Embed Size (px)
Citation preview

CHAPTER 21
Allopurinol and Other Inhibitors of Urate Synthesis
GERTRUDE B. ELION
A. Introduction
The ideal drug for the treatment of hyperuricemia would be one which reduces uric acid synthesis without interfering with important anabolic pathways or normal regulatory functions. In theory, uric acid production may be inhibited at a number of different enzymatic steps, either those involved in the de novo pathway of purine biosynthesis or those concerned with the final stages of purine catabolism. Compounds such as azaserine and diazo-oxo-norleucine which block the early steps of purine biosynthesis reduce uric acid synthesis but also interfere with nucleic acid synthesis and are therefore cytotoxic (GRAYZEL et aI., 1960; ZUCKERMAN et aI., 1959). Inhibition of xanthine oxidase, on the other hand, has proven to be a clinically safe and effective method of reducing uric acid formation.
Although xanthine oxidase has long been known to oxidize hypoxanthine and xanthine to uric acid, it has not always been apparent that the bulk of uric acid production in man involves this enzyme. Indeed, the discovery that inosinate was the first purine synthesized de novo (BUCHANAN et aI., 1957) suggested the possibility that the conversion of hypoxanthine to xanthine to uric acid might occur at the ribonucleoside or ribonucleotide level (GREENBERG, 1957). The finding that patients with congenital xanthinuria lacked xanthine oxidase (WATTS et aI., 1964), although they apparently could convert inosinate to xanthylate via the enzyme inosinate dehydrogenase, focused attention on the importance of xanthine oxidase in uric acid production. It was open to question, however, whether or not xanthine oxidase inhibition could be achieved in vivo. WESTERFELD et ai. (1959) had succeeded in inhibiting xanthine oxidase in rats only with toxic levels of carbonyl reagents. Moreover, a pteridine which was a potent xanthine oxidase inhibitor in vitro failed to give any inhibition in vivo (BYERS, 1952).
Allopurinol (4-hydroxypyrazolo(3,4-d}pyrimidine) was chosen for in vivo studies of xanthine oxidase inhibition because it was a potent inhibitor of the enzyme in vitro, was relatively nontoxic, and did not appear to interfere with anabolic processes within the cell, as judged by its lack of inhibition of the growth of bacteria or tumors (ELION et aI., 1963). In this chapter allopurinol and its oxidation product, oxipurinol, will be discussed together for reasons which will be apparent. Other xanthine oxidase inhibitors will be discussed as well.
B. Inhibition of Xanthine Oxidase In Vitro
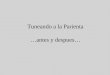
Allopurinol, a structural analog of hypoxanthine (Fig. 1), is both a substrate for and a potent inhibitor of xanthine oxidase in vitro. The binding of allopurinol to xanthine
W. N. Kelley et al. (eds.), Uric Acid© Springer-Verlag Berlin Heidelberg 1978

486 GERTRUDE B. ELION
OH
3c OH
(x) N~ I N) X.O. :tN ~ I }-OH HO~ N HO N N H H H
Hypoxanthine Xanthine Uric acid
Allopurinol Oxipurinol
Fig. 1. Structural formulas of oxypurines, uric acid, allopurinol, and oxipurinol
oxidase is about ten- to fortyfold greater than the binding of xanthine to the enzyme and the inhibition appears to be competitive when initial reaction kinetics are considered (ELlON, 1966). The K j of allopurinol depends on the source of xanthine oxidase and the pH at which the kinetics are measured. For the bovine cream enzyme the K j = 7 X 10- 7 M at pH 7.4 (ELlON, 1966), for the human liver enzyme it is 1.9 x 10- 7 M at pH 7.4 (ELlON, 1966), and for the human small intestinal enzyme it has been reported to be K j =7.6 x 10- 9 M (WATTS et aI., 1965). However, it was recognized in early studies that the enzyme kinetics of allopurinol were not simple and that preincubation of the enzyme for several minutes with allopurinol led to inactivation of the enzyme (ELlON, 1966).
The product of the enzymatic oxidation of allopurinol is the xanthine analog oxipurinol (Fig. 1) (4,6-dihydroxypyrazolo(3,4-d)pyrimidine; alloxanthine; oxoallopurinol; DHPP). Although the apparent K j of this compound initially appeared to be higher than that of allopurinol (ELlON, 1966), rapid inactivation of the enzyme occurred in the presence of a substrate, e.g. xanthine. Preincubation of the enzyme with oxipurinol alone did not inactivate the enzyme.
The explanation for these observations was soon forthcoming from experiments performed anaerobically (MASSEY et aI., 1970; EDMONDSON et aI., 1972) or in the presence of a chemical reductant (SPECTOR and JOHNS, 1970). Oxipurinol complexes very tightly (K j = 5 x 10- 10 M) with partially reduced xanthine oxidase in which the molybdenum is in the Mo(IV) state (MASSEY et aI., 1970, 1970a; SPECTOR and JOHNS, 1970, 1970 a). This binding is stoichiometric, mole for mole, to functional enzyme, i.e., only to enzyme which is turning over. The binding is not covalent, and oxipurinol can be removed by prolonged dialysis or by oxidation of the enzyme, the latter either on prolonged standing in air or by electron acceptors such as ferricyanide or 2,6-dichlorophenolindophenoI. The halftime for reactivation of the oxipurinol-xanthine-

Allopurinol and Other Inhibitors of Urate Synthesis 487
oxidase complex under aerobic conditions is about 5 h (MASSEY et aI., 1970). These studies on the enzyme inhibition have been recently reviewed (SPECTOR, 1977).
The success of allopurinol as a xanthine oxidase inhibitor in vivo is undoubtedly due in large measure to the properties of oxipurinol as an enzyme inhibitor and to its persistence in body fluids (cf. Section IV).
C. Inhibition of Xanthine Oxidase In Vivo
I. Exogenous Purines
The first evidence that allopurinol was an inhibitor of xanthine oxidase in vivo was its ability to prevent the oxidation of 6-mercaptopurine (6-MP) to 6-thiouric acid (TU) in mice (ELION et aI., 1962; EUON et aI., 1963). The conversion of 6-MP to TU is mediated by xanthine oxidase (ELION et aI., 1954; ELION et aI., 1959) and is a major catabolic pathway in the metabolism of 6-MP in man as well as in lower animals (ELION et aI., 1954, 1959, 1963, 1963a; HAMILTON and ELION, 1954). The inhibition of the oxidation of 6-MP by allopurinol in mice is accompanied by an equivalent potentiation of the antitumor and immunosuppressive properties of 6-MP and with some (unproportional) increase in toxicity (ELION et aI., 1963). The biological activities of other 6-substituted purines, e.g. 6-chloropurine, 6-methylthiopurine, and 6-propylthiopurine, all of which are substrates for xanthine oxidase, are potentiated by allopurinol in a similar manner.
In man the oxidation of 6-MP to TU is inhibited by relatively low doses of allopurinol, as evidenced by the reduction in urinary thiouric acid and the increase in the excretion of6-MP (ELION et aI., 1963, 1963a; RUNDLES et aI., 1963; VOGLER et aI., 1966). The antileukemic activity of 6-MP is also potentiated (RUNDLES et aI., 1963; VOGLER et aI., 1966). The more efficient utilization of 6-MP for the synthesis of thiopurine nucleotides when conversion to thiouric acid is blocked undoubtedly accounts for this potentiation (ELION, 1975).
II. Inhibition of Uric Acid Production
The ability of allopurinol to inhibit the oxidation of endogenous purines by xanthine oxidase results in a reduction of uric acid levels in both serum and urine and in an increase in the urinary excretion of hypoxanthine and xanthine (RUNDLES et aI., 1963, 1966; HITCHINGS, 1966; YO and GUTMAN, 1964). This has made the drug an extremely useful therapeutic agent for the treatment of the primary hyperuricemia of goUt(RUNDLES et aI., 1963, 1966, 1966a, 1969; YO and GUTMAN, 1964; KLINENBERG et aI., 1965; SCOTT, 1966) as well as for the secondary hyperuricemias associated with malignancies (KRAKOFF and MEYER, 1965; KRAKOFF and MURPHY, 1968; RUNDLES et aI., 1963, 1969; SCOTT, 1966). The decrease in uric acid production is dose-related, and serum urate levels can be regulated to the desired level by dose adjustment (HITCHINGS, 1966; RUNDLES et al., 1966) unless there is serious impairment of renal function (LEVIN and ABRAHAMS, 1966). When serum urate levels are maintained below the saturation level of sodium urate, crystalline deposits of urate dissolve and tophi decrease in size. The rate of disappearance of such deposits is dependent on the level of serum urate maintained. Some acute attacks of gout have been reported to

