Embed Size (px)
Citation preview
������������
�������������������� ����������������������
���������� � ������� �� ���� ������������� ����� ��� ���� ������� ���� ����������������������� ������������������������� �

OPR: HQ AFDC/DR (Lt Col Jackson R. Dobbins)Certified by: AFDC/DR (Col Thomas A. Bowermeister)Pages: 44Distribution: FApproved by: TIMOTHY A. KINNAN, Major General, USAF
Commander, Air Force Doctrine Center
AIR FORCE DOCTRINE DOCUMENT 2–4.213 November 1999
BY ORDER OF THESECRETARY OF THE AIR FORCE
i
FOREWORD
This document establishes operational doctrine for Air Force healthservices and outlines the principles for helping airmen maintain healthand fitness by integrating prevention-oriented health and fitness andmedical intervention. Multiple forces are shaping national and globalconcepts of health and health care. To meet the demands of this chang-ing environment, Air Force health services and the Air Force MedicalService balance operational demands and delivering world-class healthcare to airmen, their families, and beneficiaries.
Force health protection is vital to the success of Air Force operationalreadiness and our ability to support changing mission requirements. AirForce health services and medical personnel organize, train, and equip toensure a medically ready fighting force capable of supporting nationalsecurity and military operations. Together, a ready medical force andhealthy, fit fighting forces ensure Air Force stability and mission respon-siveness.
Although commanders are responsible for the morale, health, and wel-fare of their personnel and promote daily health and fitness activities, itis every airman’s responsibility to maintain individual health and fitness.This philosophy should dictate the individual’s approach to duty and per-meate the Air Force community.
TIMOTHY A. KINNAN Major General, USAF Commander, Air Force Doctrine Center
13 November 1999

ii
iii
INTRODUCTION ................................................................................... v
CHAPTER ONE— Overview ................................................................ 1Air Force Health Services Definition.................................................. 1Historical Perspective ......................................................................... 2Rules and Responsibilities .................................................................. 4
Airmen ........................................................................................... 4Supervisors ..................................................................................... 4Commanders .................................................................................. 5
CHAPTER TWO—Operations .............................................................. 7Force Health Protection Overview ..................................................... 7
Health and Fit Force ....................................................................... 8Casualty Prevention ....................................................................... 8Casualty Care Management ........................................................... 9
Air Force Medical Service Operations .............................................. 10Building Healthy Communities ......................................................... 11
Population Health ......................................................................... 11Force Enhancement ..................................................................... 13
Managed Health Care ....................................................................... 13Tailored Force ................................................................................... 14
Total Force Management .............................................................. 15Special Operations Medical Capabilities ...................................... 15
Medical Readiness ............................................................................ 16Total Force Partnership ................................................................ 16Education and Training ................................................................ 17Technology Modernization ........................................................... 17Employ the Force ......................................................................... 17Position and Sustain the Force ..................................................... 18Aeromedical Evacuation System .................................................. 19Recover the Force ......................................................................... 20Focus Medical Logistics ................................................................ 21
Customer Satisfaction ....................................................................... 22
CHAPTER THREE—Command and Control .................................. 23Command Relationships ................................................................... 23
Chief of Staff of the Air Force and HQ USAF ............................... 24Air Force Surgeon General ........................................................... 24Major Commands ......................................................................... 24
TABLE OF CONTENTS
Air Force Forces ........................................................................... 24
iv
Aerospace Expeditionary Force .................................................... 25Aeromedical Evacuation Command and Control ......................... 25
Other Considerations ........................................................................ 27CONUS Reachback ....................................................................... 27Participation in Joint Operations ................................................. 27Base Operating Support ................................................................ 28In-transit Visibility ....................................................................... 28Resources, Sourcing, and Distribution ......................................... 28Retrograde Management .............................................................. 28
Suggested Readings ............................................................................ 29
Glossary ............................................................................................... 31
v
INTRODUCTION
PURPOSE
This Air Force Doctrine Document (AFDD) establishes doctrinal guid-ance for organizing and employing health services capabilities at the op-erational level across the full range of military operations. It is a criticalelement of US Air Force operational-level doctrine and as such shouldform the basis from which Air Force commanders plan and execute theirhealth services. This AFDD implements Air Force Policy Directive (AFPD)10-13, Air and Space Doctrine.
APPLICATION
This AFDD applies to all Air Force military and civilian personnel (in-cludes Air Force Reserve Command [AFRC] and Air National Guard [ANG]units and members). The doctrine in this document is authoritative butnot directive. Therefore, commanders need to consider not only the con-tents of this AFDD, but also the particular situation when accomplishingtheir missions.
SCOPE
Air Force assets (people, information, and support systems) can beused across the range of military operations at the strategic, operational,and tactical levels of war. This AFDD discusses the fundamentals of orga-nization and employment of Air Force health services required to sup-port the operational missions assigned by commanders in chief (CINCs)and carried out by air component commanders.

vi
1
CHAPTER ONE��������
AIR FORCE HEALTH SERVICES DEFINITION
Health services form the basis for maintaining a healthy and fitforce. All airmen routinely participate in health services activi-ties. These activities are grouped into health surveillance, risk assess-ment, response to changing occupational and environmental regulation,aeromedical evacuation (AE), prevention, fitness, and health care deliv-ery. Together these activities promote, improve, conserve, or restore in-dividual emotional well-being, physical health, and fitness.
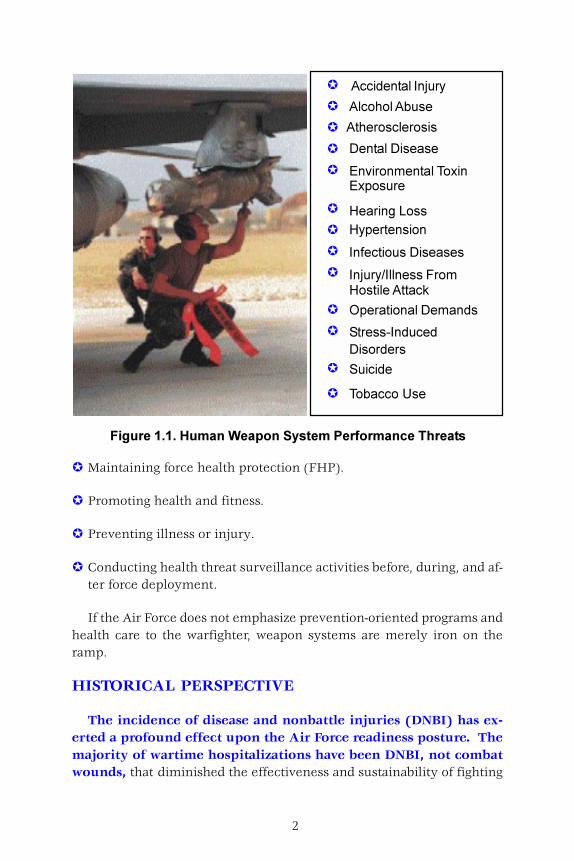
The concept of the individual as a “human weapon system” iscritical to attaining the goal of a healthy and fit force. The humanweapon system requires the same level of “life-cycle” support and main-tenance as other complex Air Force systems. Applying this principle tooccupational and operational environments enhances force preparednessand contributes to the force’s emotional and physical strength. The fol-lowing activities work together to minimize force vulnerability to envi-ronmental or enemy threats or attacks. (See figure 1.1.)
Doctrine is everybody’s business in the Air Force.
Major General I.B. Holley, Jr.USAFR, Retired
The leading idea, which should be constantly kept in view, is tostrengthen the hands of the Commanding General by keeping hisarmy in the most vigorous health, thus rendering it, in the highestdegree, efficient for enduring fatigue and privation, and for fighting.In this view, the duties … are of vital importance to the success ofan army, and commanders seldom appreciate the full effect oftheir proper fulfillment.
Major Jonathan LettermanMedical Director of the Civil War
Army of the Potomac
2
������������� ������ ���������������� ����������
� Maintaining force health protection (FHP).
� Promoting health and fitness.
� Preventing illness or injury.
� Conducting health threat surveillance activities before, during, and af-ter force deployment.
If the Air Force does not emphasize prevention-oriented programs andhealth care to the warfighter, weapon systems are merely iron on theramp.
HISTORICAL PERSPECTIVE
The incidence of disease and nonbattle injuries (DNBI) has ex-erted a profound effect upon the Air Force readiness posture. Themajority of wartime hospitalizations have been DNBI, not combatwounds, that diminished the effectiveness and sustainability of fighting
�������������� �� ����������
��� � �����
�����������������
����� ��� �
����� �������� ������ ��
������ �����
����� ���������
!��"�������� ���
�����#�$
������� �
� ���� �%
���������
�
�
�
�
�
�
�
�
�
�
�
�
�
!�����
3
forces by at least a factor of ten from World War I through OperationDESERT STORM.
In aerospace operations, aircraft losses occurred most often in train-ing, not enemy action. Human factors such as fatigue, loss of situationalawareness, and spatial disorientation were the usual causes. On 13 No-vember 1917, Aviation Cadet Sidney J. Brooks, for whom Brooks Air ForceBase is named, was killed when his aircraft crashed while attempting tocomplete his final qualifying flight at Kelly Field. It is thought that hefainted in the cockpit possibly because of an antityphoid serum injectionhe received earlier in the day. Because of this and other such incidents orneeds, the Army Air Corps, (subsequently the Army Air Forces MedicalService) in World War II, began to research noncombat stresses and toimplement measures to protect flying personnel. Since 1950, the Air ForceMedical Service (AFMS) has steadily reduced the number of DNBI andthe amount of time lost to DNBI incidents or conditions.
