Embed Size (px)
DESCRIPTION
Advances in Painful bladder syndrome. Stephen Mark Christchurch. Overview. Diagnosis: Interstitial Cystitis [IC] vs Painful bladder syndrome [PBS] Syndrome association Medical management Surgical management. IC vs PBS. - PowerPoint PPT Presentation
Citation preview
Advances in Painful bladder syndrome
Stephen MarkChristchurch
Overview
Diagnosis: Interstitial Cystitis [IC] vs Painful bladder syndrome [PBS]
Syndrome associationMedical managementSurgical management
Symptoms: Urgency, Frequency,Nocturia, Pelvic pain { bladder, urethral,vaginal, rectal,perineum}
IC: Cystoscopic findings: pain on filling, inflammation and histologic abnormality
Diagnosis: Exclusion all other pathology : UTI, OAB, Cancer, Endometriosis
IC vs PBS
ICS 2002: “supra-pubic pain,related to bladder filling,frequency,nocturia,urgency,”without other pathology”
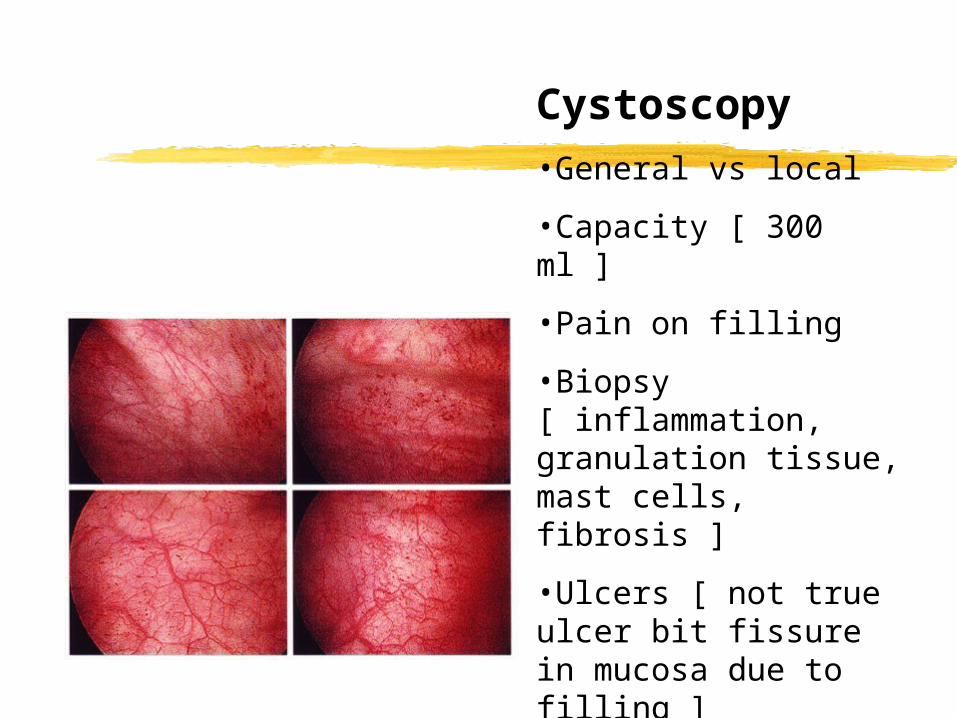
Cystoscopy•General vs local
•Capacity [ 300 ml ]
•Pain on filling
•Biopsy [ inflammation, granulation tissue, mast cells, fibrosis ]
•Ulcers [ not true ulcer bit fissure in mucosa due to filling ]
Associated complaints
Mental Health: Depression and Panic disorders are more common : J Urol 2008, 180 1378
Depression more difficult to treat in these patients
Mental health, pain and urinary symptoms are correlated.
Medical management
AnalgesiaUrinary alkaliniser, dilute urineCranberryWith-hold irritantsDMSO instillationAnticholinergics
Medical management
Sub optimalLack of efficacyProlonged time for effectPoor durability of effectRequire: safe, effective, prompt relief
of symptoms with durability
Medical management:Intravesical Resiniferatoxin
Previously effective in pilot studies Presumed action on pain C fibers Recent RCT 163 patients : No improvement in
overall symptoms, pain, urgency…etc . J Urol 2005,173.1590
Natural Hx PBS is characterised by remissions and exacerbations thus require placebo controlled RCT for effect.
Surgical managementBotox A
Single arm pilot studies only.Small numbersSome evidence to suggest Botox
may affect pain pathwaysClinical effect mainly for paralysis of
smooth and striated muscleTemporary effect
Surgical management Botox studies
Urology 2004 64, 871: 13 patients. 69% improvement. [ 1 - 8 months]
Eur Urol 2006 49. 704 14 patients. 85% improvement . 10 recurred within 5 months
Little else…..
Surgical managementHydrodistension
Diagnostic and theraputicCapacity { 300 ml}May lead to prolonged symptom
reliefRare complication of “total bladder
necrosis” J Urol 2007 177 , 149
Surgical managementReconstruction
Total vs Partial cystectomyUrethral vs stomal emptyingIndications: Pain location and relation to
bladder, capability of CIC, bladder capacity reduced…..no other confounding issues
Durable success in VERY select patients. 80% success approx. J Urol 2002 167, 603
PBS Local management algorithm
Presentation: History, exam, MSU, GA cysto and biopsy.
High volume vs Low volume. High vol: medical management, instillations,
symptomatic management… occ hydrodilatation Low vol: all of the above , if resistant consider
surgery
PBSLocal results of surgery
6 patients: age 35 - 68Total cystectomy and bladder
reconstruction1 reoperation for leakagePain resolution complete 3/4… 1 pouch
painAll resumed “ normal” lifestyle
PBSSummary
Debilitating common remitting disease
Unknown aetiologyImpairs quality of lifePoor treatment optionsSignificant economic burden to
patient and health system