488 GERTRUDE B. EUON
occur at the beginning of therapy, as they do with uricosuric agents, probably as the result of the mobilization of urate deposits. With the maintenance of serum urate levels below the saturation point, destructive arthritis improves, acute attacks become less frequent and severe, and gouty nephropathy appear to halt in most patients (SCOTT, 1966; RUNDLES et aI., 1969).
In lower mammals which oxidize uric acid to allantoin via uricase, the effect of allopurinol is to reduce allantoin production and increase oxypurine excretion (HITCHINGS, 1966; EUON et aI., 1968). Longterm animal studies have shown that the degree of inhibition of xanthine oxidase remains constant at a constant dose of allopurinol, indicating that no induction of enzyme occurs as a consequence of prolonged inhibition (HITCHINGS, 1966). This is also true in man. Gout patients do not require increased amounts of allopurinol after years of treatment; indeed, the dose may often be reduced once tophi have disappeared.
Because allopurinol reduces urinary uric acid as well as serum urate, it is used to prevent the hyperuricosuria, uric acid crystals, urinary stone formation, and urinary tract obstruction that often result from the rapid lysis of cells in patients with malignancies who are undergoing intensive chemotherapy or radiation (RUNDLES et aI., 1969). It is similarly possible to prevent the overproduction of uric acid in patients with chronic myeloproliferative diseases, e.g. polycythemia vera, multiple myeloma, and myeloid metaplasia. In individuals who are chronic uric acid stoneformers, allopurinol therapy has been able to prevent urinary stone formation (DE -VRIES et aI., 1966; DE VRIES and FRANK, 1967; RUNDLES et aI., 1969).
III. Oxypurines
The oxypurines hypoxanthine and xanthine are the immediate precursors of uric acid, whether the purines are derived from food, biosynthesis, or nucleic acid degradation. They might be expected to accumulate when xanthine oxidase is inhibited. A factor which mitigates against this is the rapid clearance by the kidney of hypoxanthine and xanthine. Unlike uric acid, the oxypurines are cleared at a rate close to the glomerular filtration rate (GOLDFINGER et aI., 1965). Consequently, serum oxypurine levels rise minimally during allopurinol therapy, in most cases remaining below 0.5 mg/lOO ml (YO and GUTMAN, 1964; EUON et aI., 1968; GOLDFINGER et aI., 1965; HITCHINGS, 1969), well below the solubilities of hypoxanthine and xanthine. The oxypurine crystals reported in the muscle of some allopurinol-treated gout patients (WATTS et aI., 1971) are probably artifacts of the method of preparation (HITCHINGS, 1971).
Elevated levels of oxypurines appear in the urine during allopurinol therapy. In most patients, however, the increase in oxypurine excretion is not as great as the decrease in uric acid excretion (HITCHINGS, 1966; RUNDLES et aI., 1963, 1966), i.e., the total amount of purine end product decreases. A similar decrease in purine endproduct is seen in rats and dogs (HITCHINGS, 1966). One reason for this is the ability of hypoxanthine and xanthine to be reutilized for nucleic acid synthesis when their oxidation to uric acid is inhibited. This has been demonstrated both in mice (POMALES et aI., 1963, 1965) and in man (RUNDLES et aI., 1963, 1966). This reutilization has the effect of reducing the amount of oxypurine excreted and of providing the nucleotides, adenylic acid and guanylic acid, which act as feedback inhibitors of the

Allopurinol and Other Inhibitors of Urate Synthesis 489
first enzyme of purine biosynthesis, glutamine phosphoribosylpyrophosphate amidotransferase. The reutilization of the oxypurines provides by the "salvage" pathway the nucleotides which would ordinarily be synthesized de novo. The fact that the total amount of nucleic acid synthesized is not affected is evidenced by the lack of either inhibition (SKIPPER et aI., 1957) or stimulation of tumor growth (ALEXANDER et aI., 1966) when allopurinol is given.
Another explanation which has been advanced for the decreased de novo purine synthesis seen in the majority of patients is the formation of allopurinol ribonucleotide which acts as a pseudofeedback inhibitor of the amidotransferase (MCCOLLISTER et aI., 1964). While this is theoretically a possibility, the quantitative aspects of nucleotide formation from allopurinol (v.i. Sections V and VI) make it unlikely in a clinical situation.
The enzyme hypoxanthine-guanine phosphoribosyltransferase (HGPRTase) is essential to both the reutilization of oxypurines and the formation of allopurinol ribonucleotide. Consequently, in children with the Lesch-Nyhan syndrome and in the small percentage of gout patients (estimated at 1 %-2% (YU et aI., 1972)) who are deficient in this enzyme, the amount of oxypurine excreted in the urine exactly parallels the decrease in uric acid production caused by allopurinol (BALIS et aI., 1967; ROSENBLOOM et aI., 1967). Thus, although such patients can still be relieved of hyperuricemia and hyperuricosuria by allopurinol, their de novo synthesis of purines is not decreased.
While variable, the ratio of xanthine to hypoxanthine appearing in the urine as a result of xanthine oxidase inhibition is generally about 2: 1. Although hypoxanthine is a very watersoluble compound, xanthine and uric acid have approximately the same low solubility in urine (KRAKOFF and MEYER, 1965; LEVIN and ABRAMS, 1966). There is, therefore, the possibility that excessive xanthine excretion might result in crystalluria or xanthine stone formation. Renal xanthine deposits can be produced in animals by chronic administration of allopurinol (HITCHINGS, 1966). The smaller the animal, the greater the amount of purine endproduct excreted in relation to its water flux. Thus, in rats and mice, which ordinarily excrete the highly soluble endproduct allantoin, the substitution of xanthine as endproduct and the relatively small volume of urine can lead to urinary xanthine concentrations of as high as 1.7 mg/ml, well above the saturation level. The limiting toxicity in these animals is the formation of renal calculi. Xanthine calculi have not, except in rare circumstances, been seen in patients treated with allopurinol. Even with aggressive therapy, urate production is rarely decreased more than 50%, and the total amount of xanthine excreted is generally below 150 mg/day. In a urine volume of 1500 ml, this would give a xanthine concentration of only 0.1 mg/ml, and where reutilization of xanthine for nucleic acids can occur, xanthine excretion is often less. However, in children with the LeschNyhan syndrome, children who are tremendous overproducers of uric acid and who lack HGPRTase, aggressive therapy with allopurinol (e.g. 9 mg/kg) has produced xanthine precipitates in the urine (SORENSEN, 1968). Xanthine crystalluria has also been reported in two cases of Burkitt's lymphoma and lymphosarcoma treated with aggressive chemotherapy and allopurinol (GREENE et aI., 1969; BAND et aI., 1970; ALBIN et aI., 1972). The natural occurrence of xanthine stones in man is not unknown, but the number reported in the literature is small (RUNDLES et aI., 1969). In xanthuric patients who have a congenital lack of xanthine oxidase and whose purine

490 GERTRUDE B. EUON
end product is almost totally xanthine, xanthine stones are rare even at levels of xanthine excretion considerably higher than those reached under allopurinol therapy. The maintenance of a high water flux is nevertheless recommended as a precautionary measure.
D. Pharmacokinetics and Clearance
Allopurinol has a solubility in water of 0.44 mg/ml at 25° C and 0.75 mg/ml at 37° C (ELION, unpublished). Its pKa = 9.34 (KRENITSKY et aI., 1967), similar to that of hypoxanthine (pKa = 8.9). The monosodium salt is soluble to the extent of 13.6 mg/ ml and can be used for intravenous (i.v.) infusion.
Oxipurinol is less watersoluble than allopurinol. Its solubility in water is 0.35 mg/ ml at 37° C. Its pKa = 7.74 (KRENITSKY et aI., 1967), close to that of xanthine (pKa = 7.4), and its solubility in urine is much greater at pH 8 (700 mg/l) than at pH 5 (20 mg/l) (LEVIN and ABRAHAMS, 1966).
Allopurinol is rapidly well absorbed from the gastrointestinal tract. Peak plasma levels in man generally occur at 0.5-1 h after ingestion (ELION et aI., 1966; NELSON,
unpublished). An oral dose of 300 mg produces a maximum plasma level of allopurinol of about 2llg/ml (NELSON, unpublished). Approximately 20% of the ingested drug has been found to be excreted in the feces (ELION et aI., 1966). Because of its rapid oxidation to oxipurinol and a renal clearance rate approximating that of glomerular filtration, allopurinol has a plasma halflife in man of about 2 h at the usual therapeutic doses (3-6 mg/kg) (ELION et aI., 1966). However, oxipurinol has a very long plasma halflife (18 h-30 h), and effective xanthine oxidase inhibition can thus be maintained at a steady state with even a single daily dose of allopurinol (RODNAN et aI., 1975).
Because of the oxidation of allopurinol, the ratio of allopurinol to oxipurinol in the plasma changes rapidly (Table 1). At high intravenous doses of allopurinol (50-100 mg/kg), the degree ofxanthine oxidase inhibition is so great that the oxidation of allopurinol itself is inhibited and its plasma halflife then approaches the glomerular filtration rate, e.g. 100 mg/kg i.v. in a dog (Table 1).
The long plasma halflife of oxipurinol is not due to either plasma protein binding or concentration in tissues. Both allopurinol and oxipurinol show no binding to plasma proteins, are freely diffusable, and are distributed in total body water. However, levels in the brain are only about 1/3 of those in other tissues (ELION et aI., 1966).
Whereas allopurinol is cleared essentially by glomerular filtration, oxipurinol is reabsorbed in the kidney tubules in a manner similar to the reabsorption of uric acid (ELION et aI., 1968). The clearance rate of oxipurinol in a man with normal renal function is approximately 15 mljmin, or 3 times the rate of urate clearance. Tubular reabsorption of oxipurinol is inhibited by uricosuric agents, e.g., probenecid, in the same way as is the reabsorption of uric acid (ELION et aI., 1966, 1968). Consequently, combined treatment with allopurinol and a uricosuric agent will lead to a lower plasma concentration of oxipurinol and to less xanthine oxidase inhibition than when allopurinol alone is given.
As oxipurinol is itself a potent xanthine oxidase inhibitor and produces a prolonged duration of enzyme inhibition, it can be used as an alternative drug in the

