Embed Size (px)
Citation preview

RESEARCH Open Access
Advancing theory development: exploringthe leadership–climate relationship as amechanism of the implementation ofcultural competenceErick G. Guerrero1,2* , Karissa Fenwick1 and Yinfei Kong3
Abstract
Background: Leadership style and specific organizational climates have emerged as critical mechanisms to implementtargeted practices in organizations. Drawing from relevant theories, we propose that climate for implementationof cultural competence reflects how transformational leadership may enhance the organizational implementationof culturally responsive practices in health care organizations.
Methods: Using multilevel data from 427 employees embedded in 112 addiction treatment programs collectedin 2013, confirmatory factor analysis showed adequate fit statistics for our measure of climate for implementationof cultural competence (Cronbach’s alpha = .88) and three outcomes: knowledge (Cronbach’s alpha = .88), services(Cronbach’s alpha = .86), and personnel (Cronbach’s alpha = .86) practices.
Results: Results from multilevel path analyses indicate a positive relationship between employee perceptions oftransformational leadership and climate for implementation of cultural competence (standardized indirect effect= .057, bootstrap p < .001). We also found a positive indirect effect between transformational leadership and eachof the culturally competent practices: knowledge (standardized indirect effect = .006, bootstrap p = .004), services(standardized indirect effect = .019, bootstrap p < .001), and personnel (standardized indirect effect = .014, bootstrapp = .005).
Conclusions: Findings contribute to implementation science. They build on leadership theory and offer evidence ofthe mediating role of climate in the implementation of cultural competence in addiction health service organizations.
Keywords: Transformational leadership, Organizational climate, Cultural competence, Implementation
BackgroundHealth care organizations require leadership toimplement practices that are effective and culturally re-sponsive to the increasing racial and ethnic diversity ofthe US population. To address the well-established dis-parities between health outcomes of racial and ethnicminorities compared to Whites, federal and private insti-tutions have supported the implementation of culturallycompetent practices [1, 2]. Cultural competence refers
to the recognition and responsiveness of organizationsto the service needs of culturally and linguisticallydiverse populations and aims to improve health carequality, engage racial and ethnic minority clients in care,and reduce outcome disparities [3–6]. Some culturallyresponsive practices, such as language and racial andethnic provider–client matching, translating materials,and using cultural stories to engage clients in services,have robust associations with health outcomes [3–6].Yet culturally responsive practices, which are consistentwith Klein and Sorra’s [7] theory of innovation imple-mentation, can be considered an innovation becausetheir implementation require active and coordinated useby many organizational members and they are not
* Correspondence: [email protected] Dworak-Peck School of Social Work, University of SouthernCalifornia, 655 West 34th Street, Los Angeles, CA 90089, USA2Marshall School of Business, University of Southern California, 655 West 34thStreet, Los Angeles, CA 90089, USAFull list of author information is available at the end of the article
© The Author(s). 2017 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, andreproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link tothe Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver(http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Guerrero et al. Implementation Science (2017) 12:133 DOI 10.1186/s13012-017-0666-9

routinely applied in health care settings. Efforts to sys-tematically examine the drivers of implementation of in-novative culturally responsive practices in health care [8]and addiction health services [9, 10] are limited.Leadership is a key factor associated with implementa-
tion of service innovations such as cultural competence,given that organizational leaders are generally respon-sible for overseeing the implementation process [11].Theory suggests that leadership affects implementationboth directly and indirectly by shaping theorganizational context, which then influences employeebehaviors [12]. Developing research shows that leaders’communication and prioritization of new norms and ex-pectations (e.g., safety) influence employee adoption ofthose norms and endorsement of congruent practices(e.g., safer work practices), generally referred to asorganizational climate. The organizational climate sup-ports and encourages employees in implementing a newpractice [13]. This leader–climate–practice mechanismhas been examined in the context of implementation ofindustrial safety [14], corporate customer services [15],and evidence-based health care practices [16]. However,it is critical to examine the extent to which this mechan-ism applies to cultural competence. Although commonlyendorsed in health care services, cultural competence re-quires creative thinking to implement key cultural as-pects (e.g., familismo, language, context) that may affectclient outcomes [1, 2]. Understanding the role of leader-ship and implementation climate in the uptake of cul-tural competence in health care is critical to improveclients’ response to treatment, particularly in substanceuse disorder treatment programs whose unique structureas generally small programs with an average of five tosix employees allows managing leaders to have directand daily interactions with employees.
Theoretical frameworkOne of the most influential leadership styles described inthe management literature is transformational leadership[17, 18]. Transformational leadership is a leader’s abilityto inspire others to follow a particular course of actionand perform beyond previous levels [19, 20]. Transform-ational leaders consider the unique talents of each staffmember or employee (these terms are used interchange-ably in this paper), give specific feedback to each staffmember based on his or her needs, stimulate new waysof solving problems, and create a shared sense of pur-pose among all staff members [19, 21]. Transformationalleadership is thought to be transmitted through aleader’s expression of his or her values and goals and se-lection, modeling, and communication of relevant infor-mation, which staff members use when weighing optionsand making decisions [16, 22, 23].
Transformational leadership has been shown to play arole in the adoption and implementation of innovationsin health care [24–26]. Leadership style influences mul-tiple organizational processes involved in delivery of in-novative practices [11]. For instance, leaders initiateadoption decisions, develop strategic goals and activitiessupporting innovation implementation, secure necessaryresources, build organizational capacity for change, scanthe internal and external contexts, and provide perform-ance feedback to the staff [9, 27, 28]. One of the mostimportant ways in which leaders affect delivery of in-novative practices is by creating an organizational con-text conducive to implementing new practices. Inparticular, leaders positively or negatively contribute tothe creation, development, and sustainment of anorganizational climate that fosters employee attitudesand behaviors that support innovative practice use [25,29, 30]. A leader in the current study refers to executiveor upper level directors who oversee the overall oper-ation of treatment programs and whose transformationalstyle may influence employees, such as middle managers(i.e., supervisors) and counselors.
