-
8/11/2019 ajr%2E04%2E1366
1/8
342 AJR:186, February 2006
AJR2006; 186:342349
0361803X/06/1862342
American Roentgen Ray Society
M E D I C A L I M A G I N G
A C E N T U R Y
O F
t al.
f Aortic
fication
C a rd i ac I ma g in g O ri g in al R es e ar ch
Aortic Valve Calcification as an
Incidental Finding at CT of theElderly: Severity and Location
asPredictors of Aortic Stenosis
Franklin Liu1
Courtney A. Coursey1
Cairistine Grahame-Clarke2
Robert R. Sciacca2
Anna Rozenshtein1
Shunichi Homma2
John H. M. Austin1
Liu F, Coursey CA, Grahame-Clarke C, et al.
Keywords:aortic valve, calcification, cardiovascular
disease, CT, heart, stenosis
DOI:10.2214/AJR.04.1366
Received August 31, 2004; accepted after revision
January 31, 2005.
1Department of Radiology, Columbia University Medical
Center, 630 W 168th St., New York, NY 10032. Address
correspondence to J. H. M. Austin.
2Department of Medicine, Columbia University Medical
Center, New York, NY 10032.
OBJECTIVE. The purpose of this study was to correlate the
severity and location of aortic
valve calcifications, as an incidental finding at chest CT of
elderly persons, with pressure gra-
dients across the valve.
MATERIALS AND METHODS. One hundred fifteen subjects who were 60
years old or
older and who showed aortic valve calcification on chest CT
(5-mm reconstructed section
width, no IV contrast material) and who had also undergone
transthoracic echocardiography
within 3 months of the CT examination were identified
retrospectively. Aortic valve calcifica-
tion scores (Agatston and volumetric) and subjective
calcification pattern scores (based on a 9-
point scale) were calculated and correlated with
echocardiographic gradients.
RESULTS. Thirty patients (26%) (median age, 81 years) were
identified who showed an in-
creased pressure gradient across the aortic valve at
echocardiography. Eighty-five subjects (74%),
including 30 age-matched but otherwise randomly selected control
subjects, showed no increase
in pressure gradient. The severity of aortic valve calcification
was greater for the 30 subjects with
an increased gradient than for the control subjects (p <
0.0001). Increased mean and peak gradi-
ents across the aortic valve correlated with the subjective
scores for aortic valve calcification
(r= 0.69 and 0.65, respectively;p < 0.0001), with Agatston
scores (r= 0.76 and 0.70, respec-
tively;p < 0.0001), and with volumetric scores (r= 0.78 and
0.73, respectively;p < 0.0001). In
terms of specific commissures, the greatest correlation with
mean and peak gradients was for pe-
ripheral left-posterior commissural calcification (r= 0.71 and
0.65, respectively;p < 0.0001) and
central rightleft commissural calcification (r= 0.69 and 0.66,
respectively;p < 0.0001).
CONCLUSION. The severity of aortic valve calcifications on chest
CT, as assessed eithersubjectively or objectively, correlated with
increased pressure gradients across the aortic valve,
particularly for calcification of the peripheral left-posterior
commissure and the central rightleft
commissure. These results indicate that the severity and
location of aortic valve calcifications on
chest CT are associated with an increased pressure gradient
across the aortic valve.
ortic stenosis is the most common
disease of a cardiac valve in in-
dustrialized countries and is mod-
erate to severe in 4.34.8% of per-
sons 75 years old or older [1]. It is the cause
of most surgical aortic valve replacements in
patients older than 75 years [2]. Over the past
60 years, the primary cause of aortic stenosis
has changed from rheumatic to senile degen-eration and
calcification [2].
Patients suspected of having aortic stenosis
usually undergo Doppler echocardiography as
part of the evaluation [3, 4]. Doppler quantifica-
tion of the systolic pressure gradient and of the
aortic valve area is useful for management deci-
sions because aortic valve area and systolic pres-
sure gradients (mean and peak) across the aortic
valve are recognized predictors of outcome [4].
Aortic valve calcification can sometimes
be seen on chest radiography, and the pres-
ence of such calcificationsusually best seen
on the lateral radiographis a sensitive
marker for clinically significant aortic steno-
sis [5]. CT is a sensitive imaging tool for de-
tecting focal calcifications, and we have noted
subjectively that aortic valve calcifications
are often seen as incidental findings on CT ofelderly persons
and that, moreover, these aor-
tic valve calcifications appear to show some
characteristic patterns. Recent studies have
shown correlations between CT measure-
ments of the severity of aortic valve calcifica-
tion and the severity of increased pressure
gradients across the valve [69]. Because the
severity and patterns of aortic valve calcifica-
tion offer the potential of aiding in presymp-
A
-
8/11/2019 ajr%2E04%2E1366
2/8
CT of Aortic Valve Calcification
AJR:186, February 2006 343
tomatic detection of aortic valve stenosis, we
undertook this study.
