Embed Size (px)
Citation preview
AGING AND LONG TERM CAREPART I: Overview of Aging,
Living Environments and Health Issues
Dr. Jassin M. Jouria is a medical doctor, professor of academic medicine, and medical author. He
graduated from Ross University School of Medicine and has completed his clinical clerkship training in various teaching hospitals throughout New York, including King’s County Hospital Center and Brookdale Medical Center, among others. Dr. Jouria has passed all USMLE medical board exams, and has served as a test prep tutor and instructor for Kaplan. He has developed several medical courses and curricula for a variety of educational institutions. Dr. Jouria has also served on multiple levels in the academic field including faculty member and Department Chair. Dr. Jouria continues to serves as a Subject Matter Expert for several continuing education organizations covering multiple basic medical sciences. He has also developed several continuing medical education courses covering various topics in clinical medicine. Recently, Dr. Jouria has been contracted by the University of Miami/Jackson Memorial Hospital’s Department of Surgery to develop an e-module training series for trauma patient management. Dr. Jouria is currently authoring an academic textbook on Human Anatomy & Physiology.
AbstractThe number of people over 65 years of age represented 12.4% of the population in the year 2000 but is expected to grow to be 19% by 2030. That means that 72.1 million older people will be seeking health care from a variety of sources in the next 20 years. This creates an environment in which specialists in geriatric health are highly sought after to deal with the specific and various issues that affect aging patients. These patients are highly likely to have chronic health issues that require long term care, either in a specialized facility or in the home. A proactive approach to managing older patients’ health is necessary to ensure that each patient gets the highest quality of care.
Continuing Nursing Education Course Director & Planners
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
1
William A. Cook, PhD, Director, Douglas Lawrence, MS, Webmaster,
Susan DePasquale, CGRN, MSN, FPMHNP-BC, Lead Nurse Planner
Accreditation Statement
This activity has been planned and implemented in accordance with the policies of NurseCe4Less.com and the continuing nursing education requirements of the American Nurses Credentialing Center's Commission on Accreditation for registered nurses.
Credit DesignationThis educational activity is credited for 5.5 hours. Nurses may only claim credit commensurate with the credit awarded for completion of this course activity.
Course Author & Planner Disclosure Policy StatementsIt is the policy of NurseCe4Less.com to ensure objectivity, transparency, and best practice in clinical education for all continuing nursing education (CNE) activities. All authors and course planners participating in the planning or implementation of a CNE activity are expected to disclose to course participants any relevant conflict of interest that may arise.
Statement of NeedNurses are front-line health professionals for the elderly. Planning for long-term care requires nurses to have the appropriate education to support the elderly and their families.
Course PurposeTo provide nursing professionals with knowledge in the area of long-term care of the elderly.Learning Objectives
1. Identify the most common housing scenarios for the elderly.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
2
2. Describe the best practices of communicating with the elderly.3. List common geriatric syndromes and disorders.4. Describe the impact and treatment of dysphagia.5. Describe the causes and treatment of malnutrition on elderly.6. Describe the emotional burden of chronic illness on the elderly.7. Discuss the importance of education about fall risks for elderly.
Target AudienceAdvanced Practice Registered Nurses, Registered Nurses and Licensed Practical Nurses and Associates
Course Author & Director Disclosures Jassin M. Jouria, MD, William S. Cook, PhD, Douglas Lawrence,
Susan DePasquale, CGRN, MSN, FPMHNP-BC – all have no disclosures
Acknowledgement of Commercial Support:
There is no commercial support for this course.
Activity Review Information:
Reviewed by Susan DePasquale, CGRN, MSN, FPMHNP-BC
Release Date: 1/1/2015 Termination Date: 6/25/2016
Please take time to complete the self-assessment Knowledge Questions before reading the article. Opportunity to complete a self-assessment of knowledge
learned will be provided at the end of the course
1. In the U.S., most elderly long-term care is provided by:a. Medicareb. Medicaidc. Family, relatives and friends
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
3
d. None of the above
2. Older age is associated with an increased prevalence of:a. chronic diseases and sensory dysfunctionb. changes in cognition c. poor balance and increased rate of falls and injuriesd. all of the above
3. True or False. Impaired cognition in the elderly has no correlation to the ability or desire to eat.a. Trueb. False
4. Elderly individuals with pneumonia frequently experience:a. more symptoms than young adultsb. aspiration pneumonia detected late, and under-diagnosedc. tachypnea or increased respiratory rate as an early sign d. answers b and c above
5. To evaluate the older adult for malnutrition, a helpful mnemonic is: a. M-E-A-L-S-O-N-W-H-E-E-L-Sb. G-O-O-D-N-U-T-R-I-T-I-O-Nc. D-I-E-T-F-O-R-L-I-F-Ed. E-L-D-E-R-W-E-L-L-N-E-S-S
6. Basic laboratory work-up for the elderly includes:a. CMP, sedimentation rate and CRPb. complete blood count, CMP, thyroid panelc. thyroid profile, liver function test, cardiac enzymesd. Genetic testing to determine medication efficacy
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
4
7. Most common conditions associated with anemia in the elderly include: a. Iron deficiency anemia b. Vitamin B12 and folate deficiencyc. Hypercalcemiad. Answers a and b above
8. Treatment of vitamin B12 deficiency includes:a. 1000 IU of vitamin B12 orally dailyb. 500 IU of vitamin B12 orally/injections every other dayc. 1000 IU of vitamin B12 injections weekly for 4 weeksd. answers a and c above
9. True or False. Dysphagia management in the elderly also help in the management of malnutrition and pneumonia.a. Trueb. False
10. True or False. Falls in the elderly include factors related to seizure, sudden onset of paralysis, or an external force.a. Trueb. False
Introduction
The United States is the third most populous country and constitutes approximately 4.5% of the total world population. Currently, the U.S. population is about 308.7 million persons and has increased two fold since 1950. In addition, the population is now qualitatively different from what it was in 1950. The Population Reference Bureau reports that the U.S. is getting bigger, older, and more diverse. In the coming
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
5
decades, specifically between 2010 and 2050, the U.S. is expected to see a rapid growth in its older population. In 2050, it is expected that the total population of U.S. citizens aged 65 and older will reach 88.5 million, which is more than two fold its population in 2010. Between 2010 and 2050, the 65+ population is expected to roughly double. Approximately one in five individuals will belong to this age group in 2050; currently this rate hovers around 1 in 7.7 individuals.
This growth in elderly population will far exceed the growth in younger age groups or categories. In the same period, the total number of people in the 85+ age group (oldest adults) will witness a far more rapid growth than the growth of older adults 65+. The 85+ population will increase three fold from 5.8 million in 2010 to approximately 19 million in 2050. This surge in the elderly population will have far reaching implications. As the U.S. ages, the demand for long-term care for the elderly will increase dramatically and their need for health services is expected to also grow. Currently, more than 6 million elderly in the U.S. require some kind of long-term care, with about a third of these requiring more substantial care.
Families, relatives and friends provide most long-term care for the elderly in the U.S. Currently, Medicare finances medical care for almost all the elderly in the total population. However, support for long-term care is often beyond the scope of Medicare. Medicaid is a state program supported by the federal government and provides long-term care financing for low-income families. However, long-term care for the elderly continues to be a major challenge for the country. Elderly who require long-term care often do not receive the quality or amount of care they may wish, need or prefer. In addition, the financial burdens on the society and the family are often quite heavy.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
6
Society and healthcare providers face a huge problem and dissatisfaction in terms of quality, scope, and financing of long-term care services. Despite a consistent growth in home-care services, nursing homes continue to dominate the long-term care services system, and the government is still struggling to manage its social and financial resources. Changing demographics in the U.S. pose a further challenge. It is estimated that the demand for long-term care among the elderly will increase to more than double in the next three decades.1 This exponential growth further exacerbates concerns about long term care for elderly. The key variables required to address this problem are institutional and non-institutional elderly care, quality of care, integration of acute and long-term care, and the adoption of sustainable financing strategies for those who require long-term care. As the population of elderly increases, questions surrounding long-term care will increasingly shape the quality of life for aging community members.
Future Projections
Approximately 10 million out of the county’s 26.2 million older households have at least one family member with a disability. It has been observed that the rates of disability increase with age. In 2007, approximately four percent of the 65+ Medicare population utilized long-term care facilities such as nursing homes. Another two percent lived in community housing. However, the picture changes drastically among the oldest adults. Among people in the 85 and older category, in 2007, approximately seven percent lived in community housing and about 15 percent resided in long-term care facilities.1
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
7

Older age is also associated with an increased prevalence of chronic diseases1 and sensory dysfunction,2 changes in cognition,3 poor balance,4 increased rate of falls, fall-related injuries, and death.4,5 In addition, physical activity and community engagement declines in the elderly. This also leads to overall declines in health.5 These age-related changes may substantially impact the healthcare and long-term care in the coming decades because the use of health-related services and long term care is strongly correlated to increasing age, as outlined below.6
FUTURE PROJECTIONS FOR THE ELDERLY POPULATION IN THE U.S.
The number of US citizens who require long-term care will jump from approximately 12 million today to 27 million in 2050.7
Baby boomers will start turning 65 between 2011 and 2029.8 During this period, 10,000 Americans will turn 65 every day.9
By 2030, the number of Americans in the age group of 65 and older will be approximately 72 million, or approximately 19% of the total U.S. population (up from over 40 million or 13% in 2010).10
By 2050, the number of elderly Americans will jump to almost 89 million, which constitutes approximately 20% of the total US population.
The percentage of the U.S. population that is age 85 and older will increase by more than 25% by 2030 and by 126% by 2050.10
From 2010 to 2030, Alaska (+217%), Nevada (+147%), Arizona (+119%) will witness highest population growth of those age 85 and older.
Life expectancy in the US has increased significantly over the last century and will continue to increase. An individual born in 2010 has an average life expectancy of 79 years, compared to almost 52 years in 1910.11,12
Life expectancy is higher for women than men. For those born in 2010, projected life expectancy for women is about 81 years, compared to 76 years for men.11
Between 2000 and 2030 the number of Americans with chronic disease or conditions will increase by approximately 37%, an addition of 46 million people.12 Twenty-seven million individuals with chronic diseases or conditions in the U.S. population will also experience functional
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
8
impairment.13,14 As of 2012, there are 5.2 million people age 65 and older who have been
diagnosed Alzheimer’s disease. By 2025, the number of people age 65 and older with Alzheimer’s disease is estimated to increase by 30% to 6.7 million. By 2050, this number may witness a three-fold increase to approximately 11 million to 16 million.15
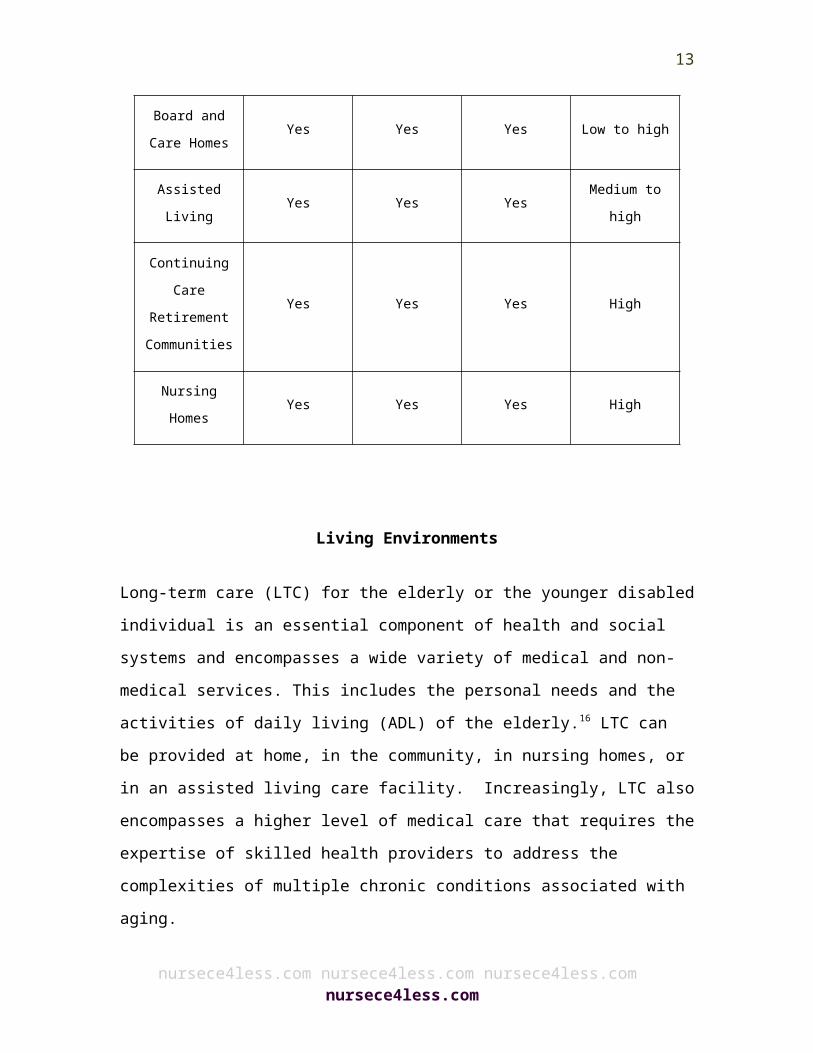
By 2020, approximately 12 million elderly will need long-term care. The majority of these people, about 70%, will be provided care at home by their family and friends. A recent study has reported that elderly have a 40 percent chance of entering a nursing home.15 Approximately 10 percent of those nursing home residents will stay there for five years or more. The cost of long-term care may vary depending on the type of care, location of the provider, and location of the elderly. The table below compares the different long-term care services.
Help with activities of daily living
Help with additional services
Help with care needs
Range of costs
Community-Based
ServicesYes Yes No
Low to medium
Home Health Care
Yes Yes Yes Low to high
In-Law Apartments
Yes Yes Yes Low to high
Housing for Aging and Disabled
Yes Yes No Low to high
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
9
Individuals
Board and Care Homes
Yes Yes Yes Low to high
Assisted Living
Yes Yes YesMedium to
high
Continuing Care
Retirement Communities
Yes Yes Yes High
Nursing Homes
Yes Yes Yes High
Living Environments
Long-term care (LTC) for the elderly or the younger disabled individual is an essential component of health and social systems and encompasses a wide variety of medical and non-medical services. This includes the personal needs and the activities of daily living (ADL) of the elderly.16 LTC can be provided at home, in the community, in nursing homes, or in an assisted living care facility. Increasingly, LTC also encompasses a higher level of medical care that requires the expertise of skilled health providers to address the complexities of multiple chronic conditions associated with aging.
The need for LTC is impacted by changes in the physical, mental, and/or cognitive functional capacities of the elderly, which in turn are greatly influenced by the environment. The type and duration of LTC involve complex issues and decision-making, and are usually difficult
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
10
to predict. The goal of LTC is to make sure that an elder who is not fully capable of long-term self-care can maintain the highest possible quality of life, with the high degree of independence, participation, autonomy, individual fulfillment, and dignity.
Appropriate and adequate LTC includes respect for individual’s values, wishes, needs and preferences. Elderly who need home-based LTC may also require other services, such as physical or mental health care and rehabilitation, together with social financial and legal support. LTC may be provided formally or informally. Facilities that provide formal LTC services usually make provisions for living accommodation for those elderly who need round-the-clock supervised care, which may include professional healthcare services, personal care and services such as housekeeping, meals and laundry.17 Such formal LTC services are provided by such facilities as a nursing home, residential continuing care facility, personal care facility.
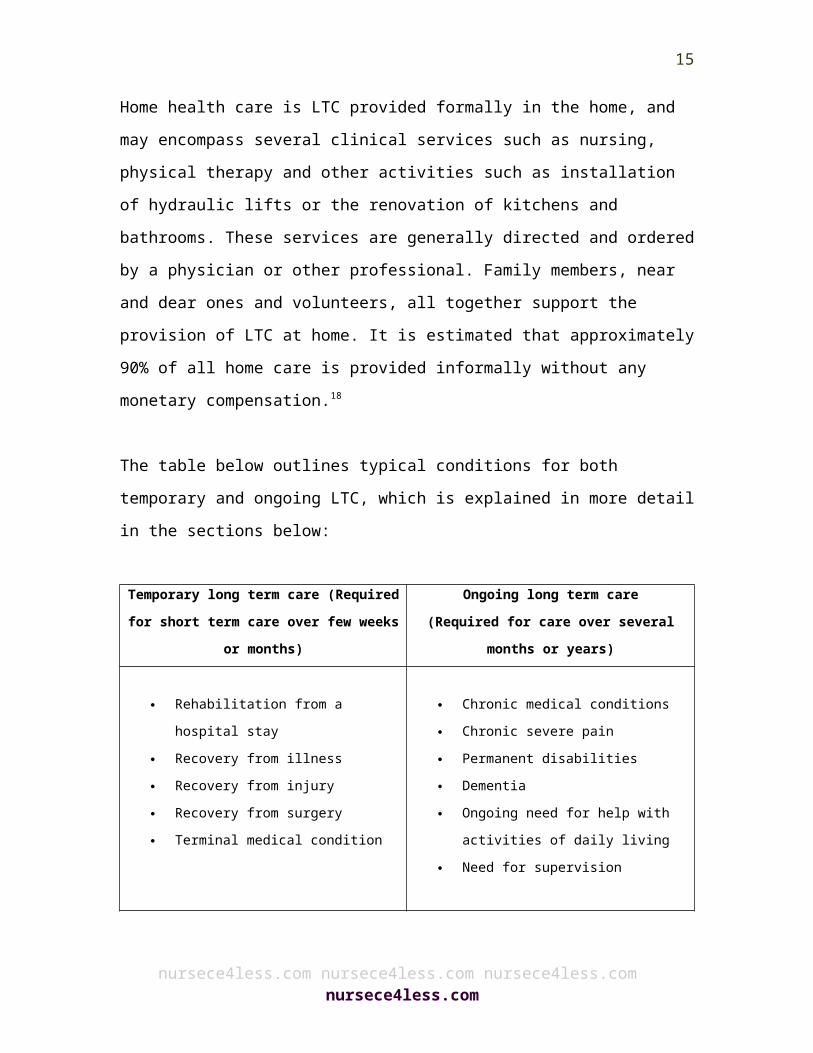
Home health care is LTC provided formally in the home, and may encompass several clinical services such as nursing, physical therapy and other activities such as installation of hydraulic lifts or the renovation of kitchens and bathrooms. These services are generally directed and ordered by a physician or other professional. Family members, near and dear ones and volunteers, all together support the provision of LTC at home. It is estimated that approximately 90% of all home care is provided informally without any monetary compensation.18
The table below outlines typical conditions for both temporary and ongoing LTC, which is explained in more detail in the sections below:
Temporary long term care Ongoing long term care
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
11

(Required for short term care over few weeks or months)
(Required for care over several months or years)
Rehabilitation from a hospital stay
Recovery from illness Recovery from injury Recovery from surgery Terminal medical condition
Chronic medical conditions Chronic severe pain Permanent disabilities Dementia Ongoing need for help with
activities of daily living Need for supervision
Services from Unpaid Caregivers
Home-based LTC encompasses health, personal, and other types of support services to help the elderly stay at home and live as independently as possible. This type of care is usually provided either in their own home or at a family member's home. In-home services can be short-term or long-term depending on the condition of an individual. For example, an individual may need these services postoperatively for few days (short term) to adequately recover from an operation. On the other hand, an individual may require ongoing in-home services for a longer term. The majority of home-based services provide personal care, such as help with activities of daily living, i.e., bathing, dressing, etc. These services are often also provided free of cost by immediate family members, friends, partners, and neighbors. Such informal care is the dominant form of care for elderly in the U.S. as well as throughout the world, despite the immense burdens that it places on the provider.
Services from Paid CaregiversTrained paid caregivers are also available for home-based LTC services. Health care professionals including nurses, home health care
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
12
aides, and therapists may provide these services. These paid services may also be provided by:
Home health care workers Friendly visitor/companion services Homemaker services Emergency response systems.
Home health care
These services may include nursing care to help an individual recover from surgery, an injury, or illness. It usually involves part-time medical services advised by a physician for a particular event or condition. Home health care may also provide different types of therapies including physical, occupational, or speech therapy. If required, provisions can also be made for temporary home health aide services.
Homemaker services
Homemaker services can be utilized without a physician's recommendation. Personal care includes help with activities of daily living such bathing, grooming and dressing. These services also provide help for meal preparation and simple household chores. These agencies do not need to be approved by Medicare to provide their services.
Friendly visitor or companion services
Volunteers usually offer friendly visitor or companion services from the community. These include regularly (paying) short visits to elderly people who live alone and are too weak to take care of themselves.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
13
Emergency response systems
These advanced systems automatically respond to medical and other emergencies with the help of electronic monitors and other resources. This type of service is particularly helpful for those who live alone or who are at risk for falls. This is a paid service.
The outline below summarizes criteria for care generally needed leading to the implementation of home-based LTC:
ELEMENTS OF HOME-BASED LONG-TERM CARE
Assessment, monitoring, and reassessment Health promotion, health protection, disease prevention, postponement of
disability Facilitation of self-care, self-help, mutual aid, and advocacy Health care, including medical and nursing care Personal care, i.e. grooming, bathing, meals Household assistance, i.e. cleaning, laundry, shopping Physical adaptation of the home to meet the needs of disabled individuals Referral and linkage to community resources Community-based rehabilitation Provision of supplies (basic and specialized), assistive devices and
equipment (i.e. hearing aids, walking frames), and drugs Alternative therapies and traditional healing Specialized support (i.e. for incontinence, dementia and other mental
problems, substance abuse) Respite care (at home or in a group setting) Palliative care, i.e. management of pain and other symptoms Provision of information to patient, family, and social networks Counseling and emotional support Facilitation of social interaction and development of informal networks Development of voluntary work and provision of volunteer opportunities to
clients
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
14
Productive activities and recreation Opportunities for physical activities Education and training of clients and of informal and formal caregivers Support for caregivers before, during, and after periods of caregiving Preparation and mobilization of society and the community for caring roles
Nursing Home CareNursing homes provide a comprehensive range of medical services, which includes 24-hour supervision and nursing care. More than 1.5 million elderly in the have spent time in a nursing home, and around one of two nursing home residents need assistance with all activities of daily living.19 By, 2050, the total number of US citizens requiring LTC is expected to increase two-fold.19 Nursing homes may vary in size and scope of services. They may offer short-term care, post hospitalization rehabilitation and hospice care.
The majority of nursing homes employ community physicians to provide care. The principal goal of nursing home care is to maximize resident autonomy, function, dignity, and comfort. Nursing homes also provide a sense of community where elderly can do social activities and make social bonds with other people. Care in a nursing home includes several different levels of care. These are further explained below.
Skilled Nursing Care This type of care is provided on a physician’s recommendation and requires the professional skills of a registered nurse or a licensed practical nurse. It is offered either directly by or under the supervision of a registered nurse.
Intermediate Nursing Care
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
15
This care is provided under periodic medical supervision and encompasses physical, psychological, social, and other restorative services. This nursing care is provided by a skilled registered nurse and includes the observation and the recording of signs and symptoms.
Personal or Custodial Care Individuals without medical training can offer this type of care. The main goal of custodial care is to meet the personal needs of the elderly, including feeding and personal hygiene.
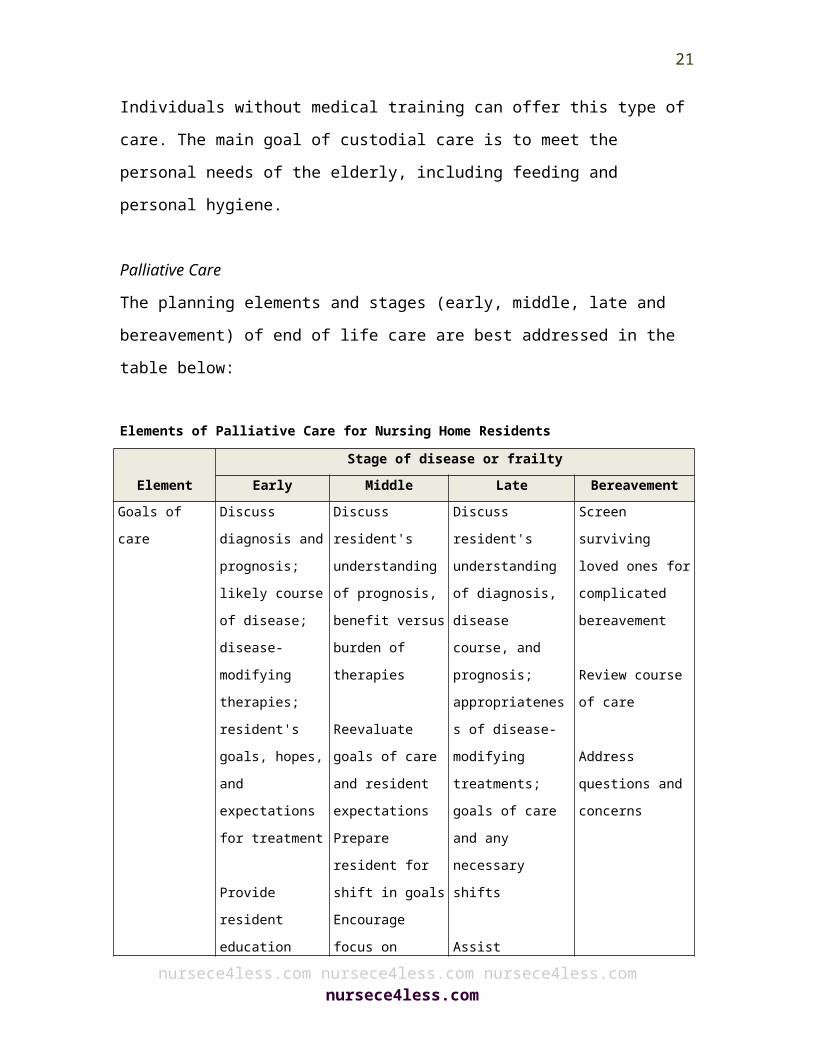
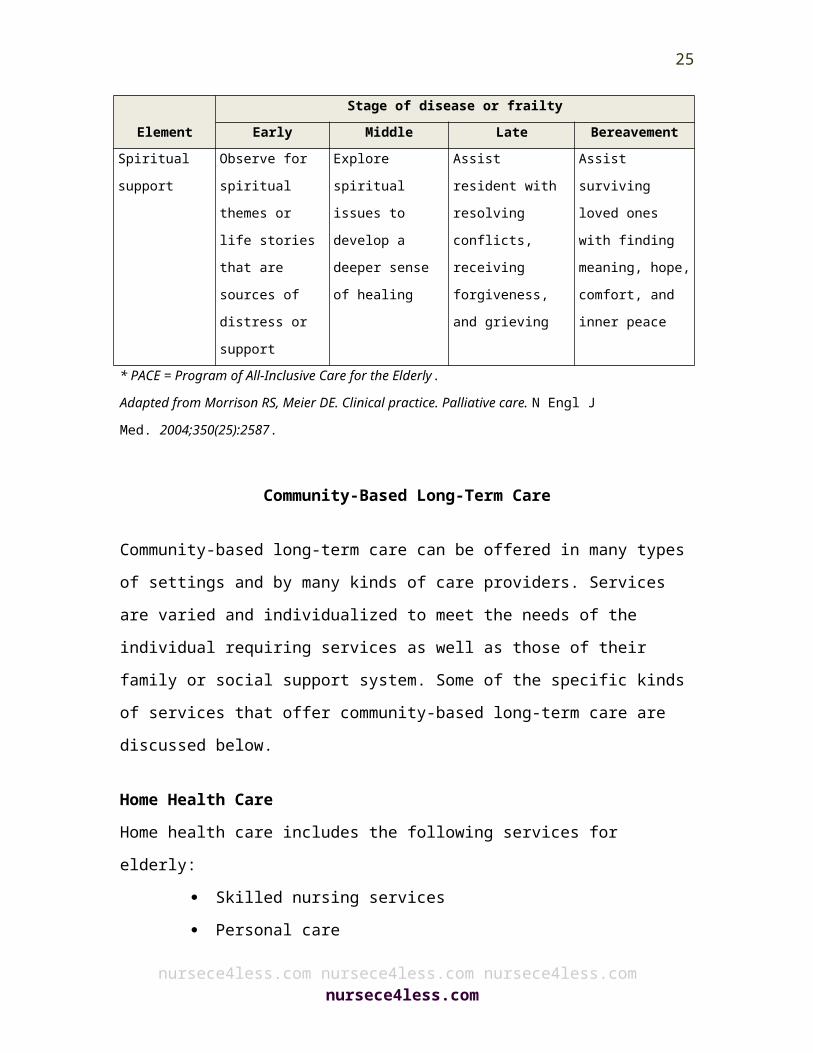
Palliative CareThe planning elements and stages (early, middle, late and bereavement) of end of life care are best addressed in the table below:
Elements of Palliative Care for Nursing Home Residents
ElementStage of disease or frailty
Early Middle Late BereavementGoals of care Discuss
diagnosis and prognosis; likely course of disease; disease-modifying therapies; resident's goals, hopes, and expectations for treatment
Provide resident
Discuss resident's understanding of prognosis, benefit versus burden of therapies
Reevaluate goals of care and resident expectations Prepare resident for shift in goals Encourage focus on important
Discuss resident's understanding of diagnosis, disease course, and prognosis; appropriateness of disease-modifying treatments; goals of care and any necessary shifts
Assist resident in planning for a
Screen surviving loved ones for complicated bereavement
Review course of care
Address questions and concerns
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
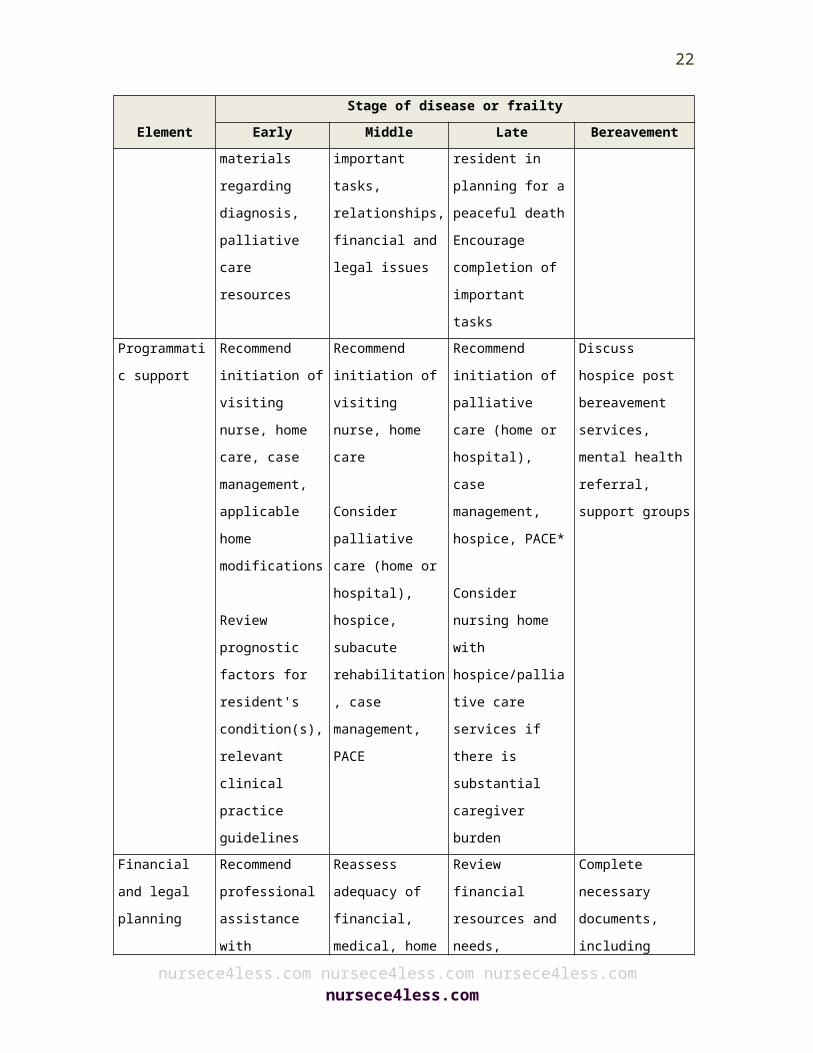
16
ElementStage of disease or frailty
Early Middle Late Bereavementeducation materials regarding diagnosis, palliative care resources
tasks, relationships, financial and legal issues
peaceful deathEncourage completion of important tasks
Programmatic support
Recommend initiation of visiting nurse, home care, case management, applicable home modifications
Review prognostic factors for resident's condition(s), relevant clinical practice guidelines
Recommend initiation of visiting nurse, home care
Consider palliative care (home or hospital), hospice, subacute rehabilitation, case management, PACE
Recommend initiation of palliative care (home or hospital), case management, hospice, PACE*
Consider nursing home with hospice/palliative care services if there is substantial caregiver burden
Discuss hospice post bereavement services, mental health referral, support groups
Financial and legal planning
Recommend professional assistance with financial planning, long-term care, future insurance needs; legal counsel with expertise in
Reassess adequacy of financial, medical, home care, and family support; long-term care planning
Consider hospice referral,
Review financial resources and needs, financial options for personal and long-term care (including hospice and Medicaid if resources are inadequate for
Complete necessary documents, including death certificate
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
17
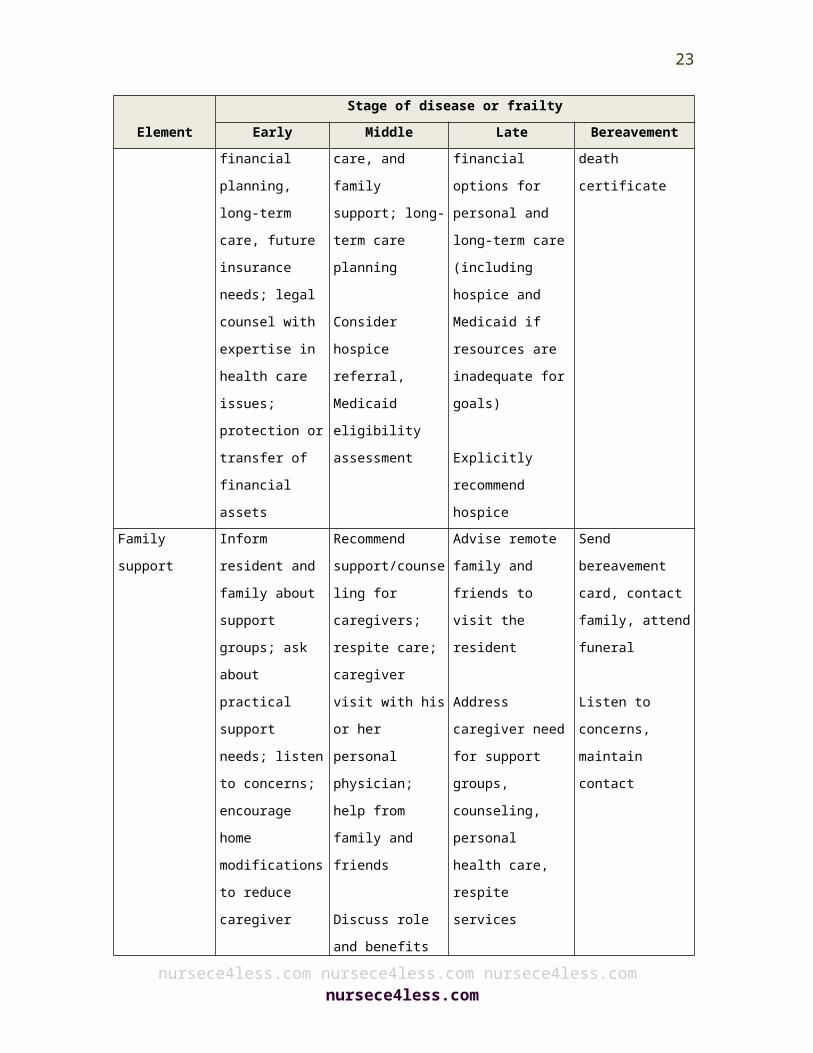
ElementStage of disease or frailty
Early Middle Late Bereavementhealth care issues; protection or transfer of financial assets
Medicaid eligibility assessment
goals)
Explicitly recommend hospice
Family support
Inform resident and family about support groups; ask about practical support needs; listen to concerns; encourage home modifications to reduce caregiver burden
Provide resident education materials regarding diagnosis, as well as general caregiver tasks and support
Recommend support/counseling for caregivers; respite care; caregiver visit with his or her personal physician; help from family and friends
Discuss role and benefits of hospice care
Provide dialogue for caregiver concerns and needs; information on practical resources, stress, depression, and adequacy of care
Advise remote family and friends to visit the resident
Address caregiver need for support groups, counseling, personal health care, respite services
Send bereavement card, contact family, attend funeral
Listen to concerns, maintain contact
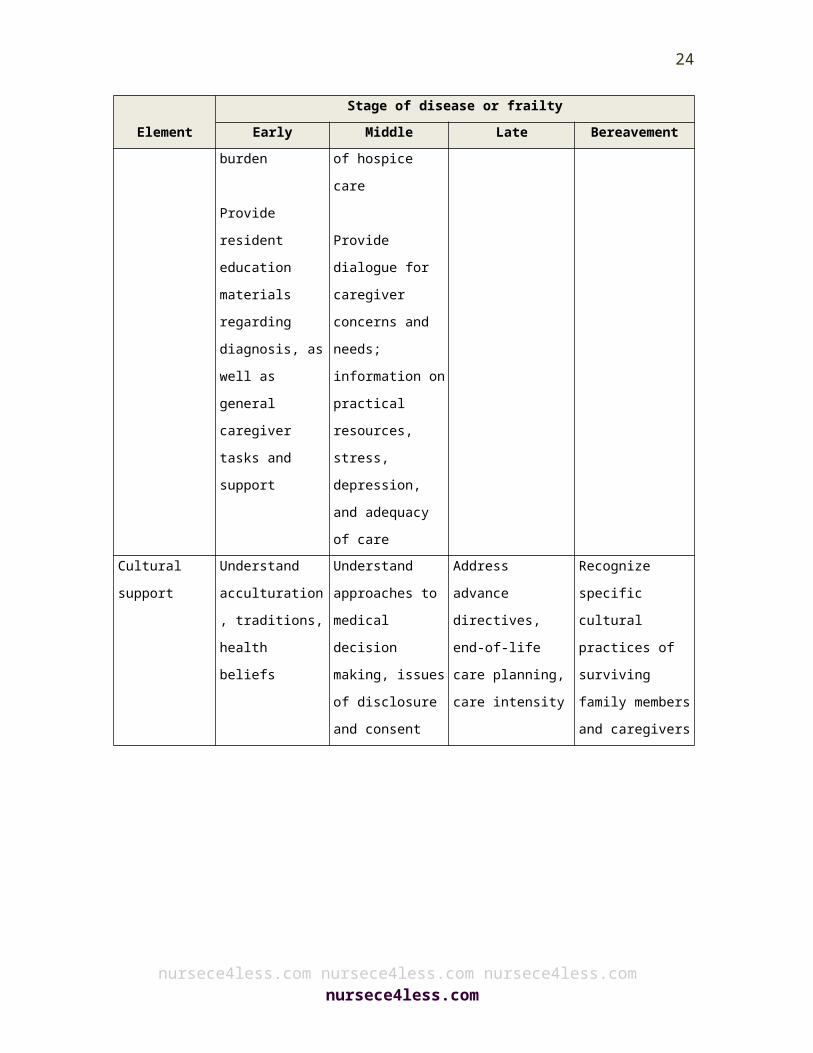
Cultural support
Understand acculturation, traditions,
Understand approaches to medical decision
Address advance directives, end-of-life care
Recognize specific cultural practices of
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
18
ElementStage of disease or frailty
Early Middle Late Bereavementhealth beliefs making, issues
of disclosure and consent
planning, care intensity
surviving family members and caregivers
Spiritual support
Observe for spiritual themes or life stories that are sources of distress or support
Explore spiritual issues to develop a deeper sense of healing
Assist resident with resolving conflicts, receiving forgiveness, and grieving
Assist surviving loved ones with finding meaning, hope, comfort, and inner peace
* PACE = Program of All-Inclusive Care for the Elderly.Adapted from Morrison RS, Meier DE. Clinical practice. Palliative care. N Engl J Med. 2004;350(25):2587.
