Embed Size (px)
Citation preview
Aktuelle Richtlinien der kardiopulmonalen Reanimation
Daniel KiblböckAbteilung für Innere Medizin II - Kardiologie
• Epidemiologie Cardiac Arrests
• Algorithmus Adult Advanced Life Support
• Ursachen einer kardiopulmonalen Reanimation
• Post-Resuscitation Care
• Prognosebeurteilung nach CPR
Themenübersicht
Ischämische Herzerkrankung
Die ischämische Herzerkrankung ist die häufigste Todesursache weltweit.
Murray CJ et al. Mortality by cause for eight regions in the world: global burden of disease study. Lancet 1997;349:1269-76
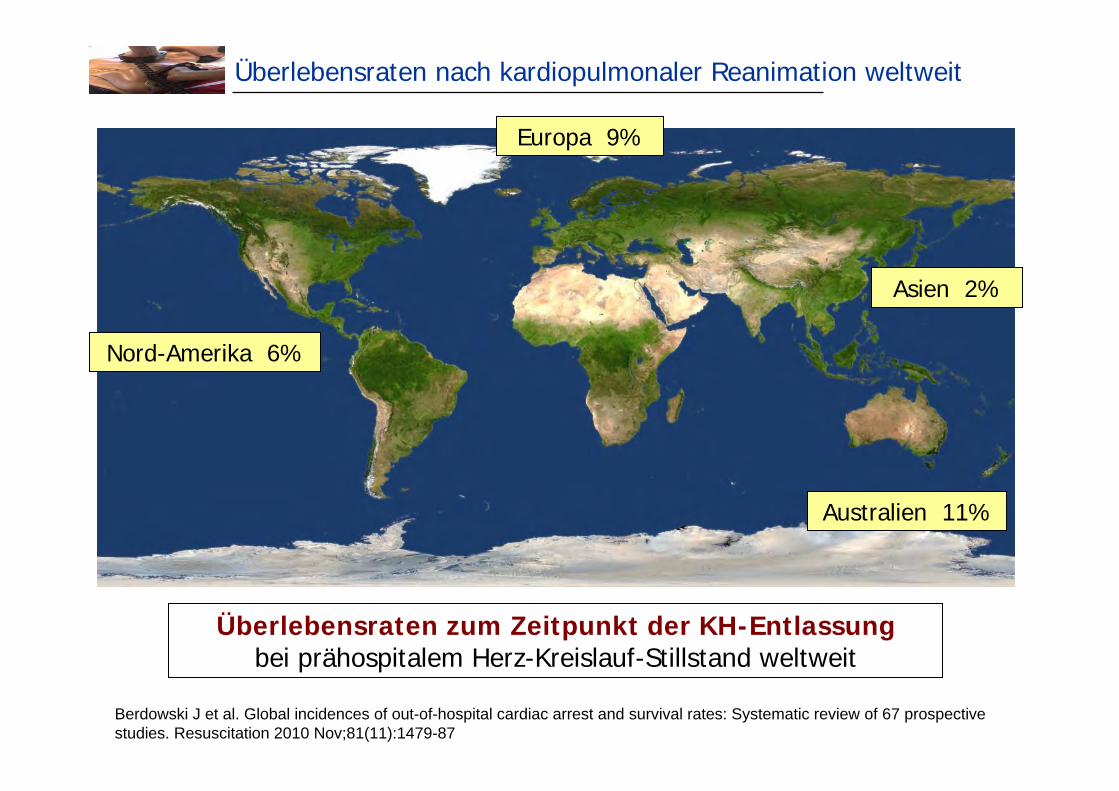
Überlebensraten nach kardiopulmonaler Reanimation weltweit
Berdowski J et al. Global incidences of out-of-hospital cardiac arrest and survival rates: Systematic review of 67 prospectivestudies. Resuscitation 2010 Nov;81(11):1479-87
Überlebensraten zum Zeitpunkt der KH-Entlassungbei prähospitalem Herz-Kreislauf-Stillstand weltweit
Nord-Amerika 6%
Europa 9%
Australien 11%
Asien 2%
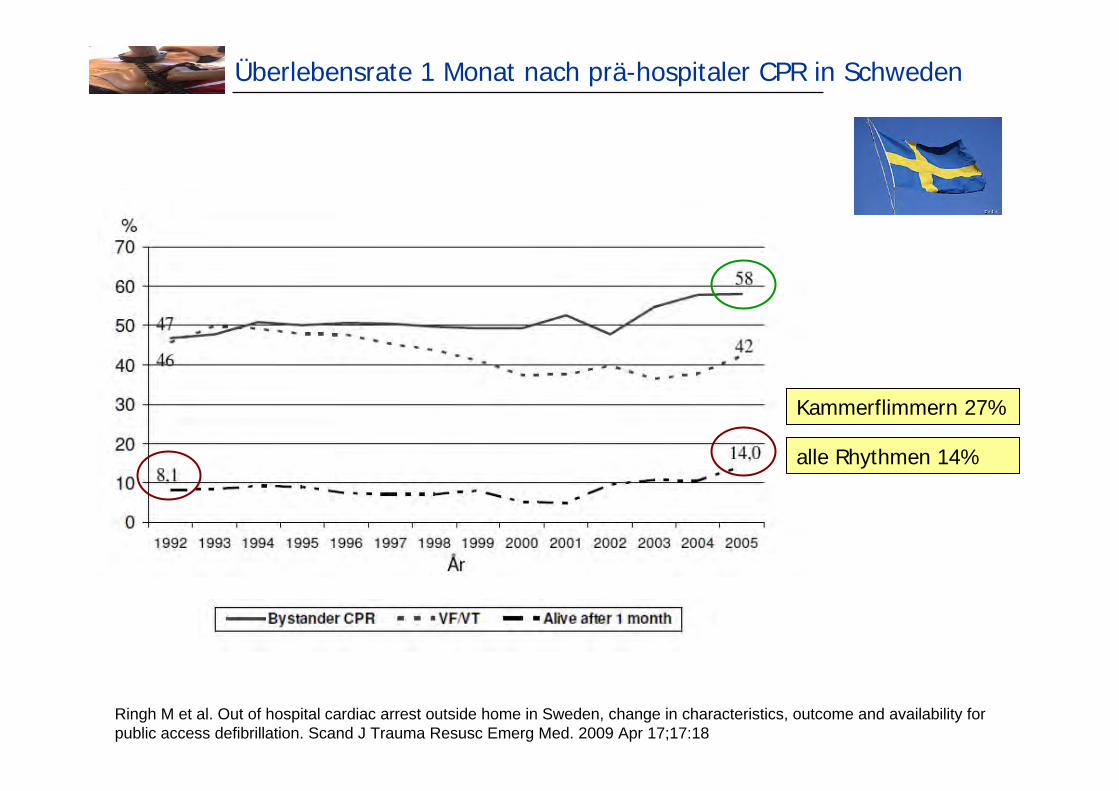
Überlebensrate 1 Monat nach prä-hospitaler CPR in Schweden
Ringh M et al. Out of hospital cardiac arrest outside home in Sweden, change in characteristics, outcome and availability forpublic access defibrillation. Scand J Trauma Resusc Emerg Med. 2009 Apr 17;17:18
Kammerflimmern 27%
alle Rhythmen 14%
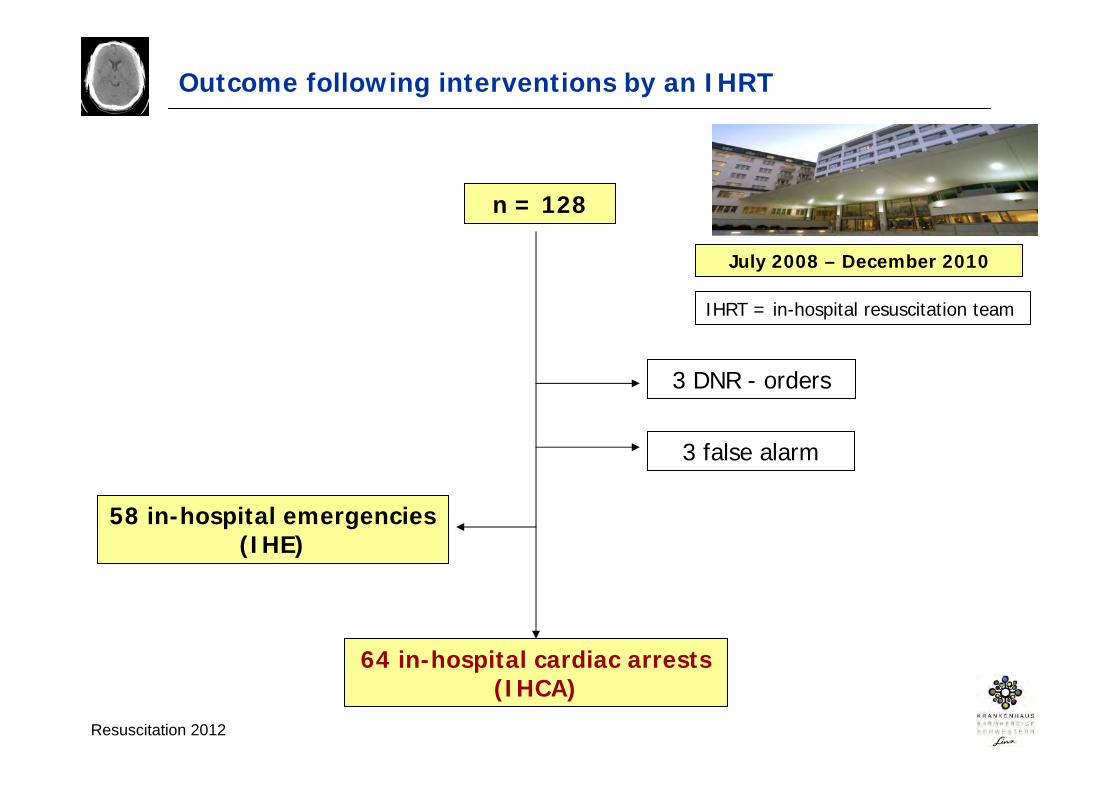
Outcome following interventions by an IHRT
n = 128
58 in-hospital emergencies(IHE)
July 2008 – December 2010
3 false alarm
64 in-hospital cardiac arrests(IHCA)
3 DNR - orders
Resuscitation 2012
IHRT = in-hospital resuscitation team
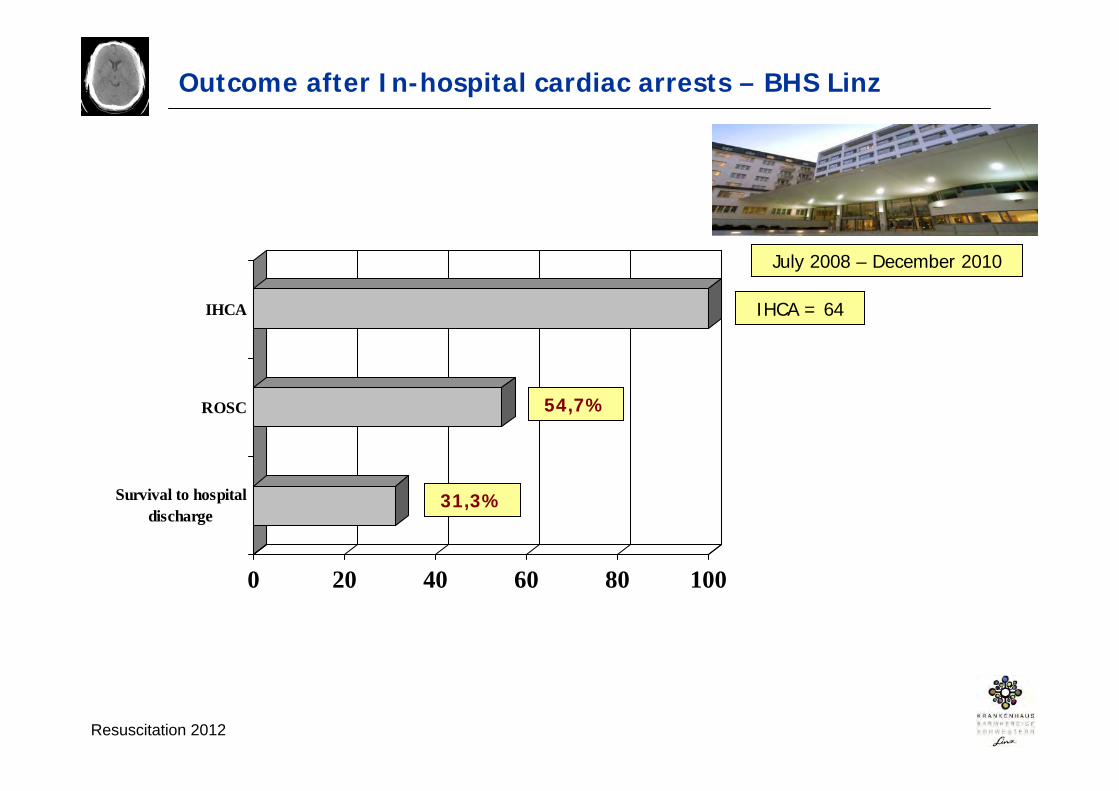
