Embed Size (px)
Citation preview

Adverse metaphase cytogenetics can be overcome by adding bortezomib and thalidomide to fractionated melphalan transplants
Yogesh S Jethava1, Alan Mitchell2, Joshua Epstein1, Maurizio Zangari1, Shmuel Yaccoby1, Erming Tian1, Sarah Waheed1, Rashid Khan1, Xenofon Papanikolaou1, Monica Grazziutti1, Michele Cottler-Fox3, Nathan Petty1, Douglas Steward1, Susan Panozzo1, Clyde Bailey1, Antje Hoering2, John Crowley2, Jeffrey Sawyer3, Gareth Morgan1, Bart Barlogie1 and Frits van Rhee1
1 Myeloma Institute, University of Arkansas for Medical Sciences, Little Rock, AR; 2
Cancer Research And Biostatistics, Seattle, WA; 3 Department of Pathology, University of Arkansas for Medical Sciences.
Running title: Randomized auto-transplant trial for low-risk myeloma
Corresponding author:
Frits van Rhee, MD, PhD Myeloma Institute University of Arkansas for Medical Sciences 4301 W Markham, #816 Little Rock, AR 72205 USA Phone: 501-526-2873 Fax: 501-526-2273 Email: [email protected]
Key Point: Conditioning with melphalan, bortezomib and thalidomide confers benefit to myeloma with abnormal metaphase cytogenetics.
Abstract count: 246 words
Text Count: 2,675 words
References: 30
Conflict of Interest Disclosure: There are no relevant conflicts to disclose.
Grant Support:
Total Therapy 4 was supported by the National Cancer Institute, National Institutes of Health Program Project Grant CA55819 (to Dr. Gareth Morgan).
Research. on January 9, 2020. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on November 3, 2016; DOI: 10.1158/1078-0432.CCR-15-2620

2
Translational Relevance
Melphalan 200mg/m2 is widely considered the standard preparatory regimenfor
autologous stem cell transplantation for myeloma. Attempts to improve conditioning with
melphalan have not been successful and included the addition of other cytotoxic agents,
skeletal targeting radioactive antibodies or radiation therapy. The present study
suggests that patients with abnormal metaphase cytogenetics, who traditionally fare
worse than their counterparts with normal metaphase cytogenetics, may benefit from
the addition of bortezomib, thalidomide and dexamethasone to a fractionated melphalan
(50mg/m2/d x 4d) conditioning regimen. Conversely, patients with a normal karyotype
are best served with preparation comprising melphalan 200mg/m2 given in a single
dose. These findings, if confirmed suggest that specific autologous stem cell
transplantation conditioning regimens can improve outcome in subgroups of myeloma
patients.
Abstract
Purpose. To determine whether a reduction in the intensity of Total Therapy (TT)
reduces toxicity and maintains efficacy.
Experimental design. 289 patients with gene expression profiling (GEP70)-
defined low-risk multiple myeloma (LRMM) were randomized between a standard arm
(TT4-S) and a light arm (TT4-L). TT4-L employed 1 instead of 2 inductions and
consolidations. To compensate for potential loss of efficacy of TT4-L, bortezomib and
thalidomide were added to fractionated melphalan 50mg/m2/d x 4.
Research. on January 9, 2020. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on November 3, 2016; DOI: 10.1158/1078-0432.CCR-15-2620

3
Results. Grade ≥3 toxicities and treatment-related mortalities were not reduced
in TT4-L. Complete response (CR) rates were virtually identical (p=0.2; TT4-S, 59%:
TT4-L, 61% at 2 years), although CR duration was superior with TT4-S (p=0.05; TT4-S,
87%; TT4-L, 81% at 2 years. With a median follow-up of 4.5yr, there was no difference
in overall survival (OS) and progression-free survival (PFS). While metaphase
cytogenetic abnormalities (CA) tended to be an adverse feature in TT4-S, as with
predecessor TT trials, the reverse applied to TT4-L. Employing historical TT3a as
training and TT3b as test set, 51 gene probes (GEP51) significantly differentiated the
presence and absence of CA (q<0.0001), 7 of which function in DNA replication,
recombination, and repair. Applying the GEP51 model to clinical outcomes, OS and
PFS were significantly inferior with GEP51/CA in TT4-S; such difference was not
observed in TT4-L.
Conclusions. We identified a prognostic CA-linked GEP51 signature, the
adversity of which could be overcome by potentially synergizing anti-MM effects of
melphalan and bortezomib. These exploratory findings require confirmation in a
prospective randomized trial.
Introduction
With the incorporation of novel agents into auto-transplant-supported high-dose
melphalan trials, the outlook of patients with multiple myeloma (MM) has greatly
improved. In our Total Therapy (TT) program, applying all MM-active agents up-front in
order to reduce or even eliminate the development or survival of drug-resistant sub-
clones, major advances have been linked to the addition of thalidomide in TT2 and
Research. on January 9, 2020. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on November 3, 2016; DOI: 10.1158/1078-0432.CCR-15-2620

4
bortezomib in TT3 (1, 2). However, when examined in the context of gene-expression
profiling (GEP) of CD138-purified plasma cells, such benefit was limited to the 85% of
patients presenting with GEP70-based low-risk MM (LR-MM) (3, 4). In recognition of the
lack of progress in high-risk MM (HR-MM), we decided in 2008 to assign low and high
risk patients to separate protocols. We are now reporting on clinical outcomes of 289
patients with LR-MM enrolled in a randomized phase III trial of Total Therapy 4 (TT4),
comparing a light arm (TT4-L) to a standard arm (TT4-S), with the goal of reducing
toxicity while maintaining efficacy in TT4-L.
Materials and Methods
The protocol schema is portrayed in supplementary table 1. Briefly, eligible
patients with GEP70-defined LR-MM were randomized between TT4-S and TT4-L. TT4
induction in both arms was similar to TT3b except for the addition of melphalan
10mg/m2 test-dosing 48hr following bortezomib 1.0mg/m2 test-dosing for the purpose of
pharmacogenomic investigations (5, 6). TT4-L differed from TT4-S by reduction from 2
cycles to 1 cycle each of induction with M-VTD-PACE prior to and consolidation with
dose-reduced VTD-PACE after tandem transplants. The transplant regimen in L-TT4
was altered from a single melphalan dose of 200mg/m2 (MEL200) in TT4-S to a
fractionated 50mg/m2/d x 4d (MEL50x4) schedule with the aim to avoid peak MEL dose
levels and reduce mucosal toxicity. To compensate for the potentially reduced efficacy
of this strategy, bortezomib, thalidomide, and dexamethasone (VTD) were added to the
fractionated MEL to exploit the observed synergism between MEL and VTD (7, 8).
Maintenance therapy was with bortezomib, lenalidomide and dexamethasone (VRD) in
both arms for 3 years. Two-hundred eighty-nine patients were randomized (TT4-S,
Research. on January 9, 2020. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on November 3, 2016; DOI: 10.1158/1078-0432.CCR-15-2620