Organizational climateOrganizational climate can be understood as employees’shared perceptions of procedures, practices, and behav-iors that are rewarded and supported by managementwith a specific purpose [31]. When the purpose involvesimplementing practices that respond to client’s nativecultural norms and values, language, and history, the re-sultant shared perceptions can be defined as climate forimplementation of cultural competence.Many definitions of climates have emerged. These def-
initions of organizational climates seem to differ basedon the language used to capture the level of agreementamong employees regarding the implicit and or explicitpriorities of the organization. These priorities are gener-ally communicated by managers through organizationalpolicies, procedures, and practices, leading to employees’shared notion of “the way things are done around here”[32, 33]. Hence, measurement of this conceptualizationhas focused on what is expected, supported, promoted,rewarded, and punished in the work context [34, 35].Moreover, organizational climate can be conceptual-
ized and measure either as a singular, molar climate(e.g., shared perceptions of organizational policies andprocedures) that influences nearly all activities in anorganization or as multiple simultaneous focused cli-mates (shared perceptions of a direct manager’s prior-ities through rewards and support of employees’ specificbehaviors and attitudes) [35]. Recent climate researchsuggested that a molar climate may lay the groundworkfor focused climates, which then serve as more proximalpredictors of outcomes [36, 37]. As a result, the latest
Guerrero et al. Implementation Science (2017) 12:133 Page 2 of 12

research on climate has focused on the development ofspecific climates for desired organizational goals (suchas customer service and safety) or processes (such ascreativity) [15]. Focused climates consist of the compo-nents of the organizational environment that are mostinfluential in orienting employee behavior toward theoutcome of interest. The development of these focusedclimates improves prediction and understanding of tar-geted outcomes and makes the climate construct morepractically relevant to managers seeking to enhance per-formance in specific areas [15, 37]. Assessment of fo-cused climates using employees’ shared perceptions ofthe consistency among policies, procedures, and practi-ces—basically “leader’s words and actions” in prioritizingimplementation of a new practice—may improve under-standing of climate as a mechanism that influences em-ployees’ attitudes and behaviors [35].Empirical research has supported the association be-
tween many specific climates and their targeted out-comes. Safety climate is associated with decreasedaccidents [38, 39], service climate is associated withgreater customer satisfaction [40, 41], climate for cre-ativity is associated with creative performance [42], andclimate for innovation is associated with greater innova-tive behavior [43]. In this study, implementation climatefor cultural competence can be defined as employees’shared perceptions of their program supervisors’ priorityto implement culturally responsive practices through ex-pectations, support, promotions, rewards, and punish-ments [34, 35]. In a strong implementation climate,employees perceive new practices as a priority ratherthan a distraction or disruption [7, 44]. Several studieshave found a positive association between implementationclimate and implementation effectiveness, although empir-ical studies of implementation climate are limited [45–47].Implementation climate can be further tailored to refer
to implementation of new knowledge, practices, or pro-cesses as promoted, rewarded, and expected by directsupervisors and perceived by employees. For example, ina strong climate for implementation of cultural compe-tence, employees perceive that the adoption, implemen-tation, and use of culturally competent knowledge,services, and practices is expected, rewarded, and sup-ported by management [48].
Organizational climate as a mediatorLeading climate scholars [35, 37, 49] have advised re-searchers to examine the relationships among leadership,climate, and outcomes in more depth. They recom-mended exploring how leaders create and maintain cli-mate and how climate mediates the relationship betweenleadership and outcomes.Understanding the leader–climate–practice mechan-
ism necessitates a theoretical explanation of how leaders
influence focused climates. Leaders may shapeorganizational climate through a social learning processin which staff members repeatedly interact with and ob-serve their leader to interpret organizational priorities[29, 50]. Leaders convey the importance of various tasksin an organization through implicit and explicit commu-nication of priorities [51, 52]. Through their behaviorand interactions with employees, they communicate thevalue of each task and their evaluation of tasks in com-parison with one another. Leaders communicate theirpriorities in several ways. They develop strategic goalsfor the organization, disseminate information, monitorand supervise staff activities, model desired behavior,and reward staff behavior in line with the prioritized be-havior or outcome [53–55]. These activities occur morefrequently or intensely for prioritized behaviors or out-comes in comparison to those that are not prioritized.Three main attributes characterize the relationship be-
tween leadership behavior patterns and communicatedpriorities [56]. Pattern orientation refers to communicat-ing a particular priority relative to other competing in-terests, pattern variability refers to the consistency ofleader behavior in communicating a particular priorityover time and among different staff members, and pat-tern simplicity is the number of contingencies that influ-ence a priority. Leaders who prioritize implementationof cultural competence may communicate this priorityby developing strategic goals and plans supporting cul-turally competent practices, allocating resources forculturally competent services, and providing supervisionand coaching to build culturally competent knowledge.In addition, they may persevere in the face of challengesto implementation and reward employees based onprovision of culturally competent services [27, 28, 57].By communicating their expectations and priorities inthese ways, leaders develop, support, and perpetuate anorganizational climate [56]. See Fig. 1.The climate–practice relationship is based on climate’s
role as a guide and sense-making mechanism that influ-ences employees’ attitudes and behaviors [58]. Employeesinterpret their environment, and climate acts as a criticaldeterminant that influences these interpretations [59, 60].
Overview of the current researchWe examined the organizational processes driving im-plementation of culturally competent knowledge, prac-tices, and services. We focused on the organizationalclimate for implementation of cultural competence(employees’ shared perceptions of middle managers’ pri-orities, expectations and rewards to implement culturalcompetence) to explore the extent to which it enhancesexecutive leaders’ transformational leadership in the im-plementation of significant culturally competent prac-tices in addiction health services. Executive or program
Guerrero et al. Implementation Science (2017) 12:133 Page 3 of 12

directors are referred to here as executive or upper levelleaders, whereas clinical supervisors are referred to asmiddle managers. Our hypotheses are as follows:Hypothesis 1Transformational leadership will be positively and in-
directly related to the implementation of culturally com-petent knowledge through climate for implementation ofcultural competence.Hypothesis 2Transformational leadership will be positively and indir-
ectly related to the implementation of culturally compe-tent service practices through climate for implementationof cultural competence.Hypothesis 3Transformational leadership will be positively and indir-
ectly related to the implementation of culturally competentpersonnel practices through climate for implementation ofcultural competence.