Community-Based Long-Term Care
Community-based long-term care can be offered in many types of settings and by many kinds of care providers. Services are varied and individualized to meet the needs of the individual requiring services as well as those of their family or social support system. Some of the specific kinds of services that offer community-based long-term care are discussed below.
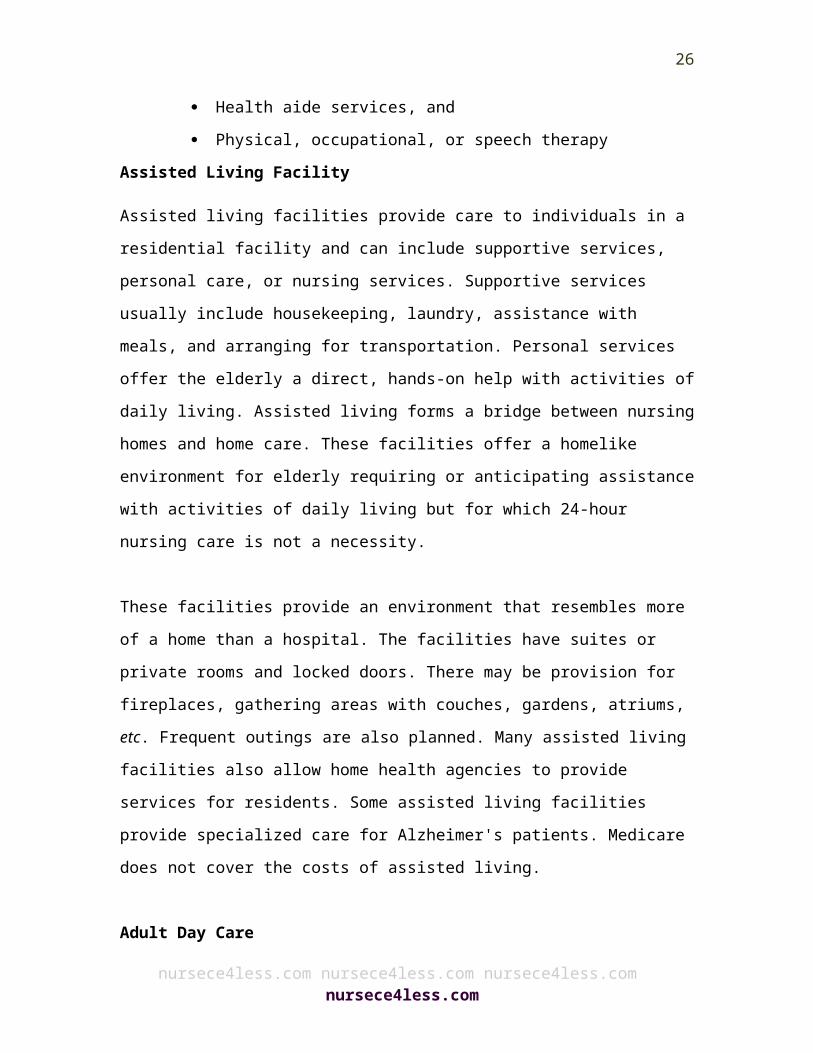
Home Health Care Home health care includes the following services for elderly:
Skilled nursing services Personal care Health aide services, and Physical, occupational, or speech therapy
Assisted Living Facility
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
19
Assisted living facilities provide care to individuals in a residential facility and can include supportive services, personal care, or nursing services. Supportive services usually include housekeeping, laundry, assistance with meals, and arranging for transportation. Personal services offer the elderly a direct, hands-on help with activities of daily living. Assisted living forms a bridge between nursing homes and home care. These facilities offer a homelike environment for elderly requiring or anticipating assistance with activities of daily living but for which 24-hour nursing care is not a necessity.
These facilities provide an environment that resembles more of a home than a hospital. The facilities have suites or private rooms and locked doors. There may be provision for fireplaces, gathering areas with couches, gardens, atriums, etc. Frequent outings are also planned. Many assisted living facilities also allow home health agencies to provide services for residents. Some assisted living facilities provide specialized care for Alzheimer's patients. Medicare does not cover the costs of assisted living.
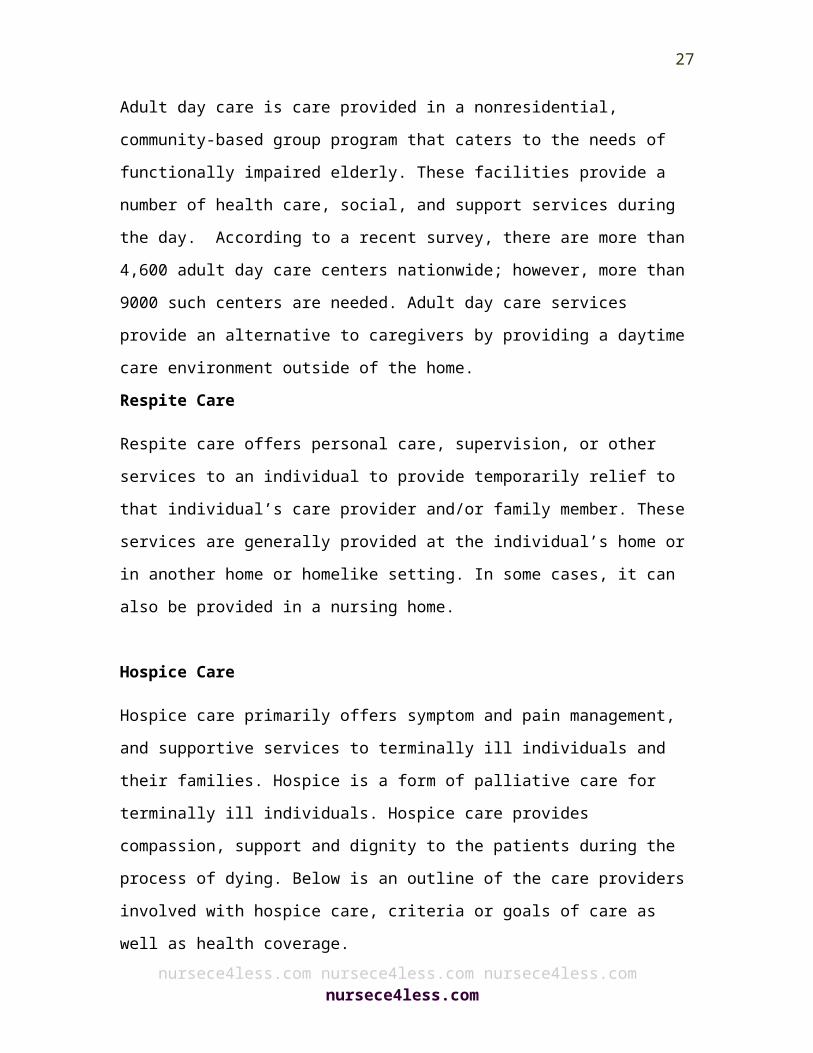
Adult Day Care
Adult day care is care provided in a nonresidential, community-based group program that caters to the needs of functionally impaired elderly. These facilities provide a number of health care, social, and support services during the day. According to a recent survey, there are more than 4,600 adult day care centers nationwide; however, more than 9000 such centers are needed. Adult day care services provide an alternative to caregivers by providing a daytime care environment outside of the home. Respite Care
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
20
Respite care offers personal care, supervision, or other services to an individual to provide temporarily relief to that individual’s care provider and/or family member. These services are generally provided at the individual’s home or in another home or homelike setting. In some cases, it can also be provided in a nursing home.
Hospice Care
Hospice care primarily offers symptom and pain management, and supportive services to terminally ill individuals and their families. Hospice is a form of palliative care for terminally ill individuals. Hospice care provides compassion, support and dignity to the patients during the process of dying. Below is an outline of the care providers involved with hospice care, criteria or goals of care as well as health coverage.
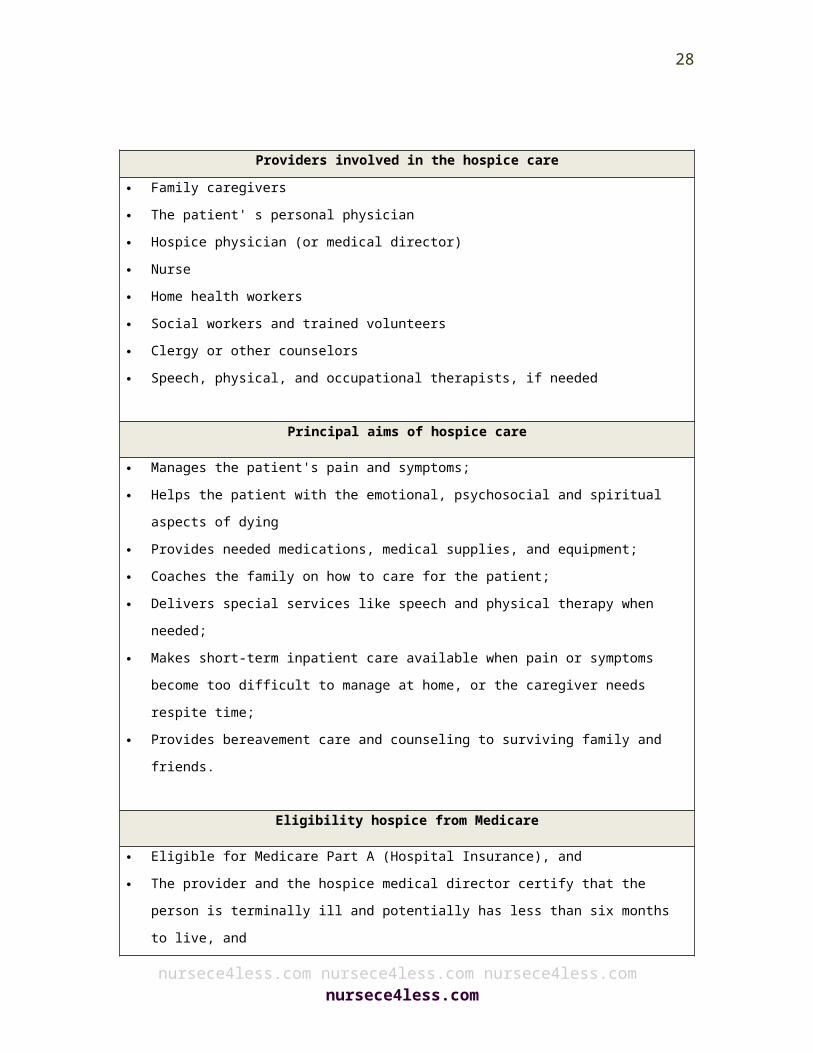
Providers involved in the hospice care
Family caregivers The patient' s personal physician Hospice physician (or medical director) Nurse Home health workers Social workers and trained volunteers Clergy or other counselors Speech, physical, and occupational therapists, if needed
Principal aims of hospice care
Manages the patient's pain and symptoms; Helps the patient with the emotional, psychosocial and spiritual aspects of
dying Provides needed medications, medical supplies, and equipment; Coaches the family on how to care for the patient; Delivers special services like speech and physical therapy when needed; Makes short-term inpatient care available when pain or symptoms become too
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
21
difficult to manage at home, or the caregiver needs respite time; Provides bereavement care and counseling to surviving family and friends.
Eligibility hospice from Medicare
Eligible for Medicare Part A (Hospital Insurance), and The provider and the hospice medical director certify that the person is
terminally ill and potentially has less than six months to live, and The person or a family member signs a statement choosing hospice care
instead of routine Medicare covered benefits for the terminal illness, and Care is received from a Medicare-approved hospice program.
Eligibility for Hospice
Common terminal conditions and the medical criteria are indicative of advanced illness. Patients are eligible for hospice only if all of the following conditions are satisfied.
Attending physician certifies that patient has a terminal condition with an expected life span of 6 months or less.
Patient decides to forego life-prolonging therapies. The patient does not have to be a DNR to be eligible for hospice.
No home hospice can refuse to admit a patient just because she/he opts to remain a “full code”.
However, this could potentially represent a red flag with regard to a full understanding of the focus of hospice care on symptom management as opposed to curative disease modifying treatment. This should be fully explained to the patient and fully documented. As an example, patients with advanced congestive heart failure (CHF) should remain on their ACE inhibitor and diuretics as tolerated because these treatments are considered palliative and help control many symptoms.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
22
These treatments may be life prolonging, but in a hospice setting they are understood to be primarily palliative.
Hospice care diagnoses can include:
Advanced End Stage Senescence or Debility Cancer Amyotrophic Lateral Sclerosis (ALS) Liver Disease Pulmonary Disease Dementia HIV Stroke and Coma
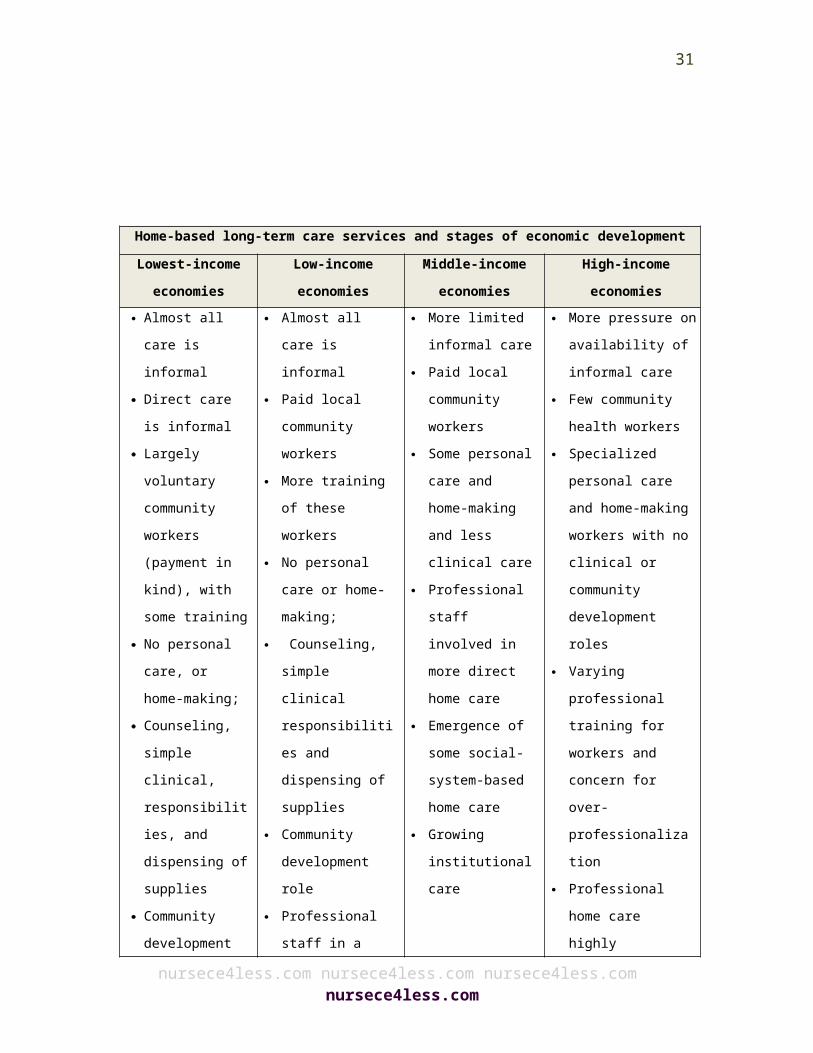
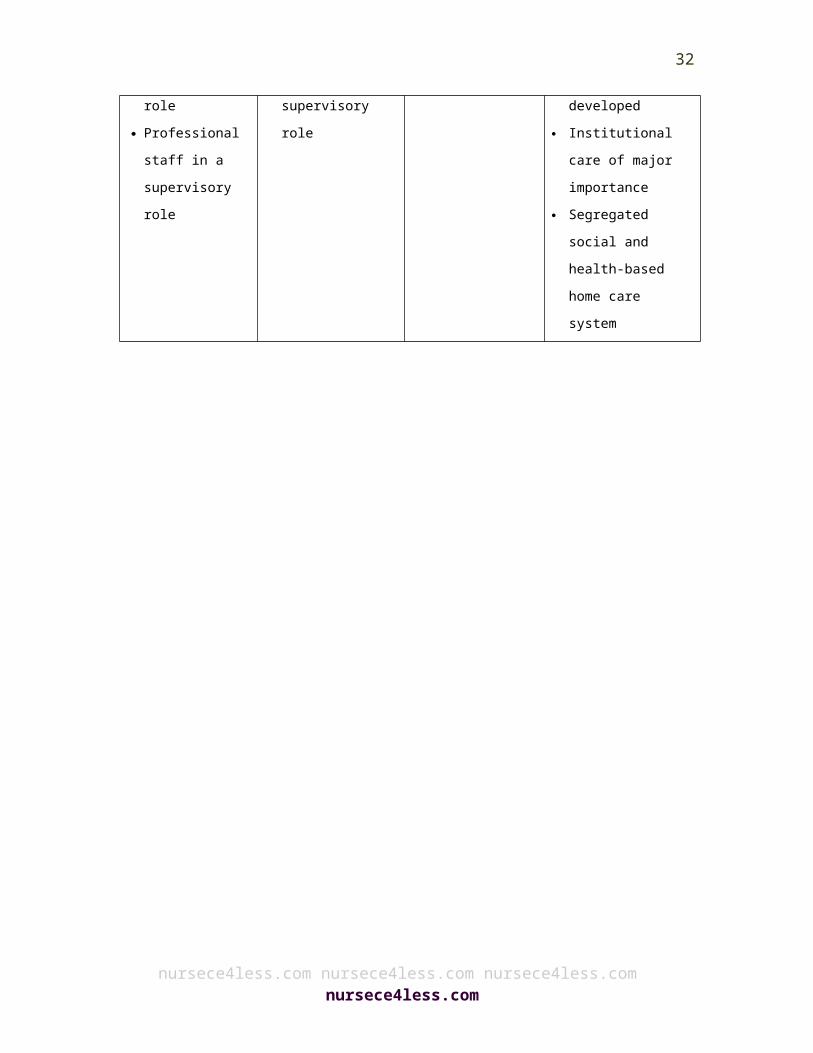
Patterns of development of home-based long-term care services at different stages of economic development are outlined below, ranging from lowest, low, middle and high income categories.
Home-based long-term care services and stages of economic developmentLowest-income
economiesLow-income economies
Middle-income economies
High-income economies
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
23
Almost all care is informal
Direct care is informal
Largely voluntary community workers (payment in kind), with some training
No personal care, or home-making;
Counseling, simple clinical, responsibilities, and dispensing of supplies
Community development role
Professional staff in a supervisory role
Almost all care is informal
Paid local community workers
More training of these workers
No personal care or home-making;
Counseling, simple clinical responsibilities and dispensing of supplies
Community development role
Professional staff in a supervisory role
More limited informal care
Paid local community workers
Some personal care and home-making and less clinical care
Professional staff involved in more direct home care
Emergence of some social-system-based home care
Growing institutional care
More pressure on availability of informal care
Few community health workers
Specialized personal care and home-making workers with no clinical or community development roles
Varying professional training for workers and concern for over-professionalization
Professional home care highly developed
Institutional care of major importance
Segregated social and health-based home care system
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
24
Long-Term Care Hospitals
Long-term care hospitals (LTCHs) account for a small percentage of total Medicare spending, but have been growing for the last few years. These are acute care hospitals, which also focus on providing care to patients who stay in the facility for more than 25 days. These hospitals offer specialized treatment to patients who may have several co-morbidities, but with a relatively good prognosis assuming adequate medical treatment and supervised care. Some patients are transferred from the intensive or critical care units of the hospital. LTCHs offer a comprehensive rehabilitation program, respiratory therapy, pain relief and management and head trauma management.
Malnutrition in the Elderly
An aging population is one of the biggest social changes that have occurred in the last few decades and is primarily due to improved standards of living. By 2050, it is estimated that the elderly will outnumber children under the age of 14 years.20 Globally and in the U.S., the elderly population is very diverse, ranging from very healthy, active and fit independent individuals, to very weak, frail and dependent older people with chronic disease and varying degrees of disabilities.
Currently approximately 13% of the US population is over 65 years old. This is expected to increase to about 20% by 2050. Globally, the elderly population will also increase dramatically in the next 30 years.21
Today, it is estimated that approximately two thirds of general and acute hospital beds are occupied by individuals over 65 years of age, and those over 75 years occupy the beds for longer times.22 The elderly bear an increased burden of disease that also affects their
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
25
nutritional status. In addition, as people age, they experience changes in body composition and metabolism that also affect nutritional status.
Body composition of elderly people
Fat mass increases till about 75 years of age, and then remains stable or decreases.23-25 In addition, it is believed that central fat accumulation increases with aging, while appendicular fat mass decreases.23-26 Several studies have linked this pattern of fat distribution to an increased risk of diabetes, stroke, hyperlipidemia, cardiac disease, and hypertension,27 and all of these conditions are commonly seen in the elderly population.
Fat free mass (FFM) decreases with age, and generally starts declining around 40–50 years of age.23,24,28,29 This loss accelerates further due to a reduction in skeletal muscle, and bone mineral density, particularly in older women. Several studies have shown that even a 10% loss of lean tissue in previously healthy people can lead to poor immunity, increased susceptibility to infections, and subsequently increased mortality.30,31 Therefore, elderly with greater FFM loss are prone to various types of disease and infections.
Etiology of weight loss
Weight loss in elderly can be categorized into three distinct types: Wasting:
Wasting is an involuntary weight loss predominantly caused by inadequate dietary intake. Chronic disease and psychosocial factors play an important role. Wasting in elderly may be seen with a background of cachexia, sarcopenia or both.
Cachexia:
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
26
Cachexia is an involuntary loss of free fat mass (FFM) or body cell mass (BCM), which is caused by increased catabolism, and increased protein degradation leading to changes in the body composition. However, weight loss may not be present in the beginning.
Cachexia is observed in several chronic diseases such as congestive heart failure, rheumatoid arthritis, HIV infection, and cancer, and also in conditions associated with metabolic stress such as trauma, decubitus ulcers and infections. Concentrations of certain cytokines, i.e. interleukin 1 (IL1), tumor necrosis factor a (TNFa) and IL6 are higher than normal in patients with cachexia and weight loss.32
Sarcopenia: Sarcopenia is an involuntary loss of muscle mass, which is primarily due to aging and not the effect of age associated chronic or co-morbid diseases. Hormonal, neural, and cytokine activity with lack of physical activity play an important role in the development of sarcopenia.
A recent study has observed that inflammatory cytokines TNFa and IL1b prevent the development of functional muscle fibers.17
Comparison of the characteristics of undernutrition due to anorexia, cachexia and sarcopenia are shown in the table below.
Anorexia Cachexia SarcopeniaAnorexia + ++ −
Weight loss + ++ +/−
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
27
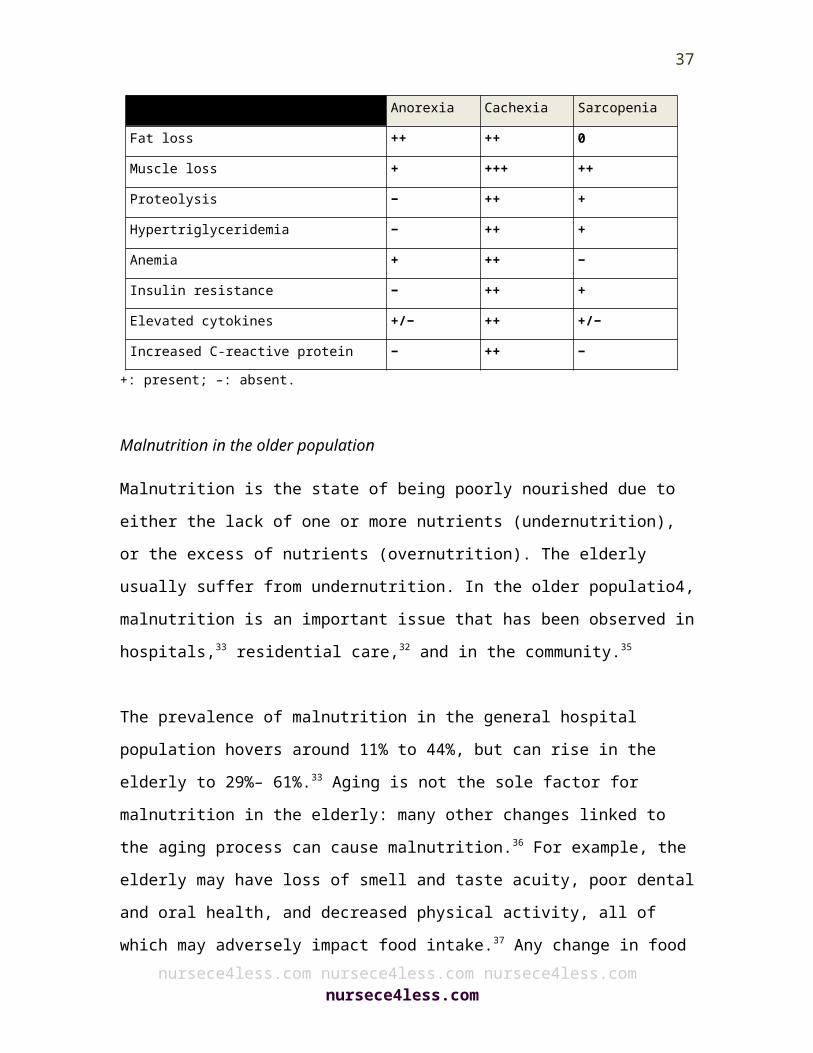
Anorexia Cachexia Sarcopenia
Fat loss ++ ++ 0
Muscle loss + +++ ++
Proteolysis − ++ +
Hypertriglyceridemia − ++ +
Anemia + ++ −
Insulin resistance − ++ +
Elevated cytokines +/− ++ +/−
Increased C-reactive protein − ++ −+: present; –: absent.
Malnutrition in the older population
Malnutrition is the state of being poorly nourished due to either the lack of one or more nutrients (undernutrition), or the excess of nutrients (overnutrition). The elderly usually suffer from undernutrition. In the older populatio4, malnutrition is an important issue that has been observed in hospitals,33 residential care,32 and in the community.35
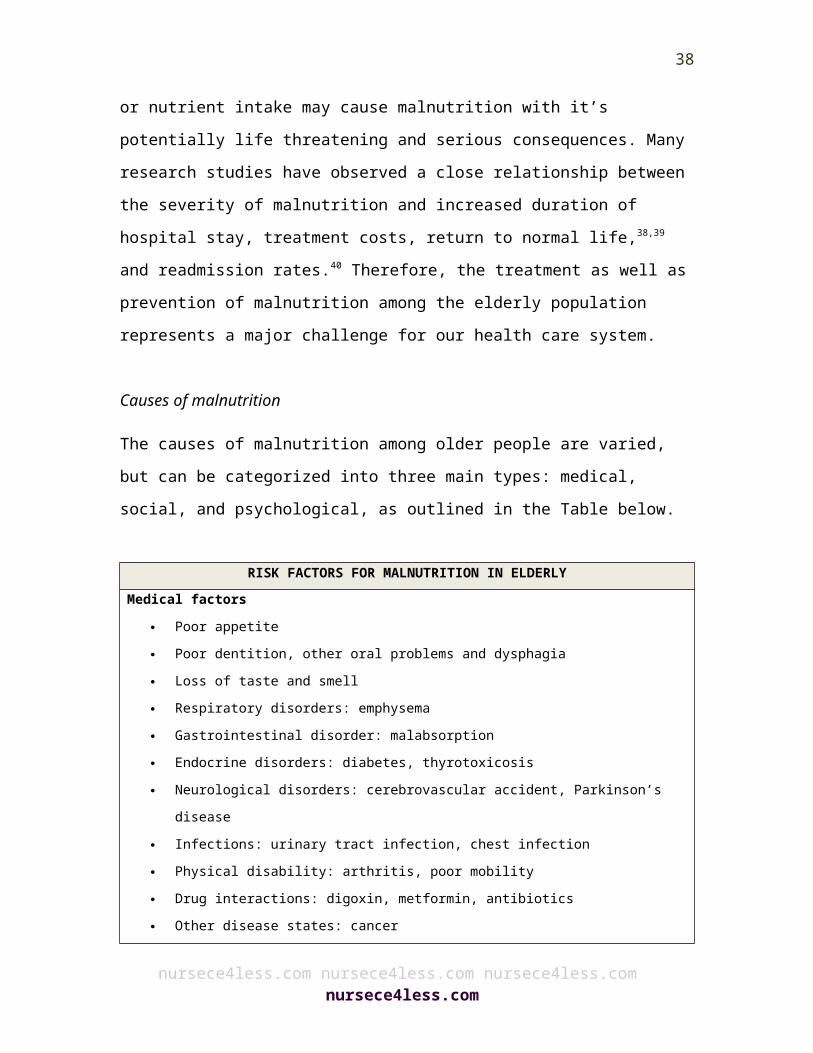
The prevalence of malnutrition in the general hospital population hovers around 11% to 44%, but can rise in the elderly to 29%– 61%.33 Aging is not the sole factor for malnutrition in the elderly: many other changes linked to the aging process can cause malnutrition.36 For example, the elderly may have loss of smell and taste acuity, poor dental and oral health, and decreased physical activity, all of which may adversely impact food intake.37 Any change in food or nutrient intake may cause malnutrition with it’s potentially life threatening and serious consequences. Many research studies have observed a close relationship between the severity of malnutrition and increased
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
28
duration of hospital stay, treatment costs, return to normal life,38,39 and readmission rates.40 Therefore, the treatment as well as prevention of malnutrition among the elderly population represents a major challenge for our health care system.