Outcome after In-hospital cardiac arrests – BHS Linz
Resuscitation 2012
IHCA = 64
0 20 40 60 80 100
Survival to hospitaldischarge
ROSC
IHCA
31,3%
54,7%
July 2008 – December 2010
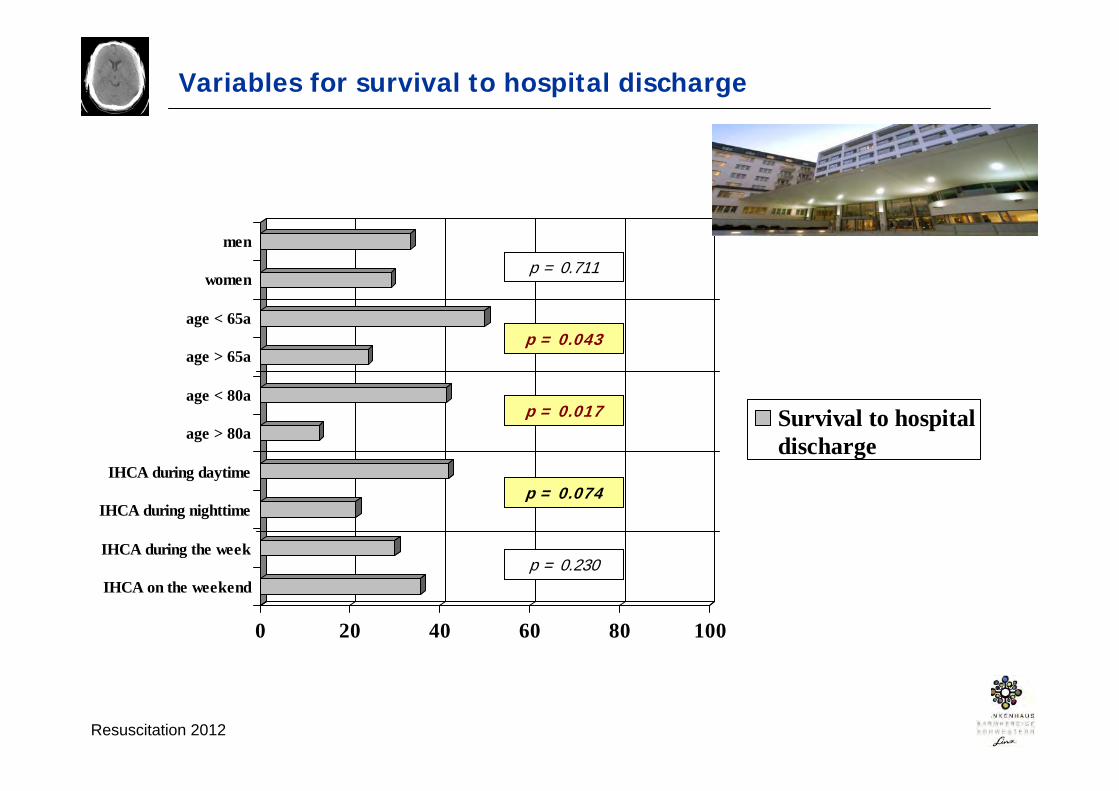
Variables for survival to hospital discharge
Resuscitation 2012
0 20 40 60 80 100
IHCA on the weekend
IHCA during the week
IHCA during nighttime
IHCA during daytime
age > 80a
age < 80a
age > 65a
age < 65a
women
men
Survival to hospitaldischarge
p = 0.043
p = 0.074
p = 0.230
p = 0.711
p = 0.017

IHCA – shockable vs. non-shockable rhythms
Resuscitation 2012
0102030405060708090
100
ROSClebend entlassen
SchockbarerRhythmus
n = 11 n = 53
Nicht-schockbarerRhythmus
p < 0.001
p = 0.067
European Resuscitation Council – ALS guidelines 2010
www.CPRguidelines.eu
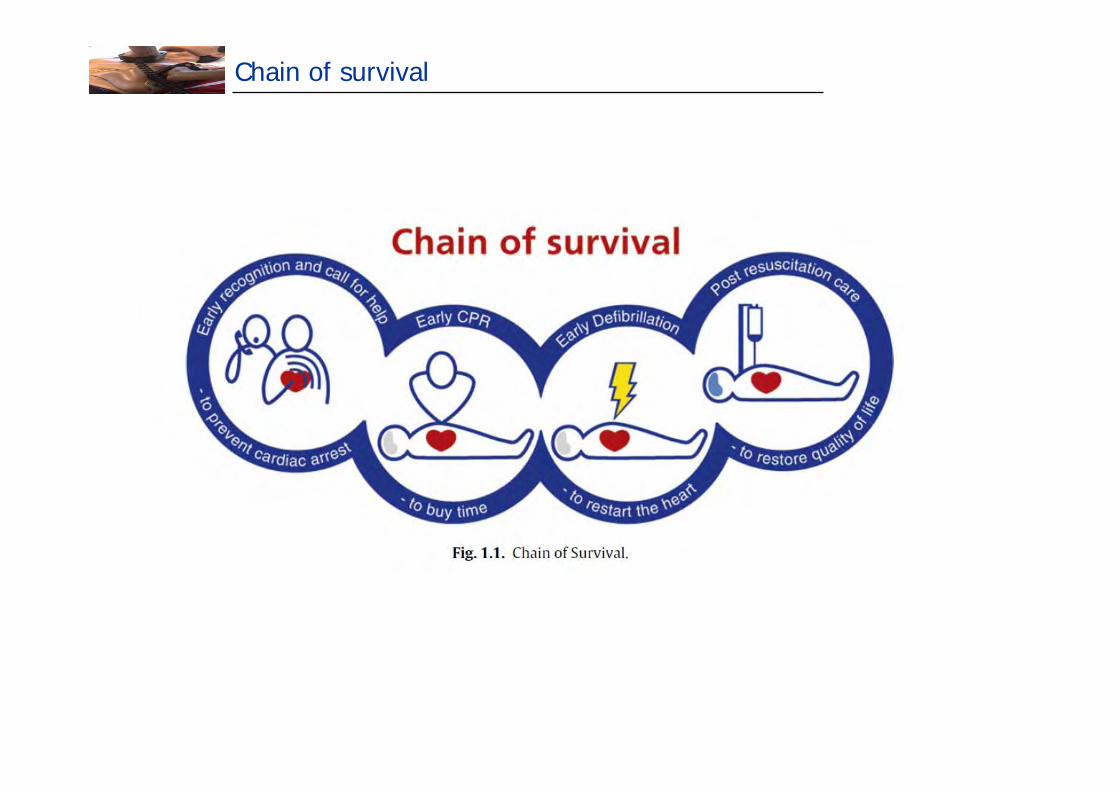
Chain of survival
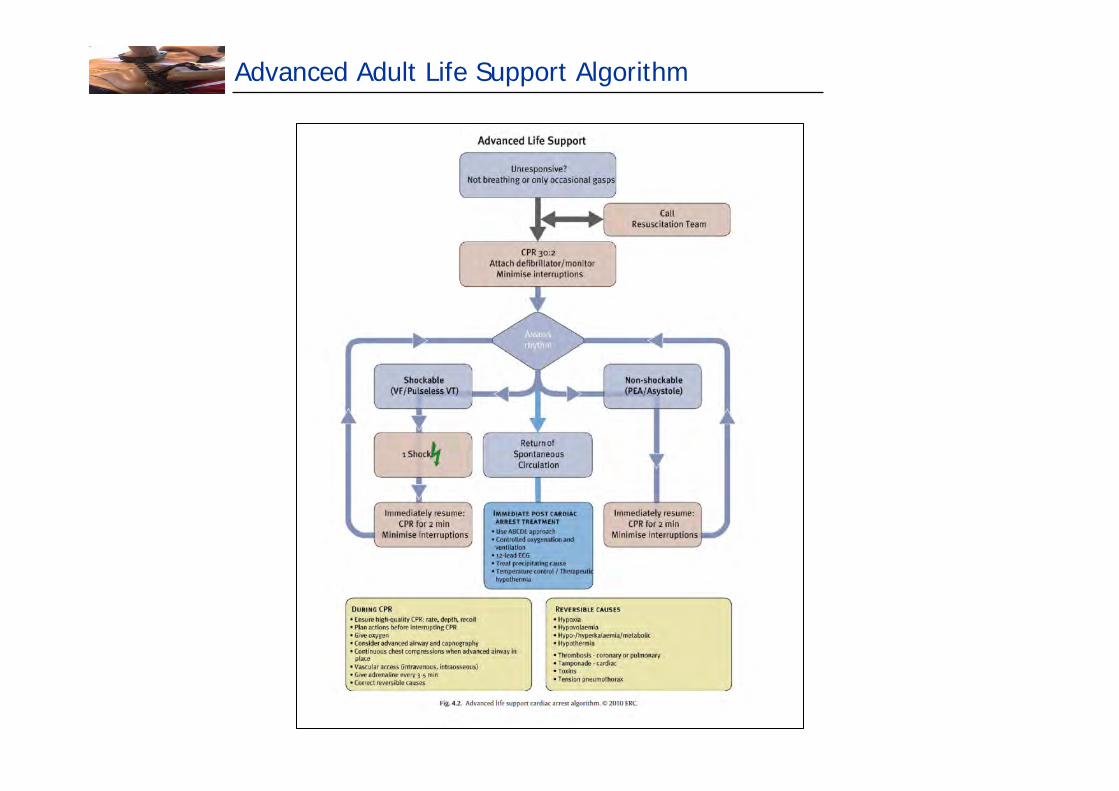
Advanced Adult Life Support Algorithm

Der reglose Patient
Notfallcheck (1)
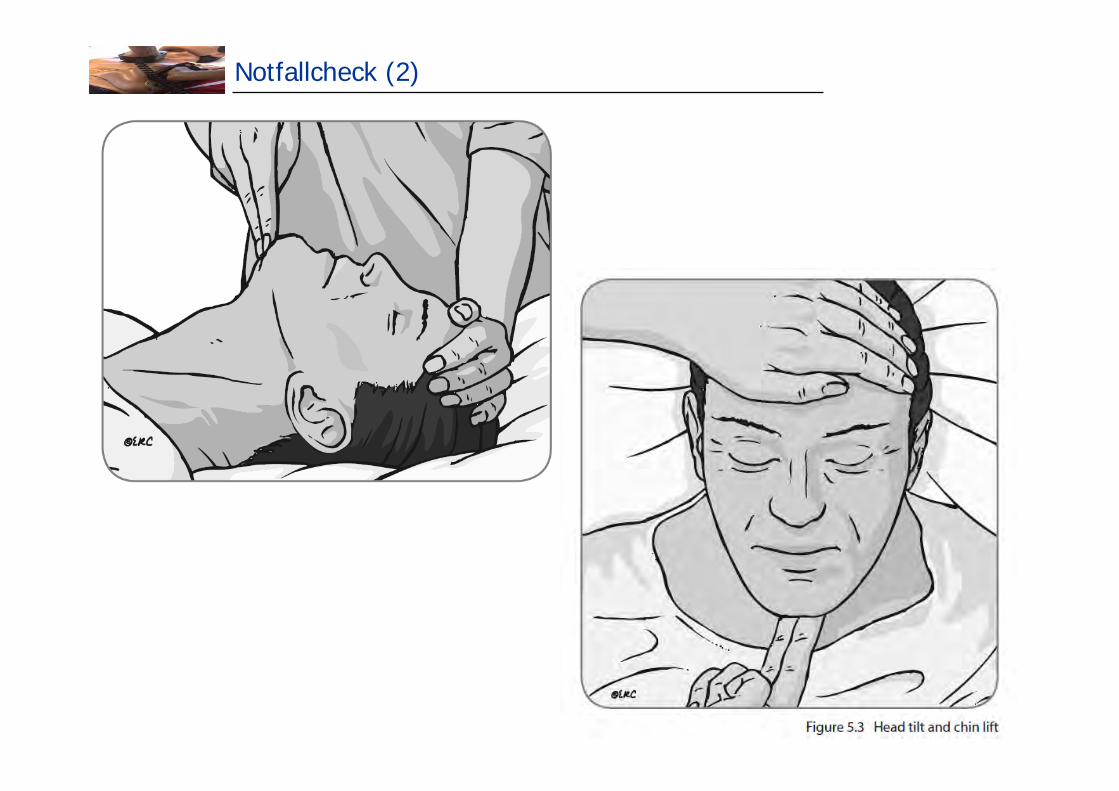
Notfallcheck (2)
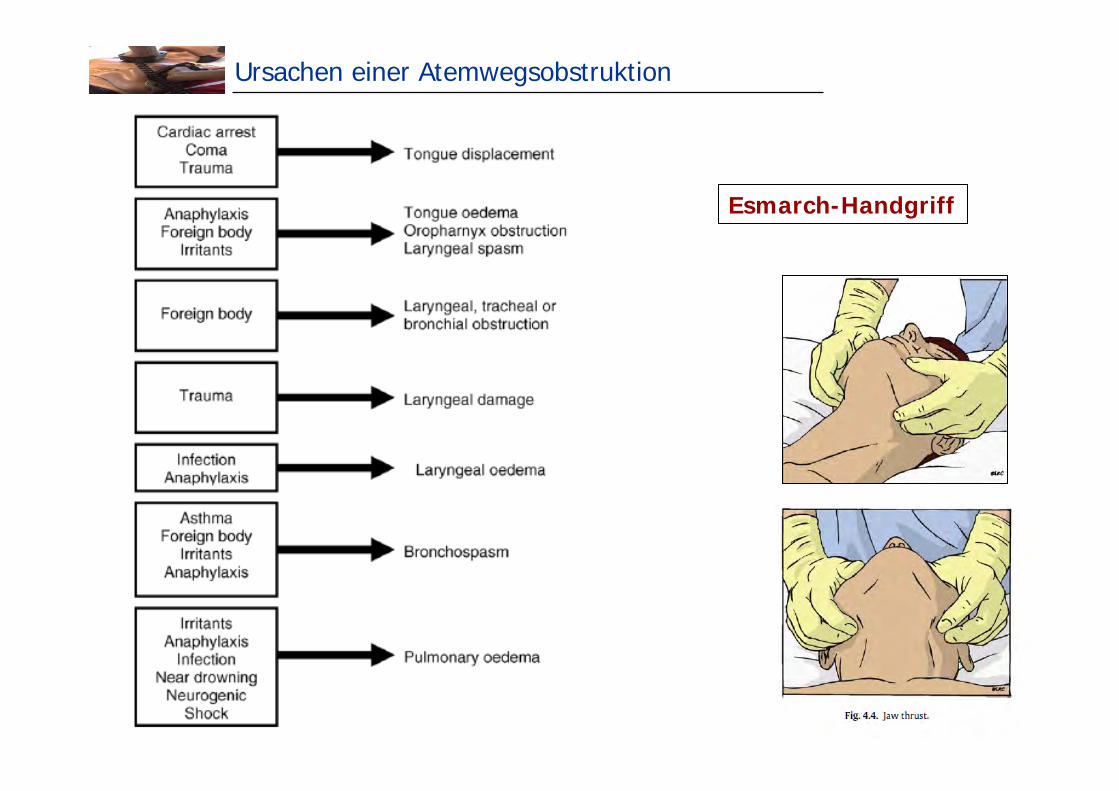
Ursachen einer Atemwegsobstruktion
Esmarch-Handgriff
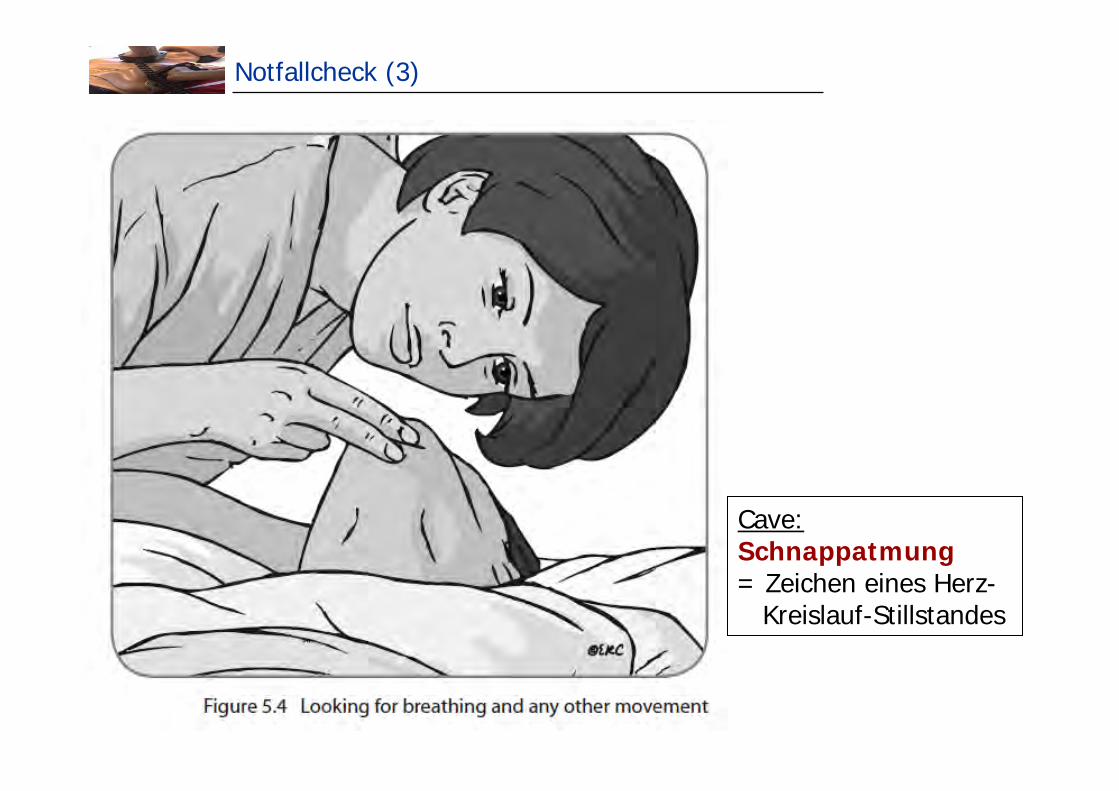
Notfallcheck (3)
Cave:Schnappatmung = Zeichen eines Herz-
Kreislauf-Stillstandes
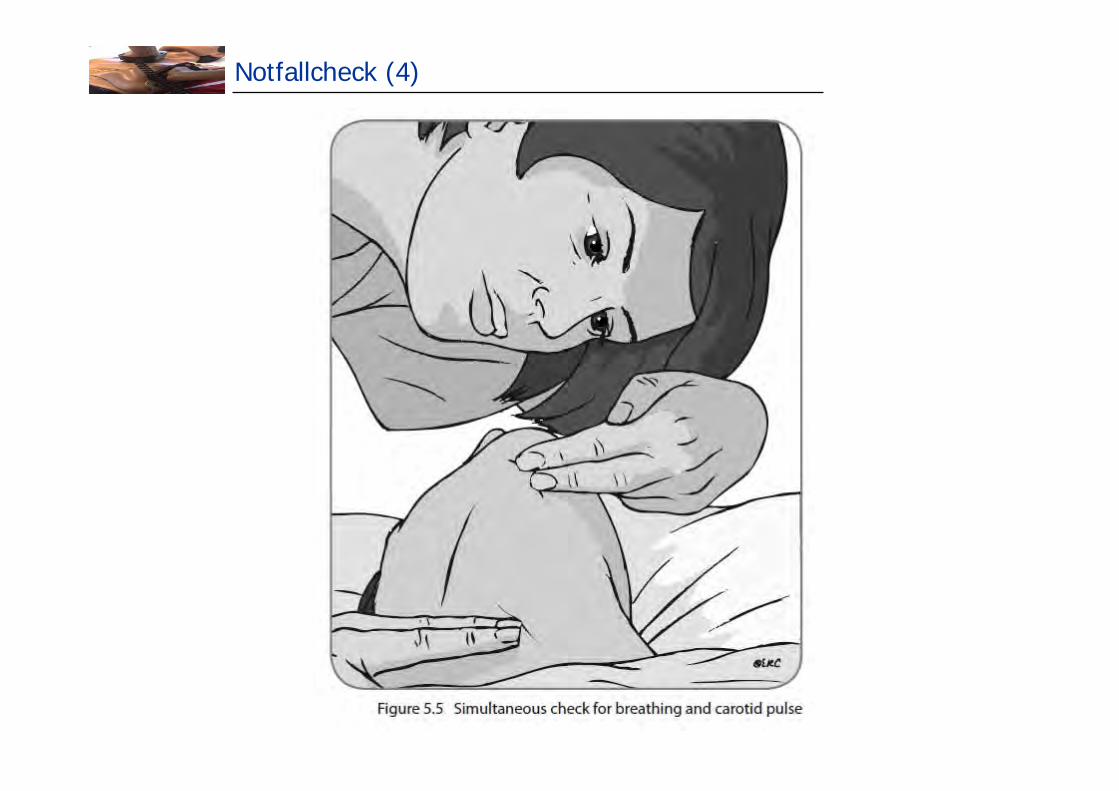
Notfallcheck (4)
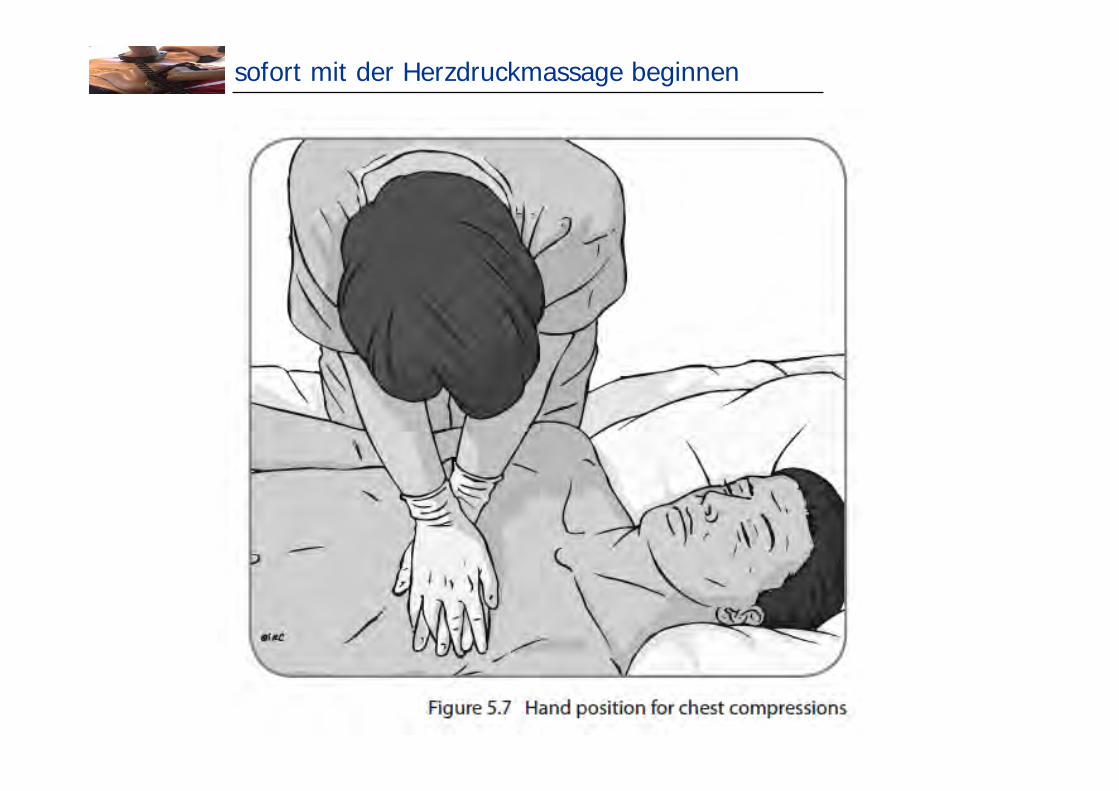
sofort mit der Herzdruckmassage beginnen
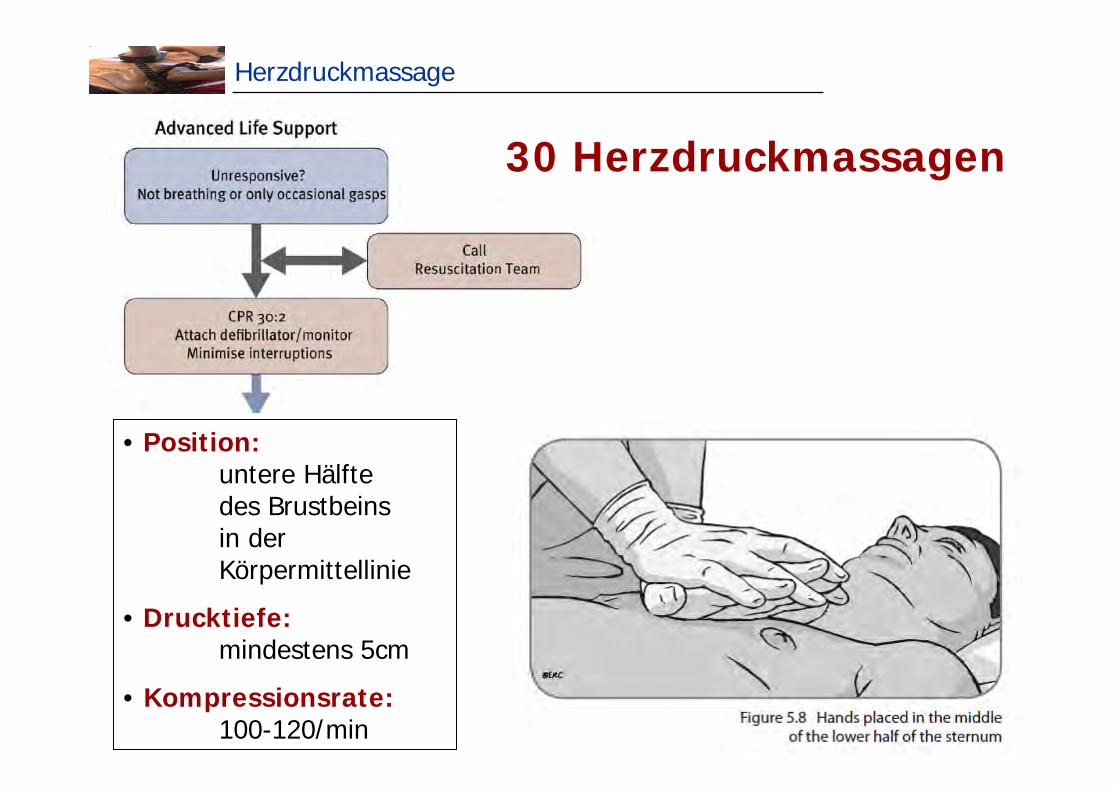
Herzdruckmassage
• Position:untere Hälftedes Brustbeins in der Körpermittellinie
• Drucktiefe: mindestens 5cm
• Kompressionsrate: 100-120/min
30 Herzdruckmassagen
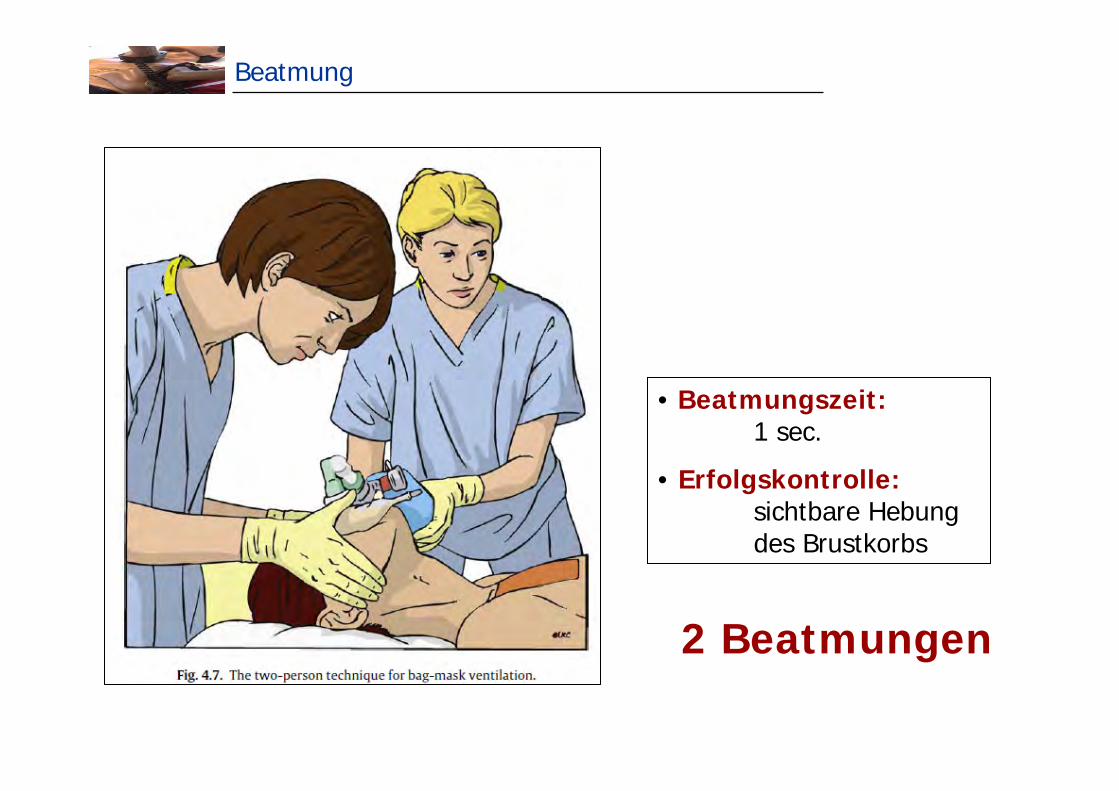
Beatmung
• Beatmungszeit: 1 sec.
