-
AKILCI ANTİBİYOTİK KULLANIMINDA HIZLI TANI YÖNTEMLERİNİN
YERİ
Dr. Vildan AVKAN-OĞUZ
Dokuz Eylül Üniversitesi Tıp Fakültesi
İnfeksiyon Hastalıkları ve Klinik Mikrobiyoloji AD.
KLİMİK Mart 2015 /ANTALYA
-
Sunum Planı
• Akılcı antibiyotik kullanımı ?
• Hangi yöntemler hızlı tanı yöntemleri ?
• Hızlı tanı yöntemlerinin artıları / eksileri ?
• Pratikte antibiyotik tedavisi ? • Gelecekte ?
-
Akılcı antibiyotik kullanımı
• 1940 – İlk antibiyotiklerin kullanıma girmesi
• 1956- Jawetz - antibiyotik kullanım problemleri
-
Akılcı antibiyotik kullanımı
• 1970 -Antibiyotiklerin uygun kullanımının arttırılması
• 1996 -‘Stewardship’
• 2007 –‘IDSA+SHEA’ Antimicrobial Stewardship Programs
(ASPs)
-
http://www.akilciilac.gov.tr/?page_id=1068&lang=tr_TR
-
Akılcı antibiyotik kullanımı
• İnfeksiyon / Kolonizasyon ? (Antibiyotik gerekli mi ?)
• Hangi sistem infeksiyonu ? Kaynak ? • Konak özellikleri ?
• Mikroorganizma/mikroorganizmalar nelerdir ? Direnç özellikleri
?.... • Lokal veriler ?
-
İnsan mikrobiyomu
Konak özellikleri ?
-
Akılcı antibiyotik kullanımı
• İnfeksiyon / Kolonizasyon ? (Antibiyotik gerekli mi ?)
• Hangi sistem infeksiyonu ? Kaynak ? • Konak özellikleri ?
• Mikroorganizma/mikroorganizmalar nelerdir ? Direnç özellikleri
?.... • Lokal veriler ?
HIZLI TESTLER ?
-
Hızlı tanı yöntemleri • Biyokimyasal/Serolojik testler;
Metabolik ürünler, antijen-antikor reaksiyonları
• Point –of-care tests; Yatak başı testler
• Moleküler temelli yöntemler
PCR; Real-time PCR, multipleks PCR vs.
Sekans analizi
• MALDI‐TOF MS (Matriks ile desteklenmiş lazer desorpsiyon /
iyonizasyon uçuş zamanı kütle spektrometresi)
• PNA-FISH ( Peptid nükleik asit floresan in situ
hibridizasyon)
-
Hızlı tanı testleri
Çiftdoğan DY, Vardar F. Çocuk Sağlığı ve Hastalıkları Dergisi
2009; 52: 159-166
-
Fournier PE, et al. Nat Rev Microbiol 2013; 11(8):574-85
-
Hızlı tanı yöntemleri • Biyokimyasal/Serolojik testler;
Metabolik ürünler, antijen-antikor reaksiyonları
• Point –of-care tests; Yatak başı testler
• Moleküler temelli yöntemler
PCR; Real-time PCR, multipleks PCR vs.
Sekans analizi
• MALDI‐TOF MS (Matriks ile desteklenmiş lazer desorpsiyon /
iyonizasyon uçuş zamanı kütle spektrometresi)
• PNA-FISH ( Peptid nükleik asit floresan in situ
hibridizasyon)
-
Hızlı tanı testleri
Caliendo AM, et al. Clin Infect Dis 2013; 57(S3):139-70
-
Hızlı tanı testleri
Moleküler yöntemler • Sistem /Sendrom temelli kitler;
Santral sinir sistemi, Kan dolaşımı sistemi Solunum sistemi,
Genitoüriner sistem, vs • Mikroorganizma temelli kitler;
MRSA/MSSA/CoNS, P.aeruginosa, K. pneumoniae C. difficile vs.