Allopurinol and Other Inhibitors of Urate Synthesis 491
Table 1. Ratios of allopurinol to oxipurinol in plasma following allopurinol administration
Species Dose Time Allopurinol/ Ref. mg/kg h Oxipurinol
Man 4.5, p.o. I 0.5 NELSON, unpublished 2 0.17 6 0.02
Dog 4, 1.v. 1 2.0 ELION et a!., 1966 2 0.35
100 1.v. 1 35 ELION, unpublished 6 11
Rat 50 ,1.v. I 3.1 NELSON et a!., 1973 6 0.3
treatment of hyperuricemia (RUNDLES, 1966a; CHALMERS et aI., 1968). However, because of its relatively poor solubility and absorption, oxipurinol must be given in doses twice as high as allopurinol to achieve the same degree of xanthine oxidase inhibition (CHALMERS et aI., 1968; ELION et aI., 1968; SIMMONDS, 1969; ELION, unpublished). It therefore appears to offer no therapeutic advantage over allopurinol.
Patients with impaired renal function poorly clear both uric acid and oxipurinoI. Lower than normal doses of allopurinol are required for individuals with gouty nephropathy to maintain a plasma concentration of oxipurinol adequate for xanthine oxidase inhibition. The relationship of steady-state plasma levels of oxipurinol to clearance of oxipurinol (or urate) at various doses of allopurinol can be approximated by a nomogram (ELION et aI., 1968). The theoretical values based on the assumption that 70% of the daily dose is excreted as oxipurinol agree well with the experimentally determined plasma concentrations (ELION et aI., 1966, 1968). In a patient with normal urate clearance, a dose of 300 mg/day of allopurinol gives a plasma level of oxipurinol of about 10 /lg/mI.
Since both allopurinol and oxipurinol are dialyzable, patients on hemodialysis who suffer from hyperuricemia require a dose of only about 300 mg of allopurinol after each dialysis to maintain an adequate oxipurinol concentration between dialyses (HAYES et aI., 1965; RUNDLES, 1966; ELION, unpublished).
E. Metabolism
The metabolic transformations of allopurinol and oxipurinol are shown in Figure 2. These will be discussed as two categories: I} plasma and urinary metabolites and 2} tissue metabolites. While all of the plasma metabolites also occur in the tissues, the nucleotides are present only in tissues.
I. Plasma and Urinary Metabolites
The principal metabolic endproduct of allopurinol is oxipurinoI. Once the plasma level of oxipurinol has reached a steady state, e.g. after 5-7 days of daily oral doses of allopurinol, the quantity of oxipurinol excreted accounts for 60-70% of the dose

492
HGPRTase
enOH ~ PNPase N:nOH ~
'~IN/N" ~I I 'N """ """ / I N 7
H Rib
Allopurinol
Phosphatase ..
Xanthine j Oxidase
Allopurinol-I-riboside
HGPRTase
o
H""-N~ Phosphatase
~~,Jl-~)N .. PNPase /0 I I
o / r.. H Rib H"'-N~ Oxipurinol-l-riboside
~",J-J OPRTase o 7 I Nucleoside
H H ~OSPhOrYlaSe 0
0,"purino1 '\. H'-N~ O~N N
~b ~ Phosphatase .. ------
Uridine Kinase
Oxipurinol-7 -riboside
Fig. 2. Metabolic transformations of allopurinol and oxipurinol
GERTRUDE B. ELION
l-Alo-S'-P
o
H'-7~ 00N N
I I , H Rib-S -P04
l-Oxi-S:""P
:x~ I ~
Rib-S'-P04
7-0xi-S'-P
(ELION et ai., 1966; ROD NAN et ai., 1975; SIMMONDS, 1969). About 6-12% of allopurinol excreted in the urine is unchanged at the usual therapeutic doses (300-400 mg/ day), and an approximately equal amount is excreted as allopurinol-I-ribonucleoside; oxipurinol-7-ribonucleoside accounts for about 3% of the dose (ELION et ai., 1966; SIMMONDS, 1969; KRENITSKY et ai., 1967).
If animals or human patients are given doses of allopurinol high enough to inhibit allopurinol oxidation (cf. Section IV), the amount of allopurinol in the urine markedly increases. Dogs given 100 mg/kg of allopurinol i.v. excreted 40-50% of the allopurinol unchanged within 24 h (ELION, unpublished). A child orally given 1200 mg of allopurinol excreted approximately 400 mg in the urine as allopurinol (SWEETMAN,1968).
Patients with xanthinuria have been shown to have little or no xanthine oxidase (ENGELMAN et ai., 1964; HOLMES et ai., 1974). In such patients one might expect to find no conversion of allopurinol to oxipurinoi. This has been the case in two xanthurics studied (ENGELMAN et ai., 1964; ELION et ai., 1966; SIMMONDS et ai., 1974a). However, in two other patients substantial amounts of oxipurinol were

Allopurinol and Other Inhibitors of Urate Synthesis
1000
300
100
~ 30 a c o
0';:;
g c ~ c::
8
10
3
0.3
~o~
:==i::.. .. ""'=------.OxiPurinol
/ • ~ (;. Allopurinol (;. ~ riboside I 0 Allopurinol
.--------11 / '" rI ,
0--0 --___ " Alo-5'-P --\ " Liver
\ " \ , \Alo-5'-P "
\Kidney '", \ ,
0.1L--~-~--L-~~\-J---L---o 2 3 4 5 6
Hours
493
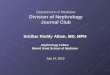
Fig. 3. Plasma and tissue concentrations of allopurinol and its metabolites in the rat at various times following an i.v. injection of 50 mg/kg allopurinol
formed from allopurinol (SIMMONDS, 1969; CHALMERS et al., 1969; AUSCHER et al., 1974). It has been hypothesized (SIMMONDS, 1969) that oxipurinol may be produced via oxipurinol-l-ribonucleotide by the action of inosinate dehydrogenase on allopurinol-I-ribonucleotide. This is unlikely, however, since studies with inosinate dehydrogenase from Sarcoma 180 (MILLER and ADAMCZYK, 1976) have shown that allopurinol-I-ribonucleotide is not a substrate for this enzyme. A more probable explanation is that some xanthuric patients have an active aldehyde oxidase. This is an enzyme which converts allopurinol to oxipurinol, though less efficiently than does xanthine oxidase (KRENITSKY et al., 1972).
Allopurinol ribonucleoside can arise from allopurinol in two different ways: by the action of purine nucleoside phosphorylase (PNPase) on allopurinol and a ribosyl donor (e.g., ribose-I-phosphate, inosine, xanthosine) (KRENITSKY et al., 1967; KRENITSKY, 1967), or by action of phosphatases on allopurinol-I-ribonucleotide (Fig.2). The nucleoside phosphorylase route appears to be more probable on the basis of drug metabolism and enzyme studies. The pertinent data will be more fully discussed below in connection with tissue metabolites. The data in Figure 3 obtained from studies in the rat following i.v. administration of allopurinol (NELSON et al., 1973) illustrate the close parallel between the plasma levels of allopurinol ribonucleoside and those of oxipurinol, suggesting that both are formed directly from allopurinol. The allopurinol-I-ribonucleotide levels in the livers and kidneys of these animals are lower by 1 or 2 orders of magnitude (Fig. 3).

494 GERTRUDE B.EuON
The small amount of oxipurinol-7-ribonucleoside found in human urine (KRENITSKY et ai., 1967; SIMMONDS, 1969) is probably produced by the action of uridine phosphorylase on oxipurinol (KRENITSKY et ai., 1967). Guinea pig intestinal uridine phosphorylase can also effect this conversion (KRENITSKY et ai., 1967). The specificities of the human and guinea pig enzymes are similar, but those of the rat are not (KRENITSKY et ai., 1965). In the rat, no urinary oxipurinol-7-ribonucleoside has been found in urine after allopurinol administration (NELSON et ai., 1973).
No oxipurinol-l-ribonucleoside has been detected in human urine. This may be a reflection either of its instability (KRENITSKY et ai., 1967) or of the fact that, although oxipurinol binds to purine nucleoside phosphorylase (K j = 0.81 mM) (KRENITSKY et ai., 1968), the velocity of its phosphorylation at 1 mM only O.lS% of that of hypoxanthine (KRENITSKY, 1967).
II. Tissue Metabolites-N ucleotides
Although the conversion of allopurinol to its ribonucleotide had been shown to be catalyzed by hypoxanthine-guanine phosphoribosyltransferase (HGPRTase) in vitro (WAY and PARKS, 19S8; MCCOLLISTER et ai., 1964; KRENITSKY et ai., 1969), early attempts to detect its formation either in vivo or in cell cultures were unsuccessful (ELION et ai., 1966; HITCHINGS, 1969; KELLEY and WYNGAARDEN, 1970). By the use of [6_ 14C] allopurinol of high specific activity, the administration of high i.v. doses to rats, and the extraction of substantial amounts of tissue (S-20 g), it became possible to isolate, identify, and quantify the amounts of both allopurinol ribonucleotide (l-alo-S'-P) and two oxipurinol ribonucleotides (l-oxi-S'-P and 7-0xi-S'-P) formed in vivo (NELSON et ai., 1973). The minimum detectable level of nucleotide metabolites in these studies was 0.01 nmole/g of tissue. The concentrations of the three mononucleotides were dependent on dose, route of administration, time, and tissue.
The levels of l-alo-S'-P in the rat following a so mg/kg i.v. dose of allopurinol were highest in the liver and kidneys (Fig. 3); after 6 h, the concentration in the kidney was undetectable (i.e., <0.01 nmoles/g). At 3 h the level in erythrocytes was 0.27 nmoles/g. The low levels of 1-alo-S'-P attained are not surprising, as the binding constant of allopurinol to HGPRTase is quite high (K j =0.99 mM at pH 7.7,38° C, for the human erythrocyte enzyme) and its velocity of conversion to ribonucleotide low (2.7% is the rate of hypoxanthine conversion at 0.12S mM) (KRENITSKY et ai., 1969). The rapid oxidation of allopurinol in vivo results in very low plasma levels (generally below 10 /lM in man after a dose of 300 mg). It is unlikely that allopurinolI-ribonucleoside can be phosphorylated to 1-alo-S'-P since there is only marginal inosine kinase activity in mammalian cells (UTTER, 1960; PAYNE et ai., 1970).
The question can now be addressed as to whether the allopurinol-I-ribonucleoside found in urine is more likely to arise indirectly via the ribonucleotide or directly from allopurinol by the action of purine nucleoside phosphorylase. The quantitative aspects of the metabolic data (cf. Fig. 3) are in favor of the phosphorylase pathway. The apparent binding constant of allopurinol to the nucleoside phosphorylase from human erythrocytes is 0.97 mM (KRENITSKY et ai., 1968), similar to its binding constant to HGPRTase. However, the velocity of conversion of allopurinol to its ribonucleoside is 10% that of hypoxanthine (at 1 mM with ribose-1-phosphate as ribosyl donor and crystalline calf-spleen nucleoside phosphorylase)