• Erfolgskontrolle: sichtbare Hebungdes Brustkorbs
2 Beatmungen
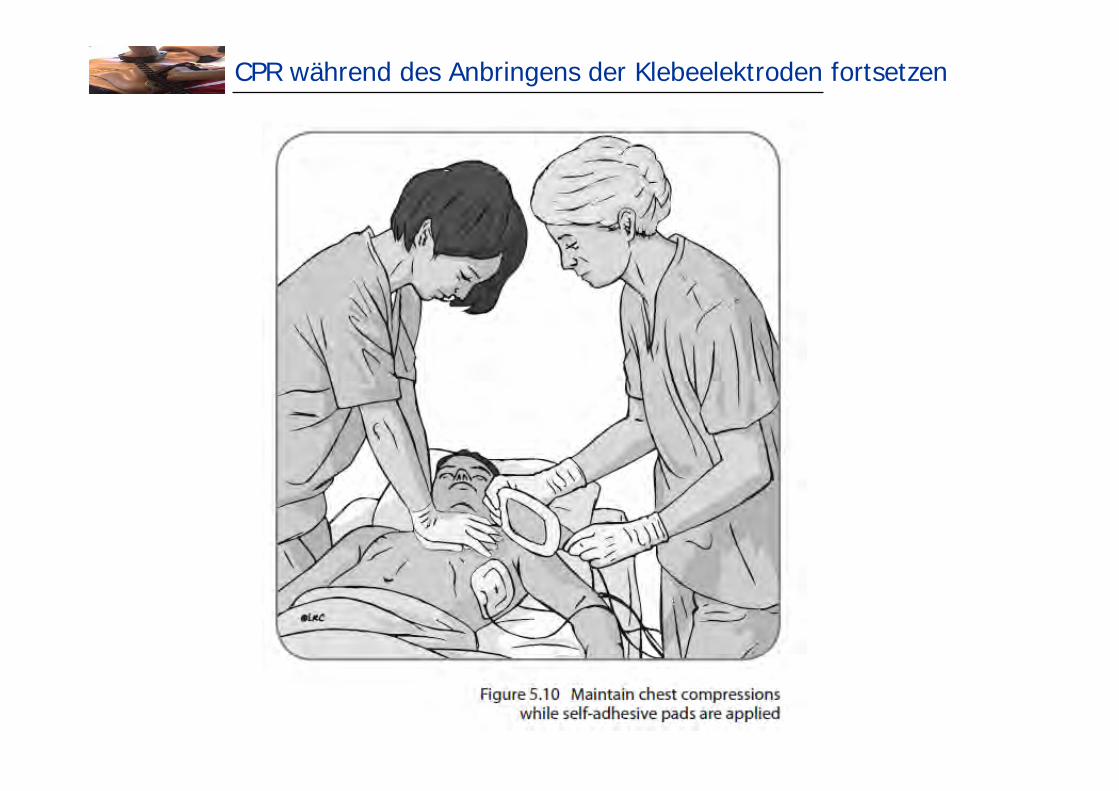
CPR während des Anbringens der Klebeelektroden fortsetzen
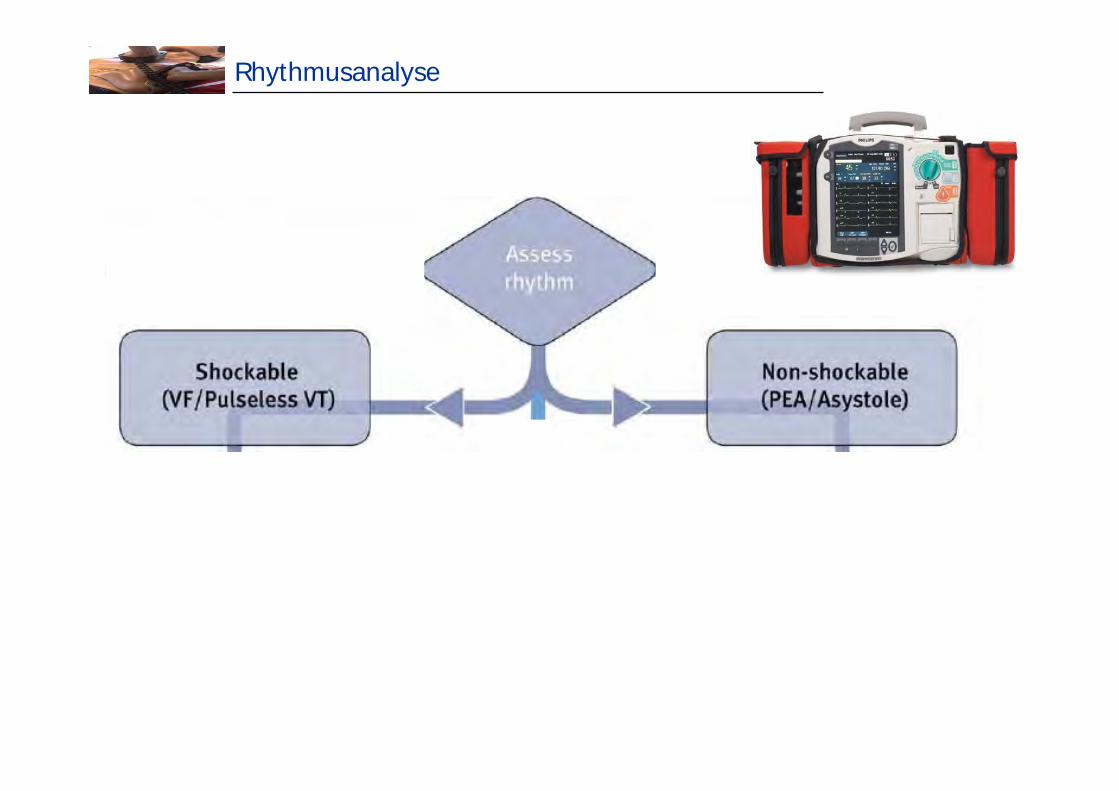
Rhythmusanalyse
Rhythmusanalyse
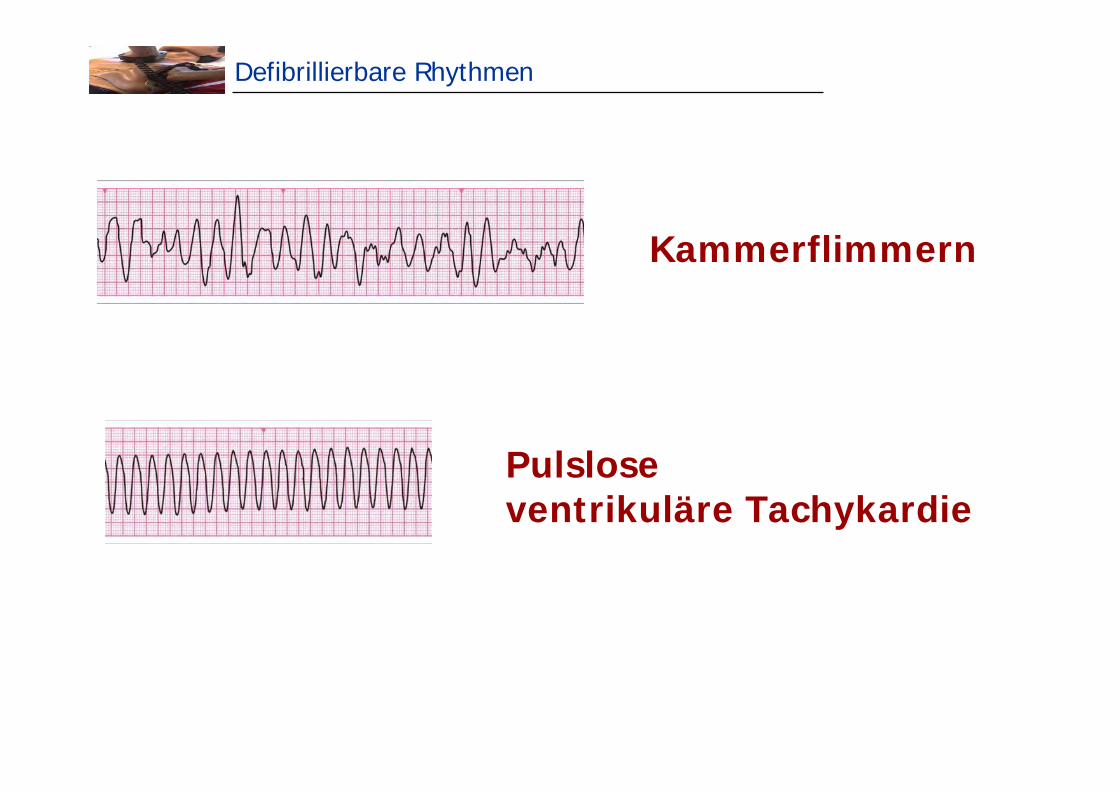
Defibrillierbare Rhythmen
Kammerflimmern
Pulslose ventrikuläre Tachykardie
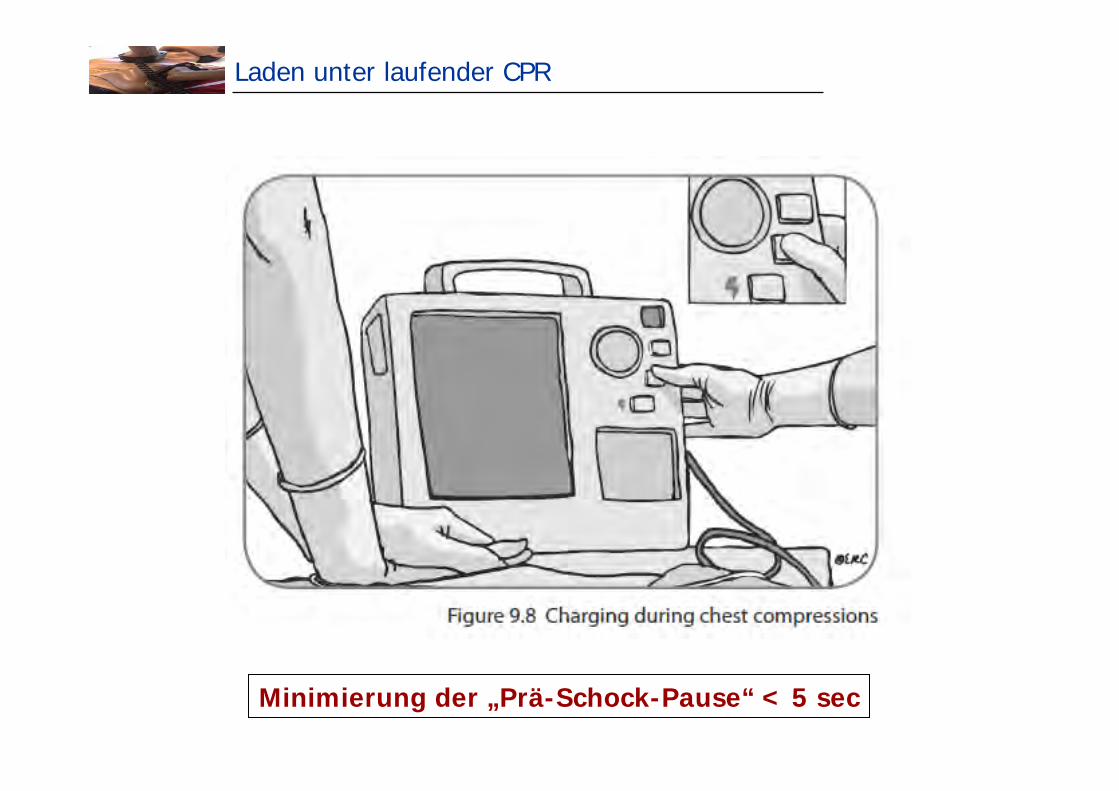
Laden unter laufender CPR
Minimierung der „Prä-Schock-Pause“ < 5 sec
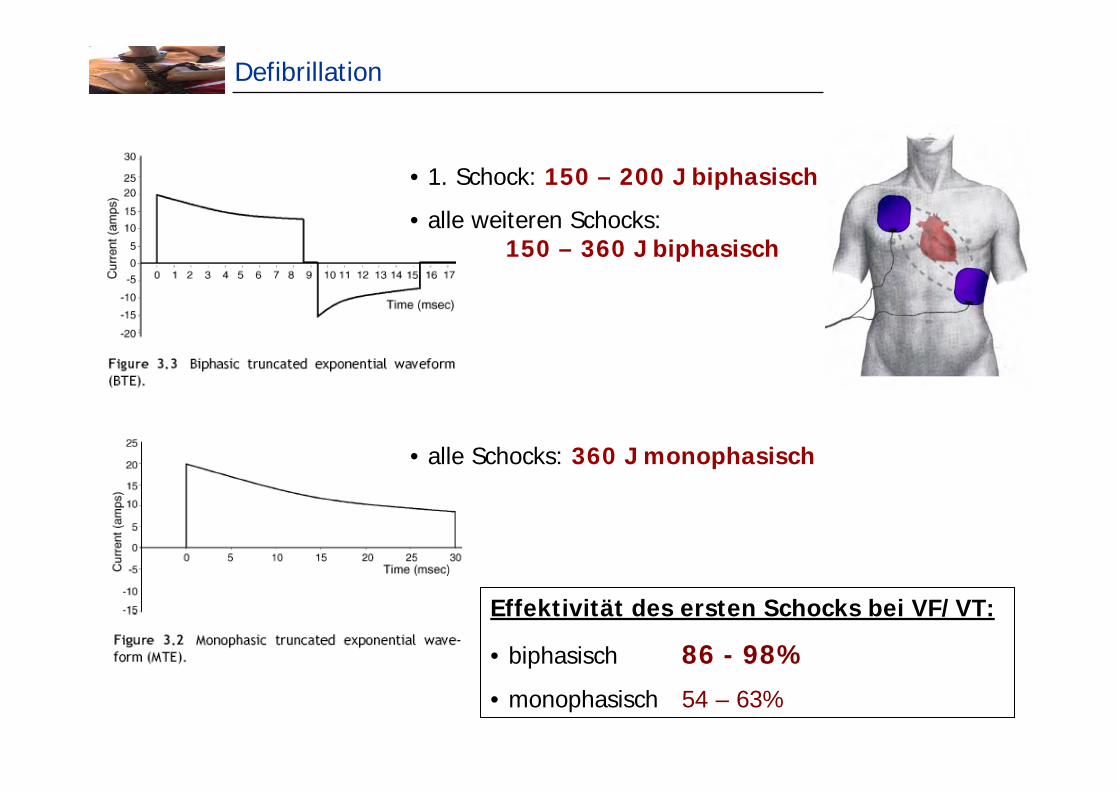
Defibrillation
• 1. Schock: 150 – 200 J biphasisch
• alle weiteren Schocks: 150 – 360 J biphasisch
• alle Schocks: 360 J monophasisch
Effektivität des ersten Schocks bei VF/VT:
• biphasisch 86 - 98%
• monophasisch 54 – 63%
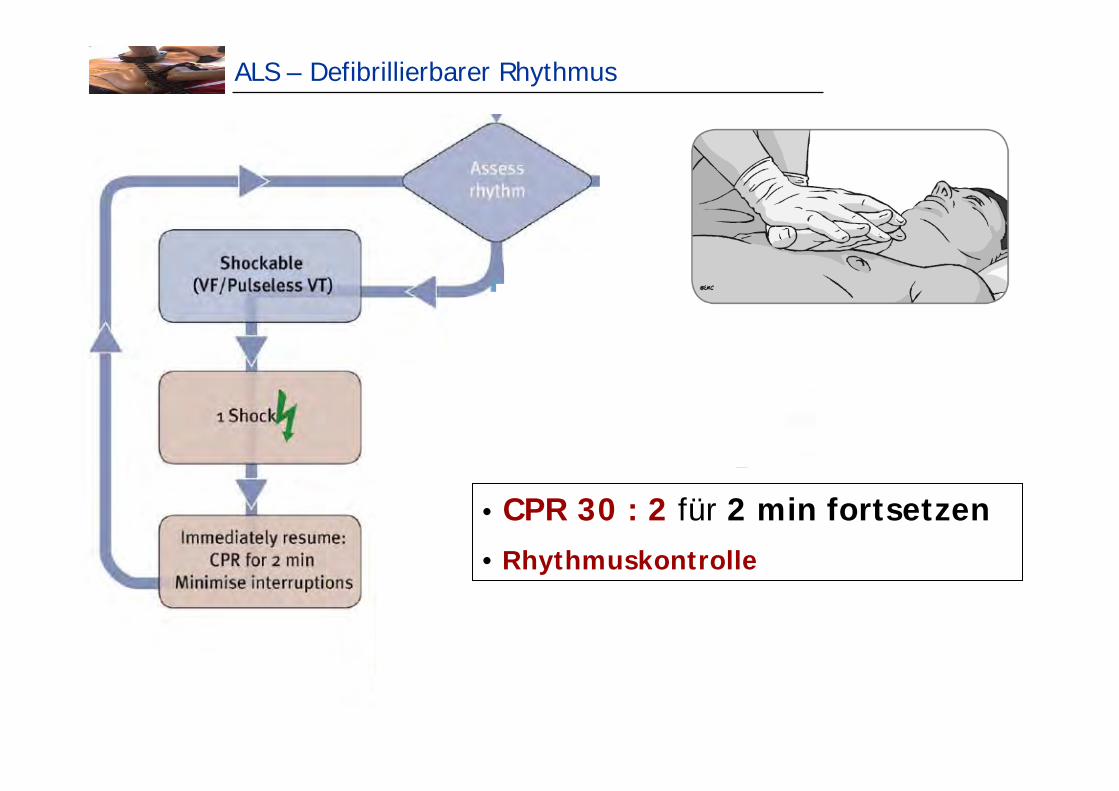
ALS – Defibrillierbarer Rhythmus
• CPR 30 : 2 für 2 min fortsetzen• Rhythmuskontrolle
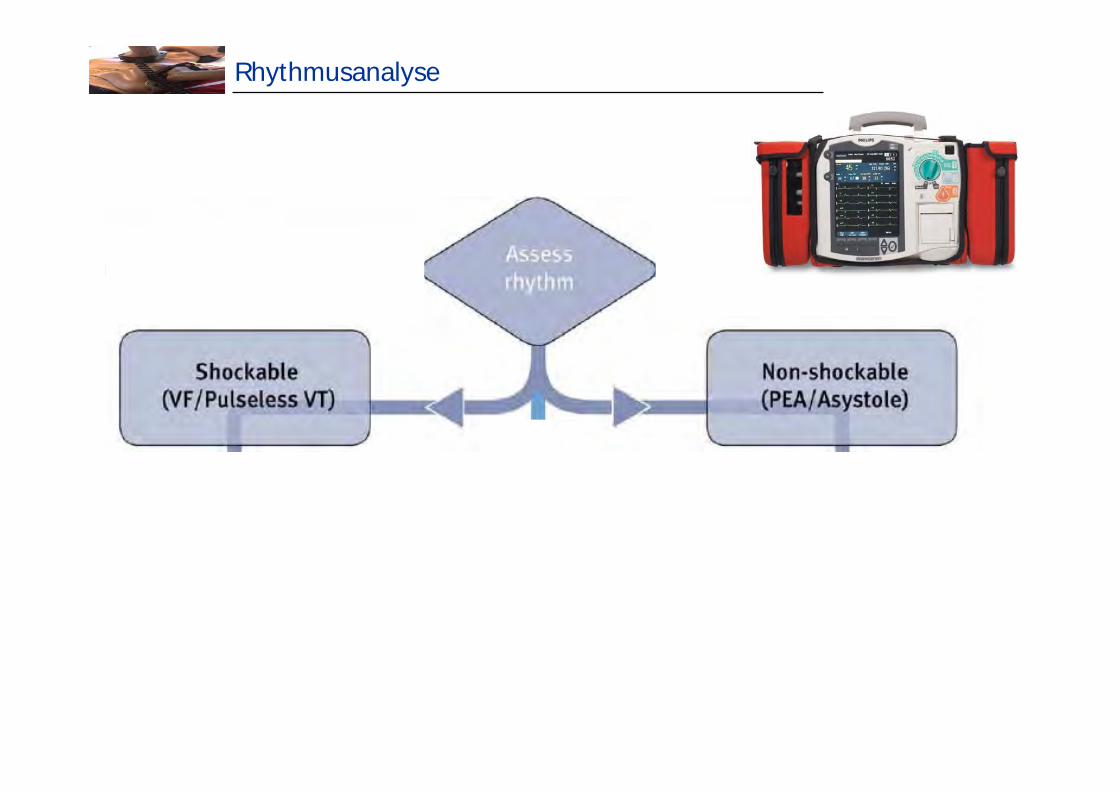
Rhythmusanalyse
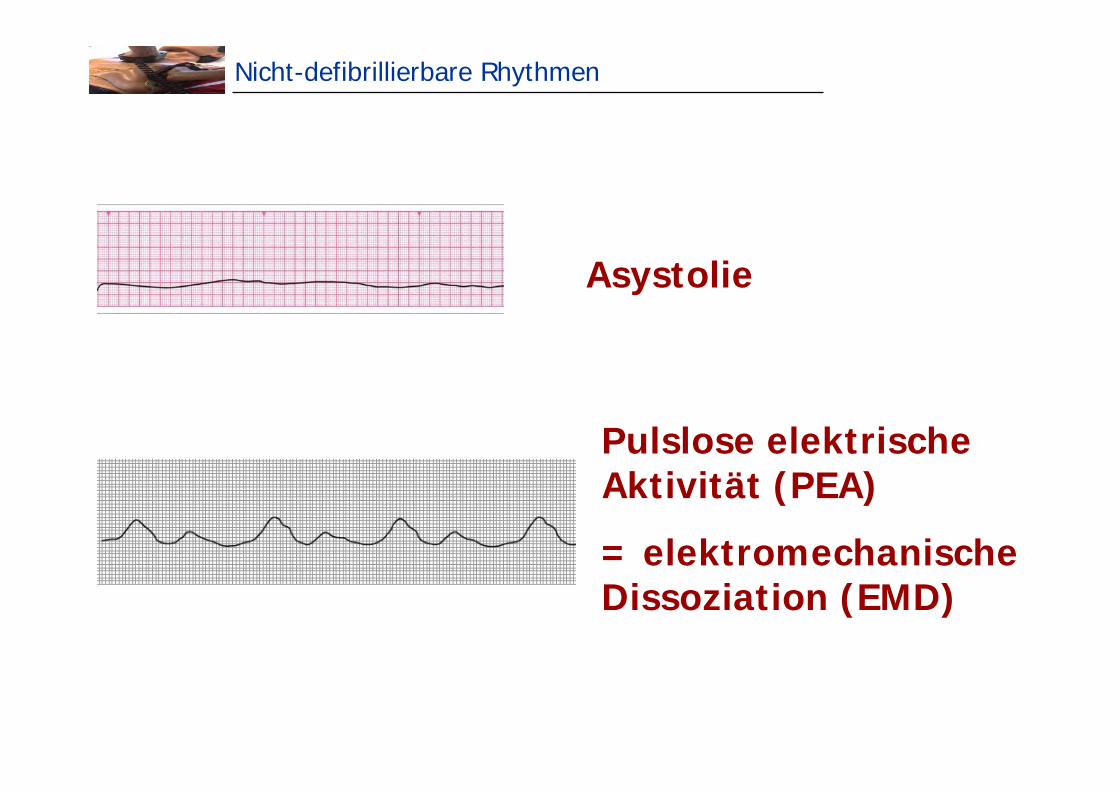
Nicht-defibrillierbare Rhythmen
Asystolie
Pulslose elektrische Aktivität (PEA)
= elektromechanische Dissoziation (EMD)
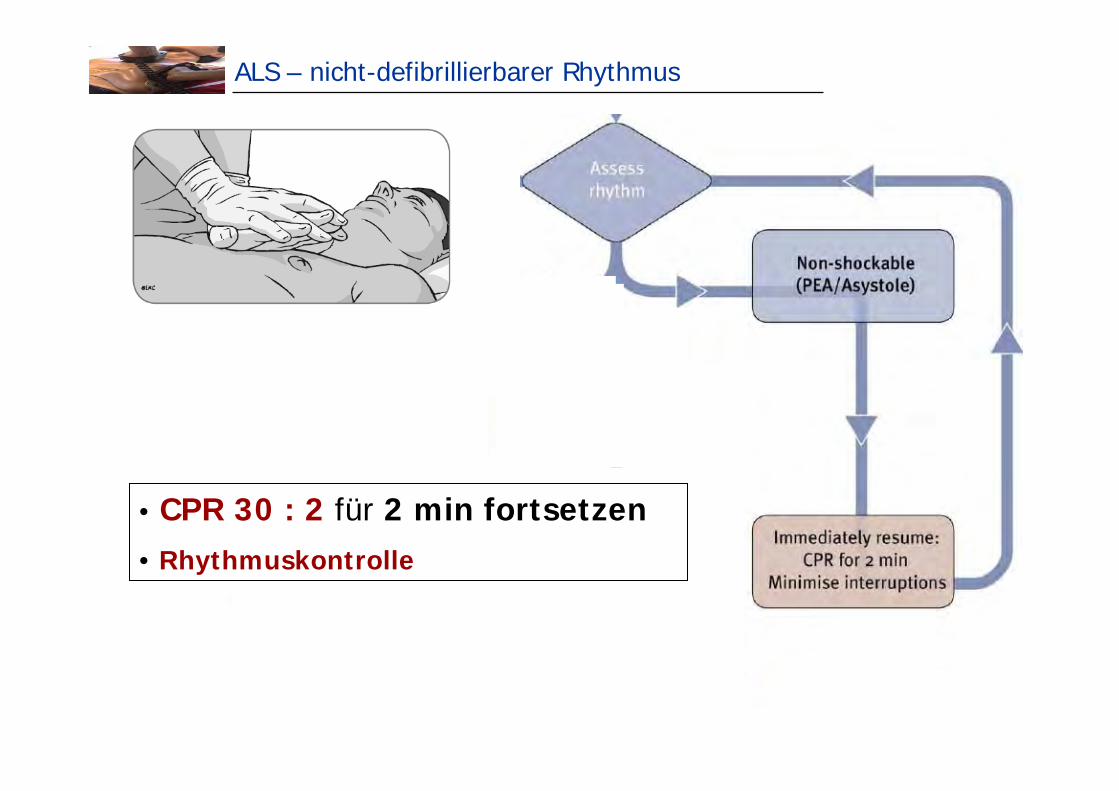
ALS – nicht-defibrillierbarer Rhythmus
• CPR 30 : 2 für 2 min fortsetzen• Rhythmuskontrolle
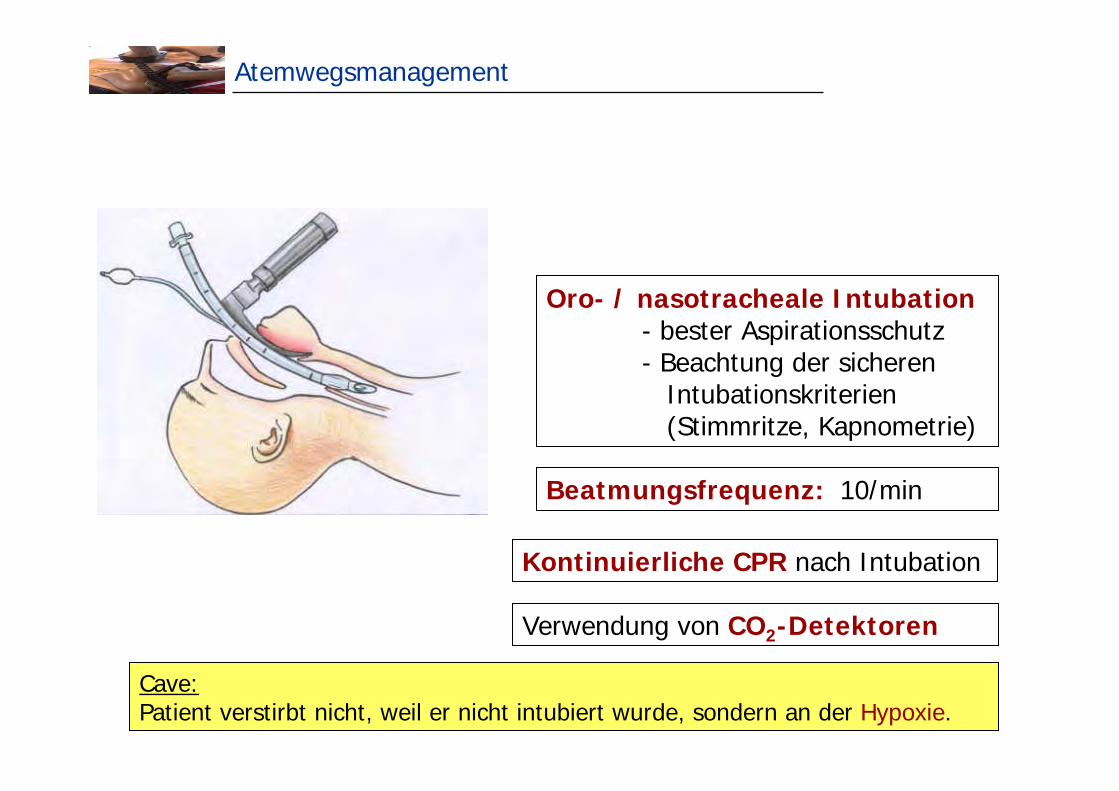
Atemwegsmanagement
Oro- / nasotracheale Intubation- bester Aspirationsschutz- Beachtung der sicheren
Intubationskriterien(Stimmritze, Kapnometrie)
Kontinuierliche CPR nach Intubation
Cave:Patient verstirbt nicht, weil er nicht intubiert wurde, sondern an der Hypoxie.
