View
244
Download
7
Embed Size (px)
DESCRIPTION
In this issue Dr Ward Dean describes Acarbose, plus articles on the forgotten role of the Thymus, how to beat the flu season and Pyridoxamine.
Citation preview
No 2, 2015US $8.00/ EU 6.00/ GB 5.00 where sold
The in-house magazine for International Antiaging Society Group Private Club Members
SPECIAL OFFERS ON ALL
FEATURED PRODUCTS
An anti-diabetic, weight loss agent
Dr Ward Dean describes Acarbose
The almost forgotten role of the thymus
Beating the flu season
Pyridoxamine - a universal agent against aging
PLUS:
*Restrictions may apply in some countries. All information is educational and does not replace your physicians advice and is subject to IAS terms and conditions which may change without notice.
TRH stands for thyrotropin releasing hormone, however TRH has a far wider role than just supporting the thyroid.
According to Dr. Walter Pierpaoli, TRH is a fundamental life-giving molecule that
boosts immunity, helps to reverse aging (by improving numerous lipid ratios)
and through this action appears to help induce signifi cant weight loss within
a few months.
A life generating moleculeTRH
TRH Abaris 20 Sublingual Tabs $209.99Dr. Walter Pierpaoli
3Dr. Dean knows all about the negative aspects of Syndrome X because he was instrumental, along with Professor Vladimir Dilman, in bringing to the attention of the world - the neuroendocrine theory of aging - on which it is based. It would seem that diabetic effects and weight gain go hand in hand, so you may find Dr. Deans detailed article about the starch blocking effects of acarbose of interest on a number of levels.
Furthermore, you will see that nutritionist, Karen Kaufman also highlights the benefits of the rare form of vitamin B6 and how it too helps to control weight, diabetes and ergo the deleterious aspects of aging.
Im also delighted to have interviewed Richard Stead, the inventor of 1st Line to find how this bioidentical agent is helping to battle viruses. I also hope that you may find my own contribution regarding the thymus gland of some interest.
Lastly, you may notice that there are other changes to the layout of the magazine. We are now offering more information on specific products and ailments. Its all designed to inform you better, so that your optimal health-span can be maintained for as long as possible.
Phil Micans, MS, PharmB Editor, Aging Matters Magazine
WELCOME Phil says thanks for finding the time 3
FOREFRONT This months news 4
AN ANTI-DIABETIC AND WEIGHT LOSS AGENT Dr Dean describes acarbose 6
THE ALMOST FORGOTTEN THYMUS GLAND What role does it play? 12
BEATING VIRUSES NATURALLY An interview about 1st Line 17
PYRIDOXAMINE, A UNIVERSAL ANTIAGING SUPPLEMENT The benefits of the rare form of B6 21
FEATURED PRODUCTS Best sellers and new items 24
A-Z PRODUCT LISTING AND PRICES Find everything in-stock here 33
CROSS-REFERENCE LISTS Find what you need here 40
TESTIMONIALS & EXPLANATIONS Nice comments from nice people 50
CONTACT DETAILS Get in touch with IAS today 51
Declaration: The IAS Aging Matters magazine is intended for IAS private club members (and therefore is not intended for the public). It focuses on the latest international nutritional, hormonal and drug therapies to help combat the signs of aging. These signs include the physical, mental and internal changes consisting of the diseases and disorders such as cancer, arthritis and senile demen-tias etc. However, the main focus is upon the prevention of such aging diseases and disorders for the healthy-aging individual.
Copyright 2015: All copyrights are acknowledged. Whilst every effort has been made to ensure accuracy, no responsibility can be accepted for illustrations, photographs, artwork or advertising ma-terials while in transmission or with the publisher or their agents.
Disclaimer: All educational information is offered under IAS terms and conditions. This information does not replace the ad-vice of your physician and restrictions may apply in some coun-tries. The opinions expressed by the writers may not be those of IAS or the magazine. All prices shown are in US Dollars and are for reference purposes only and they do not include taxes (where applicable), nor do they include shipping & handling fees. Prices, conditions and terms are subject to change without notice.
WELCOME
TOMORROWS TREATMENTS TODAY
IAS is dedicated to helping you access the worlds latest commercially available supplements- to give you and your family real choices in health and wellness. IAS promises you:
Quality: We stock the best quality products because the right materials and formulas give you the best possible results.
Brands: We carry original brands - i.e. the same ones used by top health professionals.
Choice: We have the largest range of medicines, hormones and supplements. If you are looking for things that use words like bioidentical, efficacy and synergy then youve come to the right place.
Pricing: Our prices are competitive and we regularly have special offers to help you save money on the things that are important to you and your family.
Support: Our friendly and professional customer care team are on-hand to help you. We can be bothered!
Professional: We work alongside the leaders in the field and we review the latest research to ensure that everything is up-to-date. After all, if we are informed then so are you.
Sponsorship: All over the world you will find IAS supporting, sponsoring, exhibiting and lecturing at key venues. You can meet us in person and see what we believe in.
INDEX
Ward Dean M.D., Medical Director
THE THINGS YOU NEED TO KNOW FROM THIS MONTHS NEWS
FOREFRONT
4 www.antiaging-systems.com Order hotline: 1-866-800-4677 e-mail: [email protected]
FatuousA recent re-examining of previous studies on saturated fat by academics at the University of Cambridge has concluded there is no link between eating foods such as fatty meat, cream or butter and developing heart disease. This overturns nearly half a century of mainstream dietary advice and now firmly points the finger at consuming carbs and sugar as the main culprits in the worldwide spread of diabetes and heart disease.
The researchers are calling for guidelines to be changed to reflect the growing body
of evidence to support their findings.
Lead researcher Dr Rajiv Chowdhury, said: These are interesting results that potentially stimulate new lines of scientific inquiry and
encourage careful reappraisal of our current nutritional guidelines.
Cardiovascular disease, in which the principal manifestation is coronary heart disease, remains the single leading cause of death and disability worldwide. In 2008, more than 17 million people died from a cardiovascular cause globally.
With so many affected by this illness, it is critical to have appropriate prevention guidelines which are informed by the best available scientific evidence.
The team conducted a meta-analysis of data from
72 studies involving more than 600,000 participants from 18 countries.
One of the key findings
was that total saturated fat, whether measured in the diet or the bloodstream, showed no association with heart disease.
Associate medical director at the British Heart Foundation Professor Jeremy Pearson, - which co-funded the study, said: This analysis of existing data suggests
there isnt enough evidence to say that a diet rich in polyunsaturated fats but low in saturated fats reduces the risk of cardiovascular disease.
But large scale clinical studies are needed, as these researchers recommend, before making a conclusive judgement.
Alongside taking any necessary medication, the best way to stay heart healthy is to stop smoking, stay active, and ensure our whole diet is healthy -
and this means considering not only the fats in our diet but also our intake of salt, sugar and fruit and vegetables.
FOREFRONT
55www.antiaging-systems.com Order hotline: 1-866-800-4677 e-mail: [email protected]
Eight year old girl suggests a possible cure for cancerCamilla Lisanti from Manchester in the UK may have provided her research scientist parents with a viable new direction in for their search for a cure to cancer.Over dinner one night her father Professor Micheal Lisanti asked her how she would go about curing cancer. The eight-year-old child thought for a moment and then suggested using antibiotics, like when I have a sore throat, to her sceptical
parents.Professor Lisanti and
his wife Federica Sotgia, a husband and wife cancer
research team, tested her theory at their lab at Manchester university and were stunned when their research revealed that four common antibiotics, which can cost as little as six Pence
a day compared to some of the latest drugs which can cost hundreds of Pounds, killed these stem cells in samples from breast, prostate, lung, ovarian, pancreatic,
skin and brain tumours.The antibiotics tested stop
the cancer cells from making mitochondria, which supply them with energy. Crucially, the antibiotics did not harm healthy cells.
Coffee consumption may lower risk of AlzheimersDrinking 3-5 cups of coffee per day may help to lower the risk of Alzheimers Disease by up to 20%, according to research highlighted in an Alzheimer Europe session report published by the Institute for Scientific Information on Coffee (ISIC), a not-for-profit organisation devoted to the study and disclosure of science related to coffee and health.
The report explores the
compounds within coffee, which may be responsible for this protective effect, identifying caffeine and polyphenols as key candidates. Caffeine helps prevent the formation of amyloid plaques and neurofibrulary
tangles in the brain - two hallmarks of Alzheimers
Disease. In addition to this, both caffeine
and polyphenols reduce inflammation and decrease the
deterioration of brain cells - especially in the hippocampus and cortex, areas of the brain
involved in memory.Dr. Iva Holmerova, vice
chairperson of Alzheimer Europe, commented: The findings presented in this
report are very encouraging and help to develop our understanding of the role
nutrition can play in protecting against Alzheimers Disease. Coffee is a very popular beverage enjoyed by millions of people around the world and Im pleased to know that moderate, lifelong consumption can have a beneficial effect on the
development of Alzheimers Disease.
Acarbose:An anti-diabetic and potential weight loss agentAcarbose (Glucobay, Pre-cose) is a drug approved for use in (1) insulin-dependent diabetes mellitus (Type I), (2) adult-onset diabetes mellitus (AODM, or Type II), and (3) those who suffer from im-paired glucose tolerance. As Ive previously pointed out, virtually everyone over the age of 35 is probably func-tionally glucose intolerant to some degree (Fig. 1). Using even the strictest orthodox criteria, it is estimated that up to 20% of Caucasians between the ages of 65 and 75 years have Type II Diabetes-and an additional 23% have im-paired glucose tolerance (2).
To understand how acar-
bose works, a review of a few basics of carbohydrate metab-olism is in order. Starches and complex sugars are broken down in the digestive tract into simple sugars, which are then absorbed by the body (in the lower small intestine and colon). These simple sugars are used for energy, or stored (as glycogen or fat).