Causes of malnutrition
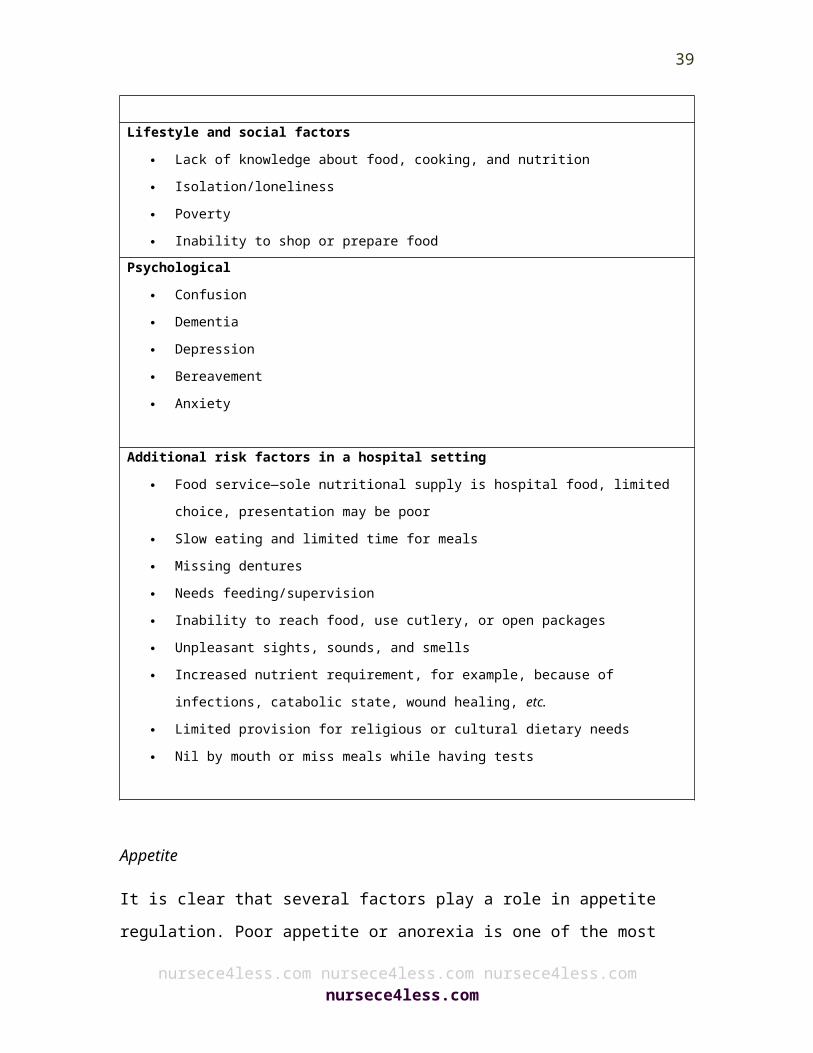
The causes of malnutrition among older people are varied, but can be categorized into three main types: medical, social, and psychological, as outlined in the Table below.
RISK FACTORS FOR MALNUTRITION IN ELDERLYMedical factors
Poor appetite Poor dentition, other oral problems and dysphagia Loss of taste and smell Respiratory disorders: emphysema Gastrointestinal disorder: malabsorption Endocrine disorders: diabetes, thyrotoxicosis Neurological disorders: cerebrovascular accident, Parkinson’s disease Infections: urinary tract infection, chest infection Physical disability: arthritis, poor mobility Drug interactions: digoxin, metformin, antibiotics Other disease states: cancer
Lifestyle and social factors Lack of knowledge about food, cooking, and nutrition Isolation/loneliness Poverty Inability to shop or prepare food
Psychological Confusion Dementia Depression Bereavement
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
29

Anxiety
Additional risk factors in a hospital setting Food service—sole nutritional supply is hospital food, limited choice,
presentation may be poor Slow eating and limited time for meals Missing dentures Needs feeding/supervision Inability to reach food, use cutlery, or open packages Unpleasant sights, sounds, and smells Increased nutrient requirement, for example, because of infections,
catabolic state, wound healing, etc. Limited provision for religious or cultural dietary needs Nil by mouth or miss meals while having tests
Appetite
It is clear that several factors play a role in appetite regulation. Poor appetite or anorexia is one of the most common causes of malnutrition and is mediated by a number of factors. Energy intake decreases with age,41,42 and the elderly are susceptible to micro-nutrient deficiencies with a poor energy intake.43 The exact mechanism behind this reduction is still unknown but several possible hypotheses have been developed. It is believed that aging is often linked with poor food intake regulation. It has been suggested that elderly fail to reduce their energy expenditure during these periods of negative energy balance.44 The elderly take longer to regain their lost weight, and are susceptible to risks associated with malnutrition during this period.
Researchers have also shown satiety is determined by a complex process involving the hormone cholecystokinin (CCK) and the relaxation of the stomach wall. CCK levels are higher in older people
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
30
with slow gastric emptying, both of which play an important role in early satiety.45 In addition, the elderly have a reduced stomach capacity. Therefore, the stomach wall stretches earlier thus causing early satiety.46 Compared to young adults, the elderly are also less responsive to the volume of the stomach contents, as measured by hunger ratings.47 It is suspected that ghrelin (hunger hormone) level is reduced with aging, trauma or illness. Aging also causes the dysregulation of peptide hormones such as CCK, peptide-YY, oxyntomodulin, glucagon-like peptide 1, and pancreatic polypeptide.
These hormones play an important role in the regulation of appetite. Older people usually have reduced levels of growth and sex hormones, but have increased levels of catecholamines and glucocorticoids.32 This hormonal imbalance leads to elevated levels of cytokines such as TNFa, IL1, IL6, and serotonin, which increase catabolism and can cause anorexia. These cytokines are also elevated in chronic inflammatory diseases, trauma, and various infections. Furthermore, the brain and neurotransmitters play an important role in the regulation of food intake. It is believed that aging leads to low levels of endogenous opioids in the brain as well as loss of opioid receptors.48 The elderly have reduced levels of nitric oxide and endogenous opioids, which play an important role in food intake regulation.
Taste and smell
A poor sense of taste and smell are also held responsible for the loss of appetite, as they are associated with decline in the pleasantness of food.49 Taste also plays a crucial role in the cephalic phase response that prepares the body for food digestion. Taste is also an important factor for the modulation of food selection and meal size by increasing the pleasure of eating and satiety.50 Aging is associated with loss of
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
31
taste and smell that and can also be exacerbated by certain medications and diseases.50,51 The exact cause of taste loss is still not known. It is believed that aging leads to reduction in the number of taste buds, and a decrease in the functioning of taste receptors, which play a key role in taste sensation.50
Many drugs such as antihistamines, lipid lowering agents and others can alter the sensation of taste and smell. The exact mechanism by which these medications alter taste or smell is still unknown. Some research studies have observed that improving the food flavor can enhance nutritional intake and cause weight gain in nursing home and hospital patients, as well as in the healthy elderly.52,53
Oral health, dental status and dysphagia
Poor oral health and dentition can significantly impact food intake in the elderly; it can cause difficulty in chewing, speaking, dryness of mouth, and can impact relationships with others.54,56 In these studies, it was shown that energy intake was lower in edentate elderly people with poor energy intake with concomitant deficiencies of micronutrients (calcium, iron, vitamins A, C and E, and some B vitamins), fiber, and protein. Dysphagia from various causes in the elderly, presbyesophagus or disease, can lead to malnutrition due to poor food intake.57
Disease and disability
In the elderly, disease may increase the risk of malnutrition. It has been observed that rates of hospital malnutrition, and worsening malnutrition increase during illness. Additionally, some drugs can adversely affect food intake. Compared to other age groups, the
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
32
elderly take more medications and are therefore more likely to have these adverse side effects.
Lifestyle and social factors
It has been observed that burden of disease, stress, poor appetite, and vision, comprise independent determinants of food intake in elderly.58 Lifestyle factors may also contribute in the development of malnutrition. Other determinants of food intake are:
Knowledge of cooking Social isolation and loneliness Food attitudes and beliefs Certain psychological factors such as stress, depression, and
bereavement Availability of services and assistance Oral health and dentition Food expenditure Food availability Degree of functional disability Appetite status Disease status
Dementia and confusion
Several studies have observed a close relationship between cognitive impairments and malnutrition in elderly. It has been observed that there is an inverse relationship between food intake and cognition, indicating that impaired cognition may adversely impact the ability or the desire to eat.59 Progressive dementia process is characterized by frequent weight loss and an altered eating pattern. Uncontrolled weight loss is a distinctive feature in the latter stages.60 Approximately 50% of the elderly with Alzheimer’s disease lose the ability to feed
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
33
themselves eight years after diagnosis.61 Furthermore, it has been observed that even in early stages of Alzheimer’s disease, some patients may experience slower oral manipulation of food and a slower swallow response.62
A recent study conducted on nursing home patients with dementia done to investigate the cause of unintentional weight loss, found a close association between weight loss in demented elderly and the process of choosing food, bringing the chosen food to the mouth, and chewing.63 Several studies have also observed that major changes in feeding ability develop during dementia and subsequently lead to weight loss and malnutrition.
Depression and other psychological factors
Several studies have observed that depression leads to malnutrition and weight loss in the elderly.64-66 Bereavement can also adversely impact eating behaviors and food intake.67 Stress and anxiety can impact and pattern food intake. For example, it has been found that low or depressed moods may push people to eat more, particularly comfort food. On the other hand, some people may resort to a fasting state instead.
Common Single Nutrient Deficiency Diseases
The tables below outline the more common nutrient deficiencies experienced by aged individuals, and the effects of protein malnutrition.
DiseaseDeficient nutrient Clinical presentations
Pellagra Niacin Dermatitis, diarrhea or constipation and dementia
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
34
DiseaseDeficient nutrient Clinical presentations
(Vit B3)
BeriberiThiamine (Vit B1)
Dry: Parasthenia, footdrop, loss of reflexes Wet: Edema, dyspnea, heart failure
Wernicke’s Syndrome
Thiamine (Vit B1)
Confusion, sixth nerve palsy, comaScurvy Vitamin C Petechiae, bleedingXeropthalmia Vitamin A Keratitis, blindness
Effects of protein energy malnutrition
DeathPressure ulcersHip fractureFallsWeaknessFatigueAnemiaEdemaCognitive abnormalitiesInfectionsImmune dysfunctionThymic atrophyDecreased delayed hypersensitivityDecreased helper T cells (CD4+)
Decreased lymphocyte response to mitogens
Decreased response to immunizations
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
35
Assessing malnutrition Initial screening for malnutrition in the elderly includes an accurate measurement of weight and height and assessment with a screening tool such as the Mini Nutritional Assessment (MNA).68 Clinical judgment plays an important role in the identification of patients at risk for malnutrition.69 Proper assessment of function is important because functional decline may lead to malnutrition or result from it.
Weight and body mass index Weight loss is an important indicator of malnutrition. Parameters for the assessment of elderly in long-term care settings are as follows:70-77
Severe weight loss is defined as greater than 5% weight loss in 1 month, 7.5% weight loss in 3 months or 10% weight loss in 6 months.
Failure to thrive can be defined as a 25% weight loss with no identifiable cause.
Measurement of weight and height are necessary to determine body mass index. A BMI of 21 or less is often consistent with malnutrition in older adults and has been linked to higher mortality. It should trigger intervention.
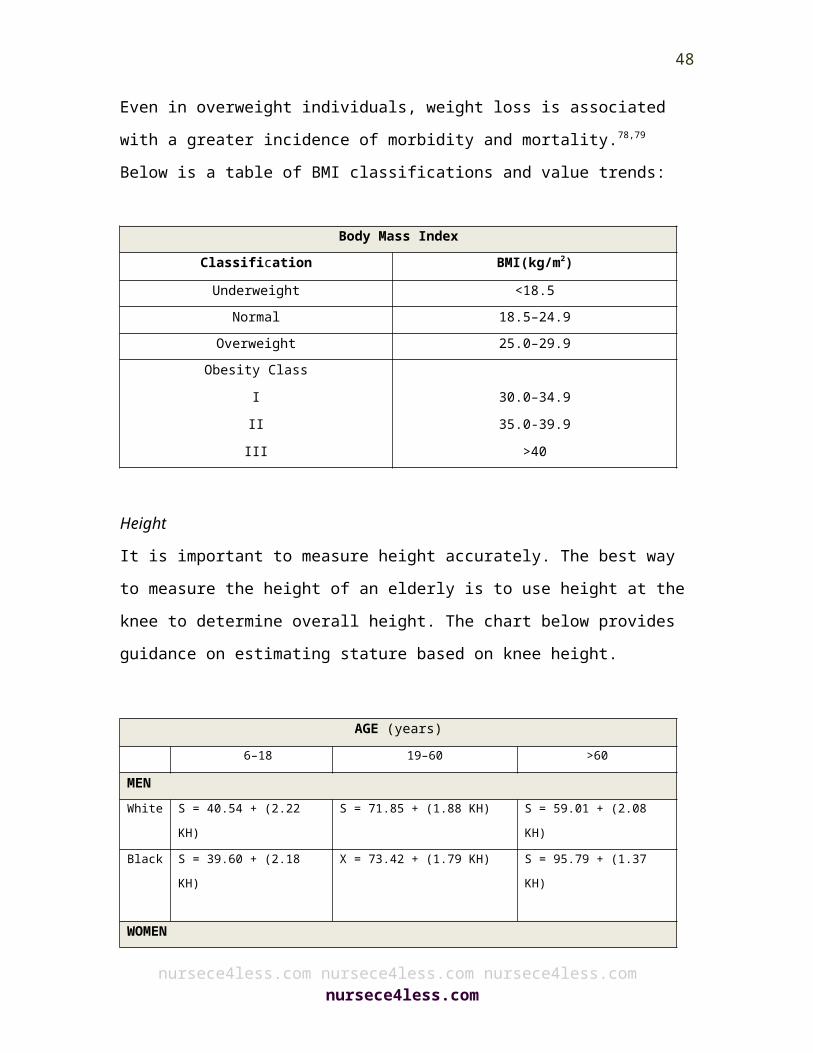
Even in overweight individuals, weight loss is associated with a greater incidence of morbidity and mortality.78,79 Below is a table of BMI classifications and value trends:
Body Mass IndexClassification BMI(kg/m2)Underweight <18.5
Normal 18.5–24.9Overweight 25.0–29.9
Obesity ClassIII
30.0–34.935.0-39.9
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
36
III >40
Height It is important to measure height accurately. The best way to measure the height of an elderly is to use height at the knee to determine overall height. The chart below provides guidance on estimating stature based on knee height.
AGE (years)6–18 19–60 >60
MENWhite S = 40.54 + (2.22 KH) S = 71.85 + (1.88 KH) S = 59.01 + (2.08 KH)Black S = 39.60 + (2.18 KH) X = 73.42 + (1.79 KH) S = 95.79 + (1.37 KH)
WOMEN White S = 43.21 + (2.14 KH) S = 70.25 + (1.87 KH) –
0.06 A)S = 75.00 + (1.91 KH) – (0.17 A)
Black S = 46.59 + (2.02 KH) S = 68.10 + (1.86 KH) – (0.06 A)
S = 58.72 + (1.96 KH)
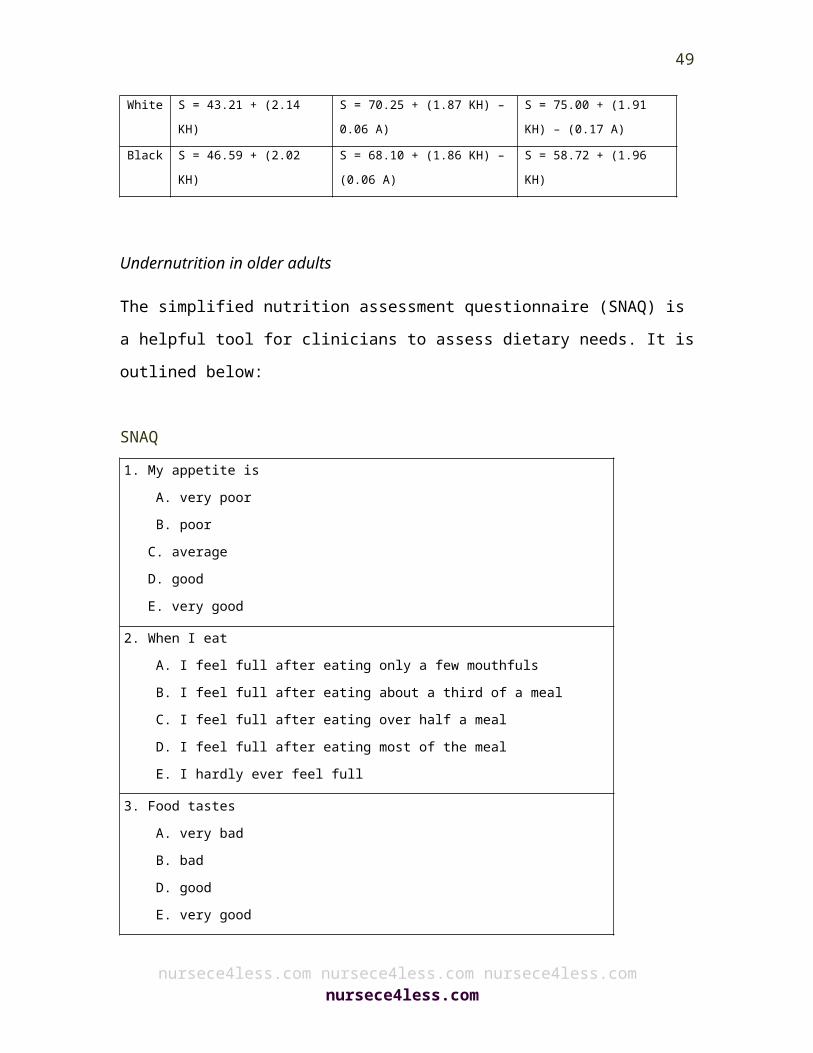
Undernutrition in older adults
The simplified nutrition assessment questionnaire (SNAQ) is a helpful tool for clinicians to assess dietary needs. It is outlined below:
SNAQ
1. My appetite is A. very poor B. poor C. average D. good E. very good
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
37
2. When I eat A. I feel full after eating only a few mouthfuls B. I feel full after eating about a third of a meal C. I feel full after eating over half a meal D. I feel full after eating most of the meal E. I hardly ever feel full
3. Food tastes A. very bad B. bad D. good E. very good
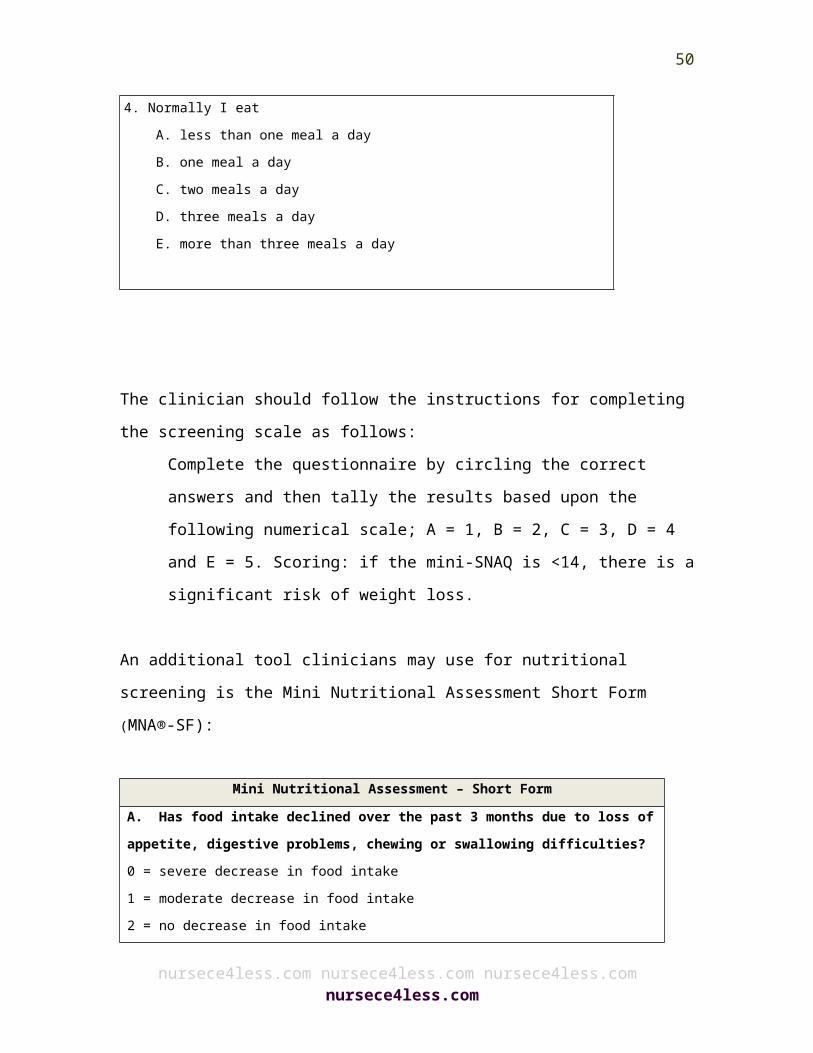
4. Normally I eat A. less than one meal a day B. one meal a day C. two meals a day D. three meals a day E. more than three meals a day
The clinician should follow the instructions for completing the screening scale as follows:
Complete the questionnaire by circling the correct answers and then tally the results based upon the following numerical scale; A = 1, B = 2, C = 3, D = 4 and E = 5. Scoring: if the mini-SNAQ is <14, there is a significant risk of weight loss.
An additional tool clinicians may use for nutritional screening is the Mini Nutritional Assessment Short Form (MNA®-SF):
Mini Nutritional Assessment – Short FormA. Has food intake declined over the past 3 months due to loss of
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
38
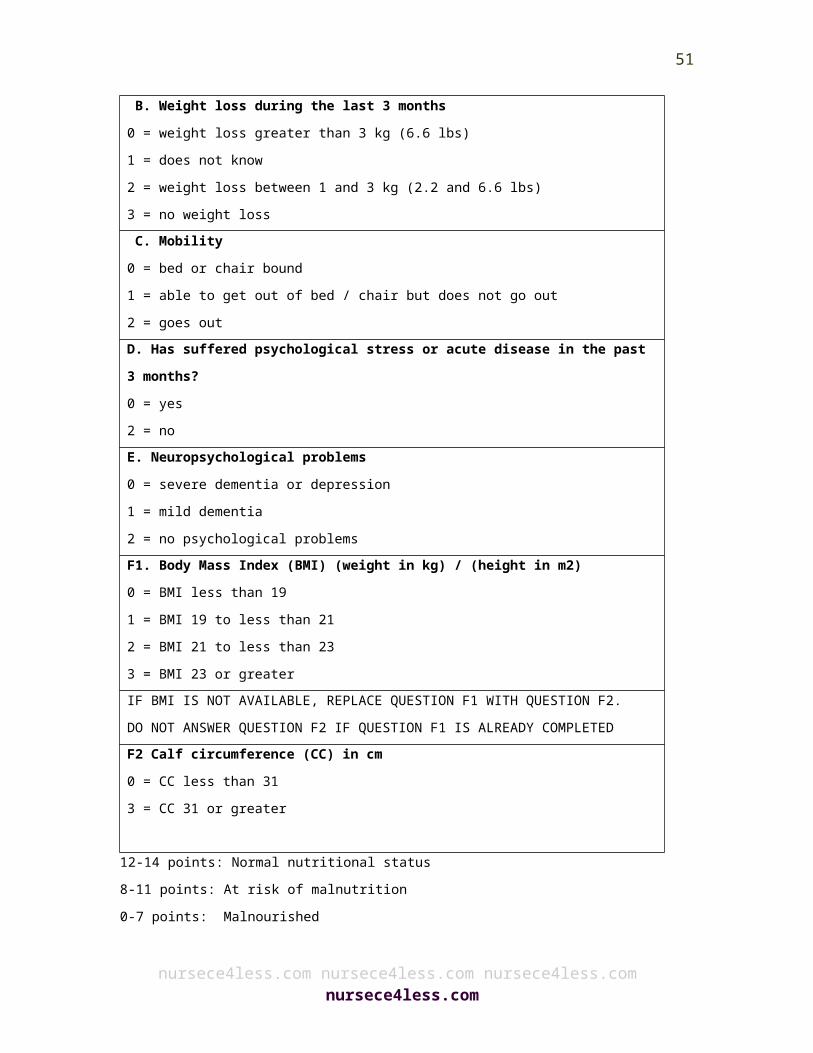
appetite, digestive problems, chewing or swallowing difficulties? 0 = severe decrease in food intake 1 = moderate decrease in food intake 2 = no decrease in food intake B. Weight loss during the last 3 months 0 = weight loss greater than 3 kg (6.6 lbs) 1 = does not know 2 = weight loss between 1 and 3 kg (2.2 and 6.6 lbs) 3 = no weight loss C. Mobility 0 = bed or chair bound 1 = able to get out of bed / chair but does not go out 2 = goes out D. Has suffered psychological stress or acute disease in the past 3 months? 0 = yes 2 = no E. Neuropsychological problems 0 = severe dementia or depression 1 = mild dementia 2 = no psychological problems F1. Body Mass Index (BMI) (weight in kg) / (height in m2) 0 = BMI less than 19 1 = BMI 19 to less than 21 2 = BMI 21 to less than 23 3 = BMI 23 or greater IF BMI IS NOT AVAILABLE, REPLACE QUESTION F1 WITH QUESTION F2. DO NOT ANSWER QUESTION F2 IF QUESTION F1 IS ALREADY COMPLETEDF2 Calf circumference (CC) in cm 0 = CC less than 31 3 = CC 31 or greater
12-14 points: Normal nutritional status 8-11 points: At risk of malnutrition0-7 points: Malnourished
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
39
The Full MNA® is a screening tool to help identify elderly patients who are malnourished or at risk of malnutrition. It is a more thorough version of the MNA®-SF. The following table explains each question and how to assign and interpret the score.
Full Mini Nutritional AssessmentA. Has food intake declined over the past 3 months due to loss of appetite, digestive problems, chewing or swallowing difficulties? 0 = severe decrease in food intake 1 = moderate decrease in food intake 2 = no decrease in food intake
Ask patient or caregiver or check themedical record• “Have you eaten less than normal over the past three months?”• If so, “is this because of lack of appetite, chewing, or swallowing difficulties?”• If yes, “have you eaten much less thanbefore, or only a little less?”
B. Weight loss during the last 3 months 0 = weight loss greater than 3 kg (6.6 lbs) 1 = does not know 2 = weight loss between 1 and 3 kg (2.2 and 6.6 lbs) 3 = no weight loss
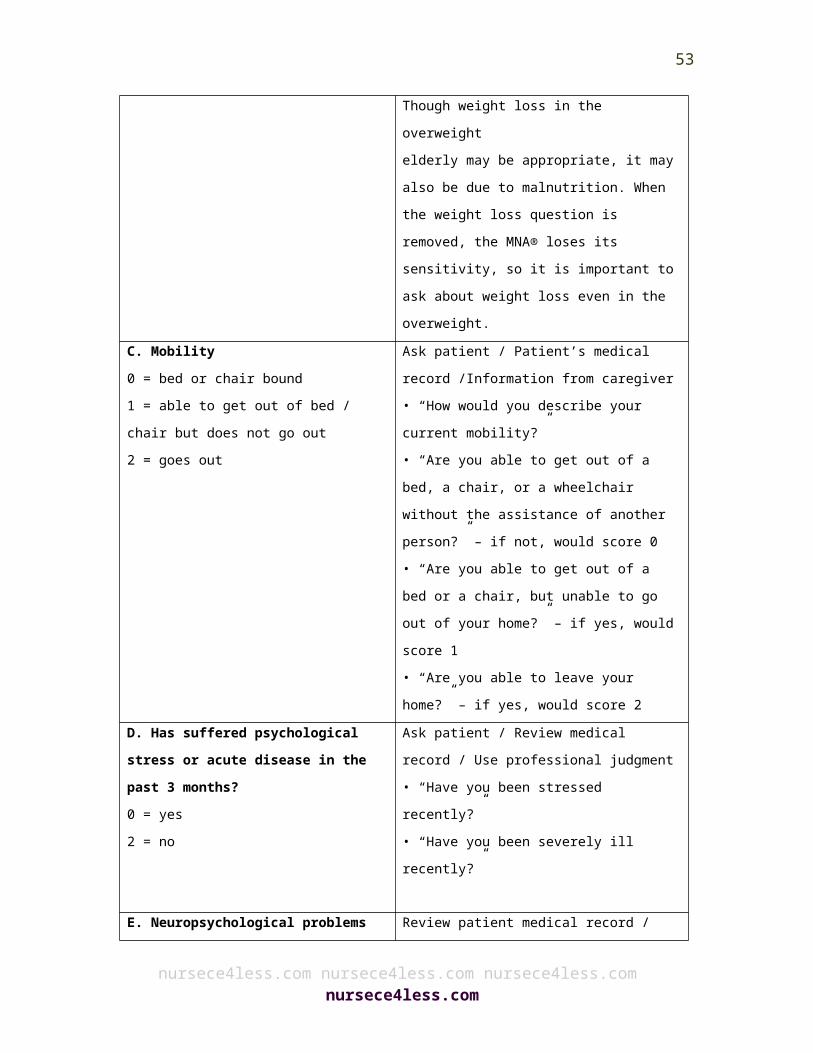
Ask patient / Review medical record (if long term or residential care)• “Have you lost any weight without trying over the last 3 months?”• “Has your waistband gotten looser?”• “How much weight do you think you have lost? More or less than 3 kg (or 6 pounds)?”Though weight loss in the overweightelderly may be appropriate, it may also be due to malnutrition. When the weight loss question is removed, the MNA® loses its sensitivity, so it is important to ask about weight loss even in the overweight.
C. Mobility 0 = bed or chair bound 1 = able to get out of bed / chair but does not go out
Ask patient / Patient’s medical record /Information from caregiver• “How would you describe your current mobility?”
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
40
2 = goes out • “Are you able to get out of a bed, a chair, or a wheelchair without the assistance of another person?” – if not, would score 0• “Are you able to get out of a bed or a chair, but unable to go out of your home?” – if yes, would score 1• “Are you able to leave your home?” – if yes, would score 2
D. Has suffered psychological stress or acute disease in the past 3 months? 0 = yes 2 = no
Ask patient / Review medical record / Use professional judgment• “Have you been stressed recently?”• “Have you been severely ill recently?”
E. Neuropsychological problems 0 = severe dementia or depression 1 = mild dementia 2 = no psychological problems
Review patient medical record / Useprofessional judgment / Ask patient,nursing staff or caregiver• “Do you have dementia?”• “Have you had prolonged or severe sadness?”The patient’s caregiver, nursing staff ormedical record can provide informationabout the severity of the patient’sneuropsychological problems (dementia).
F1 Body Mass Index (BMI) (weight in kg) / (height in m2) 0 = BMI less than 19 1 = BMI 19 to less than 21 2 = BMI 21 to less than 23 3 = BMI 23 or greater
Determining BMIBMI is used as an indicator of appropriate weight for height (Appendix 1)BMI Formula – US Units• BMI = (Weight in Pounds / [Height in inches x Height in inches]) x 703BMI Formula – Metric Units• BMI = (Weight in Kilograms / [Height in Meters x Height in Meters])1 Pound = 0.45 Kilograms1 Inch = 2.54 CentimetersBefore determining BMI, record the patient’s weight and height on the MNA®
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
41
form.1. If height has not been measured, please measure using a stadiometer or height gauge (Refer to Appendix 2).2. If the patient is unable to stand, measure height using indirect methods such as measuring demi-span, arm span, or knee height. 3. Using the BMI chart, locate the patient’s height and weight and determine the BMI.4. Fill in the appropriate box on the MNA® form to represent the BMI of the patient.5. To determine BMI for a patient with an amputation.Note: If the BMI cannot be obtained,discontinue use of the full MNA® and use the MNA®-SF instead. Substitute calf circumference for BMI on the MNA®-SF.
F2 Calf circumference (CC) in cm 0 = CC less than 31
3 = CC 31 or greaterAdditional Information:G. Lives independently (not in a nursing home)?Score 1 = Yes 0 = No
Ask patientThis question refers to the normal living conditions of the individual. Its purpose is to determine if the person is usually dependent on others for care. For example, if the patient is in the hospital because of an accident or acute illness, where does the patient normally live?• “Do you normally live in your own home, or in an assisted living, residential setting, or nursing home?”
H. Takes more than 3 prescription drugs per day?
Ask patient / Review patient’s medical record
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
42

Score 0 = Yes 1 = No
Check the patient’s medication record / ask nursing staff / ask doctor / ask patient
I. Pressure sores or skin ulcers?Score 0 = Yes 1 = No
Ask patient / Review patient’s medical record• “Do you have bed sores?”Check the patient’s medical record fordocumentation of pressure wounds or skin ulcers, or ask the caregiver / nursing staff /doctor for details, or examine the patient if information is not available in the medical record.
J. How many full meals does the patient eat daily?Score 0 = One meal 1 = Two meals 2 = Three meals
Ask patient / Check food intake recordif necessary• “Do you normally eat breakfast, lunch and dinner?”• “How many meals a day do you eat?”A full meal is defined as eating more than 2 items or dishes when the patient sits down to eat.For example, eating potatoes, vegetable, and meat is considered a full meal; or eating an egg, bread, and fruit is considered a full meal
K. Selected consumption markers for protein intake Select all that apply.• At least one serving of dairy products (milk, cheese, yogurt) per day?Yes No• Two or more servings of legumes or eggsper week?Yes
Ask the patient or nursing staff, or check the completed food intake record• “Do you consume any dairy products (a glass of milk / cheese in a sandwich / cup of yogurt / can of high protein supplement)every day?”• ”Do you eat beans / eggs? How often do you eat them?”• “Do you eat meat, fish or chicken every day?”