Verwendung von CO2-Detektoren
Beatmungsfrequenz: 10/min
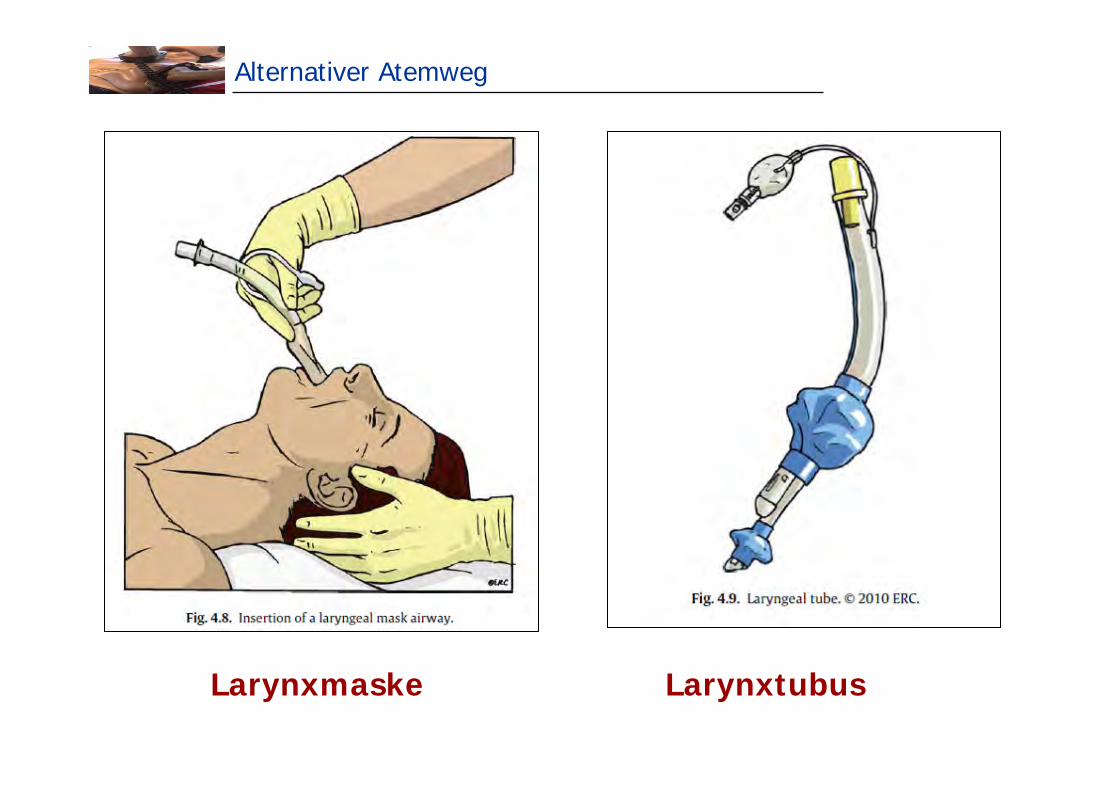
Alternativer Atemweg
Larynxmaske Larynxtubus
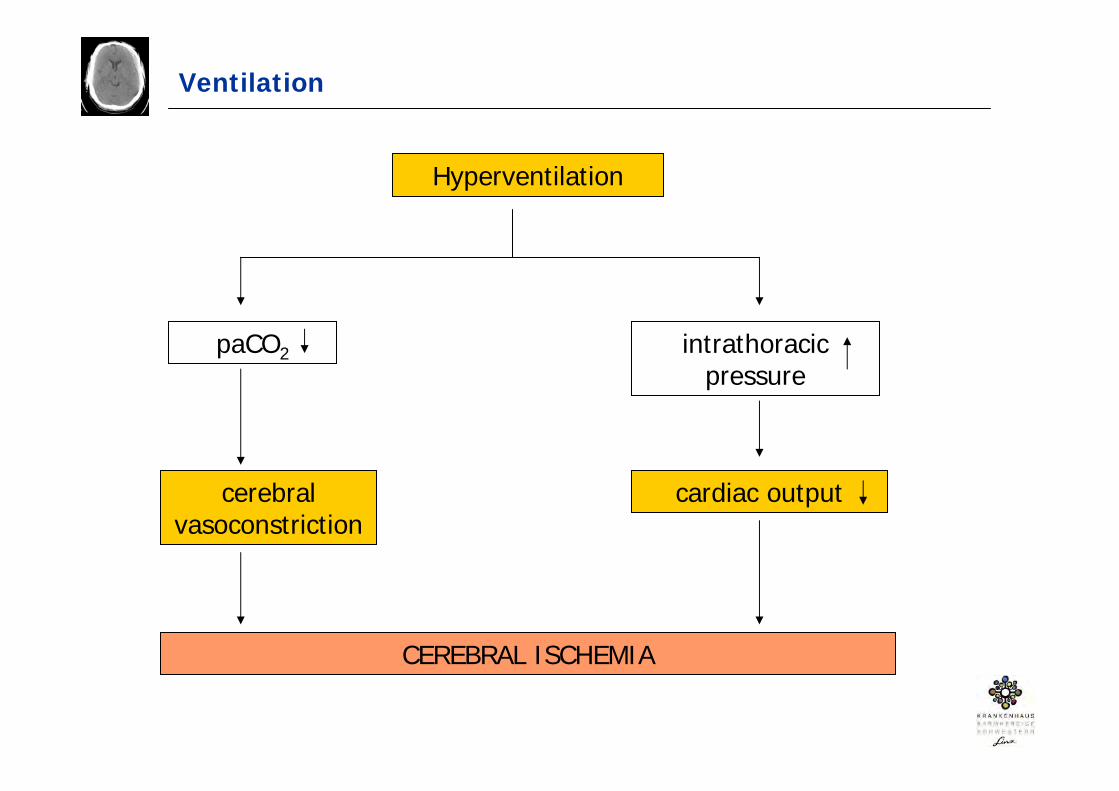
Ventilation
Hyperventilation
paCO2 intrathoracicpressure
cerebral vasoconstriction
cardiac output
CEREBRAL ISCHEMIA
Oxygenation and Ventilation
SO2 94 – 98%
Tidalvolumen 6ml/kg IBW
PaCO2 35 – 45mmHg
Nolan JP et al. Current Opinion in Critical Care 2010;16:216-222
Tulder R et al. Notfall Rettungsmed 2010;13:212-218
Neumar RW et al. Circulation 2008;118:2452-2483
Adrenalin
bei nicht-schockbaren Rhythmen (Asystolie, PEA)- Adrenalin 1mg i.v. sobald als möglich verabreichen- Adrenalin 1mg i.v. alle 3-5min
bei schockbaren Rhythmen (VF, pulslose VT)- Adrenalin 1mg i.v. nach dem 3. Schock- Adrenalin 1mg i.v. alle 3-5min
endotracheale Verabreichung wird nicht mehr empfohlen
Amiodaron
bei schockbaren Rhythmen- Amiodaron 300mg i.v. nach dem 3. Schock- Amiodaron 150mg i.v. bei therapierefraktärem Kammerflimmern
Atropin
Atropin wird aufgrund fehlender Evidenz nicht mehr empfohlen
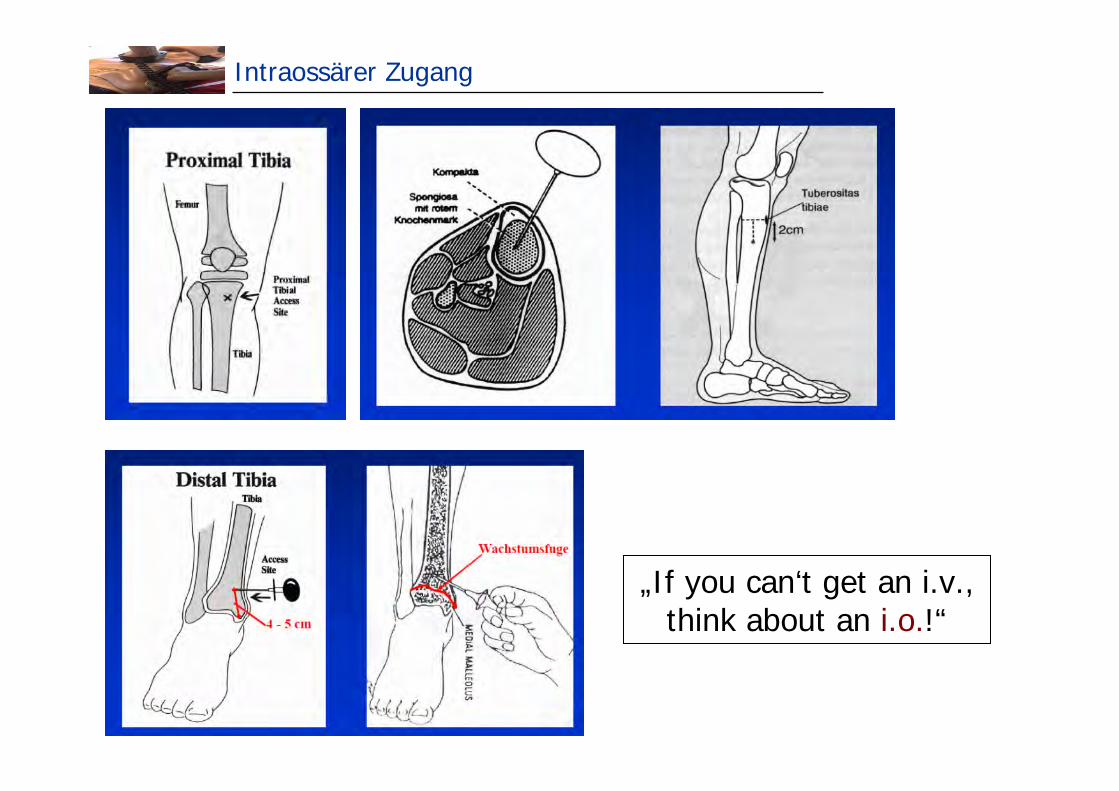
Intraossärer Zugang
„If you can‘t get an i.v., think about an i.o.!“
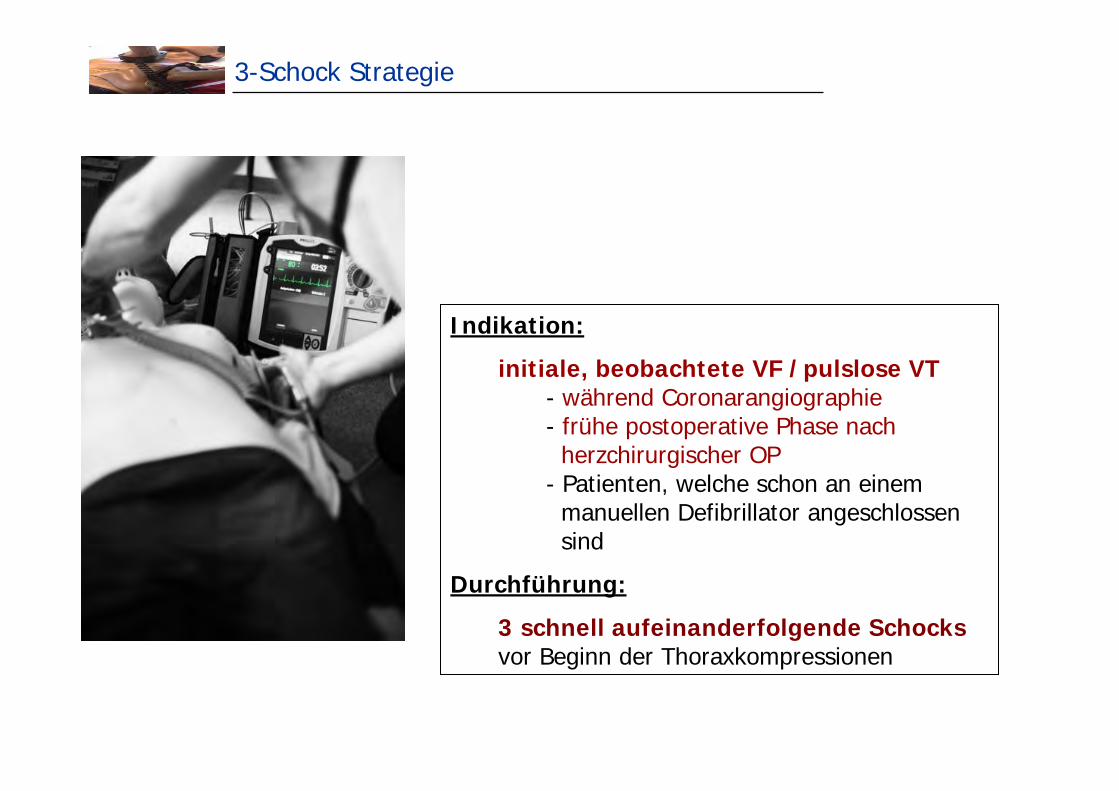
3-Schock Strategie
Indikation:
initiale, beobachtete VF /pulslose VT - während Coronarangiographie- frühe postoperative Phase nach
herzchirurgischer OP- Patienten, welche schon an einem
manuellen Defibrillator angeschlossensind
Durchführung:
3 schnell aufeinanderfolgende Schocksvor Beginn der Thoraxkompressionen
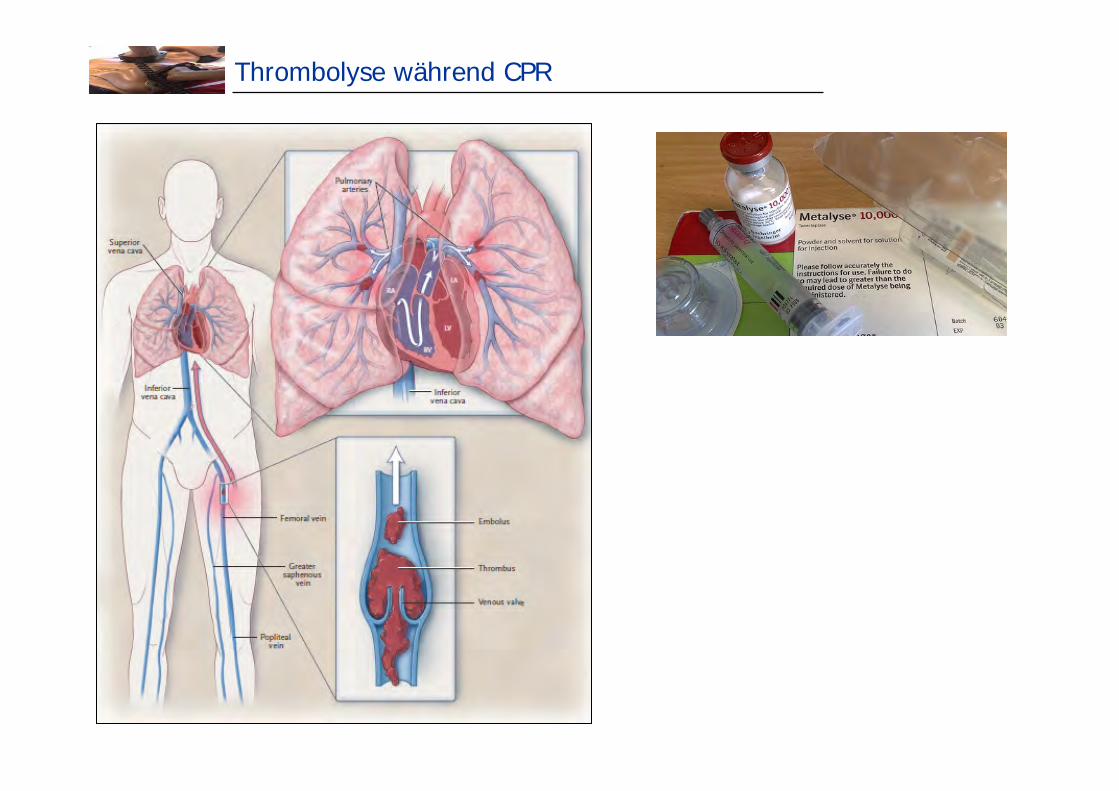
Thrombolyse während CPR
TROICA trial (1)
Böttiger BW et al. Thrombolysis during resuscitation for out-of-hospital cardiac arrest. N Engl J Med 2008;359:2651-62
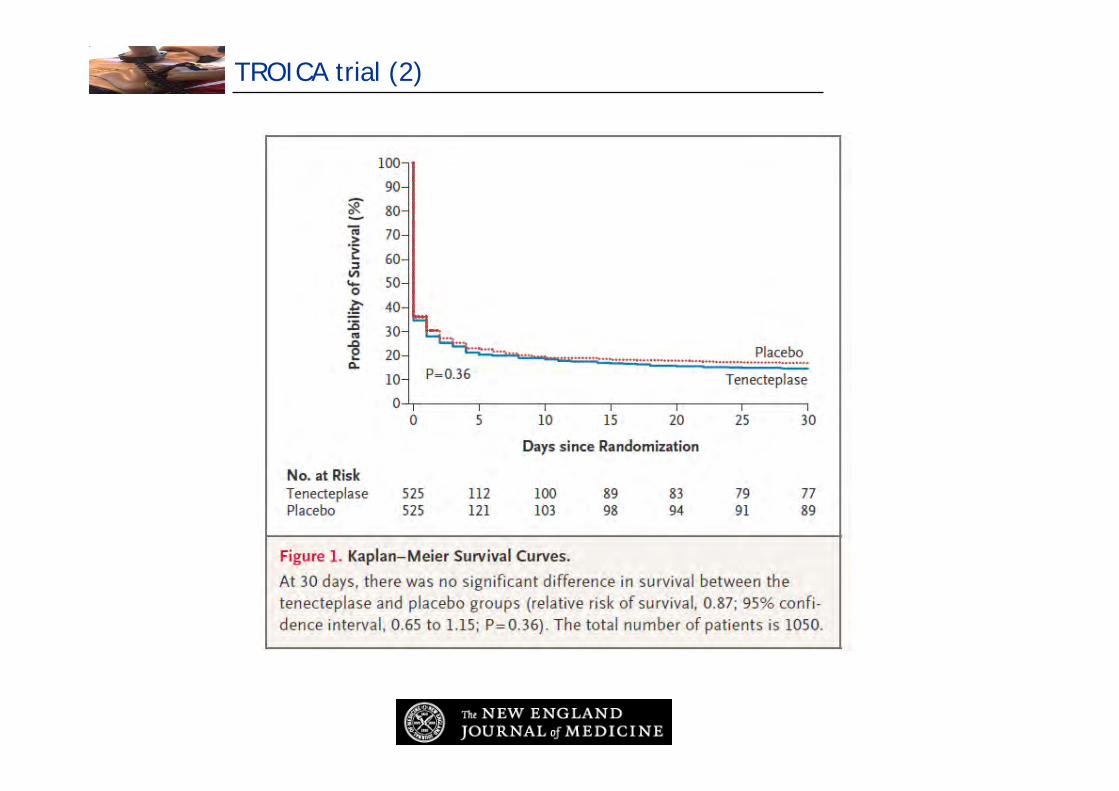
TROICA trial (2)
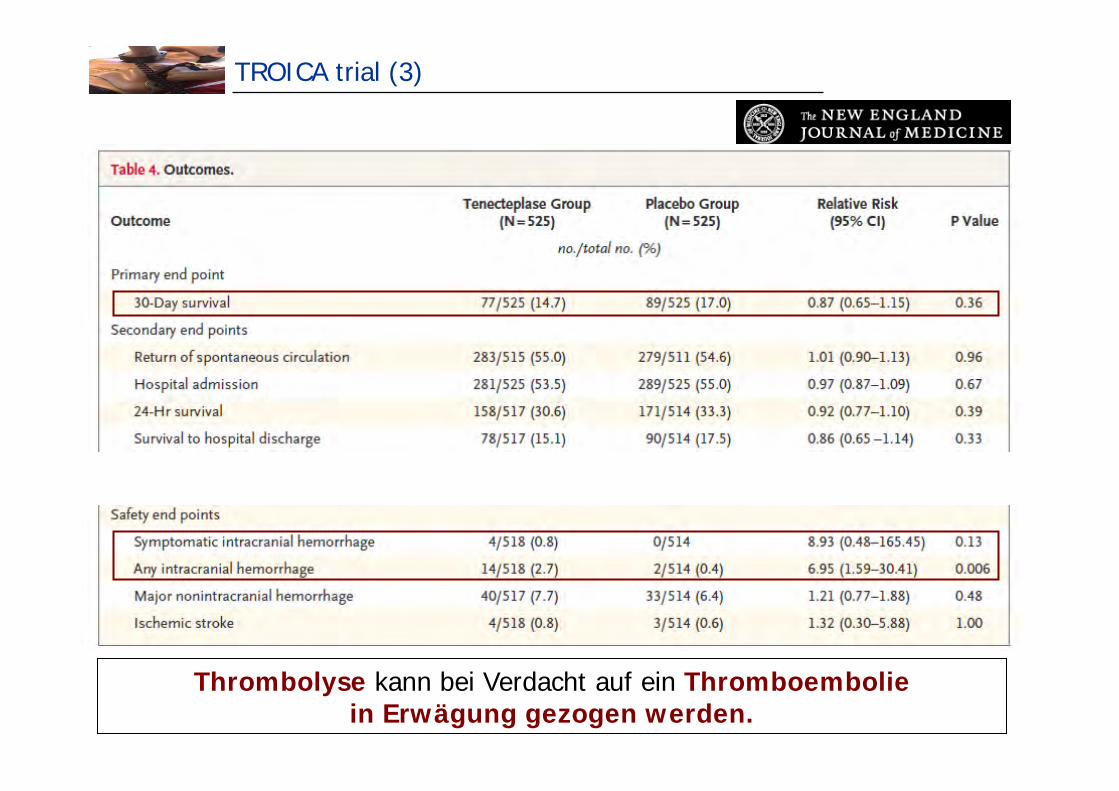
TROICA trial (3)
Thrombolyse kann bei Verdacht auf ein Thromboemboliein Erwägung gezogen werden.
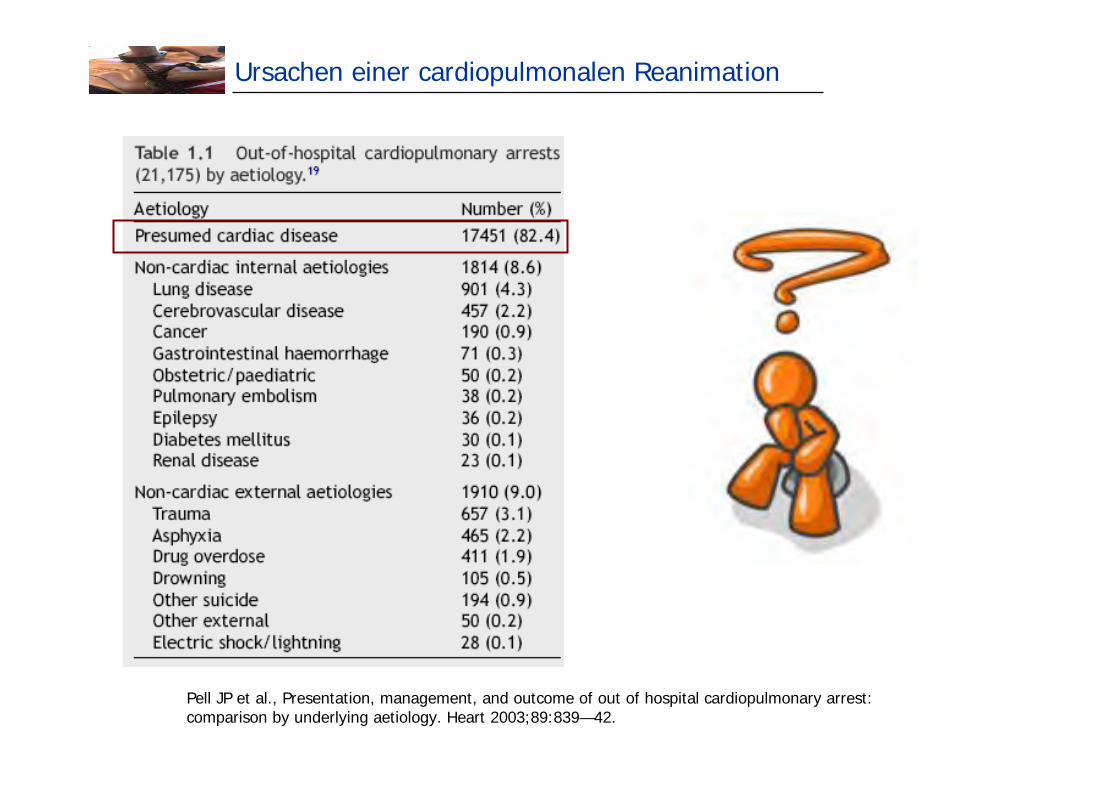
Ursachen einer cardiopulmonalen Reanimation
Pell JP et al., Presentation, management, and outcome of out of hospital cardiopulmonary arrest: comparison by underlying aetiology. Heart 2003;89:839—42.