Enzymes are essential to break down the complex carbohydrates into sugars. Certain groups of enzymes are critical to the final steps in the digestion of carbohy-drates. One of these groups is the alpha-glucosidases. Alpha glucosidases enhance the breakdown of maltose,
isomaltose, glucoamylose and sucrose (table sugar). Acar-bose acts as a potent compet-itive inhibitor of intestinal brush border alpha glucosi-dases that are essential for the breakdown of starches, dex-trins, maltose, and sucrose to absorbable monosaccharides (Fig. 2). Because of its speci-ficity for alpha glucosidases, beta glucosidases such as lactases are not affected by acarbose. Glucose is also not affected by acarbose. Conse-quently, glucose and lactose are absorbed normally when
acarbose is taken.
Effects of AcarboseAcarbose delays carbohydrate digestion and absorption (Fig. 3). Consequently, it delays and flattens post-meal rises in glucose and insulin (5, 6) (Fig. 4). Fasting and post-meal triglyceride levels are decreased (7,8) (probably due to the reduced insulin response) (3), and reductions in low-density lipoproteins (LDL)
By Ward Dean, M.D.
6 www.antiaging-systems.com Order hotline: 1-866-800-4677 e-mail: [email protected]
71-80120110100
908070605040302010
U/ml
Insu
lin
Minutes
51-60
0 60 120 180
41-5031-4021-30
11-204-10
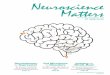
Figure 1. Progressive loss of glucose tolerance with age. This illustrates how the rise in insulin following a glucose tolerance test progressively increases with age, and takes longer to return to baseline. Only those ten years of age and younger have normal (optimal) glucose tolerance the rest of us suffer from what Dilman called pre-diabetes (1).
Figure 2. Simplified representation of alpha glucosidase inhibition. The bold blocks indicate the points at which acarbose delays the production of monosac-charides and, as a consequence, their intestinal absorption (3).
Acarbose Sites of Action
Starch Lumen Sucrose
Sucrase
GlucoseGlucoseFructose
a-amylase
MaltoseMaltotrioseDextrinsMaltose
IsomaltaseGlucoamylase
Sites of competitive inhibition
and increases in high-density lipoproteins (HDL) have been reported (9). Glycosylated haemoglobin (hemoglobin A1c [HbA1c]) is a screening and diagnostic test for diabetes, as well as a biomarker of aging (in-dicator of biological age). HbA1c tends to increase progressively with age in non-diabetic subjects (Fig. 5) (10). Acarbose has been demonstrated in numerous studies to significantly reduce HbA1c (3, 11, 12) (Fig. 6). The reduction in HbA1c has a number of other beneficial
effects, including decreased glycation of glomerular base-ment membranes, decreased advanced glycosylation end product (AGE) formation in connective tissue, decreased cataract formation, and prevention of neuropathy and retinopathy (13).
In addition, of particular significance with respect to the mechanism of ag-ing proposed by Dilmans neuroendocrine theory of aging, Balfour and McTavish (14) speculated that Acar-bose might improve insulin sensitivity (as indicated by
decreasing fasting blood glu-cose). Chiasson, et al (5) also believed Acarbose improved insulin sensitivity, based on their finding that patients taking acarbose experienced an upward trend in post-meal C-peptide levels. Further-more, acarbose appears to prevent or delay the progres-sive deterioration in pancre-atic beta cells that routinely occurs in patients with Type 2 DM (2).
Other benefits of alpha glucosidase inhibitors are their ability to prevent or at-tenuate diabetic nephropathic lesions (15), and one study even reported an improve-ment in cognitive function in both animals and elderly
patients given Acarbose (16). Because acarbose does not result in hypoglycemia, it can be safely used by those who suffer from reactive hypo-glycemiaand will probably benefit the condition due to its insulin-modulating properties.
In 2003, results from the STOP-NIDDM trial were reported (17). The trial was an international, multicentre double blind trial involv-
ing patients from Canada, Germany, Austria, Norway, Denmark, Sweden, Fin-land, Israel and Spain, from 1998-2001, involving nearly 1,500 patients with impaired glucose tolerance (IGT). The patients were randomized
A. Diet
Time (months) Time (months)
B. Sulfonylurea
D. InsulinC. Metformin
1.5
-1.5
0.5
-0.5
1
0
-1
0 3 6 9 12
1.5
-1.5
0.5
-0.5
1
0
-1
0 3 6 9 12
1.5
-1.5
0.5
-0.5
1
0
-1
0 3 6 9 12
1.5
-1.5
0.5
-0.5
1
0
-1
0 3 6 9 12
#
7www.antiaging-systems.com Order hotline: 1-866-800-4677 e-mail: [email protected]
Figure 3. Acarbose is poorly absorbed, and is excreted predominately in the feces. This illustrates how Acarbose acts non-systemically to delay carbohydrate absorption (4).
Figure 4. Effect of Acarbose vs placebo on post-prandial (after a meal) levels of glucose and insulin in diabetics treated with a sulfonylurea (6).
Figure 5. Age-related rise of HbA1c, indicating loss of glucose tolerance with increasing age (10).
Figure 6. Effect of Acarbose and placebo on HbA1c in diabetic patients treated with diet alone and diet + metformin, sulfonylurea or insulin (as indicated). The circle indicates placebo, and the square indicates the effects of acarbose (titrated to maximum 600 mg/day) added to each regimen for 12 months (5).
Without Acarbose With Acarbose
Upper small intestine
Carbohydrate resorption
Carbohydrates
Lower small intestine
Upper small intestine
Lower small intestine
Effects of Acarbose on Glucose and Insulin after a Meal
Glucose Increase Insulin Increase
% a
bove
bas
elin
e
Time (min)
100
80
60
40
20
0-30 0 30 60 90 120 150 180
Without acarbose (baseline FPG 160 mg/dL)Single-does acarbose (baseline FPG 158 mg/dL)
FPG = fasting plasma glucose
Reprinted with permission from Kado S et al. Diabetes Clin Pract. 1998;41:49-55. Copyright 1998 Elsevier. All rights reserved.
Meal
% a
bove
bas
elin
e
400
300
200
100
0-30 0 30 60 90 120 150 180
Meal
Age vs HbA1c
n=109
y=4.7+0.011x R2=0.18
AGE
% H
bA1c
6
7
5
4
00 10 20 30 40 50 60 70 80 90 100
to receive placebo or 100 mg Acarbose, three times daily. The scientists wanted to evaluate whether Acar-bose could prevent coronary artery disease, hypertension, congestive heart failure, or peripheral vascular disease.
The results of the study were dramatic. During the slightly more than three years of the study, 19 subjects taking placebo suffered heart attacks, compared to only 2 in the group taking Acarbose (Fig. 7). Acarbose treatment also had a significant effect on the risk of developing hyper-tension. Of 682 patients in the Acarbose group, only 78 developed hypertension (11%) vs 115 (17%) of those (682)
in the placebo group (Fig. 8). The authors added that Acar-bose treatment was associated with a significant reduction in body weight, BMI (Body
Mass Index), waist circumfer-ence, blood pressure, 2-hour glucose concentrations, and triglyceride levels. They concluded that Acarbose treatment was associated with a significant reduction in the incidence of cardiovascular disease and hypertension.
In 2011, scientists present-ed a comprehensive schemat-ic to connect the plethora of benefits that have been attributed to this remarkable medication (Fig. 9)
Acarbose for Weight LossAnimal studies with acarbose have consistently shown that Acarbose has a body fat-low-ering action. Balfour and McTavish (14) reported that Acarbose caused a dose-de-pendent reduction in body weight gain of genetically obese and hyperinsulinemic rats. In higher doses, acar-bose even caused a dramatic loss in weight (Fig 10).
Many studies have re-ported a beneficial effect of alpha glucosidase inhibitors on bodyweight in humans (9, 11, 20-22), although the effect was usually reported as moderate. Acarbose also demonstrated the ability to retard relapse weight gain in overweight patients who had lost weight before begin-ning treatment with Acarbose (23, 24).
In view of the salutary effect that Acarbose has on blood sugar, insulin, lipids and HbA1c, I was at first sur-prised at the modest weight loss reported by participants in the studies (especially compared to the significant benefit I routinely observe in my patients). However, upon reflection, the modest effects of Acarbose as a weight loss agent in the above stud-ies can be understood. As noted, weight loss was a usual finding in the animal studies. Most animal studies were done on normal (non-di-abetic) or obese animals. However, the human studies were quite different, as the overwhelming majority of subjects were diabetic (or had impaired glucose tolerance)and were often simultaneous-ly treated with sulfonylureas and/or insulin. Diabetics characteristically gain weight, due to insulin resistance and hyperinsulinemia. Sulfony-lurea drugs or insulin are no-torious for causing additional weight gain (Metformin, which usually results in loss of body fat, was not common-ly used in most of the earlier studies cited above).
More recent studies, however, have shown much more positive resultssince the drugs used were Acar-bose alone, or Acarbose
Prob
abili
ty o
f any
Car
diov
ascu
lar E
vent
Days After RandomizationNo. at RiskPlacebo 686 675 667 658 643 638 633 627 615 611 604 519 424 332 232Acarbose 682 659 635 622 608 601 596 590 577 567 558 473 376 286 203
0 100
0.06
0.05
0.04
0.03
0.02
0.01
0
Placebo
Acarbose
P=.04 (Log-Rank Test)P=.03 (Cox Proportional Model)
200 300 400 500 600 700 800 900 1000 1100 1200 1300 1400
Figure 7. Effect of Acarbose on the probability of remaining free of cardiovascular disease. (17).
Figure 9. Proposed cardiovascular benefits of Acarbose. (18)
Figure 8. Effect of Acarbose on the probability of remaining free of hypertension. (17).