5
n=145; TT4-L, n=144) and stratified by ISS stage and the presence of metaphase
cytogenetic abnormalities (CA). Metaphase abnormalities were deemed to be present if
at least 2 cells with the same karyotype were present. Protocol eligibility included age
>18yr and =<75yr and normal cardio-pulmonary function; liver function tests could be up
to twice normal; and creatinine levels up to 3mg/dL were acceptable. Patients had to
have active and measurable MM fulfilling CRAB criteria (9). All patients had to sign a
written informed consent in keeping with institutional, national and Helsinki Declaration
guidelines. The protocol and its revisions had been approved by the institutional review
board, which received annual progress reports. As TT4 was supported with a grant from
the National Cancer Institute, a Data Safety and Monitoring Board (DSMB) reviewed
toxicities and efficacies at least annually. We also had independent data audits every 6
to 8 months to verify adherence to protocol stipulations, examine pharmacy records and
informed consents, and verify recorded toxicities especially causes of death (COD) and
clinical efficacy in terms of complete response (CR) and CR duration (CRD),
progression-free survival (PFS) and overall survival (OS).
Patient work up was per protocol and was similar to our practice in TT3 (2).
Special studies included GEP of plasma cells (GEP-PC) and whole bone marrow
biopsies GEP-BMBX), procured from both random iliac crest sites and from magnetic
resonance imaging (MRI)-defined focal lesions under computer-assisted tomography
guidance. Random bone marrow samples were submitted for metaphase cytogenetic
analysis and interphase fluorescence in situ hybridization (FISH) for the detection of
deletion 17 p and amplification of 1q21. The protocol called for serial short-term and
longer-term studies of GEP and MRI as well as 18-fluoro-deoxyglucose positron
Research. on January 9, 2020. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on November 3, 2016; DOI: 10.1158/1078-0432.CCR-15-2620

6
emission tomography (PET). Pharmacogenomic studies called for repeat GEP sampling
from random iliac crest bone marrow and MRI-defined focal lesion(s) 48 hours after
test-dosing with bortezomib 1.0mg/m2 and again 48 hours after test-dosing with
melphalan 10mg/m2 prior to starting the full VTD-PACE program. PET follow-up studies
were scheduled on day 5 after commencing VTD-PACE and prior to first
transplantation. These correlative studies will be the subject of a separate report. Most
patients were treated in the outpatient setting and were checked daily by MM-
experienced nursing staff and weekly by their physicians. Hematopoietic progenitor
collection was started when CD34 collection criteria were met with the goal to procure at
least 20 million CD34 cells per kilogram body weight.
The primary clinical endpoint was reduction in toxicity in TT4-L versus TT4-S.
Secondary endpoints included complete response (CR) defined according to IMWG
criteria, the duration of which was measured from its onset to progression or death (10).
Overall survival (OS) was calculated from registration until the date of death.
Progression-free survival (PFS) was similarly calculated, but also incorporated
progressive disease as an event. Time to progression (TTP) was measured from
registration until the date of progression or relapse, whereas time to relapse (TTR)
focused on the subset of patients achieving CR. Death without prior progression or
relapse was included as a competing risk in analyses of TTP and TTR. Post-relapse
survival (PRS) was measured from the date of relapse or progression until death. For
all time-to-event analyses, patients were censored at the date they were last known to
be alive. Causes of death (COD) included treatment-related mortality (TRM), myeloma-
related mortality (MRM), and a third category capturing other or indeterminate causes
Research. on January 9, 2020. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on November 3, 2016; DOI: 10.1158/1078-0432.CCR-15-2620

7
(OIM) such as fatal car accident, stroke and other causes that could not be attributed to
treatment or disease. Toxicities were graded according to Version 3 of the NCI
After accrual and randomization of 289 patients, the DSMB recommended
closure of the TT4-L arm due to lack of reduction in toxicity vis-à-vis TT4-S. Two
patients randomized to TT4-L, were treated according to the standard arm after the
DSMB recommend closure of TT4-L.These patients are accounted for in the 289
patients. Higher mortality at 1 year in patients ≥65yr on both arms (10.6% and 10.2%
for TT4-L and TT4-S) prompted subsequent accrual of 74 such patients to Total
Therapy 6 (TT6) designed for previously treated patients, because its less dose-intense
therapies had resulted in TRM of 0% (11). Younger patients continue enrollment to
TT4-S but only the 289 randomized patients are the subject of this report.
Statistical Analysis
The data set was created on January 16, 2015 on 289 patients randomized
between TT4-S and TT4-L. In accordance with the intent-to-treat principle, all patients
were analyzed according to their randomized arm. The Kaplan-Meier method was used
to estimate the distributions of OS, PFS and CR duration (12). Cumulative incidences
for COD, TTP and TTR were calculated using the method of Gooley, et al. (13). Group
comparisons for survival endpoints and cumulative incidence were performed using the
log-rank test (14). Multivariate models of prognostic factors were carried out using Cox
regression (15). P-values <0.05 were considered statistically significant.
Results
Clinical Outcomes
Research. on January 9, 2020. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on November 3, 2016; DOI: 10.1158/1078-0432.CCR-15-2620