MethodsBackground and contextThis study used data from a larger study featuring asampling frame of 408 addiction health services pro-grams funded by a public health department in LosAngeles County between July 1, 2013, and December 31,2013. Data for the current study came from the secondwave of the larger study, during which all relevant vari-ables were introduced. The initial sampling procedureinvolved a random selection of 147 outpatient programslocated in communities with a population compositionof 40% or more Latino or African American residents orboth in the study region. Data collection for this waveincluded information from an average of three direct-service providers per program (one manager and twocounselors). Only programs with at least two respon-dents, a counselor, and a manager (either director or
supervisor) were included in the analysis. Most pro-grams had an executive or upper level director, a middlemanager (e.g., supervisor), and a counselor. Only 5% ofprograms had one manager with dual directorial andsupervisory responsibilities and who reported on bothprogram funding and regulation, as well as on thetransformational leadership of their executive director.Data collectors obtained staff rosters to select at ran-dom respondents within programs; overall, the samplecomposition was 25.4% directors, 15.7% supervisors,and 58.9% counselors.Considering eligible and still operating programs, the
final analytic sample featured 112 programs (92% re-sponse rate) and 427 individual participants. The 35 pro-grams not included in this wave did not differ from theoriginal analytic sample in terms of main independentvariables, such as leadership style (transformational) andcultural competence (p > .05).A treatment program was defined as an outpatient site
managed as a standalone program or by a parentorganization generally situated at a different location.The average age of participants in the sample was46 years, and 34% of participants were men. Most man-agers were African American (45%) or Latino (32%), aswere counselors (43 and 47%, respectively).Our power analysis suggest that we would have 80%
power to detect a medium effect size, which is associatedwith a Pearson’s correlation of .24, when considering 99programs and 15 variables in the statistical regressionanalysis [61]. To increase the validity of the survey mea-sures, we conducted in vivo observations and reviewedprinted materials available at each provider site (e.g.,brochures, group activities, posted signs). For example,for each dependent variable (culturally competent prac-tices), we used a matrix (Excel sheet) with key programfeatures to cross-check the consistency of staff reports
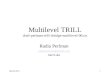
Fig. 1 Path analysis of transformational leadership, climate for implementation of cultural competence, and three culturally competent practices.Note. Control variables include program funding, licensure, and professionalism
Guerrero et al. Implementation Science (2017) 12:133 Page 4 of 12

on survey measures. All measures were responded to bysupervisors and counselors except for regulation, publicfunding, and professionalization, which were respondedto by upper level managers (i.e., directors) or managerswith both supervisory and directorial responsibilities.
Dependent variablesThe organizational cultural competence survey measureswere adapted from the Cultural Competence Self-Assessment Questionnaire [6]. This 57-item measure iscomposed of six subscales assessing culturally competentpractices: (a) knowledge of, (b) outreach to, and (c) per-sonal involvement in racial and ethnic minority commu-nities; (d) development of resources and linkages toserve racial and ethnic minorities; (e) development ofpolicies and procedures to effectively respond to the ser-vice needs of racial and ethnic minority patients; and (f )hiring and retention of employees with racial and ethnicminority backgrounds (for a full description of items, seeMason [6]). We used the 57 items to empirically developthree critical subscales as suggested by the literature:knowledge (eight items, e.g., Do you know the prevailingbeliefs, customs, norms, and values of Latinos in yourservice area?); service practices (nine items, e.g., Doesyour agency utilize interpreters to work with limitedEnglish-proficient Latinos?); and personnel practices(nine items, e.g., Does your agency utilize interpreters towork with limited English-proficient Latinos). Responseswere rated on a 4-point Likert scale (1 = not at all to 4 =often) and averaged to create total scores for each sub-scale. Higher scores indicated higher levels of culturalcompetence in each subdomain, as perceived by supervi-sors and counselors. Confirmatory factor analysis wasconducted to validate these measures (see Table 1 fordescriptive statistics; confirmatory factor analysis resultsare reported in Table 2).
Independent variablesOur main independent variables were leadership style(transformational) and climate for the implementation ofcultural competence. A 7-item measure assessed trans-formational leadership among executive or upper levelleaders (i.e., agency directors) [62]. This short versionhas been used in several studies on staff ’s perception ofdirectors’ transformational leadership in health care ser-vices [62–65]. Each director’s leadership was rated byclinical supervisors and counselors on a 5-point scale (1= strongly disagree to 5 = strongly agree) and scores weretotaled as suggested by the measure’s authors [62].Higher scores represented higher transformational lead-ership capacity as perceived by clinical supervisors andcounselors. Cronbach’s alpha for transformational lead-ership capacity was .92.
We measured climate for the implementation of cul-tural competence using six items. The development ofthese items was informed by other climate measures insafety [38], customer satisfaction [41], and innovative be-havior [43]. Climate is generally enforced through mid-dle managers’ communicated priorities, rewards, andexpectations [36, 56]. Altogether, the leadership–cli-mate–practice mechanism is supported by empirical evi-dence showing that organizational climate acts as amediator between leadership and a variety of outcomes,including innovation implementation behavior [25, 30,59, 60]. Our measure of climate was rated by clinical su-pervisors and staff members on a 5-point scale (1 = notat all to 5 = very well) and scores were aggregated byprogram and totaled as suggested by authors of climatemeasures [35, 38, 49]. Higher scores represented stron-ger employee perceptions that the implementation ofculturally competent practices was promoted, rewarded,
Table 1 Descriptive statistics from 427 participants nested in112 programs
M (SD) or % Range
Participant demographics
Age 46.6 (11.7) 19–75
Race and ethnicity
Latino 40.1
African American 27.6
White 21.6
Other 10.1
Position
Director 25.3
Supervisor 15.7
Counselor 58.8
Education
High school or lower 5.9
College 56.4
Graduate degree 32.3
Program measures
Transformational leadership 39.4 (7.5) 10–50
Climate for implementation of culturalcompetence
3.4 (0.85) 1–5
Knowledge 2.9 (0.57) 1–4
Personnel practices 2.6 (0.74) 1–4
Service practices 2.4 (0.87) 1–4
Control variables
Percentage of public funding 67.9
Licensing 96.3
Professional accreditation (Joint Commission) 32.7
Professionalization (% of staff withgraduate degree)
21.6 (18.3) 0–75
Guerrero et al. Implementation Science (2017) 12:133 Page 5 of 12

and expected by their manager. A sample item of a pro-moted practice is: “Supervisor prioritizes enhancing thestaff ’s cultural competence by helping resolve cross-cultural issues with clients.” An item measuring arewarded practice include: “Supervisor provides incen-tives to the staff to become linguistically and culturallyresponsive, despite investment of time and resources.”An item measuring an expected practice is: “Supervisorhas emphasized the importance of translation of materialand development of policies and procedures to respondto clients with limited English proficiency, despite her orhis other multiple responsibilities.” We measured the in-ternal consistency of survey items to determine their
overall reliability as a measure. Cronbach’s alpha for thisleadership measure was .88.
Control variablesThese variables included regulation, public funding, andprofessionalization. Please refer to Table 1 for a full listof variables. We assessed regulation by determiningwhether each program had a state license and accredit-ation by the Joint Commission. We also included ameasure of percentage of public revenue in each pro-gram’s budget; professionalization was measured usingthe percentage of staff members with a graduate degree.