Allopurinol and Other Inhibitors of Urate Synthesis 495
(KRENITSKY, 1967). Moreover, as judged from studies in the monkey, nucleoside phosphorylase activity is manyfold higher than HGPRTase activity in most tissues, particularly in blood cells, liver, kidneys, and lungs (KRENITSKY, 1969).
In children with the Lesch-Nyhan syndrome who lack HGPRTase (SEEGMILLER et aI., 1967), very little allopurinol ribonucleoside has been found in the urine following allopurinol administration (SWEETMAN, 1968). This has also been true in one gouty patient lacking HGPRTase (EUON, unpublished). This could be interpreted as indicating that allopurinol-I-ribonucleoside arises from the corresponding ribonucleotide. An alternative explanation is that patients lacking HGPRT have elevated hypoxanthine levels because of their inability to reutilize this purine. Such elevated levels in the serum have indeed been reported (SWEETMAN, 1968). Hypoxanthine is a much better substrate for purine nucleoside phosphorylase than is allopurinol, as its binding constant is 100 times lower than that of allopurinol and its velocity of conversion 10 times greater, and the competition of the two substrates for the enzyme would thus favor the formation of inosine rather than that of allopurinol-lribonucleoside. Xanthine is also a competitive substrate with a binding constant 25 times lower and a velocity 5 times greater than allopurinol (KRENITSKY, i967). While the formation of some allopurinol-I-riboside from the ribonucleotide is not ruled out, the bulk of evidence appears to favor its direct formation from allopurinol.
The concentrations of the oxipurinol ribonucleotides in rats given allopurinol (50 mg/kg i.v.) were lower than those of l-alo-5'-P and were undetectable in erythrocytes. The highest 7-oxi-5'-P level (2.5 JlM) was found in the kidney and the highest l-oxi-5' -P level (0.73 JlM) in the liver, both at 3 h; by 6 h these had declined to 0.39 and 0.09, respectively. Oxipurinol nucleotides were also detected following i.p. administration of 14C-oxipurinol in rats (NELSON et aI., 1973).
The formation of 7-oxi-5'-P from oxipurinol and PRPP is catalyzed by orotate phosphoribosyltransferase (OPRTase) from beef erythrocytes (FYFE et aI., 1973). This enzyme forms 5'-ribonucleotides from xanthine, uric acid, uracil, and orotic acid (HATFIELD and WYNGAARDEN, 1964, 1964a) with the ribosyl group attached to the N-l of the 2,4-dioxopyrimidine ring (corresponding to the N-3 of purines and the N -7 in the pyrazolo(3,4-d)-pyrimidine ring system). It is also possible that the oxipurinol-7-ribonucleoside formed by the action of uridine phosphorylase may serve as a substrate for uridine kinase.
The metabolic formation of l-oxi-5'-P is probably due to the action of HGPRTase on oxipurinol (Ki> 10 mM) to this enzyme and the undetectable velocity of conversion in vitro (KRENITSKY et aI., 1969) may account for the very low levels of l-oxi-5'-P found in tissues even at high doses of allopurinol. Attempts to oxidize 1-alo-5'-P to l-oxi-5'-P with IMP dehydrogenase (derived from Scarcoma 180 ascites cells) in vitro have been unsuccessful, even with a substrate concentration as high as 7.7 mM (MILLER and ADAMCZYK, 1976).
The significance of the quantities of allopurinol and oxipurinol ribonucleoside monophosphates formed in tissues will be discussed below in relation to effects on purine and pyrimidine biosynthesis.
NELSON et al. (1973) found no ribonucleoside di- or triphosphates derived from allopurinol or oxipurinol in the tissues of rats given 50 mg/kg i.v. of a radioactive drug, although the methods used would have detected 10- 9 M of these compounds. The absence of triphosphates was consistent with the lack of incorporation of allo-

496 GERTRUDE B. EUON
purinol into nucleic acids both in mouse livers (ELION et aI., 1966) and in cultured human fibroblasts (KELLEY and WYNGAARDEN, 1970). Further studies were performed in order to verify the lack of incorporation into nucleic acids under conditions which would present the most severe test, e.g., high dose, high specific activity, rapidly dividing tissue (intestine), and time of maximum mononucleotide formation (NELSON and ELION, 1975). These studies confirmed the previous conclusion that incorporation into nucleic acids does not occur. They also showed no formation of the ribonucleotides of the 4-amino or 6-amino-4-hydroxypyrazolo(3,4-d)pyrimidine (analogs of adenine or guanine) following allopurinol administration. The minute amount of 14C found in the intestinal RNA was solely in the adenine and guanine moieties of the RNA. This is consistent with the ring opening of [6_14CJ allopurinol and the loss of a small amount of 14C as radioactive carbon dioxide shown to occur in mice (ELION et aI., 1966). It is possible that this carbon is split off as 14C-formate and can then enter the I-carbon pool to be used in the biosynthesis of purines.
F. Effects on Purine Biosynthesis
The ability of allopurinol to decrease the total purine excretion (hypoxanthine + xanthine + uric acid) in humans and animals who have the enzyme HGPRTase has been mentioned above (cf. Section III C). It has been postulated that this is due to reutilization of the oxypurines for nucleic acid synthesis and feedback inhibition of de novo purine biosynthesis by the naturally occurring purine nucleotides and/or allopurinol ribonucleotide. Another possible reason for decreased de novo synthesis is a decrease in phosphoribosylpyrophosphate (PRPP) concentrations, since PRPP is required for the first step of purine biosynthesis, i.e., the reaction with glutamine to form phosphoribosylamine. Either the reutilization of oxypurines or the formation of allopurinol and oxipurinol ribonucleotides would consume PRPP. In addition, the formation of allopurinol ribonucleoside from allopurinol could deplete ribose-lphosphate, a precursor of PRPP. A decrease in PRPP has been reported in human erythrocytes for a 5 h period following a dose of allopurinol (2-4 mg/kg, p.o.), but not after oxipurinol administration (Fox et aI., 1970; Fox and KELLEY, 1971). In human fibroblasts, however, which (unlike erythrocytes) presumably have a functional de novo pathway, there is no significant drop in the PRPP level at an allopurinol concentration of 0.1 mM (10-100 times the plasma level generally found in man) (KELLEY et aI., 1971). At the high dose of allopurinol (50 mg/kg i.v.) employed in the rat studies (NELSON et aI., 1973; ELION and NELSON, 1974), enough 1-alo-5'-P and 1-oxi-5'-P could have been formed to cause a temporary decrease in PRPP levels in the liver, since the normal PRPP concentration in rat liver is approximately 10 11M (CLIFFORD et aI., 1972). However, more needs to be known about the functional capacity of PRPP synthetase and the relative amounts and turnover rates of all the enzymes utilizing PRPP before a conclusion can be reached about the significance of the effect of allopurinol on PRPP levels.
The quantitative determination of 1-alo-5'-P in the tissues of rats at various dose levels of allopurinol helps to elucidate the possible importance of this nucleotide as a pseudofeedback inhibitor. It can be calculated that if 4 11M 1-alo-5'-P is formed in a rat liver when the plasma level (at 1-3 h after an i.v. injection of 50 mg/kg) of allopurinol is between 180-55 11M, then the expected concentration of 1-alo-5'-P in