STOP NIDDM: Incidence of New Cases of Hypertension in IGT Patients
BP, blood pressure: IGT, impaired glucose tolerance; STOP NIDDM, Study to Prevent Non-Insulin Dependent Diabetes Mellitus Trial Chlasson JL, et al. JAMA 200;290:486-494.
18
16
14
12
10
8
6
4
2
00 1 2 3 4 5
Placebo
Hypertension defined as BP>140/90 mmHg
Years After Randomization
Cum
ulat
ive
Inci
denc
e (%
)
Acarbose
RRR=34% P=0.0059
Macrovascular Events
Atherogenesis
TGL, LDL/HDL
BP
IGT/ PPBGAvoid weight gain Insulin sensitivityInsulin level
Metabolic syndromeT2DM
Acarbose Inflammatorymarkers
Endothelial Dysfunction
Key: BP= blood pressure; HDL = high-density liopprotein; IGT = impaired glucose tolerance; LDL = low-density lipoprotein; PPBG = postprandial blood glucose;
T2DM = type 2 diabetes mellitus; TGL = triglycerides
8 www.antiaging-systems.com Order hotline: 1-866-800-4677 e-mail: [email protected]
combined with Metformin. In a large-scale observa-tional study of some 15,000 patients in China, Taiwan, the Middle-East, Morocco, Poland, Indonesia, Pakistan and the Philippines, with a follow-up of three years, a notable weight decrease was seen in all treatment groups (Acarbose alone, or Acarbose combined with Metformin and sulfonylureas or insulin) (25). In an even more recent study in China, 784 newly-di-agnosed diabetics were placed on Acarbose or Metformin. After 48 weeks, the scientists determined that Acarbose had similar efficacy to Metformin (in terms of glycemic control), but that more bodyweight was lost in the Acarbose-treated group (26).
Adverse effects and safetyAcarbose is a very safe drug; only about 1-2% is absorbed systemically. The most frequent side effects are all due to the unabsorbed carbohydrates, which ferment in the colon and can cause sometimes uncomfortable or embarrassing increased gas production, abdominal cramps, bloating and even di-arrhea (Fig. 11). These effects can be minimized by taking the lowest effective dosei.e., below that which causes the gastrointestinal distress. Continued use usually results in a reduction or resolution of these symptoms. As some tolerance seems to develop, dosages can be increased to the maximum recommended
dosage of 300 mg daily. In 1988, Clissold and Ed-
wards (6) reported that from the large clinical studies reported to date, acarboseeven after treatment for up to 5 years-does not produce any clinically significant adverse effects on biochemical and hematological parameters (emphasis added). In another large placebo controlled study, doses of acarbose as large as 200 mg three times daily had no toxic effect according to the results of hematologic and biochem-ical profiles, including liver function tests (5) (although these high doses did cause a higher incidence of abdom-inal side effects, as indicated in Fig. 11).
Acarbose is contraindicat-ed in people with inflamma-tory bowel disease, colonic ul-ceration or partial intestinal obstruction, predisposition to intestinal obstruction, chron-ic intestinal disease associ-ated with marked disorders of absorption or digestion, conditions which might be exacerbated by increased intestinal gas formation (like hernias), or impaired hepatic function.
DosageAcarbose works best when it is combined with food. When taken as a tablet, it is only as effective as when consumed in powdered form (Fig. 12). Odea and Tur-ton (28) recommended that Acarbose be marketed as a powder rather than a tablet, so it could be mixed into the
carbohydrate components of a meal.
Since Acarbose is not available as a powder, and is actually pleasant-tasting, I suggest that it be chewed with food at the beginning of meal or when consuming a starchy snack. I recommend that Acarbose be started at as little as 25 mg daily, to minimize side effects, and gradually advance the dosage and frequency as tolerance develops, up to a maximum dosage of 100 mg three times daily, chewed with meals. Of course, if one is on a strict high protein/Atkins Diet, Acarbose is not necessary.
Figure 10. Effect of acarbose on body weight gain and food intake of genetically obese Zucker rats. (19).
Figure 11. Incidence of adverse effects with Acarbose (usually 300-600 mg/day) in 962 diabetic patients for periods up to two years (27). The high incidence of side effects was due to the excessive doses (up to 600 mg/day) of Acarbose.
n=5 fa.fa. Zucker - Rats
Dose/ 100g Diet
BAY g 5421
g
Contr. 100 --
10mg 85 1.76 mg20mg 86 3.59 mg
40mg 73 6.09 mg
80mg 66 10.9 mg
Food Consumption
Body Weight
50
25
25
75
100-11 -5 -3 0 4 7 11 14 18 21 25 28 Days
0
BAY g 5421Dose/Rat
xDay
+|
Key:580g563g585g561g558g
Incidence (% of patients)
Flatulence
Abdominal distension
Diarrhoea
Borborygmus
Spasm, tenesmus, abdominal pain
50250
9www.antiaging-systems.com Order hotline: 1-866-800-4677 e-mail: [email protected]
Acarbose (Glucobay)30 x 100mg Chewable Tablets - $22.00
(Usually $27.49 - Aging Matters Special*: Save $5.49 per pack!)(*O er ends April 30th 2015)
*Res
tric
tions
may
app
ly in
som
e co
untr
ies.
All i
nfor
mat
ion
is ed
ucat
iona
l and
doe
s not
repl
ace
your
phy
sici
ans
advi
ce a
nd is
subj
ect t
o IA
S te
rms a
nd c
ondi
tions
whi
ch m
ay c
hang
e w
ithou
t not
ice.
Acarbose
Acarbose fi ghts diabetes, weight gain and aging! Acarbose helps to prevent the breakdown of
carbohydrates in the stomach into sugars.
Acarbose is used to help diabetics by preventing sugar spikes and it can also be a useful adjunct for weight loss too, since slowing
and preventing carbohydrate absorption aids dieting.
ConclusionI believe that acarbose, like metformin; will become increasingly recognized for its potential caloric-restric-tion-mimicking/anti-ag-ing, cardio-protective and anti-obesity effects. In fact, Acarbose and Metformin can be taken together, potenti-ating each others beneficial effects. Curiously, despite the well-documented safety and efficacy of Acarbose, it is not well known in the westand many pharmacies
have to special order it for my patients. Consequently, I was surprised to learn re-cently that alpha glucosidase inhibitors like Acarbose are the most popularly prescribed glucose-lowering agents in China. (29).
References1. Dilman V, and Dean W. The Neuroendocrine Theory of Aging and Degenerative Diseases, Center for Bio-Gerontology, Pensacola, Florida, 1992.2. Rabasa-Lhoret, R, and Chiasson, J-L. Potential of alpha-glucosidase inhibitors in elderly patients with diabetes mellitus and impaired glucose tolerance. Drugs and Aging, 1998, 13(2): 131-143. 3. Clissold SP, and Edwards C. AcarboseA preliminary review of its pharmacodynamic properties, and therapeutic potential. Drugs, 1988:35; 214-243,.4. Standl, E, and Schnell, O. Alpha-Glu-cosidase Inhibitors 2012cardiovascu-lar considerations and trial evaluation. Diabetes & Vascular Disease Research, 2012:9(3);163-169.5. Chiasson, J.L., Josse, R.G., Hunt, J.A., Palmason, C., Rodger, N.W., et al. The ef-fectiveness of Acarbose in the treatment of patients with NIDDM. A multi-centre controlled clinical trial. Ann Intern Med, 1994, 121: 928-935.6. Kado S, Murakami T, Aoki A, et al. Effect of Acarbose on postprandial lipid metabolism in type 2 diabetes mellitus. Diabetes Res Clin Pract. 1998;41:49-55.7. Lardinois CK, Greenfield MS, Schwartz HC, et al. Acarbose treatment of non-insulin dependent diabetes melli-tus. Arch Intern Med, 1984, 144: 345-7.8. Akazawa, Y., Koide, M., Oishi, M., Azuma, T., and Tashiro, S. Clinical usefulness of acarbose and fiber in the treatment of diabetes mellitus. Thera-peutics, 1982: 36: 848-9, 870-5. 9. Hoffman, J., and Spengler, M. Efficacy of a 24 week monotherapy with Acar-bose, metformin or placebo in dietary treated NIDDM patients: The Essen-II study. Am J Med, 1997, 103: 483.10. Nuttall FQ. Effect of age on the percentage of hemoglobin A1c and the percentage of total glycohemoglobin in non-diabetic persons. J Lab Clin Med, 1999, 134: 5, 451-453.11. Coniff, R.F., Shapiro, J.A., Robbins, D., et al. Reduction of glycosylat-ed hemoglobin and postprandial hyperglycemia by Acarbose in patients with NIDDM. Diabetes Care, 1995, 18: 817-24.12. Philip E, Sundaram ML, Das R, et al. Acarbose improves glycemic control as add-on or monotherapy in Indian type-2 diabetes: Findings from the GlucoVIP multinational observational study. Indian J Endocrinol Metab. 2013: 17; 9, pp.674-679.13. Magner JM, and Amatruda JM. Alpha glucosidase inhibitors in the treatment of diabetes, in: Diabetes Mel-litus: A Fundamental and Clinical Text, by: LeRoith D, Taylor SI, and Olefsky JM (eds), 2d ed, Lippincott, Williams & Wilkins, 2000.14. Balfour JA, and McTavish D. Acar-boseAn update of its pharmacology and therapeutic use in diabetes mellitus. Drugs, 1993, 46 (6): 1025-1054.15. Bischoff, H. The mechanism of alpha glucosidase inhibition in the manage-ment of diabetes. Clin Invest Med, 1995, 18: 303-11.