8
Patient characteristics are summarized in Table 1 and were not different between
the 2 arms. The consort flow diagram (supplemental figure 1) portrays the progression
of patients through the various protocol steps and lists the off-study reasons. Grade ≥ 3
toxicities occurred with similar frequencies in the 2 arms of TT4 (supplemental Table 2),
with no significant differences observed between major toxicity categories. With a
median follow-up of 4.5 years in both arms, 112 and 108 patients are alive at the time of
analysis while 100 and 92 are progression-free on TT4-S and TT4-L, respectively
(Figure 1). Two-year OS estimates are similar in both arms, 90% and 87% (Figure 1A);
the corresponding PFS estimates of 84% and 79% were also comparable (Figure 1B).
At the time of analysis, 90 and 92 had achieved CR status on TT4-S and TT4-L,
respectively, for 2-yr estimates of 59% and 61% (Figure 1C); 2-year CRD estimates are
87% and 81% (P=0.05) (Figure 1D). Median TTP was similar in both arms, with 2-yr
estimates of 8% and 11% , while there was a trend towards earlier TTR from CR on the
TT4-L arm (12% vs 8% at 2 years, p=0.07) (data not shown). COD were divided into
MRM (p=0.70), TRM (p=0.61) and OIM (p=0.25) and were not different between both
arms (Supplemental Figure 2A). Post-relapse survival (PRS) was similar in the 2 arms
(Supplemental Figure 2B).
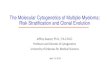
As in previous TT trials, the presence of CA affected clinical outcomes (Figure 2).
Surprisingly, the presence of CA had opposite prognostic connotations in the 2 study
arms. In TT4-S, CA showed a strong trend toward inferior OS (Figure 2A) while the
reverse applied to TT4-L (Figure 2B). Non-significant trends in opposite directions were
noted for PFS (Figure 2C, D). CRD tended to be inferior in patients with CA-type MM in
TT4-S (Figure 2E) with an opposite trend in TT4-L (Figure 2F), though neither
Research. on January 9, 2020. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on November 3, 2016; DOI: 10.1158/1078-0432.CCR-15-2620

9
comparison was statistically significant. TTR was significantly steeper in the presence of
CA in TT4-S (Figure 2G) and did not affect this outcome variable in TT4-L (Figure 2H).
Next we examined the impact of baseline factors on outcomes (Table 2 and
Table 3). The univariate cox analysis of baseline features associated with OS and PFS
across TT4 arms are summarized in Table 2. OS and PFS were inferior in the case of
older age ≥65yr, high beta-2-microglobulin (B2M) (both ≥3.5mg/L and >5.5mg/L),
presence on PET-CT of more than 3 fluoro-deoxyglucose avid focal lesions (FL), low
albumin levels (<3.5g/dL) posed a significant hazard for OS but not for PFS, and the
reverse applied to CRP elevation (≥8mg/L). There was a trend for better OS and PFS
for the CD1 and CD2 molecular subgroups (Table 2). In the presence of CA, in
comparison to its absence (no CA), OS tended to be shorter in TT4-S (p=0.08) and
longer in TT4-L (p=0.07). On multivariate analysis (Table 3), older age, B2M >5.5mg/L,
and PET-FL >3 independently imparted inferior OS and PFS. Low albumin adversely
affected OS and was of borderline significance for PFS. Patients with CA enjoyed
superior OS when randomized to TT4-L with a strong trend apparent also for PFS. In
the case of TT4-S, differences were in the opposite direction, though not significant. The
different effect of CA on outcomes by treatment arm (interaction) was statistically
significant for both OS and PFS (p = .0035 and .0491, respectively).
As we had previously reported on prognostic implication of imaging parameters,
we sought to determine whether the adverse clinical impact of PET-FL>3 pertained to
both TT4 arms (16). Regardless of treatment arm, OS and PFS were inferior for PET-FL
>3 (Supplementary Figure 3). The timing of onset of CR was not affected by PET-FL,
while CRD was superior in case of PET-FL =<3 for the TT4-S arm but not for TT4-L. A
Research. on January 9, 2020. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on November 3, 2016; DOI: 10.1158/1078-0432.CCR-15-2620

10
trend for more rapid TTP with PET-FL >3 was observed in TT4-S whereas TTP was
similar in TT4-L. TTR was significantly faster with PET-FL >3 only in case of TT4-S.
GEP probes linked to the presence of cytogenetic abnormalities (CA)
The observation of CA’s favorable OS impact in TT4-L was unexpected and at
variance with findings in all previous TT protocols (17). We therefore analyzed whether
the presence or absence of metaphase CA could be linked to certain gene probes
which might explain the superior performance in TT4-L of fractionated melphalan with
added bortezomib and thalidomide. A training set of patients with LR-MM enrolled in
TT3a was chosen for this endeavor. Among 266 untreated patients with available
baseline GEP studies, 90 (34%) exhibited CA. Among the test set of 164 patients with
baseline GEP accrued to TT3b, 67 (41%) qualified as having CA. Using a false
discovery rate of 0.0001, 51 probes significantly distinguished patients with and without
CA (Supplementary Table 3). Seven of the 51 genes function in DNA replication,
recombination, and repair; five in nucleic acid metabolism, and 4 in RNA post-
translational modification and RNA damage and repair. Ingenuity pathway analysis
identified a network of eight interrelated genes that were overexpressed in the CA
group, indicating that these MM cells have a higher proliferative activity (Supplementary
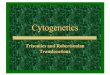
Figure 4). We then examined clinical outcomes by the GEP51-CA prediction model in
the 2 arms of TT4 (Figure 3). In TT4-S, GEP51/no-CA had superior OS and PFS
compared to GEP51/CA (Figure 3A, B), which was not observed in TT4-L (Figure 3C,
D).
Discussion
Research. on January 9, 2020. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on November 3, 2016; DOI: 10.1158/1078-0432.CCR-15-2620

