose control in childhood type 1diabetes? Pediatr Diabetes 2015;16:235–24110. Yeoh E, Choudhary P. Technology to reducehypoglycemia. J Diabetes Sci Technol 2015;9:911–91611. Karges B, Schwandt A, Heidtmann B, et al.Association of insulin pump therapy vs insulininjection therapy with severe hypoglycemia,ketoacidosis, and glycemic control among chil-dren, adolescents, and young adults with type 1diabetes. JAMA 2017;318:1358–136612. Gubitosi-Klug RA, Braffett BH, White NH,et al.; Diabetes Control and Complications Trial(DCCT)/Epidemiology of Diabetes Interventionsand Complications (EDIC) Research Group. Risk ofsevere hypoglycemia in type 1 diabetes over30 years of follow-up in the DCCT/EDIC study.Diabetes Care 2017;40:1010–1016
13. Ly TT, Nicholas JA, Retterath A, Lim EM, DavisEA, Jones TW. Effect of sensor-augmented insu-lin pump therapy and automated insulin sus-pension vs standard insulin pump therapy onhypoglycemia in patients with type 1 diabetes:a randomized clinical trial. JAMA 2013;310:1240–124714. Pedersen-Bjergaard U, Kristensen PL, Beck-Nielsen H, et al. Effect of insulin analogues on riskof severe hypoglycaemia in patients with type 1diabetes prone to recurrent severe hypoglycae-mia (HypoAna trial): a prospective, randomised,open-label, blinded-endpoint crossover trial.Lancet Diabetes Endocrinol 2014;2:553–56115. Svensson J, Johannesen J, Mortensen HB,Nordly S; Danish Childhood Diabetes Registry.Improved metabolic outcome in a Danish dia-betic paediatric population aged 0–18 yr: resultsfrom a nationwide continuous Registration. Pe-diatr Diabetes 2009;10:461–46716. Bulsara MK, Holman CDAJ, Davis EA, JonesTW. The impact of a decade of changing treatmenton rates of severe hypoglycemia in a population-based cohort of children with type 1 diabetes.Diabetes Care 2004;27:2293–229817. Svoren BM, Volkening LK, Butler DA,Moreland EC, Anderson BJ, Laffel LMB. Temporaltrends in the treatment of pediatric type 1 di-abetes and impact on acute outcomes. J Pediatr2007;150:279–28518. Rosenbauer J, Dost A, Karges B, et al.; DPVInitiative and the German BMBF CompetenceNetwork Diabetes Mellitus. Improved metaboliccontrol in children and adolescents with type 1diabetes: a trend analysis using prospectivemulticenter data from Germany and Austria.Diabetes Care 2012;35:80–8619. Fredheim S, Johansen A, Thorsen SU, et al.;Danish Society for Diabetes in Childhood andAdolescence. Nationwide reduction in the fre-quency of severe hypoglycemia by half. ActaDiabetol 2015;52:591–59920. Johansen A, Kanijo B, Fredheim S, et al.;Danish Society for Diabetes in Childhood. Prev-alence and predictors of severe hypoglycemia inDanish children and adolescents with diabetes.Pediatr Diabetes 2015;16:354–36021. Karges B, Kapellen T, Wagner VM, et al.; DPVInitiative. Glycated hemoglobin A1c as a risk factorfor severe hypoglycemia in pediatric type 1 di-abetes. Pediatr Diabetes 2017;18:51–5822. American Diabetes Association. 12. Childrenand adolescents: Standards of Medical Care inDiabetesd2018. Diabetes Care 2018;41(Suppl.1):S126–S13623. Haynes A, Hermann JM, Miller KM, et al.;T1D Exchange, WACDD and DPV registries. Se-vere hypoglycemia rates are not associatedwith HbA1c: a cross-sectional analysis of 3 con-temporary pediatric diabetes registry databases.Pediatr Diabetes 2017;18:643–65024. Gerstl EM, Rabl W, Rosenbauer J, et al.Metabolic control as reflected by HbA1c in children,
adolescents and young adults with type-1 di-abetes mellitus: combined longitudinal analysisincluding 27,035 patients from 207 centers inGermany and Austria during the last decade. EurJ Pediatr 2008;167:447–45325. Joshi KK, Haynes A, Smith G, Jones TW, DavisEA. Comparable glycemic outcomes for pediatrictype 1 diabetes patients in metropolitan andnon-metropolitan regions of Western Australia:a population-based study. Pediatr Diabetes 2018;19:486–49226. Pedersen-Bjergaard U, Pramming S,Thorsteinsson B. Recall of severe hypoglycaemiaand self-estimated state of awareness in type 1diabetes. Diabetes Metab Res Rev 2003;19:232–24027. AbrahamMB, Jones TW, Naranjo D, et al.ISPAD Clinical Practice Consensus Guide-lines 2018: assessment and managementof hypoglycemia in children and adolescentswith diabetes. Pediatr Diabetes 2018;19:178–19228. Bulsara MK, Holman CDJ, Davis EA, Jones TW.Evaluating risk factors associated with severehypoglycaemia in epidemiology studies-whatmethod should we use? Diabet Med 2004;21:914–91929. Cooper MN, O’Connell SM, Davis EA, JonesTW. A population-based study of risk factors forsevere hypoglycaemia in a contemporary cohortof childhood-onset type 1 diabetes. Diabetologia2013;56:2164–217030. O’Connell SM, Cooper MN, Bulsara MK,Davis EA, Jones TW. Reducing rates of severehypoglycemia in a population-based cohort ofchildren and adolescents with type 1 diabetesover the decade 2000-2009. Diabetes Care 2011;34:2379–238031. Karges B, Rosenbauer J, Kapellen T, et al.Hemoglobin A1c Levels and risk of severehypoglycemia in children and young adultswith type 1 diabetes from Germany and Austria:a trend analysis in a cohort of 37,539 patientsbetween 1995 and 2012. PLoS Med 2014;11:e100174232. Buckingham BA, Raghinaru D, Cameron F,et al.; In Home Closed Loop Study Group. Pre-dictive low-glucose insulin suspension reducesduration of nocturnal hypoglycemia in childrenwithout increasing ketosis. Diabetes Care 2015;38:1197–120433. Choudhary P, Ramasamy S, Green L, et al.Real-time continuous glucose monitoring signif-icantly reduces severe hypoglycemia in hypogly-cemia-unaware patients with type 1 diabetes.Diabetes Care 2013;36:4160–416234. Cryer PE. Individualized glycemic goals andan expanded classification of severe hypoglyce-mia in diabetes. Diabetes Care 2017;40:1641–164335. International Hypoglycaemia Study Group.Minimizing hypoglycemia in diabetes. DiabetesCare 2015;38:1583–1591
1636 Concurrent Improvements in HbA1c and SH Rates Diabetes Care Volume 42, September 2019