-
8/14/2019 Airbus A320 Bahrain
1/8
26 FLIGHT SAFETY AUSTRALIA NOVEMBERDECEMBER 2003
COVER STORY
Can courtesy
kill?
-
8/14/2019 Airbus A320 Bahrain
2/8
FLIGHT SAFETY AUSTRALIA NOVEMBERDECEMBER 20 03 27
ACAPTAINS FEARS that his
company would frown on him
if he conducted a missed
approach is one possible factor
in the fatal crash of a Gulf Air
A320 into the shallow waters of the
Arabian Gulf.
The failure of the first officer, a shy,
polite type, to take issue with the captains
decision to execute a 360-degree orbit
instead of a missed approach and go
around, is another possible factor in the
accident, near Bahrain International
Airpor t on August 23, 2000.
However, as with many aviation disas-
ters, the crash of GF-072 represents a
failure of the aviation system. The inves-
tigation revealed a complex series of
human, organisational and management
influences that combined to set the scene
for the accident, which culminated in thecrews failure to
respond to insistent
warnings to pull up from the aircrafts
ground proximity warning system
(GPWS).
A multinational team of accident inves-
tigators set up by the Kingdom of Bahrain
in accordance with international civil
aviation agreements found no technical
deficiencies in the aircraft or its systems.
The investigators attr ibuted the tragedy
mainly to human factors at the individual
and organisational level.They turned up
evidence of errors and procedural viola-tions committed by the
flight crew, and of
long-standing organisational and manage-
ment problems that had been identified
but not rectified.
GulfAir has since acted on many of the
recommendations made in the Accident
Investigation Boards report on the crash
and plans to implement the rest.
It is establishing a new integrated safety
management system, and has beefed up
its safety department, while stepping up
internal safety promotion.
Gulf Air flight GF-072 was a scheduledservice from Cairo
International Airport
to Bahrain International Airport (BAH).
It was operated by an Airbus Industrie
Embarrassment about making a mistake, reluctance to
challenge a captains decision and spatial disorientation
are possible factors in an accident that killed 143 people.
But, as John Mulcair and Rob Lee report, there is much
more to the story.
PH
OTO:AAP
-
8/14/2019 Airbus A320 Bahrain
3/8
28 FLIGHT SAFETY AUSTRALIA NOVEMBERDECEMBER 2003
DIETMARSCH
REIBER
A320-212. There were two pilots, six cabin
crew and 135 passengers on board.
When GF-072 was about one nm from
touchdown and at an altitude of about 600
ft, Bahrain air traffic control approved the
crews request for a 360-degree left-hand
orbit.
On completion of this manoeuvre, the
aircraft was about parallel to but beyond the
extended centreline of the landing runway,
and the crew initiated a missed approach.
With a radar vector offered by ATC, GF-072
overflew the runway in a shallow climb to
about 1,000 ft.
The aeroplane crashed into the sea about
four kilometres north-east of the airport at
about 1930, Bahrain local time. The debris
field was 700 m long and 800 m wide. Most
of the aeroplane was recovered, along withall significant
structural components, flight
control surfaces and both engines. There was
no evidence of pre-crash failure or fire
damage.
The crew GF-072s last flight began with thearrival of its crew
at the gate 25 minutes
before the scheduled departure time of 1600.
The airliner was under the command of a
37-year-old captain who had joined GulfAir
in 1979 as a cadet flight engineer. He had
later retrained as a pilot, flying on the Boeing
767 and Airbus A320 as a first officer, and,
since 1996, as a supervisory first officer.He was promoted to
captain on the Airbus
A320 on June 17, 2000. He had logged total
pilot time of 4416 pilot hours, 86 of which
were as pilot in command on the A320.
Gulf Air pilots who had flown with him
described him as responsible, knowledge-
able,open to suggestions,happy,very helpful,
professional and sharp. They differed on
whether he was overconfident.
Gulf Air hired the first officer, aged 25,
as a cadet on July 4, 1999, after he attended
its ab-initio training program. He was
promoted to A320 first officer on April 20,
2000.
He had accrued a total of 608 pilot hours,
made up of 200 hours in training, and 408
hoursrs as an A320 line pilot with Gulf Air.
Gulf Air pilots who had flown with the
first officer described him as timid, meek,
mild, polite, shy and reserved in social situ-
ations, and keen to learn.
