Embed Size (px)
Citation preview

PDFlib PLOP: PDF Linearization, Optimization, Protection
Page inserted by evaluation versionwww.pdflib.com – [email protected]

DOI: 10.1111/j.1610-0387.2007.06435.x Case Reports 379
© The Authors • Journal compilation © Blackwell Verlag, Berlin • JDDG • 1610-0379/2008/0605-0379 JDDG | 5˙2008 (Band 6)
SummaryIn the wake of expanding internation-al tourism, rickettsioses are increas-ingly observed also in central Europe.African tick bite fever is a recentlydescribed, acute febrile illness withcharacteristic skin lesions. It is causedby Rickettsia africae, which is transmit-ted to humans by ticks of theAmblyomma genus. A 60-year-oldwoman presented with a papulovesic-ular exanthem, fever, and headacheafter returning from South Africa. Apurple nodule with central necrosis(“tache noire” or ”inoculation eschar”)was noticed on the lower leg.Antibodies against rickettsia of thespotted fever group were detectedserologically. Oral doxycycline led toclearance of the disease after fewdays of treatment.
KeywordsRickettsiosis – Rickettsia – tick bitefever – tache noire – eschar – tropicaldermatosis
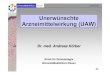
Clinical presentationThe patient presented at the Departmentof Dermatology with a generalized maculopapular and vesicular exanthem(Figure 1a). On the left lower leg therewas a tender purple nodule with centralulceration, a “tache noire” or “inocula-tion eschar” (Figure 1b). The inguinallymph nodes on both sides were swollen. Results of heart, lung, abdomi-nal, and neurological examinations werenormal.
DiagnosisLaboratory tests: Mild elevation of �-GTat 43 U/l and LDH at 279 U/l; all otherroutine parameters were normal.Serology: Titer of Rickettsia conorii anti-bodies (known cross-reactivity of the an-tiserum with other rickettsia of the spot-ted fever group [6]) was initiallyunremarkable (normal range < 1: 40),but after 7 days was positive (1: 320).There was no evidence of borreliosis, bru-cellosis or Coxiella infection. Only a pre-vious chlamydia infection was detected.Cytology of peripheral blood specimen: Nodetection of plasmodia.Virology: No evidence of recent infec-tion with HBV, HIV, CMV, EBV, HSV,VZV, or Dengue viruses.Histology: Marked edema was noted inthe papillary layer of the dermis. In theupper and deep dermis a perivascularand interstitial inflammatory infiltratewith mononuclear cells and eosinophils(Figure 2a) was found. Vasculiticchanges with fibrinoid thickening of thevessel walls were seen around cut capil-laries and venules (Figure 2b).Other test results: ECG, chest X-ray andabdominal ultrasound were normal.
Therapy and courseA diagnosed of African tick bite fever wasbased on patient history and clinicalpresentation, in particular the typical ex-anthema with vesicular skin changes andtache noir. Diagnosis was confirmed oneweek later by serological detection of an-tibodies against rickettsia of the spottedfever group. A 9-day regimen of oraldoxycycline (200 mg/day) was begun.The fever quickly subsided and did notreturn. Topical treatment consisted ofVioform lotion.
DiscussionAfrican tick bite fever is one of the mostcommon causes of febrile illness among
IntroductionRickettsia are small, Gram-negative, coc-cobacillus bacteria, which similarly toviruses, only multiply in living cells. Thereservoir for rickettsia are arthropodssuch as ticks, fleas, lice, and mites. Trans-mission occurs through the feces of thesevectors to the skin and mucous mem-branes of humans [1, 2]. Systemic vas-culitis results from involvement of theendothelial cells of small blood vessels.Current classification divides rick-ettsioses that are pathogenic to humansinto three groups: typhus fevers, spottedfever group, and scrub typhus fevers(Table 1) [3]. In the present case report,the diseases of the spotted fever group arediscussed in more detail. These includeRocky Mountain spotted fever, causedby Rickettsia rickettsii; Mediterraneanspotted fever, caused by Rickettsiaconorii; and African tick bite fever, whichis caused by Rickettsia africae [4–6].