11
The results of this phase-3 TT4 trial failed to show that TT4-L was less toxic and
was, in fact, inferior to TT4-S in terms of CRD with a trend for inferiority in case of TTR.
One-year mortality was similar, 7.6% in TT4-L and 6.9% in TT4-S (Fisher’s Exact Test
p=0.75), but low in both arms in younger patients (TT4-S, 6.2%; TT4-L, 5.2%).
Unanticipated were the opposite implications of the presence of CA on OS: adverse in
TT4-S (p=0.08) as in all previous TT trials, and favorable in TT4-L (p=0.07), with
significant opposite prognostic implications in the 2 study arms. The other clinical
endpoints were only marginally affected except for significantly faster TTR in case of CA
in TT4-S. When analyzed in the context of all competing variables, TT4-L impacted OS
of patients with CA-type MM favorably, with a strong trend apparent also for PFS. T It
seems reasonable to speculate that CA-type MM derived benefit from conditioning with
fractionated MEL VTD since T4-L employed 1 less cycle of induction and consolidation
treatment. This combination has also been found to be synergistic when used to treat
patients with VMP ineligible for stem cell transplantation in the VISTA study (18).
We previously reported that bortezomib and VTD could be added to fractionated
EL in doses up to 250mg/m2 in an advanced patient population with acceptable toxicity
and high response rates (7, 8). Others have also explored the use of bortezomib and
MEL as a conditioning regimen prior to transplantation and found that both agents can
be safely combined and possibly produce increased response rates (19-22). The
present paper is the first randomized study comparing single dose melphalan 200mg/m2
with a fractionated MELVTD schedule. The results of TT4 indicate that CA-type
myeloma benefits from MELVTD, whilst non-CA MM fares better with application of a
single high dose MEL 200mg/m2. Prior attempts to improve conditioning with MEL have
Research. on January 9, 2020. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on November 3, 2016; DOI: 10.1158/1078-0432.CCR-15-2620

12
not been successful and included the addition of other drugs, skeletal targeting
radioactive antibodies or radiation therapy (23-28).
Mono- or poly ubiquination of DNA-repair enzymes such H2AX, BRCA1, and
FANCD2 is required for recruitment to sites of DNA double stranded breaks and is
essential to the DNA damage response (29). Bortezomib reduces the availability of
nuclear ubiquitin and may thereby impair homologous recombination mediated DNA-
repair. It has been suggested that bortezomib renders myeloma cells more vulnerable
to alkylator-mediated DNA-damage by essentially inducing a BRCAness type state (30).
CA-type MM is likely to harbor more genomic chaos and may be more dependent on
efficient DNA-repair explaining the sensitivity to fractionated MEL-VTD conditioning.
Availability of GEP led us to examine whether CA-linked gene probes could be
identified. Indeed 51 genes were identified that distinguished no-CA from CA
subgroups. When examined for its clinical relevance, the GEP51 model was prognostic
in TT4-S so that GEP51/CA prediction was associated with inferior OS and PFS. In
contrast, such Kaplan-Meier plots were superimposable between these 2 groups in
TT4-L. Ingenuity pathway analysis suggests that CA-type MM has overexpression of
genes critical to proliferation. The ability to examine metaphase cytogenetics inherently
implies that the myeloma cells are able to survive and proliferate in vitro without the
support of the myeloma micro-environment. Increased ability to proliferate may be a
favorable evolutionary trait, but on the other hand stress requirements for DNA-repair to
prevent fatal mutations and cell death. In this context, one could speculate that
exposure to DNA-damaging alkylators such as MEL in the setting of bortezomib-
induced reduced DNA-repair could lead to fatal “mitotic catastrophes”.
Research. on January 9, 2020. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on November 3, 2016; DOI: 10.1158/1078-0432.CCR-15-2620

13
This is the first clinical trial, which suggests that tailoring the transplant
conditioning regimen to myeloma biology may further improve outcome. However, the
study was not designed to specifically study the impact of conditioning on outcome in
the context of metaphase CA. These preliminary findings therefore require confirmation
in future phase III studies.
Author Contributions
FvR, AH, JC and BB designed the research. JE, MZ, SY, ET, SW, RK, YJ, XP, MG, NP,
DS, SP, CB, MCF, FvR and BB performed the research. FvR, AM, AH, JC and BB
analyzed the data. FvR, AM, JC, BB and GM wrote the manuscript.
Research. on January 9, 2020. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on November 3, 2016; DOI: 10.1158/1078-0432.CCR-15-2620

14
References
1. Barlogie B, Tricot G, Anaissie E, Shaughnessy JD, Jr, Rasmussen E, van Rhee
F, et al. Thalidomide and hematopoietic-cell transplantation for multiple myeloma.
N Engl J Med 2006;354:1021-1030.
2. Barlogie B, Anaissie E, van Rhee F, Haessler J, Hollmig K, Pineda-Roman M, et
al. Incorporating bortezomib into upfront treatment for multiple myeloma: Early
results of Total Therapy 3. Br J Haematol 2007;138:176-185.
3. Shaughnessy JD, Jr., Zhan F, Burington BE, Huang Y, Colla S, Hanamura I, et
al. A validated gene expression model of high-risk multiple myeloma is defined
by deregulated expression of genes mapping to chromosome 1. Blood
2007;109:2276-2284.
4. Barlogie B, Mitchell A, van Rhee F, Epstein J, Morgan GJ, Crowley J. Curing
myeloma at last: Defining criteria and providing the evidence. Blood
2014;124:3043-3051.
5. Shaughnessy JD, Jr., Qu P, Usmani S, Heuck CJ, Zhang Q, Zhou Y, et al.
Pharmacogenomics of bortezomib test-dosing identifies hyperexpression of
proteasome genes, especially PSMD4, as novel high-risk feature in myeloma
treated with Total Therapy 3. Blood 2011;118:3512-3524.
6. Nair B, van Rhee F, Shaughnessy JD, Jr., Anaissie E, Szymonifka J, Hoering A,
et al. Superior results of Total Therapy 3 (2003-33) in gene expression profiling-
defined low-risk multiple myeloma confirmed in subsequent trial 2006-66 with
VRD maintenance. Blood 2010;115:4168-4173.
Research. on January 9, 2020. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on November 3, 2016; DOI: 10.1158/1078-0432.CCR-15-2620