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
43
No• Meat, fish or poultry every day?Yes NoScore 0.0 = if 0 or 1 Yes answer0.5 = if 2 Yes answers1.0 = if 3 Yes answersL. Consumes two or more servings of fruits or vegetables per day?Score 0 = No 1 = Yes
Ask the patient / check the completed food intake record if necessary• “Do you eat fruits and vegetables?”• ”How many portions do you have each day?”A portion can be classified as:• One piece of fruit (apple, banana, orange, etc.)• One medium cup of fruit or vegetable juice• One cup of raw or cooked vegetables
M. How much fluid (water, juice, coffee, tea, milk) is consumed per day?Score 0.0 = Less than 3 cups0.5 = 3 to 5 cups1.0 = More than 5 cups
Ask patient• “How many cups of tea or coffee do you normally drink during the day?”•”Do you drink any water, milk or fruit juice?”“What size cup do you usually use?”A cup is considered 200 – 240ml or 7-8oz.
N. Mode of Feeding?Score 0 = Unable to eat without assistance 1 = Feeds self with some difficulty 2 = Feeds self without any problems
Ask patient / Review patient medical record/Ask caregiver• “Are you able to feed yourself?” / “Can the patient feed himself/herself?”•”Do you need help to eat?” / “Do you help the patient to eat?”• “Do you need help setting up your meals (opening containers, buttering bread, or cutting meats)?”* Patients who must be fed or need help
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
44
holding the fork would score 0.** Patients who need help setting up meals (opening containers, buttering bread, or cutting meats), but are able to feed themselves would score 1 point.Pay particular attention to potential causes of malnutrition that need to be addressed to avoid malnutrition (e.g. dental problems, need for adaptive feeding devices to support eating).
O. Self-View of Nutritional StatusScore 0 = Views self as being malnourished1 = Is uncertain of nutritional state2 = Views self as having nonutritional problems
Ask the patient• “How would you describe your nutritional state?”Then prompt ”Poorly nourished?”“Uncertain?”“No problems?”The answer to this question depends upon the patient’s state of mind. If you think the patient is not capable of answering the question, ask the caregiver / nursing staff for their opinion.
P. In comparison with other people of the same age, how does the patient consider his/her health status?Score 0.0 = Not as good0.5 = Does not know1.0 = As good2.0 = Better
Ask patient• “How would you describe your state of health compared to others your age?”Then prompt ”Not as good as others of your age?”“Not sure?”“As good as others of your age?”“Better?”Again, the answer will depend upon the state of mind of the person answering the question.QMid-arm circumference (MAC) in cmScore 0.0 = MAC less than 210.5 =
Q. Mid-arm circumference (MAC) Measure the mid-arm circumference in
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
45
in cmScore 0.0 = MAC less than 210.5 = MAC 21 to 221.0 = MAC 22 or greater
cm
R. Calf circumference (CC) in cmScore 0 = CC less than 311 = CC 31 or greater
Calf circumference should be measured in cm
24-30 points-Normal nutritional status; 17-23.5 points-At Risk of Malnutrition<17 points-MalnourishedUndernutrition in older adults
The ‘Meals on Wheels’ mnemonic for treatable causes of weight loss is a helpful way to organize evaluation of the older adult. It is outlined below as: MedicationsEmotional (depression)Alcoholism, anorexia tardive dyskinesia, abuse (elder)Late life paranoiaSwallowing problemsOral problemsNosocomial infections, no money (poverty)Wandering/dementiaHyperthyroidism, hypercalcemia, hypoadrenalismEnteric problems (malabsorption)Eating problems (e.g. Tremor)Low salt, low cholesterol dietShopping and meal preparation problems, stones (cholecystitis)
Laboratory Studies Laboratory analysis for an elderly patient suspected of malnutrition should assess the presence of disease and conditions that cause
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
46
weight loss or loss of appetite. A complete blood count screens for infection and anemia, particularly megaloblastic anemia due to B12 or folate deficiency. A complete thyroid profile to detect hypothyroidism and hyperthyroidism is also required. A comprehensive metabolic panel including total protein and albumin, serum electrolytes and liver function tests should also be conducted. Urinalysis and stool analysis should also be conducted to detect infection and bleeding. Some of the important markers of malnutrition in elderly include albumin, transferrin, retinol-binding protein and thyroxine-binding prealbumin.80
Among all these markers of nutrition, serum albumin is considered to be more accurate as it is predictive of mortality and other outcomes in older people. However, these proteins are also affected by inflammation and infection; therefore, they have limited usefulness. Transferrin is a more sensitive indicator of early protein-energy malnutrition; however, it is not reliable in conditions such as iron deficiency, chronic infection, hypoxemia, and liver disease.81 A low total lymphocyte count indicates a poor prognosis and is independent of low serum albumin.80,82 Malnutrition is also associated with age-related immune impairments, including decreased lymphocyte proliferation.83 No biochemical marker or screening test can clearly indicate malnourishment. Management of Malnutrition
Only 1% of elderly individuals who are independent and healthy are malnourished; however, approximately, 16% of community-dwelling elderly in the U.S. consumed fewer than 1000 calories per day.84,85 Management of malnutrition in the elderly focuses early on offering ample food choices with high nutrient density and high caloric value after which additional caloric supplements can be considered. It also
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
47
focuses on the early diagnoses and treatment of treatable causes of malnutrition. Provision of adequate food forms the basis of the management of malnutrition.
A recent study has observed that caloric supplementation is associated with decreased length of hospitalization and mortality.86 Amino acid supplementation rich in leucine has been found to increase production of muscle protein and muscle function.87 Oral calorie supplements should ideally be taken between meals.88 Improving food taste, enhancing flavors, good ambience and time spent feeding impaired elderly also help in treating malnutrition.89-91
There are two major orexigenic or appetite stimulant drugs (megestrol acetate and dronabinol), which may be used for the management of malnutrition. Megestrol acetate causes increased food intake and leads to weight gain.92 It is more effective in women than in men. Megestrol acetate should be given with food for better absorption. A nanoparticle form of this drug is better absorbed during starvation. The major adverse effect of this drug is increased risk of deep vein thrombosis. Megestrol acetate should not be prescribed to elderly confined to bed. Its efficacy increases in combination with olanzapine (a mood altering drug).93 Dronabinol is also an effective medication that leads to a small increase in appetite as well as weight gain. It is also used as palliative care drug as it decreases nausea, increases enjoyment of food and life. Testosterone in combination with a caloric supplement can also lead to weight gain and decreases hospitalization in the frail elderly.94
Gastrointestinal tube feeding can be a life saving option for those elderly who are unable to swallow. However, tube feeding should be used selectively.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
48
Aging is associated with decreased vitamin D level.95 Low-level vitamin D in the body is associated with fractures, muscle atrophy, falls and an increased rate of mortality. Adequate supplementation with 800–1000 IU vitamin D daily may help the elderly manage low levels of vitamin D.
Anemia due to malnutrition is common in the elderly.96 Iron deficiency anemia is the most common, but vitamin B12 and folate deficiency are also seen in the elderly. Iron deficiency anemia is observed in individuals having a low iron and ferritin level. Transferrin receptors should be measured to differentiate from the anemia of chronic disease. Methylmalonic acid levels should be assessed in people with borderline low levels of vitamin B12. Treatment of vitamin B12 deficiency includes either 1000 IU of vitamin B12 orally daily or injections of 1000 IU of vitamin B12 weekly for 4 weeks.
Iron deficiency anemia is treated with oral iron once a day for 6 weeks. Reticulocyte count should be measured after 1 week of treatment. If the reticulocyte count doesn’t increase, malabsorption may be a possibility and parenteral iron may be required in such cases.
Zinc deficiency may be seen in elderly with diabetes mellitus and cancer or who are on diuretics.97 The role of zinc supplementation remains uncertain. Interventions that may be necessary for the management of undernutrition, malnutrition and nutritional deficiencies may include one or more of the following actions:98
Liberalize diet by removing or changing dietary restrictions Encourage use of flavor enhancers Increase frequency of small meals Add liquid food supplements between meals
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
49
Addition of meat, peanut butter, or protein powder to increase protein intake
Diagnose and treat depression with medications that antidepressants that do not exacerbate malnutrition
Replace or discontinue drugs that may lead to anorexia Evaluate dysphagia, swallowing impairment and the ability to
manage eating Obtain social services assessment of living situation of
community-dwelling adults.
The hospital and skilled nursing facilities present additional factors that impact nutrition. Interventions that may be carried in the institutional setting for the management of malnutrition in the elderly include:
Ensure that patients have all the necessary sensory aids such as dentures, glasses, hearing aids, etc.
Make sure that the elderly patient is seated upright close to 90 degrees.
The elderly in a long-term care facility should preferably take their meals in the dining room.
While taking meals, food and utensils should be kept unwrapped or in open containers and should be within the patient's reach.
The elderly should be given ample time to eat, facilitating their potentially slower pace of eating.
Consider the ethnic food preferences of the elderly and allow families to bring foods that the patient loves to eat.
If an elderly person must be fed or requires assistance, give adequate time for chewing, swallowing, and clearing throat before another bite. The person assisting the patient should develop a good rapport with that patient.
Those with dementia may need to be reminded to chew and swallow and may benefit from finger foods.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
50
The patient’s family should be encouraged to be present at mealtime and to assist in feeding.
Clinical Signs and Nutritional Deficiencies
Below is a Table that outlines the common systemic signs and symptoms of nutrient deficits in the elderly.
System Sign or symptom Nutrient deficiency
Skin Dry scaly skin Zinc/essential fatty acids
Follicular hyperkeratosis Vitamins A, C
Petechiae Vitamins C, K
Photosensitive dermatitis Niacin
Poor wound healing Zinc, vitamin C
Scrotal dermatitis Riboflavin
Hair Thin/depigmented Protein
Easily plucked, hair loss Protein, zinc
Nail Transverse depigmentation Albumin
Spooning Iron
Eyes Night blindness Vitamin A, zinc
Conjunctival inflammation Riboflavin
Keratomalacia Vitamin A
Mouth Bleeding gums Vitamin C, riboflavin
Glositis Niacin, pyridoxine, riboflavin
Atrophic papillae Iron
Hypogeusia Zinc, vitamin A
Neck Thyroid gland enlargement Iodine
Parotid gland enlargement Protein
Abdomen Diarrhea Niacin, folate, vitamin B12
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
51

System Sign or symptom Nutrient deficiency
Hepatomegaly Protein
Extremities Bone tenderness Vitamin D
Joint pain Vitamin C
Muscle tenderness Thiamine
Muscle wasting Protein, selenium vitamin D
Edema Protein
Neurological Ataxia Vitamin B12
Tetany Calcium, magnesium
Parasthesia Thiamine, vitamin B12
Ataxia Vitamin B12
Dementia Vitamin B12, niacin
Hyporeflexia Thiamine
Dysphagia
Dysphagia can be defined as any impairment in the swallowing process102 and is a frequent health concern in our aging population. Individuals with physiological or anatomical impairments in the mouth, pharynx, larynx, and esophagus may experience dysphagia.102 Dysphagia also increases the risk of malnutrition and pneumonia. Dysphagia is observed in 68% of elderly nursing home residents,105 around 30% of elderly admitted to the hospital,106 approximately 64% of patients after stroke,107,108 and up to 13%–38% of elderly who live independently.109-111
Predisposing factors for dysphagia in the elderly include alterations in swallowing physiology and chronic diseases. In the U.S., approximately 300,000–600,000 individuals suffer dysphagia every year.99 It is
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
52
believed that around 15% of the elderly population experience dysphagia.100 According to a recent study, from 2002–2007, dysphagia referral rates among the elderly in a single tertiary teaching hospital increased by 20%; and, 70% of the referrals were for individuals above the age of 60.101 In 2010, it is suggested that approximately 6 million elderly were at risk for dysphagia.
Aging effects on swallowing function
Aging leads to reductions in muscle mass and connective tissue elasticity, which results in poor range of motion103 and a loss of strength.104 These changes may adversely affect the process of swallowing. Most commonly, a subtle and progressive slowing of the swallowing processes occurs in the elderly. Over time, these subtle but cumulative changes may cause dysphagia and affect the upper airway.103 In addition, low moisture in the oral cavity, poor taste, and smell acuity can also lead to poor swallowing in the elderly. However, the predominant factor responsible for dysphagia in the elderly is the presence of age-related disease.
Dysphagia and its sequelae
The swallowing process is complex and many diseases and conditions can affect this vital function. Neurological diseases such as dementia, carcinoma of the esophagus and head/neck, and metabolic impairments also may play an important role in the development of dysphagia. Dysphagia in the elderly is also linked with increased mortality and morbidity.112 Common complications of dysphagia in the elderly include pneumonia and malnutrition.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
53
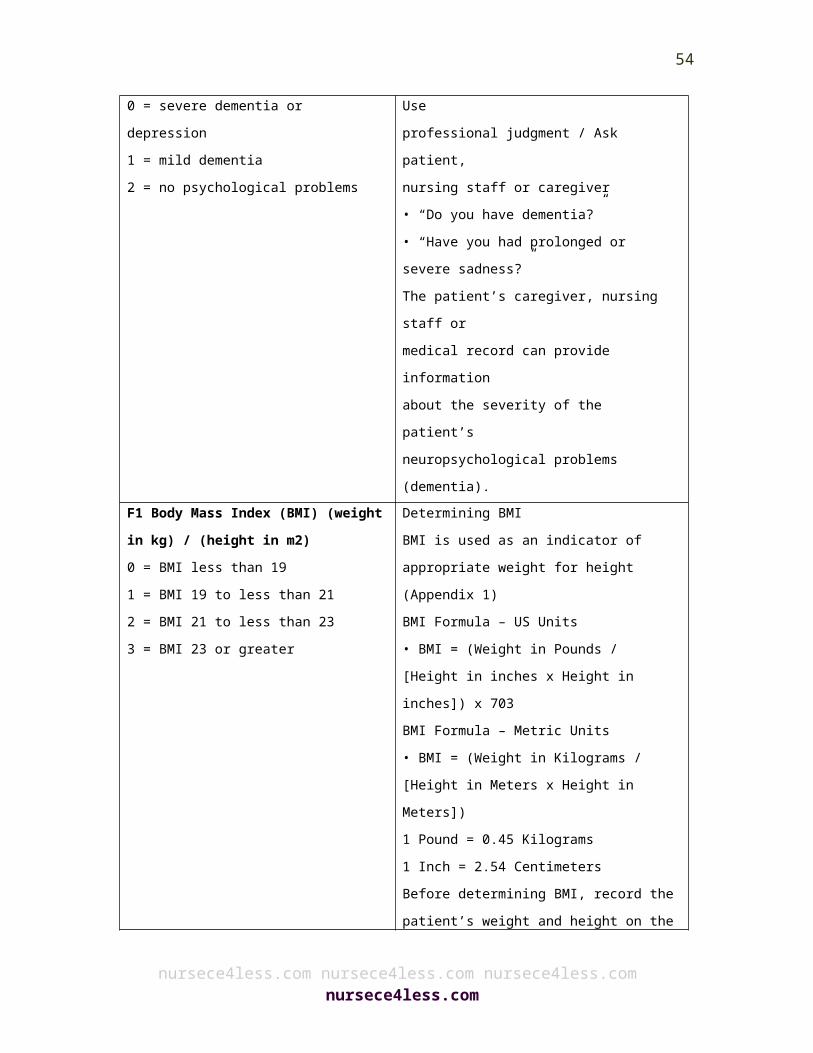
Below is a table of the common conditions that contribute to dysphagia in the elderly.
Conditions that may contribute to dysphagia
Neurologic disease Stroke Dementia Traumatic brain injury Myasthenia gravis Cerebral palsy Guillain–Barré syndrome Poliomyelitis Myopathy
Other Any tumor involving the digestive or
respiratory tract Iatrogenic diagnoses Chemotherapy Radiation therapy Medication related Other, related diagnoses Severe respiratory compromise
Progressive or neurologic disease Parkinson’s disease Huntington disease Age-related changes
Rheumatoid disease Polydermatomyositis Progressive systemic sclerosis Sjögren’s disease
Adapted from Groher ME, Crary MA. Dysphagia: Clinical Management in adults and children. Maryland Heights, MO: Mosby Elsevier; 2010.
Dysphagia and nutrition in stroke
Dysphagia is commonly seen after a stroke with estimates ranging from 30%–65%.107,108,113,114 Approximately 300,000–600,000 individuals experience dysphagia because of stroke or other neurological disorders.115 Many individuals regain functional swallowing within the first month following an episode of stroke;108 however, some individuals experience difficulty in swallowing even beyond 6 months.107,116 Common complications associated with dysphagia following stroke include malnutrition,117 pneumonia,118,119 dehydration,108,117 poorer long-term outcome,108,116 increased rehabilitation time and the need for long-term care assistance,120 increased length of hospital stay,121 increased mortality108,114,118 and increased health care costs.108 These
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
54
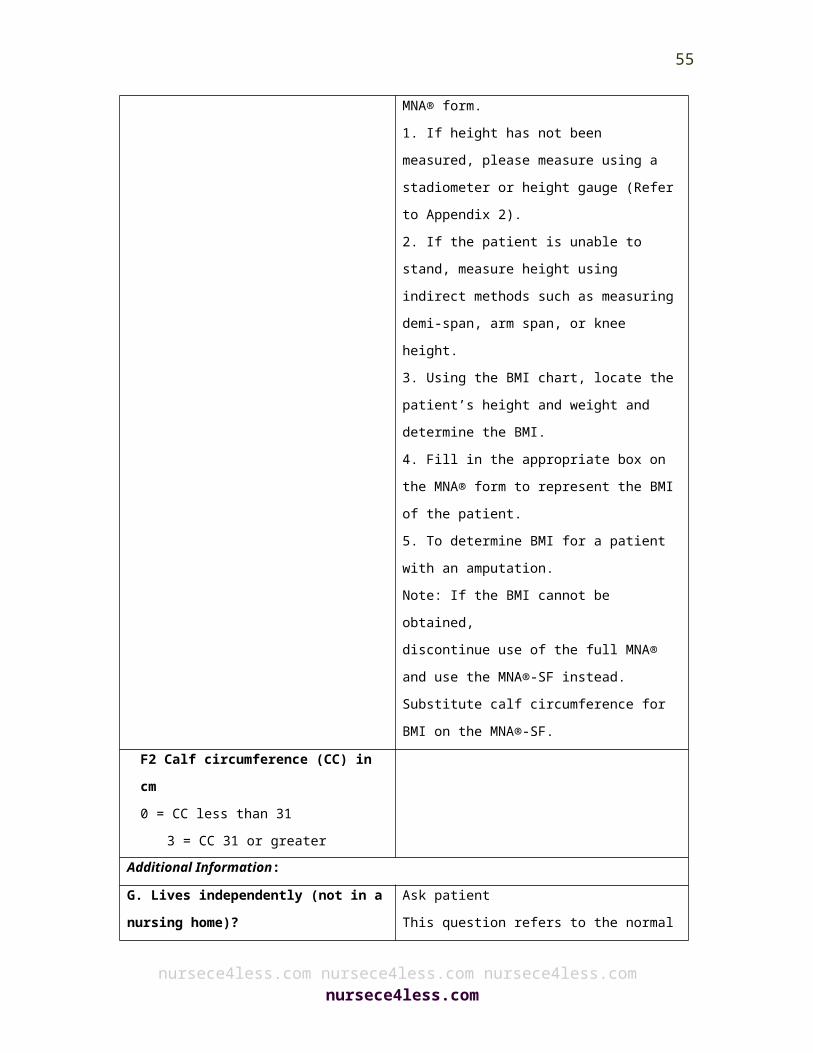
complications adversely impact the social and physical well being of the elderly, the quality of life of both elderly and caregivers, and the proper utilization of health care resources.115
During the acute phase of stroke, around 40%–60% of elderly patients report swallowing impairments.107,108 These impairments also accentuate malnutrition. Although the risk of malnutrition is increased in the presence of dysphagia post-stroke,122 pre-stroke factors must be taken into account when assessing nutritional status and predicting stroke outcome. Around 16% of stroke patients present with malnutrition. The risk and prevalence of malnutrition is 22%–26% at the time of discharge from acute care.123-125
Although, nutritional deficiencies and dysphagia often coexist, malnutrition is usually not associated with dysphagia in the acute phase of stroke.126 In fact the prevalence rate of malnutrition has increased up to 45% in the post acute rehabilitation phase.127 Poor food intake during acute hospitalization associated with dysphagia may lead to malnutrition during subsequent rehabilitation.122
Dysphagia and pneumonia in stroke
Post-stroke pneumonia affects up to one-third of acute stroke patients.128,129 Pneumonia accounts for approximately 35% of post-stroke mortality.130 The majority of stroke-related pneumonias are generally considered to be due to dysphagia and the subsequent aspiration of food. Aspiration can be defined as entry of liquid or food into the airway below the level of the true vocal cords.131 Aspiration pneumonia is the entry of swallowed materials (gastric or oral) into the airway that causes a lung infection.102 A recent study has observed
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
55

stroke patients with dysphagia have a three-fold increase in pneumonia risk, while the risk of pneumonia increases up to eleven-fold among patients after aspiration.118
Dysphagia and dementia
Dysphagia is a common feature of dementia. Approximately 45% of elderly patients with dementia experience some degree of swallowing impairment.132 Different presentations of dementia lead to varying degree of swallowing or feeding difficulties133-136 These patients usually have a slowing of the swallowing process.112 Additionally, elderly patients with dementia usually face problems with self-feeding. Dementia, dysphagia, and other related feeding dysfunctions may cause malnutrition and nutritional deficits, which combined with other factors, can lead to pneumonia and even death. The presence of dementia in elderly is closely associated with higher hospital admission rates and overall higher mortality.137
Dysphagia and nutrition in community dwelling older adults
Dysphagia contributes to poor nutritional status due to the reduced or altered oral intake of food or liquid. Dysphagia plays a role in the development of malnutrition, and malnutrition in turn can lead to poor functional capacity. Therefore, dysphagia plays an important role in the process of frailty among older patients.138 A study conducted on elderly individuals residing in community dwellings showed that approximately 37.6% those reported dysphagia,111 approximately 5.2% of these elderly reported the use of a feeding tube at some point in life, and around 12.9% took nutritional supplements to achieve an
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
56

adequate daily caloric intake.111 Several studies have observed that elderly patients with dysphagia living in the community are also susceptible to malnutrition.
Dysphagia and pneumonia in older adults
Recent findings indicate the potential association between dysphagia, pneumonia, and nutritional status in community dwelling elderly. The risk is increased for community-acquired pneumonia increases in elderly, particularly in those older than 75 years.139-141 Furthermore, deaths from pneumonitis due to aspiration are increasing.142,143 Dysphagia in the elderly also greatly increases the susceptibly to pneumonia.144
Assessment and Prevention of Dysphagia
Video fluoroscopy is considered to be the gold standard to study dysphagia. Fiberoptic endoscopic evaluation may also be considered if video fluoroscopy is not available.145 Some providers recommend these tests only for patients who fail a reliable clinical swallowing assessment.146
Clinical Symptoms of Aspiration:
Abrupt manifestations of certain respiratory symptoms (severe coughing and cyanosis) associated with drinking, eating, or the regurgitation of gastric contents.
A change in voice (hoarseness or a gurgling noise) after swallowing.
Small-volume aspirations that lead to minimal or no symptom are frequently seen in elderly and are usually not detected until these progresses to aspiration pneumonia.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
57
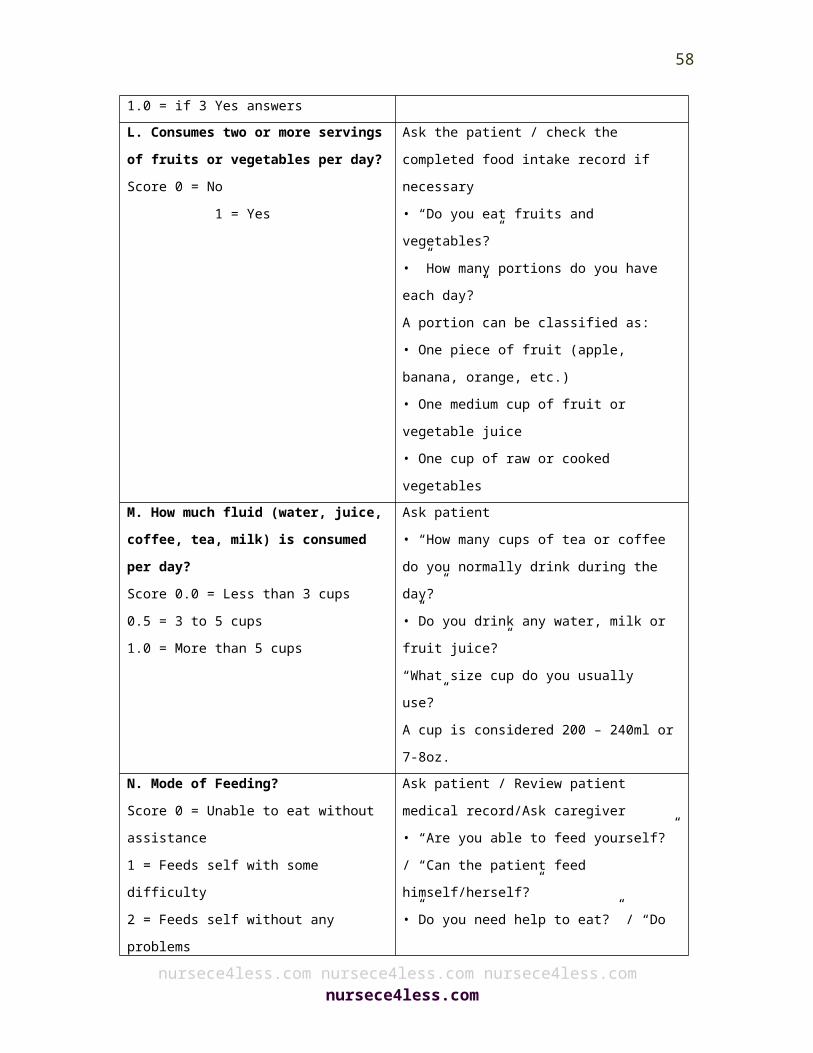
Aspiration Pneumonia:
Elderly individuals with pneumonia frequently usually experience fewer symptoms than young adults: therefore, aspiration pneumonia is usually detected late and is under-diagnosed in the elderly.
Delirium is frequently observed in elderly with aspiration pneumonias.
Tachypnea or increased respiratory rate is an early sign indicating pneumonia in elderly patients; other important symptoms of aspiration pneumonia include fever, chills, pleuritic chest pain and findings of crackles on auscultation of lungs.
High-risk elderly patients should be monitored closely for aspiration pneumonia.
Dysphagia Management
The presence of a strong relationship between swallowing process, nutritional status, and pneumonia among older patients indicates a role for dysphagia management in the elderly population. Successful and optimal swallowing interventions/techniques also help in the management of malnutrition and pneumonia. A number of dysphagia management techniques and tools can be used for the treatment of dysphagia.
Swallowing management
Dysphagia management requires multi-pronged strategies; no single strategy is appropriate for all older patients with dysphagia. Alternate sources of nutrition may be required for optimal nutrition.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
58
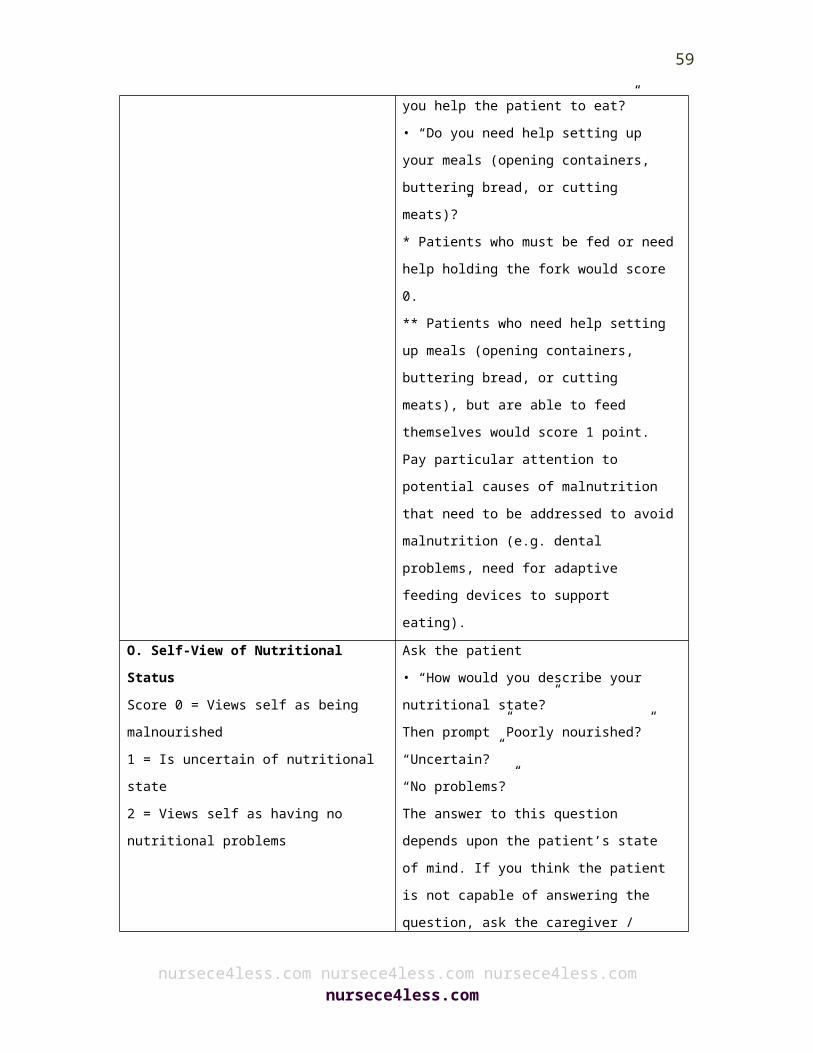
Compensatory strategies are also helpful for the continued safe oral intake of food. Compensatory strategies also include postural adjustments, swallow techniques or maneuvers, and diet modifications.112 Finally, speech therapists can play a key role in the management of patients with dysphagia.
Postural adjustments
Changes in body and/or head posture are common compensatory techniques that may help in reducing the risk of aspiration or residue.147 Postural changes can help alter the speed and flow direction of a food, which leads to a safe swallow.112 However, some research studies suggest that active rehabilitation efforts are better than these strategies for the prevention of pneumonia and malnutrition, as evidenced in the table below:148
Examples of Postural Adjustments
Technique Performance Intended outcome
Reported benefit
Body posture changesLying down • Lie down/angled
• Reduce impact of gravity during swallow
• Increased hypopharyngeal pressure on bolus
• Increased UES (Upper Esophageal Sphincter) opening
Side lying • Lie down on stronger side (lower)
• Slows bolus• Provides time to adjust/protect airway
• Reduced aspiration
Head posture changesHead extension/chin up
• Raise chin • Propels bolus to back of mouth• Widens oropharynx
• Reduced aspiration• Better bolus transport
Head flexion/chin
• Tucking chin towards • Improves airway • Reduced
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
59
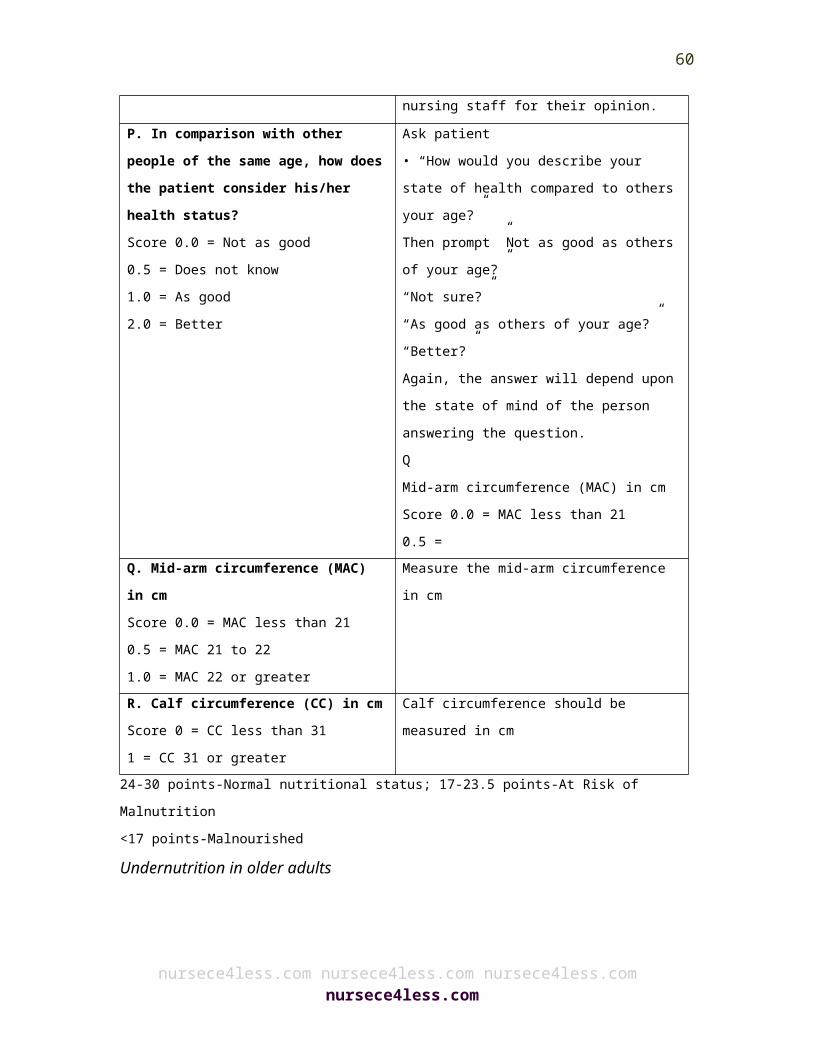
tuck the chest protection aspiration Head rotation/head turn
• Turning head towards the weaker side
• Reduces residue after swallow• Reduces aspiration
• Less residue • Reduced aspiration
Swallow maneuvers
Swallow maneuvers are different variations of the normal swallowing process in order to facilitate increased safety or efficiency of the swallow function. For instance, the supraglottic and the super supraglottic swallow techniques involve a voluntary breath hold and associated laryngeal closure to facilitate better swallowing and protect the airway during this process.112
Another technique called Mendelssohn maneuver facilitates relaxation of the upper esophageal sphincter (UES).149 Another popular maneuver is the ‘hard’ swallow that increases swallow forces leading to less residue or airway compromise.150,151 Unfortunately, there are limited and inconclusive data on the efficacy of these techniques;152-154 therefore, verification of the impact of these maneuvers using swallowing imaging studies should be conducted to ascertain the potential effect of these maneuvers before initiation of these compensatory strategies. Various types of swallow maneuvers are summarized in the table below:
TYPES OF SWALLOW MANEUVERSSwallow
maneuverPerformance Intended
outcomeReported benefit
Supraglottic swallow
Hold breath, swallow, and then
Reduce aspiration and increase
Reduces aspiration
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
60

gentle cough movement of the larynx
Super supraglottic swallow
Hold breath, bear down, swallow, and then gentle cough
Effortful swallow. Also called ‘hard’ or ‘forceful’ swallow
Swallow ‘harder’ Increased lingual force on the bolus Less aspiration and pharyngeal residue
Increased pharyngeal pressure and less residue
Mendelssohn maneuver
‘Squeeze’ swallow at apex
Improve swallow coordination
Reduced residue and aspiration
Diet Modifications
Modifying the consistency of food is the cornerstone of compensatory intervention for elderly with dysphagia.37 Thickened liquids are a common compensatory technique that is offered to elderly in hospitals and long-term care facilities.70 It is believed that thickened liquids aid in controlling the direction, speed, duration, and clearance of the food.70
Modified food diets
Solid foods can be modified to promote safe swallowing and proper nutrition. Levels of the modified diet are highlighted, as below:
LEVELS OF MODIFIED DIET
Level Description Examples of
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
61
recommended foods
Four Levels in the National dysphagia diet
Level 1: dysphagia pureed
Homogeneous, cohesive, and pudding like. No chewing required, only bolus control
Smooth, homogenous cooked cerealsPureed: meats, starches (like mashed potatoes), and vegetables with smooth sauces without lumpsPureed/strained soupsPudding, soufflé, yogurt
Level 2: dysphagia mechanically altered
Moist, semi-solid foods, cohesive. Requires chewing ability
Cooked cereals with little textureMoistened ground or cooked meatMoistened, soft, easy to chew canned fruit and vegetables
Level 3: dysphagia advanced
Soft-solids. Require more chewing ability
Well moistened breads, rice, and other starchesCanned or cooked fruit and vegetablesThin sliced, tender meats/poultry
Level 4: regular No modifications, all foods allowed
No restrictions
Adapted from Groher ME, Crary MA. Dysphagia: Clinical management in adults and children. Maryland Heights, MO. Mosby, Elsevier; 2010.