During the 1980s, inflation of health care costs ran in the double digits.Businesses and unions could not afford to have these costs consume moreand more profits or absorb their benefit flexibility. The result was anexplosion of managed care principles focused on cost containment throughimproved use of health care resources with increased emphasis on effec-tive prevention activities. US military medical service leadership real-ized they too must implement these more efficient managed care prin-ciples. This resulted in creating the TRICARE system in the early 1990sand the force tailoring of the direct military medicine system. ThroughTRICARE, the Military Health System (MHS) partnered with civilian healthcare providers to focus military medical practice on prevention and onthe development of managed-care processes.
For the AFMS, in the past, operational medicine focused on returningfighting forces to duty, requiring a tremendous need for medical inter-vention. With changes in national security strategy, the Air Force mis-sion has shifted from European or Asian theater of war scenarios to mul-tiple, less predictable regional conflicts. The dramatic drop in projectedforce losses propelled the AFMS to minimize its deployable materiel andmanpower footprints and focus operational medicine on transporting “sta-bilized” versus “stable” patients and “evacuating and replacing” patientsversus “returning them to duty.”
Air Force health services face many challenges today. They must con-tinue to focus on enhancement and sustainment of aerospace operators
4
in all operational environments. Some of these include high-altitude op-erations, extended mission deployments, directed energy threats, night-vision requirements, and an advanced aeromedical evacuation capabilityincluding critical care air transport teams (CCATTs) that can function inlow-light, noisy conditions and limited workspace.
ROLES AND RESPONSIBILITIES
A healthy and fit force increases resiliency to overcome adver-sity. All personnel should make every effort to promote emotional andphysical health and fitness, both individually and as a unit. Health aware-ness can affect individuals in all operational and domestic lifestyles andactivities, extending from the work place (i.e., safety, occupational andenvironmental hazards) to the home (i.e., leisure activities, recreation,environmental factors).
Airmen
As the core component of the organization, airmen ensure their unitsucceeds in its mission. Airmen:
� Maintain individual health and fitness.
� Encourage peers, families, and organizations to lead healthy, fitlifestyles.
� Seek appropriate health care when required.
� Recognize occupational and environmental health risks.
Participation in local base health, wellness, sports, and fitness programscan assist airmen to maintain emotional and physical fitness.
Supervisors
As an intermediate level of leadership, supervisors monitor subordi-nates to ensure application of standards and take corrective actions. Su-pervisors:
� Promote an organizational climate conducive to good health and fit-ness concepts.
5
� Emphasize individual health and fitness maintenance.
� Provide time for airmen to maintain health and fitness standards.
� Recognize factors that negatively impact human performance.
� Improve the work environment and equipment design.
� Reinforce or reward individuals or units for healthful behaviors andperformance enhancements.
� Ensure individuals receive health care when required.
Base agencies play an active role in promoting the health and wellnessof warfighters, family members, and other beneficiaries. Supervisors areaware of these agencies or the availability of local programs to help andencourage subordinates to participate. These include, but are not limitedto, health promotion programs, family support and services, fitness cen-ters, recreation centers and activities, chaplain services, childcare, andthe health and wellness centers (HAWCs).
Commanders
Commanders are ultimately responsible for the morale, health, andwell being of their troops. Commanders:
� Balance individual and organizational health and fitness with unit mis-sion requirements.
� Ensure timely response to the needs of airmen and their families.
� Ensure personnel are aware of health threats and that they participatein prevention programs.
� Ensure troop fitness by applying programs to prevent DNBI.
� Ensure individuals receive health care when required.
� Ensure human performance measures are in place that develop andmaintain a healthy and fit force.
6
The necessary tools, such as prevention-oriented health programs andpopulation-based health care delivery, are in place to support the forcesacross the entire spectrum of military operations. All commanders shouldensure participation in periodic physical, medical, and dental assessmentsto achieve optimal compliance with health and fitness standards.
7
CHAPTER TWO
OPERATIONS
FORCE HEALTH PROTECTION OVERVIEW
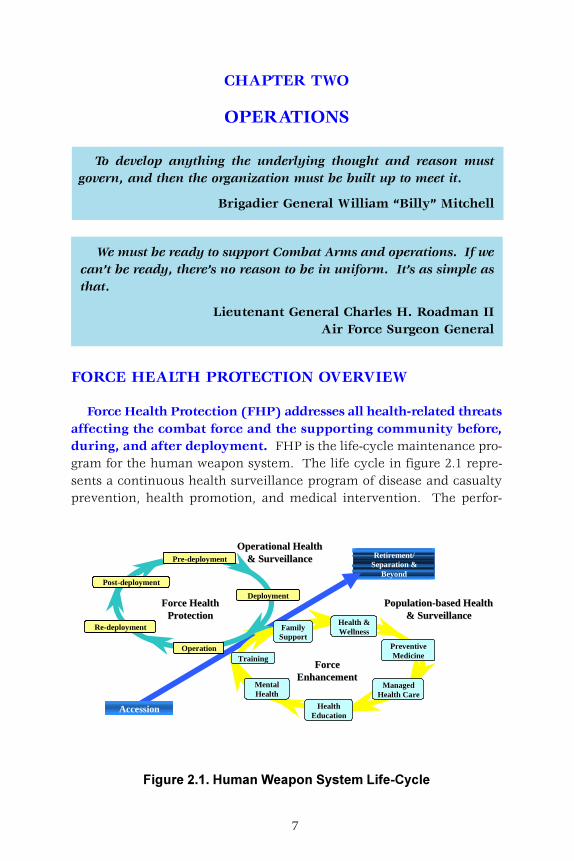
Force Health Protection (FHP) addresses all health-related threatsaffecting the combat force and the supporting community before,during, and after deployment. FHP is the life-cycle maintenance pro-gram for the human weapon system. The life cycle in figure 2.1 repre-sents a continuous health surveillance program of disease and casualtyprevention, health promotion, and medical intervention. The perfor-
To develop anything the underlying thought and reason mustgovern, and then the organization must be built up to meet it.
Brigadier General William “Billy” Mitchell
We must be ready to support Combat Arms and operations. If wecan’t be ready, there’s no reason to be in uniform. It’s as simple asthat.
Lieutenant General Charles H. Roadman IIAir Force Surgeon General
������������ ���� ���������������������
Retirement/Separation &
Beyond
Operational HealthOperational Health& Surveillance& Surveillance
FamilyFamilySupportSupport
Population-based HealthPopulation-based Health& Surveillance& Surveillance
TrainingTraining
Accession
Force HealthForce HealthProtectionProtection
ForceForceEnhancementEnhancement
Operation
Pre-deployment
Post-deployment
Re-deployment
HealthHealthEducationEducation
PreventivePreventiveMedicineMedicine
Deployment
MentalMentalHealthHealth
ManagedManagedHealth CareHealth Care
Health &Health &WellnessWellness

8
mance, enhancement, and sustainment of the human weapon systemrequire the same level of care as any other weapon system.
FHP encompassesthree interrelated ele-ments: a healthy andfit force, casualty pre-vention, and casualtycare management.
Healthy and FitForce
A healthy and fitforce is the necessary precondition for all other elements of FHP.A healthy and fit force focuses on the preventive components of psycho-logical, physical, and occupational health requiring a number of programsand components for its success. Physical fitness training, health promo-tion programs, family support services, occupational health programs,periodic health assessments, stress management, and managed care pro-grams for Department of Defense (DOD) beneficiaries are the buildingblocks for a healthy community.
Casualty Prevention
Casualty prevention concentrates on countering two types of threats:health threat and enemy threat. The health threat is composed of acomplex set of environmental and operational factors that combine toproduce DNBI—the largest number of military casualties. The enemythreat usually produces smaller numbers of more serious casualties. Fail-
9
ure to counter either threat jeopardizes mission accomplishment and ul-timately impacts achieving operational objectives. Medical readinessprovides the means to mitigate these threats.
Casualty Care Management
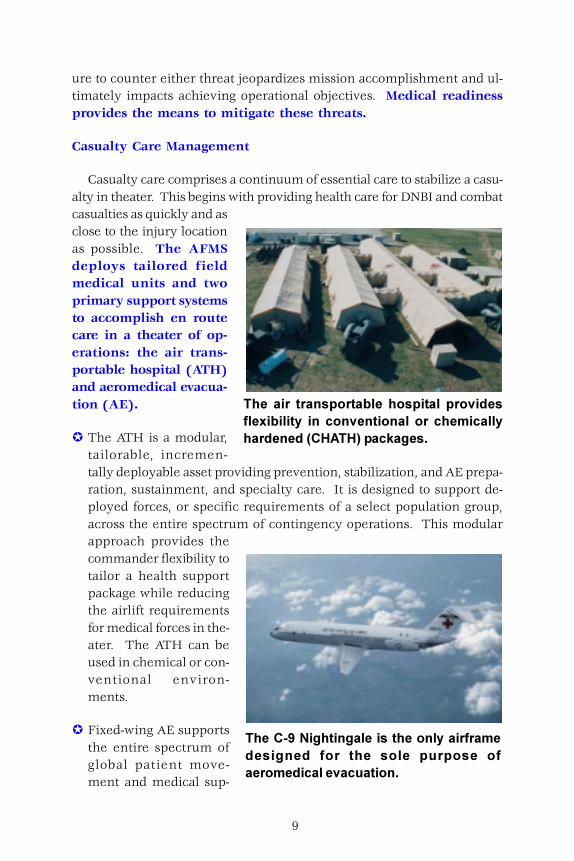
Casualty care comprises a continuum of essential care to stabilize a casu-alty in theater. This begins with providing health care for DNBI and combatcasualties as quickly and asclose to the injury locationas possible. The AFMSdeploys tailored fieldmedical units and twoprimary support systemsto accomplish en routecare in a theater of op-erations: the air trans-portable hospital (ATH)and aeromedical evacua-tion (AE).