Blaschke AJ, et al. Diagn Microbiol Infect Dis 2015;81
(1):57-59
Burilla A, Bouza E. BMC Infect Dis 2014; 14:593 Fournier PE, et
al. Nat Rev Microbiol 2013; 11(8):574-85
Tenover FC. Ann NY Acad Sci 2010; 70-80
-
Hızlı tanı testleri
Tenover FC. Ann NY Acad Sci 2010; 70-80
-
Goff DA, et al. Pharmacotherapy 2012; 32(8): 677-687
-
Hızlı tanı testleri
Direkt hasta örneği kan, balgam, BAL, BOS, vs
PCR, Gene Xpert
Kültür pozitif materyalden
MALDI-TOF PNA-FISH
PCR
Sekans analizi Bakteri tanımlanması
Direnç genlerinin saptanması Bakteri tanımı+direnç
-
O. Liesenfeld et al.
European Journal of Microbiology and Immunology 4 (2014) 1
14
driven by the amplifi cation using PCR and the indepen-
dence from inhibitory infl uences of antibiotics or other
factors present in the blood. On the contrary, laboratory
contamination, background bacterial DNA in blood, and
the potential detection of bacterial DNA from dead and
living organisms are some of the main limitations of these
methods [89]. Of importance, the turnaround time of the
molecular technology alone does not allow to preclude its
value; rapid molecular technologies have to be embedded
into well-defi ned clinical algorithms that allow transport
of the sample to the laboratory, pre-analytics, performance
of the test, and result transmission to the clinician around
the clock. In this regard, most studies using molecular
technologies have reported reduced overall turnaround
times compared to traditional blood culture but mean turn-
around times remained disappointing due to the limitations
of test performance after hours and/or over the weekend.
Furthermore, the extent of clinical benefi t (initiation,
esca-
lation, or de-escalation of antimicrobial therapy) provided
by rapid turnaround time in patients who most likely are
pre-treated with broad-range antibiotics as empiric therapy
has to be determined.
Detection of antimicrobial resistance
Despite signifi cant advances in diagnostic technologies,
many patients with suspected sepsis receive empiric anti-
microbial therapy rather than appropriate therapy dictated
by the rapid identifi cation of the infectious agent. The
result is overuse of a limited number of effective antimi-
crobials. A diagnostic strategy that incorporates sensitive
biomarkers to indicate the presence of infection followed
by pathogen-specifi c tests that are linked to a rapid
assess-
ment of drug resistance could revolutionize sepsis manage-
ment by enabling the initiation or adjustment of defi nitive
antimicrobial therapy. Rapid identifi cation of antibiotic
re-
sistance is also central to infection control policies
includ-
ing the timely isolation of patients harboring
drug-resistant
organisms. A limited number of bacterial resistance genes
can be routinely detected using commercially molecular
assays such as mecA, vanA and vanB [132], in most cases
combined with the detection of Gram-positive pathogens.
PCR tests for the presence of genes that encode resistance
in Gram-negative bacteria including ESBL and carbapen-
emases are also commercially available (e.g., Hyplex sys-
tems, Amplex, Germany; Check-Points, the Netherlands).
A DNA microarray with high coverage of known vari-
ants allows rapid molecular testing for ESBLs following
growth and isolation of single colonies [133]. However, it
remains to be shown whether the molecular detection of
antimicrobial resistance genes can replace phenotypic mi-
crobiological characterization of antimicrobial susceptibil-
ity since the presence of resistance genes does not always
translate in clinically relevant resistance.
Sample transport, lab workflow, and result reporting
Implementation of the new molecular techniques in the
clinical microbiology laboratory is needed especially in
university and emergency hospitals which are able to meet
the daily increasing demand for such specifi c tests. The
laboratory workfl ow incorporate optimized handling pre-
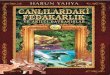
Fig. 2. Time to result of selected blood culture-dependent and
blood culture-independent technologies for the diagnosis of
sepsis;
the vertical line indicates the duration of blood culture (fixed
at 8 h or longer for this figure)Liesenfeld O, et al Eur J
Microbiol Immunol 2014; 4(1):1-25
-
Fournier PE, et al. Nat Rev Microbiol 2013; 11(8):574-85
-
Hızlı tanı testleri
• Laboratuvarda;
İşlem süresinde kısalma Tanımlanan mikroorganizma sayısında
artış Kültürü yapılamayan bakterilerin tanımlanması Zor üreyen
bakterilerin tanımlanması Antibiyotik duyarlılığının erken
saptanması
-
Hızlı tanı testleri
• Klinikte;
Etken spesifik tedavi uygulanmasında artış
Hastanede yatış süresinin kısalması
Antibiyotik kullanım süresinde kısalma
Morbidite ve mortalitede azalma
-
Hızlı tanı testleri
• Kültürde üreme gerekliliği
• Steril olmayan örneklerde ?