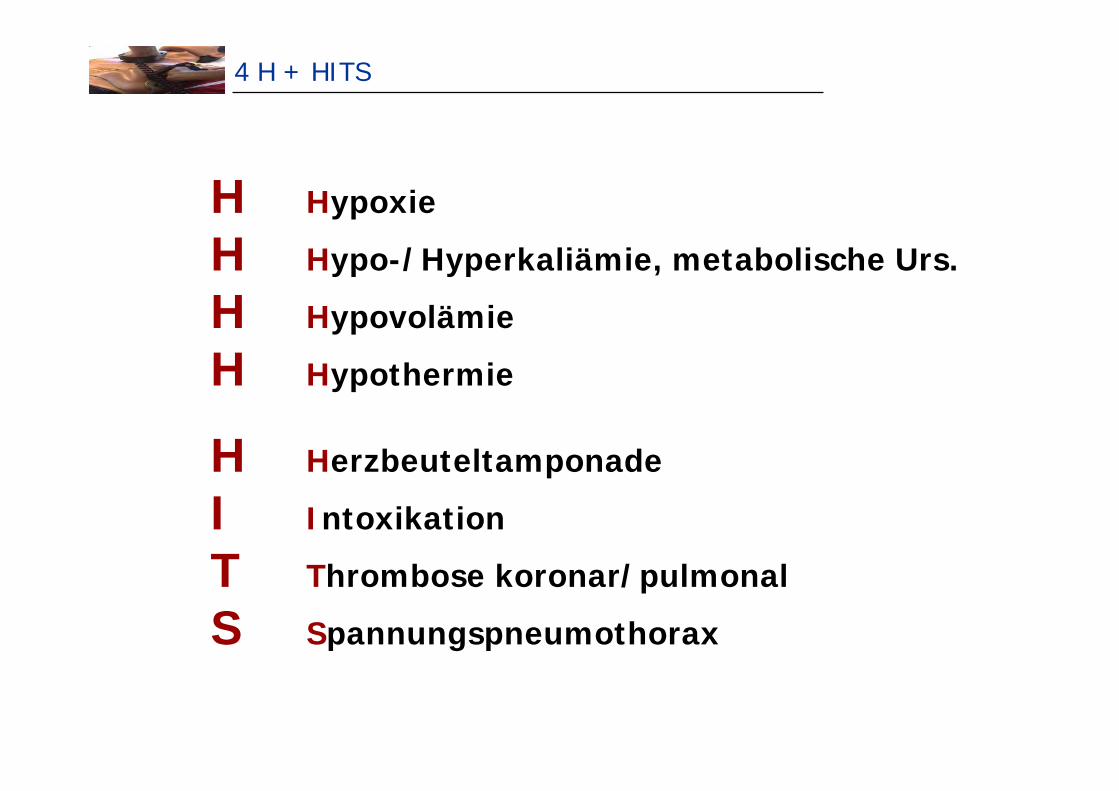
4 H + HITS
H Hypoxie
H Hypo-/Hyperkaliämie, metabolische Urs.
H Hypovolämie
H Hypothermie
H Herzbeuteltamponade
I Intoxikation
T Thrombose koronar/pulmonal
S Spannungspneumothorax
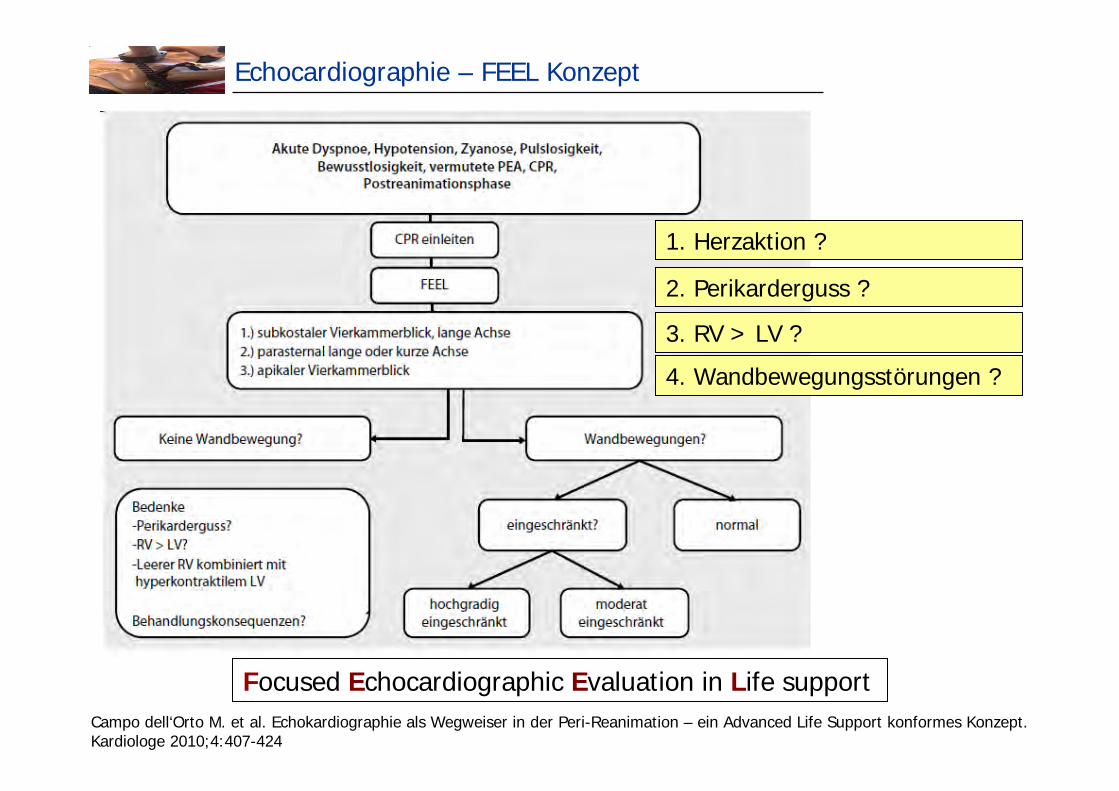
Echocardiographie – FEEL Konzept
Focused Echocardiographic Evaluation in Life supportCampo dell‘Orto M. et al. Echokardiographie als Wegweiser in der Peri-Reanimation – ein Advanced Life Support konformes Konzept. Kardiologe 2010;4:407-424
1. Herzaktion ?
2. Perikarderguss ?
3. RV > LV ?
4. Wandbewegungsstörungen ?
Return of spontaneous circulation – was nun ?!
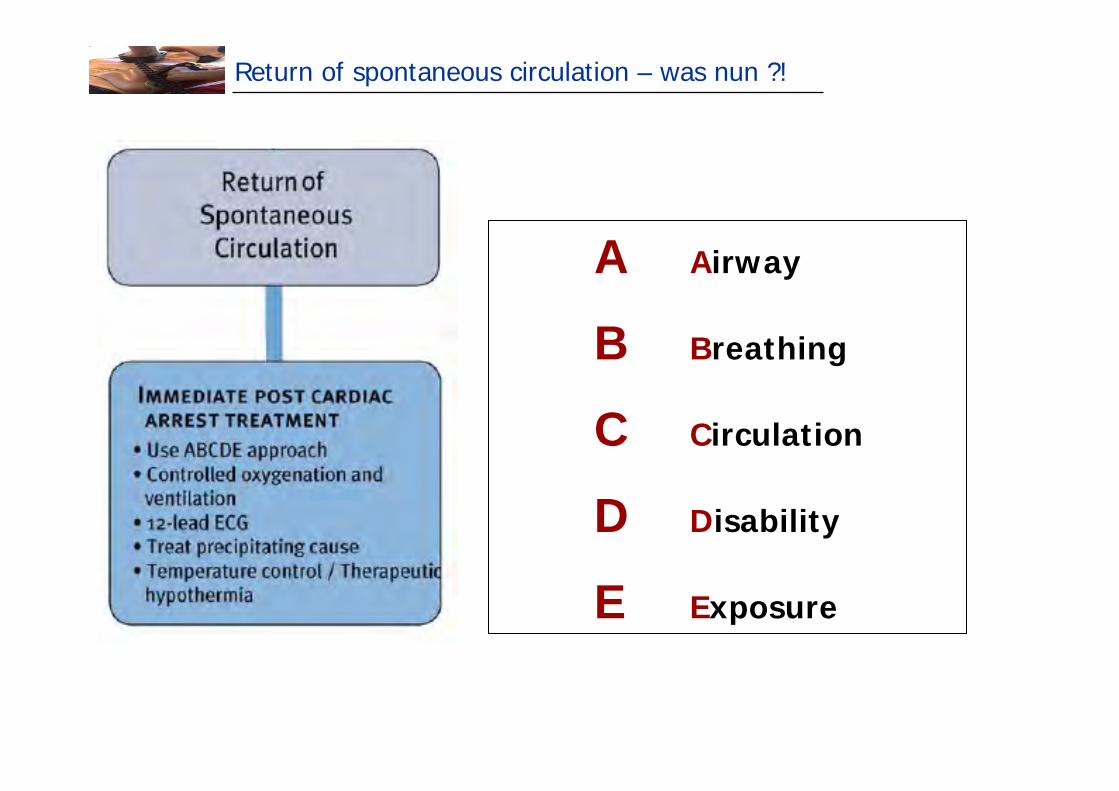
Return of spontaneous circulation – was nun ?!
A Airway
B Breathing
C Circulation
D Disability
E Exposure
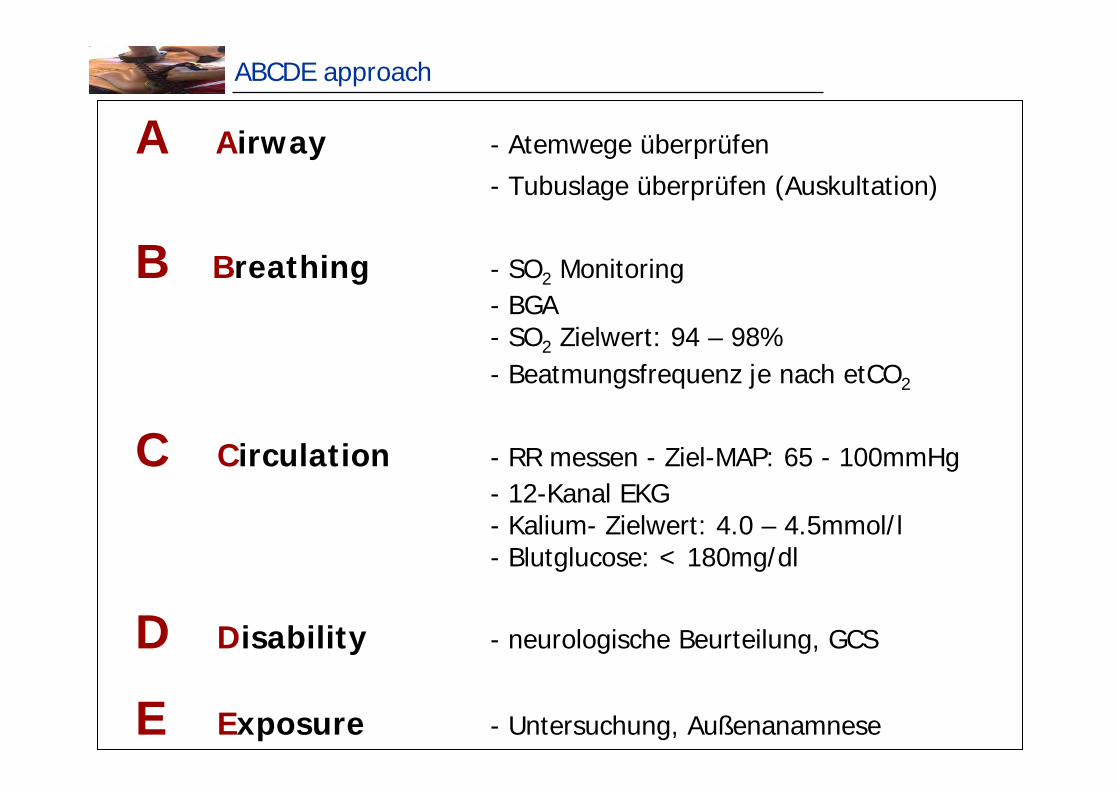
ABCDE approach
A Airway - Atemwege überprüfen
- Tubuslage überprüfen (Auskultation)
B Breathing - SO2 Monitoring- BGA- SO2 Zielwert: 94 – 98%- Beatmungsfrequenz je nach etCO2
C Circulation - RR messen - Ziel-MAP: 65 - 100mmHg- 12-Kanal EKG- Kalium- Zielwert: 4.0 – 4.5mmol/l- Blutglucose: < 180mg/dl
D Disability - neurologische Beurteilung, GCS
E Exposure - Untersuchung, Außenanamnese
Definition: Post-Reanimationssyndrom
Das Post-Reanimationssyndrom subsummiert pathophysiologische, in erster Linie inflammatorische Vorgänge, die im Zuge der Reperfusion auftreten u. eine weitere Schädigung des Organismus, insbesondere des Gehirns, vorantreiben.
Tulder R et al. Notfall Rettungsmed 2010;13:212-218
1. Post-cardiac arrest brain injury
2. Post-cardiac arrest myocardial dysfunction
3. Systemic ischemia / reperfusion injury
4. Persistent precipating pathology
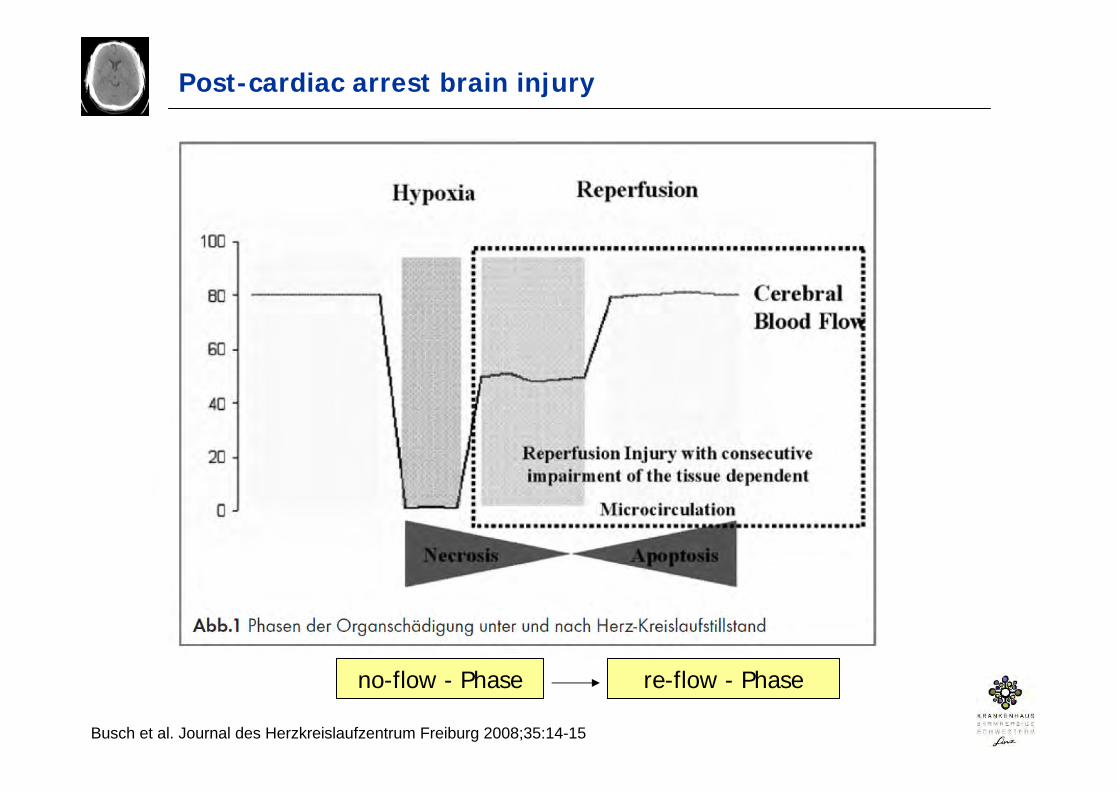
Post-cardiac arrest brain injury
no-flow - Phase re-flow - Phase
Busch et al. Journal des Herzkreislaufzentrum Freiburg 2008;35:14-15
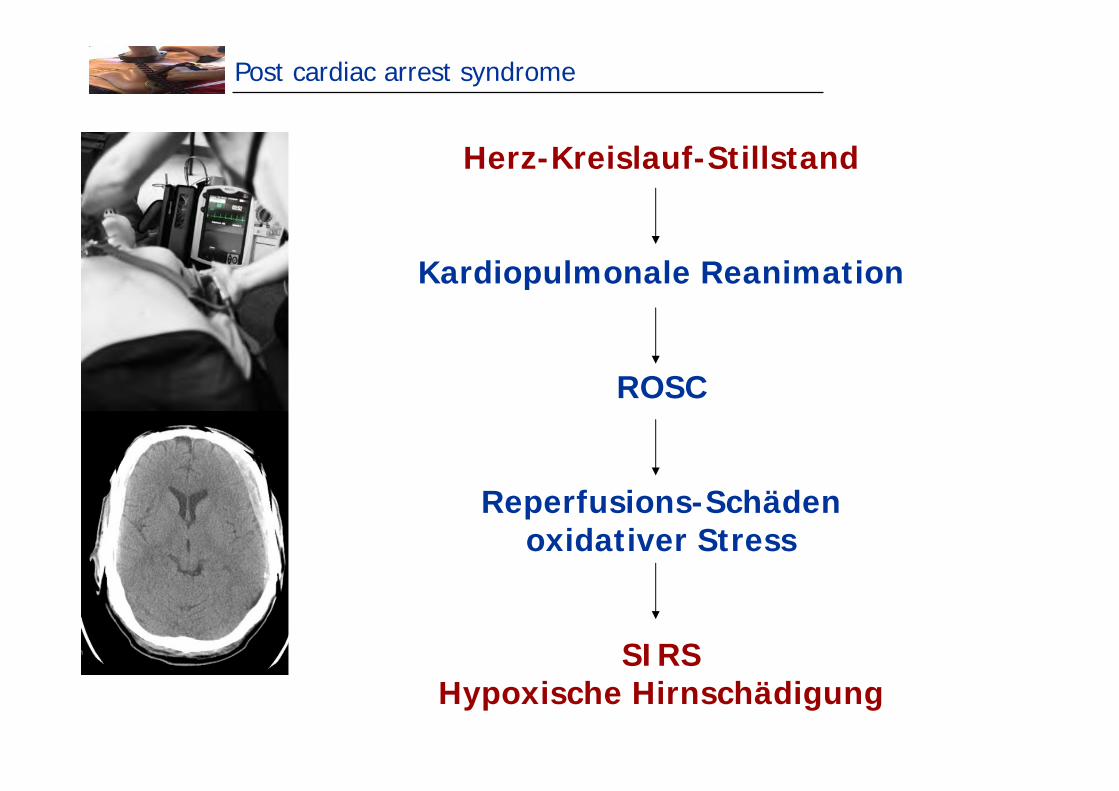
Post cardiac arrest syndrome
Herz-Kreislauf-Stillstand
Kardiopulmonale Reanimation
ROSC
Reperfusions-Schädenoxidativer Stress
SIRSHypoxische Hirnschädigung
Therapeutische Hypothermie
Therapeutische Hypothermie
Hypothermia after cardiac arrest (1)
The Hypothermia after cardiac arrest study group. N Engl J Med 2002;346(8):549-556
„Therapeutische Hypothermie in Österreich“
„Österreich hat eine lange Erfahrung mit therapeutischer Hypothermie.“
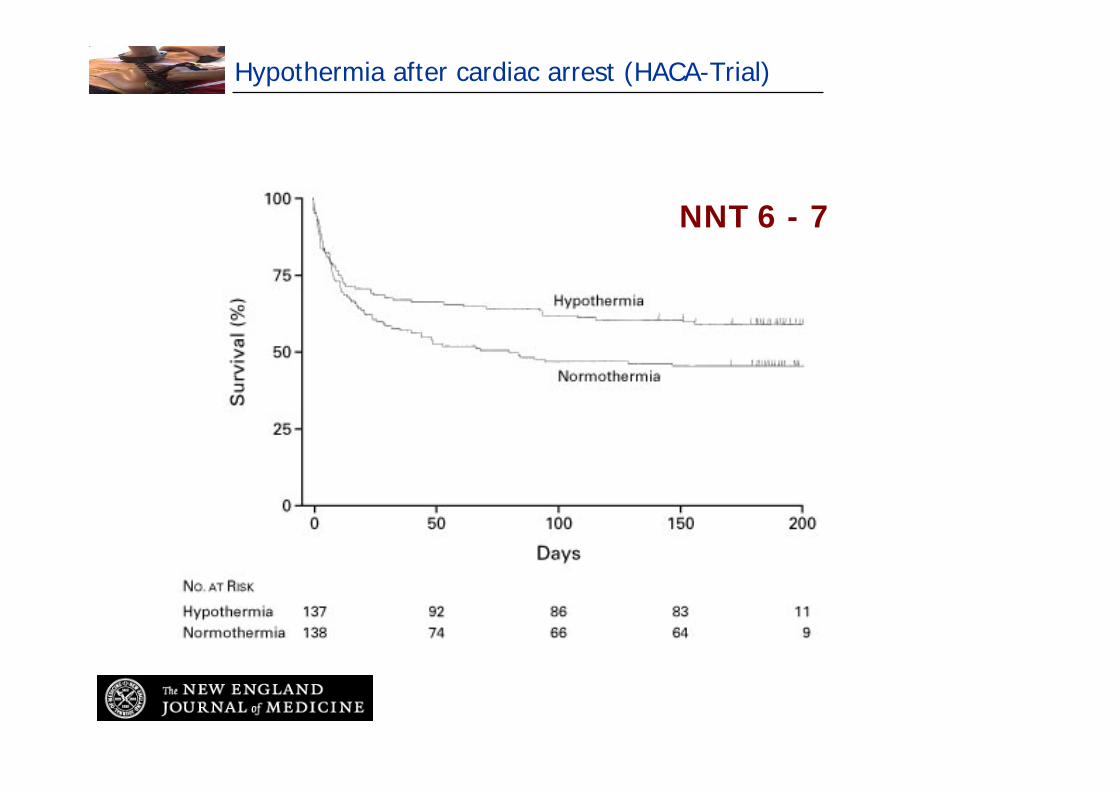
Hypothermia after cardiac arrest (HACA-Trial)
NNT 6 - 7
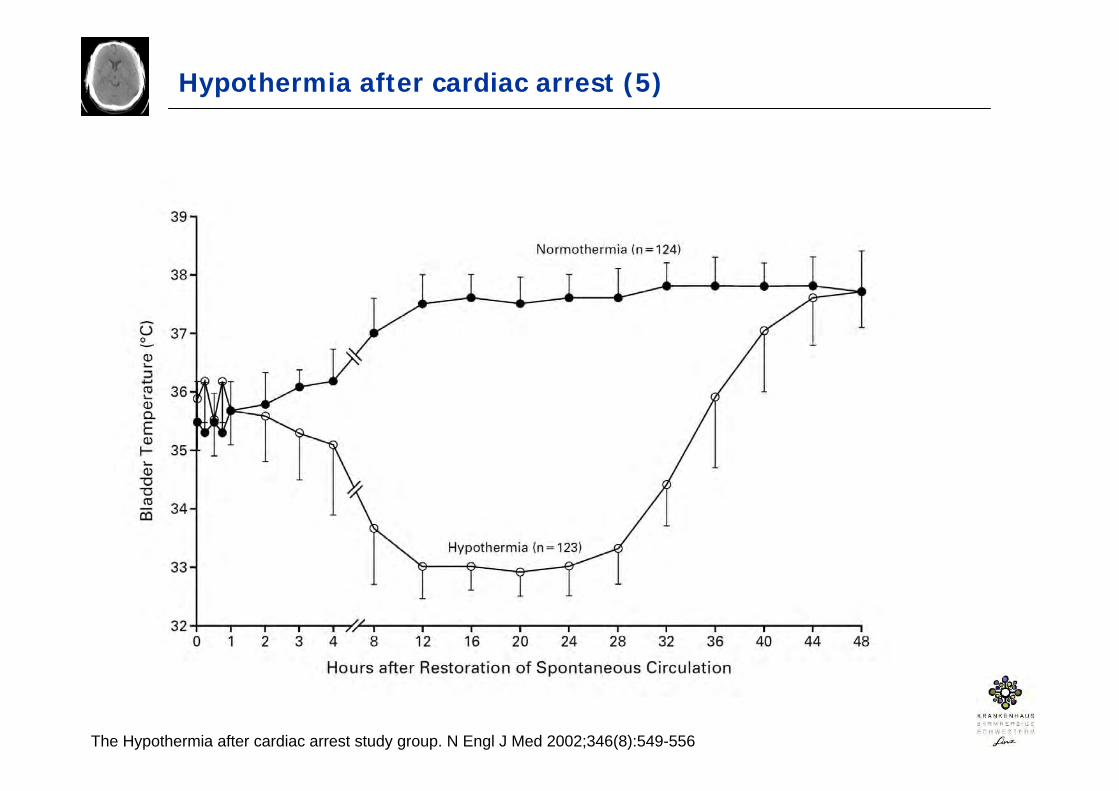
Hypothermia after cardiac arrest (5)
The Hypothermia after cardiac arrest study group. N Engl J Med 2002;346(8):549-556
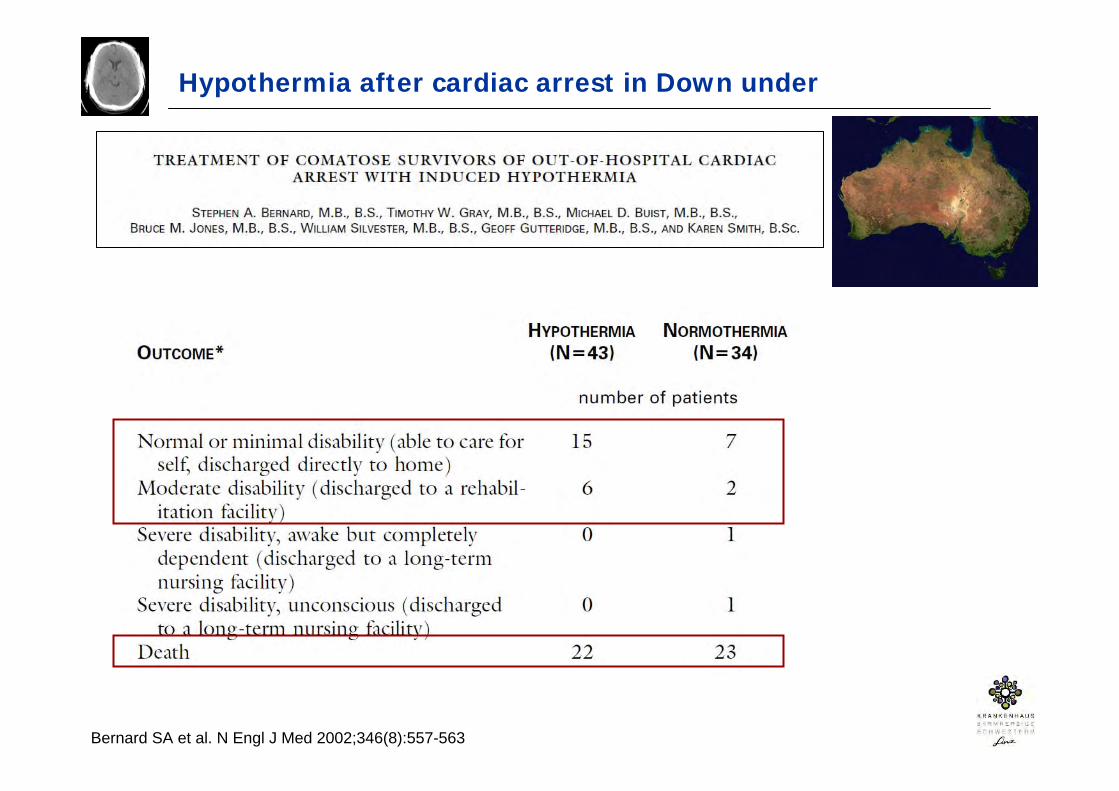
Hypothermia after cardiac arrest in Down under
Bernard SA et al. N Engl J Med 2002;346(8):557-563
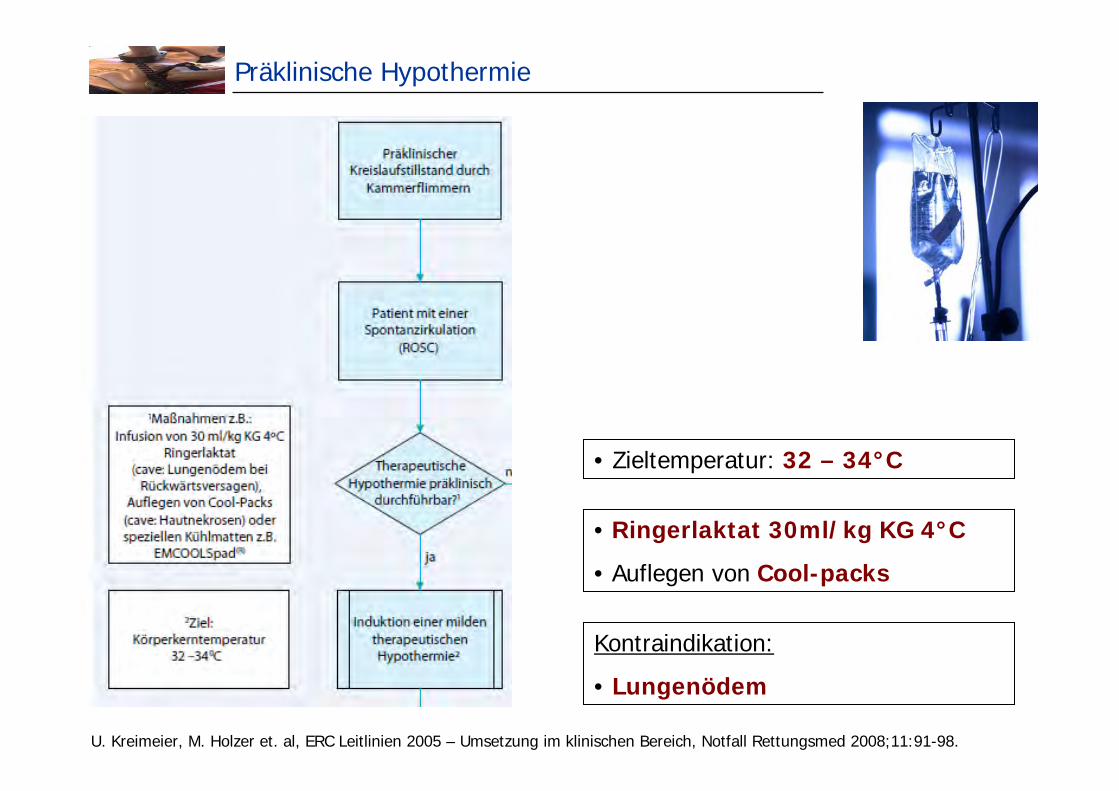
Präklinische Hypothermie
• Zieltemperatur: 32 – 34°C
• Ringerlaktat 30ml/kg KG 4°C
• Auflegen von Cool-packs
Kontraindikation:
• Lungenödem
U. Kreimeier, M. Holzer et. al, ERC Leitlinien 2005 – Umsetzung im klinischen Bereich, Notfall Rettungsmed 2008;11:91-98.