15
7. Hollmig K, Stover J, Talamo G, Zangari M, Thertulien R, van Rhee F, et al.
Addition of bortezomib (VelcadeTM) to high dose melphalan (Vel-Mel) as an
effective conditioning regimen with autologous stem cell support in multiple
myeloma (MM). Blood 2004;104:929.
8. Pineda-Roman M, Cottler-Fox M, Hollmig K, Anaissie EJ, van Rhee F, Tricot G,
et al. Retrospective analysis of fractionated high-dose melphalan (F-Mel) and
bortezomib-thalidomide-dexamethasone (VTD) with autotransplant (AT) support
for advanced and refractory multiple myeloma (AR-MM). Blood 2006;108:3102.
9. International Myeloma Working Group. Criteria for the classification of
monoclonal gammopathies, multiple myeloma and related disorders: A report of
the International Myeloma Working Group. Br J Haematol 2003;121:749-757.
10. Durie BG, Harousseau JL, Miguel JS, Bladé J. Barlogie B, Anderson K, et al.
International uniform response criteria for multiple myeloma. Leukemia
2006;20:1467-1473.
11. van Rhee F, Giralt S, Barlogie B. The future of autologous stem cell
transplantation in myeloma. Blood 2014;124:328-333.
12. Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. J
AM Stat Assoc 1958; 53:457-481.
13. Gooley TA, Leisenring W, Crowley J, Storer BE. Estimation of failure probabilities
in the presence of competing risks: New representations of old estimators. Stat
Med 1999;18:695-706.
14. Mantel N. Evaluation of survival data and two new rank order statistics arising in
its consideration. Cancer Chemother Rep 1966;50:163-170.
Research. on January 9, 2020. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on November 3, 2016; DOI: 10.1158/1078-0432.CCR-15-2620

16
15. Cox DR. Regression models and life-tables. J R Stat Soc 1972;34:187-220.
16. Waheed S, Mitchell A, Usmani S, Epstein J, Yaccoby S, Nair B, et al. Standard
and novel imaging methods for multiple myeloma: correlates with prognostic
laboratory variables including gene expression profiling data.
Haematologica 2013;98:71-8.
17. Arzoumanian V, Hoering A, Sawyer J, van Rhee F, Bailey C, Gurley J, et al.
Suppression of abnormal karyotype predicts superior survival in multiple
myeloma. Leukemia 2008;22:850-5.
18. San Miguel JF, Schlag R, Khuageva NK, Dimopoulos MA, Shpilberg O, Kropff M,
et al. Bortezomib plus melphalan and prednisone for initial treatment of multiple
myeloma. N Engl J Med 2008;359:906-917.
19. Roussel M, Moreau P, Huynh A, Mary JY, Danho C, Caillot D, et al. Bortezomib
and high-dose melphalan as conditioning regimen before autologous stem cell
transplantation in patients with de novo multiple myeloma: A phase 2 study of the
Intergroupe Francophone du Myelome (IFM). Blood 2010;115:32-37.
20. Lonial S, Kaufman J, Tighiouart M, Nooka A, Langston AA, Heffner LT, et al. A
phase I/II trial combining high-dose melphalan and autologous transplant with
bortezomib for multiple myeloma: A dose- and schedule-finding study. Clin
Cancer Res 2010;16:5079-5086.
21. Thompson PA, Prince HM, Seymour JF, Ritchie D, Stokes K, Burbury K, et al.
Bortezomib added to high-dose melphalan as pre-transplant conditioning is safe
in patients with heavily pre-treated multiple myeloma. Bone Marrow Transplant.
2011;46:764-765.
Research. on January 9, 2020. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on November 3, 2016; DOI: 10.1158/1078-0432.CCR-15-2620

17
22. Lee SR, Kim SJ, Park Y, Sung HJ, Choi CW, Kim BS et al. Bortezomib and
melphalan as a conditioning regimen for autologous stem cell transplantation in
multiple myeloma. Korean J Hematol. 2010;45:183-187.
23. Shimoni A, Smith TL, Aleman A, Weber D, Dimopoulos M, Anderlini P, et al.
Thiotepa, busulfan, cyclophosphamide (TBC) and autologous hematopoietic
transplantation: An intensive regimen for the treatment of multiple myeloma.
Bone Marrow Transplant. 2001;27:821-828.
24. Anagnostopoulos A, Aleman A, Ayers G, Donato M, Champlin R, Weber D, et al.
Comparison of high-dose melphalan with a more intensive regimen of thiotepa,
busulfan, and cyclophosphamide for patients with multiple myeloma. Cancer
2004;100:2607-2612.
25. Christoforidou AV, Saliba RM, Williams P, Qazilbash M, Roden L, Aleman A, et
al. Results of a retrospective single institution analysis of targeted skeletal
radiotherapy with (166) holmium-DOTMP as conditioning regimen for autologous
stem cell transplant for patients with multiple myeloma. Impact on transplant
outcomes. Biol Blood Marrow Transplant 2007;13:543-549.
26. Giralt S, Bensinger W, Goodman M, Posoloff D, Eary J, Wendt R, et al. 166ho-
DOTMP plus melphalan followed by peripheral blood stem cell transplantation in
patients with multiple myeloma: Results of two phase 1/2 trials. Blood
2003;102:2684-2691.
27. Desikan KR, Tricot G, Dhodapkar M, Fassas A, Siegel D, Vesole DH, et al.
Melphalan plus total body irradiation (MEL-TBI) or cyclophosphamide (MEL-CY)
as a conditioning regimen with second autotransplant in responding patients with
Research. on January 9, 2020. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on November 3, 2016; DOI: 10.1158/1078-0432.CCR-15-2620