Allopurinol and Other Inhibitors of Urate Synthesis 497
human liver would be <0.1 11M at plasma levels of < 10 11M allopurinol (following a dose of 300 mg p.o.) (ELION and NELSON, 1974). However, 0.1 11M is far below the Ki of 600 11M reported for l-alo-5'-P as an inhibitor of the pigeon liver PRPP amidotransferase (MCCOLLISTER et aI., 1964). Quantitative considerations, therefore, make it unlikely that this nucleotide is responsible for the feedback inhibition observed in man.
The purine nucleotide pool sizes in rat liver and kidneys at various times after a single i.v. or i.p. dose (20 mg/kg) of allopurinol show only minor transient changes (ELION and NELSON, 1974). In the liver there is a transient decrease in AMP, GMP, GDP, and ATP levels at 1 h with a return to normal or elevated levels at 3 h. In the kidneys, levels of AMP and ATP are slightly elevated at 1 h while GDP levels remained elevated at 24 h. It is apparent that the purine nucleotide pools can fluctuate rapidly and that the fluctuations may be different in different tissues.
In rats fed 0.1 % allopurinol of their diet for 1 month, a dose sufficient to reduce allantoin excretion by 50% and to inhibit total purine end product excretion (i.e., feedback inhibition), there was no change in mono-, di-, or triphosphates of adenosine or guanosine (ELION and NELSON, 1974). The regulatory mechanisms of purine biosynthesis appear to be very efficient in maintaining normal purine nucleotide levels.
G. Effects on Pyrimidine Biosynthesis
The finding by Fox et aI. (1970) and KELLEY and BEARDMORE (1970) that a significant increase in the excretion of orotate and orotidine occurs in both animals and man treated with allopurinol suggests some interference with pyrimidine biosynthesis. Inhibitors of orotidylate decarboxylase are formed when allopurinol or oxipurinol is incubated with red celllysates and PRPP (Fox et aI., 1971; BEARDMORE and KELLEY, 1971) and 14C-orotate metabolism is inhibited in the presence of oxipurinol (KELLEY and BEARDMORE, 1971). This has led both groups of authors to postulate that One or more ribonucleotides of allopurinol or oxipurinol are responsible for this inhibition. Once these nucleotides were isolated and synthesized (FYFE et aI., 1973), kinetic studies with orotidylate decarboxylase (ODCase) were possible. The enzyme from yeast and rat liver have exhibited bimodal kinetics (FYFE et aI., 1973, 1974), as have the ODCase from human fibroblasts (WORTHY et aI., 1974) and human red cell hemolysates (TAX et aI., 1976). BROWN et aI. (1975) have reported that the partially purified ODCase from human erythrocytes show a triphasic Lineweaver-Burk plot with Km values of 25, 3, and 0.6 11M for the monomer, dimer, and tetramer forms of the enzyme, respectively. At levels of OMP above 10 11M, the Km (211M) and Vrnax are relatively high for the rat liver ODCase and the inhibitors show high Ki values (FYFE et aI., 1973). At OMP concentrations below 211M, a lower Km (0.5 11M) and lower Vmax and Ki values have been found. These lower Ki values are probably the pertinent Ones in vivo (OMP levels in normal rat liver are below 0.1 11M and even following high dose allopurinol treatment only reach 5 11M (HITCHINGS, 1974)). The low Ki values for 1-alo-5'-P, 1-oxi-5'-P, and 7-oxi-5'-P are: 1 x 10- 6 M, 5 X 10- 10 M, and 4 x 10 - 8 M, respectively (FYFE et aI., 1973). After high dose of allopurinol i.v. in rats, the maximum levels of the three nucleotides attained in the liver and kidney, particularly the oxipurinol ribonucleotides, exceed these Ki values. If one extrapo-

498 GERTRUDE B. ELION
lates from the plasma levels of oxipurinol in the rat and from comparable levels in man, e.g., 65 ~M in man on a 300 mg daily dose, the attainable levels of 1-oxi-5'-P and 7-oxi-5'-P could be as high as 1 ~M in tissues such as liver and kidneys (ELION and NELSON, 1974). These levels would be sufficient to produce inhibition of ODCase and the consequent orotic aciduria and orotidinuria which have been observed.
How significant is this inhibition of OMP decarboxylase in relation to the amount of uridine nucleotides available for nucleic acid synthesis in vivo? The experimental evidence indicates that the effects of allopurinol and oxipurinol administration (20 mgjkg, i.v.) on the uridine-containing metabolite pools (UMP, UDP, UTP, and UDP-glucose) are small and transient (NELSON et ai., 1973). Even after 7 days of allopurinol treatment at 20 mgjkgjday, the UTP level in rat liver remains unchanged despite a marked elevation of orotidine and orotic acid in the kidneys (possibly in the tubular lumens, since the amount of these compounds in the urine becomes elevated). This apparent contradiction is clarified when the pool sizes of orotic acid and OMP are examined. A remarkable expansion of these pool sizes (to 9 and 73 times control values has been observed in rat livers within one h after allopurinol administration (HITCHINGS, 1974). These would greatly dilute any radioactive precursor used for the measurement of the inhibition of ODCase and make the inhibition appear greater than it actually is. When NaH14C0 3 is used as a precursor for uridylate, the rate of incorporation is no lower in the livers of allopurinol-treated rats than in those of normal rats (NELSON, unpublished; cf. HITCHINGS, 1975). It is apparent that the accumulation of OMP, the substrate of the blocked reaction, can partially overcome the inhibition caused by the competitive inhibitors 1-oxi-5'-P and 7-oxi-5'-P. When a steady state is reached, e.g., after 1 week of treatment, a normal turnover of pyrimidines is further aided by an increase in the activity of ODCase. This increased activity may be due to stabilization or activation of the enzyme in vivo (Fox et aI., 1971; BEARDMORE et aI., 1972; TAX et aI., 1976) or to the formation of polymeric forms of the enzyme with lower than normal Km values (BROWN et ai., 1972, 1975; GROBNER and KELLEY, 1975). It has also been suggested that the increased activity may be an artifact of the extraction procedure (BECKER et ai., 1974; GROBNER and KELLEY, 1975). In any event, the urinary leakage of orotate and orotidine, which amounts to about 10% of the estimated normal 600 mgjday turnover of pyrimidines in man, appears to be compensated for, as normal pools of uridine nucleotides are maintained.
H. Other Pharmacological Effects
I. Iron Metabolism
Because xanthine oxidase has been thought to have an important physiological role in the transport of iron from liver stores through intestinal mucosa to plasma (MAZUR et ai., 1958; MAZUR and CARLETON, 1965), the effect of allopurinol on iron metabolism has been investigated. Rats fed a diet supplemented with 5% ferric ammonium citrate and 0.01 % allopurinol have been reported to show a greater increase in hepatic iron content than rats given the iron supplement alone (POWELL, 1966; POWELL and EMMERSON, 1966). However, other investigators using larger numbers of rats and higher doses of allopurinol have found no evidence for excessive iron

Allopurinol and Other Inhibitors of Urate Synthesis 499
deposition in allopurinol-treated animals given iron-supplemented diets (UDALL, 1966; GEVIRTZ, 1967; KOZMA et aI., 1967; GRACE et aI., 1970). Allopurinol administration for 4 months to mice on a normal diet also caused no iron deposition in the liver (KOZMA et aI., 1968).
The effect of varying dosage schedules of allopurinol on iron absorption from the gastrointestinal tract of man has been measured using 59Fe. No significant difference has been found between controls and drug-treated groups in the amount of iron absorbed (DAVIS and DELLER, 1966; BOYETT et aI., 1968; GREEN et aI., 1968). Serum iron levels in patients on allopurinol therapy for months or even years have generally remained within normal limits (EMMERSON, 1966; GREEN et aI., 1968; RUNDLES et aI., 1966; SCOTT et aI., 1966a). However, there is a report of one patient showing a rise in serum iron from 70 to 130 /lg/ml during allopurinol therapy (HOENIG et aI., 1967). A liver biopsy on a patient who had been treated with allopurinol for 18 months and had received iron therapy periodically during this time showed no abnormal iron deposits (SJOBERG, 1966).
There is still considerable debate as to whether or not xanthine oxidase is required for iron transport or mobilization from ferritin (AYVAZIAN, 1964; SEEGMILLER et aI., 1964; ENGELMAN et aI., 1964). A patient with xanthinuria who suffered from a gross deficiency of xanthine oxidase in both the intestinal epithelium and the liver was found to be able to absorb orally-administered iron in a normal fashion, and this led ENGELMAN et aI. (1964) to conclude that "normal levels of intestinal xanthine oxidase activity are not needed for iron absorption." In any event, it appears that the inhibition of xanthine oxidation achieved clinically with allopurinol, generally under 50%, does not significantly alter iron metabolism.
II. Protection from Ischemia
The damage produced in tissues by ischemia is due mainly to hypoxia. Levels of A TP fall due to dephosphorylation to ADP, AMP, and adenosine; deamination produces inosinate and inosine, and the hypoxanthine resulting therefrom is converted to uric acid and then excreted (IMAI et aI., 1964; JONES et aI., 1968). The possibility that ATP could be restored to ischemic tissue if the irreversible loss of hypoxanthine by oxidation were prevented has led to an examination of the effects of allopurinol on ischemia and hemorrhagic shock. The resulting reports are somewhat conflicting.
CROWELL et aI. (1969) reported that allopurinol pretreatment increases the survival rate in dogs subjected to hemorrhagic shock, but that multiple treatment with allopurinol, hypoxanthine, atropine, heparin, and ouabain is superior to allopurinol alone (CROWELL, 1970). BAKER (1972) found that allopurinol pretreatment alone is not sufficient to protect dogs from irreversible hemhorragic shock but that when allopurinol is combined with hypoxanthine, adenine, inosine, IX-ketoglutarate, and oxalacetate, a marked increase in survival rate occurs. LEPER et aI. (1969) reported that allopurinol produces a decrease in serum uric acid but has no effect on myocardial ATP and does not lead to increased survival in cats and dogs subjected to hemorrhagic shock. However, HOPKINS et aI. (1975) did find an increase in hepatic adenosine nucleotides when oligemic dogs were treated with allopurinol 1 h after reinfusion of blood. LAZARUS et aI. (1974) found that allopurinol protects hepatic nuclear RNA synthesis during hemorrhagic shock in dogs.

