Embed Size (px)
Citation preview

Painful bladder (in women)
Professor Douglas TincelloUniversity of Leicester

Declaration of Interest
• Industry related 2012– Honorarium for Allergan advisory board – Honorarium, registration, accomodation for
Ethicon symposium at UKCS– PI on RELAX study (onaBoNT-A)
• Independent funding
• All funding managed via University business office
Tincello DG Kuwait Feb 16th -18th 2013

Hypotheses for aetiology?• Four major theories
– Autoimmune disease– Chronic infection– Neurogenic inflammation– Epithelial permeability
• None sufficient or totally convincing
Tincello DG Kuwait Feb 16th -18th 2013

?
Mast cell
Cytokines
Substance P
Histamine
Complement
“Toxins”K+
Bacteria
Viruses
Antiproliferative factor
Tincello DG Kuwait Feb 16th -18th 2013

Antiproliferative factor
• APF similar to frizzled 8 protein-related sialoglycopeptide (Keay J Urol 2005;173:909)
– G protein coupled receptor protein family– ? Inhibition of proliferation signals
• Specific receptor identified (CKAP4/p63)– Cytoskeleton associated receptor– (Conrads et al J Biol Chem 2006;281:37836)
Tincello DG Kuwait Feb 16th -18th 2013

Antiproliferative factor
• Urine of IC patients inhibits urothelial growth– 86% of IC patient vs 12% cystitis vs 8% controls– (Keay et al Urol 1998;52:974)
• APF produced by urothelium– 19/20 bladder urine vs 1/20 renal pelvis urine– (Keay et al J Urol 1999;162:1487)
• 95% sensitivity; 94% specificity – (Keay et al Urology 2001;57(6A):9)
• Irrespective of ethnic origin– (Zhang et al Urology 2003;61:897)
Tincello DG Kuwait Feb 16th -18th 2013

Antiproliferative factor• APF inhibits HB-EGF release from urothelium• Exogenous HB-EGF blocks inhibition
– (Keay et al J Urol 2000;164:2112)
• Hyrdodistention causes APF ↓ & HB-EGF ↑– (Keay et al J Urol 2000;163:1440)
• APF increases permeability of urothelium– (Zhang et al J Urol 2005;174:2382)
• Urothelial cells from IC patients grow slowly– (Keay et al Urol 2003;61:1278)
• Gene expression is “non proliferative”– (Keay et al Physiol Genomics 2003;14:107)
Tincello DG Kuwait Feb 16th -18th 2013

Antiproliferative factor
HB-EGF
APF
-
“Toxins”K+
Bacteria
Viruses
?
Tincello DG Kuwait Feb 16th -18th 2013

Diagnostic criteria…• Interstitial cystitis (NIDDK criteria)
– Originally for research, but were adopted– Tight, specific limits on functional volumes, cystoscopic
findings, symptom severity– Comprehensive exclusion criteria
• IC/CPPS (Diokno A et al. Int J Urol, 10: S3, 2003)
– “Pain” includes: burning, pressure, discomfort – At least 3 months’ duration– May be exacerbated by intercourse– Patient must have frequency and urgency
Tincello DG Kuwait Feb 16th -18th 2013

…continued…
• European Society for the Study of IC/PBS• Consensus statement June 2006 • Stop using “interstitial cystitis”• “Bladder pain syndrome”
– Chronic pain related to bladder– Plus one other symptom– Exclusion of “confusable diseases”– Cystoscopy with hydrodistension and biopsy
Tincello DG Kuwait Feb 16th -18th 2013

Confusable diseases
“The diagnosis of a confusable disease does not necessarily exclude a diagnosis of bladder pain syndrome”

A word about cystoscopy
• Cystoscopy is for excluding discrete pathology– IC & sensory urgency have same leucocytes (Al Hadithi , 2002)
– Mast cells present in up to 40% of SU patients (Frazer, 1993)
– Glomerulations occur in normal bladders (Waxman, 1998)
– Symptoms not related to cystoscopic or urodynamic data (Messing, Nigro; ICDB study, 1997)
• No longer a requirement for making a diagnosis
Tincello DG Kuwait Feb 16th -18th 2013

Patients…
• Present with bladder pain ± other symptoms• Pelvic pain can arise from several sources
– common autonomic/visceral pain pathways– may be a common pathway for diverse initial insult
• Various “pseudonyms”– urethral syndrome, sensory urgency, vulvodynia, myofascial
syndrome, endometriosis, “chronic pelvic pain”
• Management algorithm to screen for causes
Tincello DG Kuwait Feb 16th -18th 2013

How I assess patients...
• Based upon:– literature
Nordling J Eur Urol 2004;45:662O’Leary MP Urol 1997;49:58
Daha LK J Urol 2003;170:807
– Learning from conferences– clinical experience
Tincello DG Kuwait Feb 16th -18th 2013

Assessment-historySite, radiation and associations of painDuration, and exacerbations in relation to urinary
symptoms (esp bladder filling)Presence, site and duration of dyspareunia
post coital ache
Frequency and nocturia
Haematuria? ? Proven urinary tract infection
– including fastidious organisms
Tincello DG Kuwait Feb 16th -18th 2013

Assessment-examinationSymphyseal tenderness, sacroiliac tenderness
– (pain on abduction of hips or limitation of ROM)
• Hyperaesthesia in lower abdomen/perineum – (nerve entrapment)
Vulval erythema or hyperalgesia on cotton swab test in each quadrant of vestibule
Palpate bladder base, pelvic muscles for tenderness (trigger points) reproduction of symptoms
Cervical excitation, masses, endometriosis nodules
Tincello DG Kuwait Feb 16th -18th 2013