16. Stolk, R.P., Breteler, M.M.B., Ott, A., et al. Insulin and cognitive function in an elderly population. Diabetes Care, 1997, 20: 792-5.17. Chiasson JL, Josse RG, Gomis R, et al. Acarbose treatment and the risk of cardiovascular disease and hypertension in patients with impaired glucose toler-anceThe STOP-NIDDM trial. JAMA, 2003:290;486-494. 18. Arungarinathan G, McKay GA, and Fisher M. Drugs for diabetes: part 4 Acarbose. Br J Cardiol 2011;18:7881.19. Puls W, and Krause HP. Delay of carbohydrate absorption by inhibitors of intestinal alpha-glucosidases. Advances in Experimental Medicine and Biology, 1979, 119: 341-346.20. Calle-Pascual, A., Garcia-Hon-duvilla, J., Amrtin-Alvarez, P.J., et al. Influence of 16-week monotherapy with acarbose on cardiovascular risk factors in obese subjects with non-insulin-de-pendent diabetes mellitus: a controlled, double blind comparison study with placebo. Diabete Metab, 1996, 22: 201-2. 21. Johnston, P.S., Lebovitz, H.E., Coniff, R. Advantages of monotherapy with alpha-glucosidase inhibitors in elderly NIDDM patients. Diabetes, 1997, 46 Suppl 1: 158A. 22. Goto, Y., Nakagawa, S., Goto, Y., et al. Clinical utility of BAY g 5421 (acarbose) on NIDDM. Multicentre double-blind comparative study. Igaku no Ayumi, 1989, 149: 591-618. 23. Williams-Olsson T. Alpha-glucosi-dase inhibition in obesity. Acta Medica Scandinavica, 1985, 706 (Suppl 1): 1-39.24. Williams-Olsson T., Krotkiewski, M., Sjostrom, L. Relapse-reducing effects of acarbose after weight reduction in severely obese subjects. J Obesity and Weight Regulation, 1985, 4: 20-32.25. Li C, Hung YJ, Qamruddin K, et al. International noninterventional study of Acarbose treatment in patients with type 2 diabetes mellitus. Diabetes Res Clin Pract. 2011. Apr;92(1):57-64. 26. Yang W, Liu J, Shan Z, et al. Acarbose compared with metformin as initial therapy in patients with newly di-agnosed type 2 diabetes: an open-label, non-inferiority randomised trial. Lancet Diabetes Endocrinol. 2014;2(1):4655. 27. Hillebrand, I., Boehme, K., Frank, G., Fink, H., Berchtold, P. The effects of the alpha glucosidase inhibitor BAY g 5421 (acarbose) on meal-stimulated elevations of circulating glucose, insulin, and triglyceride levels in man. Research in Experimental Medicine, 1979, 175: 81-86.28. ODea, Kerin, and Turton, Janice. Optimum effectiveness of intestinal al-pha-glucosidase inhibitors: Importance of uniform distribution through a meal. American J Clin Nutr, 41: March, 1985, 511-516.29. Standl E and Schnell O. Alpha-glu-cosidase inhibitors 2012Cardiovascu-lar considerations and trial evaluation. Diabetes & Vascular Disease Research 2012:9(3);163-169.
Plas
ma
Glu
cose
(mm
ol/l) 8
7
6
5
4
3
0 30 60 90 120 150 180
Plas
ma
Insu
lin (m
U/l)
Time (min.)
10
20
40
50
60
70
0
30
GBR + 50mg Acarbose tabletGBR + 50mg Acarbose powder
Figure 12. Comparison of Acarbose powder and tablets on post-meal glucose and insulin concentrations. After ingestion of 75 gram starch (ground brown riceGBR) with 50 mg Acarbose--either mixed in the meal as a powder (- - -) or eaten with the first mouthful as a tablet ( ----- ), clearly shows that Acarbose powder mixed with the food is much more effective than when consumed as a tablet (28).
10 www.antiaging-systems.com Order hotline: 1-866-800-4677 e-mail: [email protected]
Acarbose (Glucobay)30 x 100mg Chewable Tablets - $22.00
(Usually $27.49 - Aging Matters Special*: Save $5.49 per pack!)(*O er ends April 30th 2015)
*Res
tric
tions
may
app
ly in
som
e co
untr
ies.
All i
nfor
mat
ion
is ed
ucat
iona
l and
doe
s not
repl
ace
your
phy
sici
ans
advi
ce a
nd is
subj
ect t
o IA
S te
rms a
nd c
ondi
tions
whi
ch m
ay c
hang
e w
ithou
t not
ice.
Acarbose
Acarbose fi ghts diabetes, weight gain and aging! Acarbose helps to prevent the breakdown of
carbohydrates in the stomach into sugars.
Acarbose is used to help diabetics by preventing sugar spikes and it can also be a useful adjunct for weight loss too, since slowing
and preventing carbohydrate absorption aids dieting.
The thymus gland is small in size, weighing no more than 1.5 ounces and is located in the upper region of the chest. Its importance in the regula-
tory function of the immune system was recognized in the 1960s, when thymus gland removal in animals resulted in a distinct and progressive
depression of the immune system and when left un-checked, usually resulted in the death of the animal from an uncontrollable infection.
However, when thymus tissue was implanted into such animals, partial or complete recovery took place.
Important insight was gained from experiments with thymectomised animals in which, instead of a new thymus implant, an infusion chamber was implanted, (which did not allow cells to pass through). When thymus tissue, or a cell free thymus extract was placed in these chambers, the immune
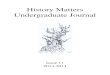
Figure 1: Shows the relation between a decrease in blood levels of thymic peptides and the direct correlated increase with thymus dependant immunity and its increase on age related diseases. Published by the World Health Organisation, technical report series, 630 (1978).
The almost forgotten role of the thymus By Phil Micans, MS, PharmB
12 www.antiaging-systems.com Order hotline: 1-866-800-4677 e-mail: [email protected]
0 5 10 15 20 25 30 35 40 45 50 75 80 85 Years
Age related disease
Thymus dependent immunity
Blood thymosin levels
Diseases of childhood
By Leslie J Farer
13www.antiaging-systems.com Order hotline: 1-866-800-4677 e-mail: [email protected]
system function of the animals also improved. This helped to prove that water soluble thymic substances, not associated with intact thymic cells, can considerably influence immune defense (1).
Later research demon-strated that the thymus gland produced a family of specific immune-regulatory polypep-tides, known collectively as thymic hormones. It has also been shown that other organs (i.e. the spleen), also synthesis similar peptides (2).
The precise mechanism of action of these thymic pep-tides has still not been fully elucidated. There is however, no doubt that the involution of the thymus gland, which starts very early, often at puberty, is associated with a decrease in thymic func-tion and a weakening of the immune defense system in elderly individuals (3, 4).
It has also been shown, that thymectomy in older persons, accelerates in a last-ing manner, the age related decrease in the immune system (2). More recent re-
search has demonstrated that the thymic hormones have a marked effect on the mat-uration and differentiation of T-cells. The great signif-icance of the T-cell system for immune defense is also well documented. For whilst increasing age is associated with a generalized weakening of immune defense, the de-crease in the function of the T-cell system appears to play the greatest role in the overall decrease in immune defense.
Furthermore, thymus hor-mones are known to reduce autoimmune reactions and help to prevent bone mar-row injury, by assisting the production of white and red blood cells (5).
So as the thymus gland begins to atrophy (shrink/
decline) by the age of 20, it is considered to be a major bio-marker of aging (6). Therefore, as Figure 1 indicates, the re-duction in thymus hormone production is considered to be a major link between a decreasing immune system with advancing age.
But interestingly, thymus gland hormones do not increase all immune function activity, but rather appear to be able to actually reduce im-munity where it is excessive, (as seen by high T4/T8 ratios in rheumatoid arthritis). For while thymus hormones improve immune function where it is weak, (i.e., low T4/T8 ratios in HIV), thymus hormones have been shown to be able to normalize the T4/T8 ratio to the ideal healthy T4/T8 ratio of 1.74 (7).
Thymus and allergiesMeanwhile, whilst thymus hormones increase antibod-ies where theyre needed, they have also been shown to be able to reduce the levels of the
allergy antibody IgE, thus having benefits for patients suffering with allergies such as allergic rhinitis, asthma and atopic dermatitis, etc. (5).
Thymus and growth hormone Furthermore, some of the health benefits of thymus hormones may be due to a relation between the thymus and the pituitary gland. The pituitary gland is the center of production for growth hor-mone and thymus hormones. By increasing the number and activity of T-cells, this enables T-cells to secrete growth hormone releasing hormone (8, 9).
This may help to explain some of the anabolic chang-es seen in patients who are undergoing thymus hormone supplementation. Certainly it is noted that when the thy-mus gland is removed, it is accompanied by degeneration
Figure 2 shows the reduction in the number of joints
afflicted with pain, (which is elicited by movement and by pressure for rheumatoid
arthritis sufferers), when treated with Thym-Uvocal
. There is a very significant improvement within 6-weeks
which continues past 74-weeks.
Figure 3 shows the reduction in morning stiffness for rheumatoid arthritis sufferers when using Thym-Uvocal . There is a marked improvement within 6-weeks which continues on past 74-weeks.
Minutes (N=60)160
140
120
100
80
60
40
20
0
160
140
120
100
80
60
40
20
00 2 4
Weeks Weeks6
Minutes (N=17)
68 70 72 74
Number of joints (N=60/ 17)
Weeks
201816141210
86420
0 2 4 6 68 70 72 74
in pituitary cells (2) with a resultant catabolic action.
Thym-Uvocal , a whole natural thymus product from GermanyHowever, it has not been shown that one can isolate a single thymic hormone with the whole complex of functions of the thymus gland. It would rather appear that single isolated molecules carry out single psycholog-ical functions, (e.g. T-cell differentiation), but not other functions. For this reason, it is still considered appropriate to produce and administer a natural, complex mixture of extracted thymus hormones, capable of comprehensive modulation and stimulation of immune defenses.