500 GERTRUDE B. ELION
In dogs and sheep with myocardial ischemia produced by coronary artery ligation, allopurinol has some protective effect (DE WALL et aI., 1971). Allopurinol also increases the survival rate in dogs undergoing cardiac arrest induced by electric shock (PARKER and SMITH, 1972) and prevents the rise in serum uric acid usually observed under these conditions. An improved survival rate has also been reported in rats subjected to experimental myocardial infarction and treated pre- and postoperatively with allopurinol (WENZELIDES and MEYER, 1975; WENZELIDES et aI., 1975). On the other hand, SHATNEY et al. (1976) found no benefit from postoperative allopurinol treatment in dogs subjected to myocardial infarction.
Of possible relevance to the effects of allopurinol on experimental myocardial ischemia is the increased coronary and aortic flow observed in open-chested dogs treated with relatively high (above 50 mg/kg) i.v. doses of sodium allopurinol (ELLIS et aI., 1973; STANLEY, 1971). Moreover, MANZKE and DORNER (1975) found an increase of both ATP and 2,3-diphosphoglycerate levels in erythrocytes of allopurinol-treated patients (7-10 mg/kg p.o. daily) as well as a shifting of the oxygen dissociation curve to the right with an increase in the oxygen desaturation of about 5% at a mean central venous oxygen pressure of 40 mmHg.
During the transplant of organs, the period of warm ischemia often determines the success or failure of the functioning graft. Allopurinol has been reported to reduce damage due to kidney ischemia (VASKO et aI., 1972), and pretreatment of canine donor kidneys with allopurinol has been shown to increase the survival time of such allografts (TOLEDO-PEREYRA and NAJARIAN, 1973, 1975; OWENS et aI., 1974; CHATTERJEE and BERNE, 1976). Significantly higher levels of ATP, ADP, and AMP were found in the kidneys of allopurinol-treated rats during ischemic and postischemic recovery than in control animals (CUNNINGHAM et aI., 1974). TOLEDOPEREYRA et al. (1975) have found that pretreatment of donor dogs with a combination of allopurinol, isoproterenol, and heparin can prevent the irreversible damage caused by 30 min of liver ischemia prior to the transplant. In a canine model for small bowel preservation and transplant, the addition of allopurinol to the 24 h perfusate has resulted in a significant improvement in the survival of the transplant (TOLEDO-PEREYRA et aI., 1975); a similar effect has been noted with pancreaticoduodenal allografts (TERSIGNI et aI., 1975). However, in a randomized double-blind clinical study in which allopurinol was either added or withheld from the perfusate used to preserve cadaver kidneys, allopurinol did not show a consistent beneficial effect (TOLEDO-PEREYRA et aI., 1977).
Based on the high levels of xanthine oxidase and low levels of plasmalogens found in atherosclerotic plaques, OSTER (1968, 1971) has theorized that xanthine oxidase is responsible for "plasmalogen disease," and that this was a forerunner of atherosclerosis, angina pectoris, and myocardial infarction. OSTER (1968) treated nine angina patients with 600 mg allopurinol/day in an attempt to increase the concentration of plasmalogens in the blood and heart. He reported that this reduced both the number and severity of angina attacks and permitted a reduction in the dose of nitroglycerine. No controlled studies have been reported.
III. Tryptophan Pyrrolase Inhibition
Allopurinol noncompetitively inhibits the activity of rat liver tryptophan pyrrolase in vitro with a Ki = 8 X 10- 7 M (BECKING and JOHNSON, 1967); it also inhibits the

Allopurinol and Other Inhibitors of Urate Synthesis 501
activity of cortisol-induced or tryptophan-induced enzyme, both in vivo and in vitro (CHYTIL, 1968; GREEN and CURZON, 1968; MOON, 1971; BADAWY and EVANS, 1973; HILLIER et aI., 1975; GREEN et aI., 1976). HILLIER et aI. (1975) reported a reduction in serum tryptophan levels in rats injected intraperitoneally with allopurinol; BECKING and JOHNSON (1967) found no such alteration in plasma tryptophan levels but did report that the rats excreted less kynurenine than normal. It has been suggested that xanthine oxidase participates in the activation of tryptophan pyrrolase (JULIAN and CHYTIL, 1970; CHYTIL, 1968) and that allopurinol exerts its effect via xanthine oxidase inhibition. However, BADAWY and EVANS (1973) have presented evidence to support the idea that the inhibition of rat liver tryptophan pyrrolase by allopurinol is due to prevention of the conjugation of the apoenzyme with its haem activator and not to a regulatory effect of xanthine oxidase on tryptophan pyrrolase activity. A lack of effect of oxipurinol (alloxanthine) on pyrrolase activity in vitro or in vivo has been reported by BADAWY and EVANS (1973). BECKING and JOHNSON (1969), however, have found oxipurinol to be an active inhibitor in vitro.
Since allopurinol prevents the decrease in brain 5-hydroxytryptamine (5-HT) provoked by hydrocortisone (GREEN and CURZON, 1968), it has been suggested (GREEN and CURZON, 1968; HASKOVEC et aI., 1972; BADAWY and EVANS, 1974) that allopurinol might have some application in the treatment of depression, particularly if given in conjunction with tryptophan. In a 3 week trial in which allopurinol alone was given to seven depressed patients, no improvement in their condition was noted (HASKOVEC et aI., 1972).
IV. Drug Interactions
Since hyperuricemia occurs in a variety of disease states, allopurinol is often given in conjunction with other drugs. Some drug interactions are predictable from the inhibitory effects of allopurinol on xanthine oxidase. The inhibition of the oxidation of 6-MP to thiouric acid (cf. Section lILA.) by allopurinol is evidenced by an increased urinary excretion of 6-MP, an increase in the thiopurine ribonucleotides formed in tissues (ELION, 1975), an increased antitumor activity (ELION et aI., 1963; RUNDLES et aI., 1963; VOGLER et aI., 1966), and an increased toxicity of 6-MP in man and in animals (ELION et aI., 1963; LEVINE et aI., 1969; RAGAB et aI., 1974). One species which does not show this potentiation of toxicity is the rabbit (WALKER et aI., 1973), even though the rabbit does show an increased excretion of free 6-MP when given allopurinol at a dose of 50 mg/kg. In humans given high i.v. doses of 6-MP, allopurinol shows no effect on the plasma halflife of 6-MP (COFFEY et aI., 1972) although the production of TU is almost completely inhibited. Since the cytotoxicity of 6-MP is due not to the compound itself but to the nucleotides formed from it (HITCHINGS and ELION, 1972), the plasma halflife of 6-MP cannot be correlated with its biological activity. If the capacity of the enzyme systems for the conversion of 6-MP to its nucleotides is insufficient, excess 6-MP will be excreted. The potentiation of the antileukemic activity and toxicity of 6-MP in man (vide supra) have been demonstrated after oral administration of both 6-MP and allopurinol. A similar potentiation occurs with azathioprine, the immunosuppressive agent which is rapidly converted to 6-MP in vivo (ELION and HITCHINGS, 1975).
Several nitrofurans, e.g., nitrofurazone and 2-(2-furyl)-3-(5-nitro-2-furyl} acrylamide, act as electron acceptors for xanthine oxidase, and their metabolism is there-

502 GERTRUDE B. EUON
fore blocked by allopurinol (TATSUMI et aI., 1973). The reduction of the nitrothiazole niridazole by rat liver xanthine oxidase is also inhibited by allopurinol (MORITA et aI., 1971). The inhibition of hepatic cytosol nitroreductase activity may be related in rats to the enhancing effect of allopurinol on the bladder carcinogenicity of N-[4-nitro-(5-nitro-2-furyl)-2-thiazolyl] formamide (F ANFT) (WANG et aI., 1976); allopurinol does not alter the abnormal excretion of tryptophan metabolites related to F ANFT administration. Allopurinol has delayed or prevented bladder carcinogenesis in rats fed 2-acetaminofluorene with or without tryptophan (ROMAS et aI., 1973).
The oxidation of tolbutamide to carboxy tolbutamide, an inactive metabolite, is catalyzed by rat liver xanthine oxidase and aldehyde oxidase (McDANIEL et aI., 1969). GLOGNER (1970) has reported the excretion of smaller amounts of carboxytolbutamide in patients given allopurinol 1 h previously.
Allopurinol decreases the therapeutic efficacy of methotrexate against leukemia L 1210 in mice, presumably because of the decreased catabolism of systemic purines; this effect has not been observed in P288 leukemia (GRINDEY and MORAN, 1975). Coadministration of allopurinol does not alter the toxicity of methotrexate in normal mice.
Because oxipurinol is extensively reabsorbed in the kidney, several interactions occur among drugs which affect renal tubular reabsorption. Uricosuric drugs, e.g. probenecid, increase the excretion of oxipurinol (cf. Section IV). A high dose of aspirin (2.4-3.6 g/day) also increases oxipurinol excretion slightly (RUNDLES and ELION, unpublished), probably because of its uricosuric effect (YO and GUTMAN, 1959). Thiazide diuretics, which also inhibit the reabsorption of uric acid and oxipurinol, produce an increased effect of oxipurinol upon pyrimidine metabolism, as shown both by increased orotic acid and orotidine excretion and by increased levels of orotate phosphoribosyltransferase and orotidylate decarboxylase in erythrocytes (WOOD et aI., 1972, 1974). The increased excretion of pyrimidine metabolites produced by combined therapy with chlorthiazide and allopurinol amounts to approximately 15% of the total normal production compared to 10% or less with allopurinol alone. However, WOOD et aI. (1974) state: "It is doubtful if this interaction presents a sufficient challenge to the patient to contraindicate the use of the combination."
Allopurinol administration has some effect on the metabolism of drugs by liver microsomal enzymes. VESELL et al. (1970) report an increased plasma halflife of dicoumarol and antipyrine in man during allopurinol treatment, with large individual variations in the extent of this prolongation. In dogs given dicoumarol (2 mg/kg every other day) and allopurinol (50 mg/kg/day for 20 days) there has been no significant change in either the plasma level of dicoumarol or the prothrombin clotting times (WELCH, 1973), although the plasma halflife of antipyrine in dogs has been prolonged by allopurinol treatment in a dose-related fashion. RAWLINS and SMITH (1973) have found allopurinol to have no significant effect on steady-state plasma concentrations in patients given warfarin or phenylbutazone. If allopurinol affects the metabolism of dicoumarol in man, the extent of the interaction appears to be below the level of clinical significance.
Because allopurinol and probenecid are often given together in the treatment of tophaceous gout, the effect of allopurinol on the plasma halflife of probenecid has been of interest (TJANDRAMAGA et aI., 1972). In 8 out of 14 subjects, a prolongation of