Case reportPatient historyA 60-year-old woman first noticed a purplenodule on her lower left leg three daysbefore returning home from a three-week trip through South Africa. Thenext day she developed a fever of 38.8 °Cand chills. At the same time, a general-ized non-pruritic rash appeared. She alsohad a headache for several days. The pa-tient had no recollection of a tick biteand had taken continual malaria prophy-laxis. Six days after the onset of symptoms,she was admitted to the Department of Infectious Diseases at the University Hospital of Cologne in Germany.
African tick bite fever –
Papulovesicular exanthem with
fever after staying in South Africa
Jan Schuster1, Iliana Tantcheva-Poor1,Claudia Wickenhauser2,Jens-MarcusChemnitz3,Nicolas Hunzelmann1,Thomas Krieg1,Karin Hartmann1
(1) Department of Dermatology, University of Cologne, Germany(2) Institute of Pathology, University of Cologne, Germany(3) Clinic I for Internal Medicine, University of Cologne, Germany
JDDG; 2008 • 6:379–382 Submitted: 13. 4. 2007| Accepted: 17. 4. 2007

travelers to Africa [5, 6]. The disease wasfirst described in 1934 by Pijper in SouthAfrica, although the pathogen Rickettsiaafricae was not identified until 1992 byKelly [4, 7]. Rickettsia africae is transmit-ted to humans by cattle ticks of the Am-blyomma genus (especially Amblyommavariegatum and Amblyomma hebraeum).This is an aggressive tick species. Unlikeother ticks it does not wait passively un-til a potential host comes its way, but in-stead actively seeks one. This explainswhy African tick bite fever often occursin clusters [5]. Rickettsia africae is foundmainly in rural regions of African coun-tries south of the Sahara and in Guade-loupe. In these countries the seropreva-lence of antibodies against rickettsia isvery high (up to 70 %) [2, 3].For decades the name “African tick bitefever” was used synonymously withMediterranean spotted fever (Table 1)[4]. Indeed, it is difficult to distinguishbetween the two. Both occur in Africa,and have a marked antibody cross reac-tivity. Often, skin changes are the decid-ing factor in differential diagnosis. InAfrican tick bite fever, there are usuallyone or more taches noires at tick bitesites. Multiple taches noires are consid-ered a pathognomonic sign of Africantick bite fever. Up to 50 % of patientshave a generalized exanthem. UnlikeMediterranean or Rocky Mountain spot-ted fever, the rash may be vesicular ratherthan only maculopapular, as was also thecase in our patient. Another factor dis-tinguishing African tick bite fever fromRocky Mountain spotted fever is that pa-tients almost never have hemorrhage orpetechia. African tick bite fever is oftenaccompanied by local lymphadenopathy.
380 Case Reports African tick bite fever
JDDG | 5˙2008 (Band 6)
Figure 1: Characteristic papulovesicular exanthem (a) and inoculation eschar (b; lower left leg, proximal lateral) in a patient with African tick bite fever.
Figure 2: Histologic examination shows perivascular and interstitial infiltrates with mononuclearcells and eosinophils (a), and fibrinoid swelling of vessel walls (b).

Other generalized symptoms includefever, headache, fatigue, flu-like symp-toms, myalgia, and neck stiffness. As yetthere are no reports of severe complica-tions or related deaths. The incubationperiod is 5–7 days [4–6].A presumptive clinical diagnosis of rick-ettsiosis can be confirmed serologically.Serologic testing uses antiserum againstRickettsia conorii antibodies, which alsoexhibits cross-reactivity with other rick-ettsia of the spotted fever group [6]. It isimportant to recall that the increase inthe antibody titer in rickettsiosis is typi-cally delayed, often not rising until after3 weeks. Similarly, in our patient, serol-ogy was initially negative and was notpositive until the end of the second weekof illness. Along with serologic studies,immunohistochemistry, PCR, and cul-tures can be used for further pathogenidentification [8, 9].Differential diagnosis includes all febrileillnesses with exanthema and headache.These include measles, influenza, viralmeningoencephalitis, infectious mononu-cleosis, recent HIV infection, recurrentfever, abdominal typhus, and malaria.The treatment of choice is i.v. or oraldoxycycline (2 x 100 mg/die) for at least7 days [6]. Alternatively, for instanceduring pregnancy, chloramphenicol (4 x500 mg/daily) can be administered [1].In the literature there are also reports ofsuccessful treatment of rickettsiosis with
ciprofloxacin (2 x 750 mg/daily), and inchildren with clarithromycin andazithromycin [10]. Preventive measuresinclude wearing protective clothing andshoes as well as avoiding contact with an-imals and regularly checking the bodyfor ticks. Insect repellents can provideadded protection [6]. Currently, there isno vaccination available [1]. <<<
Conflict of interestNone.