18
myeloma is inferior compared to historical controls receiving tandem transplants
with melphalan alone. Bone Marrow Transplant 2000;25:483-487.
28. Moreau P, Facon T, Attal M, Hulin C, Michallet M, Maloisel F, et al. Comparison
of 200 mg/m(2) melphalan and 8 Gy total body irradiation plus 140 mg/m(2)
melphalan as conditioning regimens for peripheral blood stem cell transplantation
in patients with newly diagnosed multiple myeloma: Final analysis of the
Intergroupe Francophone du Myélome 9502 randomized trial. Blood
2002;99:731-735.
29. Neri P, Ren L, Gratton K, Stebner E, Johnson J, Klimowicz A, et al. Bortezomib-
induced "BRCAness" sensitizes multiple myeloma cells to PARP inhibitors. Blood
2011;118:6368-6379.
30. Fonseca R. Innovation in myeloma treatments PARP excellence! Blood
2011;118:6234-6235.
Research. on January 9, 2020. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on November 3, 2016; DOI: 10.1158/1078-0432.CCR-15-2620

Table 1: Patient characteristics
Factor All
Patients S-TT4 L-TT4 Median Age (yr) 61.4
(N=289)(30.4 - 75.9)
60.4 (N=145)(34.2 - 75.2)
62.2 (N=144) (30.4 - 75.9)
Age >= 60yr 157/289 (54%)
74/145 (51%)
83/144 (58%)
Female 111/289 (38%)
60/145 (41%)
51/144 (35%)
IgA 46/287 (16%)
22/143 (15%)
24/144 (17%)
IgG 179/287 (62%)
93/143 (65%)
86/144 (60%)
ISS Stage 1 86/289 (30%)
44/145 (30%)
42/144 (29%)
ISS Stage 2 124/289 (43%)
61/145 (42%)
63/144 (44%)
ISS Stage 3 79/289 (27%)
40/145 (28%)
39/144 (27%)
Albumin < 3.5 g/dL
123/289 (43%)
58/145 (40%)
65/144 (45%)
B2M >= 3.5 mg/L
153/289 (53%)
77/145 (53%)
76/144 (53%)
B2M > 5.5 mg/L 79/289 (27%)
40/145 (28%)
39/144 (27%)
Creatinine >= 1.5 mg/dL
31/289 (11%)
15/145 (10%)
16/144 (11%)
Hemoglobin < 10 g/dL
109/289 (38%)
55/145 (38%)
54/144 (38%)
Baseline PET FL > 0
166/261 (64%)
82/126 (65%)
84/135 (62%)
Baseline PET FL > 3
95/261 (36%)
45/126 (36%)
50/135 (37%)
Baseline FL-SUV > 3.9
79/168 (47%)
40/84 (48%)
39/84 (46%)
Cytogenetic abnormalities
112/283 (40%)
53/142 (37%)
59/141 (42%)
amp1q21 (FISH)
63/259 (24%)
31/127 (24%)
32/132 (24%)
Research. on January 9, 2020. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on November 3, 2016; DOI: 10.1158/1078-0432.CCR-15-2620

2
Factor All
Patients S-TT4 L-TT4 delTP53 (FISH) 19/259
(7%) 11/127 (9%)
8/132 (6%)
GEP 70 High Risk
2/286 (1%)
0/143 (0%)
2/143 (1%)
GEP CD-1 subgroup
16/286 (6%)
6/143 (4%)
10/143 (7%)
GEP CD-2 subgroup
56/286 (20%)
23/143 (16%)
33/143 (23%)
GEP HY subgroup
102/286 (36%)
49/143 (34%)
53/143 (37%)
GEP LB subgroup
45/286 (16%)
25/143 (17%)
20/143 (14%)
GEP MF subgroup
8/286 (3%)
6/143 (4%)
2/143 (1%)
GEP MS subgroup
35/286 (12%)
22/143 (15%)
13/143 (9%)
GEP PR subgroup
24/286 (8%)
12/143 (8%)
12/143 (8%)
n/N (%): n- Number with factor, N- Number with valid data for factor ND: No valid observations for factor Bold print signifies Fisher’s exact test p-value < 0.05
Research. on January 9, 2020. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on November 3, 2016; DOI: 10.1158/1078-0432.CCR-15-2620

Table 2: Univariate Cox analysis of baseline features associated with overall survival (OS) and progression-free survival (PFS) across TT4 arms
Overall Survival Progression-Free
Survival
Variable n/N (%) HR (95%
CI) P-value HR (95%
CI) P-value Univariate TT4-L 144/289
(50%) 1.14
(0.71, 1.82)
0.593 1.24 (0.83, 1.85)
0.290
Age >= 65 yr 96/289 (33%)
2.27 (1.41, 3.64)
<.001 1.89 (1.26, 2.82)
0.002
Albumin < 3.5 g/dL
132/289 (46%)
1.90 (1.17, 3.08)
0.010 1.43 (0.96, 2.14)
0.077
B2M >= 3.5 mg/L
153/289 (53%)
2.40 (1.44, 4.01)
<.001 1.79 (1.18, 2.70)
0.006
B2M > 5.5 mg/L
79/289 (27%)
1.93 (1.18, 3.14)
0.009 1.88 (1.24, 2.85)
0.003
Creatinine > 1.5 mg/dL
31/289 (11%)
1.30 (0.65, 2.62)
0.461 1.70 (0.98, 2.94)
0.060
CRP >= 8 mg/L 80/288 (28%)
1.60 (0.98, 2.61)
0.058 1.56 (1.03, 2.36)
0.037
Hb < 10 g/dL 109/289 (38%)
1.42 (0.88, 2.28)
0.151 1.31 (0.87, 1.96)
0.193
Baseline PET FL > 0
166/261 (64%)
1.49 (0.86, 2.57)
0.153 1.35 (0.86, 2.12)
0.187
Baseline PET FL > 3
95/261 (36%)
2.72 (1.63, 4.52)
<.001 2.13 (1.40, 3.26)
<.001
GEP CD-1 subgroup
16/285 (6%)
0.22 (0.03, 1.57)
0.131 0.30 (0.07, 1.21)
0.090
Research. on January 9, 2020. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on November 3, 2016; DOI: 10.1158/1078-0432.CCR-15-2620