Allopurinol and Other Inhibitors of Urate Synthesis 503
the t 1/2 of probenecid was found during concurrent allopurinol and probenecid treatment; however, there was very considerable individual variation. The increased excretion of oxipurinol caused by the uricosuric action of probenecid makes this drug interaction rather complex.
Cyclophosphamide is both activated and inactivated by liver microsomal enzymes. Although allopurinol prolongs the plasma halflife of cyclophosphamide itself, the plasma alkylating activity and the excretion of cyclophosphamide and its urinary metabolites remain unchanged (BAGLEY et aI., 1973). BAGLEY et ai. have concluded that alterations in the rate of cyclophosphamide metabolism by drugs in the absence of renal failure do not change toxicity or therapeutic effect. The Boston Collaborative Drug Surveillance Program (1974) reported from a retrospective study greater bone marrow depression in cancer patients given cyclophosphamide and allopurinol than in those given cyclophosphanide alone. LYON (1974) has questioned the interpretation of these data. In an animal study, ALBERTS and VAN DALLEN WETTERS (1975) found that allopurinol potentiated the antileukemic activity of cyclophosphamide while lowering its toxicity to normal marrow.
An increased incidence of ampicillin rashes has been reported in a retrospective study in hospitalized patients receiving allopurinol and ampicillin concomitantly (Boston Collaborative Drug Surveillance Program, 1972). As data on uric acid levels were not available, the authors felt that it was not clear whether the potentiation was due to allopurinol or to hyperuricemia.
V. Reduction of Urinary Calculi
The effectiveness of allopurinol in reducing uric acid urinary calculi (DE VRIES and FRANK, 1967; DE VRIES and SPERLING, 1974) is to be expected from its inhibitory effect on uric acid synthesis. The frequent occurrence of uric acid abnormalities in patients with calcium oxalate nephrolithiasis (COE and KAVALACH, 1974) and the fact that calcium oxalate stones are unusually common in patients with gout (PRIEN and PRIEN, 1968; GUTMAN and YO, 1968) suggest that hyperuricosuria and calcium oxalate stone formation might be related (SMITH and BOYCE, 1969; COE and RAISER, 1973). The success of allopurinol treatment in reducing the number of calcium oxalate stones in chronic stone formers has been encouraging (SMITH and BOYCE, 1969; COE and RAISER, 1973; SMITH, 1977; cf. Chapter by F. L. COE). The fact that sodium urate accelerates the precipitation of calcium oxalate in vitro (PAK and ARNOLD, 1975; COE et aI., 1975) provides an explanation for the effect of allopurinol, as the reduction of urinary urate concentration would make the heterogeneous nucleation of calcium oxalate stones less likely.
A patient with adenine phosphoribosyltransferase deficiency was found to produce urinary stones of 2,8-dihydroxyadenine (SIMMONDS et aI., 1976); allopurinol treatment effectively eliminated these stones. Since 2,8-dihydroxyadenine is the product of adenine oxidation via xanthine oxidase, this effect was anticipated.
J. Toxicology
The acute toxicity of allopurinol in rodents is very low, with an oral LD 50 = 700-2000 mg/kg in mice and an LD 50 = > 6000 mg/kg in rats (Burroughs Well come Co.,

504 GERTRUDE B.ELION
unpublished reports). Female mice and rats tolerate higher doses than do males (IWATA et aI., 1969, 1974). Chronic animal studies show that deaths are not due to the drug per se but are rather caused by concretions of xanthine in the kidneys (cf. Section III.C.). The smaller the animal, the higher the ratio of its purine endproduct to the water flux and the greater the danger of xanthine deposits (HITCHINGS, 1966). Dogs have tolerated oral doses of 30 mg/kg daily for a year without toxicity, but have also shown some kidney damage after a year on 90 mg/kg/day (Burroughs Wellcome Co., unpublished reports). Monkeys given very high i.v. doses of allopurinol (1300 mg/M2/day) for 14 days have shown some anemia and marrow hypocellularity as well as an interstitial nephritis produced by crystalline deposits of oxipurinol in the kidneys (KANN et aI., 1968). Oxipurinol urinary stones have also been reported in a child given daily doses of 15 mg/kg oxipurinol together with, 37.5 mg/ kg allopurinol (LANDGREBE et aI., 1975).
Allopurinol is well tolerated by most patients and serious complications in therapy are rare. The most common side-effect is a maculopapular skin rash which occurs in approximately 3% of all patients and which disappears upon discontinuation of the drug (SCOTT, 1966). A few extreme hypersensitivity reactions of the Stevens-Johnson type have been reported. Gastric irritation and malaise have been noted occasionally but usually do not require that the drug be dropped. Transient leukopenia, thrombocytopenia, leucocytosis, or eosinophilia occurs rarely. A few cases of hepatomegaly and elevated serum glutamic oxalacetic transaminase have been reported; these appear to be related to hypersensitivity to the drug. Patients with poor renal function have more side-effects than do others, possibly as a result of the poor clearance of oxipurinol.
K. Other Xanthine Oxidase Inhibitors
I. Thiopurinol
Another xanthine oxidase inhibitor currently in use for the reduction of hyperuricemia in man is thiopurinol (4-mercaptopyrazolo(3,4-d)pyrimidine), the 4-thio analog of allopurinol (DELBARRE et aI., 1968; SERRE et aI., 1970; GRAHAME et aI., 1974). Thiopurinol is a somewhat weaker competitive inhibitor of xanthine oxidase in vitro than is allopurinol (ELION et aI., 1968; DELBARRE et aI., 1968; CARTIER and HAMET, 1973) and shows a similar progressive inhibition of the enzyme due to the formation of the tighter binding inhibitor, 6-hydroxy-4-mercaptopyrazolo(3,4-d)pyrimidine (MASSEY et aI., 1970). As judged by the urinary excretion of metabolites in man (Au SCHER et aI., 1974) and by studies with radioactive compounds in the pig (SIMMONDS et aI., 1974), thiopurinol is not as well absorbed from the gastrointestinal tract as is allopurinol. No significant amount of thiopurinol is excreted unchanged; it is rapidly converted in vivo to its 6-hydroxy derivative (AuscHER et aI., 1974; GRAHAME et aI., 1974; SIMMONDS et aI., 1974). An indication that very little removal of the sulfur occurs in vivo is the virtual absence of oxipurinol in the urine after thiopurinol administration (ELION et aI., 1968; GRAHAME et aI., 1974; SIMMONDS et aI., 1974). Unlike allopurinol and oxipurinol, thiopurinol is bound to plasma and cellular proteins, and approximately 30% of the initially bound material is nondialyzable (DEAN et aI., 1974).

Allopurinol and Other Inhibitors of Urate Synthesis 505
It has been generally found that the urinary excretion of oxypurines (xanthine and hypoxanthine) does not rise as much after therapy with thiopurinol as with allopurinol (DELBARRE et aI., 1968; SERRE et aI., 1970; SIMMONDS et aI., 1974; GRAHAME et aI., 1974). This has been interpreted in the mouse as being due to the lower degree of xanthine oxidase inhibition achieved with thiopurinoI. To achieve similar amounts of oxypurine excretion in the mouse, it has been necessary to give a higher dose of thiopurinol (28 mg/kg) than of oxipurinol (12.5 mg/kg) or allopurinol (3.1 mg/kg) (ELION et aI., 1968). When equal doses of allopurinol and thiopurinol are administered to man, allopurinol is approximately twice as effective as thiopurinol in reducing serum urate. A dose of 200-300 mg/day of allopurinol produced reductions in serum urate of 35%, 37%, and 34%, while this dose of thiopurinol reduced serum urate an average of 22%, 26%, 13%, respectively, in three separate studies (DELBARRE et aI., 1968, 1968a; RYCKEWAERT, 1970). Since oxypurine excretion is related to the degree of xanthine oxidase inhibition (up to the point where reutilization of oxypurines occurs) (HITCHINGS, 1966), a lower degree of inhibition would be expected to produce lower oxypurine excretion.
It has been suggested (DELBARRE et aI., 1968) that, in man, thiopurinol may be a better pseudofeedback inhibitor of purine biosynthesis de novo than is allopurinol. The kinetics of the interactions of both thiopurinol and allopurinol with the HGPR Tase from human erythrocytes are comparable (KRENITSKY et aI., 1969; CARTIER and HAMET, 1973; AUSCHER et aI., 1974a), and there is no indication that the amounts of ribonucleotide formed from the two compounds are appreciably different. Both reduce PRPP levels in erythrocytes (CARTIER and HAMET, 1973). As the amount of allopurinol ribonucleotide formed in vivo is alone not high enough to inhibit PRPP amidotransferase (cf. Section VI), one might assume that thiopurinol ribonucleotide is a more potent inhibitor of the amidotransferase. No evidence for this is available. Patients deficient in HGPRTase show a decrease in uric acid excretion after allopurinol but not after thiopurinol treatment (DELBARRE et aI., 1970; GRAHAME et aI., 1974; AUSCHER et aI., 1974a). This is consistent with the poor in vivo xanthine oxidase inhibition by thiopurinol. Neither allopurinol nor thiopurinol had any effect on oxypurine excretion in a xanthinuric man who was apparently deficient in xanthine oxidase (AUSCHER et aI., 1974).
Thiopurinol administration to rats has resulted in an increased urinary excretion of orotic acid and orotidine similar to that seen with allopurinol administration (NELSON, unpUblished). SIMMONDS et aI. (1974) found no such increase in a study of pigs given 20 mg/kg thiopurinol twice daily; however, this dose also had no effect on the purine metabolism of the pigs. At higher doses (e.g. 300 mg/kg/day), thiopurinol did show a marked effect on allantoin excretion in the pig, but pyrimidine excretion has not been reported (GRAHAME et aI., 1976).
II. Other
There is a recent report of a new class of xanthine oxidase inhibitors, 3,5-disubstituted-1,2,4-triazoles (DUGGAN et aI., 1975). Several of these compounds have been found to depress urate synthesis in dogs and spider monkeys. No information about their activity in man is available.