While most felt his reserved nature would
not stop his speaking up dur ing flight oper-
ations, others felt he might have been too
reserved to challenge a captain.The crash After an uneventful
flight fromCairo, the aircraft was prepared for a visual
approach and landing on Runway 12 at
Bahrain. At the time, Runway 12 had no
instrument landing system.The weather was
fine, and the night was clear and dark with
no moon.
The conversation and sounds in the
cockpit for the 30 minutes before the acci-
dent were recorded on the cockpit voice
recorder (CVR).
At 1926:37,the captain stated:OK,visual
with airfield. Seconds later, the flight datarecorder (FDR)
showed that the autopilot
and flight director were disengaged.
At 1926:49 and about 2.9 nm from the
runway, the aircraft descended through
1,000ft. At 1926:51, with GF-072 about 2.8
nm from the runway, at an altitude of 976 ft
and a speed of 207 knots, the captain said:
Have to be established by 500 feet. Flaps
two were selected.
As the approach to Runway 12 continued,
the captain said at 1927:06, and again at
1927:13,.were not going to make it.
At 1927:23,he instructed the first officer to
tell him to do a 360 (degree) left (orbit).
Bahrain tower approved the request. The left
turn was initiated about 0.9 nm from the
runway, at an altitude of 584 ft and an
airspeed of 177 knots.
During the left turn, the flap configura-
tion went from flaps two to flaps three and
then to flaps full. At 1928:17, the captain
called for the landing checklist.
At 1928:28, with the Airbus about halfway
through the left turn, the first officer advised
that the landing checklist was complete.After completing about
three-quarters of
the 360-degree turn , the aircraft rolled wings
level.
The Airbus altitude during the left turn
ranged from 965 ft to 332 ft, while its bank
angle reached a maximum of about 36
degrees.
At 1928:57, after being cleared again by
Bahrain tower to land on Runway 12, the
captain stated:We overshot it.
The aircraft began to turn left again,
followed by changes consistent with an
increase in engine thrust. At 1929:07, thecaptain said:Tell him
going around. The
FDR indicated an increase to maximum
take-off/go around (TOGA) engine thrust.
Bahrain tower provided radar vectors,
with instructions to fly heading three zero
zero (300 degrees), climb (to) 2,500.
COVER STORY
The A320 that crashed into the Arabian Gulf in 2000, pictured a
year before the accident.
-
8/14/2019 Airbus A320 Bahrain
4/8
The auto thrust remained active throughout
the approach until TOGA was selected.
The flaps were moved to position three
and the landing gear was selected up. The
gear remained retracted until the end of the
recording.
At 1929:41,with the aircraft at an altitude
of 1,054 ft and an airspeed of191 knots,and
having just crossed over Runway 12, the
CVR recorded the beginning of 14 seconds
sounding of the repetitive chime of the auralmaster warning
consistent with a flap over-
speed followed by the first officer saying,
speed, overspeed limit
About two seconds after the master
warning began, and with the aircraft still
accelerating under TOGA power, the FDR
data indicated movement of the captains
side stick, which was held forward of the
neutral position for some 11 seconds, with a
maximum forward deflection of about 9.7
degrees.
During this time the aircrafts pitch atti-
tude decreased from about five degrees noseup to about 15.5
degrees nose down. The
recorded vertical acceleration decreased
from about +1.0 to about +0.5 G, while
airspeed increased from about 193 to about
234 knots.
About 1929:51, with the aircraft
descending through 1,004 ft at an airspeed of
221 knots, a single aural voice warning of
sink rate from the GPWS was recorded,
followed by the repetitive GPWS aural
warning whoop whoop, pull up, which
continued until the end of the CVR
recording.
At 1929:52, the captain requested, flapsup. About 1929:54, the
CVR indicated that
the master warning ceased for about one
second but began again and lasted about
three seconds.
Two seconds after the GPWS warnings
began, the captains side stick was moved aft
of the neutral position, with a maximum aft
deflection of some 11.7 degrees.
These data showed this nose-up
command was not maintained and subse-
quent movements never exceeded 50 per
cent of full-aft availability, and the aircraft
continued to descend. FDR data indicatedno movement of the first
officers side stick
throughout the approach and accident
sequence.