Feeding dependence and targeted feeding
Those elderly patients with stroke and dementia may become dependent upon others for feeding because of cognitive dysfunction and/or certain physical limitations. Feeding dependence may lead to an increased aspiration risk and associated complications in elderly patients with dysphagia. Such patients may require specific training on
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
62
feeding. Other techniques may be required to monitor the intake of food in order to provide increased safety, decreased fatigue, and improved feedback on swallowing during the course of the meal.131
Eating in environments without external stimuli and distractions is also helpful, particularly in skilled nursing or long-term care health care facilities. Introduction of angled utensils, cups without rims, etc., may also be beneficial for elderly patients with dysphagia.37
Provision of alternate nutrition
Alternate nutrition strategies can be the best form of compensation. Optimal and adequate non-oral feeding can benefit elderly with malnutrition and nutritional deficiencies. Malnutrition in the elderly together with other factors may lead to cardiovascular disease, poor cognitive function, impaired immunity, and poorly healing or non healing pressure ulcers and wounds.155,156
Swallow rehabilitation
The principal aim of swallow rehabilitation is overall improvement in process of swallowing. Exercise-based swallowing techniques may be employed to facilitate better functional swallowing, prevent or minimize dysphagia-related complications or morbidities, and improve swallowing physiology.157-160 Some of the exercise-based approaches for swallow rehabilitation are discussed in the table below:
Exercise-based swallow rehabilitation approachesProgram Focus Intended
outcomeReported benefit
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
63
Lingual resistance • Strengthening tongue with progressively increasing intensity
• Increased tongue strength• Improved swallow function
• Increased tongue muscle mass• Increased swallow pressure• Reduced aspiration
Shaker/head-lift • Strengthening suprahyoid muscles• Improve elevation of larynx• Increasing upper esophageal sphincter opening
• Improve strength of muscles for greater upper esophageal sphincter opening
• Increased larynx elevation• Increased upper esophageal sphincter opening• Less post-swallow aspiration
EMST (expiratory muscle strength training)
• Strengthening submental muscle• Improve expiratory pressures for better airway protection
• Improve expiratory drive• Reduce penetration and aspiration
• Better penetration-aspiration scores in Parkinson’s disease• Increased maximum expiratory pressure• Increased submental muscle electromyography activity during swallowing
MDTP (McNeill dysphagia therapy program)
• Swallow as exercise with progressive resistance
• Improve swallowing including strength and timing
• Improved swallow strength• Improved movement of swallow structures• Improved timing
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
64
• Weight gain
Falls In The Elderly
Falls may be defined as a sudden, unintentional change in position of an elderly leading to a position at a lower level, on an object, the floor, or the ground, other than as a consequence of seizure, sudden onset of paralysis, or an external force.161 There are number of factors that contribute to increased incidence of falls in elderly. Falls can be life threatening and can severely impact the quality of life, general health, and the independence of elderly persons.
Falls in the elderly are caused by complex interactions among the various risk factors, which may be characterized as intrinsic (patient related) or extrinsic (external to the patient).162-164 It is estimated that approximately 30-40% of community-dwelling elderly fall at least once per year.165-166 In the elderly, falls are among the leading causes of fatal and nonfatal injuries.167 The mortality rate due to falls is around 10 per 100,000 persons for elderly individuals in the 65-74 years age group and 147 per 100,000 persons for elderly individuals in the 85 years or older age group.168
The economic burden for fall-related injuries among community-dwelling elderly in 2000 was estimated to be approximately $19.2 billion.169 Another study has projected that by 2020 this cost could shoot up to $43.8 billion.170 It is important to note that majority of falls among elderly are preventable.171
Unintentional injuries are one of the leading causes of death in elderly, with falls accounting for two-thirds of such deaths.172 In nursing homes,
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
65
fall rates increase by two-fold when compared with the non-institutionalized population.173 Falls in the elderly are associated with poorer survival174 and great financial burden.175-176 Falls are the main cause of the traumatic spinal cord injury in elderly.177 Additionally, even non-injurious falls adversely impact the individual’s quality of life, lead to an increased fear of falling,178 and limit mobility and activity.179 The prevalence of risk factors associated with falls in elderly is greater in the nursing home setting and the majority of elderly residents have multiple risk factors.180
Some of the well-established risk factors in the long-term care setting include muscular weakness, poor balance and gait, poor vision, cognitive and functional dysfunction, delirium, orthostatic hypotension, certain medications, urinary incontinence and co-morbidities such as depression, stroke, arthritis, etc.181 In 2010, the overall rate of reported nonfatal fall injury episodes was 43 per 1,000 and elderly who were more than 75 years of age had the highest rate. The risk factors, screening and assessment, and interventions for older adults related to fall risk are listed in the tables below.
Risk Factors for Falls in Older PersonsNon-modifiable Risk Factors Modifiable Risk Factors
Age older than 80 yearsArthritisCognitive impairment/dementiaFemale sexHistory of cerebrovascular accident or transient ischemic attackHistory of fallsHistory of fracturesRecently discharged from hospital (within one month)
Environmental hazardsMedications (especially psychoactive)Polypharmacy (four or more prescription medications)
Metabolic factors Dehydration Diabetes mellitus Low body mass index
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
66
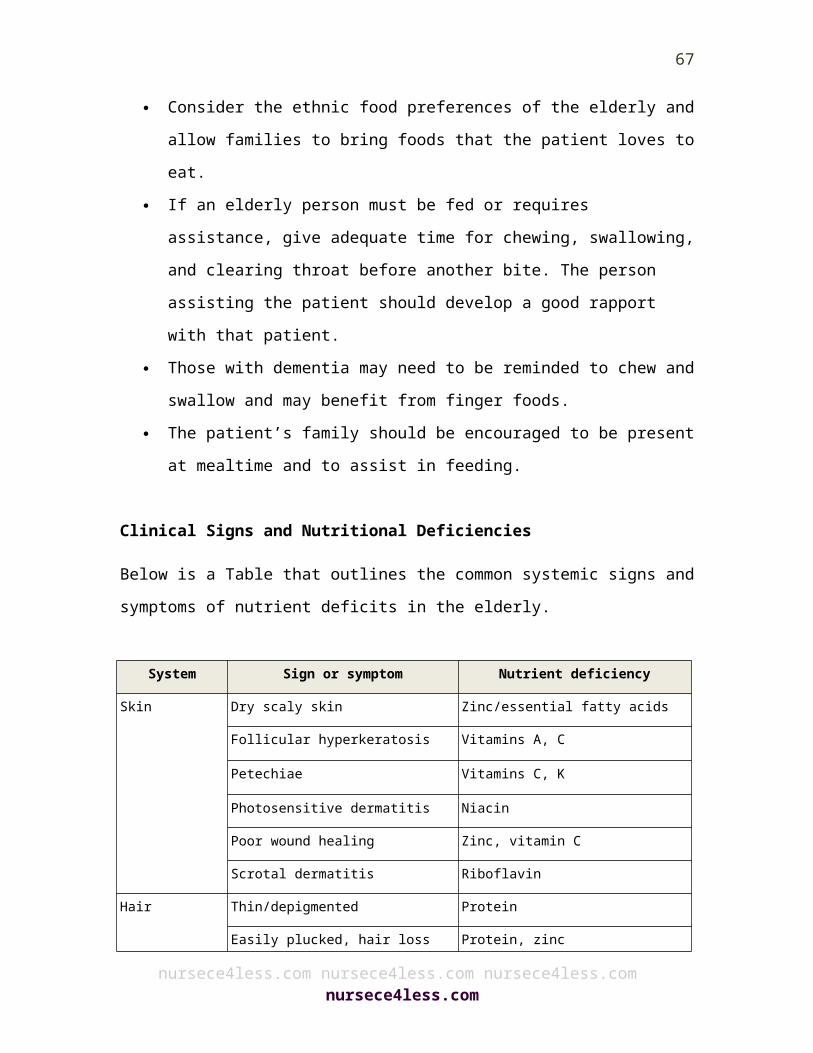
Vitamin D deficiency
Musculoskeletal factors Balance impairment Foot problems Gait impairment Impaired activities of daily living Lower extremity muscle weakness Musculoskeletal pain Use of assistive device
Neuropsychologic factors Delirium Depression Dizziness or vertigo Fear of falling Parkinson disease Peripheral neuropathy
Sensory impairment Auditory impairment Multifocal lens use Visual impairment
Other Acute illness Alcohol intoxication Anemia Cardiac arrhythmia Inappropriate footwear Obstructive sleep apnea Orthostatic hypotension Urinary incontinence
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
67
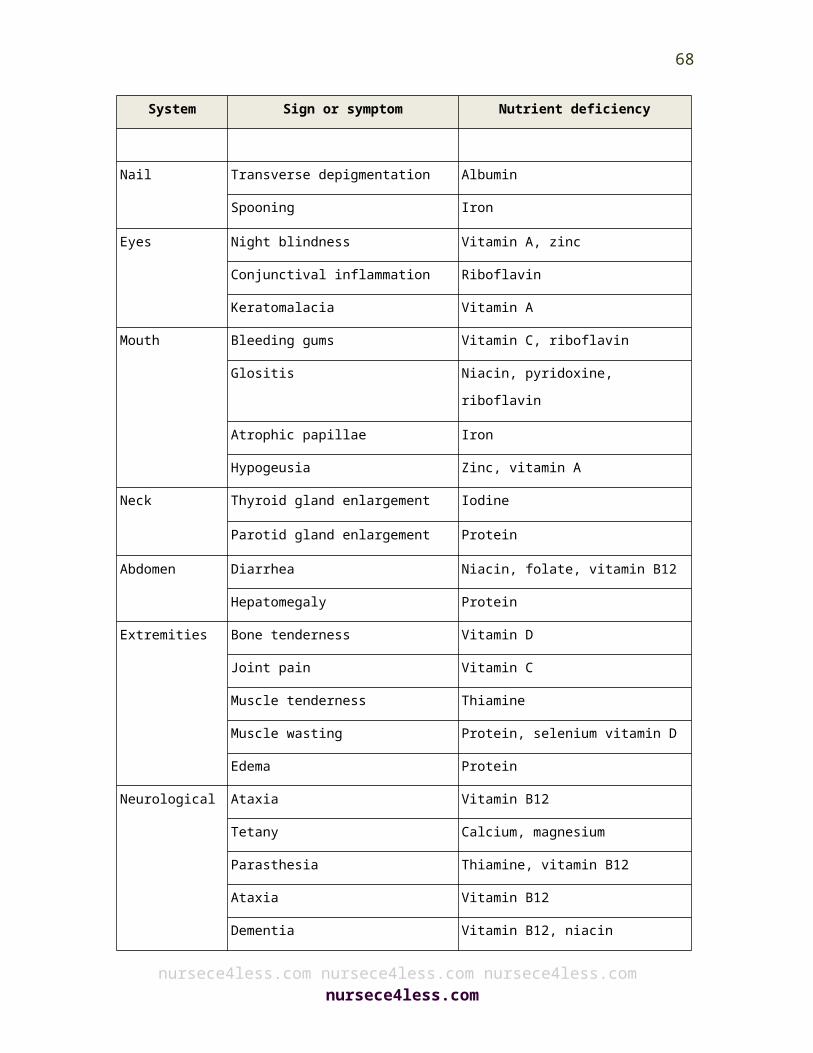
Screening and Assessment1. The elderly patient should be asked about his or her history of falls during
the past year.2. An elderly person who reports a fall should be asked about the frequency
and circumstances of the fall(s).3. The elderly should be asked about their difficulties with walking or balance.4. The elderly who present for medical attention due to a fall, report a history
of recurrent falls in the past one-year, or report problems in walking or balance should undergo a multifactorial fall risk assessment.
5. Older persons presenting with a single fall should be evaluated for gait and balance.
6. The elderly who have fallen must be assessed for gait and balance.7. The elderly who are unable to perform or perform poorly on a standardized
gait and balance test should be provided a multifactorial fall risk assessment.
8. A multifactorial fall risk assessment is also needed for elderly who exhibit unsteadiness.
9. A fall risk assessment is not required for an elderly person who has only had a single fall and has no significant difficulties with balance, gait or unsteadiness.
10. Only a clinician (or clinicians) with appropriate skills and training should assess the elderly.
11. The multifactorial fall risk assessment must encompass the following:
Focused Historya. History of falls in detail b. Medication review: c. History of relevant risk factors.
Physical Examinationsa. Comprehensive assessment of gait, balance, and mobility levels and
lower extremity joint functionb. Neurological function including assessment of cognition,
proprioception, lower extremity peripheral nerves, reflexes, assessment of extrapyramidal , cortical, and cerebellar function
c. Muscle strength (lower extremities)d. Cardiovascular status
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
68
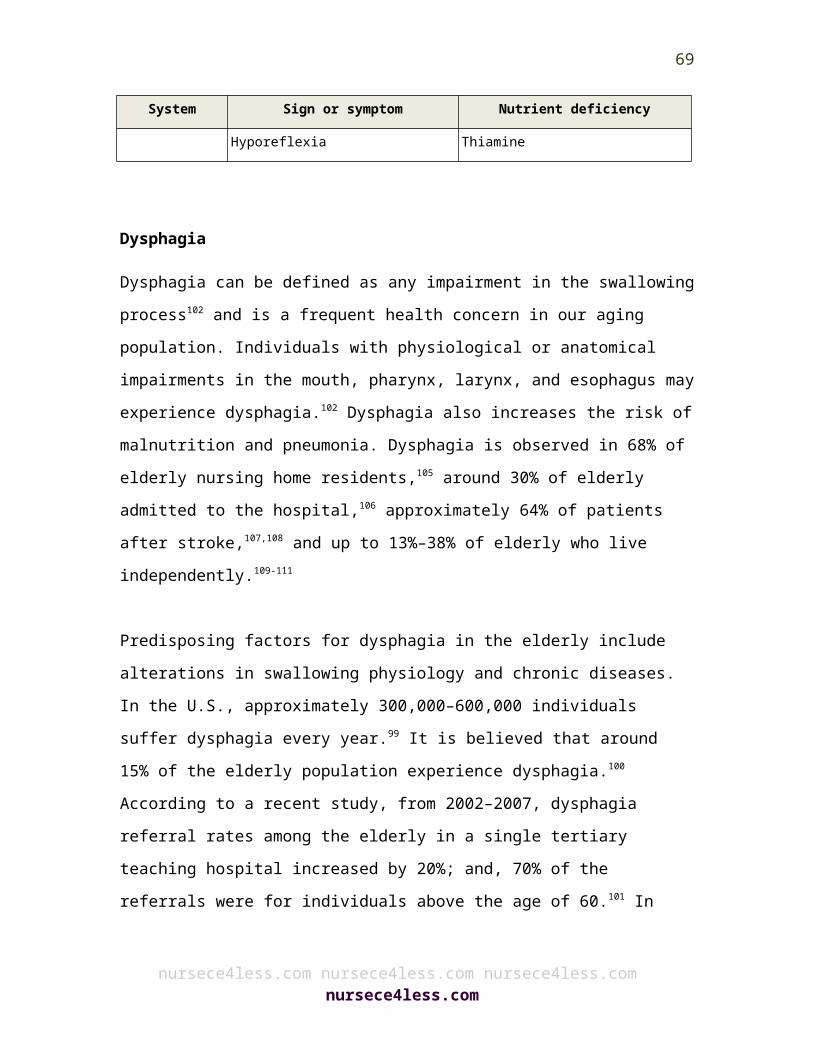
e. Assessment of visual acuityf. Examination of the feet and footwear
Functional Assessmenta. Assessment of activities of daily living (ADL) skills b. Assessment of the individual's perceived functional ability and fear
related to falling
Environmental Assessmenta. Environmental assessment including home safety.
Interventions: Elderly Living In the Community1. After a thorough multifactorial fall risk assessment, direct interventions should
be initiated tailored to the identified risk factors, together with an optimal exercise program.
2. A strategy to reduce the risk of falls should include multifactorial assessment of known fall risk factors and management of the risk factors identified.
3. The components most commonly included in efficacious interventions were: Adaptation or modification of home environment Withdrawal or minimization of psychoactive medications Withdrawal or minimization of other medications Management of postural hypotension Management of foot problems and footwear Exercise, particularly balance, strength, and gait training
4. All elderly individuals who are at risk of falling should be provided an exercise program that encompasses balance, gait, and strength training. Flexibility and endurance training should also be preferably included, but not as sole components of the program.
5. Intervention should include an educational component complementing and addressing issues specifically pertaining to the intervention being provided, tailored to individual cognitive function and language.
6. All such interventions should be carried out by healthcare professionals and other qualified healthcare professionals.
7. If indicated, psychoactive drugs/medications and should either be minimized or withdrawn, with appropriate tapering.
8. The aim should be to reduce either the total number of medications or dose of the medication medications. All medications should be reviewed, and if
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
69
required minimized or withdrawn.9. Exercise should be included for fall prevention in community-residing elderly. 10. An exercise program such as Tai Chi or physical therapy that targets strength,
gait and balance, is an effective intervention for the reduction of falls. 11. Exercise programs should be individualized according to the physical abilities
and health profile of the elderly. Qualified health professionals or fitness instructors should recommend programs.
12. An older person should not wear multifocal lenses when walking, especially on stairs.
13. Postural hypotension in the elderly should be should be adequately treated.14. Dual chamber cardiac pacing should be considered for elderly with
cardioinhibitory carotid sinus hypersensitivity that experience unexplained recurrent falls.
15. Those elderly who have proven vitamin D deficiency should be supplemented with vitamin D supplements with at least 800 IU per day; and, least 800 IU per day should be offered to elderly with suspected vitamin D deficiency or who are otherwise at an increased risk for falls.
16. Foot problems should be investigated and optimal treatment should be provided to those elderly living in the community.
17. The elderly should be advised that walking with shoes of low heel height and high surface contact area may reduce the risk of falls.
18. Health care professionals should carry out home environment assessment. Intervention should also encompass a multifactorial assessment and intervention for those elderly who have fallen or who are prone to falls.
19. The intervention should encompass removal of recognized hazards in the home, and evaluation and interventions to promote the safe performance of daily activities.
20. Educational and informational programs are an important component of a multifactorial intervention for the elderly.
OLDER PERSONS IN LONG-TERM CARE FACILITES1. Multifactorial interventions to reduce the risk of falls should be
contemplated for those elderly in long-term care settings. 2. Exercise programs should also be contemplated to reduce the risk of falls in
those elderly living in long-term care settings. Special care is needed to reduce the risk of injury in frail individuals.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
70
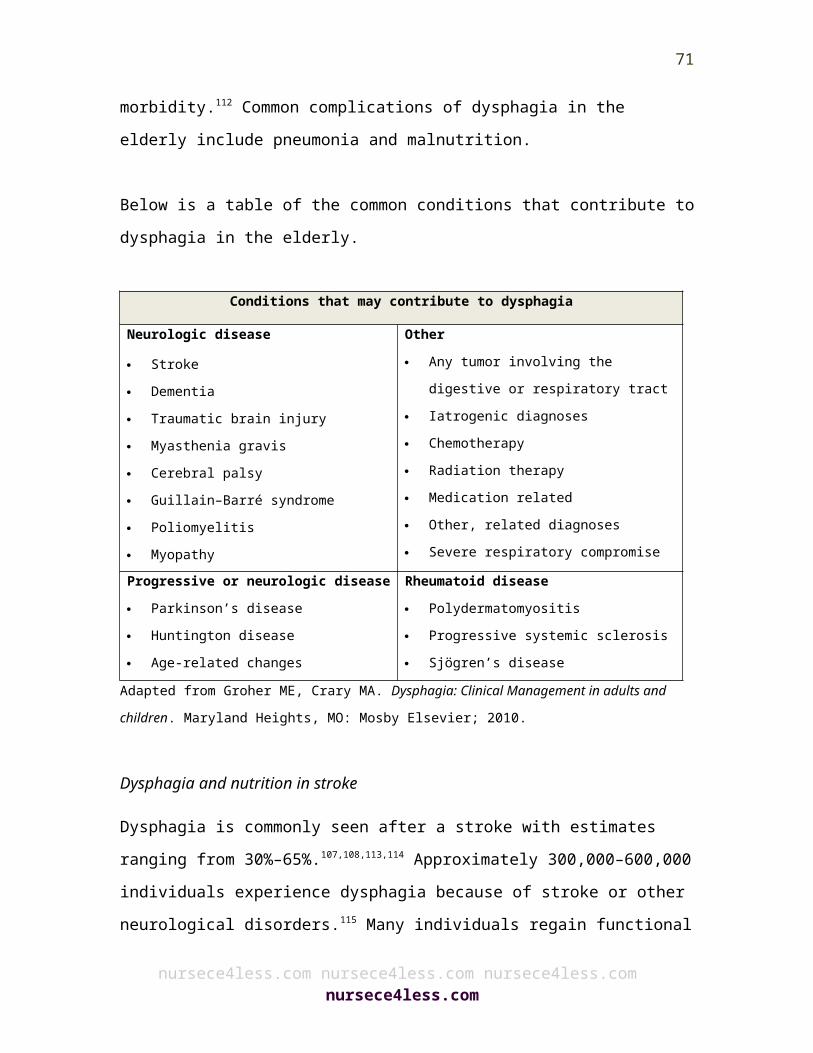
3. Vitamin D supplements (minimum of 800 IU per day) should be given to those elderly living in long-term care settings with suspected or proven vitamin D deficiency.
4. Vitamin D supplements (minimum of 800 IU per day) should be considered in those elderly residing in long-term care settings who have impaired gait or balance or who are otherwise are susceptible to falls.
Summary
The population in the U.S. is getting older and, in the coming decades, the trend will only increase. Between 2010 and 2050, it is expected that in the U.S. there will be a rapid growth in its older population. By 2050, it is expected that the total national population aged 65 and older will reach 88.5 million, which is more than two fold its population in 2010. Between 2010 and 2050, the 65+ population will rise rapidly. This growth in the elderly population will far exceed the growth in younger age groups or categories. As the US ages, the demand for long-term care for elderly will increase dramatically and the need for health services to help the elderly will grow exponentially. It is the families, relatives and friends of the elderly that provide most of the long-term care required. Medicaid provides long-term care financing for low-income families. However, long-term care continues to be a major challenge for the country and especially the elderly.
It is estimated that the demand for long-term care among the elderly will increase to more than double in the next three decades. LTC for the elderly encompasses a wide variety of services that includes non-medical as well as medical care. It also caters to the health or personal needs of the elderly.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
71

Long-term care assists the elderly with various types of support services such as activities of daily living. It can also be provided at home, in the community, in nursing homes, or in assisted living. The need for LTC is impacted by changes in the physical, mental, and/or cognitive functional capacities of the elderly, which in turn are greatly influenced by the environment. The type and duration of LTC are a complex issue and usually difficult to predict. The goal of LTC is to make sure that an elderly individual who is not fully capable of long-term self-care can maintain the highest possible quality of life, with a high degree of independence, participation, autonomy, individual fulfillment, and dignity.
Home-based LTC encompasses health, personal, and other types of support services to help the elderly stay at home and live independently as much as possible. This type of care is usually provided either in the home of the elderly person or at a family member's home. Trained caregivers that receive compensation are also available for home-based LTC services. Home healthcare may include nursing care to help an individual recover from surgery, an injury, or illness. Homemaker services can be availed even without a provider's recommendation. Nursing homes provide a comprehensive range of medical services, which includes 24-hour supervision and nursing care. Skilled nursing care is provided on a physician’s recommendation and requires the professional skills of a registered nurse or a licensed practical nurse. Intermediate nursing care is provided under periodic medical supervision and encompasses physical, psychological, social, and other restorative services. Individuals without medical training can offer personal or custodial care.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
72
Community-based LTC such as home health care, assisted living facility, adult day care, respite care, and hospice care can be offered in many types of settings and by many kinds of care providers. Assisted living facilities provide care to individuals in a residential facility and include supportive services, personal care, and/or nursing services. Adult day care is care provided in a nonresidential, community-based group program that caters to the needs of functionally impaired elderly. Respite care offers personal care, supervision, or other services to a debilitated individual to provide temporary relief to a patient’s care provider and family member. Hospice care primarily offers symptom and pain management, and supportive services to terminally ill individuals and their families. Hospice is a form of palliative care for terminally ill individuals. LTC hospitals are acute care hospitals, but also focus on providing care to patients who stay in the facility for more than 25 days.
In the older population, malnutrition is an important issue. Malnutrition is the state of being poorly nourished due to under-nutrition, for example the lack of one or more nutrients; or, over nutrition, such as an excess of nutrients. The causes of malnutrition among older people are varied, and they can be categorized into three main types: medical, social, and psychological. Management of malnutrition in the elderly focuses early on offering ample food choices and high calorie food after which additional caloric supplements can be considered.
Dysphagia is a frequent health concern in our aging population. Video fluoroscopy is considered to be the gold standard used to study dysphagia. Successful and optimal swallowing interventions or techniques can help in the management of complication related to dysphagia malnutrition and pneumonia. A number of dysphagia
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
73
management techniques and tools can be used for the treatment of dysphagia.
Comorbid conditions complicate the care of the elderly. Often these conditions contribute to falls. Fall risk in the older population is caused by complex interactions among various multiple risk factors, which may be characterized as intrinsic or extrinsic. Elderly patients and their families need to be adequately educated about health risk factors and prevention, such as fall risk, to avoid complications and further loss of health.
Please take time to help the NURSECE4LESS.COM course planners evaluate nursing knowledge needs met following completion of this course by
completing the self-assessment Knowledge Questions after reading the article. Correct Answers, page 80.
1. In the U.S., most elderly long-term care is provided by:a. Medicareb. Medicaidc. Family, relatives and friendsd. None of the above
2. Older age is associated with an increased prevalence of:a. chronic diseases and sensory dysfunctionb. changes in cognition c. poor balance and increased rate of falls and injuries
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
74
d. all of the above
3. True or False. Impaired cognition in the elderly has no correlation to the ability or desire to eat.a. Trueb. False
4. Elderly individuals with pneumonia frequently experience:a. more symptoms than young adultsb. aspiration pneumonia detected late, and under-diagnosedc. tachypnea or increased respiratory rate as an early sign d. answers b and c above
5. To evaluate the older adult for malnutrition, a helpful mnemonic is: a. M-E-A-L-S-O-N-W-H-E-E-L-Sb. G-O-O-D-N-U-T-R-I-T-I-O-Nc. D-I-E-T-F-O-R-L-I-F-Ed. E-L-D-E-R-W-E-L-L-N-E-S-S
6. Basic laboratory work-up for the elderly includes:a. CMP, sedimentation rate and CRPb. complete blood count, CMP, thyroid panelc. thyroid profile, liver function test, cardiac enzymesd. Genetic testing to determine medication efficacy
7. Most common conditions associated with anemia in the elderly include: a. Iron deficiency anemia b. Vitamin B12 and folate deficiencyc. Hypercalcemia
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
75
d. Answers a and b above
8. Treatment of vitamin B12 deficiency includes:a. 1000 IU of vitamin B12 orally dailyb. 500 IU of vitamin B12 orally/injections every other dayc. 1000 IU of vitamin B12 injections weekly for 4 weeksd. answers a and c above
9. True or False. Dysphagia management in the elderly also help in the management of malnutrition and pneumonia.a. Trueb. False
10. True or False. Falls in the elderly include factors related to seizure, sudden onset of paralysis, or an external force.a. Trueb. False
Correct Answers:1. c2. d3. b4. d5. a6. b7. d8. d9. a10. b
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
76
Footnotes:1. Y. Gorina and H. Lentzner, “Multiple causes of death in old age,” Aging Trends,
no. 9, pp. 1–9, 2008.2. C. F. Dillon, Q. Gu, H. J. Hoffman, and C. W. Ko, “Vision, hearing, balance, and
sensory impairment in Americans aged 70 years and over: United States, 1999–2006,” NCHS Data Brief, no. 31, pp. 1–8, 2010.
3. Administration on Aging, “A profile of older americans: 2009, disability and activity limitations, ”http://www.aoa.gov/AoARoot/Aging_Statistics/Profile/2009/16.aspx.
4. R. H. Lawrence, S. L. Tennstedt, L. E. Kasten, J. Shih, J. Howland, and A. M. Jette, “Intensity and correlates of fear of falling and hurting oneself in the next year: baseline findings from a roybal center fear of falling intervention,” Journal of Aging and Health, vol. 10, no. 3, pp. 267–286, 1998.
5. B. J. Vellas, S. J. Wayne, L. J. Romero, R. N. Baumgartner, and P. J. Garry, “Fear of falling and restriction of mobility in elderly fallers,” Age and Aging, vol. 26, no. 3, pp. 189–193, 1997
6. Federal Interagency Forum on Aging-Related Statistics, “Older Americans 2010: key indicators of well-being,” Hyattsville, Md, USA
7. Kaye H, Harrington C, LaPlante M. Long-Term Care: Who Gets It, Who Provides It, Who Pays, And How Much? Health Affairs. January 2010 2010; 29(1):11-21.
8. Administration on Aging (AoA). A Profile of Older Americans: 2009. 2010; http://www.aoa.gov/ AoARoot/Aging_Statistics/Profile/2009/4.aspx.
9. PEW Research Center. 10,000 - Baby Boomers Retire. http://pewresearch.org/databank/ dailynumber/?NumberID=1150.
10. U.S. Census Bureau, Population Division. Table 2. Projections of the Population by Selected Age Groups and Sex for the United States: 2010 to 2050 (NP2008-T2) 2008; www.census.gov.
11. Murphy S, Xu J, Kochanek K. Deaths: Preliminary Data for 2010. National Vital Statistics Reports 2012; http://www.cdc.gov/nchs/data/nvsr/nvsr60/nvsr60_04.pdf..
12. Glover J. United States Life Tables: 1890,1901,1910, and 1901-1910. 1921; http://www.cdc.gov/ nchs/data/lifetables/life1890-1910.pdf.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
77
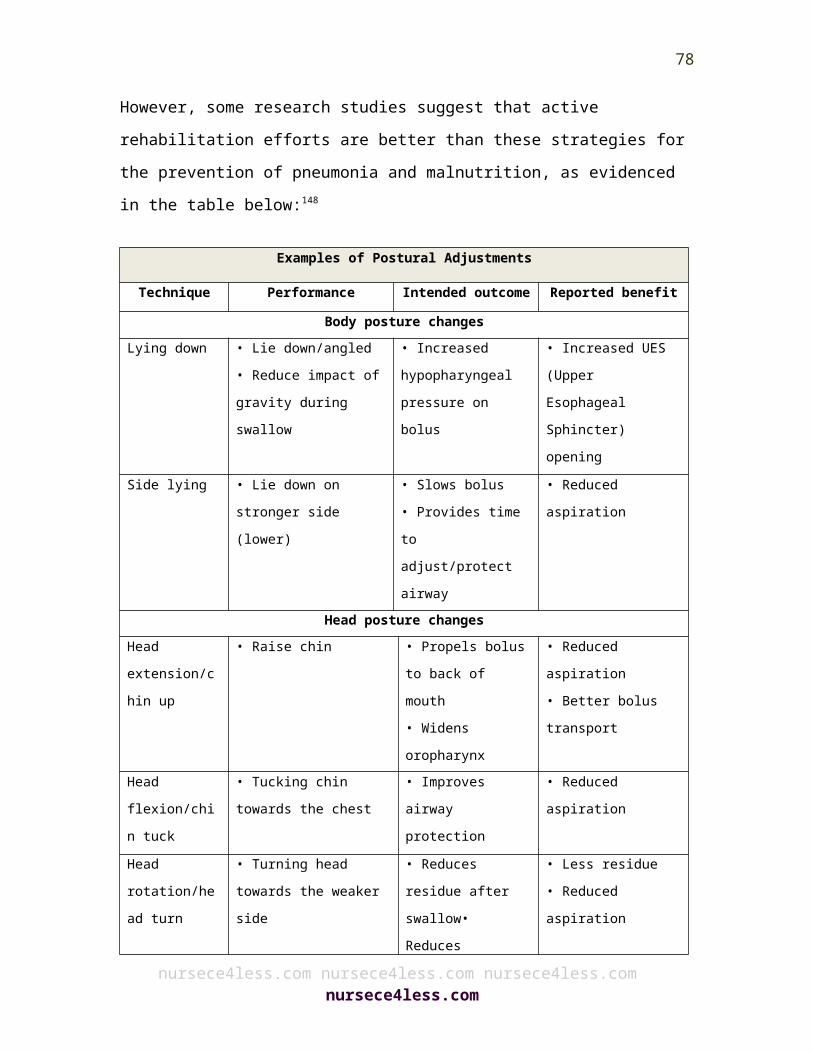
13. Anderson G. Chronic Care: Making the Case for Ongoing Care. 2010; http://www.rwjf.org/files/ research/50968chronic.care.chartbook.pdf.