Materials and Methods
A medical informatics-assisted search of com-
puterized medical records at Columbia University
Medical Center yielded 1,257 adult patients, 643 ofwhom were 60
years old or older and had under-
gone both chest CT and transthoracic echocardiog-
raphy within a 3-month interval between 1999 and
2002. Study subjects were then chosen from these
643 patients. Any patient who had a bicuspid aortic
valve, cardiac transplant, or previous aortic valve
surgery was excluded from the study. Patients se-
lected for study each showed aortic valve calcifica-
tion on CT, which was performed without IV con-
trast material and reconstructed at a width of 5 mm.
Rheumatic valve disease, poor left ventricular func-
tion, and coexisting aortic regurgitation were not
exclusion criteria. These criteria yielded a pool of
115 patients. Thirty (26%) of these patients (19women, 11 men;
ages, 6192 years; mean, 79 9
[SD] years; median, 81 years) (study subjects)
showed evidence of an increased gradient across
the aortic valve at echocardiography, either as a
peak pressure gradient of 15 mm Hg or more, a
mean pressure gradient of 10 mm Hg or more, or
both. Among the 85 (74%) of these 115 patients
who showed aortic valve calcification on CT but no
evidence of an increase in pressure gradient across
the aortic valve at echocardiography (control sub-
jects), 30 age-matched control subjects (17 women,
13 men; 6391 years old; mean, 78 8 years; me-
dian, 80 years) were otherwise selected randomly.
Chest CT scans (0.75-sec scanning time per sec-tion, 120140 kVp,
200240 mA), each with the
patient in the supine position, were obtained on four
single-detector CT scanners (Somatom Plus-4, Sie-
mens Medical Solutions) using collimation of 5
mm, and on one 4-MDCT scanner (Siemens Vol-
ume Zoom) from August 1999 through December
2002. Images were reconstructed using a high-spa-
tial-frequency algorithm and reconstructed section
width of 5 mm. Each CT study was evaluated quan-
titatively for aortic valve calcification using Agat-
ston and volumetric calcification scores [10, 11]
(Vitrea 2 software, Vital Images) on a PACS
(Kodak) workstation. Pixels having a CT attenua-
tion of 130 H or greater were considered to beshowing
calcification [10]. The calcifications as-
sessed were limited to the region of the aortic valve
and specifically excluded any arcuate or other focal
calcifications of atherosclerosis of the aortic root,
calcifications of atherosclerosis of the proximal
right and left coronary arteries, and calcification of
the superomedial aspect of the mitral annulus.
All chest CT studies were also reviewed indepen-
dently (at soft-tissue settings of 350-H width and 35-
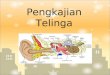
Fig. 1Diagram showscommissures of aorticvalve as seen en
face.Valve on CT of supinepatient is slightly obliqueto axial plane
but issimilar in appearance tothis schematic depiction.
Ac = central right-posterior commissure,Ap = peripheral
right-posterior commissure,Bc = central rightleftcommissure,Bp =
peripheral rightleftcommissure,Cc = central left-posterior
commissure,Cp = peripheral left-posterior commissure.
Bp
Bc
Ap
Ac
Cc
Cp
H center, and bone settings of 1,500-H width and
300-H center) by two experienced thoracic radiolo-
gists who were blinded to all clinical data except
each patients age and sex, including blinding to each
patients echocardiographic data. Aortic valve calci-
fications were characterized subjectively by the fol-
lowing criteria: presence and location (central or pe-
ripheral half for each commissure [Fig. 1]);
subjective grade of severity (scale of 19), both over-
all and in each location (Fig. 1); and number of 5-
mm sections with calcification present. The 9-point
subjective scale of severity corresponded to the fol-lowing
scores for calcification (see Fig. 2 for exam-
ples): 1 = judged absent, but mild calcification was
considered and rejected; 2 = judged mild, but ab-
sence of calcification was considered and rejected;
3 = judged unequivocally mild; 4 = judged mild, but
moderate calcification was considered and rejected;
5 = judged moderate, but mild calcification was con-
sidered and rejected; 6 = judged unequivocally mod-
erate; 7 = judged moderate, but severe calcification
was considered and rejected; 8 = judged severe, but
moderate calcification was considered and rejected;
and 9 = judged unequivocally severe. An average of
the subjective scores by the two radiologists for over-
all calcification of the aortic valve and for each re-gion of
the aortic valve was used for statistical anal-
ysis. An average of the objective scores (Agatston
and volumetric) of the two radiologists for the quan-
tity of aortic valve calcification was also used for sta-
tistical analysis.
Transthoracic echocardiography reports were
obtained from the echocardiography database.
Echocardiography was performed by experienced
technicians using Agilent Sonos 4500 or 5500 ma-
chines. The echocardiographic scans were each in-
terpreted by various experienced cardiologists sub-
specializing in echocardiography, none of whom
was aware at the time of the reporting of the inclu-
sion of the subject in this study.
The peak instantaneous transvalvular aortic jet
velocity was determined using the modified Ber-
noulli equation. The valve was examined from mul-
tiple acoustic windows to obtain the highest peak
jet velocity. Mean Doppler velocities were calcu-
lated by averaging the instantaneous Doppler gra-
dients throughout the ejection period using an on-line
quantification package. Three cardiac beats
were averaged and the spectral display velocity
curve was traced by hand. There were no cases of
additional subaortic or supraaortic stenosis. No aor-
tic valve gradients were unobtainable for technical
reasons (e.g., poor acoustic windows).