The Germany Compa-ny, Strathmann AG, have a long-established product called Thym-Uvocal , which is known to be an effective whole and natural thymus hormone agent that is very well tolerated, with impres-sive actions in those dis-ease states associated with impaired immune defenses, including old age.
Thym-Uvocal is not just a desiccated whole thymus glandular extract, of the type found in health food stores. The active substances in Thym-Uvocal are obtained by a selective, multi-stage biotechnology process. The starting material is thymus glands from strictly selected and healthy calves, raised in Australia.
Tissue from any given ani-mal is only used after a veteri-nary physician has examined the live animal and issued a certificate of good health. Before the tissue is processed, histological and bacterio-logical tests are performed. During the multi-stage processing, proteins and prohormones in the tissue are enzymatically cleaved to short-chain pharmaceutically active oligopeptides.
Then filtration and special heat treatment ensure the inactivation and removal of any microorganisms. The controlled and reproducible manufacturing process pro-duces an activation and con-centration of the desired low molecular weight peptides.
The various thymus gland hormones range in their molecular weight from 860 Daltons (Thymulin) to 5600 Daltons (Thymopoietin), and since animal experiments and human clinical research has found no single thymus gland hormone to be capable of performing all the im-mune optimizing functions induced by the thymus gland hormones as a whole, a pharmaceutically balanced thymus gland polypeptide hormone mixture is both more natural, and more likely to be safe and effec-tive, than any single specific thymic hormone, (10).
It is interesting to note, that Thym-Uvocal has been
used clinically in Europe since 1976 and still represents one of the finest thymic sup-plements available anywhere on the world market today.
Thym-Uvocal and cancerThe main indications for Thym-Uvocal have been to strengthen the immune sys-tem, particularly in patients with malignant disease. The immune system is partially or completely impaired in pa-tients with malignant tumors, particularly if they are also being treated with cytostatic drugs and/or radiation.
Thym-Uvocal has been administered along with treatment, and has reduced side-effects, with no inter-actions or contraindications being reported to date. Many physicians have also reported improvement in the underly-ing disease, with regression of existing tumors, a delay in metastasis and better remis-sion times (13).
Possible positive effects on the underlying cancer disease with Thym-Uvocal include:
1. Regression of an existing tumor.
2. Delayed metastasis.3. Prolonged remission time.4. Improvement in the qual-
ity of life.
Thym-Uvocal and rheumatic diseaseIn the area of rheumatic disease, Thym-Uvocal can being about subjective and
Figure 4: The connection of thymus hormones to immunity, disease and stress.
14 www.antiaging-systems.com Order hotline: 1-866-800-4677 e-mail: [email protected]
ThymusHormones
Immune Defense
Conflicts Stress
Conflicts Stress
Disease
objective improvement, leading to both a reduction in inflamed joints and reduction in the number and severity of painful joints (shown in figures 2 and 3).
It is assumed that the com-bination of active substances has a positive immunomod-ulating effect on the autoim-mune processes. Our atten-tion here is focused upon patients who cannot tolerate the usual doses of non-ste-roidal drugs used in rheuma-tism, or in whom such drugs no longer have the desired effect. Administration of Thym-Uvocal can make it possible in many cases to decrease the effective dosage of non-steroidal anti-inflam-matories, and/or prevent a switch to steroids.
The possible improve-ments in rheumatism with Thym-Uvocal include:
1. Reduction in morning stiffness.
2. Increase in locomotor activity.
3. Increase in mobility.4. Positive change in labora-
tory findings.5. Reduction of pain.
Both specialists and gener-al practitioners very often report astonishing objective improvement in their pa-tients. This has included less disability, better mobility and reduced swelling of the joints. Frequent reports include the ability of Thym-Uvocal
administration to allow lower doses of non-steroidal anti-inflammatories, and that long term use has allowed them to wean rheumatism patients off steroids (11).
ConclusionImmuno-incompetence can result from disease and vice-versa. Some drugs can treat disease, but weaken the immune defense systems at the same time. Physical and psychological stress can cause disease directly, or do the same indirectly by caus-ing immuno-incompetence, (see figure 4).
As is shown in figure 1, there is a close correlation between decreasing thymic activity, worsening immu-no-competence and increas-ing susceptibility to disease as we grow older. As it is known that blood thymus levels decline after the age of
25, this helps to explain why older individuals are the most important group for supple-mentation with thymus, yet the thymus gland is virtually completely overlooked by mainstream medicine, even by some in the field of endo-crinology!
There is no doubt that the thymus gland appears to be the most forgotten about gland in medicine today!
Yet, because of the im-mune stimulation induced by Thym-Uvocal supplementa-tion, it has been applied for a number of different indica-tions which all involve im-mune system decline. These include infections (viral and bacterial), allergies and states of exhaustion (chronic fatigue), Aids, cancer and arthritic disorders.
An interesting comment was made by biochemist James South MA, who noted in his article (12); the overlooked but vital role of the thymus, that in addition to its immune enhancing properties, the personal use of Thym-Uvocal for himself and his wife, induced a state
of well-being and had vi-talizing effect on them both.
The dosages depend upon the need, and vary from 1 capsule (240mg each) twice a day, to 2 capsules three times a day. Its effects can normally be noted within 3-7 days. Side-effects are very rare and to date no known contraindi-cations have been reported.
References
1. Goldstein et al. Thymosin and the Immunopathology of Aging. Federa-tion Proc., 33, 2053-56, 1974.2. J. Goss & M. Flye. The Thymus Regulator of Cellular Immunity. Aus-tin: R.G. Landes Co. 1993.3. M. Sztein et al. Modulation of Interleukin 2 Receptor Expression on Normal Human Lymphocytes by Thymic Hormones. Proc. Nat. Acad. Sci. USA, 83, 6107-11, 1986.4. M. Zatz & A. Goldstein. Mech-anism of Action of Thymosin. J. Immunol., 134, 1032-38, 19855. N. Kouttab et al. Thymomodulin: Biological Properties and Clinical Applications. Med. Oncol. and Tumor Pharmacother. 6, 5-9, 1989.v 6. R. Klatz & C. Khan Grow Young with HGH NY: Harper Collins 1997.7. P. Cazzola et al. In Vivo Modulat-ing Effect of a Calf Thymus Acid Lysate on Human T Lymphocyte Subsets and CD4+/ CD8+ Ratio in the Course of Different Diseases. Curr. Ther. Res., 42, 1011-17, 1987.8. D. Weigant and J. Blalock. Immu-no-reactive Growth Hormone- Releas-ing Hormone in Rat Leukocytes. J. Neuroimmunol. 29, 1-13, 1990.9. K. Kelly et al. A pituitary- Thymus Connection during Aging. Ann. N.Y. Acad. Sci. 521, 88-98, 1988.10. Thym-Uvocal, Immunotherapeutic Agent; A 32 page booklet published by Medalfa AG, Pratteln, Switzerland, 31 references plus many case histories.11. Z. Fahmy. Immuno-stimulation therapy with Thymus Extract in rheu-matoid arthritis. A journal of medical practice (in German titled- Erfahrung-sheilkunde), Vol. 31, No 5, May 1982, pp. 423-427.12. J. South, The thymus gland, its overlooked but vital role. IAS An-ti-Aging Bulletin, v3, i6, Fall 1998, pp 7-15.13. Procedures of the International Thymus Consensus Conference, Ther-apeutic relevance of thymic peptides in the treatment of tumor patients. Quarnbek, Germany, April 12-13, 1997
15www.antiaging-systems.com Order hotline: 1-866-800-4677 e-mail: [email protected]
There is no doubt that the thymus gland appears to be the most forgotten about gland
in medicine today!
*Res
tric
tions
may
app
ly in
som
e co
untr
ies.
All i
nfor
mat
ion
is ed
ucat
iona
l and
doe
s not
repl
ace
your
phy
si-
cian
s ad
vice
and
is su
bjec
t to
IAS
term
s and
con
ditio
ns w
hich
may
cha
nge
with
out n
otic
e.
Thym-Uvocal is the only thymus extract
supplement that contains all 13 of the thymic
peptides. Your immune system is continuously
assaulted by a barrage of viruses and bacteria
that can compromise your health. To bolster
your immune system we recommend Thym-
Uvocal , a whole natural thymus product from
Germany. Thym-Uvocal is produced to rigorous
pharmaceutical standards which make it the
worlds best quality thymus extract supplement.
THYM-UVOCAL
13 Ways to boost immunity and well-being in one natural product
*O er valid until April 30th
Thym-Uvocal 90 x 200mg Caps $99.99 FOR A LIMITED TIME ONLY $94.99 - SAVE $5 ON EACH PACK*
Beating the flu seasonAn interview with Richard Stead about the power of OSCNRichard Stead is a British chemist who has introduced oxythiocynate ions (OSCN) as a
supplement to the world. OSCN is a natural molecule in the human body that appears to
literally represent the bodys first line of immunity.
18 www.antiaging-systems.com Order hotline: 1-866-800-4677 e-mail: [email protected]
PM: Richard thank you very much for your time today to help explain the work youve been doing.
RS: My pleasure Phil.
PM: I suppose the first ques-tion to ask is why did you look at the OSCN molecules in the first place?
RS: Our original interest was for a technology to replace Chlorine as an antibacterial wash for cut and prepared vegetables, and maybe even fresh meat. The technology worked very well--as good as was achieved by the chlorine based systems, but also a great deal safer for workers, the environment and the actual foods.
PM: So why hasnt the food industry adopted them?
RS: Chlorine is a very cheap material. Although ours worked out to be 5 times more expensive than chlo-rine--and 5 times cheap is still relatively cheapand despite the fact that the su-permarkets and the proces-sors liked the product, neither would agree to bear the ad-ditional costs. So we failed to enter the food market. I had always told the processors that if one of their workers fell into our wash water they would come out healthier
than before they fell in. With this in mind I determined to use the technology to create an alternative to existing systems for pathogen elim-ination an alternative to antibiotics as our first target, and then a system to remove airborne pathogens.