� The ATH is a modular,tailorable, incremen-tally deployable asset providing prevention, stabilization, and AE prepa-ration, sustainment, and specialty care. It is designed to support de-ployed forces, or specific requirements of a select population group,across the entire spectrum of contingency operations. This modularapproach provides thecommander flexibility totailor a health supportpackage while reducingthe airlift requirementsfor medical forces in the-ater. The ATH can beused in chemical or con-ventional environ-ments.
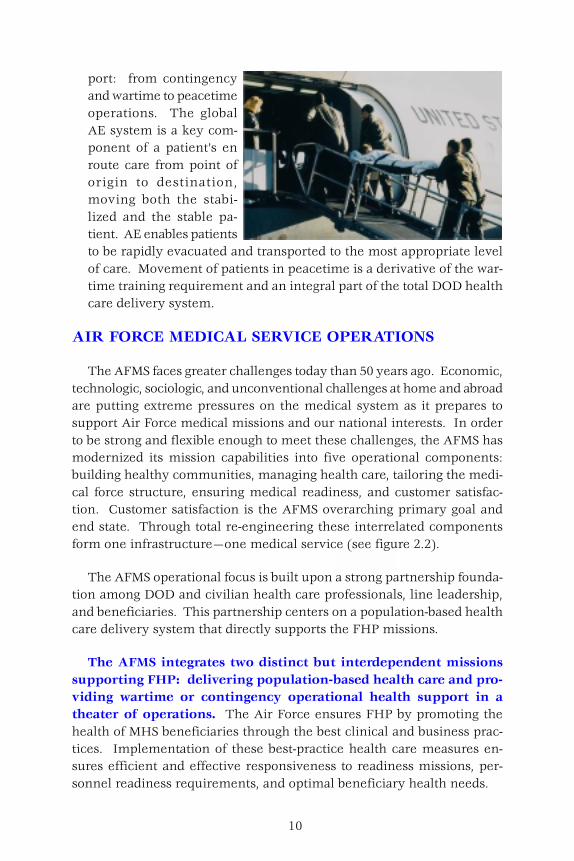
� Fixed-wing AE supportsthe entire spectrum ofglobal patient move-ment and medical sup-
���� ��� �� ������ ���� ������ �� ����� �����!�������� ��� ���������� �� ��� ������ ���� � ��� �"��#��$�� �% ���
������&�'������� ��������������� ���� �� ������ � ���� ���� ����� �������� �� ����� �� ���� �� ����
10
port: from contingencyand wartime to peacetimeoperations. The globalAE system is a key com-ponent of a patient’s enroute care from point oforigin to destination,moving both the stabi-lized and the stable pa-tient. AE enables patientsto be rapidly evacuated and transported to the most appropriate levelof care. Movement of patients in peacetime is a derivative of the war-time training requirement and an integral part of the total DOD healthcare delivery system.
AIR FORCE MEDICAL SERVICE OPERATIONS
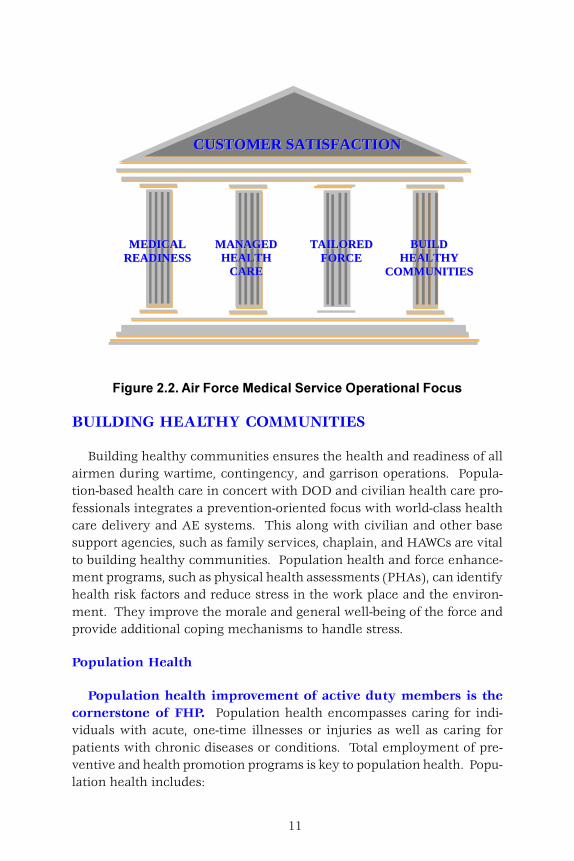
The AFMS faces greater challenges today than 50 years ago. Economic,technologic, sociologic, and unconventional challenges at home and abroadare putting extreme pressures on the medical system as it prepares tosupport Air Force medical missions and our national interests. In orderto be strong and flexible enough to meet these challenges, the AFMS hasmodernized its mission capabilities into five operational components:building healthy communities, managing health care, tailoring the medi-cal force structure, ensuring medical readiness, and customer satisfac-tion. Customer satisfaction is the AFMS overarching primary goal andend state. Through total re-engineering these interrelated componentsform one infrastructure—one medical service (see figure 2.2).
The AFMS operational focus is built upon a strong partnership founda-tion among DOD and civilian health care professionals, line leadership,and beneficiaries. This partnership centers on a population-based healthcare delivery system that directly supports the FHP missions.
The AFMS integrates two distinct but interdependent missionssupporting FHP: delivering population-based health care and pro-viding wartime or contingency operational health support in atheater of operations. The Air Force ensures FHP by promoting thehealth of MHS beneficiaries through the best clinical and business prac-tices. Implementation of these best-practice health care measures en-sures efficient and effective responsiveness to readiness missions, per-sonnel readiness requirements, and optimal beneficiary health needs.
11
BUILDING HEALTHY COMMUNITIES
Building healthy communities ensures the health and readiness of allairmen during wartime, contingency, and garrison operations. Popula-tion-based health care in concert with DOD and civilian health care pro-fessionals integrates a prevention-oriented focus with world-class healthcare delivery and AE systems. This along with civilian and other basesupport agencies, such as family services, chaplain, and HAWCs are vitalto building healthy communities. Population health and force enhance-ment programs, such as physical health assessments (PHAs), can identifyhealth risk factors and reduce stress in the work place and the environ-ment. They improve the morale and general well-being of the force andprovide additional coping mechanisms to handle stress.
Population Health
Population health improvement of active duty members is thecornerstone of FHP. Population health encompasses caring for indi-viduals with acute, one-time illnesses or injuries as well as caring forpatients with chronic diseases or conditions. Total employment of pre-ventive and health promotion programs is key to population health. Popu-lation health includes:
����������#���������(� �� ����������)��� ���� �������
MMAANNAAGGEEDDHHEEAALLTTHH
CCAARREE
TTAAIILLOORREEDDFFOORRCCEE
BBUUIILLDDHHEEAALLTTHHYY
CCOOMMMMUUNNIITTIIEESS
MMEEDDIICCAALLRREEAADDIINNEESSSS
CCUUSSTTOOMMEERR SSAATTIISSFFAACCTTIIOONN
12
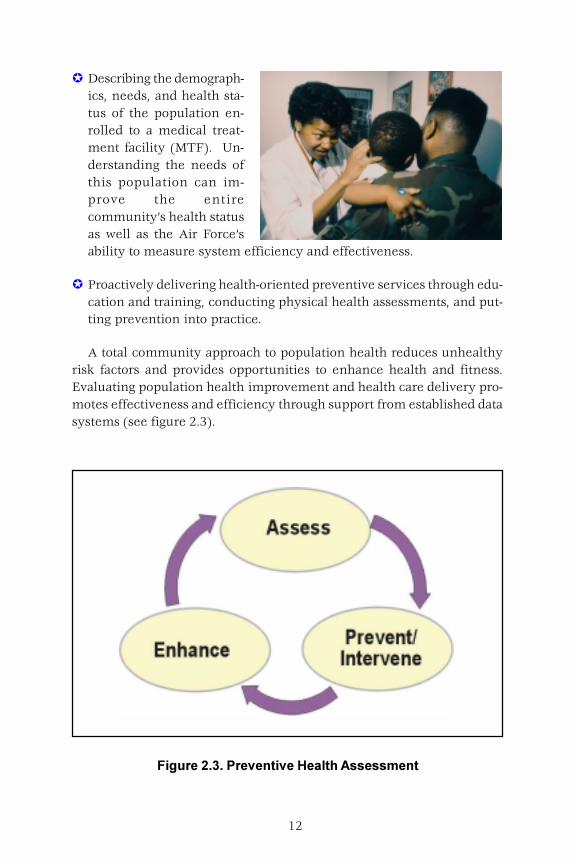
� Describing the demograph-ics, needs, and health sta-tus of the population en-rolled to a medical treat-ment facility (MTF). Un-derstanding the needs ofthis population can im-prove the entirecommunity’s health statusas well as the Air Force’sability to measure system efficiency and effectiveness.