Table 2 Confirmatory factor analysis of culturally competent practices (knowledge, service, and personnel)
Obs Itemtest
Itemrest
Interitemcovariance
α
Knowledge
How well are you able to describe differences within various Latino or Hispanic groups? 424 .701 .557 .292 .888
How well are you able to describe the strengths of Latino groups in your service area? 427 .807 .716 .277 .861
How well are you able to describe the social problems of Latino groups in your community? 425 .866 .804 .270 .849
Do you know the prevailing beliefs, customs, norms, and values of Latinos in your service area? 426 .834 .749 .267 .856
Do you know the social service needs of Latinos that go unaddressed by the formal social service system? 421 .829 .736 .261 .857
Do you know how the causes of mental illnesses are viewed by Latino groups in your area? 430 .773 .656 .274 .870
Full scale .274 .884
Service practices
Does your agency use Latino-specific assessment instruments for diagnosis? 294 .737 .647 .613 .832
Does your agency use Latino culture-specific treatment approaches? 290 .761 .683 .605 .830
Does your agency envision community empowerment as a treatment goal? 291 .745 .660 .602 .831
Does your agency review case practice on a regular basis to determine relevancy to clients of color? 288 .749 .659 .594 .831
Does your agency provide or facilitate child care? 298 .688 .569 .612 .842
Does your agency provide or facilitate transportation (e.g., bus tickets, ride sharing)? 296 .627 .495 .632 .850
Does your agency include clients’ families and community in services? 298 .734 .637 .599 .833
Does your agency translate agency materials into Spanish? 302 .634 .520 .640 .846
Does your agency offer payment arrangements for indigent or low-income clients? 296 .499 .361 .688 .860
Full scale .621 .855
Personnel practices
Does staff utilize cultural consultants who can help them work more effectively? 422 .516 .375 .486 .863
Does your agency provide training that help staff work with Latinos? 419 .570 .445 .475 .856
Does your agency utilize interpreters to work with limited English-proficient Latinos? 418 .503 .346 .485 .869
In your program, are there Latinos represented in managerial and administrative positions? 424 .759 .670 .421 .834
In your program, are there Latinos represented in direct-service positions? 426 .709 .620 .444 .840
In your program, are there Latinos represented in administrative support positions? 421 .770 .691 .425 .832
In your program, are there Latinos represented in board positions? 413 .789 .712 .418 .830
In your program, are there Latinos represented in agency consultants? 410 .816 .750 .416 .827
In your program, are there Latinos represented in subcontractors? 400 .711 .711 .420 .831
Full scale .443 .858
Obs observations
Guerrero et al. Implementation Science (2017) 12:133 Page 6 of 12

These factors are associated with implementation of newpractices in addiction health services [26, 63, 66].
Statistical analysesStudies have shown that leadership across organizationsis nested in different settings [67], requiring adjustmentfor context to properly evaluate leadership influence. Inthis case, hierarchical linear modeling was needed toanalyze nested data [68]. In our study, we accounted forcontrol variables, program funding, license, professionalaccreditation, and professionalism, which play a role inthe implementation and delivery of new practices [26,69]. The hierarchical linear modeling analysis consid-ered staff members at level 1 to be nested in programsat level 2.As reported in other studies using these data [65], be-
cause we assumed data was missing at random, we reliedon maximum likelihood estimation in multivariate re-gressions, which allows us to obtain unbiased estimateparameters [70]. Our highest rate of missing data for anygiven variable was 4%. This procedure was conducted inStata/SE version 12.Confirmatory factor analysis was conducted in Stata/
SE using maximum likelihood estimation procedures aswell to validate our measure of climate for the imple-mentation of cultural competence consistent with otherorganizational level research [71]. The results of the ana-lysis are shown in Tables 2 and 3.To validate our measure of climate for the implemen-
tation of cultural competence and determine whether itis a unit-level construct, we relied on established meth-odologies applied to organizational constructs followingthe approach used by Glisson and James ([72], p. 780).First, we used 'confirmatory factor analysis to determinewhether responses justify a latent concept of climate forimplementation of cultural competence. Second, we con-ducted a within-group consistency analysis using rWG totest whether members of each of the 112 treatmentprograms agreed with one another in their responses tothe leadership scales [73]. This approach is common inorganizational research to justify whether individual levelresponses can be aggregated and represent programmeasures. Third, we conducted between-group analysisusing eta squared via analysis of variance and intraclasscorrelation coefficient via hierarchical linear modeling totest between-group differences among program staffmembers for each construct.' [74].Finally, we used hierarchical linear modeling path ana-
lyses in Stata version 13. We selected a random-interceptsmodel to estimate relationships between individual-levelmeasures nested in programs [68, 75]. Specifically, we ranthree regression models, one per outcome, while control-ling for program regulation, funding, and professionalismto estimate the contribution of transformational leadership
to cultural competence outcomes via climate for the imple-mentation of cultural competence. Our analyses used indi-vidual measures while controlling for staff measuresembedded in programs. The path model was imple-mented using the GSEM builder in Stata/SE version12. This model studied both the direct effects of thecausal variable (i.e., transformational leadership) onthe outcome (culturally responsive practices) and itsindirect effects through the mediator (implementationclimate). These analyses respond to the main researchquestion: To what extent does climate for implemen-tation of cultural competence play a mediating role inthe relationship between transformational leadershipand program implementation of cultural competence(knowledge, services, and personnel practices)?
ResultsWe conducted confirmatory factor analysis to validateour outcome measures of cultural competence and me-diator variable of climate for implementation of culturalcompetence. The 57-item measure of cultural compe-tence [6] resulted in three dimensions of organizationalcultural competence—knowledge (six items), servicepractices (nine items), and personnel practices (nineitems)—that are consistent with theoretical and empir-ical descriptions of this concept [4–6]. See Table 2.
Table 3 Psychometric properties of climate for theimplementation of cultural competence
Item Obs M (SD) ICC Awg α
Item 1: Supervisor provides incentivesto the staff to become linguisticallyand culturally responsive, despiteinvestment of time and resources
237 2.916(1.121)
0.596(0.434)
.885
Item 2: Supervisor createsopportunities to talk to the staff aboutways to respond to clients’ culturaland linguistic service needs despite hisor her other administrativeresponsibilities (e.g., documentationand billing)
239 3.410(1.045)
0.665(0.285)
.847
Item 3: Supervisor provides clearguidance about how to respond toclients’ cross-cultural issues despitebusy schedule
241 3.577(1.014)
0.602(0.410)
.829
Item 4: Supervisor has emphasized theimportance of translation of materialand development of policies andprocedures to respond to clients withlimited English proficiency, despite heror his other multiple responsibilities
238 3.378(1.043)
0.540(0.449)
.845
Item 5: Supervisor prioritizesenhancing the staff’s culturalcompetence by helping resolvecross-cultural issues with clients
240 3.546(0.967)
0.636(0.453)
.850
Test scale .07 0.774(0.221)
.878
Guerrero et al. Implementation Science (2017) 12:133 Page 7 of 12

Cultural competence: knowledgeWe excluded two of the original eight items becausethey had item-rest correlations less than .50, resulting ina six-item scale. As shown in Table 2, Cronbach’s alphafor this scale was very high (.88), with all items contrib-uting in the same direction and item-test and item-restcorrelations greater than .56. Therefore, for ease of inter-pretation, we averaged the six items to create a new ag-gregate measure.