At 1929:59, the captain requested, Flaps
all the way and the first officer responded,
Zero!
This was the last comment from the crew
recorded on the CVR, which stopped
recording at 1930:02.
The FDR data showed continuous move-
ment of the flap position toward the zero
position after the captains Flaps up
command. The last flap position recorded on
the FDR was about two degrees ofextension.
The investigation To find out what visualcues the pilots had,
investigators retraced
the flight path of GF-072 in a helicopter.The
flight was carried out at night, in meteoro-
logical and visual conditions similar to those
on the night of the accident. The recon-
structed flight path was recorded on video.
The cockpit view calculations of the fieldof view from the A320
cockpit, supported by
the video reconstruction of the flight path,
indicated that all external visual cues were
lost about 1629:41 as the last lights on the
ground passed under the nose ofthe aircraft.
The forward sidestick input by the captain
started at 1629:45, when the aircraft was
accelerating into complete darkness.
Somatogravic illusion The crew would havebeen vulnerable to a
kind of spatial disori-
entation known as the somatogravic illusion.
The absence of visual cues combined with
rapid forward acceleration and the force of
gravity create a powerful pitch up sensation.
In such cases, particularly on dark night
takeoffs, pilots often respond by lowering
the nose. In some cases,the aircraft descends
and hits the ground, usually at a shallow
angle of impact.
The US Naval Aerospace Medical Research
Laboratory used the FDR data from GF-072
in a perceptual study. At the time of the
captains forward sidestick input at 1929:45,
he would have experienced a pitch-up sensa-
tion of about 12 degrees, the study showed.
The application of forward sidestick input
by the captain for 11 seconds resulted in theaircraft pitching
down to an angle of 15
degrees, which is the maximum pitch-down
angle allowed by the A320 flight control
system. This would have almost cancelled
out the perceived pitch-up sensation. In the
absence of any external visual cues, and with
its attention probably focused on the flap
overspeed, the crew probably believed it was
in near-level flight.
The cockpit instruments would have been
displaying the true pitch attitude of the
aircraft. However, the captain, as pilot flying,
did not use this source of information,suggesting that he did
not perceive the att i-
tude information from his Primary Flight
Display.
FLIGHT SAFETY AUSTRALIA NOVEMBERDECEMBER 20 03 29
COVER STORY
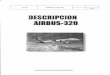
Perceived pitch versus actual pitch Just before the captain
pushed the sidestick
forward (t=1929:43). Source: Accident investigation report Gulf
Air Flight GF-072. See
http://www.bahrainairport.com/caa/gf072.html.
Perceived pitch Actual pitch
-
8/14/2019 Airbus A320 Bahrain
5/8
Other research after the accident included
studies to determine the effects of certain
variables on altitude loss during GPWS
recovery, simulations of the approach,orbit
and go-around of GF-072 at BAH, and a
series of flight tests.
Variables examined in the GPWS recovery
study were the amount of the pilots pitch-upcommand, the time
between the GPWS
warning and the pilots reaction to it, and the
duration of the pitch command input.
An A320 fixed-base engineering simulator
at Airbus Industries facilities at Toulouse,
France was used to simulate the approach,
orbit and go-around of GF-072.
The simulator also allowed investigators
to fly the approach to Runway 12 and to
observe cockpit warnings during flap over-
speed and GPWS warnings.
During one of the simulator sessions, the
360-degree turn and go-around manoeuvreswere performed to
approximate the flight path
and the sequence and timing of events recorded
on the FDR recovered from the aircraft.
The team considered several scenarios:
The pilots were instructed to recover with
full aft stick movement at the onset of the
GPWS alert. The simulator recovered with
about 300 ft altitude loss.
Half back stick was applied instead of
full back stick. The delay between th e
GPWS warnin g and the stick commandwas approximately four
seconds. The
simulator recovered with about 650 ft alti-
tude loss.
The co-pilot performed a recovery after he
had verified that the captain had taken no
action to recover from the GPWS alert. The
co-pilot depressed the priority button on his
side stick, announced his control override,
and applied full aft side stick input. The
simulator recovered with about 400ft of alti-
tude loss.