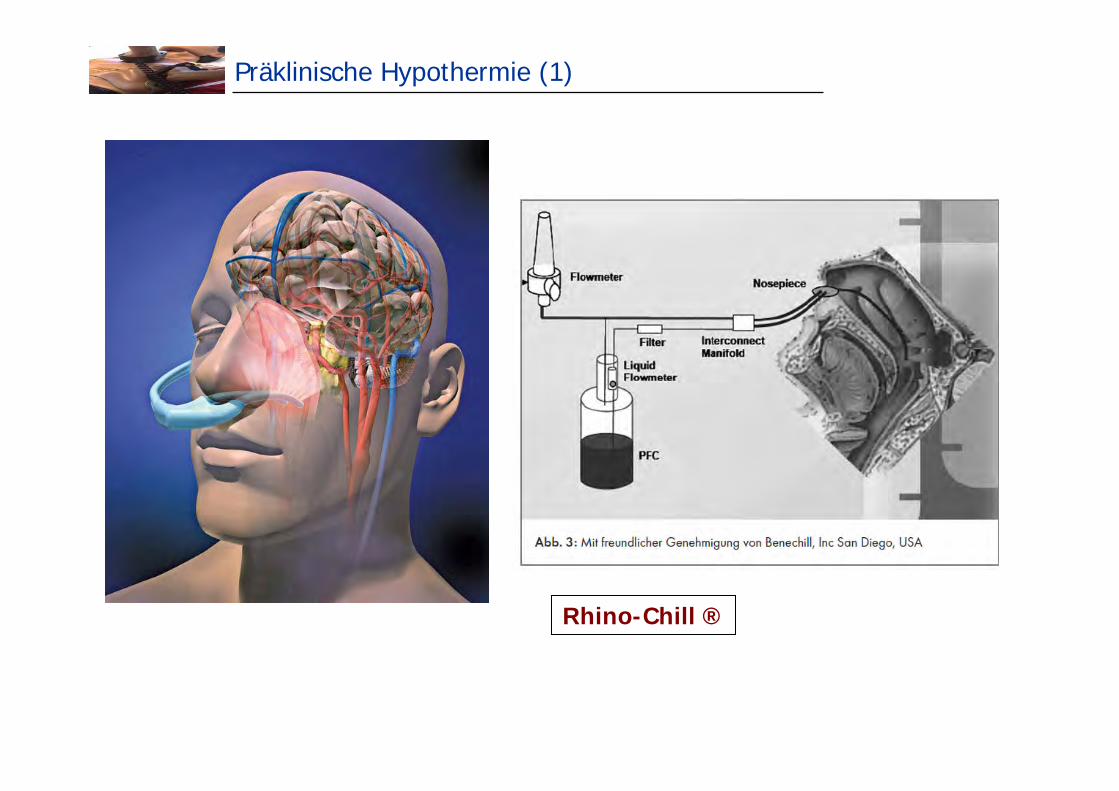
Präklinische Hypothermie (1)
Rhino-Chill ®
Präklinische Hypothermie (2)
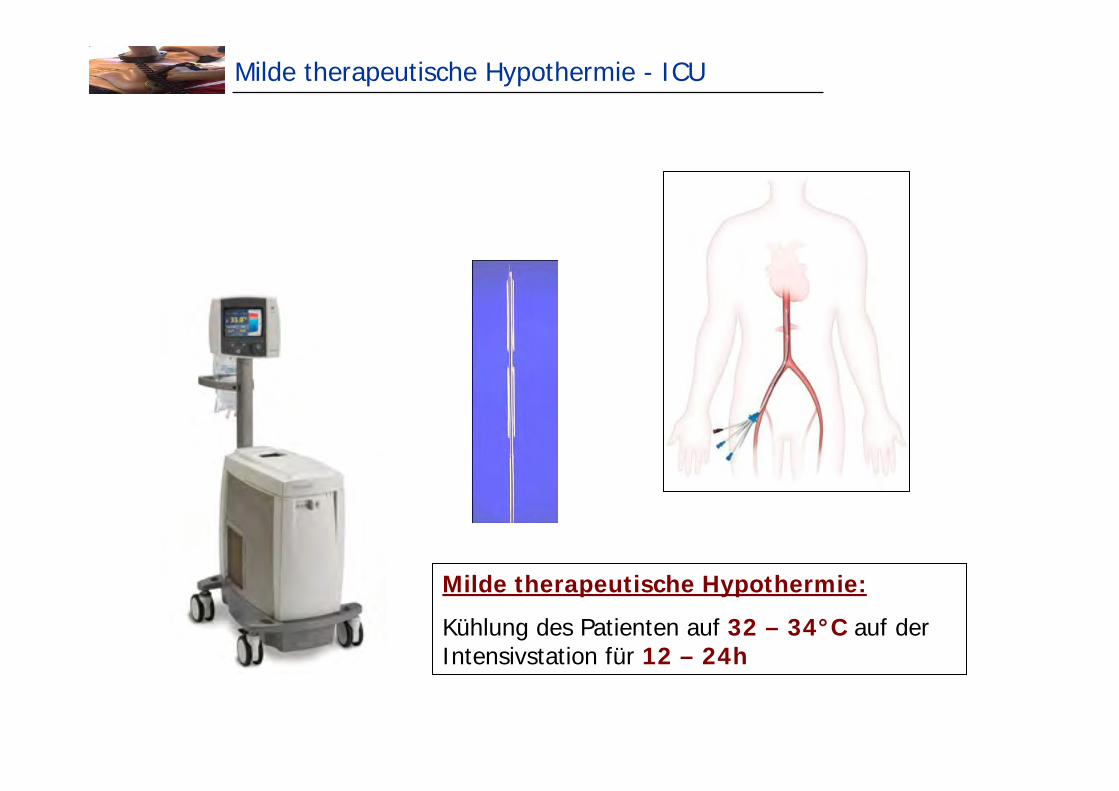
Milde therapeutische Hypothermie - ICU
Milde therapeutische Hypothermie:
Kühlung des Patienten auf 32 – 34°C auf der Intensivstation für 12 – 24h
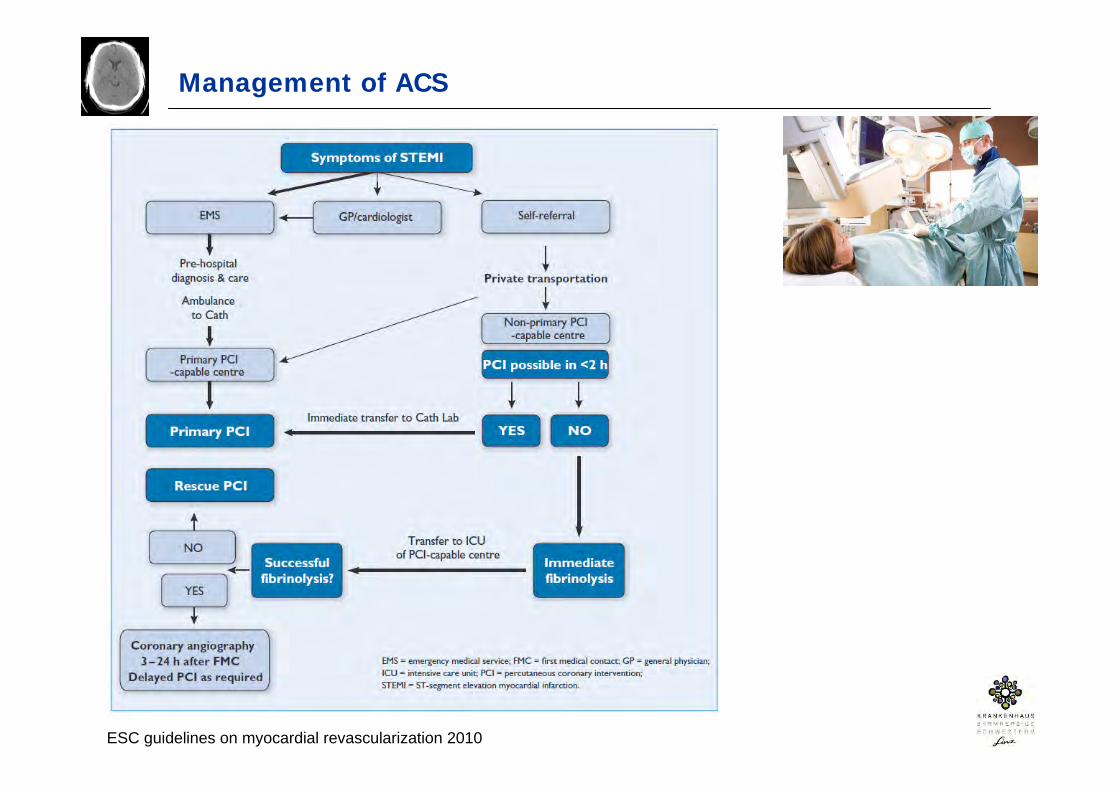
Management of ACS
ESC guidelines on myocardial revascularization 2010
Prognosebeurteilung nach CPR – klinische Untersuchung
• Klinische Untersuchung:
- Fehlen des Pupillen-Licht- und Corneal-Reflexes72h nach CPR ist ein verläßlicher Marker für ein schlechtes neurologisches Outcome
FPR 0%, 95% CI 0-9% [1]
- Fehlen des vestibulären-oculären Reflexes 24h nach CPR
FPR 0%, 95% CI 0-14% [2]
[1] Zandbergen EG et al. Prediction of poor outcome within the first 3 days of postanoxic coma. Neurology 2006;66:62-8
[2] Young GB et al. Anoxic-ischemic encephalopathy: clinical and electrophysiological associations with outcome. Neurocrit Care 2005;2:159-64
Prognosebeurteilung nach CPR – biochemische Marker
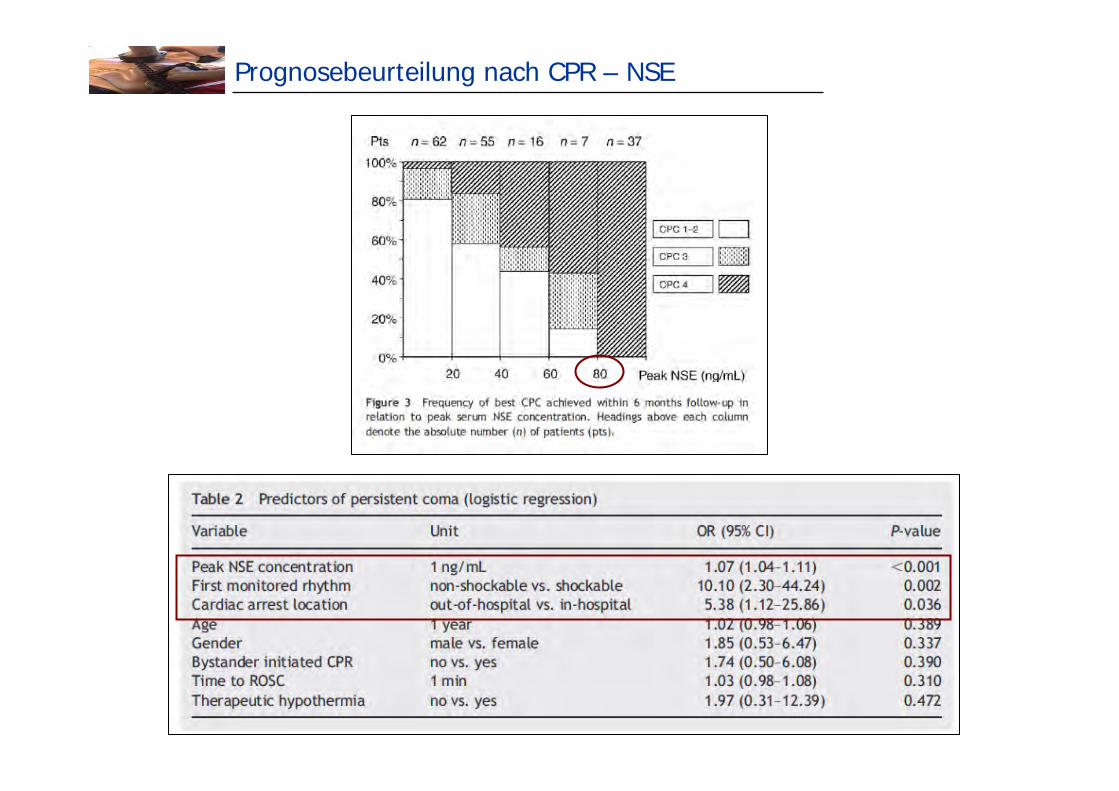
Prognosebeurteilung nach CPR – NSE
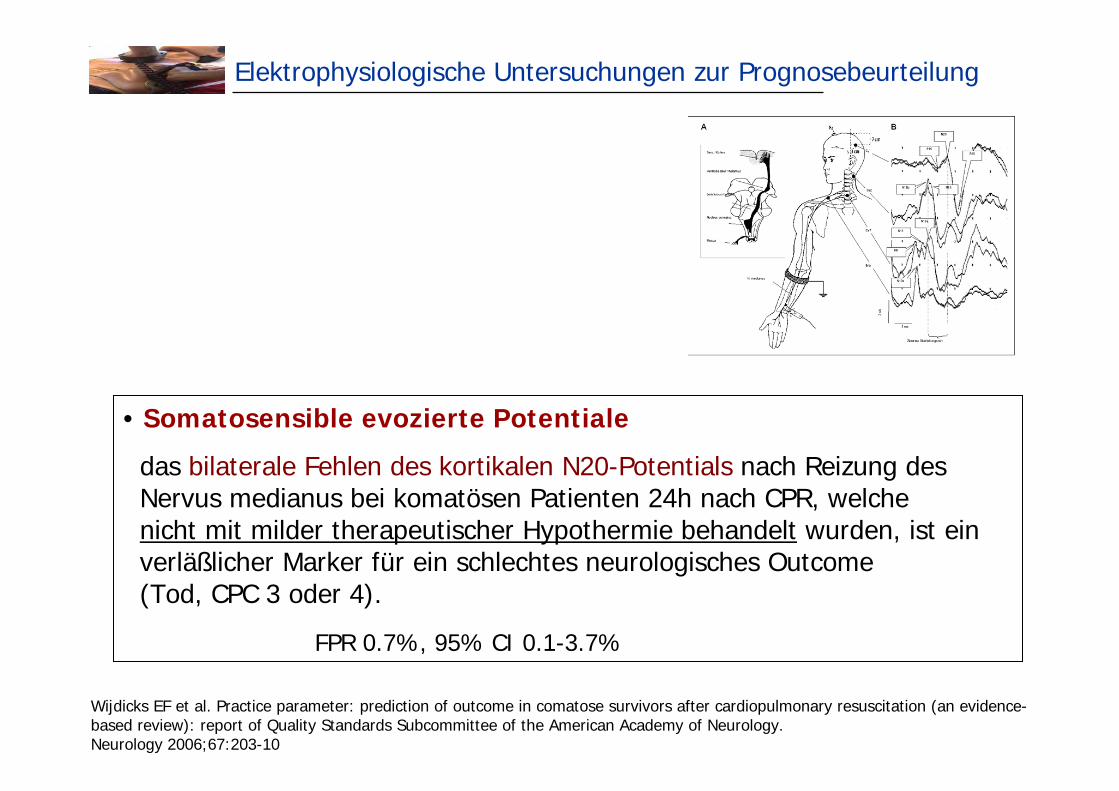
Elektrophysiologische Untersuchungen zur Prognosebeurteilung
• Somatosensible evozierte Potentiale
das bilaterale Fehlen des kortikalen N20-Potentials nach Reizung des Nervus medianus bei komatösen Patienten 24h nach CPR, welche nicht mit milder therapeutischer Hypothermie behandelt wurden, ist ein verläßlicher Marker für ein schlechtes neurologisches Outcome (Tod, CPC 3 oder 4).
FPR 0.7%, 95% CI 0.1-3.7%
Wijdicks EF et al. Practice parameter: prediction of outcome in comatose survivors after cardiopulmonary resuscitation (an evidence-based review): report of Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2006;67:203-10

Überlebensraten nach kardiopulmonaler Reanimation weltweit
Berdowski J et al. Global incidences of out-of-hospital cardiac arrest and survival rates: Systematic review of 67 prospective studies. Resuscitation 2010 Nov;81(11):1479-87
Überlebensraten zum Zeitpunkt der KH-Entlassungbei prähospitalem Herz-Kreislauf-Stillstand weltweit
Nord-Amerika 6%
Europa 9%
Australien 11%
Asien 2%
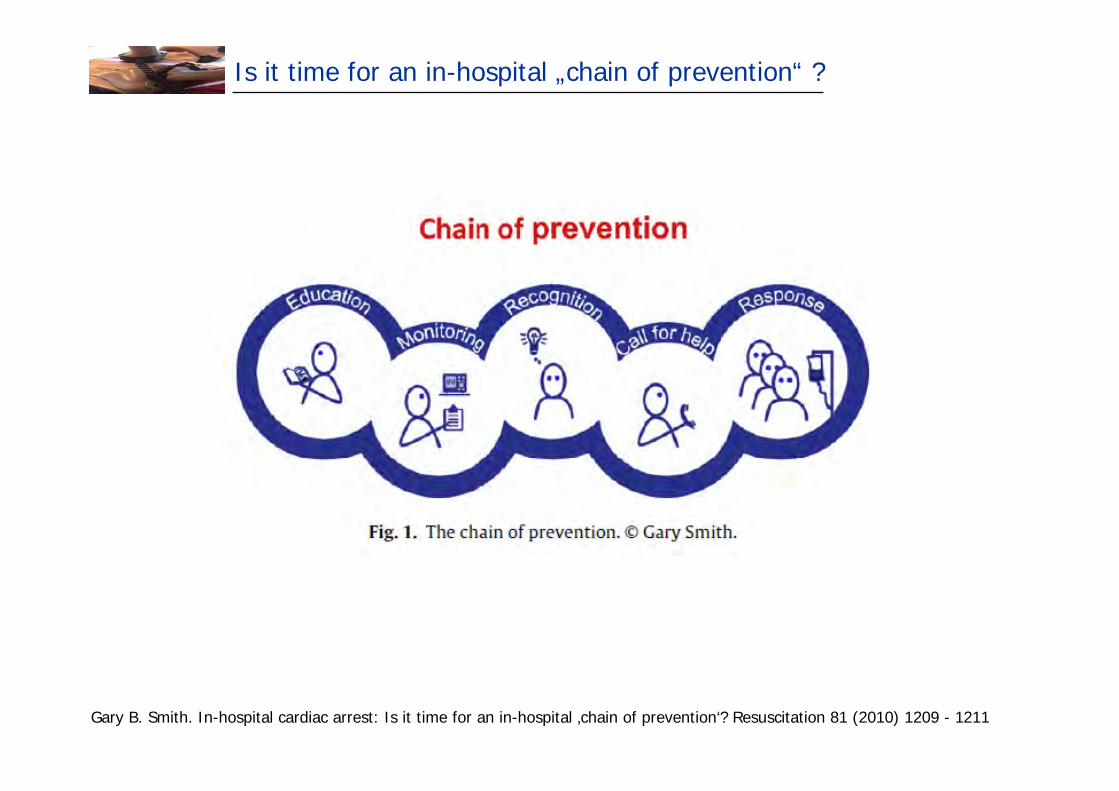
Is it time for an in-hospital „chain of prevention“ ?