2
Overall Survival Progression-Free
Survival
Variable n/N (%) HR (95%
CI) P-value HR (95%
CI) P-value GEP CD-2
subgroup 56/285 (20%)
1.47 (0.85, 2.54)
0.171 1.49 (0.94, 2.37)
0.090
GEP HY subgroup
102/285 (36%)
0.84 (0.50, 1.39)
0.489 0.74 (0.48, 1.14)
0.175
GEP LB subgroup
44/285 (15%)
1.26 (0.69, 2.30)
0.454 1.47 (0.90, 2.40)
0.126
GEP MF subgroup
8/285 (3%)
1.13 (0.28, 4.61)
0.867 1.12 (0.35, 3.53)
0.853
GEP MS subgroup
35/285 (12%)
0.75 (0.34, 1.64)
0.470 0.69 (0.34, 1.36)
0.280
GEP PR subgroup
24/285 (8%)
1.25 (0.57, 2.72)
0.583 1.33 (0.69, 2.56)
0.393
TT4-S only
Any CA vs No CA
53/142 (37%)
1.84 (0.93, 3.64)
0.081 1.42 (0.79, 2.56)
0.244
TT4-L only
Any CA vs No CA
59/142 (42%)
0.51 (0.25, 1.07)
0.074 0.71 (0.40, 1.26)
0.248
HR- Hazard Ratio, 95% CI- 95% Confidence Interval, P-value from Wald Chi-Square Test in Cox Regression NS2- Multivariate results not statistically significant at 0.05 level. All univariate p-values reported regardless of significance. Multivariate model uses stepwise selection with entry level 0.1 and variable remains if meets the 0.05 level. A multivariate p-value greater than 0.05 indicates variable forced into model with significant variables chosen using stepwise selection.
Research. on January 9, 2020. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on November 3, 2016; DOI: 10.1158/1078-0432.CCR-15-2620

Table 3: Multivariate Cox regression analysis of baseline features associated with overall survival (OS) and progression-free survival (PFS) across TT4 arms
Overall Survival Progression-Free
Survival
Variable n/N (%) HR (95%
CI) P-value HR (95%
CI) P-value Multivariate
Age >= 65 yr 86/257 (33%)
2.01 (1.19, 3.38)
0.0086 1.76 (1.14, 2.72)
0.0110
Albumin < 3.5 g/dL
118/257 (46%)
1.90 (1.12, 3.20)
0.0167 1.46 (0.95, 2.24)
0.0838
B2M > 5.5 mg/L
67/257 (26%)
2.40 (1.35, 4.29)
0.0030 2.08 (1.30, 3.35)
0.0024
Baseline PET FL > 3
93/257 (36%)
2.94 (1.73, 5.01)
<.0001 2.24 (1.44, 3.49)
0.0003
Any CA vs No CA (TT4-L) *
58/133 (44%)
0.36 (0.16, 0.79)
0.0113 0.56 (0.30, 1.05)
0.0698
Any CA vs No CA (TT4-S) *
50/124 (40%)
1.73 (0.81, 3.71)
0.1575 1.35 (0.71, 2.56)
0.3565
HR- Hazard Ratio, 95% CI- 95% Confidence Interval, P-value from Wald Chi-Square Test in Cox Regression P-value for the CA by Treatment arm interactions, OS: p = 0.0035; PFS: p = 0.0491 * Denominators represent the total number of patients relevant to this hazard ratio rather than the total number of patients in the model.
Research. on January 9, 2020. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on November 3, 2016; DOI: 10.1158/1078-0432.CCR-15-2620

Figure Legend
Figure 1: Survival Outcomes in TT4 by arm (A: OS, B: PFS, C: CR, D: CRD)
Figure 2: Clinical outcomes according to the presence of cytogenetic abnormalities (no
CA vs CA) by TT4 arm
Figure 3: Clinical outcomes according to 51-gene model predicting CA versus no-CA
Research. on January 9, 2020. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on November 3, 2016; DOI: 10.1158/1078-0432.CCR-15-2620

Figure 1: Survival outcomes in TT4 by arm (A: OS, B: PFS, C: CR, D: CRD)
A
B
C
D
Overall Survival: UARK 2008-01Randomized Patients Only
By Treatment Arm
0%
20%
40%
60%
80%
100%
0 1 2 3 4 5 6Years from Registration
S-TT4L-TT4
Events / N33 / 14536 / 144
2-YearEstimate
90% (85, 95)87% (81, 92)
Logrank P-value = .59
Progression-Free Survival: UARK 2008-01Randomized Patients Only
By Treatment Arm
0%
20%
40%
60%
80%
100%
0 1 2 3 4 5 6Years from Registration
S-TT4L-TT4
Events / N45 / 14552 / 144
2-YearEstimate
84% (78, 90)79% (72, 85)
Logrank P-value = .29
Time to Complete Response: UARK 2008-01Randomized Patients Only
By Treatment Arm
0%
20%
40%
60%
80%
100%
0 1 2 3 4 5 6Years from Registration
S-TT4L-TT4
Events / N90 / 14292 / 140
2-YearEstimate58.5%60.7%
P = .20
CR Duration: UARK 2008-01Randomized Patients Only
By Treatment Arm
0%
20%
40%
60%
80%
100%
0 1 2 3 4 5 6Years from CR
S-TT4L-TT4
Events / N14 / 9026 / 92
2-YearEstimate
87% (80, 94)81% (73, 89)
Logrank P-value = .05
Research. on January 9, 2020. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on November 3, 2016; DOI: 10.1158/1078-0432.CCR-15-2620