The 360-degree turn was performed but
the pilots were instructed to make no furthercontrol inputs
after selection of TOGA
power. The simulator tr immed nose down
to counter the noseup effect due to the thrust
increase and to maintain +1.0G, the target
when the side stick is in the neutral position
in Normal Law. The pitch remained positive
and the aircraft climbed slowly.
The 360-degree turn was initiated to match
the flight path and sequence and timing of
events recorded on the FDR. But instead of
rolling wings level upon reaching a headingof about 211 degrees
magnetic, as the
captain of GF-072 had done, the 360-degree
turn was continued at a moderate bank
angle at the pilots discretion to align with
Runway 12, and the approach and landing
were continued. The pilots were able to
successfully land on Runway 12 from the
360-degree turn.
In th is final scenario, the pilots noted that
the approach was not stabilised and little
time was available to successfully complete
the final approach and landing.
On September 27, 2000 a flight demon-stration in an A320 test
aircraft observed
various conditions similar to the flight
profile flown on August 23, 2000. It was
30 FLIGHT SAFETY AUSTRALIA NOVEMBERDECEMBER 2003
COVER STORY
A
CCIDENTINVESTIGATIONREPORTGULFAIRFLIGHTGF-0
72
-
8/14/2019 Airbus A320 Bahrain
6/8
FLIGHT SAFETY AUSTRALIA NOVEMBERDECEMBER 20 03 31
flown in daylight in visual meteorological
conditions.
Additional tests were performed to simu-
late the 360-degree orbit of the accident
flight, but continuing to turn at the end of
the orbit instead of rolling out.
Several scenarios were flown, with a
similar flap configuration sequence to that
in GF-072, or with full flaps.
The pilots were able to align the aircraft
with the runway and perform low
approaches down to 50ft where a go-around
was performed.
With no evidence that the accident was
caused by aircraft technical problems, the
investigation focused on human factors.
Investigators analysed the role and
performance of individuals as components
of a system.The considered systemic factors, such as
training deficiencies, inadequate procedures,
faulty documentation, lack of currency, poor
equipment design, poor supervision, failure
on the part of the company to take action on
previous violations and commercial pres-
sures to take shortcuts.
On the night of the accident, there was no
evidence the approach briefing in keeping
with standard operating procedures (SOPs)
had been carried out aboard GF-072.
Although the aircraft was established on
the VOR-radial of 301 degrees at the FAF
(final approach fix), other parameters were
far from the required standard for a
stabilised approach: the speed was 223 knots
instead of 136 knots; the flap position was
one instead of full, and the altitude was 1,662
ft rather than 1,500.
Unless the speed was reduced, the captain
could not have selected landing flaps to full.
Excessive speed was one reason for not
achieving the required stabilised approach
configuration.
Although the captain used speed brakes
three times from 1922:49 to 1926:13, he
could not achieve the required approachconfiguration before
reaching the FAF. The
aircrafts speed of 223 knots at the FAF was
87 knots greater than the target speed.
However, rather than initiating a missed
approach, the captain decided to continue
with the approach, during which the speed
remained excessive.
Investigators suggested the reason for the
excessive speed could be the planning of the
descent, or the omission of the descent clear-
ance from the descent profile.
The GF-072 simulation and flight tests
showed that, based on the aircraft configu-ration, speed and
altitude at the FAF, a
successful landing could have been achieved,
especially if the speed brakes had been
deployed continuously.
To do so would have involved manoeu-
vring with a steep approach angle and rapid
deceleration, however, and this would have
unsettled the passengers.
The captain did not stabilise the approach
on the correct path at 500 ft in the required
landing configuration, as required by
company SOPs.
When he apparently concluded that the
landing could not be made, the captain
elected to carry out a Three Six Zero to the
left. This was non-standard procedure.
Following the accident, Gulf Air issued a
fleet instruction that: Once an aircraft is
established and descending on the final
approach to the runway of intended landing,
360-degree turns and other manoeuvres for
descent profile adjustments are notpermitted.
The investigators concluded that the
circumstances in the cockpit and the behav-
iour of the captain indicated that he prob-
ably experienced information overload.
Departure from SOPs Even though GPWSvoice warnings to pull up
sounded every
second from 1929:51, neither flight crew
member responded according to SOPs.
Instead, the captain concentrated on
dealing with the flap over-speed which, at
that stage, was not a critical emergency situ-
ation endangering the aircraft.The investigators said the
accident could
have been prevented if the pilot flying had
adhered to SOPs.