� Proactively delivering health-oriented preventive services through edu-cation and training, conducting physical health assessments, and put-ting prevention into practice.
A total community approach to population health reduces unhealthyrisk factors and provides opportunities to enhance health and fitness.Evaluating population health improvement and health care delivery pro-motes effectiveness and efficiency through support from established datasystems (see figure 2.3).
��������*�+������������ ����#���������
13
Force Enhancement
Prevention-oriented programs in peacetime strengthen forceperformance during wartime, contingency, and MOOTW and de-creases combat casualties and DNBI. Participation in stress reducingrecreational activities and regular physical fitness programs enhancesperformance and minimizes limitations caused by illness and injury.Assuring garrison or deployed forces that their families have access tohealth care increases force effectiveness and decreases emotional stress.
Environmental safety and occupational health issues are included inprevention-oriented health programs. The health of the human weaponsystem in the work place and of the community is a vital part of forceenhancement. Anticipating, evaluating, and controlling risks that im-pact the health of the population optimizes productivity and performancein mission accomplishment. The AFMS’s direct involvement with hu-man performance and the design and operation of military weapon andsupport systems can increase effective airman-weapon system integra-tion.
MANAGED HEALTH CARE
Managed care is evolving toprimarily focus on prevention-oriented health care as a re-sult of changing technologyand health care industry stan-dards. Prevention-oriented,population-based health careis vital to supporting combatarms. Managed care is designedto meet peacetime operationaldemands and deliver world-classhealth care to Air Force and DOD communities. It enables AFMS person-nel to maintain the necessary skills and experience to mitigate diseaseand injury and render casualty management and treatment in support ofmilitary operations, humanitarian assistance, and MOOTW.
Leadership provides the foundation for managed care delivery througha coordinated and cooperative effort from the Air Force community.Warfighters and their families must have personalized health care thatconsiders the military member’s working environment and the stresses
14
involved at work and in thehome. The right numberand specialty mix of healthcare providers for individu-als are essential to optimiz-ing personalized healthcare. Evaluation and as-sessment of this “wholeenvironment” approachimprove or modify healthservices to meet customerneeds.
TAILORED FORCE
Health services assets may fill a supporting role for aerospace mis-sions, may operate in humanitarian or civic actions, or operate in con-junction with a multinational effort, a contingency, or war. To meetoperational and peacetime requirements, the AFMS organizes,trains, and equips to provide a ready medical force. The AFMS
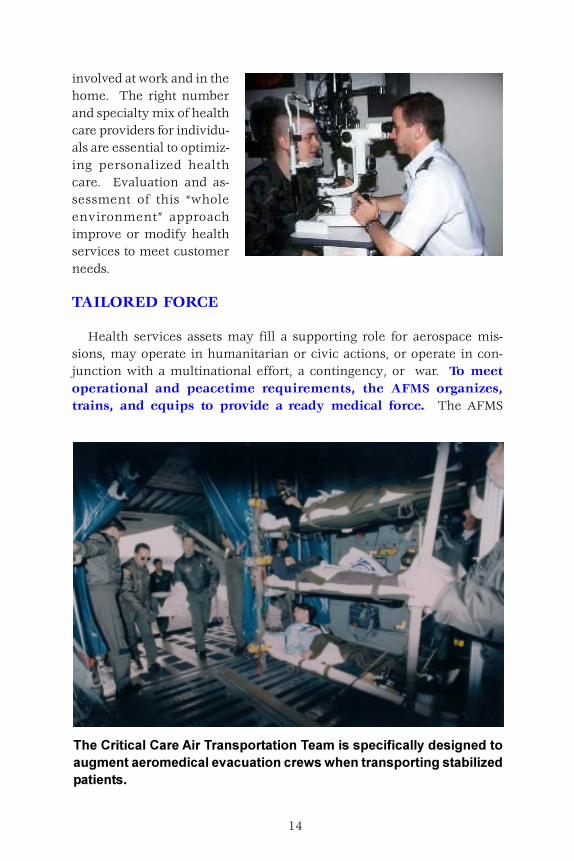
���������� ��� ���#����� ������ ������� ������������� ���� ������ ��� ������� ����� �� ���� �� ��������,��,������ ������������ ����-� � ������
15
provides an infrastructure designed to promote and sustain a medicallyready force throughout the entire spectrum of military operations.
AFMS assets are tailored to meet these specific operational and envi-ronmental requirements and include specialized medical units, expand-able ATH modules, and a fixed-wing AE system. Two examples of thesespecialized packages are the air transportable clinic (ATC) and the CCATT.
Total Force Management
The AFMS uses total force man-agement and tailors resources tomeet military unique missionsthrough mobile, lighter, and tailoredequipment and personnel unit typecodes (UTCs). The focus is on hav-ing the right force size and specialtyskills mix, at the right place, at theright time. From accessions to retire-ment, professional standards need tobe met to achieve the right forcestructure of health professionals.
Special Operations MedicalCapabilities
Special operations health servicespersonnel and equipment interfacewith traditional medical assets pro-viding an interoperable combat sup-port capability. Air Force specialoperations medical resources providesupport outside the boundary of tra-ditional medical infrastructure. These capabilities are usually in areas ofhigher health and operational threat. Special operations medical mis-sions provide:
� Operational medical flights with special operations forces medical ele-ments (SOFME).
� Special tactics personnel such as pararescuemen providing advancedcare for survival and recovery assistance.
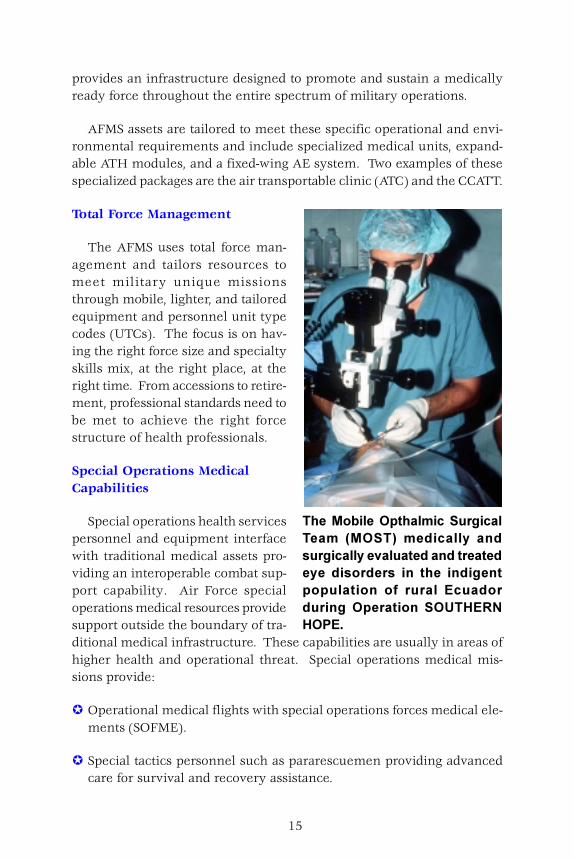
����(������)��� ����������� ��� �� "()��$� �� �� ���� � ������ ������ �� �� � � ���� �� ���� ���� ���� ��� ���� �� ���������� ����� ��� ��� �� .�� �� ������)��� ����� �)/��.0'�)+.
16
� Psychological preselection screening.
� Comprehensive medical and operational flight training to support deepoperations casualty evacuation via special operations aircraft.
� Focused medical logistics capability.
� Rapidly deployable, modular, small footprint equipment packages.
MEDICAL READINESS
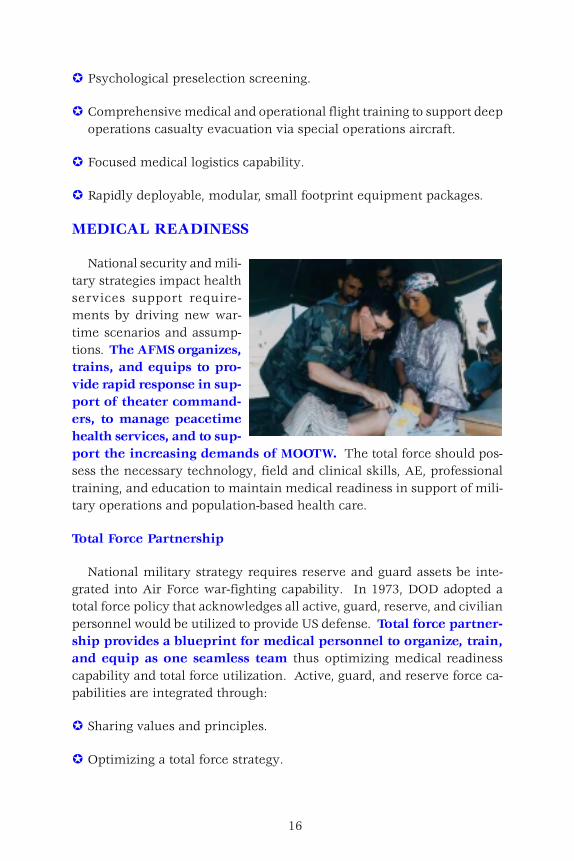
National security and mili-tary strategies impact healthservices support require-ments by driving new war-time scenarios and assump-tions. The AFMS organizes,trains, and equips to pro-vide rapid response in sup-port of theater command-ers, to manage peacetimehealth services, and to sup-port the increasing demands of MOOTW. The total force should pos-sess the necessary technology, field and clinical skills, AE, professionaltraining, and education to maintain medical readiness in support of mili-tary operations and population-based health care.