A retrospective chart review was conducted for
the 30 study and the 30 control subjects, document-
ing clinical variables that have been shown to be as-
sociated with aortic stenosis: history of cigarette
smoking [1, 1214], diabetes mellitus [13, 14], sys-
temic hypertension [1, 13] and coronary artery dis-
ease [15]. The presence of coronary artery disease
was based on the mention in the patients record ofcoronary
artery disease, angina with positive
stress test, or myocardial infarction, but not
chest pain. Serum chemical tests that have been
associated with aortic stenosis were evaluated: se-
rum calcium [13,14], low-density and high-density
lipoprotein [13, 14], triglyceride [14], and creati-
nine [13, 16] levels were also recorded. Each labo-
ratory value recorded was the single data point clos-
est in time to the patients CT examination.
-
8/11/2019 ajr%2E04%2E1366
3/8
Liu et al.
344 AJR:186, February 2006
The relationships between pressure gradients
and CT aortic valve calcification data and clinical
variables were determined using the Spearmans
rank correlation. Differences in the presence and
distribution of aortic valve calcification between
patients and control subjects were tested using the
nonparametric rank-sum test. Differences in the
distribution of clinical factors between study and
control subjects were tested using the two-sided
Fishers exact test. Apvalue of less than 0.05 was
considered significant for analyses. This study was
approved by our institutional review board.
Results
Findings for study subjects and control
subjects are presented in Tables 1 and 2. The
average peak and mean gradients in the study
population were 42 31 [SD] mm Hg and
25 20 mm Hg, respectively; median scores
A B
C D
Fig. 2Aortic valve calcifications on CT (section thickness, 5
mm) in four elderly patients.A,Example of severe calcification
(subjective grade, 8.5 on 9-point scale; peak gradient, 75 mm Hg;
mean gradient, 49 mm Hg), both centrally and peripherally in
valve,involving rightleft commissure (arrow) and left-posterior
commissure (arrowhead). Patient is an 88-year-old woman.B,Example
of moderate calcification (subjective grade, 6.5 on 9-point scale;
peak gradient, 25 mm Hg; mean gradient, 19 mm Hg) involving center
of valve and left-posteriorcommissure. Patient is an 86-year-old
man.C,Example of moderate calcification (subjective grade, 5 on
9-point scale; peak gradient, 17 mm Hg; mean gradient, 10 mm Hg)
involving mainly left-posterior commissureand rightleft commissure.
Patient is an 84-year-old man.D,Example of mild calcification
(subjective grade, 3 on 9-point scale; peak gradient, 18 mm Hg;
mean gradient, 10 mm Hg) involving mainly right-posterior and
rightleft
commissures centrally. Patient is a 74-year-old woman.
-
8/11/2019 ajr%2E04%2E1366
4/8
CT of Aortic Valve Calcification
AJR:186, February 2006 345
were 30 and 17 mm Hg, respectively
(Table 1). Severity scores for aortic valve cal-cification
(9-point scale) between the two ra-
diologists agreed within 1 point for 71.9% of
the assessments and within 2 points for 84.4%
of the assessments.
Agatston scores and volumetric scores for
severity of aortic valve calcification both dif-
fered significantly between study and control
subjects (p < 0.0001) (Table 3). The number
of 5-mm-thick sections showing aortic valve
calcification differed significantly between
study and control subjects (p = 0.0004)(Table 3). In addition,
study and control sub-
jects differed significantly in the overall sub-
jective calcification grade (p < 0.0001), in-
cluding at each of the six designated locations
of valve calcification (p < 0.01) (Table 3). Di-
abetes mellitus was documented in 13 (43%)
of the control subjects and in four (13%) of
the study subjects, but information concern-
ing diabetes mellitus was not available for 11
TABLE 1: Aortic Valve Calcifications at CT: Increased
EchocardiographicGradients for 30 Study Patients
PatientNo. Sex Age (yr)
Calcification ScoreEchocardiographicGradients (mm Hg)
Subjectivea Agatston Volumetr ic
No. of 5-mmSectionsInvolved Peak Mean
1 F 61 4.5 1,092 1,026 4 38 17
2 M 64 8.5 4,645 3,856 5 75 49
3 F 65 2 33 39 1 18 10
4 M 66 6 1,345 1,108 4 34 21
5 F 67 2 50 78 3 19 10
6 M 68 7 2,867 2,294 4 24 21
7 F 70 7 695 611 4 71 49
8 F 71 3 150 266 2 45 23
9 F 74 3 192 190 2 18 10
10 F 76 2.5 222 249 2 24 15
11 F 77 6.5 607 609 3 40 22
12 F 78 4.5 669 617 3 30 2013 F 78 3 15 31 2 15 9
14 M 79 4.5 533 447 3 80 52
15 F 81 3 121 199 3 32 17
16 F 81 3 50 76 2 18 10
17 M 82 3 113 99 2 19 10
18 M 82 3.5 172 313 3 44 23
19 M 84 5 459 422 2 17 10
20 F 84 5 390 386 3 18 9
21 F 84 8.5 2,744 2,152 4 125 75
22 F 85 8.5 2,672 2,066 4 61 34
23 M 86 6.5 1,219 982 4 25 15
24 F 87 5.5 90 94 2 30 1525 F 88 8 6,286 4,868 7 85 55
26 M 88 3 348 374 3 28 15
27 M 89 7 1,454 1,112 3 50 35
28 F 89 8.5 4,727 3,624 4 128 86
29 M 91 4.5 97 158 3 21 11
30 F 92 4 115 106 2 20 11
Median 81 4.5 424.5 404 3 30 17
aOn a scale ranging from 1, absent, to 9, severe.