Cultural competence: service practicesAfter inconsistent results, we reduced the original 14items to nine that contributed in the same direction andhad consistent levels of item-test and item-rest correla-tions, with only one less than .57. As seen in Table 2,Cronbach’s alpha for this scale was high (.86). We createda new aggregated scale to measure culturally competentservice practices by averaging the final nine items.
Cultural competence: personnel practicesWe excluded seven of the original 16 items because theyhad inconsistent item-test (< .74) and item-rest (< .67)correlations. As shown in Table 2, the resulting nine-item scale had a high Cronbach’s alpha (.86) and allitems contributed in the same direction. As in the previ-ous measures, these items were averaged to create a newaggregate measure.
Climate for implementation of cultural competenceAs seen in Table 3, Cronbach’s alpha for midlevelleaders’ prioritization of implementing cultural compe-tence was very high (.88). In addition, all items contrib-uted in the same direction and had item-test and item-rest correlations greater than .57. Given this informationand for ease of interpretation, we created a new measureby averaging our items representing promoted,rewarded, and expected culturally competence practices.
Within- and between-group analysesWe computed indexes of within- and between-programconsistency of responses for the measure of program cli-mate for implementation of cultural competence. Wecalculated rWG values to assess within-programconsistency and found an average rWG of .72 (not re-ported in tables), indicating a high level of consistencyof responses within programs. We calculated intraclasscorrelation coefficients and reviewed the eta-squaredvalues to determine between-program differences of .68.The intraclass correlation coefficient (type 1 indicatesthe proportion of total variance between programs,whereas eta squared indicates the proportion of totalvariation between programs [68, 72, 76, 77]. Type 1intraclass correlation coefficient values (.07 in this study)are typically less than .20 and usually smaller than eta-
squared values [76] supporting that program member-ship contributed to the resulting estimates. Theconsistency in within-program responses and discrep-ancy in between-program variance justified aggregatingindividual-level responses to the program level on mea-sures of climate for implementation of cultural compe-tence. This program-level measure was included in thefollowing cross-level analyses of relationships betweenindividual-level and program-level variables.
Path analysis: hypothesis testingResults from each of the three path regression analysesindicated that transformational leadership was indirectlyassociated with implementation of three culturallycompetent practice outcomes through climate forimplementation of cultural competence. See Fig. 1. Wedescribe the results of the path analysis based on thethree study hypotheses.We found support for hypothesis 1, which posited that
transformational leadership would be positively and in-directly related to the implementation of culturally com-petent knowledge through climate for implementation ofcultural competence. Employees’ and supervisors’ higherratings of their director’s transformational leadershipwere indirectly associated with higher degree of imple-mentation of culturally competent knowledge(standardized indirect effect = .006, bootstrap p = .004).We found support for hypothesis 2, which posited that
transformational leadership would be positively and indir-ectly related to the implementation of culturally compe-tent service practices through climate for implementationof cultural competence. Employees’ and supervisors’higher ratings of their director’s transformational leader-ship were indirectly associated with higher degree of im-plementation of service practices (standardized indirecteffect = .019, bootstrap p < .001).We found support for hypothesis 3, which posited that
transformational leadership would be positively and in-directly related to the implementation of culturally com-petent personnel practices through the role of climatefor implementation of cultural competence. Employees’and supervisors’ higher ratings of their director’s trans-formational leadership were indirectly related to higherdegree of implementation of culturally competentpersonnel practices (standardized indirect effect = .014,bootstrap p = .005). The main mediation models pre-sented adequate fit statistics (χ2 = 127.20, df = 22, p< .001, RMSEA < .001, CFI ≈ 1.000, TLI ≈ 1.000).Compared with the indirect relationships found, the
analysis highlighted stronger direct relationships amongvariables of interest. Transformational leadership waspositively associated with climate for implementation ofcultural competence (standardized indirect effect = .057,bootstrap p < .001). In particular, the relationship between
Guerrero et al. Implementation Science (2017) 12:133 Page 8 of 12

climate for implementation of cultural competence andpractices were robust—climate was positively associatedwith knowledge (standardized direct effect = .103, boot-strap p = .025), service practices (standardized direct ef-fect = .336, bootstrap p < .001), and personnel practices(standardized direct effect = .241, bootstrap p < .001).
DiscussionThe current study examined three areas: (a) exploration ofa focused climate and development of an associated meas-ure, climate for implementation of cultural competence;(b) development of culturally competent practices mea-sures; and (c) examination of the model (relationships be-tween leadership and these new measures). Findingshighlight the importance of focused climates in maximiz-ing the influence of transformational leadership on em-ployees’ implementation of congruent practices in healthcare. The measure representing climate for implementa-tion of cultural competence had adequate psychometricproperties and was further used to test a conceptualframework of the role of leadership in implementationprocesses in addiction health services organizations.The culturally competent practices measures had ad-
equate psychometric properties. The three measures(knowledge, services, and personnel practices) repre-sented main areas of cultural competence in health care[3–5]. The examination of the relationships betweenleadership and these new program measures revealed as-sociations among employee perceptions of executive orupper level directors leadership style, perceptions ofmiddle managers’ expectations, promotion, and rewardsregarding the implementation of cultural competence(climate), and their reported implementation of in-creased knowledge about racial and ethnic minoritycommunities, culturally tailored service practices, andculturally tailored personnel practices. We found that di-rectors’ transformational leadership influenced supervi-sors’ expectations to implement cultural competence andthat this cascading influence may affect implementation ofcongruent culturally responsive practices. These findingsextend knowledge regarding the role of leadership and cli-mate in the implementation process in health care.