Gary B. Smith. In-hospital cardiac arrest: Is it time for an in-hospital ‚chain of prevention‘? Resuscitation 81 (2010) 1209 - 1211
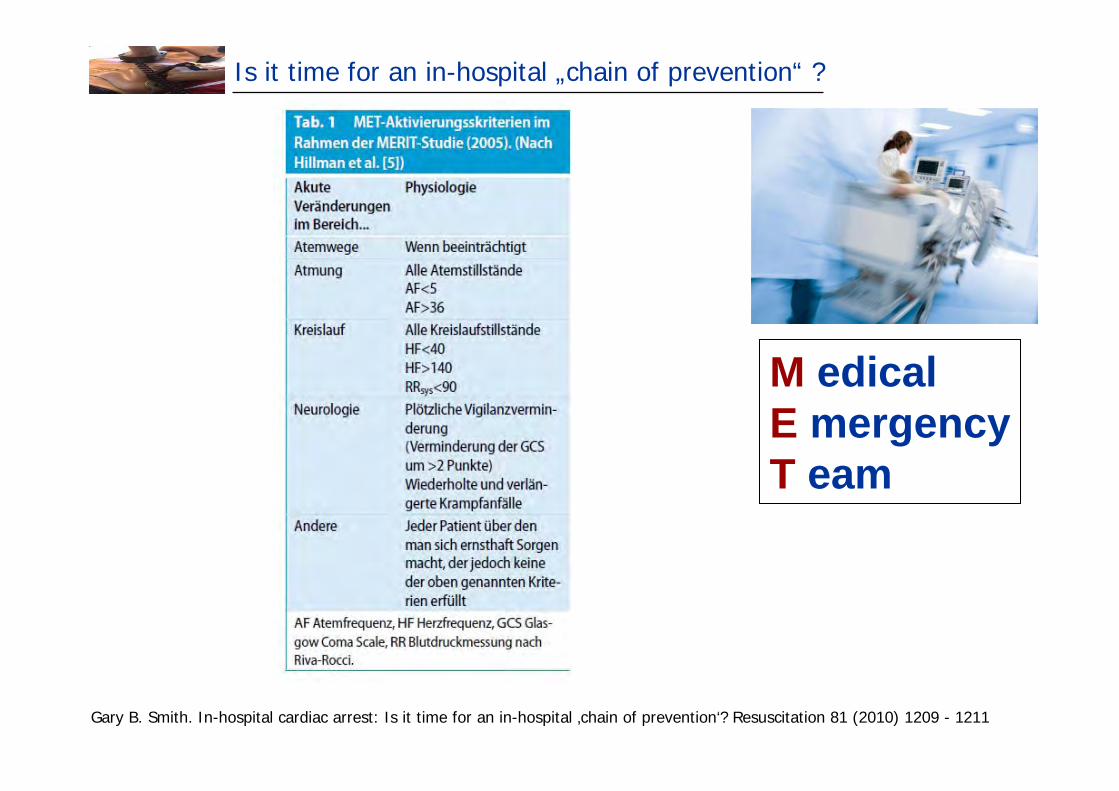
Is it time for an in-hospital „chain of prevention“ ?
Gary B. Smith. In-hospital cardiac arrest: Is it time for an in-hospital ‚chain of prevention‘? Resuscitation 81 (2010) 1209 - 1211
M edicalE mergencyT eam
Zusammenfassung – JUST DO IT
• Herzdruckmassage
• Herzdruckmassage
• Herzdruckmassage
• 30 HDM : 2 Beatmungen
• bei VFib/VT Defibrillation
• Prä-Schock Pausen kurz halten
• Intubation zur Atemwegssicherung
• alternative supraglottische Atemwegssicherung erwägen
• Hyperventilation vermeiden
• Medikamente- VFib/VT: Adrenalin, Amiodaron- Asystolie: Adrenalin
• prä- u. innerklinische Hypothermie

Herzlichen Dank für die Aufmerksamkeit
Weitere Informationen u. Kurse
CPR guidelines 2010 Download unter www.CPRguidelines.eu
ALS-Kurse des Austrian Resuscitation Council www.arc.or.at
ERC Advanced Life Support Kurs

Plötzliche Herztod
Zheng ZJ et al. Sudden cardiac death in the United States, 1989 – 1998. Circulation 2001;104:2158-76
Der plötzliche Herztod ist für mehr als 60% der Todesfälle bei Erwachsenen mit koronarer Herzerkrankung verantwortlich.
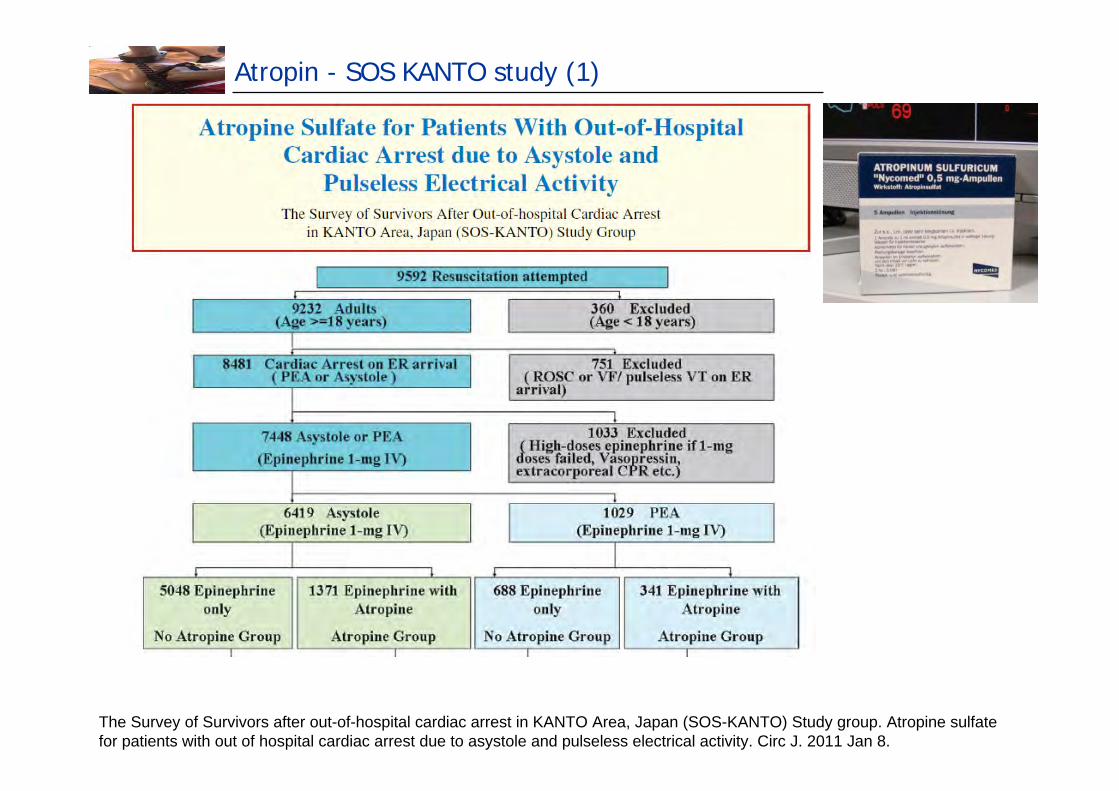
Atropin - SOS KANTO study (1)
The Survey of Survivors after out-of-hospital cardiac arrest in KANTO Area, Japan (SOS-KANTO) Study group. Atropine sulfate for patients with out of hospital cardiac arrest due to asystole and pulseless electrical activity. Circ J. 2011 Jan 8.
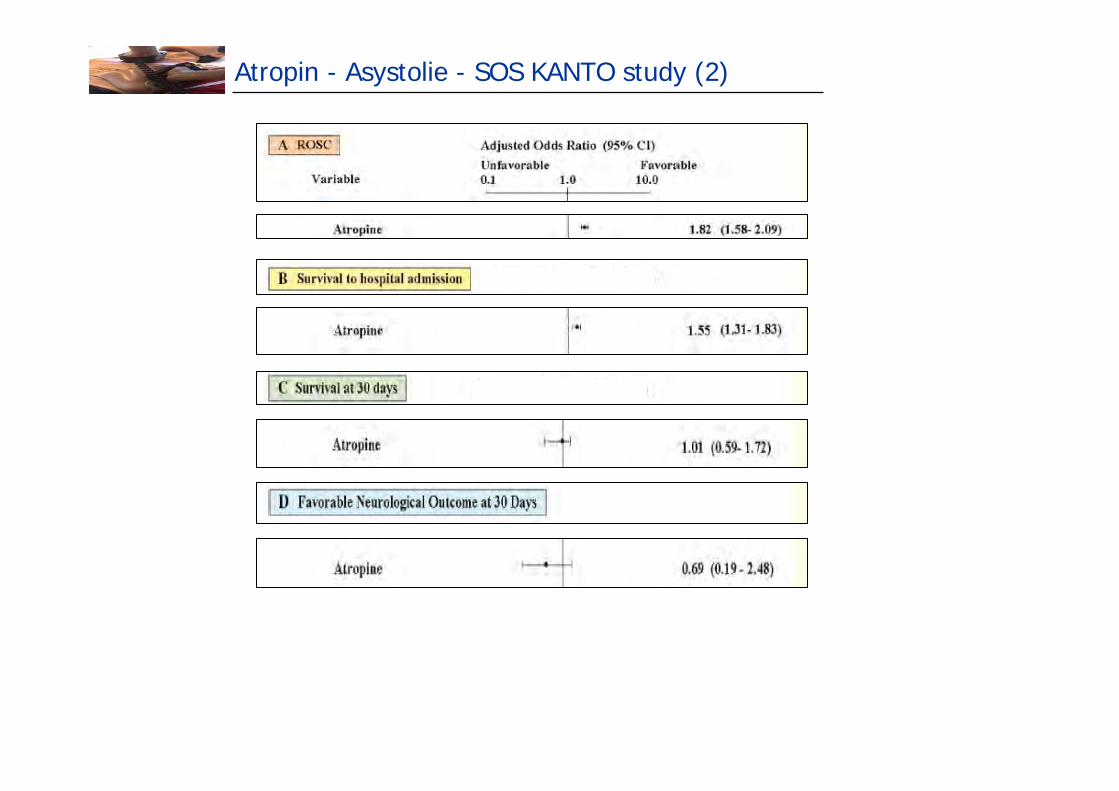
Atropin - Asystolie - SOS KANTO study (2)
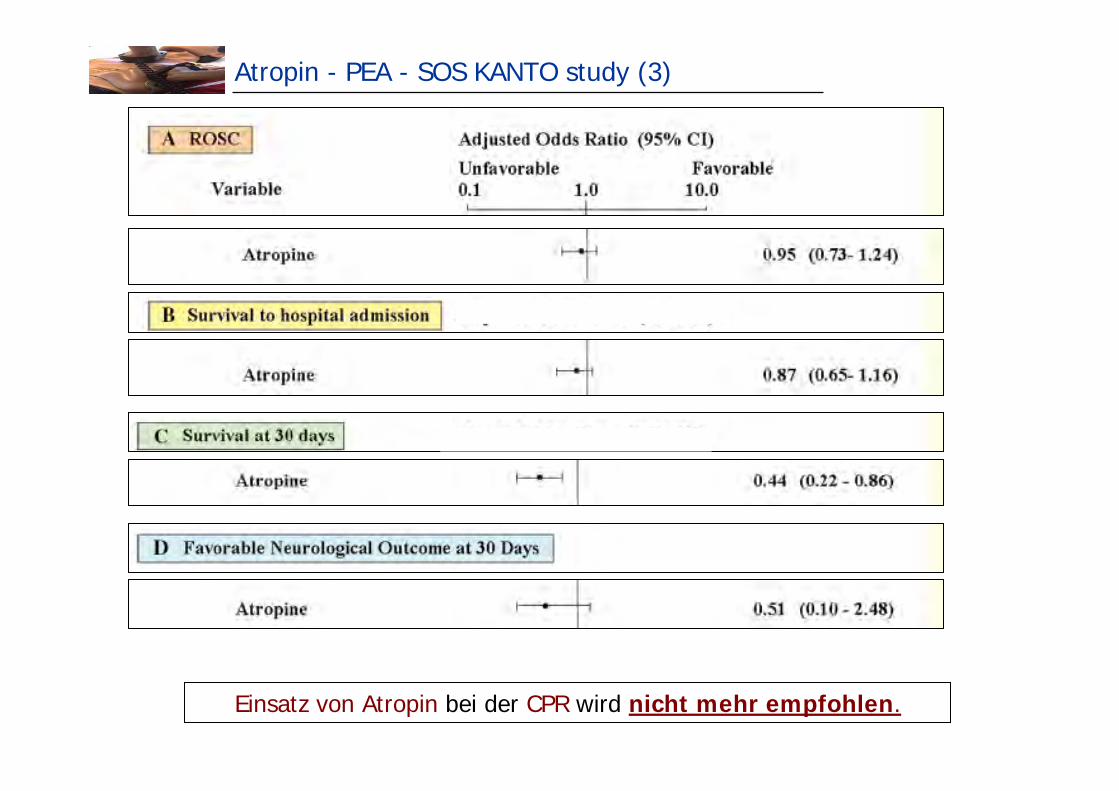
Atropin - PEA - SOS KANTO study (3)
Einsatz von Atropin bei der CPR wird nicht mehr empfohlen.
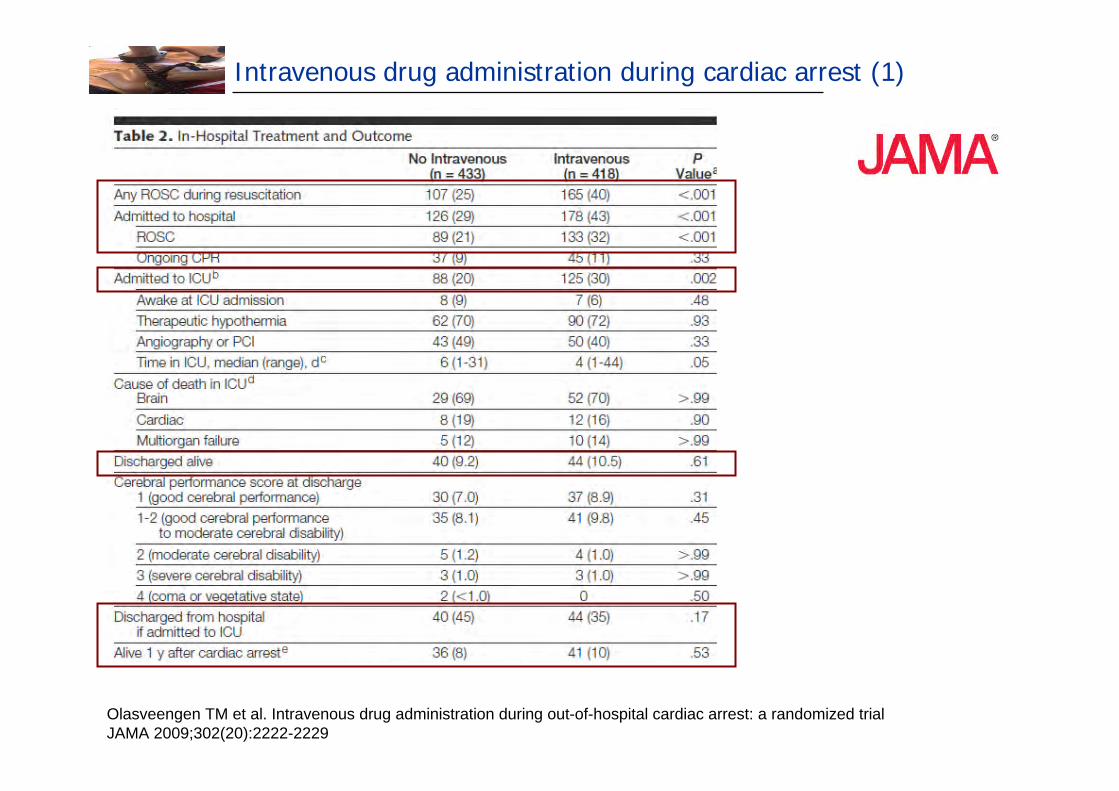
Intravenous drug administration during cardiac arrest (1)
Olasveengen TM et al. Intravenous drug administration during out-of-hospital cardiac arrest: a randomized trialJAMA 2009;302(20):2222-2229
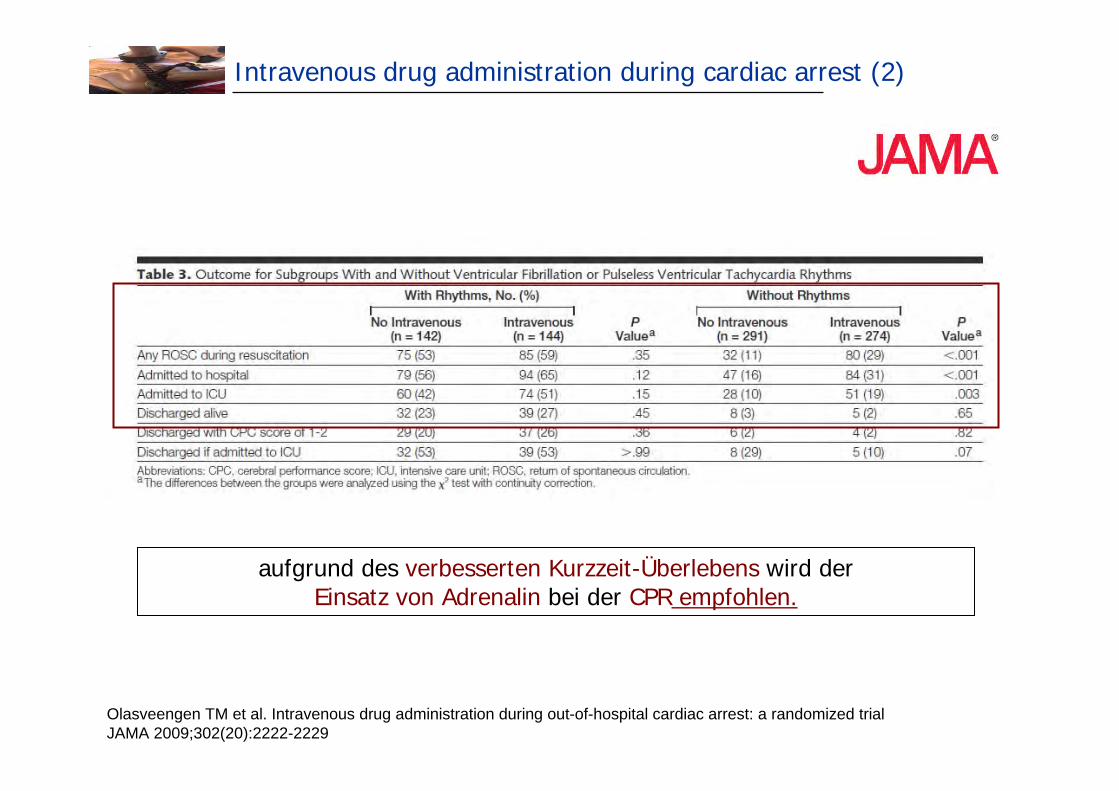
Intravenous drug administration during cardiac arrest (2)
aufgrund des verbesserten Kurzzeit-Überlebens wird derEinsatz von Adrenalin bei der CPR empfohlen.