• Moleküler testlerin ölü bakteriyi ayıramaması
• Test negatifliğinin infeksiyonu dışlamaması
• Minimal inhibitor konsantrasyon (MIC) ?
-
Hızlı tanı testleri
• Klasik yöntemlerle birlikte değerlendirilmesi gerekliliği
• Yorum farkı olması Antibiyotik tedavisi alan hastalarda ?
Polimikrobiyal infeksiyonlar ? Mutasyon varlığı - direnç ? Direnç
genotip- fenotip uyumu ? • Maliyet analizi ?
-
Baron EJ, et al. Clin Infect Dis 2013;57(4):e22-121
-
Akılcı antibiyotik kullanımı
• İnfeksiyon / Kolonizasyon ? (Antibiyotik gerekli mi ?)
• Hangi sistem infeksiyonu ? Kaynak ? • Konak özellikleri ?
• Mikroorganizma/mikroorganizmalar nelerdir ? Direnç özellikleri
?.... • Diğer laboratuvar testleri - Bölgesel veriler
-
Diğer Laboratuvar Testleri
• WBC, CRP, Prokalsitonin
Bakteriyel-viral infeksiyon ? Duyarlılığı yüksek Özgüllüğü düşük
(prokalsitonin özgüllüğü CRP’den daha yüksek) Tedavi süresince
prokalsitonin düzey izlemi önerisi (+)
-
Wien Klin Wochenschr. 2015 Jan 14. [Epub ahead of print]
Comparison of diagnostic values of procalcitonin, C-reactive
protein and blood neutrophil/lymphocyte ratio levels in predicting
bacterial infection in hospitalized patients with acute
exacerbations of COPD. Tanrıverdi H1, Örnek T, Erboy F, Altınsoy B,
Uygur F, Atalay F, Tor MM. Author information 1Faculty of Medicine,
Chest Diseases Department, Bülent Ecevit University, Esenköy,
Kozlu, 67100, Zonguldak, Turkey, [email protected]. Abstract
BACKGROUND: Viral or bacterial upper respiratory infections are the
most common cause of acute exacerbation of chronic obstructive
pulmonary disease (AECOPD). Based on available data, no reliable
parameter has been presented to distinguish between bacterial and
nonbacterial exacerbations. Therefore, we compared the diagnostic
value of procalcitonin (PCT) level, which is a newer marker for
predicting bacterial infections in patients with AECOPD, to routine
parameters such as C-reactive protein (CRP) levels and the
neutrophil/lymphocyte (N/L) ratio. METHODS: This study included all
consecutive patients who were admitted for a diagnosis of AECOPD
between January 1 and March 31, 2014. PCT, CRP, and the N/L ratio
were assessed in addition to cultures from tracheal aspirates or
sputum on the first day of admission. Patients with a pneumonic
infiltration on chest radiographs, or an extrapulmonary infection
focus, or whose blood samples were not obtained for PCT and/or CRP
at the same time as sputum culture were excluded from the study.
RESULTS: A total of 77 patients were included with a mean age of
71.7 ± 9.5 years. Bacteria were isolated in 37.4 % of the patients.
Mean PCT levels were significantly higher in patients with positive
sputum cultures than in patients with negative sputum cultures. The
cut-off values for PCT, CRP, and the N/L ratio for predicting a
bacterial infection were 0.40 ng/mL, 91.50 mg/L, and 11.5,
respectively; sensitivity was 61, 54, and 61 % respectively;
specificity was 67, 52, and 58 %, respectively; and the area under
the curve (AUC) values were 0.64, 0.52, and 0.58, respectively. The
AUC value of PCT was significantly better for predicting bacterial
infection compared with the CRP level or the N/L ratio (p = 0.042).