Theoretical implicationsFindings contribute to leadership theory on the embeddedmechanisms that explain leadership influence on climateand practice implementation. Findings are consistent withemerging studies supporting the leadership–climate–prac-tice mechanism in different organizational settings [14, 15,78]. Because few studies have investigated the leadershipprocess of implementation of cultural competence, our pri-mary contribution lies in developing a measure of climatefor implementation of cultural competence and identifying
its relationship with the implementation of three validatedmeasures of culturally responsive practices.At the core of the leadership process related to influ-
encing followers’ attitudes and behavior is the role of so-cial exchange explained by social learning theory [79,80]. However, additional embedded mechanisms play arole in influencing followers’ attitudes and behaviors. Forinstance, the social learning model relies on transform-ational leaders’ modeling behavior to emphasize princi-ples (e.g., culture matters) and norms and behaviors(e.g., service providers should understand their clients’culture to serve them effectively). These principles andnorms may influence followers including middle man-agers, who in turn play a critical role in developing andmaintaining an organizational climate focused on imple-mentation of cultural competence [14, 15].By considering additional embedded mechanisms and
players in the social exchange dynamics described in sociallearning theory, this study highlights the importance ofconsidering the hierarchical and role functions of trans-formational (executive) leaders and middle managers.Transformational leaders promote growth and a commonvision [21, 81]. However, middle managers may need totranslate this vision into specific priorities, norms, and be-haviors that are actionable at the employee level. Execu-tive leaders may value culture, whereas middle managersprioritize employee cross-cultural training and employeesbuild their knowledge of clients’ cultural backgrounds andtailored service practices.
Limitations and suggestions for future researchWe acknowledge that our data have several limitationsthat should be considered when interpreting our find-ings. We did not test causal or temporal relationshipsbecause we relied on cross-section data, but informed bya conceptual framework. Second, program measureswere provided by an average of three staff members perprogram, not including more individuals to indicategreater agreement on program climate for implementa-tion of cultural competence can be a limitation. How-ever, these outpatient clinics are generally small,independent, and similar to doctor’s offices. As such,these programs represent work environments that influ-ence shared perceptions. We also acknowledge limita-tions on our measurement approach. We relied onindividual respondent data and controlled for theirnested structure instead of examining a true cross-levelinteraction relying only on measures separately aggre-gated at the counselor, supervisor, and director levels.Also, our measurement of climate for implementation,which relied on employees’ perceptions of supervisors’priorities, or what is expected, rewarded, and promoted,needs to be further evaluated in terms of its discriminantvalidity. Emerging research has highlighted a strong
Guerrero et al. Implementation Science (2017) 12:133 Page 9 of 12

relationship between middle managers’ reported com-mitment to innovation and implementation effectiveness[82, 83]. Distinguishing between middle-managers’ self-reported commitment to implementation and em-ployees’ perceptions of their manager’s expectations, re-wards, and priorities is critical to identifying differentmechanisms of implementation.Finally, we consider a limitation measuring implemen-
tation based on staff members’ reports of their program’sdelivery or use of culturally responsive practices, ratherthan directly observing practices being implemented.Nonetheless, we relied on large, multilevel data fromemployees nested in programs and measures featuringdifferent scales. This last issue reduces commonmethods bias and improves the rigor of our analysis.
ConclusionsFindings underscore the empirical and theoretical im-portance of the leadership–climate relationship to imple-menting culturally competent practices in addictionhealth services. This is an important goal for these pro-grams, which are located in one of the most ethnicallydiverse communities in the USA. Therefore, leadershipdevelopment initiatives in health care can focus onteaching leaders to align incentives and communicatemessages consistent with desired practices. Findings arerelevant to executive leaders who may use a transform-ational leadership style (e.g., employee promotion) to in-fluence midlevel supervisors’ implementationexpectations and priorities. By doing so, program leaderscan establish an effective leadership–climate–practiceapproach in their programs that strategically aligns di-rectors’, supervisors’, and employees’ focus to enhancetheir organization’s capacity to implement culturallycompetent services for racial and ethnic minority clients.
AcknowledgementsWe appreciate the contributions of participants in the study. We also thankVeronica Serret and Tenie Khachikian for their support in summarizing dataand Eric Lindberg for proofreading and editing the final draft.
FundingFunding for the first author’s role in this study was provided by a NationalInstitute on Drug Abuse research grant (R33DA035634) and animplementation fellowship training grant (R25MH080916). This work was alsosupported by National Institute on Drug Abuse grant (R01DA038466) andNational Institute of Mental Health grant (R01MH072961). The content issolely the responsibility of the authors and does not necessarily representthe official views of the National Institutes of Health.
Availability of data and materialsPlease contact authors for data requests.
Authors’ contributionsEG was the study principal investigator and developed the theoreticalbackground and conceptualization of the study. KF developed the literaturereview, and YK contributed to the study design, writing, data analysis, andediting. All authors read and approved the final manuscript.
Ethics approval and consent to participateThis research was performed in accordance with the Declaration of Helsinkiand approved by the Institutional Review Board at University of SouthernCalifornia (No. UP-14-00105).
Consent for publicationNot applicable.
Competing interestsThe authors declare that they have no competing interests.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations.
Author details1Suzanne Dworak-Peck School of Social Work, University of SouthernCalifornia, 655 West 34th Street, Los Angeles, CA 90089, USA. 2MarshallSchool of Business, University of Southern California, 655 West 34th Street,Los Angeles, CA 90089, USA. 3Mihaylo College of Business and Economics,California State University, Fullerton, Fullerton, CA 90089, USA.
Received: 25 January 2017 Accepted: 6 November 2017
References1. Institute of Medicine. Crossing the quality chasm: a new health system for
the twenty-first century. Washington, DC: National Academies Press; 2001.2. Institute of Medicine. Unequal treatment: confronting racial and ethnic
disparities in health care. Washington, DC: National Academies Press; 2013.3. Betancourt JR, Green AR, Carrillo JE, Park ER. Cultural competence and
health care disparities: key perspectives and trends. Health Aff. 2005;24:499–505.
4. Brach C, Fraser I. Can cultural competency reduce racial and ethnic healthdisparities? A review and conceptual model. Med Care Res Rev. 2000;57(suppl 1):181–217.
5. Harper M, Hernandez M, Nessman T, Mowery D, Worthington J, Issacs M.Organizational cultural competence: a review of assessment protocols.Tampa: University of South Florida, College of Behavioral and CommunitySciences, Louis de la Parte Florida Mental Health Institute, Department ofChild and Family Studies, Research and Training Center for Children’sMental Health; 2009.
6. Mason JL. Cultural competence self-assessment questionnaire: a manual forusers. Portland: Portland State University, Research and Training Center onFamily Support and Children’s Mental Health; 1995.
7. Klein KJ, Sorra JS. The challenge of innovation implementation. Acad ManagRev. 1996;21:1055–80.
8. Fiscella K, Franks P, Gold MR, Clancy CM. Inequality in quality. JAMA. 2000;283:2579–84.
9. Becan JE, Knight DK, Flynn PM. Innovation adoption as facilitated by achange-oriented workplace. J Subst Abus Treat. 2012;42:169–78.
10. Guerrero EG, Garner BR, Cook B, Kong Y. Does the implementation ofevidence-based and culturally competent practices reduce disparities inaddiction treatment outcomes? Addict Behav. 2017;73:119–23.
11. Battilana J, Gilmartin M, Sengul M, Pache AC, Alexander JA. Leadershipcompetencies for implementing planned organizational change. LeadershQ. 2010;21:422–38.