14. Medical Expenditure Panel Survey, 2006. 15. Alzheimer’s Association. 2012 Alzheimer’s Disease Facts and Figures,
Alzheimer’s & Dementia, Volume 8, Issue 2. http://www.alz.org/downloads/Facts_Figures_2012.pdf
16. "Defusing the demographic "time-bomb" in Germany." Bull World Health Organ 2012;90:6–7 | doi:10.2471/BLT.12.020112
17. Health Canada. Long-Term Facilities-Based Care. 18. Saltman, R.B., Dubois, H.F.W. and Chawla, M. (2006). The impact of aging on
long-term care in Europe and some potential policy responses, International Journal of Health Services, 36(4): 719-746.
19. Jones AL, Dwyer LL, Bercovitz AR, Strahan GW. The National Nursing Home Survey: 2004 overview. Vital Health Stat 13. 2009;(167):1–155.
20. WHO. World Health Day–toolkit for organizers. Available from:http://www.who.int/world.health.day/2012/toolkit/background/en/index.html .
21. Office of National Statistics. Population trends. PT 118, table 1.4 (population age and sex). London: ONS, 2004.
22. Office for National Statistics. Living in Britain: results from the 2002 General Household Survey. London: ONS, 2004.
23. Kyle UG, Genton L, Hans D, et al. Total body mass, fat mass, fat-free mass, and skeletal muscle in older people: cross-sectional differences in 60-year-old persons. J Am Geriatr Soc 2001;49:1633–40.
24. Baumgartner RN, Stauber PM, McHugh D, et al. Cross-sectional age differences in body composition in persons 60+ years of age. J Gerontol A Biol Sci Med Sci 1995;50:M307–16.
25. Silver AJ, Guillen CP, Kahl MJ, et al. Effect of aging on body fat. J Am Geriatr Soc 1993;41:211–13.
26. Enzi G, Gasparo M, Biondetti PR, et al. Subcutaneous and visceral fat distribution according to sex, age, and overweight, evaluated by computed tomography. Am J Clin Nutr 1986;44:739–46.
27. Kuczmarski RJ. Need for body composition information in elderly subjects. Am J Clin Nutr 1989;50(suppl 5):1150–7.
28. Forbes GB, Reina JC. Adult lean body mass declines with age: some longitudinal observations. Metabolism 1970;19:653–63.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
78
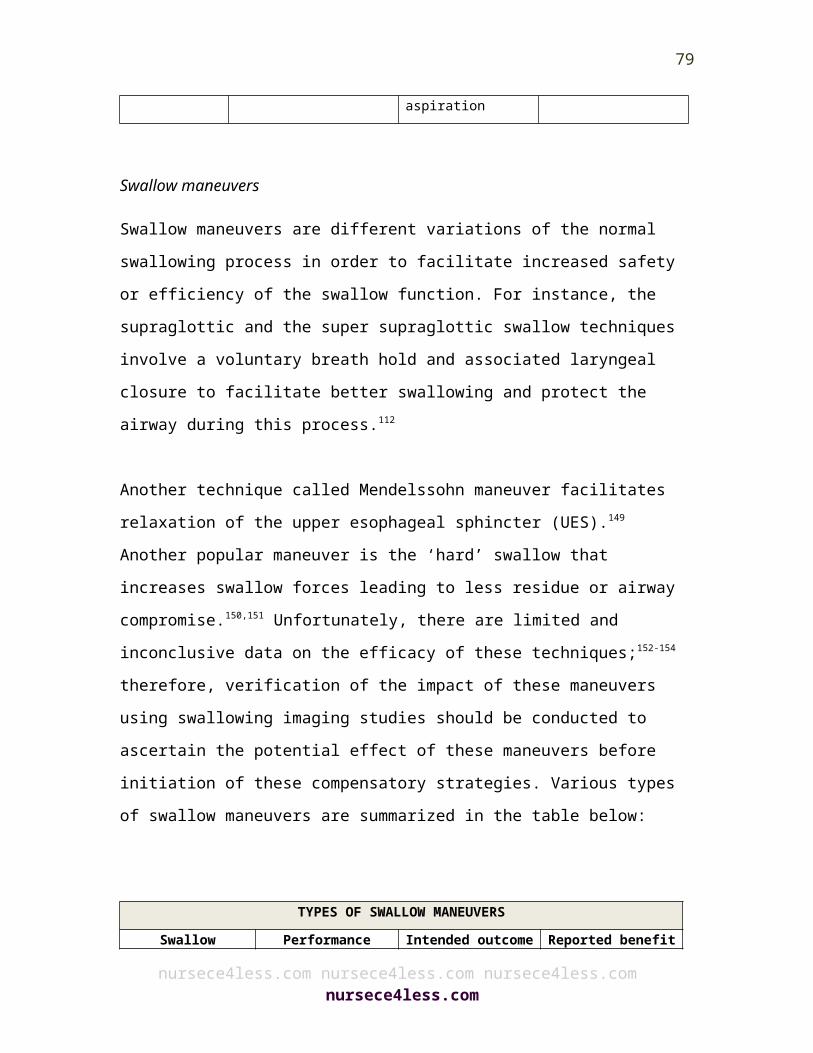
29. Novak LP. Aging, total body potassium, fat-free mass, and cell mass in males and females between ages 18 and 85 years. J Gerontol 1972;27:438–43.
30. Broadwin J, Goodman-Gruen D, Slymen D. Ability of fat and fat-free mass percentages to predict functional disability in older men and women. J Am Geriatr Soc 2001;49:1641–5.
31. Landers KA, Hunter GR, Wetzstein CJ, et al. The interrelationship among muscle mass, strength, and the ability to perform physical tasks of daily living in younger and older women. J Gerontol A Biol Sci Med Sci 2001;56:B443–8.
32. Yeh SS, Schuster MW. Geriatric cachexia: the role of cytokines. Am J Clin Nutr 1999;70:183–97.
33. Corish CA, Kennedy NP. Protein-energy undernutrition in hospital in-patients. Br J Nutr 2000;83:575–91.
34. Finch S, Doyle W, Lowe C, et al. National Diet and Nutrition Survey: people aged 65 years and over, Vol 1.Report of the diet and nutrition survey. London: The Stationery Office, 1998.
35. Edington J, Kon P, Martyn CN. Prevalence of malnutrition in patients in general practice. Clin Nutr 1996;15:60–3.
36. Landi F, Zuccala G, Gambassi G, et al. Body mass index and mortality among older people living in the community. J Am Geriatr Soc 1999;47:1072–6.
37. Gariballa SE, Sinclair AJ. Nutrition, aging and ill health. Br J Nutr 1998;80:7–23.38. Delmi M, Rapin CH, Bengoa JM, et al. Dietary supplementation in elderly
patients with fractured neck of the femur. Lancet 1990;335:1013–16.39. Robinson G, Goldstein M, Levine GM. Impact of nutritional status on DRG length
of stay. JPEN 1987;11:49–51.40. Friedmann JM, Jensen GL, Smiciklas WH, et al. Predicting early nonelective
hospital readmission in nutritionally compromised older adults. Am J Clin Nutr 1997;65:1714–20.
41. de Groot CP, van Staveren WA, de Graaf C. Determinants of macronutrient intake in elderly people. Eur J Clin Nutr 2000;54(suppl 3):S70–6.
42. Wakimoto P, Block G. Dietary intake, dietary patterns, and changes with age: an epidemiological perspective. J Gerontol A Biol Sci Med Sci 2001;56:65–80.
43. de Groot CP, van den BT, van Staveren W. Energy intake and micronutrient intake in elderly Europeans: seeking the minimum requirement in the SENECA study. Age Aging 1999;28:469–474.
44. Das SK, Moriguti JC, McCrory MA, et al. An underfeeding study in healthy men and women provides further evidence of impaired regulation of energy expenditure in old age. J Nutr 2001;131:1833–8.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
79
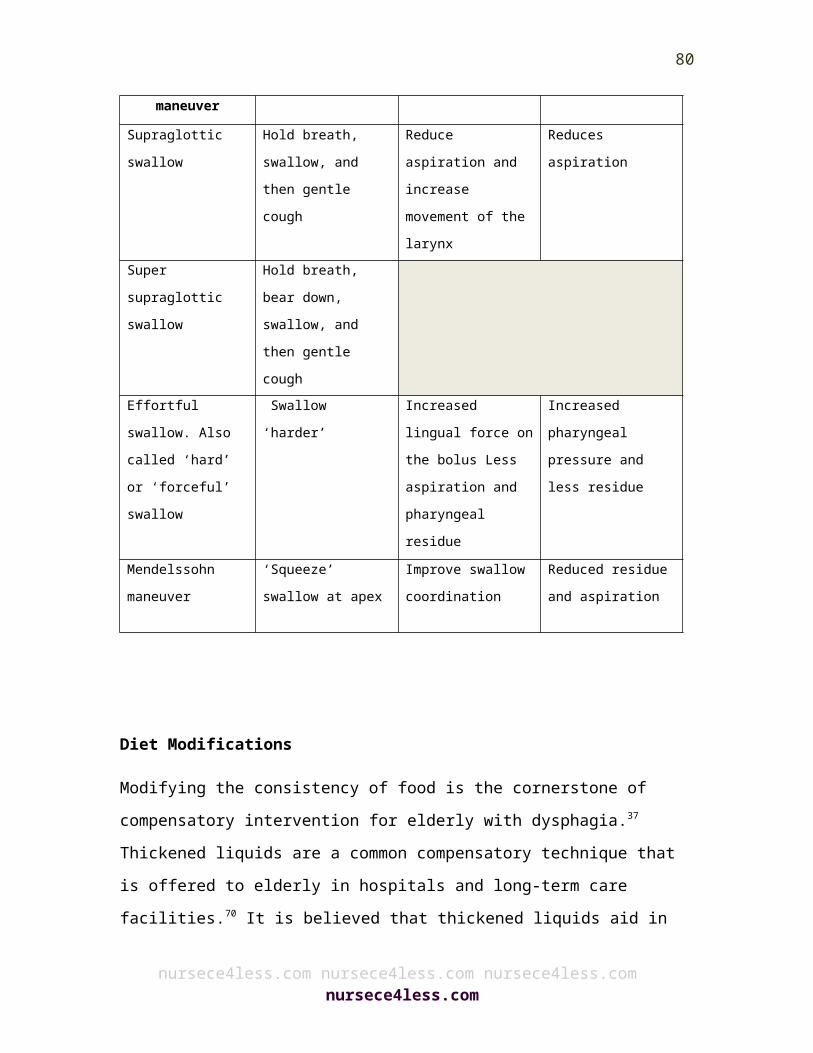
45. Clarkston WK, Pantano MM, Morley JE, et al. Evidence for the anorexia of aging: gastrointestinal transit and hunger in healthy elderly vs. young adults. Am J Physiol 1997;272:R243–8.
46. Morley JE. Decreased food intake with aging. J Gerontol A Biol Sci Med Sci 2001;56:81–8.
47. De Castro JM. Age-related changes in spontaneous food intake and hunger in humans. Appetite 1993;21:255–72.
48. Chapman IM, I. Endocrinology of anorexia of aging. Baillieres Clin Endocrinol Metab 2004;18:437–52.
49. Hetherington MM. Taste and appetite regulation in the elderly. Proc Nutr Soc 1998;57:625–31.
50. Schiffman SS. Taste and smell losses in normal aging and disease. JAMA 1997;278:1357–62.
51. Duffy VB, Backstrand JR, Ferris AM. Olfactory dysfunction and related nutritional risk in free-living, elderly women. J Am Diet Assoc 1995;95:879–84.
52. Schiffman SS. Intensification of sensory properties of foods for the elderly. J Nutr 2000;130(suppl 4):927–30S.
53. Mathey MF, Siebelink E, de Graaf C, et al. Flavor enhancement of food improves dietary intake and nutritional status of elderly nursing home residents. J Gerontol A Biol Sci Med Sci 2001;56:M200–5.
54. P. E. Petersen, “The World Oral Health Report 2003: Continuous improvement of oral health in the 21st century—The approach of the WHO Global Oral Health Programme,” Community Dentistry and Oral Epidemiology, vol. 31, no. 1, pp. 3–24, 2003.
55. J. G. Steele, A. E. Sanders, G. D. Slade et al., “How do age and tooth loss affect oral health impacts and quality of life? a study comparing two national samples,” Community Dentistry and Oral Epidemiology, vol. 32, no. 2, pp. 107–114, 2004.
56. E. Musacchio, E. Perissinotto, P. Binotto et al., “Tooth loss in the elderly and its association with nutritional status, socio-economic and lifestyle factors,” Acta Odontologica Scandinavica, vol. 65, no. 2, pp. 78–86, 2007
57. Keller HH. Malnutrition in institutionalized elderly: how and why? J Am Geriatr Soc 1993;41:1212–18.
58. Payette H, Gray-Donald K, Cyr R, et al. Predictors of dietary intake in a functionally dependent elderly population in the community. Am J Public Health 1995;85:677–83.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
80
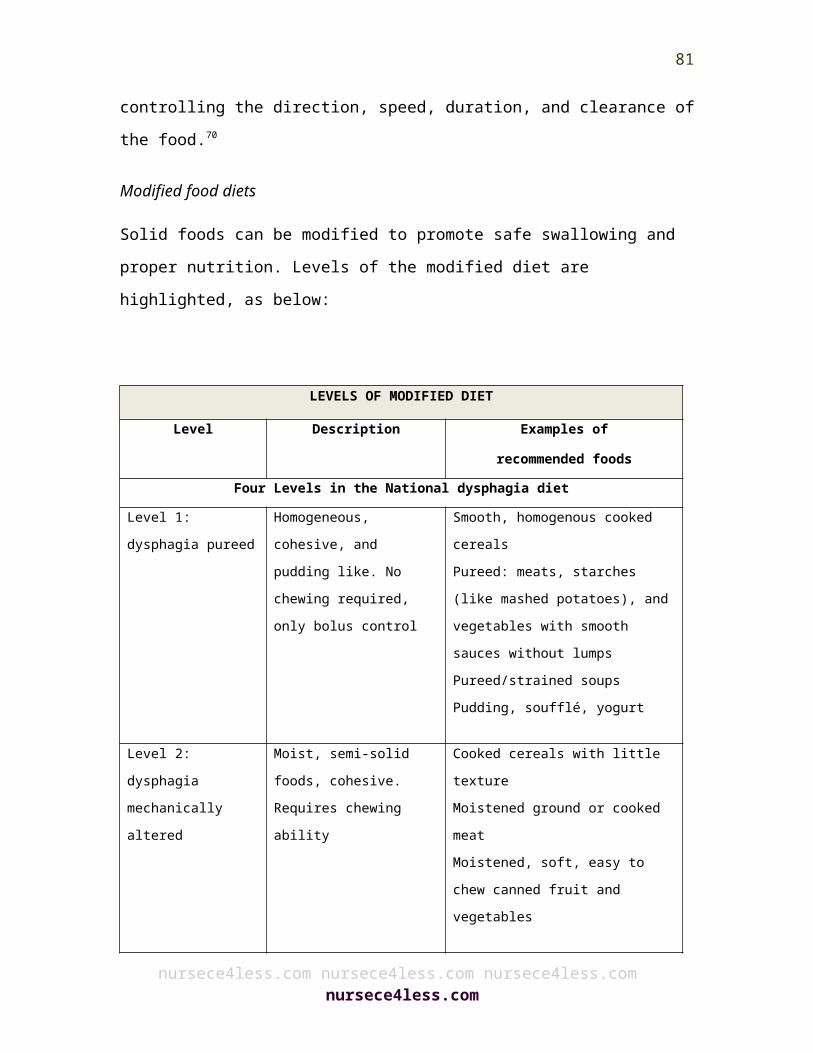
59. Incalzi RA, Capparella O, Gemma A, et al. Inadequate caloric intake: a risk factor for mortality of geriatric patients in the acute-care hospital. Age Aging 1998;27:303–10.
60. Claggett MS. Nutritional factors relevant to Alzheimer’s disease. J Am Diet Assoc 1989;89:392–6.
61. Volicer L, Seltzer B, Rheaume Y, et al. Progression of Alzheimer-type dementia in institutionalised patients: a cross sectional study. J Appl Gerontol 1987;6:83–94.
62. Priefer BA, Robbins J. Eating changes in mild-stage Alzheimer’s disease: a pilot study. Dysphagia 1997;12:212–21.
63. Berkhout AMM, Cools HJM, van Houwelingen HC. The relationship between difficulties in feeding oneself and loss of weight in nursing home patients with dementia. Age Aging 1998;27:637–41.
64. Blaum CS, Fries BE, Fiatarone MA. Factors associated with low body mass index and weight loss in nursing home residents. J Gerontol A Biol Sci Med Sci 1995;50:M162–8.
65. Thompson MP, Morris LK. Unexplained weight loss in the ambulatory elderly. J Am Geriatr Soc 1991;39:497–500.
66. Westin T, Jansson A, Zenckert C, et al. Mental depression is associated with malnutrition in patients with head and neck cancer. Arch Otolaryngol Head Neck Surg 1988;114:1449–53.
67. Rosenbloom CA, Whittington FJ. The effects of bereavement on eating behaviors and nutrient intakes in elderly widowed persons. J Gerontol 1993;48:S223–9.
68. Feldblum I, et al. Characteristics of undernourished older medical patients and the identification of predictors for undernutrition status. Nutr J. 2007;6:37.
69. Morley JE, et al. Nutritional deficiencies in long-term care: Part I. Detection and diagnosis. Ann Long-Term Care. 2004;12(Suppl 2):S1-S7.
70. White H. Weight loss in advanced Alzheimer's disease, Part I. Contributing factors and evaluation. Ann Long-Term Care: Clinical Care and Aging. 2004;12(5):33-37.
71. DiMaria-Ghalili RA, Guenter PA. The mini nutritional assessment. Am J Nurs. 2008;108(2):50-59.
72. Bagley B. Nutrition and health. Am Fam Physician. 1998;57(5):933-934.73. Yesavage JA. Geriatric depression scale. Psychopharmacol Bull. 1988;24(4):709-
711.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
81
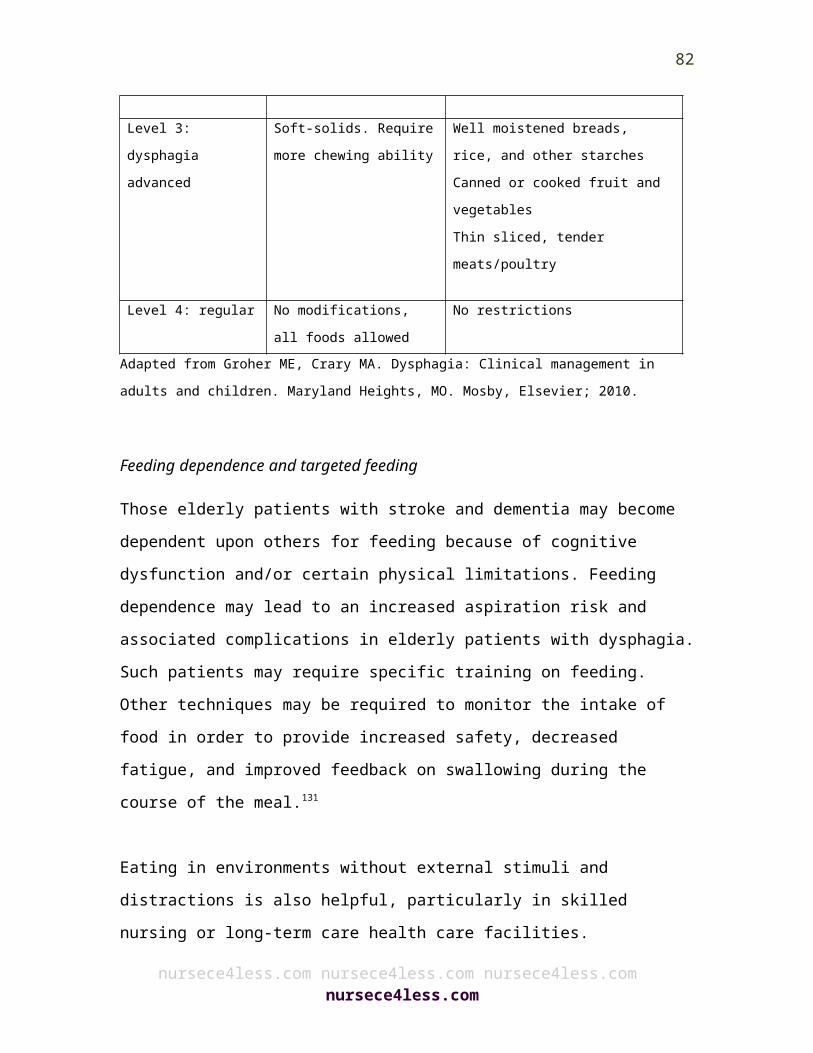
74. Carolan Doerflinger DM. How to try this: the mini-cog. Am J Nurs. 2007;107(12):62-71.
75. Borson S, et al. The Mini-Cog as a screen for dementia: validation in a population-based sample. J Am Geriatr Soc. 2003;51(10):1451-1454.
76. Thomas DR. Introduction to Weight Loss in Older Persons. Malvern, Pa.: HMP Communications; 2007.
77. Thomas DR, et al. Nutritional management in long-term care: development of a clinical guideline. Council for Nutritional Strategies in Long-Term Care. J Gerontol A Biol Sci Med Sci. 2000;55(12):725-734.
78. Wolfe RR. The Danger of Weight Loss in the Elderly. Malvern, Pa.: HMP Communications; 2007.
79. Flood M, Newman AM. Obesity in older adults: synthesis of findings and recommendations for clinical practice. J Gerontol Nurs. 2007;33(12):19-35.
80. Alpers DH, Klein S. Approach to the patient requiring nutritional supplementation. In Yamada T, ed. Textbook of Gastroenterology, 4th edn. Baltimore: Lippincott Williams & Wilkins, 2003
81. Jeejeebhoy KN, Baker JP, Wolman SL, et al. Critical evaluation of the role of clinical assessment and body composition studies in patients with malnutrition and after total parenteral nutrition. Am J Clin Nutr 1982;35:1117 -27
82. Gariballa SE, Sinclair AJ. Nutrition, aging and ill health. Br J Clin Nutr1998;80:7 -23
83. Gariballa S. Nutrition and older people: special considerations relating to nutrition and aging. Clin Med2004;4:411 -14
84. Wallace JI. Malnutrition and enteral/parenteral alimentation. In: Hazzard WR, Blass JP, Ettinger WH Jr, Halter JB, Ouslander JG, editors. Principles of geriatric medicine and gerontology. 4th ed. New York: McGraw-Hill; 1999. pp. 1455–69.
85. Endoy MP. Anorexia among older adults. American Journal for Nurse Practitioners. 2005 May;9(5):31–8.
86. Milne AC, Potter J, Vivanti A, Avenell A. Protein and energy supplementation in elderly people at risk from malnutrition. Cochrane Database Syst Rev 2009; 15 (2): CD003288.
87. Morley JE, Argiles JM, Evans WJ et al. Nutritional recommendations for the management of sarcopenia. J Am Med Dir Assoc 2010; 11: 391–6.
88. Wilson MM, Purushothaman R, Morley JE. Am J Clin Nutr 2002; 75: 944–7.89. Nijs K, de Graaf C, van Staveren WA, de Groot LC. Malnutrition and mealtime
ambiance in nursing homes. J AmMed Dir Assoc 2009; 10: 226–9.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
82
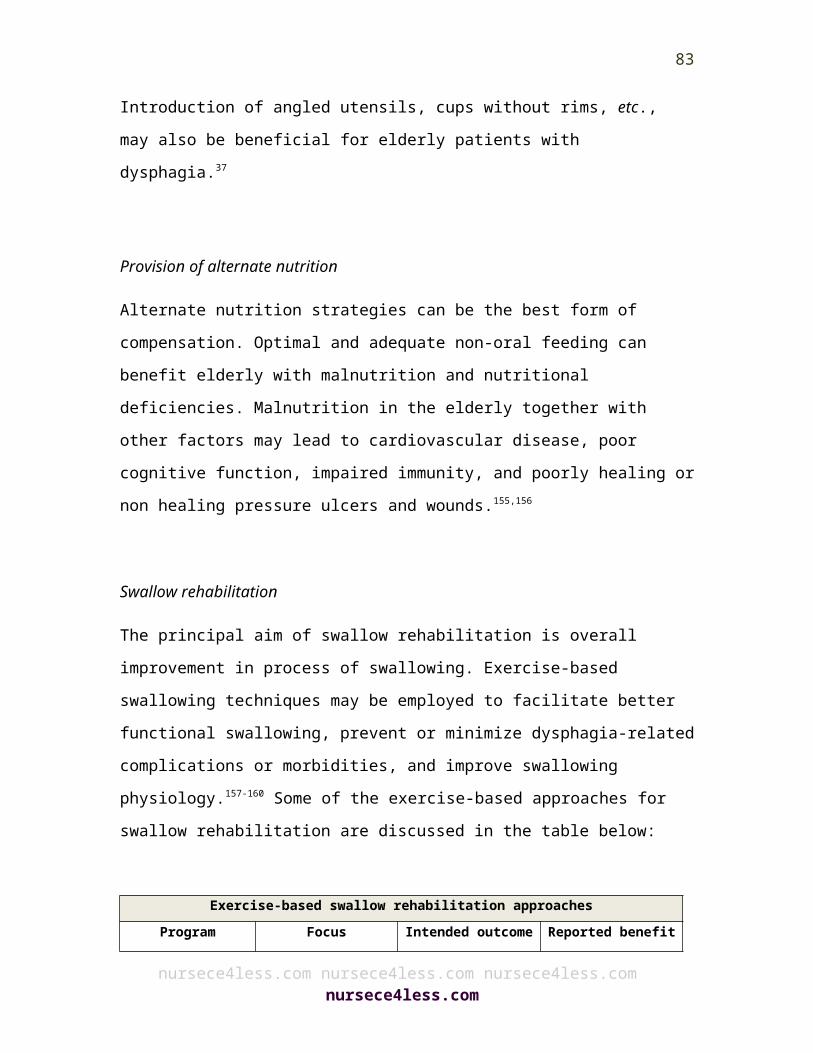
90. Keller HH, Gibbs-Ward A, Randall-Simpson J et al. Meal rounds: an essential aspect of quality nutrition services in long-term care. J Am Med Dir Assoc 2006; 7: 40–5.
91. Rahman AN, Simmons SF. Individualizing nutritional care with between-meal snacks for nursing home residents. J Am Med Dir Assoc 2005; 6: 215–8.
92. Berenstein EG, Ortiz Z. Megestrol acetate for the treatment of anorexia- cachexia syndrome. Cochrane Database Syst Rev 2005; 18 (2): CD004310.
93. Navari RM, Brenner MC. Treatment of cancer-related anorexia with olanzapine and megestrol acetate: a randomized trial. Support Care Cancer 2010; 18: 951–6.
94. Chapman IM, Visvanathan R, Hammond AJ et al. Effect of testosterone and a nutritional supplement, alone and in combination, on hospital admissions in undernourished older men and women. Am J Clin Nutr 2009; 89: 880–9.
95. Perry HM 3rd, Horowitz M, Morley JE et al. Longitudinal changes in serum 25-hydroxyvitamin D in older people. Metabolism 1999; 48: 1028–32.
96. Argento V, Roylance J, Skudlarska B et al. Anemia prevalence in a home visit geriatric population. J Am Med Dir Assoc 2008; 9: 422–6.
97. Niewoehner CB, Allen JI, Boosalis M et al. Role of zinc supplementation in type II diabetes mellitus. Am J Med 1986; 81:63–8.
98. Huffman GB. Evaluating and treating unintentional weight loss in the elderly. Am Fam Physician. 2002 Feb 15;65(4):640–50.
99. US Department of Health and Human Services. Agency for Healthcare Research and Quality. Diagnosis and treatment of swallowing disorders (dysphagia) in acute-care stroke patients. Evidence report/technology assessment (Summary). Archived EPC Evidence Reports. 1999:1–6.
100. Barczi SR, Sullivan PA, Robbins J. How should dysphagia care of older adults differ? Establishing optimal practice patterns. Semin Speech Lang. 2000;21:347–361.
101. Leder SB, Suiter DM. An epidemiologic study on aging and dysphagia in the acute care hospitalized population: 2000–2007. Gerontology. 2009;55:714–718.
102. Crary MA, Groher ME. Introduction to Adult Swallowing Disorders. Philadelphia, PA: Butterworth Heinemann; 2003.
103. Logemann JA, Stewart C, Hurd J, Aschman D, Matthews N. Diagnosis and Management of Dysphagia in Seniors. 2008. Available at: http://americandysphagianetwork.org/physician_education_course.
104. Fucile S, Wright PM, Chan I, Yee S, Langlais ME, Gisel EG. Functional oral-motor skills: Do they change with age? Dysphagia. 1998;13:195–201.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
83
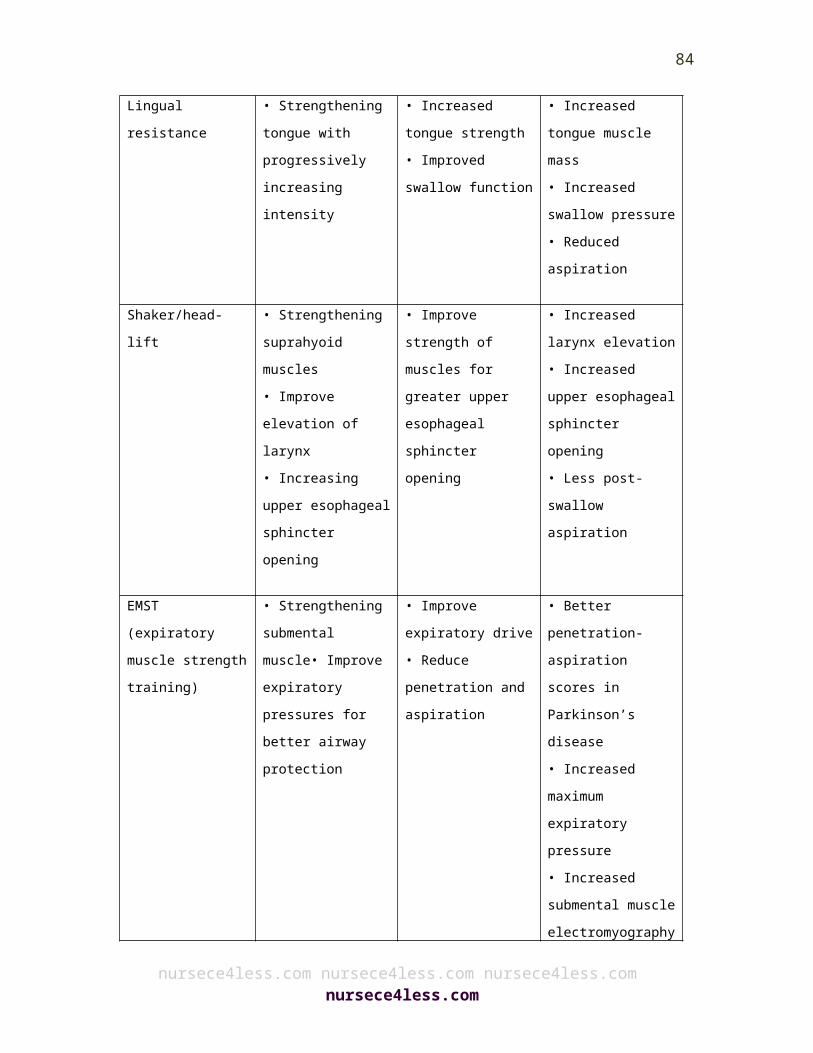
105. Steele CM, Greenwood C, Ens I, Robertson C, Seidman-Carlson R. Mealtime difficulties in a home for the aged: not just dysphagia. Dysphagia. 1997;12:43–50, discussion 51.
106. Lee A, Sitoh YY, Lieu PK, Phua SY, Chin JJ. Swallowing impairment and feeding dependency in the hospitalised elderly. Ann Acad Med Singapore. 1999;28:371–376.
107. Mann G, Hankey GJ, Cameron D. Swallowing function after stroke: prognosis and prognostic factors at 6 months. Stroke. 1999;30:744–748.
108. Smithard DG, O’Neill PA, Parks C, Morris J. Complications and outcome after acute stroke. Does dysphagia matter? Stroke. 1996;27:1200–1204.
109. Kawashima K, Motohashi Y, Fujishima I. Prevalence of dysphagia among community-dwelling elderly individuals as estimated using a questionnaire for dysphagia screening. Dysphagia. 2004;19:266–271.
110. Serra-Prat M, Hinojosa and impaired safety and efficacy of swallow in independently living older persons. J Am Geriatr Soc. 2011;59:186–187.
111. Roy N, Stemple J, Merrill RM G, López D, et al. Prevalence of oropharyngeal dysphagia, Thomas L. Dysphagia in the elderly: preliminary evidence of prevalence, risk factors, and socioemotional effects. Ann Otol Rhinol Laryngol. 2007;116:858–865.
112. Groher ME, Crary MA. Dysphagia: Clinical Management in Adults and Children. Maryland Heights, MO: Mosby Elsevier; 2010.
113. Mann G, Hankey GJ, Cameron D. Swallowing disorders following acute stroke: prevalence and diagnostic accuracy. Cerebrovasc Dis. 2000;10:380–386.
114. Paciaroni M, Mazzotta G, Corea F, et al. Dysphagia following Stroke. Eur Neurol. 2004;51:162–167.
115. Carnaby-Mann G, Lenius K, Crary M. Update on Assessment and Management of Dysphagia Post Stroke. Northeast Florida Medicine. 2007;58:31–34.