Total Force Partnership
National military strategy requires reserve and guard assets be inte-grated into Air Force war-fighting capability. In 1973, DOD adopted atotal force policy that acknowledges all active, guard, reserve, and civilianpersonnel would be utilized to provide US defense. Total force partner-ship provides a blueprint for medical personnel to organize, train,and equip as one seamless team thus optimizing medical readinesscapability and total force utilization. Active, guard, and reserve force ca-pabilities are integrated through:
� Sharing values and principles.
� Optimizing a total force strategy.
17
� Using technology effectively and efficiently.
� Training for joint taskings.
� Creating a dynamic environment to maximize force readiness andsustainability.
Education and Training
FHP addresses health-related threats affecting combat forces and thesupporting community, emphasizes disease and casualty prevention, andincludes health promotion, education, and medical intervention. Formaltechnical and professional training is needed to ensure force readinessand occupational, technical, and professional skills. Specialized training,such as self-aid, buddy care, and trauma life-support assist total force air-men and civilians in casualty care and management. Planners shoulddesign realistic training, exercises, and simulations to include health ser-vices support during military operations.
Technology Modernization
Integration of new technologies is vital to force readiness. The accel-erated pace of technological change and revolution in national strategybrings great pressure to bear on reducing infrastructure and demandscontinuous review and analysis of health services support. New drugtherapies, diagnostics, and modernization initiatives, such as filmless ra-diology, noninvasive vital signs monitoring, telemedicine, and hemor-rhage-stopping bandages will continue to ensure a light, mobile, expedi-tionary medical force. This modernization, integrated with war skills andhealth care protocols, enhances force survivability.
Employ the Force
During the transition to war or contingency operations, airmen per-form intense set-up operations in a new environment where they mustinitially adapt. Special attention to FHP and health and safety risks mustbe considered. As operational forces are received into the theater of op-erations, medical, civil engineering, and services personnel should ad-vise commanders on the proper setup of drinking water systems, foodpreparation and storage facilities, waste storage and disposal, fitness, rec-reational facilities, housing, industrial operations infrastructure, and other
18
public health and safety issues. This critical guidance on, and assistancein, bed-down planning activities help mitigate DNBI.
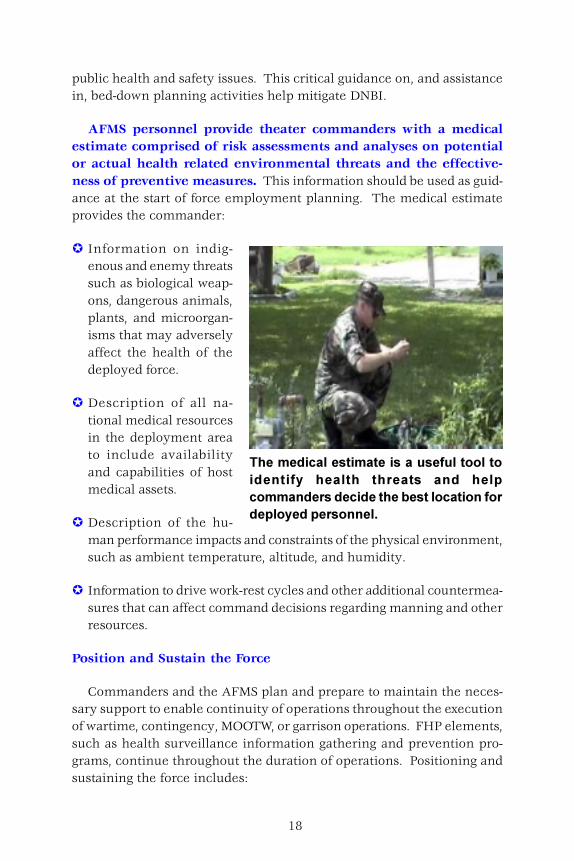
AFMS personnel provide theater commanders with a medicalestimate comprised of risk assessments and analyses on potentialor actual health related environmental threats and the effective-ness of preventive measures. This information should be used as guid-ance at the start of force employment planning. The medical estimateprovides the commander:
� Information on indig-enous and enemy threatssuch as biological weap-ons, dangerous animals,plants, and microorgan-isms that may adverselyaffect the health of thedeployed force.
� Description of all na-tional medical resourcesin the deployment areato include availabilityand capabilities of hostmedical assets.
� Description of the hu-man performance impacts and constraints of the physical environment,such as ambient temperature, altitude, and humidity.
� Information to drive work-rest cycles and other additional countermea-sures that can affect command decisions regarding manning and otherresources.
Position and Sustain the Force
Commanders and the AFMS plan and prepare to maintain the neces-sary support to enable continuity of operations throughout the executionof wartime, contingency, MOOTW, or garrison operations. FHP elements,such as health surveillance information gathering and prevention pro-grams, continue throughout the duration of operations. Positioning andsustaining the force includes:
������ �� ������� ������ ���������������� ������� �� ���� ���� ��� � � �������� � ���� ��� �������������� �������� ������ ����������
19
� Oversight of food, water, disease carrying pests, and other individual,occupational, or environmental health-related factors important to the-ater commanders.
� Protection of health records data. Although medical information isnot classified, it can become an operations security (OPSEC) indicatordepending upon the situation or mission. Eliminating these indica-tors may entail restrictions on medical information dissemination.
� Reduction of nuclear, biological, chemical (NBC) and conventional ef-fects on the operational forces. The AFMS employs protection mea-sures and support equipment to detect or counter potential and ad-verse NBC and conventional threats. In concert with civil engineeringpersonnel, medical support to the commander includes advice regard-ing chemical and biological detection systems.
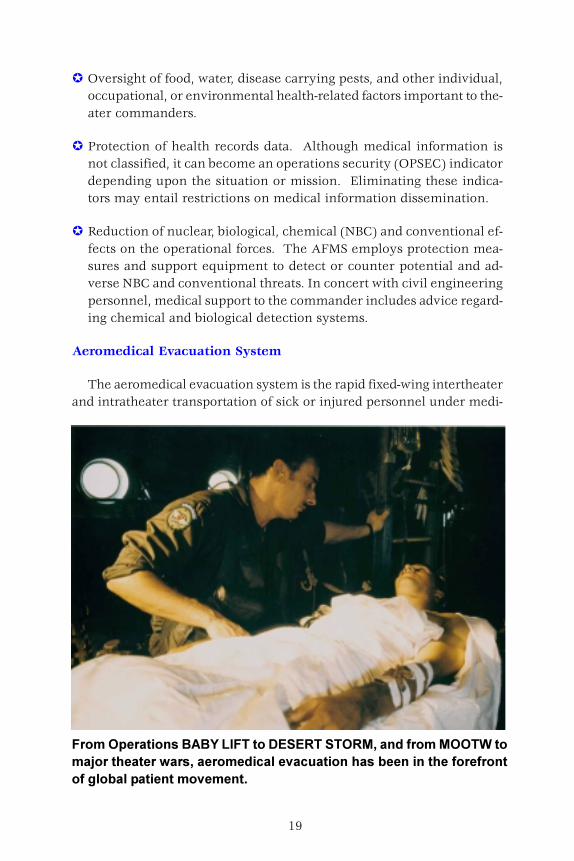
Aeromedical Evacuation System
The aeromedical evacuation system is the rapid fixed-wing intertheaterand intratheater transportation of sick or injured personnel under medi-
�����)��� ������1#12��3������4.�.0����)0(5� � ������())������ 6������ ����, ��5� ����� �� ���� �� ������ ������������������������������ ��� ��������������
20
cal supervision to appropriate levels of health care. Movement of patientsnormally requires specially qualified AE crewmembers to accompany thepatient, specific air traffic control considerations to comply with patientdriven altitude and pressurization restrictions, and special medical equip-ment. This robust and responsive system is highly capable of en routetreatment of stabilized and stable casualties. It is designed to quicklyevacuate patients who require more care than is available in theater, orlonger recovery than the theater evacuation policy mandates.
� Intertheater AE—Redes-ignated or dedicatedmilitary AE aircraft areused during daily opera-tions to transport pa-tients between the origi-nating theater and pointsoutside the theater, to in-clude the continentalUnited States (CONUS)and other theaters. Con-tingency intertheater AEwill normally be accomplished using dedicated Civil Reserve Air Fleet(CRAF) airframes. Redesignated or dedicated military AE aircraft maybe used on an urgent or priority basis or when AE CRAF capability isexceeded. Alternatives to AE CRAF or military aircraft may be pur-sued when competing airlift or evacuee requirements reduce airframeavailability. These alternatives could include using other organic mili-tary aircraft, even CRAF passenger aircraft, or obtaining authorizationfor commercial travel for ambulatory patients who do not require in-flight supportive medical care.
� Intratheater AE—Involves movement of patients within the theater ofoperations from aeromedical staging facilities (mobile and fixed) to thenext level of care facilities. This movement of casualties is usuallyaccomplished using dedicated or scheduled aeromedical aircraft.
Recover the Force
The AFMS plans for and maintains the ability to support postconflictoperations. All base services and force protection measures remain untilall personnel have departed from a deployment site. Planning begins
21
prior to deployment and continues throughout the mission or conflict,and includes:
� Reconstituting health records. Health records must document all health-related incidents and occupational and environmental exposures sus-tained by an individual while deployed. This is critical to follow-uphealth care of returning forces.