12. Dinh JE, Lord RG, Gardner WL, Meuser JD, Liden RC, Hu J. Leadership theoryand research in the new millennium: current theoretical trends andchanging perspectives. Leadersh Q. 2014;25:36–62.
13. Zohar D. The effects of leadership dimensions, safety climate, and assignedpriorities on minor injuries in work groups. J Organ Behav. 2002;23:75–92.
14. Zohar D. Safety climate: conceptualization, measurement, andimprovement. In: Schneider B, Barbera KM, editors. The Oxford handbook oforganizational climate and culture. New York: Oxford University Press; 2014.p. 317–34.
15. Schneider B, Ehrhart MG, Macey WH. Organizational climate and culture.Annu Rev Psychol. 2013;64:361–88.
16. Aarons GA, Ehrhart MG, Farahnak LR, Sklar M. Aligning leadership acrosssystems and organizations to develop strategic climate for evidence-basedpractice implementation. Annu Rev Public Health. 2014;35:255–74.
Guerrero et al. Implementation Science (2017) 12:133 Page 10 of 12

17. Judge TA, Piccolo RF. Transformational and transactional leadership: a meta-analytic test of their relative validity. J Appl Psychol. 2004;89:755–68.
18. Yukl G. Effective leadership behavior: what we know and what questionsneed more attention. Acad Manag Perspect. 2012;26(4):66–85.
19. Bass BM, Avolio BJ. Improving organizational effectiveness throughtransformational leadership. Thousand Oaks: Sage; 1994.
20. Piccolo RF, Bono JE, Heinitz K, Rowold J, Duehr E, Judge TA. The relativeimpact of complementary leader behaviors: which matter most? LeadershQ. 2012;23:567–81.
21. Bass BM, Avolio BJ, Jung DI, Berson Y. Predicting unit performance byassessing transformational and transactional leadership. J Appl Psychol.2003;88:207–18.
22. Edmondson AC. Managing the risk of learning: psychological safety in workteams. In: West MA, Tjosvold D, Smith KG, editors. International handbook oforganizational teamwork and cooperative working. Chichester: Wiley; 2002.p. 255–75.
23. Zhu W, Riggio RE, Avolio BJ, Sosik JJ. The effect of leadership on followermoral identity: does transformational/transactional style make a difference?J Leadersh Org Stud. 2011;18:150–63.
24. Aarons GA. Transformational and transactional leadership: association withattitudes toward evidence-based practice. Psychiatr Serv. 2006;57:1162–9.
25. Aarons GA, Sommerfeld DH. Leadership, innovation climate, and attitudestoward evidence-based practice during a statewide implementation. J AmAcad Child Adolesc Psychiatry. 2012;51:423–31.
26. D’Aunno T. The role of organization and management in substance abusetreatment: review and roadmap. J Subst Abus Treat. 2006;31:221–33.
27. May C. Towards a general theory of implementation. Implement Sci.2013;8:18.
28. Weiner BJ, Lewis MA, Linnan LA. Using organization theory to understandthe determinants of effective implementation of worksite health promotionprograms. Health Educ Res. 2009;24:292–305.
29. Dragoni L. Understanding the emergence of state goal orientation inorganizational work groups: the role of leadership and multilevel climateperceptions. J Appl Psychol. 2005;90:1084–95.
30. Michaelis B, Stegmaier R, Sonntag K. Shedding light on followers’innovation implementation behavior: the role of transformationalleadership, commitment to change, and climate for initiative. J ManagPsychol. 2010;25:408–29.
31. Schneider B. The climate for service: an application of the climate construct.In: Schneider B, editor. Organizational climate and culture. San Francisco:Jossey-Bass; 1990. p. 383–412.
32. Reichers AE, Schneider B. Climate and culture: an evolution of constructs. In:Schneider B, editor. Organizational climate and culture. San Francisco:Jossey-Bass; 1990. p. 5–39.
33. Schneider B. Organizational climates: an essay. Pers Psychol. 1975;28:447–79.34. Jacobs SR, Weiner BJ, Bunger AC. Context matters: measuring
implementation climate among individuals and groups. Implement Sci.2014;9:46.
35. Zohar D. Thirty years of safety climate research: reflections and futuredirections. Accid Anal Prev. 2010;42:1517–22.
36. Ehrhart MG, Schneider B, Macey WH. Organizational climate and culture: anintroduction to theory, research, and practice. New York: Routledge; 2014.
37. Schneider B, Ehrhart MG, Macey WH. Organizational climate research:achievements and the road ahead. In: Ashkanasy NM, Wilderom CPM,Peterson MF, editors. The handbook of organizational culture and climate.Thousand Oaks: Sage; 2011. p. 29–49.
38. Zohar D. A group-level model of safety climate: testing the effect of groupclimate on microaccidents in manufacturing jobs. J Appl Psychol. 2000;85:587–96.
39. Beus JM, Payne SC, Bergman ME, Arthur W. Safety climate and injuries: anexamination of theoretical and empirical relationships. J Appl Psychol. 2010;95:713–27.
40. Johnson JW. Linking employee perceptions of service climate to customersatisfaction. Pers Psychol. 1996;49:831–51.
41. Hong Y, Liao H, Hu J, Jiang K. Missing link in the service profit chain: ameta-analytic review of the antecedents, consequences, and moderators ofservice climate. J Appl Psychol. 2013;98:237–67.
42. Hunter ST, Bedell KE, Mumford MD. Climate for creativity: a quantitativereview. Creat Res J. 2007;19:69–90.
43. Scott SG, Bruce RA. Determinants of innovative behavior: a path model ofindividual innovation in the workplace. Acad Manag J. 1994;37:580–607.
44. Klein KJ, Knight AP. Innovation implementation: overcoming the challenge.Curr Dir Psychol Sci. 2005;14:243–6.
45. Klein KJ, Conn AB, Sorra JS. Implementing computerized technology: anorganizational analysis. J Appl Psychol. 2001;86:811–24.
46. Holahan PJ, Aronson ZH, Jurkat MP, Schoorman FD. Implementingcomputer technology: a multiorganizational test of Klein and Sorra’s model.J Eng Technol Manag. 2004;21:31–50.
47. Dong L, Neufeld DJ, Higgins C. Testing Klein and Sorra’s innovationimplementation model: an empirical examination. J Eng Technol Manag.2008;25:237–55.
48. Ehrhart MG, Aarons GA, Farahnak LR. Assessing the organizational contextfor EBP implementation: the development and validity testing of theImplementation Climate Scale (ICS). Implement Sci. 2014;9:157.