Correspondence toPriv.-Doz. Dr. Karin HartmannKlinik und Poliklinik für Dermatologieund VenerologieUniversität zu KölnJoseph-Stelzmann-Straße 9D-50931 KölnTel.: +49-22 1-47 8-45 00Fax: +49-22 1-47 8-45 38E-mail: [email protected]
References1 Jensenius M, Fournier PE, Raoult D.
Rickettsioses and the international tra-veler. Clin Infect Dis 2004; 39: 1493–1499.
2 Bassetti S. Rickettsiosen der Zeckenbissfie-ber-Gruppe. Internist 2004; 45: 669–675.
3 Parola P, Paddock CD, Raoult D. Tick-borne rickettsioses around the world:
emerging diseases challenging old con-cepts. Clin Microbiol Rev 2005; 18:719–756.
4 Kelly P, Matthewman L, Beati L, Ra-oult D, Mason P, Dreary M, MakombeR. African tick bite fever: a new spottedfever group rickettsiosis under an oldname. Lancet 1992; 340: 982–983.
5 Raoult D, Fournier PE, Fenollar F.Rickettsia africae, a tick-borne patho-gen in travelers to sub-Saharan Africa.N Engl J Med 2001; 344: 1504–1510.
6 Jensenius M, Fournier PE, Kelly P, My-rvang B, Raoult D. African tick bite fe-ver. Lancet Infect Dis 2003; 3: 557–564.
7 Pijper A. Tick-bite fever: a clinical lec-ture. S Afr Med J 1934; 8: 551–556.
8 Stenos J, Graves SR, Unsworth NB. Ahighly sensitive and specific real-timePCR assay for the detection of spottedfever and typhus group Rickettsiae. Am J Trop Med Hyg 2005; 73: 1083–1085.
9 Owen CE, Bahrami S, Malone JC, Cal-len JP, Kulp-Shorten CL. African tickbite fever. A not-so-uncommon illnessin international travelers. Arch Derma-tol 2006; 142: 1312–1314.
10 Cascio A, Colomba C, Antinori S, Pa-terson DL, Titone L. Clarithromycinversus azithromycin in the treatment ofMediterranean spotted fever in child-ren: a randomized controlled trial. ClinInfect Dis; 34: 154–158.
African tick bite fever Case Reports 381
JDDG | 5˙2008 (Band 6)
Table 1: The most common rickettsioses.
Disease Pathogen Region Vector
Spotted fever group
Rocky Mountain spotted fever R. rickettsii North, Central, and South America Ticks
Mediterranean spotted fever R. conoriiMediterranean countries, Africa, India,Black Sea region
Ticks
African tick bite fever R. africae Africa south of the Sahara, Guadeloupe Ticks
Rickettsialpox R. akari USA, former USSR, Korea, Africa Ticks
Queensland tick typhus R. australis Australia Mites
North Asian tick typhus R. sibiricaSiberia, Mongolia, Pakistan, northern China
Ticks
Typhus fever group
Epidemic typhus R. prowazekii Central and South America, Africa, Asia Lice
Murine typhus R. typhi Worldwide Fleas
Scrub typhus group
Japanese tick fever Orienta tsutsugamushi Asia, South Pacific, Australia Mites