� Preparing for retrograde movement. Units returning to home stationmust perform decontamination, pack equipment, mark items for re-furbishment or disposal, and arrange for disposal of hazardous wastefollowing theater guidance and plans.
� Conducting medical surveillance. Effective, comprehensive, medicalsurveillance includes collecting relevant postdeployment health infor-mation from returning individuals. This ensures a valid database thatcan be used to provide comprehensive individual health care and en-sure a complete and reliable medical intelligence database for futuredeployments.
� Repatriating. Every major US military conflict includes the possibleevent of capture and detention of US forces. AFMS personnel mustplan for this possibility to provide appropriate follow-up care for repa-triated US prisoners of war (POWs), including their families, who alsoneed support during and after the conflict.
� Redeploying. During redeployment activities, Air Force personnel mayencounter numerous demands to attend to the needs of the indigenouspopulation. Close coordination and cooperation among military forcesand government or nongovernment agencies are particularly criticalduring the transition period when forces are redeploying and func-tions begin transferring to nonmilitary organizations.
Focused Medical Logistics
Focused medical logistics is comprised of four elements: joint theaterlogistics command and control (C2), CONUS reachback, time definitedelivery, and velocity instead of inventory. The fusion of positive con-trol, information, and transportation enables the Air Force to rapidly or-der, ship, track, shift, and deliver medical materiel on time directly to thewarfighter. The term “positive control” as it pertains to focused medical
22
logistics is the direct integration and control of all functions in the supplychain, including procurement, transportation, and distribution. OtherServices and the Defense Logistics Agency may provide assistance. Fo-cused medical logistics reduces lead-time, transportation requirements,duplicate orders, overstocking, and the in-theater “footprint” of theaterbuffer stock. Buffer stock is the minimum quantity of life saving andother critical materiel to sustain operations if the flow of materiel is dis-rupted.
When considering deployable platform equipment and supplies, or theacquisition of either, emphasis should be placed on multiuse, easily main-tainable, and commercially available products. Maximum standardiza-tion of pharmaceutical and medical-surgical equipment and suppliesamong Services should be an important consideration for joint planning.
CUSTOMER SATISFACTION
A customer-focused culture centers on FHP and prevention-orientedhealth programs and processes. Customer satisfaction, from the theatercommander to the family member or beneficiary, is a result of effectivecommunication, leadership, education, and training. Applying the bestclinical practices contributes to customer satisfaction and is a result ofconstant performance measurement and management as well as userevaluation of product delivery, services, and support systems. Commit-ment to answering the needs of the individual ensures stability and conti-nuity of world-class health care.
The people who make up our Air Force team are the most importantthing for our service to focus on. They are the foundation of ourstrength. We must recruit, train and retain the highest quality forcepossible. If we are to be successful, then we must take care of ourpeople and their families.
General Ronald R. Fogleman, USAF, RetiredAir Force Chief of Staff
23
CHAPTER THREE
COMMAND AND CONTROL
Health services must support the global responsibilities of the Air Force.The AFMS structure and processes are simple, responsive, and flexible tosupport joint or multinational operations. They are organized based onthe principle of “centralized control and decentralized execution” to ex-ploit asset flexibility and versatility. AFMS commanders ensure the mostcurrent health-related information is available to sustain the fighting force.Health information systems and programs required to facilitate this shouldbe in place and fall under the most direct command and control structurepossible to ensure timely support to the warfighters.
COMMAND RELATIONSHIPS
Clear and effective command relationships are central to effective op-erations. Health services C2 requirements are coordinated, integrated,and allocated, as appropriate, at the highest levels of C2 infrastructure.C2 relationships must remain flexible enough to meet any situational need,(i.e., the type of operation, mission objectives, existing host-nation infra-structure, or multinational participation). AFMS communications shouldbe reliable within the theater and from the theater to the CONUS. Thesecommunications should also link forward medical elements, through eachlevel of capability, to final destination hospitals. Development of Air Forcehealth systems should incorporate the changing nature of global opera-tions, e.g., emerging telemedicine capabilities. Health information man-agement systems provide:
� Interoperability with other DOD medical systems.
� Timely, accurate, and relevant information on blood management,patient tracking and movement, and medical logistics.
� Status of medical units, evacuation workload, and critical resources.
While commanders might incorporate some limited medical technol-ogy support into C2 systems, care must be taken not to violate the GenevaConventions, and thus cause medical facilities to loose their protectedstatus. For example, medical facilities cannot retain their protected statusand house information transfer nodes that will transmit data supporting
24
military operations, in addition to medical information. System develop-ers must understand these requirements to effectively implement andsupport aerospace and medical operations.
Chief of Staff of the Air Force and Headquarters, USAF
The Chief of Staff of the Air Force is responsible for organizing, train-ing, and equipping the fighting force. Headquarters, United States AirForce develops policy regarding C2 operations, reporting, training, andmaintenance operations, and maintains C2 integrity during military op-erations by allocating appropriate resources.
Air Force Surgeon General
The Air Force Surgeon General (SG) is primarily responsible for devel-oping and coordinating health care policy for the AFMS. The SG is alsoresponsible for coordinating and aligning health care programs and ser-vices to integrate with other Services’ medical departments and the Of-fice of the Assistant Secretary of Defense for Health Affairs (OASD-HA).This supports a DOD enterprise-wide health care system.
Major Commands
The Air Force organizes, trains, and equips air forces through majorcommands (MAJCOMs). The MAJCOMs provide forces to combatantcommands for employment. MAJCOM organizations are based on com-bat, mobility, space, and special operations, and the materiel support re-quired for those operations. For example, Air Mobility Command is theAE proponent for active and air reserve component forces. The MAJCOMSurgeon is responsible for planning and executing health services opera-tions to support wartime or contingency operations.
Air Force Forces
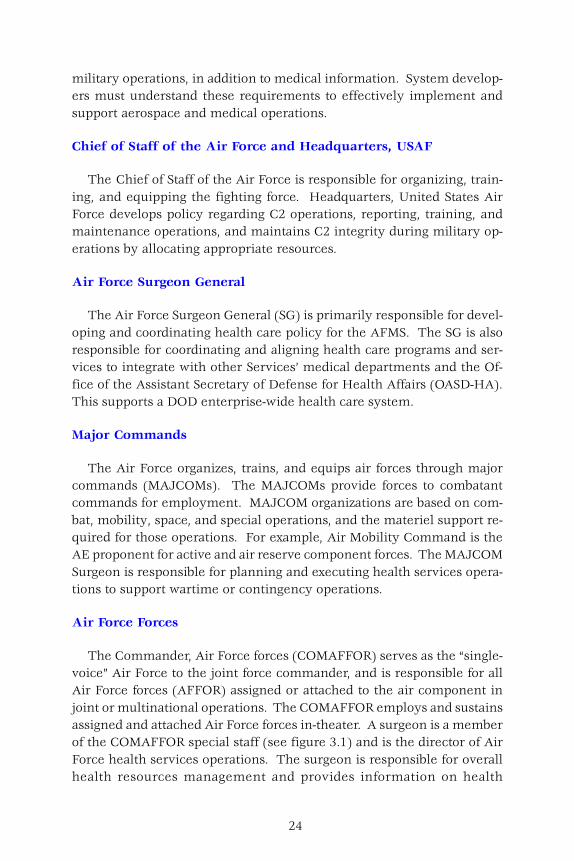
The Commander, Air Force forces (COMAFFOR) serves as the “single-voice” Air Force to the joint force commander, and is responsible for allAir Force forces (AFFOR) assigned or attached to the air component injoint or multinational operations. The COMAFFOR employs and sustainsassigned and attached Air Force forces in-theater. A surgeon is a memberof the COMAFFOR special staff (see figure 3.1) and is the director of AirForce health services operations. The surgeon is responsible for overallhealth resources management and provides information on health
25
surveillance and risk assessments, sustainment, and other force healthprotection issues.
The surgeon does not exercise direct control but provides a planning,coordination, and oversight role on the COMAFFOR special staff. Theorganizational structure represented in figure 3.1 is only one example ofhow a COMAFFOR can organize the staff.
Aerospace Expeditionary Force
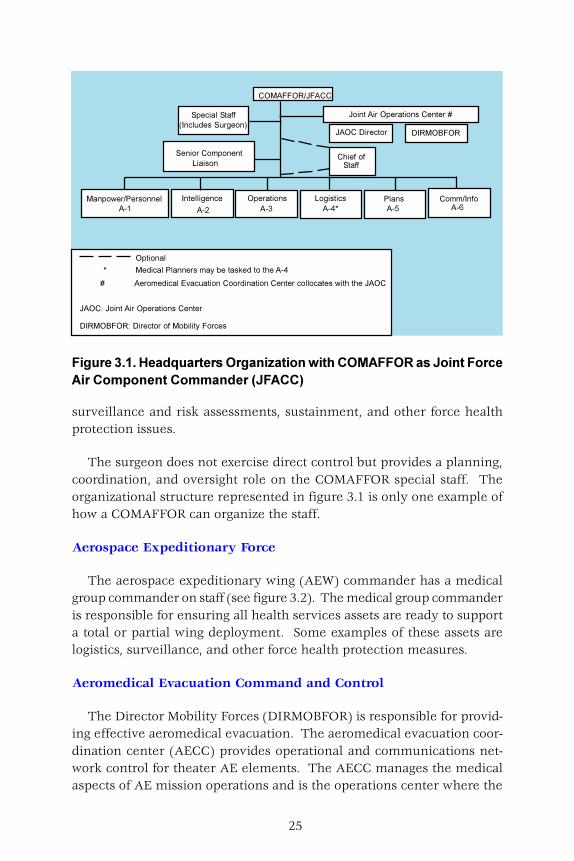
The aerospace expeditionary wing (AEW) commander has a medicalgroup commander on staff (see figure 3.2). The medical group commanderis responsible for ensuring all health services assets are ready to supporta total or partial wing deployment. Some examples of these assets arelogistics, surveillance, and other force health protection measures.