(37%) of the 30 control subjects or for three
(10%) of the 30 study subjects (Table 4).
The Agatston and volumetric calcium
scores were each found in the 30 study sub-
jects to correlate positively with mean
(r= 0.76 and 0.78, respectively;p < 0.0001)
and peak (r= 0.70 and 0.73, respectively;p < 0.0001)
gradients at echocardiography
(Table 3). The number of 5-mm-thick sec-
tions showing calcification also correlated
positively with mean and peak gradients
(r= 0.56 and 0.53, respectively; p < 0.003)
(Table 3). The subjective calcification grade
in five of the six designated commissural re-
gions of the aortic valve correlated positively
with peak and mean gradients (r= 0.480.71
and r= 0.470.66, respectively; p < 0.01),
except for the peripheral right-posterior com-
missure, which showed no significant corre-
lation (Table 3). The highest CTechocardio-
graphic correlations were found forperipheral left-posterior
commissural calcifi-
cation (mean, r= 0.71; peak, r= 0.65; each
p < 0.0001) and central rightleft commis-
sural calcification (mean, r= 0.69; peak,
r= 0.66; eachp < 0.0001) (Table 3). None of
the serum chemical or clinical variables cor-
related significantly with mean or peak gradi-
ents (Table 4).
Discussion
These results indicate that the severity of
aortic valve calcifications, as assessed subjec-
tively on routine chest CT of subjects 60 years
old or older, correlated with increased meanand peak pressure
gradients across the aortic
valve and was significantly greater in patients
with an increased gradient across the valve
than in patients with a normal gradient across
the valve. Furthermore, the location of aortic
valve calcifications proved to be of interest:
increased mean and peak pressure gradients
correlated most strongly with the severity of
commissural calcifications in the central half
of the rightleft commissure and in the pe-
ripheral half of the left-posterior commissure.
The incidental finding of aortic valve calcifi-
cations on routine chest CT examinations has
been described previously, yet few studies haveexamined its
clinical relevance. In an early ret-
rospective study of 100 patients (40 years or
older) who underwent chest CT examination
(1.0-cm collimation), Woodring and West [17]
identified five patients with aortic valve calcifi-
cation, three of whom had echocardiograms
showing a significantly increased gradient
across the aortic valve. Lippert et al. [18], in a
retrospective study of 109 patients (mean age,
-
8/11/2019 ajr%2E04%2E1366
5/8
Liu et al.
346 AJR:186, February 2006
TABLE 2: Aortic Valve Calcifications at CT for 30 Control
Subjects with NormalAortic Valve Echocardiographic Gradients
Patient No. Sex Age (yr)
Calcification Score No. of 5-mmSectionsInvolvedOverall
Subjectivea Agatston Volumetric
1 M 63 1.5 0 0 1
2 M 65 4.5 71 129 33 F 65 2 13 32 2
4 F 67 2.5 77 77 1
5 M 66 2.5 21 43 2
6 M 68 2.5 76 84 1
7 F 71 2 146 174 3
8 F 72 1.5 0 0 0
9 F 72 2 136 119 1
10 M 73 1.5 0 0 0
11 F 74 3.5 87 110 2
12 F 77 3 37 56 1
13 F 79 1 26 39 1
14 M 80 1.5 18 55 1
15 F 80 3 62 88 3
16 F 80 1 0 0 3
17 F 80 2 27 47 3
18 F 81 3 42 69 1
19 F 82 2.5 5 16 2
20 F 82 1 14 25 2
21 M 82 3 259 288 3
22 M 82 2.5 189 181 2
23 M 83 1 4 12 1
24 F 84 9 2,487 1,955 5
25 F 85 2 16 48 3
26 M 86 2 0 0 0
27 F 89 1 78 98 4
28 M 87 6 964 779 4
29 M 88 1 2 6 1
30 M 91 3 530 462 4
Median 80 2 32 55.5 2
aOn a scale ranging from 1, absent, to 9, severe.
60 years) who underwent both chest CT (0.5- to
1.0-cm collimation) and echocardiography
over a 2-year period, found aortic valve calcifi-cation in 30%
of their patients, and five patients
showed a hemodynamically significantly in-
creased gradient, defined as a peak gradient of
25 mm Hg or greater. They concluded that aor-
tic valve calcification detected on CT is a com-
mon finding that is usually clinically insignifi-
cant; however, they noted that calcification was
seen in all cases of a hemodynamically signifi-
cantly increased gradient across the valve.