49. Weiner BJ, Belden CM, Bergmire DM, Johnston M. The meaning andmeasurement of implementation climate. Implement Sci. 2011;6:78.
50. Bandura A. Social foundations of thought and action: a social-cognitiveview. Englewood Cliffs: Prentice-Hall; 1986.
51. Berson Y, Avolio BJ. Transformational leadership and the dissemination oforganizational goals: a case study of a telecommunication firm. Leadersh Q.2004;15:625–46.
52. Chreim S, Williams BE, Coller KE. Radical change in healthcare organization:mapping transition between templates, enabling factors, andimplementation processes. J Health Organ Manag. 2012;26:215–36.
53. Schein EA. Organizational culture and leadership. 2nd ed. San Francisco:Jossey-Bass; 1992.
54. Wimbush JC, Shepard JM. Toward an understanding of ethical climate: itsrelationship to ethical behavior and supervisory influence. J Bus Ethics. 1994;13:637–47.
55. Zohar D. The influence of leadership and climate on occupational healthand safety. In: Hofmann DA, Tetrick LE, editors. Health and safety inorganizations: a multilevel perspective. San Francisco: Jossey-Bass; 2003. p.201–30.
56. Zohar D, Luria G. Climate as a social-cognitive construction of supervisorysafety practices: scripts as proxy of behavior patterns. J Appl Psychol. 2004;89:322–33.
57. Aarons GA, Ehrhart MG, Farahnak LR. The implementation leadership scale(ILS): development of a brief measure of unit level implementationleadership. Implement Sci. 2014;9:45.
58. Jung DI, Chow C, Wu A. The role of transformational leadership inenhancing organizational innovation: hypotheses and some preliminaryfindings. Leadersh Q. 2003;14:525–44.
59. Carr JZ, Schmidt AM, Ford JK, DeShon RP. Climate perceptions matter: ameta-analytic path analysis relating molar climate, cognitive and affectivestates, and individual level work outcomes. J Appl Psychol. 2003;88:605–19.
60. Gil F, Rico R, Alcover CM, Barrasa Á. Change-oriented leadership, satisfactionand performance in work groups. J Manag Psychol. 2005;20:312–28.
61. Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed.Hillsdale: Lawrence Erlbaum; 1988.
62. Broome KM, et al. Leadership, burnout, and job satisfaction in outpatientdrug-free treatment programs. J Subst Abus Treat. 2009;37:160–70.
63. Guerrero EG. Enhancing access and retention in substance abuse treatment:the role of Medicaid payment acceptance and cultural competence. DrugAlcohol Depend. 2013;132:555–61.
64. Guerrero EG, Aarons GA, Palinkas LA. Organizational capacity for serviceintegration in community-based addiction health services. Am J PublicHealth. 2014;104:e40–7.
65. Guerrero EG, He A, Kim A, Aarons GA. Organizational implementation ofevidence-based substance abuse treatment in racial and ethnic minoritycommunities. Adm Policy Ment Health Ment Health Serv Res. 2014;41:737–49.
66. Guerrero EG. Managerial capacity and adoption of culturally competentpractices in outpatient substance abuse treatment organizations. J SubstAbus Treat. 2010;39:329–39.
67. Snijders TB, Bosker RR. Multilevel analysis: an introduction to basic andadvanced multilevel modeling. Thousand Oaks: Sage; 1999.
68. Bryk AS, Raudenbush SW. Hierarchical linear models. Newbury Park: Sage;1992.
69. Roman PM, Ducharme LJ, Knudsen HK. Patterns of organization andmanagement in private and public substance abuse treatment programs. JSubst Abus Treat. 2006;31:235–43.
70. Allison PD. Missing data: quantitative applications in the social sciences. Br JMath Stat Psychol. 2002;55:193–6.
Guerrero et al. Implementation Science (2017) 12:133 Page 11 of 12

71. Aarons GA, Sawitzky AC. Organizational culture and climate and mentalhealth provider attitudes toward evidence-based practice. Psychol Serv.2006;3:61–72.
72. Glisson C, James LR. The cross-level effects of culture and climate in humanservice teams. J Organ Behav. 2002;23:767–94.
73. James LR, Demaree RG, Wolf G. rwg: an assessment of within-groupinterrater agreement. J Appl Psychol. 1993;78:306–9.
74. Rentsch JR. Climate and culture: interaction and qualitative differences inorganizational meanings. J Appl Psychol. 1990;75:668–81.
75. Hedeker D, Gibbons RD, Flay BR. Random-effects regression models forclustered data with an example from smoking prevention research. JConsult Clin Psychol. 1994;62:757–65.
76. Bliese PD. Within-group agreement, non-independence, and reliability:implications for data aggregation and analysis. In: Klein KJ, Kozlowski SW,editors. Multilevel theory, research, and methods in organizations. SanFrancisco: Jossey-Bass; 2000. p. 349–81.
77. Cohen J, Cohen P. Applied multiple regression/correlation analysis for thebehavioral sciences. 2nd ed. Hillsdale: Lawrence Erlbaum; 1983.
78. Aarons GA, Ehrhart MG, Farahnak LR, Hurlburt MS. Leadership andorganizational change for implementation (LOCI): a randomized mixedmethod pilot study of a leadership and organization developmentintervention for evidence-based practice implementation. Implement Sci.2015;10:11.
79. Bass BM, Waldman DA, Avolio BJ, Bebb M. Transformational leadership andthe falling dominoes effect. Group Org Manag. 1987;12:73–87.
80. Mayer DM, Kuenzi M, Greenbaum R, Bardes M, Salvador RB. How low doesethical leadership flow? Test of a trickle-down model. Organ Behav HumDecis Process. 2009;108:1–13.
81. Avolio BJ, Gardner WL, Walumbwa FO, Luthans F, May DR. Unlocking themask: a look at the process by which authentic leaders impact followerattitudes and behaviors. Leadersh Q. 2004;15:801–23.
82. Birken SA. Where the rubber meets the road: a mixed-method study ofmiddle managers’ role in innovation implementation in health careorganizations. Chapel Hill: University of North Carolina at Chapel Hill; 2011.
83. Birken SA, Lee SY, Weiner BJ, Chin MH, Schaefer CT. Improving theeffectiveness of health care innovation implementation: middle managersas change agents. Med Care Res Rev. 2013;70:29–45.
• We accept pre-submission inquiries
• Our selector tool helps you to find the most relevant journal
• We provide round the clock customer support
• Convenient online submission
• Thorough peer review
• Inclusion in PubMed and all major indexing services
• Maximum visibility for your research
Submit your manuscript atwww.biomedcentral.com/submit
Submit your next manuscript to BioMed Central and we will help you at every step:
Guerrero et al. Implementation Science (2017) 12:133 Page 12 of 12