PM: It is clear that new viruses pose major threats to world health, and lead-ing scientists are regularly exclaiming that antibiotics are becoming less effective by the day. What can nature teach us?
RS: Indeed, Phil, I like to say Nature has the an-swer--chemistry is the key, and I do believe that OSCN is one of those answers.
PM: So where in the human body can one find OSCN molecules?
RS: Principally in saliva, air-ways, tears and mothers milk.
PM: And what role do they play?
RS: The OSCN molecule is created on demand when necessary to destroy low lev-els of pathogens. We say low levels because it is to cope with those pathogens that come into our eyes or into our mouths, on our fingers or on foods. One reason our
Grandmothers told us to chew our foods more was to ensure that saliva was able to get all surfaces of the food and destroy any pathogens. Maybe our modern way of eating fast food too fast is the cause of numerous stomach bugs?
Ed. For more technical details and references please refer to Pro-fessor Paul Claytons article The age of antibiotics is coming to an end in issue 1, 2012 of the Aging Matters magazine.
PM: Do OSCN have other advantages not attributable to antibiotics? The possibil-ity of bacteria being able to develop resistance is almost zero.
RS: OSCN do not attack healthy gut flora. Why is this important? There is a growing acknowledgement that the microflora in our gut is related to so much of our wellbeing and as a consequence, any disruption
(referred to as dysbiosis) can lead to a wide range of brain/mental and bodily malfunc-tions. Therefore, any medica-tion that does good- without disrupting the gut flora is a real bonus.
PM: With such benefits, why has there never been an OSCN supplement before?
RS: It is hard to explain, but I have a couple of comments: First, it is hard to cover the technology of the molecule with a patent, and this alone would stop many pharma companies from looking at the product; second is the relative short stability of the molecule. This makes it dif-ficult to be factory-produced and bottled or encapsulated.
PM: How did you overcome this issue?
RS: With difficulty, is the short answer, but we were determined. So with a great deal of creative thinking, de-
...any medication that does good - without disrupting
the gut flora is a real bonus...
In an age of the ever-growing threat of viruses and pathogens and the failing
of established antibiotics, Phil Micans (PM) interviewed Mr Richard Stead (RS)
about how OSCN may be one possible answer to bolster immunity.
19www.antiaging-systems.com Order hotline: 1-866-800-4677 e-mail: [email protected]
sign and heart ache we finally achieved a system used by patients/caregivers to create the OSCN at the point/time of use
PM: What sort of conditions have OSCNs been tested against?
RS: In laboratory conditions, the list of pathogens against which OSCN has been successful is huge. We are in the middle of clinical trials against 4 different conditions, plus, a further trial for Lymes disease is about to start.
PM: And what have been the responses from health professionals and patients using the kit?
RS: I cannot say we have been 100% successful, but almost all users have seen positive benefits and improvements in their conditions/symptoms. Of particular success is gut dysbiosis. The removal of the overload of bad bacteria by OSCN has allowed sufferers to start to build up the good gut flora and then onto diets to rebuild their health. But the removal of the bad bacte-ria is essential as a first step. Gut dysbiosis is evident in almost all sufferers of chronic conditions, for example, autism, MS, chronic fatigue, and many others.
PM: How does one dose OSCN?
RS: The dosing regimens are difficult to determine. If we could know exactly how
many bad bacteria were present then a very accurate dosing schedule could be created. But until we have fast identity of the pathogen and measurement of bacterial loads, dosing has to be based upon a clinicians experience and knowledge of the patient. We always try to bring down pathogen levels to a level at which the immune system can take over. Therefore, if a sufferer has had the condition for a long time (e.g. for many months or even years) then a higher dose is needed than for a recent infection. For people prone to regular infec-tions, then maybe a monthly maintenance dose is an idea to consider. The effect would be to regularly reduce the build-up of pathogens that are always invading us and getting past our defences, but which are not yet at a level to cause symptoms.
PM: Have there been any side-effects or contraindica-tions?
RS: None known in the low doses used. However, a good side effect identified often by chronic sufferers has been the Herxheimer reaction that of the liver being overloaded by the poisons given off by dying and dead pathogens, killed by the OSCN. This good sign of efficacy lasts but a short time and most practitioners/clini-cians can prepare the patient/liver in advance.
PM: Some of the literature has suggested that OSCNs
can have a slight lowering effect on the thyroid, would you care to comment on that?
RS: Yes, we have read the papers. Our opinion is that its not affected in the doses that we advocate, i.e. one or two kits/ 25/50 mg per day. But those concerned can easily offset this by adding a few drops of iodine daily, if they wish, or as is suggested by their practitioner.
PM: Are there any other steps that folks can take along with OSCN to make the program synergistic?
RS: We recognise that the effect of OSCN is to destroy pathogens. That on its own does not make the patient healthy. There is no residual effect after our molecule has been used and the patient could remain open to the same pathogen or other path-ogens unless they take steps to improve their health and immune competence. This is an important aspect of work-ing with Practitioners and clinicians. We are all different as individuals and so require
different diets to bring us back to good health. Phil, just before we finish, I am very excited about our trials that are near to their conclusion and hope that the results are good and that we will then be able to present one or more papers to medical magazines for them to publish. If the results are good, we will of course let you know, and then we will start new trials on other conditions and my idea is to look at airways and topical conditions. Maybe your readers have suggestions together with guidance where we can find support groups of sufferers of a particular condition willing to find new treatments?
PM: Thats very exciting, I am sure that our readers will want to know their details when they become available.
RS: It will be my pleasure to report once they are published, and thanks for al-lowing me this chance to talk about OSCN, the prospects for which I find so exciting.
PM: Thank you very much.
We always try to bring down pathogen levels to a level at which the immune system can take over.
1st Line produces oxythiocyanates
to neutralise infections including
viruses, just as your body does.
So next time youre feeling under the weather use
1st Line, the natural way to boost your 1st Line
of immune defense.
SELF DEFENSE
1st LineOSCN Kit $79.99
*Res
tric
tions
may
app
ly in
som
e co
untr
ies.
All i
nfor
mat
ion
is ed
ucat
iona
l and
doe
s not
repl
ace
your
phy
sicia
ns a
dvic
e an
d is
subj
ect t
o IA
S te
rms a
nd c
ondi
tions
whi
ch m
ay c
hang
e w
ithou
t not
ice.
SPECIAL OFFER SAVE $5.00 ONLY $74.99**(offer ends 30th April 2015)
21www.antiaging-systems.com Order hotline: 1-866-800-4677 e-mail: [email protected]
We are constantly being bombarded with messages from the media, the department of public health, and the World Health Organization (WHO) about how overweight and sedentary we have become.
The incidence of obesity has reached epidemic proportions. Our growing waistlines coupled with our sedentary lifestyles have put us at risk for developing Type 2 diabetes as well as a host of oth-er chronic degenerative diseases. I raise this issue, because in the face of all this public discussion, it is easy to ignore the public health warnings, particularly if you are an individual of normal weight and consider yourself at low risk of developing diabetes.
Actually, when one looks at the disease Diabetes Mellitus (DM), it is apparent that what is truly occurring is an accelerated form of aging. Aging is occurring in all of us. It is important to make note of the many microvas-cular and macrovascular compli-cations of diabetes because these complications provide us with clues from which we can form a logical and rational anti-aging protocol.
There are a number of differ-ent theories of aging. One of the oldest and best known theories is Denham Harmans free radical theory of aging which dates back to 1956. This theory posits that unpaired oxygen electrons, which are produced during aerobic respiration, cause cumulative oxidative damage, resulting in the effects of aging and death. Harman posited that endogenous oxygen radical generation occurs within the body, as a by product of enzymatic redox chemistry. Therefore the necessary ingredi-ent for life oxygen is a double
edged sword. While we cant live without breathing in oxygen, we cannot utilize oxygen without it damaging our cells.
Another theory of aging is Johan Bjorkstens cross-linking theory of aging. The cross-link-ing theory of aging and the free radical theory of aging are not mutually exclusive, but synergis-tic. Ironically the cross-linking theory of aging is actually based upon processes described by the food chemist Louis Camille Maillard in 1912 who outlined the non-enzymatic chemical reactions between proteins and carbohydrates that cause foods to turn brown.
This process also occurs in the body when a reduced sugar (usu-ally glucose) attaches to a protein. An intermediate reversible product is formed. That product is a Schiff base. As the protein/glucose complex continues to be exposed to additional sugar a more stable, less reversible complex forms. That complex is known as an Amadori prod-uct. Amadori products further degrade into a number of highly reactive carbonyl compounds. These compounds are known as Advanced Glycation End products (AGEs) or when lipids or fats are involved Advanced Lipoxidation End products (ALEs). AGE/ALEs go on to react with other fats, proteins, amino acids, nucleic acids and a variety of other cells. AGEs in tissues increase the rate of free radical production, cause tissue injury,
Pyridoxamine: A universal weapon against agingBy Karen Kaufmann, MS1st Line produces
oxythiocyanates to neutralise
infections including viruses, just as
your body does.
So next time youre feeling under the weather use
1st Line, the natural way to boost your 1st Line
of immune defense.
SELF DEFENSE
1st LineOSCN Kit $79.99
*Res
tric
tions
may
app
ly in
som
e co
untr
ies.
All i
nfor
mat
ion
is ed
ucat
iona
l and
doe
s not
repl
ace
your
phy
sicia
ns a
dvic
e an
d is
subj
ect t
o IA
S te
rms a
nd c
ondi
tions
whi
ch m
ay c
hang
e w
ithou
t not
ice.