Our study confirms the results of four re-
cent studies that the echocardiographic as-
sessment of the severity of aortic stenosis cor-relates well
with CT Agatston- and
volumetric-based scoring of aortic valve cal-
cification [69]. Two of these studies used an
MDCT scanner (2.7-mm collimation [6] and
2.5-mm collimation [7], the latter study ECG-
gated) and two of the studies used ECG-gated
electron beam tomography (EBT) (3-mm col-
limation) [8, 9]. The validity of EBT in quan-
tifying aortic valve calcification has been
confirmed in a recent histomorphometric an-
alysis [19]. However, our study did not use
ECG gating or an EBT scanner. Rather, it ex-
tends the original results of the four earlier
studies [69] to the arena of clinical radiology
practice using subjective assessment of aortic
valve calcification.Furthermore, MDCT has recently been
shown to be comparable to EBT for assessing
aortic valve calcification, although low levels
of aortic valve calcification tended to show
higher levels of interscan variability than
moderate to high levels, despite ECG gating
[7]. Multidetector, ECG-gated CT has also re-
cently been shown to have good agreement of
the assessment of aortic valve calcification
with the quantity of calcium in the aortic
valve in surgical specimens [20]. The results
of our study suggest that ECG gating may not
be necessary for clinically useful assessment
on CT of aortic valve calcification [6].The predictive value of
commissural pat-
terns of aortic valve calcification has not, to
our knowledge, been evaluated previously. In
an autopsy study of elderly patients with se-
vere aortic stenosis, nodular calcific deposits
were found on the aortic aspects of the valve
cusps adjacent to commissures, which were
mostly unfused [21]. Two major patterns of
aortic valve calcification have been described
previously in pathology specimens: first, a
coaptation pattern in which calcifications oc-
cur as two spokes, parallel and immediately
adjacent to each other on each side of the line
of cusp coaptation [22]; and second, a radialpattern in which
calcifications occur as mul-
tiple spokes radiating from the cusp attach-
ment toward the center of the cusp [22]. To
our knowledge, the observation that the cen-
tral rightleft commissure and the peripheral
left-posterior commissure are the sites of the
strongest correlations between the severity of
aortic valve calcifications and transvalvular
gradients has not previously been reported.
Two mechanisms appear likely to explain
these associations. One is that these two
specific regions may represent the sites of
greatest mechanical stress for the stenotic
aortic valve [22], probably in associationwith decreased
compliance of the sinuses of
Valsalva [23]. Another possibility is that the
left aortic cusp, which forms the posterior
aspect of the rightleft commissure and the
left aspect of the left-posterior commissure,
tends to be the largest of the three cusps [24]
and perhaps is thus the cusp most associated
with the stresses that lead to calcific depos-
its. However, Cujec and Pollick [25] have
-
8/11/2019 ajr%2E04%2E1366
6/8
CT of Aortic Valve Calcification
AJR:186, February 2006 347
reported that the cusp most likely to be in-
volved in isolated aortic valve thickening is
most commonly the noncoronary cusp, fol-
lowed by the right and then the left. A defi-
nite mechanism for preferential correlation
of calcification of the central rightleft
commissure and of the peripheral left-pos-
terior commissure and increased pressure
gradients across the aortic valve remains to
be elucidated. A limitation of the present
study is that the aortic valve is slightly ob-
lique to the axial projection of CT, so the
three commissures do project slightly ob-
liquely with respect to the plane of a section
through the valve.
TABLE 3: Indices of Aortic Valve Calcifications at CT and
Correlations with Echocardiographic Gradients
Index Study Subjects Control Subjects paMean Gradient
Correlation pbPeak Gradient
Correlation pc
Agatston score 1,139 1,622 180 477 < 0.0001 0.76 < 0.0001
0.70 < 0.0001
Volumetric score 948 1,253 166 374 < 0.0001 0.78 < 0.0001
0.73 < 0.0001
Number of sections showing calcification 3.1 1.1 2.0 1.2 0.0004
0.56 0.0012 0.53 0.0027
Subjective scored
Overall grade 5.0 2.1 2.5 1.7 < 0.0001 0.69 < 0.0001 0.65
< 0.0001
Ac (central right-posterior commissure) 2.4 0.7 1.2 1.7 0.0012
0.52 0.0033 0.47 0.0090
Ap (peripheral right-posterior commissure) 1.4 1.5 0.4 1.1
0.0019 0.08 0.68 0.12 0.52
Bc (central rightleft commissure) 3.2 2.5 0.9 1.9 < 0.0001
0.69 < 0.0001 0.66 < 0.0001
Bp (peripheral rightleft commissure) 3.2 2.5 1.5 2.9 < 0.0001
0.48 0.0072 0.51 0.0037
Cc (central left-posterior commissure) 3.7 2.9 1.5 1.9 0.0056
0.55 0.0017 0.49 0.0062
Cp (peripheral left-posterior commissure) 3.8 2.7 1.5 2.0 0.0005
0.71 < 0.0001 0.65 < 0.0001
Central commissure 4.8 2.4 2.4 1.9 < 0.0001 0.76 < 0.0001
0.71 < 0.0001
Peripheral commissure 4.7 2.2 2.0 1.9 < 0.0001 0.76 <
0.0001 0.72 < 0.0001
A (right-posterior commissure) 3.2 2.5 1.4 1.8 0.0004 0.44 0.016
0.41 0.023
B (rightleft commissure) 3.9 2.4 1.1 1.9 < 0.0001 0.69 <
0.0001 0.65 0.0001
C (left-posterior commissure) 4.4 2.7 2.0 1.9 0.0004 0.63 0.0002
0.58 0.0008
NoteResults for study subjects and control subjects are
expressed as mean SD. Values for pwere derived using chi-square
test.aFor study subjects vs control subjects.bFor correlation among
study subjects.cFor correlation among study subjects.dOn a scale
ranging from 1, absent, to 9, severe.