Departures from SOPs, particularly
during the approach and final phases of
flight, included:
During the descent and the first approach,
the aircraft had significantly higher speeds
than standard.
During the first approach, standard
approach configurations were not
achieved, and the approach was not
stabilised on the correct approach path by
500ft. When the captain perceived that he was
not going to make iton the first approach,
standard go-around and missed approach
procedures were not initiated. Instead, the
captain executed a 360-degree orbit close to
the runway at low altitude with considerable
variations in altitude, bank angle and g
force.
A rotation to 15 degrees pitch up was not
carried out during the go around after the
orbit.
Neither the captain nor the first officer
responded to hard GPWS warnings. In the approach and final
phases offlight,there
were several deviations of the aircraft from the
standard flight parameters and profile.
During the approach and final phases of
flight, the first officer did not call out or draw
the captains attention to several deviations
from the standard flight parameters and
profile.
Big questions The investigators regardedtwo questions as
critical:Why did the captain
violate the SOPs, and why was there no chal-
lenge or comment from the first officer?
The captains sudden decision to execute
an orbit was apparently aimed at avoiding
the need for a standard missed approach
procedure. A missed approach is a perfectlyroutine safety
procedure, although in prac-
tice it is relatively rare. However, there could
be reasons why a captain might be reluctant
to carry out such a procedure.
At the time of the accident, a go-around
required the submission to the company of
an air safety report describing the circum-
stances.Although Gulf Air said its policy was
not to take action against pilots who had
conducted missed approaches, the investi-
gation found that some pilots at the time
believed, rightly or wrongly, that company
management would view such actions
unfavourably.As a post-accident safety initiative, Gulf
Air issued a fleet instruction, stating: All
pilots are further assured that no discipli-
nary action whatsoever will be taken against
any crew that elects to carry out a go around
for safety-related reasons, including inability,
for whatever reason, to stabilise an approach
by the applicable minimum height.
Another factor could be that captains
might have feared losing the respect of rela-
tively junior first officers if they executed
missed approaches.
Investigators said the CVR showed thatthe first officer
performed his routine role
of communicating with ATC, reading the
checklist and carrying out the checks.
COVER STORY
The investigators regarded
two questions as critical:Why did the captain violate
the SOPs, and why was
there no challenge or
comment from the first
officer?
-
8/14/2019 Airbus A320 Bahrain
7/8
32 FLIGHT SAFETY AUSTRALIA NOVEMBERDECEMBER 2003
However, it also revealed that he played
little effective part in flight deck manage-
ment and decision making. He did not raise
any issues with the captain or question his
decisions, even though the captain
performed non-standard procedures and
manoeuvres.
Crew resource management Evidence fromthe training records of
the first officer indi-
cated that he was seen as shy and
unassertive, and that his operational
performance overall was marginal.
However, investigators also observed that
at no stage during the approach did the
captain consult the first officer on any oper-
ational decisions. The first officer was a valu-
able, but untapped, resource available to the
captain, and crew resource management was
virtually non-existent in the cockpit of GF-072.
Although Gulf Air had been required by
Sultanate of Oman regulations to provide a
formal CRM training programme since June
1999, the original company CRM
programme, established in 1992 and active
unt il early 1997, appeared to have been
discontinued with a change ofmanagement.
The acting manager of human factors at
the time of the accident said that his prede-
cessor had resigned in frustration over his
attempts to re-establish the program.
Another factor contributing to the depar-
ture from SOPs could be that a company might not emphasise
strongly enough the
importance of, the reasons for and the need
to adhere to SOPs.
And although Gulf Air had a flight datamonitoring and analysis
system in place, the
system was not functioning satisfactorily at
the time of the accident. Such systems can
help identify the level of compliance with
SOPs by detecting events including unsta-
bilised approaches or times when an aircraft
had exceeded specific pre-programmed
parameters, such as airspeed, in a particular
configuration.
CFIT training CFIT (controlled flight intoterrain) accidents
account for the highest
proportion of fatalities in commercial aviation.
The CFIT training in the A320 fleet in GulfAir was severely
limited at the time of the
accident. Airbus Industr ies A320 normal
course syllabus includes a GPWS pull-up
demonstration. However, there was no
similar syllabus for Gulf Air and no require-
ment to execute such a demonstration for its
A320 fleet.