Aeromedical Evacuation Command and Control
The Director Mobility Forces (DIRMOBFOR) is responsible for provid-ing effective aeromedical evacuation. The aeromedical evacuation coor-dination center (AECC) provides operational and communications net-work control for theater AE elements. The AECC manages the medicalaspects of AE mission operations and is the operations center where the
������������ ���������������������������������������������������������������������� ���������
��������������
�� �������
�� ���������
�� ���� ������� ������������
������ ������ ���������
������ �����
���
����� ������
�� �� ����!"
#������$
��%%�������&
����'���#����������(
�
�� ����
��) ����#��������%�*�+�����,�)����������!
�� �����%����� � ���
-����.)���.�����/
����0��� ���� ������� ����������
���������0�� ������������+ � �*�������
�������������������%�) ����12��.�� �������) ��� ���������������������' �����������
26
overall planning, coordinating and directing of theater AE operations areaccomplished. The AECC is responsible for identifying and coordinatingAE airlift requirements, notifying the appropriate elements of airlift sched-ules, and monitoring the execution of AE missions to balance the require-ment for theater bed space and evacuation capacity. The AECC serves asthe liaison team in the Air Mobility Division for deployed medical units intheater and the tanker/airlift control center for air mobility assets. TheAECC should be deployed simultaneously and independently from the jointair operations center (JAOC) but requires collocation with JAOC (see figure3.1).
The Theater Patient Movement Requirements Center (TPMRC) is respon-sible to the theater CINC and is the centralized agency that initially identi-fies evacuee requirements to the next level of care. AE C2 elements actupon patient movement requests identified by theater CINC or US Trans-portation Command (USTRANSCOM) patient regulating and movementorganizations.
The Global Patient Movement Requirements Center (GPMRC) is the singlemanager for regulating intertheater patient movement to CONUS-basedmedical treatment facilities. The GPMRC centrally coordinates patient
��������!�"������#�����������$%�� �������&�'���
��%%.� ��� ���
������3�����
����%�) ���
����������
�������
����
����������
��������
����
4�����.����������� �������
5��������� ��
�� �� ���#����
����������
������
����
�����
��2 ���
� 2 ��1�� �����
� �� ��)�*���%�
��.� �*�������
�� ��
����������
��������
����
� ��������%+��
� �����.�� ��
� �� ��
����.��-���/4���������2 ���
�����
12��.�� �������%�) ���
���.���*�����
����%�) ������� ��
�����
�� �� ��.�2� ������
#������ ��������3�����
��)������%�� ����%%.� ��� ��
����� ����� ��
����� ���
�� �����%����� � ���
�14���
����
�����%�� ��
27
movement requirements and matches them with available, appropriate trans-portation.
OTHER CONSIDERATIONS
CONUS Reachback
A seamless data flow from the forward location through the entire sup-port pipeline must be in place to ensure the success of CONUS reachback.Tailored medical support packages with CONUS reachback capability arenecessary to fully optimize footprint reduction and minimize the logisticsstrain placed upon the theater. Early stabilization and evacuation coupledwith early reporting and notification for required replacements may alsoassure successful reachback efforts.
Participation in Joint Operations
The theater CINC or joint task force (JTF) commander has authority toorganize in a manner that provides optimum effectiveness for the mission.AF health services assets should be responsive and flexible to support
(�����)��**����+�)��� ����*�� ����#�����������+��������������������,��*�������� �,�#��&� �*� -����� *�����)� ���+� ���� ��� �**����+�� ��������� ����������������� ����������.'���������
28
changing theater operational requirements. Joint participation providessmaller, mobile, flexible, and enhanced elements tailored to provide es-sential care for missions ranging from major theater wars to MOOTW.
Base Operating Support
Base operating support should provide all necessary infrastructure priorto initiating prevention and other health care programs. Organizationalsupport structures should be in place to enable health services programsto function. This support may be provided from joint, host nation, orcoalition resources.
In-transit Visibility
In-transit visibility is the ability to instantaneously track the identity,status, and location of DOD unit and nonunit cargo, passengers, and pa-tients throughout the spectrum of military operations. AFMS personnelshould coordinate with logistics functions and Personnel Support for Con-tingency Operation (PERSCO) to provide timely and accurate informa-tion and accountability on all patients and medical materiel.
Resources, Sourcing, and Distribution
The COMAFFOR retains the ability to source, distribute, and redistrib-ute theater force support resources after coordination with the JFC. Thesurgeon retains the capability to meet AFFOR requirements using CO-NUS reachback as the primary resupply method, focusing on velocity notinventory; this phrase refers to the requirement for medical logistics sup-port to be responsive, flexible, and precise. It must also deliver a timelyflow of material direct to the warfighter.
Retrograde Management
An aggressive retrograde support program adjusts to existing opera-tional demands through flexible procedures and priority movement ofassets. The AFMS plans retrograde management to ensure maximumrecovery of health services assets.
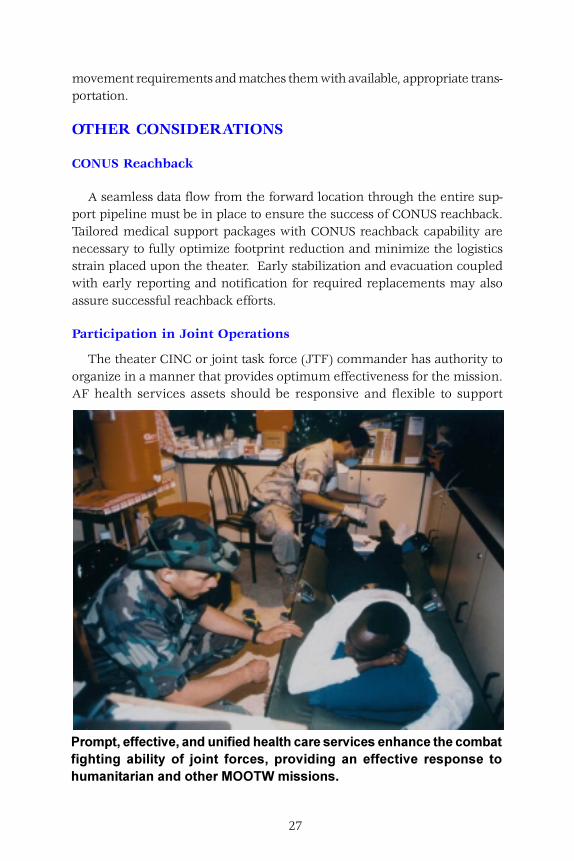
������������������� ��������������������������
29
Suggested Readings
Air Force Publications
AFDD 1, Basic Air Force Doctrine.
AFDD 2, Organization and Employment of Aerospace Power.
AFDD 2.3, Military Operations Other Than War.
AFDD 2-4, Combat Support.
AFDD 2.4-1, Force Protection.
Joint Publications
Joint Pub 4-02, Doctrine for Health Services Support in Joint Operations.
Joint Pub 4-02.1, Joint Tactics, Techniques, and Procedures for Health Ser-vices Logistics Support in Joint Operations.
Joint Pub 4-02.2, Joint Tactics, Techniques, and Procedures for Patient Move-ment in Joint Operations.
Joint Pub 6-0, Doctrine for Command, Control, Communications, and Com-puters (C4) Systems support to Joint Operations.
Other Publications
Article 21. Geneva Convention for the Amelioration of the Condition ofthe Wounded and Sick in Armed Forces in the Field (GSW). 12 August1949.