TABLE 4: Clinical Data and Correlations with Echocardiographic
Gradients
Clinical Data Study Subjects Control Subjects paMean
Gradient
Correlation pbPeak Gradient
Correlation pc
Serum data
Low-density lipoprotein (mg/dL) 97 44 106 37 0.57 0.03 0.89 0.06
0.81
High-density lipoprotein (mg/dL) 45 19 44 13 0.92 0.21 0.37 0.26
0.26
Triglyceride (mg/dL) 121 52 128 78 0.91 0.06 0.80 0.08 0.72
Corrected calcium (mg/dL) 8.9 0.5 8.8 0.6 0.76 0.01 0.98 0.04
0.85
Creatinine (U/L) 1.4 1.0 1.2 0.9 0.43 0.17 0.39 0.17 0.38
Erythrocyte sedimentation rate (mm/hr) 42 22 38 36 0.32 0.23
0.36 0.18 0.48
Additional clinical data
Coronary artery disease 13 / 29 9 / 19 1
Hypertension 21 / 29 12 / 19 0.54
Cigarette smoking 15 / 27 14 / 19 0.24
Diabetes mellitus 13 / 27 4 / 19 0.07
NoteResults for serum chemical data are expressed as mean SD.
Results for additional clinical data are expressed as numbers of
patients with positive findings dividedby numbers of patients for
whom relevant data were available. Values for pwere derived from
two-sided Fischers exact test.
aFor study subjects vs control subjects.bFor correlation among
study subjects.cFor correlation among study subjects.
-
8/11/2019 ajr%2E04%2E1366
7/8
Liu et al.
348 AJR:186, February 2006
Although the severity of aortic valve calci-
fication did correlate in our study with gradi-
ents across the aortic valve, the association
was an imperfect predictor: as false-nega-
tives, two (6.7%) of 30 subjects with an in-
creased gradient had subjective calcification
scores of 2 or less on our 9-point subjectivescale, and four
(13.3%) of these 30 subjects
had an Agatston score of 50 or less (Table 1).
As false-positives, two (6.7%) of the 30 con-
trol subjects had a subjective severity score of
6 or more on the 9-point scale, and four
(13.3%) of these 30 control subjects had an
Agatston score of 200 or more (Table 2). Nev-
ertheless, these percentages are sufficiently
low to support strongly the clinical precept
that more than minimal aortic valve calcifica-
tion of an elderly person on CT is an indica-
tion for echocardiographic evaluation.
The quantity of aortic valve calcification at
the time of diagnosis of aortic stenosis ap-pears to be of
prognostic import: the greater
the quantity of calcification, the more rapid
will be the loss of valve area [4, 16, 26, 27].
Moreover, the smaller the valve area, the
greater the rate of progression of aortic steno-
sis, according to two studies [4, 26], although
not according to a third study [28]. The rate of
progression is variable [4, 26, 28], but the
mean rate of progression of calcific aortic
stenosis has been described as in the range of
a loss of valve area of approximately 0.1 cm2
per year [4, 26, 28] and as a mean increase of
mean gradient of 67 mm Hg per year [4, 28],
at least as long as cardiac failure does not su-pervene [4, 29].
None of the patients in our se-
ries was in a state of cardiac failure. Five-year
event-free survival after the diagnosis of an
increased aortic valve gradient in asympto-
matic subjects, defining an event as either
death or aortic valve replacement, has been
reported as only 26% 10% [4]. In another
series of 128 consecutive asymptomatic per-
sons with severe aortic stenosis, 4-year event-
free survival was only 20% 5% [27].
Serum chemical values showed no signifi-
cant differences between study and control
subjects in our study (Table 4). Although
prior studies have implicated elevated serumcholesterol [1, 12,
13], creatinine [1, 30, 16],
and calcium [30] levels as risk factors for pro-
gression of aortic stenosis, our results, based
on a single serum test, support no such asso-
ciations. The progression of aortic stenosis
does appear to be multifaceted, including cur-
rent cigarette smoking as a major risk factor
for rapid progression [1, 27], and having an
association with coronary artery atheroscle-
rotic disease that may respond to serum lipid-
lowering therapy [12]. We did not assess ther-
apeutic interventions in this study.
Advanced age is not necessarily a contrain-
dication to aortic valve replacement for aortic
stenosis. Long-term postoperative survival
and quality of life were termed excellent in arecent series of
105 subjects 7589 years old
(mean, 79 years) [7]. Detecting aortic valve
stenosis in this age group, in candidates ap-
propriate for aortic valve replacement, may
be clinically beneficial.