Nor did Gulf Airs A320 training program
emphasise GPWS response training. The
Airbus training program requires an instant,
instinctive side stick response when a hard
GPWS warning occurs.
Organisational deficiencies: The investiga-
tors found that from 1998 to the time of theaccident, the
manager of flight safety was the
only person in his department, and he did
not report directly to the highest executive
level within the company. They labelled this
a serious organisational deficiency.
They also noted that for many years Gulf
Air had not participated in the regular six-
monthly meetings of the International Air
Transport Associations safety committee, at
which the latest safety information is shared
freely and confidentially between airlines,
manufacturers and safety specialists.
This had greatly restricted GulfAirs aware-ness of developments
in areas such as acci-
dent investigation case studies,safety and risk
management, training and safety information.
COVER STORY
.. .airlines with positive
safety cultures, strongly
motivated towards
compliance with the
regulations, are in the
interests of the regulator.
Grim search Wreckage from Gulf Air Flight 072 is recovered from
the Arabian Gulf.
PHOTO:AAP
-
8/14/2019 Airbus A320 Bahrain
8/8
FLIGHT SAFETY AUSTRALIA NOVEMBERDECEMBER 20 03 33
The regulator: The investigators also exam-ined the relationship
between Gulf Air and
its regulator,the Sultanate of Omans Direc-
torate General of Civil Aviation and Meteo-
rology (DGCAM).
A review of correspondence between
DGCAM and GulfAir revealed letters citing
non-compliance with civil aviation regula-
tions (CARs). In some areas, GulfAir did not
rectify problems identified by DGCAM.
The company lacked several programs
required by CARs. And it did not meet
regulations in areas including crew
resource management, quality manage-
ment, safety awareness and other areas of
crew training.
An evaluation of Gulf Air carried out by
the International Civil Aviation Organisa-
tion for DGCAM in October 1998 turned upevidence of delayed or
non-compliance with
regulatory requirements.
The ICAO review concluded that, except
for isolated incidents, most of the infrac-
tions could be traced to inadequate super-
visory oversight within Gulf Air, rather
than a deliberate disregard for the regula-
tions.
DGCAM was well aware of this situation,
and had made many unsuccessful efforts to
correct it, including imposing various sanc-
tions on the airline.Despite this,GulfAir did
not implement many changes sought by
DGCAM.
A review of relevant information and
documentation covering the three years
preceding the accident indicated that, despite
intensive efforts,DGCAM could not get Gulf
Air to comply with some critical regulatory
requirements.
The investigators said regulatory authori-
ties and airlines had complementary roles in
maintaining the safety of the aviation system.
Strong and effective regulators are in the
interests of airlines because they provide an
independent means of quality control in
airline operations.
Conversely, airlines with positive safety
cultures,strongly motivated towards compli-
ance with the regulations, are in the interestsof the
regulator.
At the time of the accident, this was not
the case with the DGCAM and Gulf Air.The
regulator needs to check that airline
resources,structures and processes necessary
to ensure regulatory compliance are
adequate, the investigators said. It also needs
the political support of the government to
fulfill its safety role. This broader issue was
the subject of a specific recommendation in
the GF-072 investigation report.
Meanwhile,James Hogan, GulfAirs pres-
ident and chief executive, says a lot has
changed since the accident. The airline has
enhanced regular fleet instructions and
improved crew training, he says.
The airline now electronically analyses
flight data to ensure adherence to standard
operating procedures, while all GulfAir crew
must be trained intensively in CRM, says
Hogan,who took up his position at the helm
of the airline after the accident.
Gulf Air has incorporated into its flight
crew training program modules driving
home the risks posed by spatial disorienta-
tion, a problem also addressed in the first
issue of the companys upgraded safety
magazine.
And during the accident investigation,
Gulf Air reviewed its A320 flight trainingprogram. This led to
the reorganisation of
the companys operations division, a move
Hogan says ensures a high level of pilot
training.
John Mulcair is a journalist based in Sydney.
Rob Lee is an international aviation safety
consultant and former director of the Australian
Bureau of Air Safety Investigation. He was a
consultant to the Kingdom of Bahrain GulfAir
Bahrain investigation team.
COVER STORY