S-TT4 L-TT4
A
B
C
D
Overall Survival: UARK 2008-01Patients Randomized to S-TT4
By Presence of Cytogenetic Abnormalities
0%
20%
40%
60%
80%
100%
0 1 2 3 4 5 6Years from Registration
No CAAny CA
Events / N16 / 8917 / 53
2-YearEstimate
94% (89, 100)83% (72, 94)
Logrank P-value = .08
Overall Survival: UARK 2008-01Patients Randomized to L-TT4
By Presence of Cytogenetic Abnormalities
0%
20%
40%
60%
80%
100%
0 1 2 3 4 5 6Years from Registration
No CAAny CA
Events / N26 / 8310 / 59
2-YearEstimate
81% (72, 89)95% (89, 100)
Logrank P-value = .07
Progression-Free Survival: UARK 2008-01Patients Randomized to S-TT4
By Presence of Cytogenetic Abnormalities
0%
20%
40%
60%
80%
100%
0 1 2 3 4 5 6Years from Registration
No CAAny CA
Events / N25 / 8920 / 53
2-YearEstimate
88% (81, 95)77% (66, 89)
Logrank P-value = .24
Progression-Free Survival: UARK 2008-01Patients Randomized to L-TT4
By Presence of Cytogenetic Abnormalities
0%
20%
40%
60%
80%
100%
0 1 2 3 4 5 6Years from Registration
No CAAny CA
Events / N34 / 8318 / 59
2-YearEstimate
72% (63, 82)86% (77, 96)
Logrank P-value = .26
Figure 2: Clinical outcomes according to the presence of cytogenetic abnormalities (no CA vs CA) by
TT4 arm
Research. on January 9, 2020. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on November 3, 2016; DOI: 10.1158/1078-0432.CCR-15-2620

E
F
G
H
CR Duration: UARK 2008-01Patients Randomized to S-TT4
By Presence of Cytogenetic Abnormalities
0%
20%
40%
60%
80%
100%
0 1 2 3 4 5 6Years from CR
No CAAny CA
Events / N6 / 528 / 35
2-YearEstimate
92% (85, 100)79% (65, 93)
Logrank P-value = .13
CR Duration: UARK 2008-01Patients Randomized to L-TT4
By Presence of Cytogenetic Abnormalities
0%
20%
40%
60%
80%
100%
0 1 2 3 4 5 6Years from CR
No CAAny CA
Events / N16 / 5110 / 39
2-YearEstimate
76% (65, 88)87% (76, 98)
Logrank P-value = .54
Time to Relapse from CR: UARK 2008-01Patients Randomized to S-TT4
By Presence of Cytogenetic Abnormalities
0%
20%
40%
60%
80%
100%
0 1 2 3 4 5 6Years from CR Onset
No CAAny CA
Events / N2 / 526 / 35
2-YearEstimate
3.9%15.4%
P = .03
Time to Relapse from CR: UARK 2008-01Patients Randomized to L-TT4
By Presence of Cytogenetic Abnormalities
0%
20%
40%
60%
80%
100%
0 1 2 3 4 5 6Years from CR Onset
No CAAny CA
Events / N10 / 517 / 39
2-YearEstimate15.8%7.9%
P = .79
Research. on January 9, 2020. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on November 3, 2016; DOI: 10.1158/1078-0432.CCR-15-2620

A B
C
D
O v e r a l l S u r v i v a l f o r P a t i e n t s w i t h G E P D a t a A v a i l a b l e i n T T 4B y P r e d i c t e d C A f o r A r m A : S - T T 3
0 %
2 0 %
4 0 %
6 0 %
8 0 %
1 0 0 %
0 2 4 6 8Y e a r s
P r e d i c t e d N o C AP r e d i c t e d a n y C A
D e a t h s / N1 6 / 9 71 7 / 4 3
3 - Y e a rE s t i m a t e
9 2 % ( 8 6 , 9 7 )7 4 % ( 5 9 , 8 8 )
L o g r a n k P - v a l u e = . 0 0 2
O v e r a l l S u r v i v a l f o r P a t i e n t s w i t h G E P D a t a A v a i l a b l e i n T T 4B y P r e d i c t e d C A f o r A r m B : L - T T 3
0 %
2 0 %
4 0 %
6 0 %
8 0 %
1 0 0 %
0 2 4 6 8Y e a r s
P r e d i c t e d N o C AP r e d i c t e d a n y C A
D e a t h s / N2 2 / 8 31 4 / 5 7
3 - Y e a rE s t i m a t e
7 9 % ( 7 1 , 8 8 )8 4 % ( 7 4 , 9 4 )
L o g r a n k P - v a l u e = . 6 3
P r o g r e s s i o n F r e e S u r v i v a l f o r P a t i e n t s w i t h G E P D a t a A v a i l a b l e i n T T 4B y P r e d i c t e d C A f o r A r m B : L - T T 3
0 %
2 0 %
4 0 %
6 0 %
8 0 %
1 0 0 %
0 2 4 6 8Y e a r s
P r e d i c t e d N o C AP r e d i c t e d a n y C A
E v e n t s / N3 1 / 8 32 1 / 5 7
3 - Y e a rE s t i m a t e
7 1 % ( 6 1 , 8 1 )7 7 % ( 6 6 , 8 8 )
L o g r a n k P - v a l u e = . 7 9
P r o g r e s s i o n F r e e S u r v i v a l f o r P a t i e n t s w i t h G E P D a t a A v a i l a b l e i n T T 4B y P r e d i c t e d C A f o r A r m A : S - T T 3
0 %
2 0 %
4 0 %
6 0 %
8 0 %
1 0 0 %
0 2 4 6 8Y e a r s
P r e d i c t e d N o C AP r e d i c t e d a n y C A
E v e n t s / N2 3 / 9 72 1 / 4 3
3 - Y e a rE s t i m a t e
8 3 % ( 7 6 , 9 1 )6 5 % ( 4 9 , 8 0 )
L o g r a n k P - v a l u e = . 0 0 2
Figure 3: Clinical outcomes according to 51-gene model predicting CA versus no-
CA
Research. on January 9, 2020. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on November 3, 2016; DOI: 10.1158/1078-0432.CCR-15-2620

Published OnlineFirst November 3, 2016.Clin Cancer Res Yogesh Jethava, Alan Mitchell, Joshua Epstein, et al. transplantsbortezomib and thalidomide to fractionated melphalan Adverse metaphase cytogenetics can be overcome by adding
Updated version
10.1158/1078-0432.CCR-15-2620doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2016/11/03/1078-0432.CCR-15-2620.DC1
Access the most recent supplemental material at:
Manuscript
Authoredited. Author manuscripts have been peer reviewed and accepted for publication but have not yet been
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/early/2016/11/03/1078-0432.CCR-15-2620To request permission to re-use all or part of this article, use this link
Research. on January 9, 2020. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on November 3, 2016; DOI: 10.1158/1078-0432.CCR-15-2620