A limitation of our study is that the aortic
valve was assessed on echocardiography only
by Doppler gradients and not by assessment
of the continuity equation [31]. Had the con-
tinuity equation been used, it would have al-
lowed the aortic valve area to be determined
and would thereby have lessened the possibil-
ities of either overcalculation or undercalcu-
lation of aortic valve stenosis because of co-existing aortic
regurgitation or poor function
of the left ventricle, respectively [31]. During
the time of our study, our echocardiography
laboratory did not routinely use the continuity
equation, which involves time-consuming
measurement of the outflow tract diameter of
the left ventricle.
EBT scans have been shown to yield excel-
lent reliability for Agatston and volumetric
assessment of aortic valve calcification in a
context of ECG gating [32]. Shavelle et al. [8]
have suggested that aortic valve calcification
at EBT showing Agatston scores in excess of
a certain level (e.g., 150) warrant echocardio-graphic
assessment [8].
Two other limitations of this study are that
it excluded subjects with a bicuspid aortic
valve [33] and also excluded subjects younger
than 60 years. Aortic valve calcification is
well recognized as occasionally occurring in
subjects younger than 60 years, especially in
those with a bicuspid aortic valve or in those
who had rheumatic fever in childhood. How-
ever, we chose to limit our study to subjects
with a tricuspid aortic valve and 60 years old
or older because this population is at major
risk for the underdiagnosis of senile degener-
ation of the aortic valve before clinically sig-nificant
stenosis of the valve develops [2].
Another limitation of our study is that it was
retrospective and used a rather small sample
(30 subjects with aortic valve stenosis). We
suggest that a prospective study of a larger se-
ries, including subjects younger than 60 years,
would be advisable for further understanding
the clinical importance of CT detection of un-
anticipated aortic valve calcification.
Both a limitation and a strength of our study
is that the CT examinations did not use the
most sensitive of modern CT technologic ap-
proaches (we used mostly single-detector ex-
aminations, slice thickness was 0.5 cm, scan-
ning time was 0.75 sec, and ECG gating was
not used). In assessing coronary artery calcifi-cations on CT,
sections thinner than 0.5 cm and
scanning times shorter than 0.75 sec, in a con-
text of ECG gating, produce more accurate cal-
cium scoring than the techniques of our study
[10, 34]; presumably, the same observation
also holds for the calcified aortic valve [35].
However, aortic valve calcification at MDCT
has been shown, using 2.7-mm collimation and
no ECG gating, to correlate closely with the se-
verity of aortic stenosis [6]. Correspondingly,
the strength of our study is that, because no
ECG gating was used, our positive results offer
a clinically practical guideline: if the subjective
rating of aortic valve calcifications is greaterthan mild,
especially for the central rightleft
commissure and the peripheral left-posterior
commissure, then echocardiographic evalua-
tion may be indicated.
References
1. Stewart BF, Siscovick D, Lind BK, et al. Clinical
factors associated with calcific aortic valve disease.
J Am Coll Cardiol1997; 29:630634
2. Dare AJ, Veinot JP, Edwards WD, Tazelaar HD,
Schaff HV. New observations on the etiology of
aortic valve disease: a surgical pathologic study
of 236 cases from 1990. Hum Pathol 1993;24:13301338
3. Carabello BA. Aortic stenosis.N Engl J Med2002;
346:677682
4. Otto CM, Burwash IG, Legget ME, et al. Prospec-
tive study of asymptomatic valvular aortic stenosis:
clinical, echocardiographic, and exercise predictors
of outcome. Circulation1997; 95:22622270
5. Szamosi A, Wassberg B. Radiologic detection of
aortic stenosis. Acta Radiol Diagn Stockh 1983;
24:201207
6. Cowell SJ, Newby DE, Burton J, et al. Aortic valve
calcification on computed tomography predicts the
severity of aortic stenosis. Clin Radiol 2003;
58:7127167. Morgan-Hughes GJ, Owens PE, Roobottom CA,
Marshall AJ. Three dimensional volume quantifi-
cation of aortic valve calcification using multislice
computed tomography.Heart2003; 89:11911194
8. Shavelle DM, Budoff MJ, Buljubasic N, et al. Use-
fulness of aortic valve calcium scores by electron
beam computed tomography as a marker for aortic
stenosis.Am J Cardiol2003; 92:349353
9. Kaden JJ, Freyer S, Weisser G, et al. Correlation of
-
8/11/2019 ajr%2E04%2E1366
8/8
CT of Aortic Valve Calcification
AJR:186, February 2006 349
degree of aortic valve stenosis by Doppler echocar-
diogram to quantity of calcium in the valve by elec-
tron beam tomography. Am J Cardiol 2002;
90:554557
10. Agatston AS, Janowitz WR, Hildner FJ, Zusmer
NR, Viamonte M Jr, Detrano R. Quantification of
coronary artery calcium using ultrafast computedtomography.J Am
Coll Cardiol1990; 15:827832
11. Callister TQ, Cooil B, Raya SP, Lippolis NJ, Russo
DJ, Raggi P. Coronary artery disease: improved re-
producibility of calcium scoring with an electron-
beam CT volumetric method. Radiology 1998;
208:807814
12. Mohler ER, Sheridan MJ, Nichols R, Harvey WP,
Waller BF. Development and progression of aortic
valve stenosis: atherosclerotic risk factorsa
causal relationship? A clinical morphologic study.