SPECIAL OFFER SAVE $5.00 ONLY $74.99**(offer ends 30th April 2015)
22 www.antiaging-systems.com Order hotline: 1-866-800-4677 e-mail: [email protected]
inflammation, and can deposit anywhere. For example, when AGEs attach to LDL cholesterol, the LDL cholesterol is rapidly oxidized and is more likely to deposit within a blood vessel thereby contributing to plaque formation and atherosclerosis. AGEs form at an accelerated rate in hyperglycemia, diabetes, and metabolic syndrome.
However, AGEs are a univer-sal symptoms of aging. They can deposit in any organ or tissue, including the skin, the lungs, the blood vessels, the lens of the eye, the neurons in the brain, and in the filtering mechanism in the kidney. Whenever and wher-ever AGEs deposit, the normal functioning of that organ, tissue or cell is compromised. There is evidence that AGEs can bind with DNA and have a mutagenic effect (contributing to the risk of cancer and autoimmune disease).
When we think of the for-mation of AGEs and ALEs we generally think of them forming endogenously as a result of the glucose that is already within the body. We often forget that there are also dietary AGEs and ALEs. Our exposure to AGEs and ALEs occurs as an end result of normal metabolism. However we can also be contrib-uting to the problem through the intake of dietary, exogenous AGEs. So, no matter who we are, how fit we are, how thin we are, we cannot escape the effects of these cross linked proteins.
PyridoxamineVitamin B6 exists in 3 naturally occurring forms: pyridoxine, pyridoxal and pyridoxamine (PM). Pyridoxine is the form most commonly seen in sup-plements. However, each can be phosphorylated at the 5 position. Pyridoxal 5 phosphate (PLP) and pyridoxamine 5 phosphate (PMP) are the active coenzyme forms. Pyridoxine is found in plant sources. Pyridoxamine and pyridoxal are found in animal sources where they exist mainly in their phosphorylated forms. All 3 forms have some ability to function as anti-glycation agents inhibiting the formation of AGE/
ALEs, but it is pyridoxamine (PM) that is the most potent agent of the three forms.
Pyridoxamine prevents the formation of AGEs. It works by trapping reactive carbonyl groups and it also demonstrates free radical quenching proper-ties. Accumulation of AGEs is a physiologic consequence of tissue aging. Tissue deposits of AGEs and circulating AGEs are a hallmark of diabetes mellitus. Damage from AGEs is also seen in a variety of other vascular and degenerative diseases. AGE generation potentiates oxidative damage and lipid peroxidation in target tissues. The tissue dam-age caused by AGEs and ALEs further drives inflammation. The more we understand about the role of AGEs in normal global aging, the more impor-tant a pharmacologic agent like pyridoxamine becomes. Pyridoxamine has multiple mechanisms of action which can are best summarized in a study published in 2005. PM inhibits post Amadori steps of the Maillard reaction by seques-tering catalytic metal ions and blocking oxidative degradation on Amadori intermediate.
PM also has the capacity to scavenge toxic carbonyl prod-ucts of sugar and lipid degra-dation, and to inhibit reactive oxygen species. Pyridoxamine has been shown to limit the formation of AGEs without affecting glycemic control. There is additional evidence that high blood lipids contribute to the formation of AGE/ALEs even in the absence of hyperglyce-mia. Pyridoxamine inhibited the formation of both toxic end products demonstrating a protective effect on vascular and renal function in an animal model. It is quite unique that PM demonstrates the ability
to prevent lipid peroxidation and therefore ALE formation. Pyridoxamine inhibited the formation of ALEs by trapping malondialdehyde (MDA) an important intermediate in ALE formation. The beauty of pyridoxamine lies not only in its multiple mechanisms of action, but also in its tolerability. There are little or no contraindications for its use.
The role of AGEs in health and diseaseThere are a variety of chronic and degenerative diseases as-sociated with the accumulation of AGEs in tissues and organs. Many of these conditions we consider a normal part of growing older. The toxic AGEs can deposit anywhere compro-mising physiologic function. AGEs deposit in the lens of the eye leading to the formation of cataracts. When AGEs deposit in the vascular system, long lived proteins such as collagen and elastin become stiff and hypertension is just one of many possible consequences. It is hard to envision a chronic degenera-tive condition or disease of aging that would not benefit from the inhibition of AGE/ALEs formation. Although AGEs in proteins are probably correla-tive, rather than causative, with respect to aging, they accumu-late to high levels in tissues in age-related chronic diseases such as atherosclerosis, diabetes, arthritis and neurodegenerative disease. Inhibition of AGE for-mation could inhibit oxidative and inflammatory damage in target tissues, slowing the pro-gression and pathophysiology of aging. This could lead to a signif-icant improvement of the quality of life of the aging population. It is evident that AGE/ A`LEs likely
contribute to both diabetic and non diabetic vascular damage. AGEs accumulate in tissues and organs in rheumatoid arthritis and Alzheimer disease. As mentioned above, diabetes melli-tus provides us with a model of accelerated aging. AGE/ALEs contribute to the various mi-crovascular and macrovascular complications which occur in the disease.
Just as AGEs compromise the flexibility and efficiency in the vascular system, AGE deposition in the kidney compromise the kidneys filtering capacity and can lead to nephropathy and kidney failure. Culling the most recent literature was enlighten-ing. There is now evidence that AGEs may contribute to colon cancer and melanoma.
Pyridoxamine may prove to be a therapy for primary hyperoxaluria (which causes the formation of kidney stones. AGEs may well interfere with osteoclast activity by altering the structural integrity of bone matrix proteins and osteoclast induced bone resorption, there-by contributing to an increased risk of bone fracture. There may even prove to be a link between AGEs and osteoarthritis (OA) the most common cause of chronic pain and disability in older adults.
ConclusionIn conclusion, pyridoxamine may prove one of our most pow-erful nutritional weapons in the war against chronic degenerative disease and aging itself.
Pyridoxamine may prove one of our most powerful nutritional weapons in the war against chronic
degenerative disease and aging itself.
Pyridoxamine is the rarest and most potent form
of the three naturally occurring B vitamins. It is
particularly eff ective in the late stages of glycation
and at reducing the formation of advanced
lipoxidation end products (ALEs).
PyridoxamineRAREST AND MOST POTENT FORM OF VITAMIN B6
*Res
tric
tions
may
app
ly in
som
e co
untr
ies.
All i
nfor
mat
ion
is ed
ucat
iona
l and
doe
s not
repl
ace
your
phy
sici
ans
advi
ce a
nd is
subj
ect t
o IA
S te
rms a
nd c
ondi
tions
whi
ch m
ay c
hang
e w
ithou
t not
ice.
PyridoxPro (Pyridoxamine) 60 x 50mg Tabs $29.99FOR A LIMITED TIME ONLY $24.99SAVE $5 ON EACH PACK*
*Off er valid until April 30th
24 www.antiaging-systems.com Order hotline: 1-866-800-4677 e-mail: [email protected]
Unique formula:
Can-C eye-drops are the formula from the original published human trials. They contain a purified and racemized form of n-acetylcarnosine (made in Japan); this natural di-peptide has potent anti-glycating and anti-oxidant properties that prevents lipid peroxidation. Note that the formula is important- its not all about the n-acetylcarnosine; the specific carrier agents and their purity are also important. If you look at the Can-C formula you will see differences to the copycats, (remember it is only Can-C that is patented in recognition of the original work). If you want the best possible results in the fastest possible time, then choose Can-C to deliver them according to the clinical trials.
Clinical trial:
Patients placed two-drops of Can-C into their eyes twice daily for a 6-month period, the outcome was:
90% saw an improvement in their visual acuity.
88.9% of patients showed improvement in the clarity of their lens.
There have been numerous reports of cataract shrinkage and even disappearance with documented evidence that Can-C eye-drops remain effective (and safe) more than 24-months later. The most commonly expressed initial reports are that glare is significantly improved, (for example night driving is much safer) and color perception is enhanced.
Improving eye-sight:
More evidence is mounting that Can-C is efficacious for many conditions including:
Cataracts (particularly the senile version)
Glaucoma Presbyopia Corneal disorders Eye strain Ocular inflammation Blurred vision Vitreous opacities and
lesions Diabetes mellitus
complications Contact lens users Dry eye syndrome
Of special interest may be to persons who wear contact lenses. This is because Can-C inhibits the accumulation of lactic acid and therefore contacts can be worn for longer periods without pain.
We have also received reports that Can-C not only aids dry-eye syndrome with its lubricants, but that Can-C helps to unclog proteins from the lacrimal ducts, thus releasing more natural tears onto the eye.
In a similar way, it is also believed that the unclogging of proteins in the eyes drain, (the Schlemm valve), helps to reduce intraocular pressure and thus aids glaucoma.
A BREAKTHROUGH FOR CATAR ACT
SPOTLIGHT: CAN-C
24 www.antiaging-systems.com Order hotline: 1-866-800-4677 e-mail: [email protected]
Can-C eye-drops are the original brand- developed by Innovative Vision
Products (IVP). This group were the first to research, publish and prove how
eye-drops can reduce and even eradicate cataract. Accordingly there are active
US and EU patents (and others pending) on this unique and special product.
Dr. Kyriazis book, The Cataract Cure, details the usefulness and evidence of Can-C eye-drops. It is now available as a FREE e-book at: www.antiaging-systems.com/can-c-ebook
Above: Can-C Plus capsules
Right: A womans eye shows the cataract before treatment. Far Right: 5-months later after use of Can-C eye-drops (two drops twice
daily), there is no longer a visible cataract and eyesight has improved.
Before: After:
25www.antiaging-systems.com Order hotline: 1-866-800-4677 e-mail: [email protected]
Dr. Rudmans research concluded that after injecting his elderly patients with GH, many of them had reversals of their biological age markers by as much as 20-years; specifically having noted improved skin, hair, muscle mass, decreased fat levels and enhanced levels of stamina, strength and well-being.