116. Smithard DG, Smeeton NC, Wolfe CD. Long-term outcome after stroke: does dysphagia matter? Age Aging. 2007;36:90–94.
117. Altman KW, Yu GP, Schaefer SD. Consequence of dysphagia in the hospitalized patient: impact on prognosis and hospital resources. Arch Otolaryngol Head Neck Surg. 2010;136:784–789
118. Martino R, Foley N, Bhogal S, Diamant N, Speechley M, Teasell R. Dysphagia after stroke: incidence, diagnosis, and pulmonary complications. Stroke. 2005;36:2756–2763.
119. Martino R, Martin RE, Black S. Dysphagia after stroke and its management. CMAJ. 2011.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
84
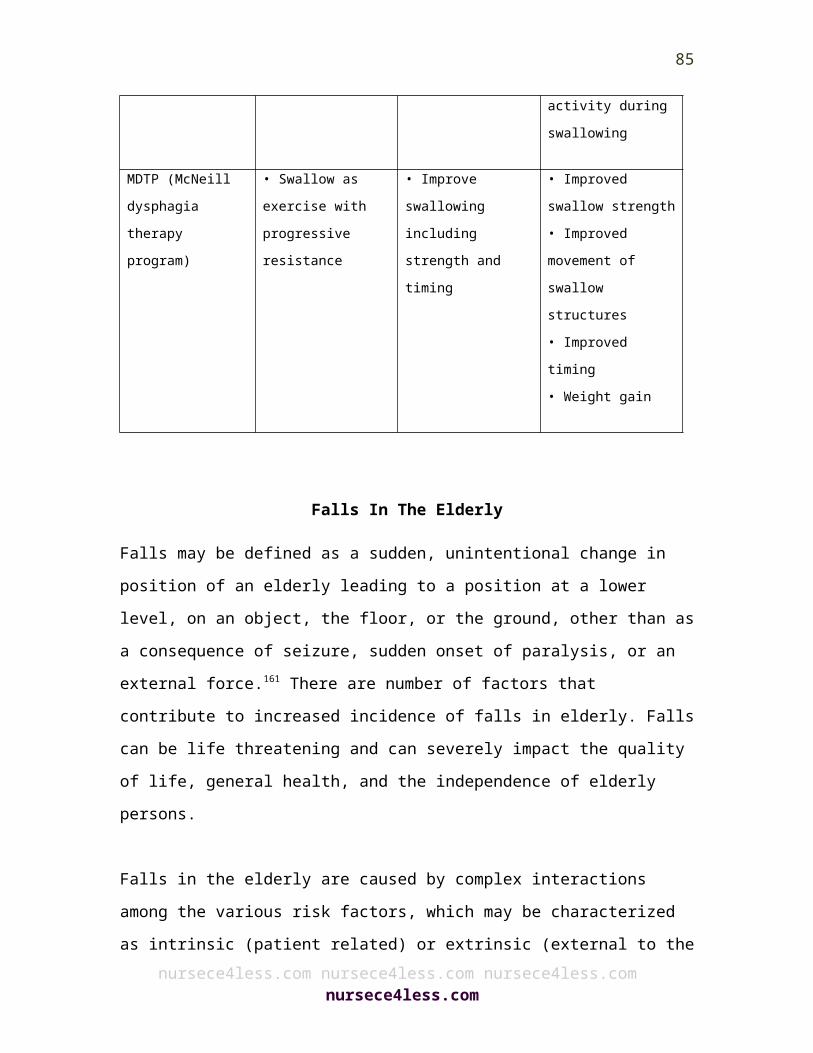
120. Maeshima S, Osawa A, Miyazaki Y, et al. Influence of dysphagia on short-term outcome in patients with acute stroke. Am J Phys Med Rehabil. 2011;90:316–320.
121. Guyomard V, Fulcher RA, Redmayne O, Metcalf AK, Potter JF, Myint PK. Effect of dysphasia and dysphagia on inpatient mortality and hospital length of stay: a database study. J Am Geriatr Soc. 2009;57:2101–2106.
122. Foley NC, Martin RE, Salter KL, Teasell RW. A review of the relationship between dysphagia and malnutrition following stroke. J Rehabil Med. 2009;41:707–713.
123. Axelsson K, Asplund K, Norberg A, Alafuzoff I. Nutritional status in patients with acute stroke. Acta Med Scand. 1988;224:217–224.
124. Davalos A, Ricart W, Gonzalez-Huix F, et al. Effect of malnutrition after acute stroke on clinical outcome. Stroke. 1996;27:1028–1032.
125. Gariballa SE, Parker SG, Taub N, Castleden CM. Influence of nutritional status on clinical outcome after acute stroke. Am J Clin Nutr. 1998;68:275–281.
126. Crary MA, Carnaby-Mann GD, Miller L, Antonios N, Silliman S. Dysphagia and nutritional status at the time of hospital admission for ischemic stroke. J Stroke Cerebrovasc Dis. 2006;15:164–171.
127. Finestone HM, Foley NC, Woodbury MG, Greene-Finestone L. Quantifying fluid intake in dysphagic stroke patients: a preliminary comparison of oral and nonoral strategies. Arch Phys Med Rehabil. 2001;82:1744–1746.
128. Sellars C, Bowie L, Bagg J, et al. Risk factors for chest infection in acute stroke: a prospective cohort study. Stroke. 2007;38:2284–2291.
129. Masiero S, Pierobon R, Previato C, Gomiero E. Pneumonia in stroke patients with oropharyngeal dysphagia: a six-month follow-up study. Neurol Sci. 2008;29:139–145.
130. Pikus L, Levine MS, Yang YX, et al. Videofluoroscopic studies of swallowing dysfunction and the relative risk of pneumonia. Am J Roentgenol. 2003;180:1613–1616.
131. Ney DM, Weiss JM, Kind AJ, Robbins J. Senescent swallowing: impact, strategies, and interventions. Nutr Clin Pract. 2009;24:395–413.
132. Horner J, Alberts MJ, Dawson DV, Cook GM. Swallowing in Alzheimer’s disease. Alzheimer Dis Assoc Disord. 1994;8:177–19.
133. Morley JE. Nutrition in the elderly. Curr Opin Gastroenterol. 2002;18:240–245. 134. Claggett MS. Nutritional factors relevant to Alzheimer’s disease. J Am Diet
Assoc. 1989;89:392–396.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
85
135. Makowska I, Kloszewska I, Grabowska A, Szatkowska I, ymarczyk K. Olfactory deficits in normal aging and Alzheimer’s disease in the Polish elderly population. Arch Clin Neuropsychol. 2011;26:270–279.
136. Serby M, Larson P, Kalkstein D. The nature and course of olfactory deficits in Alzheimer’s disease. Am J Psychiatry. 1991;148:357–360.
137. Zuliani G, Galvani M, Sioulis F, et al. Discharge diagnosis and comorbidity profile in hospitalized older patients with dementia. Int J Geriatr Psychiatry. 2012;27:313–320.
138. Serra-Prat M, Palomera M, Gomez C, et al. Oropharyngeal dysphagia as a risk factor for malnutrition and lower respiratory tract infection in independently living older persons: a population-based prospective study. Age Aging. 2012;41:376–381.
139. Kaplan V, Angus DC, Griffin MF, Clermont G, Scott Watson R, Linde-Zwirble WT. Hospitalized community-acquired pneumonia in the elderly: age- and sex-related patterns of care and outcome in the United States. Am J Respir Crit Care Med. 2002;165:766–772.
140. Marik PE, Kaplan D. Aspiration pneumonia and dysphagia in the elderly. Chest. 2003;124:328–336.
141. Ewig S, Birkner N, Strauss R, et al. New perspectives on community-acquired pneumonia in 388 406 patients. Results from a nationwide mandatory performance measurement programme in healthcare quality. Thorax. 2009;64:1062–1069.
142. Murphy S, Xu J, Kochanek KD. Deaths: Preliminary Data for 2010. National Vital Statistics Report: Center for Disease Control and Prevention; January 11, 2012. Available at: http://www.cdc.gov/nchs/data/nvsr/nvsr60/nvsr60_04.pdf.
143. Almirall J, Bolibar I, Vidal J, et al. Epidemiology of community-acquired pneumonia in adults: a population-based study. Eur Respir J. 2000;15:757–763.
144. Loeb MB, Becker M, Eady A, Walker-Dilks C. Interventions to prevent aspiration pneumonia in older adults: a systematic review. J Am Geriatr Soc. 2003;51:1018–1022.
145. Rofes, L., Arreloa, V., Almirall, J., Cabre, M., Campins, L., Garcia-Peris, P., Speyer, R., & Clave P. (2011). Diagnosis and management of oropharyngeal dysphagia and its nutritional and respiratory complications in the elderly. Gastroenterology Research and Practice. Volume 2011, 1-13. oi:10.1155/2011/818979
146. Leder, S.B., Suiter, D.M., Warner, H.L., Acton, L.M., & Swainson, B.A. (2012). Success of recommending oral diets in acute stroke patients based on passing
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
86
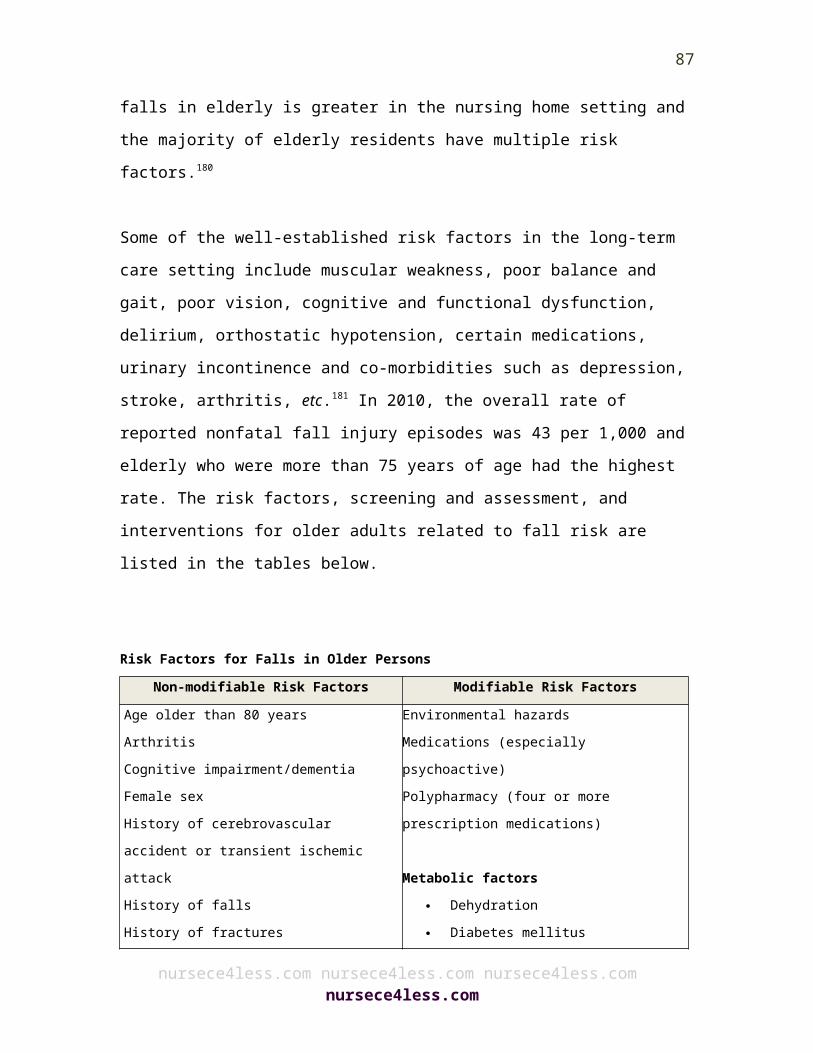
a 90-cc water swallow challenge protocol. Topics in Stroke Rehabilitation, 19(1), 40-44.
147. Rasley A, Logemann JA, Kahrilas PJ, Rademaker AW, Pauloski BR, Dodds WJ. Prevention of barium aspiration during videofluoroscopic swallowing studies: value of change in posture. Am J Roentgenol. 1993;160:1005–1009.
148. Carnaby G, Hankey GJ, Pizzi J. Behavioural intervention for dysphagia in acute stroke: a randomised controlled trial. Lancet Neurol. 2006;5:31–37.
149. Kahrilas PJ, Logemann JA, Krugler C, Flanagan E. Volitional augmentation of upper esophageal sphincter opening during swallowing. AM J Physiol. 1991;260:G450–G456.
150. Hind JA, Nicosia MA, Roecker EB, Carnes ML, Robbins J. Comparison of effortful and noneffortful swallows in healthy middle-aged and older adults. Arch Phys Med Rehabil. 2001;82:1661–1665.
151. Huckabee ML, Butler SG, Barclay M, Jit S. Submental surface electromyographic measurement and pharyngeal pressures during normal and effortful swallowing. Arch Phys Med Rehabil. 2005;86:2144–2149.
152. Elmstahl S, Bulow M, Ekberg O, Petersson M, Tegner H. Treatment of dysphagia improves nutritional conditions in stroke patients. Dysphagia. 1999;14:61–66.
153. Neumann S, Bartolome G, Buchholz D, Prosiegel M. Swallowing therapy of neurologic patients: correlation of outcome with pretreatment variables and therapeutic methods. Dysphagia. 1995;10:1–5.
154. Carnaby-Mann GD, Crary MA. Adjunctive neuromuscular electrical stimulation for treatment-refractory dysphagia. Ann Otol Rhinol Laryngol. 2008;117:279–287.
155. Chandra RK. Nutrition and the immune system: an introduction. Am J Clin Nutr. 1997;66:460S–463S.
156. Hengstermann S, Fischer A, Steinhagen-Thiessen E, Schulz RJ. Nutrition status and pressure ulcer: what we need for nutrition screening. J Parenter Enteral Nutr. 2007;31:288–294.
157. Robbins J, Gangnon RE, Theis SM, Kays SA, Hewitt AL, Hind JA. The effects of lingual exercise on swallowing in older adults. J Am Geriatr Soc. 2005;53:1483–1489.
158. Carnaby-Mann G, Crary MA, Schmalfuss I, Amdur R. “Pharyngocise”: Randomized Controlled Trial of Preventative Exercises to Maintain Muscle Structure and Swallowing Function During Head-and-Neck Chemoradiotherapy. Int J Radiat Oncol Biol Phys. 2011;83:210–219.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
87

159. Carnaby-Mann GD, Crary MA. McNeill dysphagia therapy program: a case-control study. Arch Phys Med Rehabil. 2010;91:743–749.
160. Crary MA, Carnaby GD, Lagorio LA, Carvajal PJ. Functional and Physiological Outcomes from an Exercise-Based Dysphagia Therapy: A Pilot Investigation of the McNeill Dysphagia Therapy Program. Arch Phys Med Rehabil. 2012.
161. Feder G, Cryer C, Donovan S, Carter Y. Guidelines for the prevention of falls in people over 65. The Guidelines’ Development Group. BMJ. 2000;321(7267):1007–1011.
162. Kannus P, Sievänen H, Palvanen M, Järvinen T, Parkkari J. Prevention of falls and consequent injuries in elderly people. Lancet. 2005;366:1885-93. [PMID: 16310556]
163. Tinetti ME. Clinical practice. Preventing falls in elderly persons. N Engl J Med. 2003;348:42-9.
164. Connell BR, Wolf SL. Environmental and behavioral circumstances associated with falls at home among healthy elderly individuals. Atlanta FICSIT Group. Arch Phys Med Rehabil. 1997;78:179-86.
165. Centers for Disease Control and Prevention (CDC). Self-reported falls and fall-related injuries among persons aged > or = 65 years—United States, 2006. MMWR Morb Mortal Wkly Rep. 2008;57:225-9.
166. Rubenstein LZ, Josephson KR. The epidemiology of falls and syncope. Clin Geriatr Med. 2002;18:141-58.
167. Centers for Disease Control and Prevention (CDC). Fatalities and injuries from falls among older adults-United States, 1993-2003 and 2001-2005. MMWR Morb Mortal Wkly Rep. 2006;55:1221-4.
168. Public health surveillance of 1990 injury control objectives for the nation. MMWR CDC Surveill Summ. 1988;37:1-68.
169. Guideline for the prevention of falls in older persons. American Geriatrics Society, British Geriatrics Society, and American Academy of Orthopaedic Surgeons Panel on Falls Prevention. J Am Geriatr Soc. 2001;49:664-72.
170. Englander F, Hodson TJ, Terregrossa RA. Economic dimensions of slip and fall injuries. J Forensic Sci. 1996;41:733-46.
171. National Institute for Health and Clinical Excellence. Falls: The Assessment and Prevention of Falls in Older People. London: National Institute for Health and Clinical Excellence; 2004.
172. Rubenstein L. Falls in older people: epidemiology, risk factors and strategies for prevention. Age Aging. 2006;35:ii37–ii41. doi: 10.1093/aging/afl084.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
88
173. Rubenstein LZ, Josephson KR. The epidemiology of falls and syncope. Clin Geriatr Med.2002;18:141–158. doi: 10.1016/S0749-0690(02)00002-2.
174. Nurmi IS, Luthje PM, Kataja JM. Long-term survival after falls among the elderly In institutional care. Arch Gerontol Geriatr. 2004;38:1–10.
175. Stevens JA, Corso PS, Finkelstein EA, Miller TR. The costs of fatal and non-fatal falls among older adults. Inj Prev. 2006;12:290–295. doi: 10.1136/ip.2005.011015.
176. Carroll N, Delafuente J, Cox F, Narayanan S. Fall-related hospitalization and facility costs among residents of institutions providing long-term care. Gerontologist. 2008;48:213–222. doi: 10.1093/geront/48.2.213.
177. van den Berg M, Castellote J, Mahillo-Fernandez I, Pedro-Cuesta J. Incidence of spinal cord injury worldwide: a systematic review. Neuroepidemiology. 2010;34:184–192. doi: 10.1159/000279335.
178. Cumming R, Salkeld G, Thomas M, Szonyi G. Prospective study of the impact of fear of falling on activities of daily living, Sf-36 Scores, and nursing home admission. J Gerontol A Biol Sci Med Sci. 2000;55:M299–M305. doi: 10.1093/gerona/55.5.M299.
179. Tinetti M, Powell L. Fear of falling and low self-efficacy: a case of dependence in elderly persons.J Gerontol. 1993;48:35–38. doi: 10.1093/geronj/48.Special_Issue.35.
180. Becker C, Rapp K. Fall prevention in nursing homes. Clin Geriatr Med. 2010;26:693–704. doi: 10.1016/j.cger.2010.07.004.
181. Rubenstein LZ, Josephson KR, Robbins AS. Falls in the nursing home. Ann Intern Med.1994;121:442–451.
182. McGlone J, Gupta S, Humphrey D, Oppenheimer S, Mirsen T, Evans DR. Screening for early dementia using memory complaints from patients and relatives. Arch Neurol. 1990;47:1189-93.
183. Ha¨nninen T, Reinikainen KJ, Helkala EL, Koivisto K, Mykka¨nen L, Laakso M, et al. Subjective memory complaints and personality traits in normal elderly subjects. J Am Geriatr Soc. 1994;42:1-4.
184. O’Hara MW, Hinrichs JV, Kohout FJ, Wallace RB, Lemke JH. Memory complaint and memory performance in the depressed elderly. Psychol Aging. 1986;1:208-14.
185. Tierney MC, Szalai JP, Snow WG, Fisher RH. The prediction of Alzheimer disease. The role of patient and informant perceptions of cognitive deficits. Arch Neurol. 1996;53:423-7
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
89

186. Turvey CL, Schultz S, Arndt S, Wallace RB, Herzog R. Memory complaint in a community sample aged 70 and older. J Am Geriatr Soc. 2000;48:1435-41.
187. Federal Interagency Forum on Aging Related Statistics: Older Americans 2004: Key Indicators of Well-Being. http://www.agingstats.gov/chartbook2004/population.html
188. Hebert LE, Scherr PA, Bienias JL, Bennett DA, Evans DA. Alzheimer disease in the U.S. population: Prevalence estimates using the 2000 Census. Archives of Neurology2003;60(8):1119–22.
189. Seshadri S, Wolf PA, Beiser A, Au R, McNulty K, White R, et al. Lifetime risk of dementia and Alzheimer’s disease. The impact of mortality on risk estimates in the Framingham Study. Neurology 1997;49(6):1498–504.
190. Hebert LE, Scherr PA, McCann JJ, Beckett LA, Evans DA. Is the risk of developing Alzheimer’s disease greater for women than for men? American Journal of Epidemiology 2001;153(2):132–6.
191. Hebert LE, Beckett LA, Scherr PA, Evans DA. Annual incidence of Alzheimer disease in the United States projected to the years 2000 through 2050. Alzheimer Disease & Associated Disorders 2001;15(4):169–73.
192. U.S. Census Bureau. Current Population Reports, Special Studies, P23-209, 65+ in the United States: 2005. U.S. Government Printing Office, ed. Washington, D.C., 2005.
193. Centers for Disease Control and Prevention and The Merck Company Foundation. The State of Aging and Health in America, 2007. Whitehouse Station, N.J.: The Merck Company Foundation; 2007.
194. Miniño A, Murphy SL, Xu J, Kochanek K. Deaths: Final Data for 2008. National Vital Statistics Reports, Hyattsville, Md.; National Center for Health Statistics, 2011.
195. Arrighi HM, Neumann PJ, Lieberburg IM, Townsend RJ. Lethality of Alzheimer disease and its impact on nursing home placement. Alzheimer Disease & Associated Disorders 2010;24(1):90–5.
196. Mitchell SL, Teno JM, Miller SC, Mor V. A national study of the location of death for older persons with dementia. Journal of the American Geriatrics Society 2005;53(2):299–305.
197. Unpublished tabulations based on data from the Medicare Current Beneficiary Survey for 2008. Prepared under contract by Julie Bynum, M.D., M.P.H., Dartmouth Institute for Health Policy and Clinical Care, Dartmouth Medical School, November 2011.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
90
198. Prepared under contract by Julie Bynum, M.D., M.P.H., Dartmouth Institute for Health Policy and Clinical Care, Dartmouth Medical School, November 2011.
199. MetLife Mature Market Institute. Market Survey of Long-Term Care Costs: The 2011 MetLife Market Survey of Nursing Home, Assisted Living, Adult Day Services, and Home Care Costs. New York, N.Y.: Metropolitan Life Insurance Company, 2011.
200. Fortinsky RH, Fenster JR, Judge JO. Medicare and Medicaid home health and Medicaid waiver services for dually eligible older adults: Risk factors for use and correlates of expenditures. Gerontologist 2004;44(6):739–49.
201. Hirdes JP, Fries BE, Morris JN, Ikegami N, Zimmerman D, Dalby DM, et al. Home care quality indicators (HCQIs) based on the MDS-HC. Gerontologist 2004;44(5):665–79.
202. Mitchell G, Salmon JR, Polivka L, Soberon-Ferrer H. The relative benefits and cost of Medicaid home- and community based services in Florida. Gerontologist 2006:46(4):483–94.
203. Partners in Care giving. A National Study of Adult Day Services, 2001-2002. Winston-Salem, N.C.: Wake Forest University School of Medicine, 2002.
204. O’Keeffe J, Siebenaler K. Adult Day Services: A Key Community Service for Older Adults. U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, Washington, D.C., July 2006.
205. American Health Care Association. Nursing Facility Patient Characteristics Report. Table 12: Medical Condition: Mental Status, June 2011.
206. American Health Care Association. LTC Stats: Nursing Facility Operational Characteristics Report. Table 5: Nursing Facility Beds in Dedicated Special Care Units, June 2011.
207. "Practical Tips for Daily Life | UCSF Memory and Aging Center". Memory.ucsf.edu. Retrieved 2012-08-17.
208. Salmans, Sandra (1997). Depression: Questions You Have – Answers You Need. People's Medical Society.
209. Alexopoulos G. Pharmacotherapy of depressive disorders in older patients. Minneapolis: McGraw-Hill Healthcare Information, 2001
210. Hasin DS, Goodwin RD, Stinson FS, Grant BF. Epidemiology of major depressive disorder: Results from the National Epidemiologic Survey on Alcoholism and Related Conditions. Arch. Gen.Psychiatr 2005;62:1097–106.
211. U.S. Department of Health and Human Services (1999). Older Adults and Mental Health. In: Mental Health: A Report of the Surgeon General. Available at: http://www.surgeongeneral.gov/library/mentalhealth/chapter5/sec1.html
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
91
212. Chapman DP, Perry GS, Strine TW (2005). The vital link between chronic disease and depressive disorders. Prev Chronic Dis; 2(1):A14.
213. Teresi, J., Abrams, R., Holmes, D., Ramirez, M., & Eimicke, J. (2001). Prevalence of depression and depression recognition in nursing homes. Social Psychiatry and Psychiatric Epidemiology, 36(12), 613-620.
214. Mazure CM, Maciejewski PK, Jacobs SC, Bruce ML. Stressful life events interacting with cognitive/ personality styles to predict late-onset major depression. Am. J. Geriatr. Psychiatry 2002;10:297– 304.
215. Fiske A, Gatz M, Pedersen NL. Depressive symptoms and aging: The effects of illness and non-health related events. J. Gerontol. B Psychol. Sci. Soc. Sci 2003;58:P320–8.
216. Prigerson HG, Frank E, Kasl SV, Reynolds CF, Anderson B, et al. Complicated grief and bereavement related depression as distinct disorders: Preliminary empirical validation in elderly bereaved spouses. Am. J. Psychiatry 1995;152:22–30.
217. Zisook S, Kendler KS. Is bereavement-related depression different than non-bereavement-related depression? Psychol. Med 2007;37:779–94.
218. Cole MG, Dendukuri N. Risk factors for depression among elderly community subjects: A systematic review and meta-analysis. Am. J. Psychiatry 2003;160:1147–56.
219. Torges CM, Stewart AJ, Nolen-Hoeksema S. Regret resolution, aging, and adapting to loss. Psychol. Aging 2008;23:169–80.
220. Umberson D, Wortman CB, Kessler RC. Widowhood and depression: Explaining long-term gender differences in vulnerability. Journal of Health and Social Behavior 1992;33:10–24.
221. Knight BG, Flynn Longmire CV, Dave J, Kim JH, David S. Mental health and physical health of family caregivers for persons with dementia: A comparison of African American and white caregivers. Aging Ment. Health 2007;11:538–46.
222. Schulz R, McGinnis KA, Zhang S, Martire LM, Hebert RS, Beach SR, et al. Dementia patient suffering and caregiver depression. Alzheimer Disease and Associated Disorders 2008;22:170–6.
223. Williamson, GM.; Shaffer, DR. The activity restriction model of depressed affect: Antecedents and consequences of restricted normal activities. In: Williamson, GM.; Shaffer, DR.; Parmelee, PA., editors. Physical illness and Depression in Older Adults: A Handbook of Theory, Research, and Practice. Kluwer Academic/Plenum Publishers; New York: 2000. p. 173-200.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
92

224. Gallo JJ, Anthony JC, Muthén BO. Age differences in the symptoms of depression: A latent trait analysis. J. Gerontol 1994;49:P251–64.
225. Christensen H, Jorm AF, Mackinnon AJ, Korten AE, Jacomb PA, et al. Age differences in depression and anxiety symptoms: A structural equation modelling analysis of data from a general population sample. Psychol. Med 1999;29:325–39.
226. Butters MA, Whyte EM, Nebes RD, Begley AE, Dew MA, et al. The nature and determinants of neuropsychological functioning in late-life depression. Arch. Gen. Psychiatry 2004;61:587–95.
227. Kockler M, Heun R. Gender differences of depressive symptoms in depressed and nondepressed elderly persons. Int. J. Geriatr. Psychiatry 2002;17:65–72.
228. Paradiso S, Vaidya J, Tranel D, Kosier T, Robinson RG. Nondysphoric depression following stroke. Neuropsychiatry. Clin. Neurosci 2008;20:52–61.
229. Ehrt U, Brønnick K, Leentjens AF, Larsen JP, Aarsland D. Depressive symptom profile in Parkinson's disease: A comparison with depression in elderly patients without Parkinson's disease. Int. J. Geriatr. Psychiatry 2006;21:252–8.
230. Park JH, Lee SB, Lee TJ, Lee DY, Jhoo JH, et al. Depression in vascular dementia is quantitatively and qualitatively different from depression in Alzheimer's disease. Dement. Geriatr. Cogn. Disord 2007;23:67–73.
231. L indau ST, Schumm LP, Laumann EO, Levinson W, O’Muircheartaigh CA, Waite LJ. A study of sexuality and health among older adults in the United States. N Engl J Med 2007;357:762–74.
232. Waite LJ, Laumann EO, Das A,Schumm LP. Sexuality: measures of partnerships, practices, attitudes, and problems in the National Social Life, Health and Aging Study. J Gerontol B Psychol Sci Soc Sci 2009;64(Suppl 1):156–66.
233. L indau ST, Gavrilova N. Sex, health, and years of sexually active life gained due to good health: evidence from two US population based cross sectional surveys of aging. BMJ 2010;340:c810.
234. Walsh KE, Berman JR. Sexual Dysfunction in the older woman: an overview of the current understanding and management. Drugs Aging 2004;21:655–75.
235. H oward JR, O’Neill S, Travers C. Factors affecting sexuality in older Australian women: sexual interest, sexual arousal, relationships and sexual distress in older Australian women. Climacteric 2006;9:355–67.
236. Woloski–Wruble AC, Oliel Y, Leefsma M, Hochner-Ceinikier D. Sexual activities, sexual and life satisfaction, and successful aging in women. J Sex Med 2010 Apr 1
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
93
237. DeLamater J, Hyde JS, Fong MC. Sexual satisfaction in the seventh decade of life. J Sex Marital Ther 2008;34:439–54.
238. Hartmann U, Phillippsohn S, Heiser K, Ruffer-Hesse C. Low sexual desire in midlife and older women: personality factors, psychosocial development, present sexuality. Menopause 2004;11(6 Pt 2):726–40.
239. Wylie K, Kenney G. Sexual dysfunction and the aging male. Maturitas 2010;65:23–7.
240. O ’Donnell A, Araujo A, McKinnlay J. The health of normally aging men: The Massachussets Male Aging Study (1987-2004). Experimental Gerontology 2004;39:975–84.
241. Bhasin S, Enzlin P, Coviello A, et al. Sexual dysfunction in men and women with endocrine disorders. Lancet 2007;369:597–611.
242. Basson R, Schultz W. Sexual sequelae of general medical disorders. Lancet 2007;369:409–24.
243. elderabus.org.uk ,244. Administration on Aging. (1998). The national elder abuse incidence study:
Final report.245. Acierno, R., Hernandex-Tejada, M., Muzzy, W., and Steve, K. (2009). The
national elder mistreatment study (NCJ Publication No. 2264560. Washington, DC: U.S. Department of Justice
246. Bulman, P., (April 2010). "Elder abuse emerges form the shadows of public consciousness."NIJ Journal. 265, 4-7.
247. Klein, A., Tobin, T., Salomon, A., and Dubois, J. (2008). A statewide profile of abuse of older women and the criminal justice response (NCJ Publication No. 222459). Washington, DC: U.S. Department of Justice.
248. Choi, N.G., and Mayer, J. (2000). "Elder Abuse, Neglect, and Exploitation." Journal of Gerontological Social Work, 33(4), 5-25. doi:http://dx.doi.org/10.1300/J083v33n02_02
249. Laumann, E.O., Leitsch, S.A., and Waite, L.J. (2008). "Elder mistreatment in the United States: Prevalence estimate from a nationally representative study." Journals of Gerontology: Series B, Psychological Sciences and Social Sciences, 63 (4), S248-S254
250. Rinkler, A.G., (2009). "Recognition and perception of elder abuse by prehospital and hospital-based care providers." Archives of Gerontology and Geriatrics. 48, 110-115.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
94
251. U.S. Department of Health and Human Services, Centers for Medicare and Medicaid Services. (2009) Nursing Home Data Compendium. Washington, D.C.: Author.
252. National Center for Assisted Living. (2009). Assisted Living Resident Profile. Washington DC: Author.
253. Lifespan of Greater Rochester, Inc., Weill Cornell Medical Center of Cornell University. & New York City Department for the Aging. (2011) Under the Radar: New York State Elder Abuse Prevalence Study. New York: Author.
254. Acierno R, Hernandez MA, Amstadter AB, Resnick HS, Steve K, Muzzy W, et al. (2010). Prevalence and correlates of emotional, physical, sexual, and financial abuse and potential neglect in the United States: The national elder mistreatment study. American Journal of Public, 100(2), 292-297.
255. Teaster PB, Dugar T, Mendiondo M, Abner EL, Cecil KA, & Otto JM. (2004). The 2004 survey of adult protective services: Abuse of adults 60 years of age and older. Washington DC: National Center on Elder Abuse.
256. National Research Council. (2003) Elder mistreatment: Abuse, neglect and exploitation in an aging America. Washington, D.C.: The National Academies Press.
257. Lifespan of Greater Rochester, Inc., Weill Cornell Medical Center of Cornell University. & New York City Department for the Aging. (2011) Under the Radar: New York State Elder Abuse Prevalence Study. New York: Author.
258. National Center on Elder Abuse, Westat, Inc. (1998). The national elder abuse incidence study: Final report. Washington D.C.: Authors.
259. Robinson, De Benedictis, Segal. "Elder Abuse and Neglect". Help Guide. Retrieved 15 December 2012.
260. "What is Elder Abuse?" . Administration on Aging. Retrieved 17 December 2012.261. Shilling, D. (2008, November/December). "Improving the court system's
response to elder abuse," Victimization of the Elderly and Disabled, 11, 49, 51-52, 59, 62-63.
262. Nursing Home Abuse Laws (NHAL) 263. Oregon Revised Statutes.264. "Signs and symptoms of elder abuse and neglect in care". Advocare
Incorporated. 265. Robinson, Lawrence; Tina De Benedictis, Jeanne Segal (November 2012). "Elder
abuse and neglect: Warning signs, risk factors, prevention, and help".
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
95
266. Dong X, Simon M, Mendes de Leon C, Fulmer T, Beck T, Hebert L, et al. (2009) Elder self-neglect and abuse and mortality risk in a community-dwelling population. Journal of the American Medical Association, 302(5),517-526.
267. Comijs, H.C., Penninx, B.W.J.H., Knipscheer, K.P.M., & van Tilburg, W. (1999). Psychological distress in victims of elder mistreatment: The effects of social support and coping. Journal of Gerontology, 54B(4), 240-245.
268. Bitondo Dyer C., Pavlik V. N., Murphy K. P., and Hyman D. J. (2000). The high prevalence of depression and dementia in elder abuse or neglect. Journal of the American Geriatrics Society. 48, 205-208.