Clin Cardiol1991; 14:995999
13. Mohler ER III. Are atherosclerotic processes in-
volved in aortic valve calcification? Lancet2000;
356:52452514. Faggiano P, Aurigemma GP, Rusconi C, Gaasch
WH. Progression of valvular aortic stenosis in
adults: literature review and clinical implications.
Am Heart J1996; 132:408417
15. Peter M, Hoffmann A, Parker C, Luscher T, Burck-
hardt D. Progression of aortic stenosis: role of age
and concomitant coronary artery disease. Chest
1993; 103:17151719
16. Bahler RC, Desser DR, Finkelhor RS, Brener SJ,
Youssefi M. Factors leading to progression of valvu-
lar aortic stenosis.Am J Cardiol1999; 84:10441048
17. Woodring JH, West JW. CT of aortic and mitral
valve calcification.J Ky Med Soc1989; 8:177180
18. Lippert JA, White CS, Mason AC, Plotnick GD.
Calcification of aortic valve detected incidentally
on CT scans: prevalence and clinical significance.
AJR1995; 164:7377
19. Pohle K, Dimmler A, Feyerer R, et al. Quantifica-
tion of aortic valve calcification with electron beam
tomography: a histomorphometric validation study.
Invest Radiol2004; 4:23023420. Willmann JK, Weishaupt D, Lachat
M, et al. Elec-
trocardiographically gated multi-detector row CT
for assessment of valvular morphology and calcifi-
cation in aortic stenosis. Radiology 2002;
225:120128
21. Roberts WC, Perloff JK, Constantino T. Severe val-
vular aortic stenosis in patients over 65 years of age:
a clinicopathologic study. Am J Cardiol 1971;
27:497506
22. Thubrikar MJ, Aouad J, Nolan SP. Patterns of cal-
cific deposits in operatively excised stenotic or
purely regurgitant aortic valves and their relation to
mechanical stress.Am J Cardiol1986; 58:304308
23. Robicsek F, Thubrikar MJ, Fokin AA. Cause of de-generative
disease of the trileaflet aortic valve: re-
view of subject and presentation of a new theory.
Ann Thorac Surg2002; 73:13461354
24. Vollebergh FE, Becker AE. Minor congenital vari-
ations of cusp size in tricuspid aortic valves: possi-
ble link with isolated aortic stenosis. Br Heart J
1977; 39:10061011
25. Cujec B, Pollick C. Isolated thickening of one aortic
cusp: preferential thickening of the noncoronary
cusp.J Am Soc Echocardiogr 1988; 1:430432
26. Piper C, Bergemann R, Schulte HD, Koerfer R,
Horstkotte D. Can progression of valvar aortic
stenosis be predicted accurately?Ann Thorac Surg
2003; 76:676680
27. Rosenhek R, Binder T, Porenta G, et al. Predictors
of outcome in severe, asymptomatic aortic stenosis.
N Engl J Med2000; 343:611617
28. Brener SJ, Duffy CI, Thomas JD, Stewart WJ. Pro-
gression of aortic stenosis in 394 patients: relation
to changes in myocardial and mitral valve dysfunc-
tion.J Am Coll Cardiol1995; 25:30531029. Zile MR, Gaasch WH.
Heart failure in aortic steno-
sis: improving diagnosis and treatment. N Engl J
Med2003; 348:17351736
30. Palta S, Pai AM, Gill KS, Rai RG. New insights
into the progression of aortic stenosis: implica-
tions for secondary prevention. Circulation2000;
101:24972502
31. Otto C. Textbook of echocardiography. Philadel-
phia. PA: Saunders, 2000:237239
32. Budoff MJ, Mao S, Takasu J, Shavelle DM, Zhao X-
Q, OBrien KD. Reproducibility of electron-beam
measures of aortic valve calcification.Acad Radiol
2002; 9:11221127
33. Beppu S, Suzuki S, Matsuda H, et al. Rapidity ofprogression
of aortic stenosis in patient with con-
genital bicuspid aortic valves.Am J Cardiol1993;
71:322327
34. Hong C, Pilgram TK, Zhu F, Joe BN, Towler DA,
Bae KT. Improving mass measurement of coronary
artery calcification using threshold correction and
thin collimation in multi-detector row computed to-
mography: in vitro experiment.Acad Radiol2003;
10:969977
35. Kizer JR, Gefter WB, deLemos AS, Scoll BJ,
Wolfe ML, Mohler ER III. Electron beam com-
puted tomography for the quantification of aortic
valvular calcification. J Heart Valve Dis 2001;
10:361366














![AJR Assignment 1 Universal Design [1]](https://img.pdfslide.net/doc/110x75/577daabc1a28ab223f8b4ae5/ajr-assignment-1-universal-design-1.jpg)