CONCLUSION: PCT was better than CRP and the N/L ratio for
predicting a bacterial infection in hospitalized patients with
AECOPD. However, we find PCT not so reliable in predicting
bacterial infection in AECOPD due to sensitivity and specificity of
less than 80 % and a low AUC value.
-
Akılcı antibiyotik kullanımı • İnfeksiyon / Kolonizasyon ?
(Antibiyotik gerekli mi ?)
• Hangi sistem infeksiyonu ? Kaynak ? • Konak özellikleri ?
• Mikroorganizma/mikroorganizmalar nelerdir ? Direnç özellikleri
?.... • Diğer laboratuvar testleri • Bölgesel veriler
-
Bölgesel veriler 1000 yatak 58 YBÜ yatak sayısı
2014 yılı - DEÜ verileri (Prof Dr Z Gülay)
-
Bölgesel veriler
Solunum örnekleri Tür adı %
1 Acinetobacter spp 35,2
2 P. aeruginosa 16,1
3 Candida 12,4
4 K. pneumoniae 10,4
5 S. maltophilia 7,8
İdrar örnekleri Tür adı %
1. Candida 48,1
2. Enterococcus spp 12,4
3. E. coli 10,8
4. P. aeruginosa 9,2
5. K. pneumoniae 8,1
Kan örnekleri
Tür adı %
1. Co NS spp 52,7
2. Acinetobacter spp 10,8
3. K. pneumoniae 10,0
4. P. aeruginosa 5,6
5. S. maltophilia 5,6
Yara örnekleri
Tür adı %
1.K. pneumoniae 15.3
2. Acinetobacter spp 13.5
3. Enterococcus spp 13.5
4. Enterobacter spp 6.8
5. S. aureus 6.8
-
Bölgesel veriler 1000 yatak 58 YBÜ yatak sayısı
2014 yılı - DEÜ verileri (Prof Dr Z Gülay)
Bakteri Sayı % (Tüm
bakteriler) % (Tür)
ESBL Pozitif Enterobacteriaceae 129 10,70 55,8
Escherichia coli 30 58,8
Klebsiella pneumoniae 86 74,9
Enterobacter spp. 7 36,8
Diğer Enterobacteriaceae 6 13,1
Karbapenem Dirençli Enterobacteriaceae 6,14 32,1
Escherichia coli 1,9
Klebsiella pneumoniae 60,0
Enterobacter spp. 15,7
Diğer Enterobacteriaceae 2,1
Karbapenem Dirençli A. baumannii 13,52 97,1
Karbapenem Dirençli P. aeruginosa 4,56 61,1
MRSA 0,33 13,3
VRE 0,74 *11,4/16/3,4
*: Tüm enterokoklar içerisindeki VRE oranı/E.faecium VRE
Oranı/E.faecalis VRE oranı
-
Livermore DM, Wain J. Infect Chemother 2013; 45(1):1-10
-
Fournier PE, et al. Nat Rev Microbiol 2013; 11(8):574-85
-
Fournier PE, et al. Nat Rev Microbiol 2013; 11(8):574-85
Gelecekte
-
Gelecekte
• Steril olmayan hasta örneklerinden moleküler testler ?
• Plasmid ilişkili direnç genleri ?
• Fenotipik ve genotipik uyum ?
-
PLOS ONE | DOI:10.1371/journal.pone.0116746 March 18, 2015
-
Sonuç
• İnfeksiyon / Kolonizasyon ayrımı mutlaka yapılmalı
• Konak ve bakteri özellikleri birlikte değerlendirilmeli •
Kültür hala altın standart
• Hızlı tanı yöntemleri ümit verici
MAKUL yöntem ; Hızlı tanı yöntemleri + klasik yöntemler
-
Sonuç
• Hastanede yatış süresinin kısalma
• Antibiyotik kullanım süresinde kısalma
• Morbidite ve mortalitede azalma