Its not entirely surprising given the multi-faceted role of growth hormone, plus as its name suggests it is involved in the growth and repair of tissues, but unfortunately blood levels of it decline dramatically past the age of 35 (see figure 1), despite the fact that there is evidence that the pituitary gland continues making significant amounts of it.
GH injectionsThe issue with injecting GH, (brand names include Genotropin, Saizen and Zomacton), other than its expense, is that it does have to be injected to be effective, this is because as a 191 chain amino-acid it simply cant be absorbed via any other route, thus daily injections can become a chore.
Furthermore, many countries have decided that GH injections be classified as a controlled substance, partly because of its anabolic actions. Controlled substances often require special import and export licenses; this is over-and-above the requirement for a prescription.
Furthermore, the research of Dr. Richard Walker has highlighted that bolus injections of GH are not
bioidentical and that as they induce spikes of GH into the blood they could end up damaging the pituitary gland, leading to a down-regulation of its own production of GH, or even to stop GH production altogether.
GHRPsBut meanwhile, Dr. Walkers research has shown that the use of GHRPs, (growth hormone releasing peptides) have a much safer profile whilst enjoying the same benefits- even if they provide them a little more slowly. We would recommend that you read his extensive article in the Aging Matters magazine, No3, 2014 to understand fully how they operate. What we can say is that GHRPs, (GHRP2, GHRP6 and sermorelin) have the following benefits: They can be sublingually, intra-nasally and even orally, passing into blood and thus avoiding the need for needles. Their feedback loop means that they cannot cause the pituitary to down-regulate. GHRPs are not controlled substances. Rather than inducing a spike of GH in the blood, GHRPs augment (improve) each release of GH naturally into the blood, for which there are several peaks daily, (although the rising from bed peak is the highest one) - see figure 2.
SynergySermorelin is actually the precursor to GH, being the first 29 amino acids and is
applied via the sublingual route. Sermorelins function may be to release existing stores of GH from the pituitary- rather than encourage more production as a pure agonist would. Dr. Walker has highlighted that combining sermorelin with GHRP2 or GHRP6 has a highly synergistic effect, in some cases eliciting up to a 5x greater quantity of GH into blood, an action that can be equivocated to using injectable GH itself. Note: You can also hear Dr. Walker discuss this with us on the IAS video page.
DifferencesThere is no definitive answer yet as to the specific differences between GHRP2 and GHRP6; our own experiences, including information received from physicians and patients who use these products suggests the following: GHRP6 may induce more hunger feelings than GHRP2 and could improve levels of IGF-1 more. Therefore this option may be better recommend for those
who want to put on muscle mass. GHRP2 may create less hunger feelings and therefore could be preferable to those who want to stimulate GH for fat loss. Also as the GHRP6 (Releasing-Pro) is a nasal spray, those who dont like that feeling may prefer GHRP2-Pro since it is an oral liquid simply swallowed.
SummaryGHRPs have created a genuine efficacious alternative; they are simpler/ easier to use and at the same time they have a better/ safer profile than injectable GH.
A REAL OR AL ALTERNATIVE TO GH INJECTIONS
SPOTLIGHT: GHRPS
Ever since Dr. Rudmans work in the 1980s and then the release of Dr. Klatzs book
grow young with HGH in the 1990s, there has been a strong interest in the use of
growth hormone (GH) in antiaging medicine.
Figure 1 (top): The typical GH levels in blood with age, note
that geriatric levels are reached as early as during the 30s. Figure
2 (middle) shows the 24 hour profile of subcutaneous (and
also intravenous) GH. Compare that to figure 3 (bottom), the natural peaks of GH in both
young and elderly patients. Only GHRPs naturally amplify these
bioidentical patterns.
26 www.antiaging-systems.com Order hotline: 1-866-800-4677 e-mail: [email protected]
This is important because the thyroid gland is of pivotal importance to our overall health, but like the majority of hormones as we age the production of thyroid hormones decline. This lack of thyroid function is the root cause of a wide variety of age-related health disorders. Ergo, supplementation with a synthetic or a natural thyroid can have a significant positive effect on a wide range of age-related problems.
The importance of the thyroid gland
The hormones produced by the thyroid control the bodys metabolism- the rate at which it burns calories for energy. It also controls the bodys utilization of fat, so a decline in the secretion of hormones from the thyroid gland, (known as hypothyroidism) can result in wide range of symptoms such as poor concentration, confusion, memory problems, cold hands and feet and weight gain.Another serious condition which can be caused by and result from an underactive thyroid are painful musculoskeletal issues that affect tendons, muscles and ligaments.
How can I be sure if I need a thyroid supplement?
Apart from recognising the types of effects listed above, your doctor can of course get your blood levels of
thyroid checked, but another, simpler method is to take your body temperature when you wake in the morning. It should be in the range of 97.8 to 98.2 degrees Fahrenheit, if it is regularly lower you could be hypo-thyroid and if higher then hyper-thyroid.
Choosing between synthetic and natural thyroid supplements
IAS stocks a comprehensive range of both synthetic and natural thyroids, although we advocate the use of a natural supplement over a synthetic, this is because products such as Armour are of a porcine origin, so they naturally contain the full spectrum of T1, T2, T3 and T4 thyroid hormones, (note the bottles only list the amounts of T3 and T4 because very few physicians are familiar with T1 and T2).
Thyroid doses
Natural desiccated thyroids are measured in grains; with one grain being equivalent to approximately 60 mg. IAS carries doses from grain to 2 grains, with brands including Armour, ERFA and Nature. IAS also provides synthetic T3 in 20 mcg and T4 in 100 mcg tablets.
Thyroid supplements provide potent antiaging protection
Many aging individual can benefit from taking a thyroid supplement because this remarkable hormone has such a profound affect across so many different conditions. Many antiaging physicians consider thyroid support an essential part of any serious attempt to improve a persons health-span and longevity.
FOR THE HYPOTHYROID EPIDEMIC
SPOTLIGHT: THYROID SUPPORT
26 www.antiaging-systems.com Order hotline: 1-866-800-4677 e-mail: [email protected]
Dr. Broda Barnes in the 1970s estimated that 40% of the adult population was
deficient in thyroid hormones; he published this statement in his excellent book-
hypothyroidism, the unsuspected epidemic. Since then, pupils of Dr. Barnes, such as
Dr. Richard Wilkinson, have suggested that this figure could be even greater now!
Above: The position of the thyroid gland
Conversion between synthetic and natural thyroid productsThe table provided is a helpful guide to what the suggested conversion rates are
for those wishing to make the switch between synthetic thyroids and natural versions. As always we recommend consulting with a physician
before making changes to your program.
Dose of Desiccated thyroid (grains) Equivalents (mg)
Dose of T3 (lithyronine) (mcg)
Dose of T4 (levothyroxine) (mcg)
0.5 32 12.5 50
1 65 25 100
2 130 50 200
3 200 75 300
4 260 100 400
5 325 125 500
27
A former Soviet military secret!What their research uncovered - that was used for two decades on many thousands of men and women - was a remarkable link between short chain peptides and DNA. This former military secret is now available to the public as peptide bioregulators. Their published research has identified that each organ / gland / tissue uses a highly specific short chain peptide, obtained from food, to act as a short-cut to initiate protein synthesis. These peptides, unlike proteins, can enter the blood through the stomach. Through a comprehensive list of patents and even copyrighted PowerPoint slides, the Russian research group have shown that each of the concentrated
peptide bioregulators so far examined, interact with particular strands of DNA - effectively and very specifically activating repair and regenerative processes.
This is a remarkable story since what we are describing here are peptides that act as individualised gene switches. To date, they have been tested for many years on thousands of individuals, without report of any serious side effects or contraindications. We believe that they could be set to out do stem cells. Why? Because this peptide therapy is relatively cheap, highly specific, can be taken orally and doesnt require any suppression of the immune system to operate fully (as stem cells do).
Original material from the trialsThe peptide bioregulators available via IAS are the bovine originals; sourced from carefully chosen Danish calves and processed through pharmaceutical processes and filters. They are not the synthetic versions which have not been studied/ proven.
Peptide bioregulators act as they sound- to regulate; for example, Thyreogen
the thyroid peptide would increase thyroid activity if it were too low, but decrease it if it were too high!
DosingDoses are very dependent upon the need and unlike hormones these peptides do not have to be taken every day, hence making them a cost effective regime. A typical/ average use could be considered as follows:
Start with an intensive course: 2 capsules once a day for 30-days. Thereafter use 2 capsules once a day for 10-days, repeat every 2, 3, 4 or even as little as 6-months.
The story of the peptide bioregulators is a remarkable one and we recommend that you to read the articles and interviews and see the video on the IAS website.
www.antiaging-systems.com Order hotline: 1-866-800-4677 e-mail: [email protected]
THE DISCOVERY OF GENE SWITCHES IN FOOD
SPOTLIGHT: PEPTIDE BIOREGULATORS
Today Professor Vladimir Khavinson is the President of the European Academy of
Gerontology and Geriatrics, but in the 1980s he was a Colonel in the Soviet Union
military medical corps. At the time, he and his team were approached by Kremlin officials,
they wanted them to find a way to protect their troops from a myriad of problems; issues
such as radiation for submariners in nuclear submarines to troops that may be blinded
from known, (but thankfully unused) new weapons such as battlefield lasers.
PEPTIDES CURRENTLY AVAILABLE:
Cerluten is the... brain peptide bioregulator. Chelohart is the... heart peptide bioregulator.Chitomur is the... bladder peptide bioregulator.Endoluten is the... pineal peptide bioregulator. Glandokort is the... adrenal peptide bioregulator. Gotratix is the... muscle peptide bioregulato