Olasveengen TM et al. Intravenous drug administration during out-of-hospital cardiac arrest: a randomized trialJAMA 2009;302(20):2222-2229
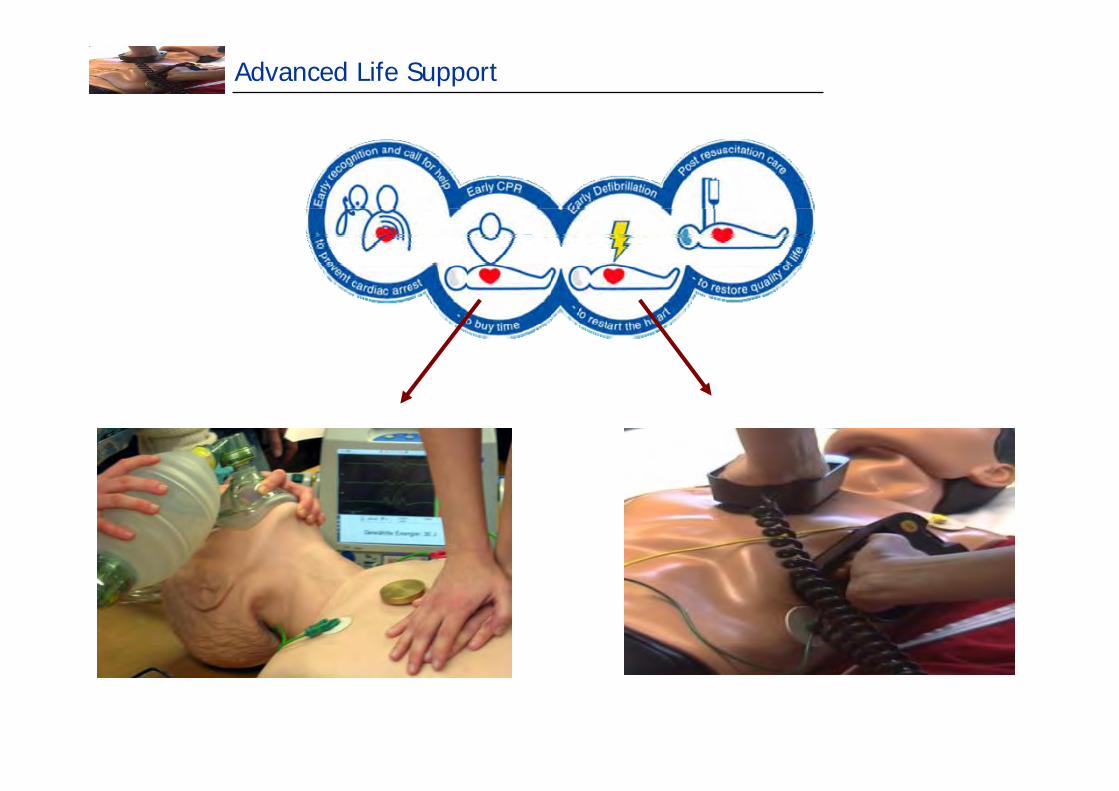
Advanced Life Support

Präkordialer Faustschlag
Indikation:
unmittelbar nach beobachtetem u. monitorüberwachter Herz-Kreislauf-Stillstand
+ pulsloser VT / VF
+ kein Defibrillator sofort verfügbar
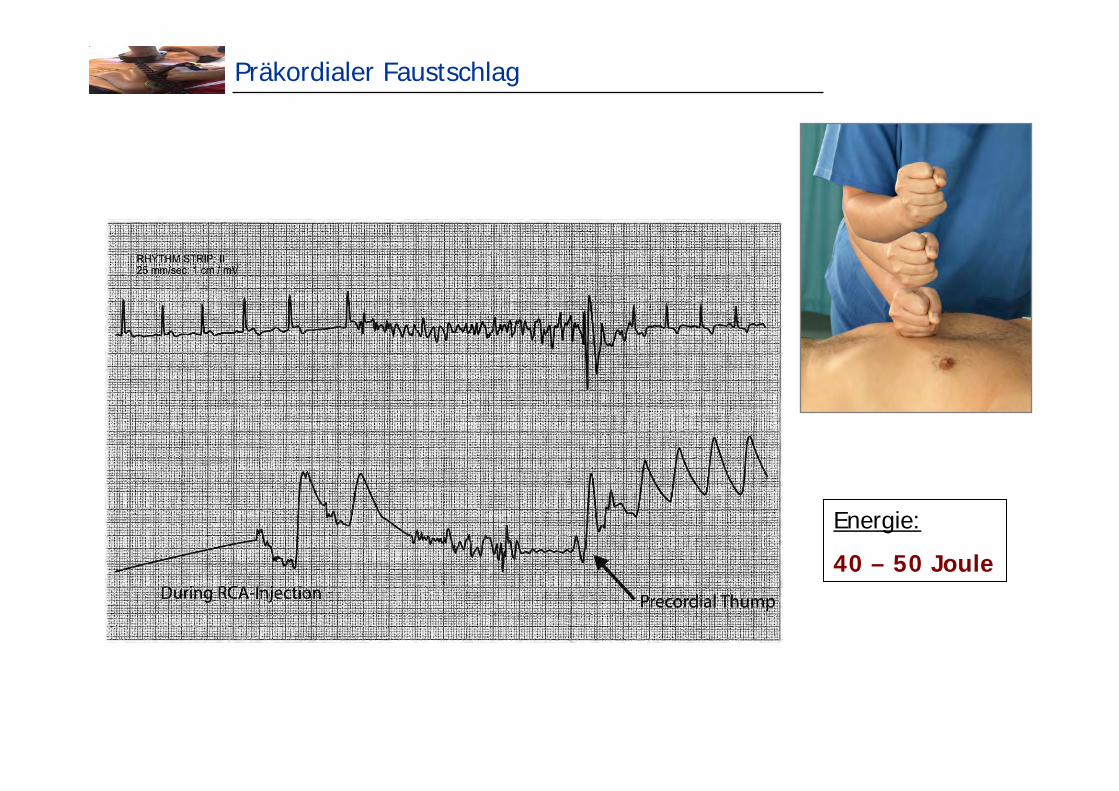
Präkordialer Faustschlag
Energie:
40 – 50 Joule
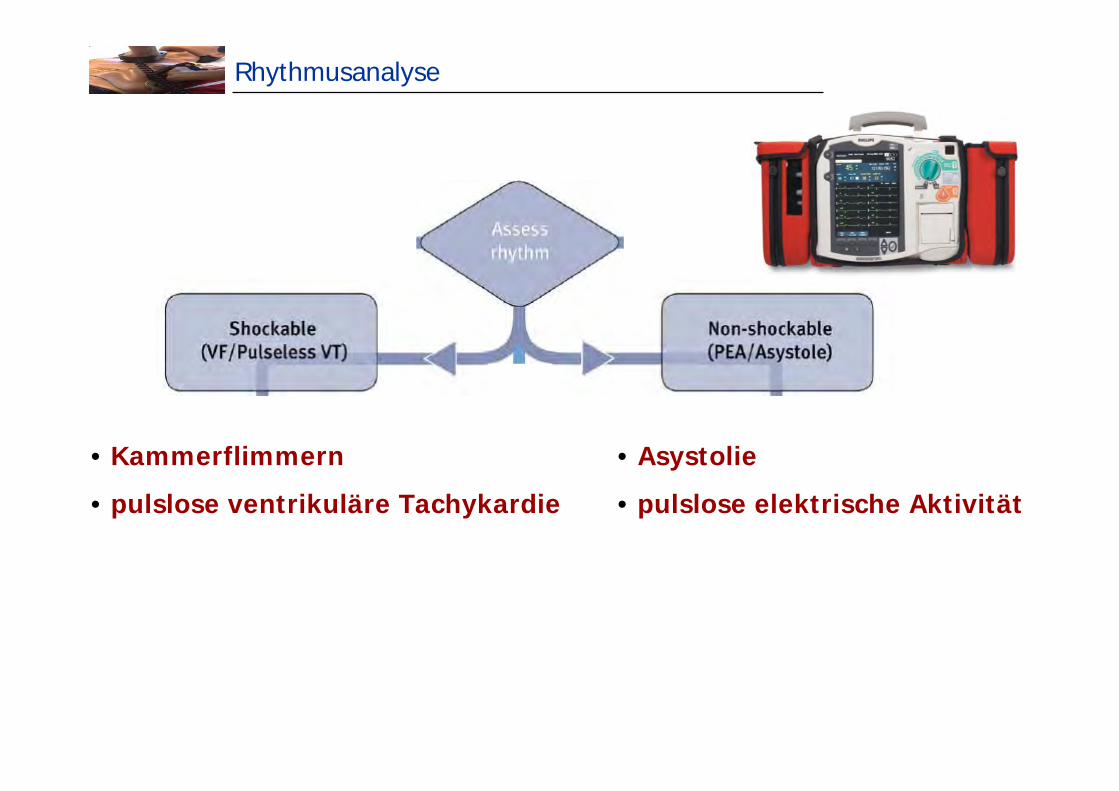
Rhythmusanalyse
• Kammerflimmern
• pulslose ventrikuläre Tachykardie
• Asystolie
• pulslose elektrische Aktivität
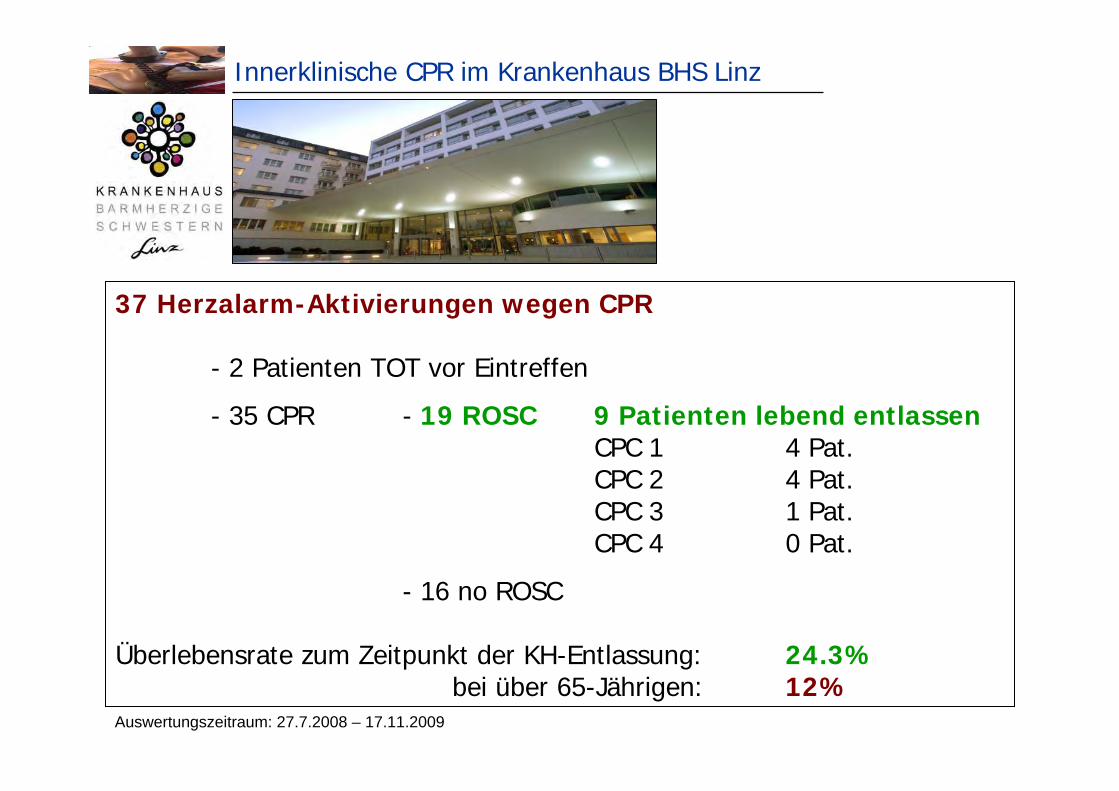
Innerklinische CPR im Krankenhaus BHS Linz
Auswertungszeitraum: 27.7.2008 – 17.11.2009
37 Herzalarm-Aktivierungen wegen CPR
- 2 Patienten TOT vor Eintreffen
- 35 CPR - 19 ROSC 9 Patienten lebend entlassenCPC 1 4 Pat.CPC 2 4 Pat.CPC 3 1 Pat.CPC 4 0 Pat.
- 16 no ROSC
Überlebensrate zum Zeitpunkt der KH-Entlassung: 24.3%bei über 65-Jährigen: 12%
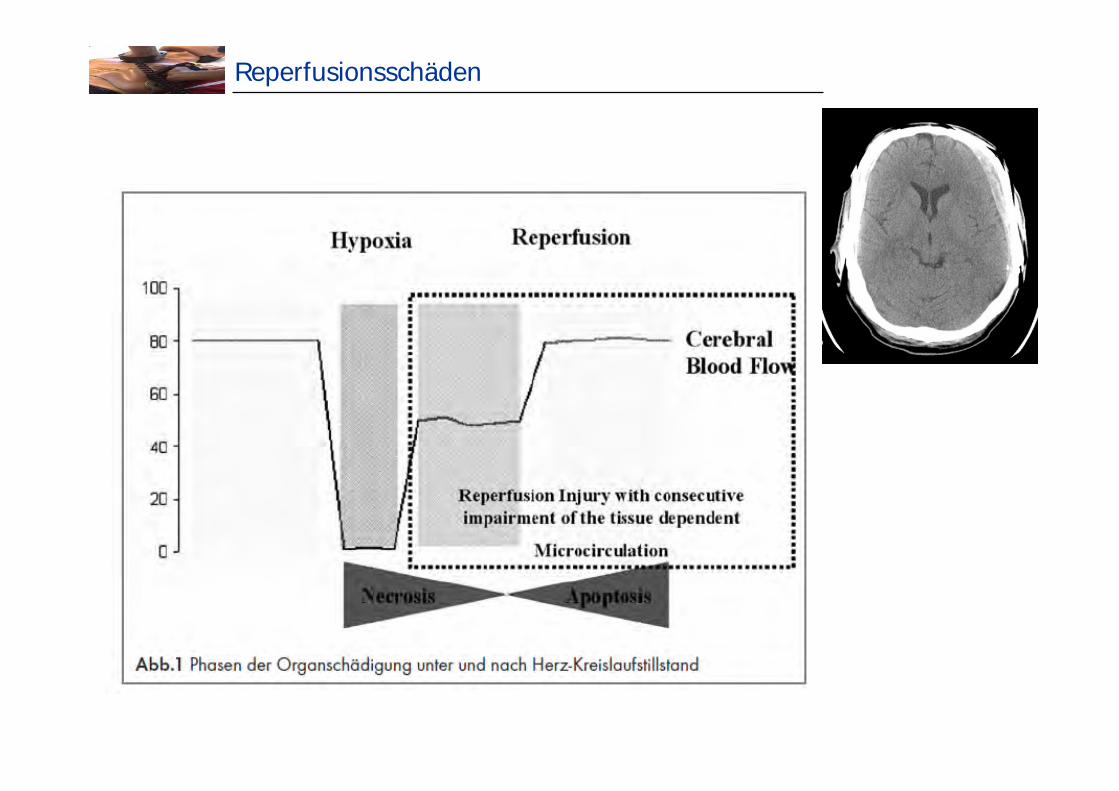
Reperfusionsschäden

Aktuelle Guidelines der kardiopulmonalen Reanimation
Daniel KiblböckInterne II - Kardiologie

„Alternative“ präklinische Hypothermie
Milde therapeutische Hypothermie
Wann ?
Wie ?
Warum ?
Milde therapeutische Hypothermie
NEJM 2002;346:549-556
NEJM 2002;346:557-563
ILCOR Consensus 2010
AustralianResuscitation
Council
ResuscitationCouncil ofAsia
International Liaison Committee on Resuscitation
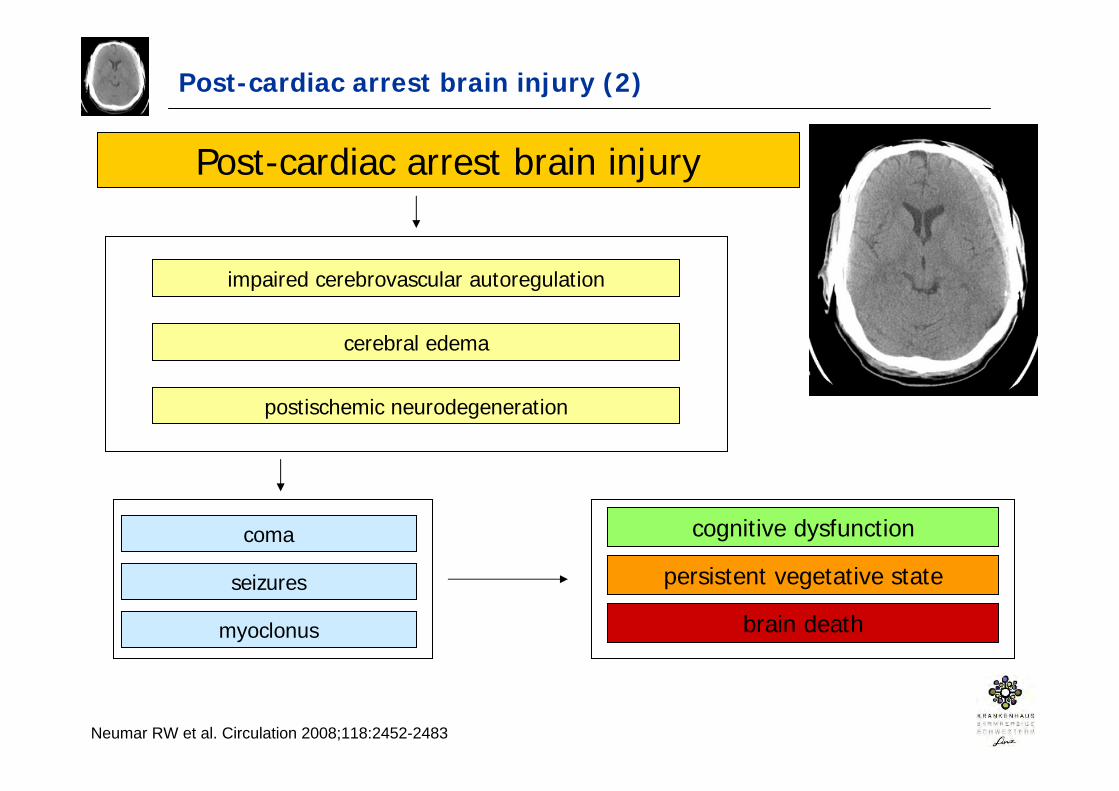
Post-cardiac arrest brain injury (2)
Neumar RW et al. Circulation 2008;118:2452-2483
Post-cardiac arrest brain injury
impaired cerebrovascular autoregulation
cerebral edema
postischemic neurodegeneration
coma
seizures
myoclonus
cognitive dysfunction
persistent vegetative state
brain death
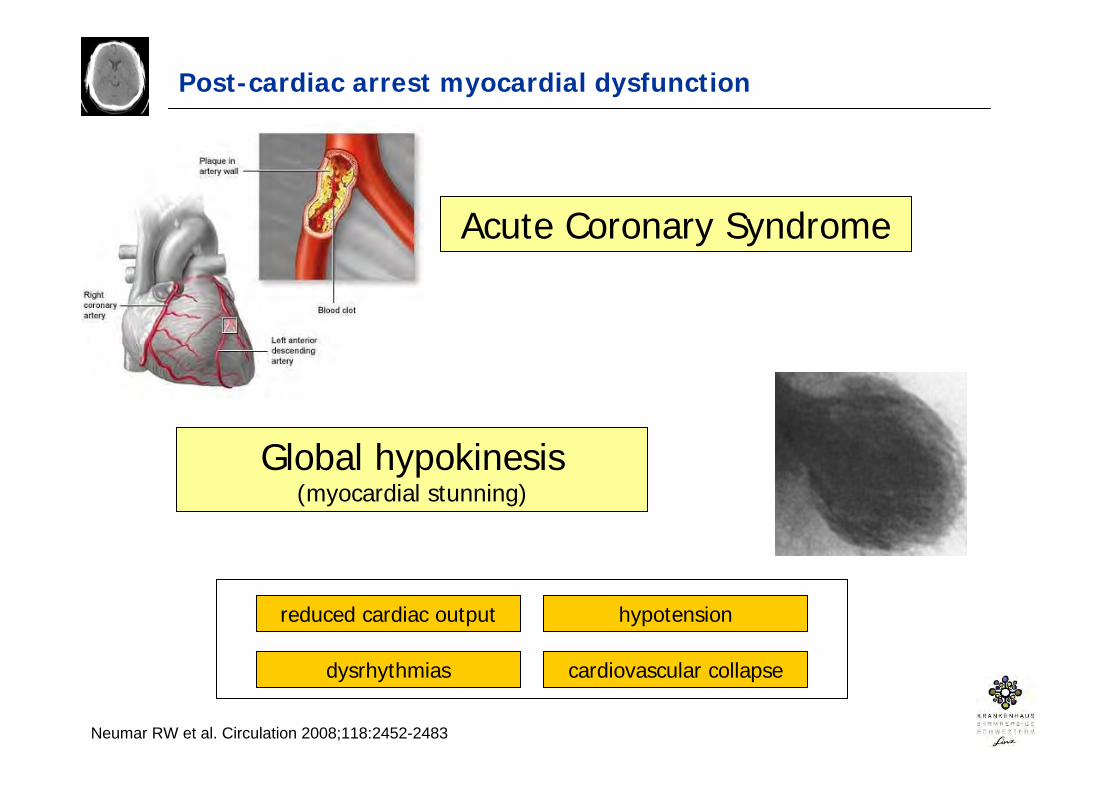
Post-cardiac arrest myocardial dysfunction
Acute Coronary Syndrome
Global hypokinesis(myocardial stunning)
Neumar RW et al. Circulation 2008;118:2452-2483
reduced cardiac output hypotension
dysrhythmias cardiovascular collapse
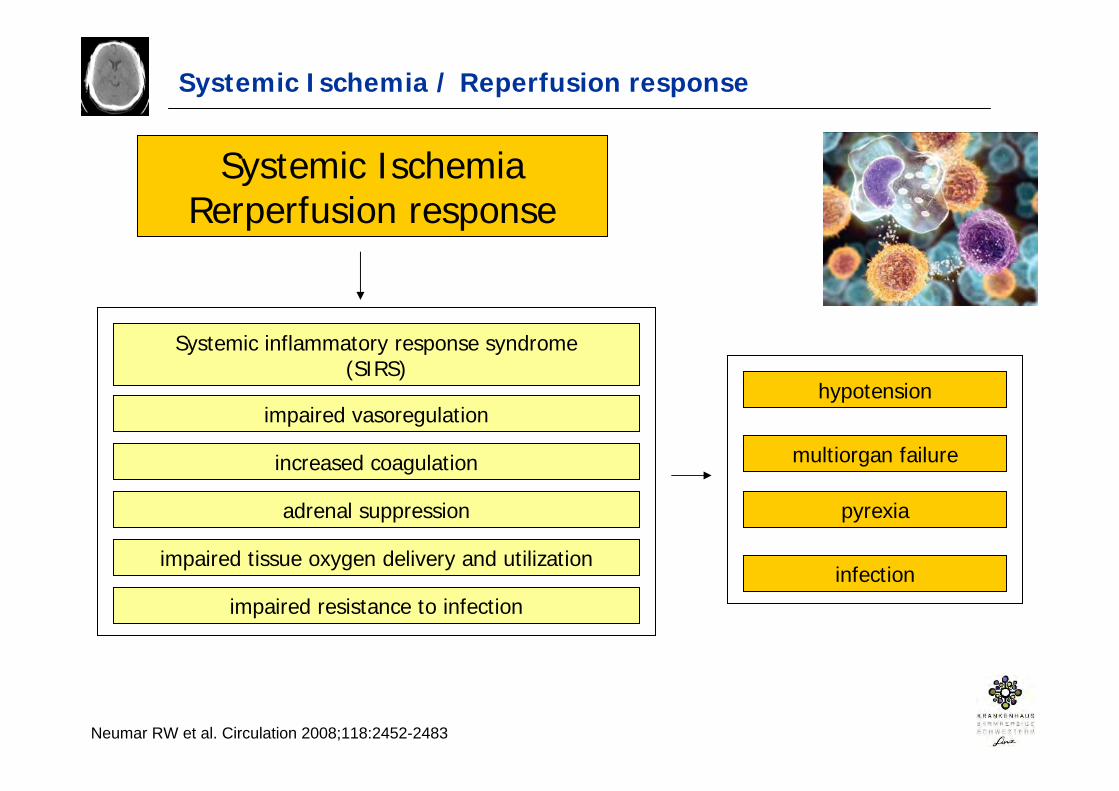
Systemic Ischemia / Reperfusion response
Systemic IschemiaRerperfusion response
Systemic inflammatory response syndrome(SIRS)
Neumar RW et al. Circulation 2008;118:2452-2483
impaired vasoregulation
increased coagulation
adrenal suppression
impaired tissue oxygen delivery and utilization
impaired resistance to infection
hypotension
multiorgan failure
pyrexia
infection
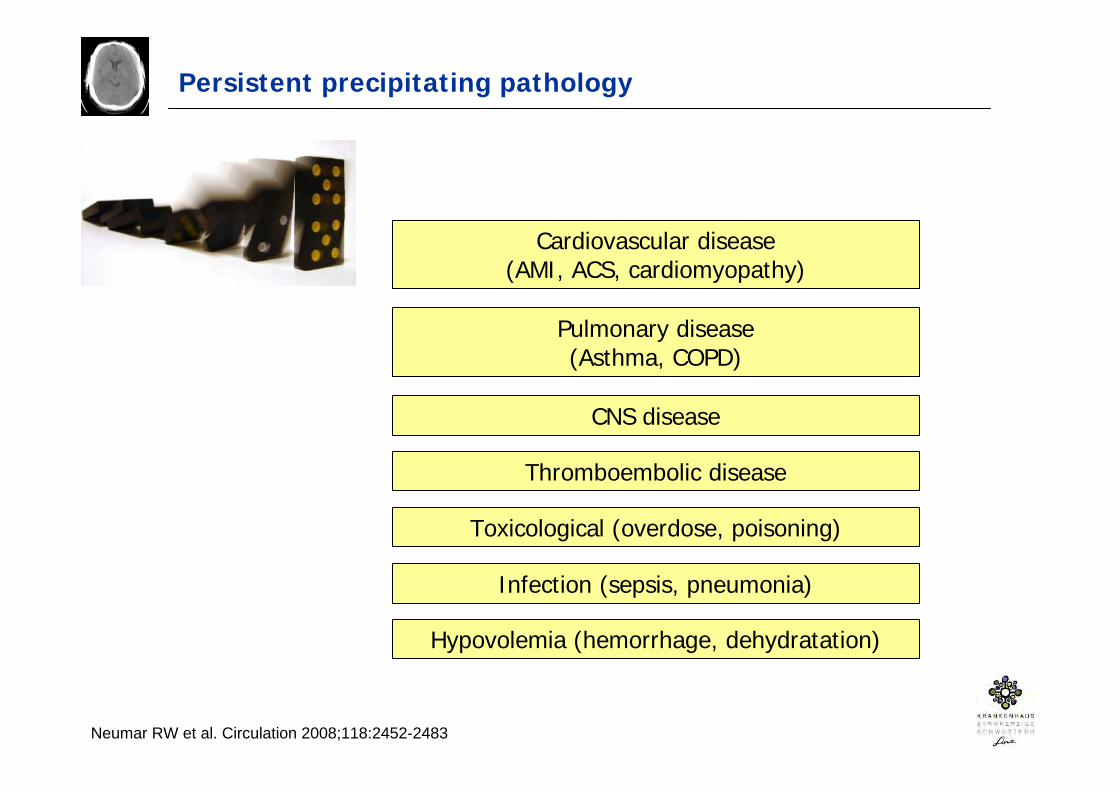
Persistent precipitating pathology
Cardiovascular disease(AMI, ACS, cardiomyopathy)
Pulmonary disease(Asthma, COPD)
CNS disease
Thromboembolic disease
Toxicological (overdose, poisoning)
Infection (sepsis, pneumonia)
Hypovolemia (hemorrhage, dehydratation)
Neumar RW et al. Circulation 2008;118:2452-2483

Kardiovaskuläre Erkrankungen in Europa
Sans S et al. The burden of cardiovascular diseases mortality in Europe. Task force of the European Society of Cardiology on cardiovascular mortality and morbidity statistics in Europe. Eur Heart K 1997;18:1231-48
In Europa sind 40% aller Todesfälle bei unter 75-Jährigen durch kardiovaskuläre Erkrankungen bedingt.




![Evaluation der Kernspintomographie zur Verlaufsbeobachtung ... · therapeutischer Effekte zu entwickeln wie den Bath Ankylosing Spondylitis Radiology Index (BASRI) [54], schlug aufgrund](https://img.pdfslide.net/doc/110x75/5d4d07a188c9932c688b909e/evaluation-der-kernspintomographie-zur-verlaufsbeobachtung-therapeutischer.jpg)
