Assessment-investigationUrine culture (including fastidious/anaerobes)3 day urinary diary
frequency, nocturiadaytime voided volumes vs waking void volume
• Urodynamics – (sometimes)
• Double fill cystoscopy and hydrodistension– (sometimes)
Tincello DG Kuwait Feb 16th -18th 2013

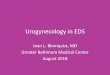
Compare daytime and waking
volumes
All vols usually < 350mls
PBS likely
Urodynamics ± cystoscopy
Day vols < 350mlWaking vol > 350ml
PBS unlikely
Refer for bladder retraining
Urodynamics if no better
Day vols include >350 mls
PBS very unlikely
UDS unlikely to be useful
Bladder drill + PFE
Tincello DG Kuwait Feb 16th -18th 2013

UrodynamicsDO excluded
“PBS”Sensation
Capacity
First sensation <150 ml
Capacity <350 ml
“Sensory urgency”Sensation
Capacity normal
First sensation <150 ml
Capacity ≥ 350ml
(with coaxing!)
“Normal”
First sensation ≥ 150 ml
Capacity ≥ 350 ml
Tincello DG Kuwait Feb 16th -18th 2013


Treatment
• Specific treatment for specific conditions– endometriosis– vulvodynia– myofascial syndrome/pelvic muscle trigger points– Sacroiliac or symphyseal joint pain
• PBS symptoms & normal bladder capacity
• PBS and reduced bladder capacity
Tincello DG Kuwait Feb 16th -18th 2013

Normal bladder capacity
• Bladder drill +/- diary to increase functional capacity• Retrain sensations• Anticholinergics may be of some benefit
– modulate sensation of urgency & discomfort?
• If no improvement…– treat as if reduced capacity
Tincello DG Kuwait Feb 16th -18th 2013

Reduced capacity
• “interstitial cystitis” or PBS– Quality of published work is poor– Most use NIDDK criteria (most severe patients)– Placebo effect is large– Few RCTs
• Pain control and patient support
• Intravesical therapy• Oral therapy• Recent systematic review (Giannantoni 2012 Eur Urol 61:29-53)
Tincello DG Kuwait Feb 16th -18th 2013

Intravesical therapy• Distension under GA for 10 minutes
– 55% response rate but transient (Hanno 1991 Semin Urol 9:143; Pontari 1997 Urol 49 (5A):114)
• DMSO (Six to eight weeks of instillations 1-2/week)– Response rate up to 90%; 40% relapse rate– No RCT data(Parkin 1997 Urol 49 (5A):105; Pontari 1997 Urol 49 (5A):114; Peeker 2000 J Urol 164:1912)
• Hyaluronic acid– success rate of 30-70%– One randomised trial, no placebo
(Kallestrup 2005 Scand J Urol Nephrol 39:143; Reidl 2008 IUGA J 19:717; Cervigni 2012 IUGA J 23: 1187; Yi-Song 2012 IUGA J in press; Lai M-C 2012 Int J Urol in press)

Intravesical therapy•Botulinum toxin
– Mixed data from non –RCTs– 75% improved at 3 months
• 80% fall in pain, 40% in frequency
– 75% relapse by 6 months– RCT data (n=2) confirm efficacy
• Fall in pain and frequency @ 3/12• Trigone injection shows greater effect
– 50% reduction in frequency & noturia
(Liu 2007 Urol 10:463; Kuo 2005 Urol Int 75:170; Smith 2004 Urol 64:871; Giannantoni 2008 J Urol 179:1031; 2010 Curr Drug Del 7:1; Kuo 2009 BJU Int 104:657; Pinto 2010 Eur Urol 58; 360)

Oral treatments• Cimetidine
– RCT of 400 mg significant reductions in pain and nocturia (Seshadri 1994 Urol 44:614; Thilagarajah 2001 BJU Int 87:207)
• Pentosan polysulphate– 3 of 5 RCTs show a difference– 25%+ improvement in 25% vs 13% (Parsons 1987 J Urol 138:513; Mulholland 1990 Urol 35:552; Parsons 1993 J Urol 150:845)
• Amitriptyline– Success of 65-90% (Hanno 1994 Urol Clin N Amer 21:121; Pranikoff 2001
Urol 51 (5A); 179)
– Titration from 25mg nocte to 100mg (van Ophoven 2004 J Urol 172:533)

Recent data
• Systematic review– Giannantoni Eur Urol 2012;61:29-53
– 29 RCTs and 57 non random studies– Standardised mean difference
• 0.8 = large effect• 0.5 = moderate effect
– Assessed four outcomes• IC symptom index• Pain• Urgency• Frequency

IC symptom index

Pain

Urgency

Frequency

Conclusions...
• Cyclosporin A– Effect on 3 of 4 outcomes (? Data)
• Amitriptyline– Effect on all four outcomes– 25mg – 100mg titrated at night
• PPS– Limited efficacy– Non-random studies suggest 50% long term effectGiannantoni Eur Urol 2012;61:29-53

...cont’d...• BCG
– Limited effect– Concerns re use from cancer studies
• BoNTA– Effective at pain relief– ? Additional effect from trigone injection
• “The inability to propose definite conclusions from the results coming from most of the proposed treatments...”Giannantoni Eur Urol 2012;61:29-53

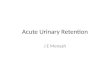
Pain clinic
Oral Rx: cimetidine
amitriptyline
Intravesical Rx: DMSOBoNT-A
Reduced capacity
Cystoscopy & distension
Better? Disch’gY
Specific condition identified
Treat
Specific condition identified
Treat
Urodynamics
? Bladder drill, alkalinisation
Normal capacity
Day vols >350 mls
Waking vol > 350ml
All vols < 350mls
N
History, exam, MSSU, FV Chart