269. National Committee for the Prevention of Elder Abuse, Virginia Tech, Metlife Mature Market Institute (2011). The metlife study of elder financial abuse: Crimes of occasion, desperation and predation against america's elders. Westport, CT: Authors
270. Dong, X. (2005). "Medical Implications of Elder Abuse and Neglect." Clinics in Geriatric Medicine. 21:293-313.
271. Naila Francis - Dr. Lauren Jodi Van Scoy Poses Critical Questions About Death in First Book - PhillyBlurbs.com - The Intelligencer, July 10/11, 2011.
272. Julie Appleby. Debate surrounds end-of-life health care costs. USA Today, July 10/11, 2011.
273. Hoover, D. R.; Crystal, S.; Kumar, R.; Sambamoorthi, U.; Cantor, J. C. (2002). "Medical Expenditures during the Last Year of Life: Findings from the 1992–1996 Medicare Current Beneficiary Survey". Health Services Research 37 (6): 1625–1642. doi:10.1111/1475-6773.01113. PMC 1464043.PMID 12546289.
274. Lo B: Overview of ethical guidelines. In Resolving ethical dilemmas: a guide for clinicians 2nd edition. Lippincott Williams and Wilkins; 2000:11-18.
275. Latimer EJ: Ethical care at the end-of-life. CMAJ 1998, 158(13):1741-1747.276. Simonds AK: Ethics and decision making in end stage lung disease. Thorax
2003, 58(3):272-277.277. Yeolekar ME, Mehta S, Yeolekar A: End-of-life care: issues and challenges. J
Postgrad Med 2008, 54(3):173-175.278. Heyland DK, Cook DJ, Rocker GM, Dodek PM, Kutsogiannis DJ, Peters S, Tranmer
JE, O-Callaghan CJ: Decision-making in the ICU: perspectives of the substitute decision-maker. Intensive Care Med 2003, 29:75-82.
279. Heyland DK, Tranmer J, O'Callaghan CJ, Gafni A: The seriously ill hospitalized patient: preferred role in end-of-life decision making? J Crit Care 2003, 18(1):3-10.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
96
280. Bomba PA: Enabling the transition to hospice through effective palliative care. Case Manager 2005, 16(1):48-52.
281. Ahern P: End-of-life- not end of story. Mod Healthcare 2007, 37(25):24.282. Herbst L: Hospice care at the end-of-life. Clin Geriatr Med 2004, 20(4):753-765.283. Wiese CHR, Vossen-Wellmann A, Morgenthal HC, Popov AF, Frag BM, Hanekop
GG: Emergency calls and need for emergency care in patients looked after by a palliative care team: retrospective interview study with bereaved relatives. BMC PalliatCare 2008, 7(11):
284. Mercadante S, Intravaia G, Villari P, Ferrera P, Fabrizio D, Casuccio A: Controlled sedation for refractory symptoms in dying patients. J Pain Symptom Manage 2008 in press.
285. Castellano G: The criminalization of treating end-of-life patients with risky pain medication and the role of the extreme emergency situation. Fordham Law Rev 2007, 76(1):203-34.
286. Griffith R: Controlled drugs and the principle of double effect. Br J Community Nurs 2006, 11(8):352-357.
287. Gallagher A, Wainwright P: Terminal sedation: promoting ethical nursing practice. Nurs Stand 2007, 21(34):42-6.
288. Boyle J: Medical ethics and double effect: the case of terminal sedation. Theor Med Bioethic 2004, 25(1):51-60.
289. Lo B, Rubenfeld G: Palliative sedation in dying patients: "we turn to it when everything else hasn't worked". JAMA 2005, 294(14):1810-6.
290. Kagawa-Singer M, Blackhall LJ: Negotiating cross-cultural issues at the end-of-life: "You got to go where he lives". JAMA 2001, 286(23):2993-3001.
291. Blackhall LH, Murphy ST, Frank G, Michel V, Azen S: Ethnicity and attitudes toward patient autonomy. JAMA 1995, 274:820-825.
292. Newman Giger J, Davidhizar RE, Fordham P: Multi-cultural and multi-ethnic considerations and advance directives: developing cultural competency. Journal of Cultural Diversity 2006, 13(1):3-9.
293. Andersen J: Cultural competence and health care: Japanese, Korean, and Indian patients in the United States. Journal of Cultural Diversity 2001, 8(4):109-121.
294. Betancourt JR, Green AR, Carrillo JE, Ananeh-Firempong O: Defining cultural competence: a practical framework for addressing racial/ethnic disparities in health and health care. Public Health Reports 2003, 118:293-302.
295. Searight HR, Gafford J: Cultural diversity at the end-of-life: issues and guidelines for family physicians. Am Fam Physician2005, 71(3):429-430
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
97
296. Vachon M, Fillion L, Achille M: A conceptual analysis of spirituality at the end-of-life. J Palliat Med 2009, 12:53-9.
297. Hakim RB, Teno JM, Harrell FE, Knaus WA, Wenger N, Phillips RS, Lavde P, Califf R, Connors AF, Lynn J: Factors associated with donot- resuscitate orders: patients' preferences, prognoses, and physicians' judgments. Ann Intern Med 1996, 125:284-293.
298. Rosenfeld KE, Wenger NS, Phillips RS, Connors AF, Dawson NV, Layde P, Califf RM, Liu H, Lynn J, Ove RK: Factors associated with change in resuscitation preference of seriously ill patients. The SUPPORT Investigators. Study to understand prognoses and preferences for outcomes and risks of treatments. Arch Intern Med 1996, 156:1558-1564.
299. Miller DL, Jahnigen DW, Gorbien MJ, Simbartl L: Cardiopulmonary resuscitation: how useful? Attitudes and knowledge of an elderly population. Arch Intern Med 1992, 152:578-582.
300. Hamel MB, Lynn J, Teno JM, Covinsky KE, Wu AW, Galanos A, Desbiens NA, Phillips RS: Age-related differences in care preferences, treatment decisions, and clinical outcomes of seriously ill hospitalized adults: lessons from SUPPORT. J Am Geriatr Soc 2000, 48:S176-S182.
301. Marco CA, Schears RM: Societal Preferences regarding cardiopulmonary resuscitation. Am J Emerg Med 2002, 20:207-211.
302. Layde PM, Beam CA, Broste SK, Connors AF, Desbiens N, Lynn J, Phillips RS, Reding D, Teno J, Vidaillet H: Surrogates' predictions of seriously ill patients' resuscitation preferences. Arch Fam Med 1995, 4:518-523.
303. Wenger NS, Phillips RS, Teno JM, Ove RK, Dawson NV, Liu H, Califf R, Lavde P, Hakim R, Lynn J: Physician understanding of patient resuscitation preferences: insights and clinical implications. J Am Geriatr Soc 2000, 48:S44-51.
304. Golin CE, Wenger NS, Liu H, Dawson NV, Teno JM, Desbiens NA, Lynn J, Oye RK, Phillips RS: A prospective study of patient-physician communication about resuscitation. J Am Geriatr Soc 2000, 48:S52-60.
305. Fischer GS, Tulsky JA, Rose MR, Siminoff LA, Arnold RM: Patient knowledge and physician predictions of treatment preferences after discussion of advance directives. J Gen Intern Med 1998, 13:447-454.
306. Beach MC, Morrison RS: The effect of do-not-resuscitate orders on physician decision-making. J Am Geriatr Soc 2002, 50:2057-2061.
307. Patient Self-Determination Act- Omnibus Budget Reconciliation Act of 1990. Pub L No. 101–508.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
98
308. Jacobson JA, White BE, Battin MP, Francis LP, Green DJ, Kasworm ES: Patients' understanding and use of advance directives. West J Med 1994, 160:232-236.
309. Silviera M, DiPiero A, Gerrity M, Feudtner C: Patients' knowledge of options at the end-of-life: ignorance in the face of death. JAMA 2000, 284(19):2483-2488.
310. Teno J, Lynn J, Wenger N, Phillips RS, Murphy DP, Connors AF, Desbiens N, Fulkerson W, Bellamy P, Knaus WA: Advance directives for seriously ill hospitalized patients: effectiveness with the patient self-determination act and the SUPPORT intervention. SUPPORT Investigators. Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatment. J Am Geriatr Soc 1997, 45(4):500-507.
311. Taylor DM, Ugoni AM, Cameron PA, McNeil JJ: Advance directives and emergency department patients: ownership rates and perceptions of use. Intern Med J 2003, 33(12):586-592.
312. Upadya A, Visvanathan M, Thorevska N, Amoateng-Adjepong Y: Patient, physician, and family member understanding of living wills. Am J Respir Crit Care Med 2002, 166:1430-1435
313. The SUPPORT Principle Investigators: A controlled trial to improve care for seriously ill hospitalized patients. JAMA 1995, 274:1591-98.
314. Llovera I, Mandel FS, Ryan JG, Ward MF, Sama A: Are emergency department patients thinking about advance directives? Acad Emerg Med 1997, 4:976-980.
315. Hanson LC, Tulsky J, Danis M: Can clinical interventions change care at the end-of-life? Ann Intern Med 1997, 126:381-388.
316. Robinson R, Eagen MK, Price TJ: Innovative solutions: taking advance directives to the community. Dimens Crit Care Nurs 2008, 27:154-156.
317. Llovera I, Ward MF, Ryan JG, Lesser M, Sama AE, Crough D, Mansfield M, Lesser LI: Why don't emergency department patients have advance directives? Acad Emerg Med 1999, 6:1054-1060.
318. Iserson KV: Prehospital advance directives -a better way. J Emerg Med 2002, 23:419-20.
319. Morrison LJ, Morrison RS: Palliative care and pain management. Med Clin N Am 2006, 90(5):983-1004.
320. Von Gunten CF, Ferris FD, Emanuel LL: Ensuring competency in end-of-life care: communication and relational skills. JAMA 2000, 284(23):3051-3057.
321. O'Mara K: Communication and conflict resolution in emergency medicine. Emerg Med Clin North Am 1999, 17(2):451-459.
322. Buckman R: How to break bad news: a guide for health care professions Baltimore, MD: Johns Hopkins University Press; 1992.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
99
323. Hobgood C, Harward D, Newton K, Davis W: The educational intervention "GRIEV_ING" improves the death notification skills of residents. Acad Emerg Med 2005, 12(4):296-301.
324. Moskop JC: Informed consent and refusal of treatment: challenges for emergency physicians. Emerg Med Clin N Am 2006, 24:605-618.
325. Miller SS, Marin DB: Assessing capacity. Emerg Med Clin N Am 2000, 18(2):233-242.
326. Sorger BM, Rosenfeld B, Pessin H, Timm AK, Cimino J: Decision making capacity in elderly, terminally ill patients with cancer. Behav Sci Law 2007, 25:393-404.
327. Teno J, Clarridge B, et al. Family perspectives on end-of-life care at the last place of care. JAMA. 2004;291:88–93.
328. Casarett D, Quill T. “I’m not ready for hospice”: strategies for timely and effective hospice discussions” Ann Intern Med. 2007;146:443–9.
329. Connor S, Pyenson B, et al. Comparing hospice and non-hospice patient survival among patients who die within a three-year window. J Pain Symptom Manage.2007;33:238–46.
330. Pyenson B, Connor S, et al. Medicare cost in matched hospice and non-hospice cohorts. J Pain Symptom Manage. 2004;28:200–10.
331. The University of Texas M. D. Anderson Cancer Center [http://www.mdanderson.org/patients_public/about_cancer/dis play.cfm?id=33540A76-72DF-11D4- AEBD00508BDCCE3A&method=displayFull]. accessed 3/15/09
332. University of Washington School of Medicine - Physician-Assisted Suicide [http://depts.washington.edu/bioethx/topics/ pas.html].
333. Steinbrook R: Physician-assisted death- from Oregon to Washington state. N Engl J Med 2008, 359(24):2513-2515.
334. Mayou R, Hawton K, Feldman E, et al. Psychiatric problems among medical admissions. Int J Psychiatry Med 1991;21:71-84.
335. Guthrie E. Emotional disorder in chronic illness: psychotherapeutic 4 Blazer DG, Kessler RC, McGonagle KA, et al. The prevalence and distribution of major depression in a national community sample: the national comorbidity survey. Am J Psychiatry 1994;151:979-986.
336. McDaniel JS, Musselman DL, Porter MR, et al. Depression in patients with cancer: diagnosis, biology and treatment. Arch Gen Psychiatry 1995;52:89-99.
337. Blazer DG, Kessler RC, McGonagle KA, et al. The prevalence and distribution of major depression in a national community sample: the national comorbidity survey. Am J Psychiatry 1994;151:979-986.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
100
338. Powell T. Consultation-liaison psychiatry and clinical ethics. Psychosomatics 1997;38:321-326.
339. Breitbart W. Identifying patients at risk for and treatment of major psychiatric complications of cancer. Support Care Cancer 1995;3:45-60.
340. Draper B, Anstey K. Psychosocial stressors, physical illness and the spectrum of depression in elderly inpatients. Aust N Z J Psychiatry 1996;30:567-572.
341. Koenig HG, Kuchibhatla M. Use of health services by hospitalized medically ill depressed elderly patients. Am J Psychiatry 1998;155:871-877.
342. Harris EC, Barraclough BM. Suicide as an outcome for mental disorders: a meta-analysis. Br J Psychiatry 1997;170:205-223.
343. Saravay SM. Psychiatric interventions in the medically ill: outcomes and effectiveness research. Psychiatr Clin North Am 1996;19:467-480.
344. Morris PLP, Robinson RG, Samuels J. Depression, introversion and mortality following stroke. Aust N Z J Psychiatry 1993;27:443-449.
345. Parickh RM, Robinson RG, Lipsey JR, et al. The impact of post-stroke depression on recovery in activities of daily living over two year follow-up. Arch Neurol 1990;47:785-789.
346. Glassman AH, Shapiro PA. Depression and the course of coronary artery disease. Am J Psychiatry 1998;55:4-11.
347. Beliles K, Stoudemire A. Psychopharmacologic treatment of depression in the medically ill. Psychosomatics 1998;39(suppl):2S-19S.
348. Chaturvedi SK, Maguire P, Hopwood P. Antidepressant medications in cancer patients. Psychooncology 1994;3:57-60.
349. Schwartz CE, Steinmuller RI, Dubler N. The medical psychiatrist as physician for the chronically mentally ill. Gen Hosp Psychiatry 1998;20:52-61.
350. Pratt LA, Ford LE, Crum RM, et al. Depression, psychotropic medication, and risk of myocardial infarction: prospective data from the Baltimore ECA follow-up. Circulation 1996;94:3123-3129.
351. Michelson D, Stratakis C, Hill L, et al. Bone mineral density in women with depression. N Engl J Med 1996;335:1176-1181.
352. Smith GC. From consultation-liaison psychiatry to psychosocial advocacy: maintaining psychiatry’s scope. Aust N Z J Psychiatry 1998;32:753-761.
353. Mayou R, Sharpe M. Patients whom doctors find difficult to help. Psychosomatics 1995;36:323-325.
354. Salmon P, Peters S, Stanley I. Patients’ perceptions of medical explanations for somatisation disorders: qualitative analysis. BMJ 1999;318:372-376.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
101
355. Cope H, David A, Pelosi A, et al. Predictors of chronic “postviral” fatigue. Lancet 1994;344:864-868.
356. Rabkin JG, Remien R, Katoff L, et al. Resilience in adversity among long-term survivors of AIDS. Hosp Community Psychiatry 1993;44:162-167.
357. Dow KH, Ferrell BR, Leigh S, et al. An evaluation of the quality of life among long-term survivors of breast cancer. Breast Cancer Res Treat 1996;39:261-273.
358. Burstein HJ, Gelber S, Guadagnoli E, et al. Use of alternative medicine by women with early stage breast cancer. N Engl J Med 1999;340:1733-1739.
359. Holland J. Use of alternative medicine—a marker for distress [editorial]? N Engl J Med 1999;340:1758-1759.
360. Cohen LM, McCue JD, Germain M, et al. Denying the dying: advance directives and dialysis discontinuation. Psychosomatics 1997;38:27-34.
361. Slevin ML, Stubbs L, Plant HJ, et al. Attitudes to chemotherapy: comparing views of patients with cancer with those of doctors, nurses, and general public. BMJ 1990;300:1458-1460.
362. Parker JC, Smarr KL, Buckelew SP, et al. Effects of stress management on clinical outcomes in rheumatoid arthritis. Arthritis Rheum 1995;38:1807-1818.
363. Smyth JM, Stone AA, Kael L. Effects of writing about stressful experiences on symptom reduction in patients with asthma and rheumatoid arthritis: a randomized trial. JAMA 1999;281:1304-1309.
364. Kelly B, Varghese F. The emotional hazards of medical practice. In: Sanders MR, Mitchell C, Byrne GJA, eds. Medical consultation skills. Melbourne: Addison-Wesley, 1997:472-488.
365. Committee on the Future Health Care Workforce for Older Americans, Board on Health Care Services, INSTITUTE OF MEDICINE OF THE NATIONAL ACADEMIES. "RETOOLING FOR AN AGING AMERICA: BUILDING THE HEALTH CARE WORKFORCE". THE NATIONAL ACADEMIES PRESS.
366. National Alliance for Care giving and the United Hospital Fund (2005), (presentation), National Alliance for Care giving and the United Hospital Fund
367. U.S. Department of Health and Human Services (2001), (presentation), Rockville: Agency for Healthcare Research and Quality
368. George LK, Gwyther LP. Caregiver well-being: a multidimensional examination of family caregivers of demented adults. Gerontologist. 1986;26:253–9.
369. Thompson TL, Robinson JD, Beisecker AE. The older patient-physician interaction. In: Nussbaum JF, Coupland J, eds. Handbook of Communication and Aging Research, 2nd ed. Mahwah, NJ: Lawrence Erlbaum Assoc; 2004.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
102
370. Halter JB. The challenge of communicating health information to elderly patients: a view from geriatric medicine. In: Park DC, Morrell RW, Shifren K, eds. Processing of Medical Information in Aging Patients: Cognitive and Human Factors Perspectives. Mahwah, NJ: Lawrence Erlbaum Assoc; 1999.
371. Ostuni E, Mohl GR. Communication with elderly patients. Dent Econ. 1994;84(3):27–32.
372. Wiebe C. What did you say? Tips for talking more clearly to patients. ACP Observer. December 1997.
373. Baker SK. Thirty ways to make your practice more patient-friendly. In: Woods D, ed.Communication for Doctors: How to Improve Patient Care and Minimize Legal Risk. Oxford: Radcliffe; 2004.
374. Dreher BB. Communication Skills for Working With Elders. New York: Springer; 1987.
375. Osborne H. Communicating with clients in person and over the phone. Issue Brief Cent Medicare Educ. 2003;4(8):1–8.
376. Breisch SL. Elderly patients need special connection. Am Acad Orthop Surg Bull. February 2001;49(1).
377. Nussbaum JF, Pecchioni LL, Robinson JD, Thompson T. Communication and Aging. Mahwah, NJ: Lawrence Erlbaum Assoc; 2000.
378. Meryn S. Improving doctor-patient communication: not an option but a necessity. BMJ. 1998;316(7149):1922.
379. Schopick JE. Hippocrates was right: treat people, not their disease. In: Woods D, ed.Communication for Doctors: How to Improve Patient Care and Minimize Legal Risk. Oxford: Radcliffe; 2004:12–13.
380. National Council on Patient Information and Education. Eight easy ways to make the medicine go down. In: Woods D, ed. Communication for Doctors: How to Improve Patient Care and Minimize Legal Risk. Oxford: Radcliffe; 2004:6–7.
381. Woods D. Seven ways to build trust with your patients on their first visit. In: Woods D, ed.Communication for Doctors: How to Improve Patient Care and Minimize Legal Risk. Oxford: Radcliffe; 2004: 23–24.
382. Lewis A. Non-compliance: a $100 billion problem. The Remington Report 1997;5(4):14-5.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
103
383. Col N, Fanale JE, Kronholm P. The role of medication noncompliance and adverse drug reactions in hospitalizations of the elderly. Arch Intern Med 1990;150:841-5.
384. Colt HG, Shapiro AP. Drug-induced illness as a cause for admission to a community hospital. J Am Geriatr Soc 1989;37:323-6.
385. Hallas J, Harvald B, Gram LF, et al. Drug related hospital admissions: the role of definitions and intensity of data collection, and the possibility of prevention. J Intern Med1990;228(2):83-90.
386. Segal E, Tamir A, Ish-Shalom S. Compliance of osteoporotic patients with different treatment regimens. Isr Med Assoc J 2003;5(12):859-62.
387. Kuo YF, Raji MA, Markides KS, et al. Inconsistent use of diabetes medications, diabetes complications, and mortality in older Mexican Americans over a 7-year period: data from the Hispanic established population for the epidemiologic study of the elderly. Diabetes Care 2003;26(11):3054-60.
388. Raji MA, Kuo YF, Salazar JA, et al. Ethnic differences in antihypertensive medication use in the elderly. Ann Pharmacother 2004;38(2):209-14. Epub 2003 Dec 15.
389. Dunbar-Jacob J, Bohachick P, Mortimer MK, et al. Medication adherence in persons with cardiovascular disease. J Cardiovasc Nurs 2003;18(3):209-18.
390. DiMatteo MR. Social support and patient adherence to medical treatment: a meta-analysis. Health Psychol 2004;23(2):207-18.
391. Kilbourne AM, Reynolds CF, Good CB, et al. How does depression influence diabetes medication adherence in older patients? Am J Geriatr Psychiatry 2005;13(3):202-10.
392. Maddigan SL, Farris KB, Keating N, et al. Predictors of older adults' capacity for medication management in a self-medication program: a retrospective chart review. J Aging Health 2003;15:332-52.
393. McKellar JD, Humphreys K, Piette JD. Depression increases diabetes symptoms by complicating patients' self-care adherence. Diabetes Educ 2004;30:485-92.
394. Park H, Hong Y, Lee H, et al. Individuals with type 2 diabetes and depressive symptoms exhibited lower adherence with self-care. J Clin Epidemiol 2004;57:978-84.
395. Thomas EJ, Brennan TA. Incidence and types of preventable adverse events in elderly patients: population based review of medical records. BMJ 2000;320(7237):741-4.
396. Spiers MV, Kutzik DM, Lamar M. Variation in medication understanding among the elderly. Am J Health Syst Pharm 2004;61:373-80.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
104
397. Okuno J, Yanagi H, Tomura S. Is cognitive impairment a risk factor for poor compliance among Japanese elderly in the community? Eur J Clin Pharmacol 2001;57(8):589-94.
398. Kiortsis DN, Giral P, Bruckert E, et al. Factors associated with low compliance with lipid-lowering drugs in hyperlipidemic patients. J Clin Pharm Ther 2000;25(6):445-51.
399. Coleman EA, Smith JD, Raha D, et al. Posthospital medication discrepancies: prevalence and contributing factors. Arch Intern Med 2005;165(16):1842-7.
400. Gonski PN, Stathers GM, Freiman JS, et al. A critical review of admission and discharge medications in an elderly Australian population. Drugs Aging 1993;3:358-62. 51. McKinley BT, Mulhall BP, Jackson JL. Perceived versus actual medication regimens among internal medicine patients. Mil Med 2004;169(6):451-4.
401. Moore C, Wisnivesky J, Williams S, et al. Medical errors related to discontinuity of care from an inpatient to an outpatient setting. J Gen Intern Med 2003;18(8):646-51.
402. Meredith S, Feldman PH, Frey D, et al. Possible medication errors in home healthcare patients. J Am Geriatr Soc 2001;49:719-24.
403. Zhan C, Sangl J, Bierman AS, et al. Potentially inappropriate medication use in the community-dwelling elderly: findings from the 1996 Medical Expenditure Panel Survey. JAMA 2001;286(22): 2823-9.
404. Zhan C, Correa-de-Araujo R, Bierman AS, et al. Suboptimal prescribing in elderly outpatients: potentially harmful drug-drug and drug-disease combinations. J Am Geriatr Soc 2005;53(2):262-7.
405. Ellenbecker CH, Frazier SC, Verney S. Nurses' observations and experiences of problems and adverse effects of medication management in home care. Geriatric Nursing 2004;25(3):164-70.
406. Hill-Briggs F, Gary TL, Bone LR, et al. Medication adherence and diabetes control in urban African Americans with type 2 diabetes. Health Psychol 2005;24(4):349-57.
407. Ogedegbe G, Harrison M, Robbins L, et al. Barriers and facilitators of medication adherence in hypertensive African Americans: a qualitative study. Ethn Dis 2004;14(1):3-12.
408. Jackson JE, Doescher MP, Saver BG, et al. Prescription drug coverage, health, and medication acquisition among seniors with one or more chronic conditions. Med Care 2004;42:1056-65.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
105
409. Yilmaz MB, Pinar M, Naharci I, et al. Being well-informed about statin is associated with continuous adherence and reaching targets. Cardiovasc Drugs Ther 2005;19(6):437-40.
410. Atkin PA, Finnegan TP, Ogle SJ, et al. Functional ability of patients to manage medication packaging: a survey of geriatric inpatients. Age Aging 1994;23(2):113-6.
411. Jeste SD, Patterson TL, Palmer BW, et al. Cognitive predictors of medication adherence among middle-aged and older outpatients with schizophrenia. Schizophr Res 2003;63(1-2):49-58.
412. Esposito L. The effects of medication education on adherence to medication regimens in an elderly population. J Adv Nurs1995;21:935-43.
413. 168. Park D, Morrell RW, Frieske D, et al. Medication adherence behaviors in older adults: effects of external cognitive supports. Psychol Aging1992;7(2):252-6.
414. Barber N, Parsons J, Clifford S, et al. Patients' problems with new medication for chronic conditions. Qual Saf Health Care 2004;13(3):172-5.
415. Beers MH, Baran RW, Frenia K. Drugs and the elderly, Part 1: The problems facing managed care.Am J Manag Care 2000;6:1313-20.
416. Bergman-Evans B. Improving medication management for older adult clients. Iowa City, IA: University of Iowa Gerontological Nursing Interventions Research Center;2004.
417. Fick DM, Cooper JW, Wade WE, et al. Updating the Beers criteria for potentially inappropriate medication use in older adults: results of a U.S. consensus panel of experts. Arch Intern Med 2003;163(22):2716-24.
418. Ellenbecker CH, Frazier SC, Verney S. Nurses' observations and experiences of problems and adverse effects of medication management in home care. Geriatric Nursing 2004;25(3):164-70.
419. Hill-Briggs F, Gary TL, Bone LR, et al. Medication adherence and diabetes control in urban African Americans with type 2 diabetes. Health Psychol 2005;24(4):349-57.
420. Ogedegbe G, Harrison M, Robbins L, et al. Barriers and facilitators of medication adherence in hypertensive African Americans: a qualitative study. Ethn Dis 2004;14(1):3-12.
421. Jonsson P, McNamee M, Campion E. The “Do not resuscitate” order: a profile of its changing use. Archives of Internal Medicine 1988;148:2373–5.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
106
422. Somogyi-Zalud E, Zhong Z, Lynn J, et al. Elderly persons’ last six months of life: findings from the hospitalized elderly longitudinal project. Journal of the American Geriatrics Society 2000;48(5 suppl);131–9S.
423. Terry M, Sweig S. Prevalence of advance directives and do-not resuscitate orders in community facilities. Archives of Family Medicine 1994;3:141–5.
424. Berlowitz D, Wilking S, Moskowitz M. Do-not-resuscitate orders at a chronic care hospital. Journal of the American Geriatrics Society 1991;39:472–6.
425. Meyers R, Lurie N, Breitbucher R, et al. Do-not-resuscitate orders in an extended-care study group. Journal of the American Geriatrics Society 1990;38:1011–15.
426. Teno J, Braco K, Mor V, et al. Changes in advance care planning in nursing homes before and after the patient self-determination act: report of a 10-state survey. Journal of the American Geriatrics Society 1997;45:939–44.
427. Krumholz H, Phillips R, Hamel M, et al. Resuscitation preferences among patients with severe congestive heart failure. Circulation 1998;21:77–81.
428. Stolman C, Gregory J, Dunn D. Evaluation of the do not resuscitate orders at a community hospital. Archives of Internal Medicine 1989;149:1851–6.
429. Fader A, Gambert S, Nash M. Implementing a “do-not-resuscitate” policy in a nursing home. Journal of the American Geriatrics Society 1989;37:544–8.
430. Miller D, Jahnigen D, Gorbien M. Cardiopulmonary resuscitation: how useful? Archives of Internal Medicine 1992;152:578–82.
431. Godkin M, Toth E. Cardiopulmonary resuscitation and older adults’ expectations. Gerontologist 1994;34:797–802.
432. Lo B, McLeod G, Saika G. Patient attitudes to discussing life-sustaining treatment. Archives of Internal Medicine 1986;146:1613–15.
433. Layton R, Adelman H, Wallach P, et al. Discussions about the use of life-sustaining treatments: a literature review of physicians’ and patients’ attitudes and practices. Journal of Clinical Ethics 1994;5:195–203.
434. Hamel MB, Lynn J, Teno JM, et al. Age-related differences in care preferences, treatment decisions, and clinical outcomes of seriously ill hospitalized adults: lessons from SUPPORT. Journal of the American Geriatrics Society 2000;48:176-82S
435. Schoenwetter R, Walker R, Solomon M, et al. Life values, resuscitation preferences, and the applicability of living wills in an older population. Journal of the American Geriatrics Society 1996;44:954–58.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
107
436. Romero L, Lindeman R, Koehler K, et al. Influence of ethnicity on advance directives and end-of life decisions. Journal of the American Medical Association 1997;277:298.
437. Danis M, Mutran E, Fitzsimmons J, et al. Attitudes associated with the desire for life-sustaining treatments in elderly patients. Clinical Research 1991;39:624A.
438. Gunasekera N, Tiller D, Clements L, et al. Elderly patients’ views on cardiopulmonary resuscitation. Age and Aging 1986;15:364–8.
439. Pulchalski C, Zhong Z, Jacobs M, et al. Patients want their family and physician to make resuscitation decisions for them: observations from SUPPORT and HELP. Journal of the American Geriatrics Society 2000;48suppl 5):84–90S.
440. Zweibel N, Cassel C. Treatment choices at the end of life: a comparison of decisions by old patients and their physician-selected proxies. Gerontologist 1989;29:615–21.
441. MiIler D. Factors influencing physicians in recommending in-hospital resuscitation. Archives of Internal Medicine 1993;153:199–203.
442. Schneidermann L, Kaplan R, Pearlman R, et al. Do physicians’ own preferences for life-sustaining treatment influence their perceptions of patients’ preferences? Journal of Clinical Ethics 1993;4:28–33.
443. Ebell M, Doukas D, Smith M. The do-not-resuscitate order: a comparison of physician and patient preferences and decision-making. American Journal of Medicine 1991;91:255–60.
444. Purvis R, Law E, Still J, et al. Nurses’ attitudes toward do-not-resuscitate orders. Journal of Burn Care Rehabilitation 1998;19:538–41.
445. Granja C, Teixeira-Pinto A, Costa-Pereira A. Attitudes toward do not resuscitate decisions: differences among health care professionals in a Portuguese Hospital. Intensive Care Medicine 2001;27:555–8.
446. Dickenson D. Are medical ethics out of touch? Practitioner attitudes in the US and UK towards decisions at the end of life. Journal of Clinical Ethics 2000;26:254–60.
447. Seferian EG, Afessa B. Demographic and clinical variation of adult intensive care unit utilization from a geographically defined population. Crit Care Med. 2006; 34(8):2113-9.
448. Burack OR, Weiner AS, Reinhardt JP, Annunziato RA., What matters most to nursing home elders: quality of life in the nursing home. J Am Med Dir Assoc. 2012;13(1):48-53.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
108
449. Dickens AP, Richards SH, Greaves CJ, Campbell JL., Interventions targeting social isolation in older people: a systematic review. BMC Public Health. 2011;11:647.
450. Skingley A. Older people, isolation and loneliness: implications for community nursing. 2013;18(2):84-90.
451. Gopinath B, Rochtchina E, Anstey KJ, Mitchell P. Living alone and risk of mortality in older, community-dwelling adults., JAMA Intern Med. 2013, 25;173(4):320-1.
452. Salsman JM, Butt Z, Pilkonis PA, Cyranowski JM, Zill N, Hendrie HC, Kupst MJ, Kelly MA, Bode RK, Choi SW, Lai JS, Griffith JW, Stoney CM, Brouwers P, Knox SS, Cella D. Emotion assessment using the NIH Toolbox., Neurology. 2013;80(11 Suppl 3):S76-86.
453. Reuben DB, Magasi S, McCreath HE, Bohannon RW, Wang YC, Bubela DJ, Rymer WZ, Beaumont J, Rine RM, Lai JS, Gershon RC. Motor assessment using the NIH Toolbox. Neurology. 2013;80(11 Suppl 3):S65-75.
454. Weintraub S, Dikmen SS, Heaton RK, Tulsky DS, Zelazo PD, Bauer PJ, Carlozzi NE, Slotkin J, Blitz D, Wallner-Allen K, Fox NA, Beaumont JL, Mungas D, Nowinski CJ, Richler J, Deocampo JA, Anderson JE, Manly JJ, Borosh B, Havlik R, Conway K, Edwards E, Freund L, King JW, Moy C, Witt E, Gershon RC. Cognition assessment using the NIH Toolbox. Neurology. 2013 Mar 12;80(11 Suppl 3):S54-64.
455. Dunn W, Griffith JW, Morrison MT, Tanquary J, Sabata D, Victorson D, Carey LM, Gershon RC., Neurology. 2013;80(11 Suppl 3):S41-4.
456. Hodes RJ, Insel TR, Landis SC; NIH Blueprint for Neuroscience Research. e NIH toolbox: setting a standard for biomedical research. Neurology. 2013 Mar 12;80 (11 Suppl 3):S1.
The information presented in this course is intended solely for the use of healthcare professionals taking this course, for credit, from NurseCe4Less.com.The information is designed to assist healthcare professionals, including nurses,in addressing issues associated with healthcare.
The information provided in this course is general in nature, and is not designed
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
109
to address any specific situation. This publication in no way absolves facilities of their responsibility for the appropriate orientation of healthcare professionals.Hospitals or other organizations using this publication as a part of their ownorientation processes should review the contents of this publication to ensure accuracy and compliance before using this publication.
Hospitals and facilities that use this publication agree to defend and indemnify,and shall hold NurseCe4Less.com, including its parent(s), subsidiaries, affiliates, officers/directors, and employees from liability resulting from the use of this publication.
The contents of this publication may not be reproduced without written permission from
NurseCe4Less.com.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com
110