30
31
Glossary
Abbreviations and Acronyms
AE aeromedical evacuationAECC aeromedical evacuation coordination centerAFDD Air Force doctrine documentAFFOR Air Force forcesAFMS Air Force Medical ServiceAFRC Air Force Reserve CommandAMC Air Mobility CommandATC air transportable clinicATH air transportable hospital
C2 command and controlCCATT Critical Care Air Transport TeamCHATH chemically hardened air transportable hospitalCINC commander in chief; commander of a combatant
commandCOMAFFOR Commander, Air Force forcesCONUS continental United StatesCRAF Civil Reserve Air Fleet
DIRMOBFOR Director Mobility ForcesDNBI disease and nonbattle injury
FHP force health protection
GPMRC Global Patient Movement Requirements Center
HAWC health and wellness center
JAOC joint air operations centerJFACC joint force air component commanderJP joint publicationJTF joint task forceMAJCOM major command
MHS Military Health SystemMOOTW military operations other than warMOST Mobile Ophthalmic Surgical TeamMTF medical treatment facility
32
NBC nuclear, biological, and chemical
OASD-HA Office of the Assistant Secretary of Defense forHealth Affairs
OPSEC operations security
PERSCO Personnel Support for Contingency OperationPHA physical health assessmentPOW prisoner of war
SG Surgeon GeneralSOFME special operations forces medical elements
TPMRC Theater Patient Movement Requirements Center
USTRANSCOM United States Transportation CommandUTC unit type code
Definitions
aeromedical evacuation. The movement of patients, under medicalsupervision, to and between medical treatment facilities by air transpor-tation. Also called AE. (JP 1-02)
aeromedical evacuation coordination center. A coordination center,within the joint air operations center’s airlift coordination team, whichmonitors all activities, related to AE operations execution. It managesthe medical aspects of the AE mission and serves as the net control sta-tion for AE communications. It coordinates medical requirements withairlift capability, assigns medical missions to the appropriate AE elements,and monitors patient movement activities. Also called the AECC. (JP 1-02)
aeromedical evacuation system. A system that provides: a. control ofpatient movement by air transport; b. specialized medical aircrew, medi-cal crew augmentees, and specialty medical attendants and equipmentfor inflight medical care; c. facilities on or in the vicinity of air strips andair bases for limited medical care of intransit patients entering, en routevia, or leaving the system: d. communication with originating, destina-tion, and en route medical facilities concerning patient transportation.(JP 1-02) [A system that provides control of patient movement by air. Includes
33
specialized medical aircrews, medical crew augmentees, and specialty medicalattendants and equipment for in-flight medical care; facilities on or in the vi-cinity of air strips and air bases for medical care of in-transit patients, andcommunication with originating, destination, and enroute medical facilitiesconcerning patient transportation.] {Italicized definition in brackets appliesonly to the Air Force and is offered for clarity.}
air force medical service. The title given to the Air Force medical com-munity. Encompasses every health care discipline such as: physicians,nurses, technicians, dentists, bioenvironmental engineers, medical admin-istrators, etc. Also called the AFMS.
air transportable clinic. The air transportable clinic (ATC) providesthe equipment for aerospace medical support to flying squadrons and adeployed population of 300-500 personnel. Capabilities include very lim-ited outpatient clinical services and initial trauma response for 30 days.The ATC is dependent upon base operating support such as power andtranspiration and assumes other medical facilities are available and pro-vides hospital services, aeromedical evacuation, and necessary back-upsupport. The ATC is generally staffed by a Squadron Medical Element(SME).
air transportable hospital. The air transportable hospital (ATH) is thepremier deployable medical system composed of subcomponent build-ing blocks so medical capabilities, airlift, and support requirements canmatch specific operational requirements. The ATH provides medical ser-vices and theater hospitalization throughout the entire spectrum of con-tingencies from humanitarian operations to major theater wars (MTWs).The ATH can expand up to a 50-bed facility with the ability of supporting3000-5000 personnel for 30 days, providing second level and limited thirdlevel of care capabilities. These capabilities include Advanced CardiacLife Support (ACLS); Advanced Trauma Life Support (ATLS); emergencyservices; outpatient services; limited in-patient holding capability; resus-citative, general, and orthopedic surgery; laboratory services; x-ray ser-vices; pharmacy services; dental services; medical maintenance, and ad-ministration. It also provides the capability to stabilize casualties for re-turn to duty or evacuation.
casualty. Any person who is lost to the organization by having beendeclared dead, or by duty status-whereabouts unknown, missing, ill, orinjured. (JP 1-02)
34
chemically hardened air transportable hospital. The chemically hard-ened ATH (CHATH) shelter is formed of sections of TEMPER tents inwhich a chemical/biological protective liner is installed and an over-pres-sure environment is created. Airlocks allow the movement of medicine,food, water, and waste in and out of the CHATH without compromisinghospital cleanliness or chemical and biological protection. A chemicallyhardened air management plant (CHAMP) is a major component of theCHATH, and is used to create the required “over-pressure” and air filter-ing capability for the hospital.
en route care. Enroute care requires the use of state of the art, light-weight critical care equipment to ensure the evacuation system is able tosuccessfully transport a patient from the point of injury or illness to de-finitive care. (JP 4-02)
equipment. In health services, to prevent health threats caused by theenvironment, appropriate monitoring and control materiel should be madeavailable to prepositioned health services personnel prior to deploymentand employment of forces.
evacuation. The process of moving any person who is wounded, in-jured, or ill to and/or between medical treatment facilities. (JP 1-02)
focused medical logistics. Consists of four elements: 1. Joint TheaterLogistics Command and Control. Ensures clear lines of authority for re-sponsive logistics support and allows the commander in chief (CINC) toprioritize and allocate scarce Service resources to eliminate redundancyin theater. 2. CONUS Reachback. Requests for logistics support are for-warded from the theater directly to a sustaining base, usually CONUS.Reachback provides complete electronic commerce abilities, ensuring fullintegration with industry, total asset visibility, and seamless integrationof information systems. 3. Time Definite Delivery. “Just enough” requiredmateriel is delivered just before needed at precisely the right time andplace. 4. Velocity Not Inventory. Logistics support must be responsive,flexible, and precise. It must deliver a constant and rapid flow of materieldirect to the warfighter.
focused medical logistics distribution. Tactical: This level of focusedmedical logistics takes place at the deployed unit and joint theater levels.It requires fully integrated systems and processes in the form of a jointmedical logistics distribution and management element. Operational: This
35
level of focused medical logistics is currently located at Fort Detrick, MD,in the form of a Global Medical Logistics Operations Center whose pur-pose is to plan and to prepare to support the CINC’s medical require-ments. Strategic: This level of focused medical logistics provides for anagile and flexible procurement and distribution system for the medicalcommunity. It is responsive to rapidly changing requirements that moveswithout interruption or organizational barriers from industry to the field.
force health protection. Force health protection (FHP) is the term usedto describe the integrated preventive, surveillance, and clinical programsthat are designed to protect the “total force.” The goal of FHP is to providea fit and healthy force when and where the mission requires, while simul-taneously adapting the medical forces to a technologically advanced forcethat is smaller and more mobile. FHP is about preventing medical threatsfrom affecting military forces. It is designed to improve existing health,proactively address health threats, and finally provide care for any illnessor injury that does occur.
forward aeromedical evacuation. That phase of evacuation which pro-vides airlift for patients between points within the battlefield, from thebattlefield to the initial point of treatment, and to subsequent points oftreatment within the combat zone. (JP 1-02)
health threat. Health threats include potential enemy actions or envi-ronmental conditions that might act to reduce the effectiveness of fight-ing forces. Medical intelligence is key to countering medical threats andis produced from the analysis of information concerning medical aspectsof foreign areas that have potential impact on operations.
in-transit visibility. The ability to track the identity, status, and loca-tion of Department of Defense units, and nonunit cargo (excluding bulkpetroleum, oils, and lubricants) and passengers; medical patients; andpersonal property from origin to consignee or destination across the rangeof military operations. (JP 1-02)
managed care. A system of health care delivery integrating quality, ac-cess, and cost that provides world-class service.
medical regulating. The actions and coordination necessary to arrangefor the movement of patients through the echelons of care. This processmatches patients with a medical treatment facility which has the neces-sary health service support capabilities, and it also ensures that bed space
36
is available. (JP 1-02) [Process of selecting destination medical treatment fa-cilities with the necessary medical services support capability for patients be-ing medically evacuated, between, into, or out of different theaters of geographiccombatant command and CONUS, or routine missions supporting popula-tion-based health care.] {Italicized definition in brackets applies only to theAir Force and is offered for clarity.}
patient. A sick, injured, wounded, or other person requiring medical/dental care or treatment. (JP 1-02)
population-based health care. The process of improving the overallhealth of a defined population through needs assessment, proactive de-livery of preventive services, condition management, and outcomes mea-surements. Needs assessment describes the characteristics and needs ofindividuals and groups in the population. It forms the basis for preven-tion/intervention program development, delivery, and effectiveness.Proactive delivery of preventive services is the foundation for improvingpopulation health. Prevention can be considered part of the set of indi-vidual and population conditions to be managed. Condition managementis the efficient delivery of evidence-based interventions. Outcomes mea-surements evaluate the population’s health-status improvement and thedelivery system’s effectiveness and efficiency.
population health. The health of defined populations and what deter-mines their health status. This includes the aggregate effect of individualphysiological, behavioral, and physical characteristics; economic and so-cial factors; external forces impinging upon the population, such as chemi-cal and physical environmental factors; and the effect of resource invest-ment of those multiple determinants.
population needs assessment. The process of collecting, analyzing,and describing individual and group characteristics (age, gender, occupa-tion, educational level, domicile, etc.) and health needs and practices (cur-rency for preventive services, risk factors, health-care utilization, etc.)within a defined population.
special operations forces medical element. The Special OperationsForces Medical Element (SOFME) personnel provide quality medical careto special operations warfighters. Prevention and treatment of diseaseand illness is a mission requirement and recognized as a force multiplier.When required, SOFME personnel are trained to provide medical careaboard special operations aircraft, for the movement of patients from
37
forward areas in or near the combat zone, to other points of definitivemedical care.
squadron medical element. The Squadron Medical Element (SME) is ateam of two independent medical technicians (IDMT) and one flight sur-geon assigned to a flying squadron. The SME deploys with and providesgeneral medical support to that flying squadron. See air transportableclinic.
stabilized patient. A patient whose airway is secured, hemorrhage iscontrolled, shock treated, and fractures are immobilized. (JP 1-02.)
stable patient. A patient for whom no inflight medical intervention isexpected but the potential for medical intervention exists. (JP 1-02.)

38