506 GERTRUDE B. ELION
References
Ablin,A, Stephens,B.G., Hirata,T., Wilson,K., Williams,H.E.: Nephropathy, xanthinuria, and orotic aciduria complicating Burkitt's lymphoma treated with chemotherapy and allopurinol. Metabolism 21,771-778 (1972)
Alberts, D. S., Van Dallen Wetters, T.: Allopurinol potentiates cyclophosphamide antileukemic activity. Proc. Amer. Ass. Cancer Res. 16,84 (1975)
Alexander,J.A, Wheeler,G.P., Hill,D.D., Morris,H.P.: Effects of 4-hydroxypyrazolo(3,4-d)pyrimidine upon the catabolism of purines by various tissues of the rat and upon the rate of growth of Morris 5123-C hepatoma. Biochem. Pharmacol.15, 881-889 (1966)
Alken,C.E., May,P., Braun,J.s.: Analysis of treatment results in uric acid lithiasis with and without hyperuricemia. Advanc. expo Med. BioI. 41B, 535-540 (1974)
Auscher, c., Mercier, N., Pasquier, c.: Allopurinol and thiopurinol: effect in vivo on urinary oxypurine excretion and rate of synthesis of their ribonucleotides in different enzymatic deficiencies. Advanc. expo Med. BioI. 41B, 657--662 (1974a)
Auscher, c., Pasquier, c., Mercier, N., Delbarre, F.: Urinary excretion of 6-hydroxylated metabolite and oxypurines in a xanthin uric man given allopurinol or thiopurinol. Advanc. expo Med. BioI. 41B, 663-667 (1974)
Ayvazian,J. H.: Xanthinuria and hemochromatosis. New Engl. J. Med. 270, 18-22 (1964) Badawy,AA-B., Evans,M.: The mechanism of rat liver tryptophan pyrrolase activity by
4-hydroxypyrazolo[3,4-dJpyrimidine (allopurinol). Biochem. J. 133,585-591 (1973) Badawy,AA., Evans,M.: Tryptophan plus a pyrrolase inhibitor for depression? Lancet 197411,
1209-1210 Bagley, C. M., Jr., Bostick, F. W., De Vita, V. T., Jr.: Clinical pharmacology of cyclophosphamide.
Cancer Res. 33, 226-233 (1973) Baker, C. H.: Protection against irreversible haemorrhagic shock by allopurinol. Proc. Soc. expo
BioI. (N.Y.) 141, 694-698 (1972) Balis,M.E., Krakoff,I.H., Berman,P.H., Dancis,J.: Urinary metabolites in congenital hyperuri
cosuria. Science 156,1122-1123 (1967) Band, P. R., Silverberg,D. S., Henderson,J. F., Ulan,R. A, Wensel,R. H., Bannerjee, T. K., Lit
tle,A S.: Xanthine nephropathy in a patient with lymphosarcoma treated with allopurinol. New Eng!. J. Med. 283, 354-357 (1970)
Beardmore,T.D., Cashman,J.S., Kelley,W.N.: Mechanism of allopurinol-mediated increase in cultured human fibroblasts. J. clin. Invest. 51,1823-1832 (1972)
Beardmore, T. D., Kelley, W. N.: Mechanism of allopurinol-mediated inhibition of pyrimidine biosynthesis. J. Lab. clin. Med. 78, 696-704 (1971)
Becker,M.A, Argubright, K. F., Fox,R. M., Seegmiller,J. E.: Oxipurinol-associated inhibition of pyrimidine synthesis in human lymphoblasts. Molec. Pharmacol. 10,657-668 (1974)
Becking, G. c., Johnson, W. J.: The inhibition of tryptophan pyrrolase by allopurinol, an inhibitor of xanthine oxidase. Canad. J. Biochem. 45,1667-1672 (1967)
Becking,G.C., Johnson,W.1.: Pyrazolo- and triazolopyrimidines as inhibitors of tryptophan pyrrolase. Life Sci. 811, 843-851 (1969)
Boston Collaborative Drug Surveillance Program: Excess of ampicillin rashes associated with allopurinol or hyperuricemia. New Eng!. 1. Med. 286, 505-507 (1972)
Boston Collaborative Drug Surveillance Program: Allopurinol and cytotoxic drugs. Interaction in relation to bone marrow depression. J. Amer. med. Ass. 227, 1036-1040 (1974)
Boyett,J.D., Vogler,W.R., Furtado,V. deP., Schmidt,F.H.: Allopurinol and iron metabolism in man. Blood 32, 460--468 (1968)
Brown,G.K., Fox,R.M., O'Sullivan,W.J.: Alteration of quarternary structural behavior of an hepatic orotate phosphoribosyltransferase-orotidine-5' -phosphate decarboxylase complex in rats following allopurinol therapy. Biochem. Pharmaco!' 21, 2469-2477 (1972)
Brown, G. K., Fox,R. M., O'Sullivan, W.J.: Interconversion of different molecular weight forms of human erythrocyte orotidylate decarboxylase. J. bioI. Chern. 250, 7352-7358 (1975)
Buchanan,1.M., Flaks,J.G., Hartman,S. c., Levenberg,B., Lukens,L.N., Warren,L.: The enzymatic synthesis of inosinic acid de novo. In: Wolstenholme, G. E. W., O'Connor, C. M. (Eds.): Chemistry and Biology of Purines, Ciba Foundation Symposium, May 1956, pp. 233-252. Boston: Little Brown 1957

Allopurinol and Other Inhibitors of Urate Synthesis 507
Burroughs Wellcome Co.: Unpublished reports Byers, S. 0.: Xanthine oxidase studies. J. Amer. pharm. Ass. sci. Ed. 41, 611---613 (1952) Cartier, P. H., Hamet, M.: Mechanism of anti uric action of 4-oxy- and 4-thiopyrazolopyrimidines.
Biochem. Pharmacol. 22, 3061-3075 (1973) Chalmers,R. A., Kromer, H., Scott,J. T., Watts,R. W. E.: A comparative study of the xanthine
oxidase inhibitors allopurinol and oxipurinol in man. Clin. Sci. 35, 353-362 (1968) Chalmers,R.A., Parker,R., Simmonds,H.A., Snedden,W., Watts,R.W.E.: The conversIon of
4-hydroxypyrazolo[3,4-dJpyrimidine (allopurinol) into 4,6-dihydroxypyrazolo[3,4-dJpyrimidine (oxipurinol) in vivo in the absence of xanthine-oxygen oxido reductase. Biochem. J. 112,527-532 (1969)
Chatterjee, S. N., Berne, T. V.: Protective effect of allopurinol in renal ischemia. Amer. J. Surg. 131,658---659 (1976)
Chytil,F.: Activation of liver tryptophan oxygenase by adenosine 3',5'-phosphate and by other purine derivatives. J. bioI. Chern. 243, 893-899 (1968)
Clifford, A., Riumallo,J. A., BaIiga, B. S., Munro, H. N., Brown, P. R.: Liver nucleotide metabolism in relation to amino acid supply. Biochim. biophys. (Arnst.) Acta 277, 443--458 (1972)
Coe, F. L., Kavalach,A. G.: Hypercalciuria and hyperuricosuria in patients with calcium nephrolithiasis. New Engl. J. Med. 291,1344-1350 (1974)
Coe,F.L., Lawton,R.L., Goldstein,R.B., Tembe,V.: Sodium urate accelerates precipitation of calcium oxalate in vitro. Proc. Soc. expo BioI. (N.Y.) 149, 926-929 (1975)
Coe,F.L., Raiser,L.: Allopurinol treatment of uric acid disorders in calcium stone formers. Lancet 19731, 129-131
Coffey,J. J., White, C A., Lesk, A. B., Rogers, W. I., Serpick,A. A.: Effect of allopurinol on the pharmacokinetics of6-MP in cancer patients. Cancer Res. 32,1283-1289 (1972)
Crowell,J. W.: Oxygen transport in the hypotensive state. Fed. Proc. 29, 1848-1853 (1970) Crowell,J.W., Jones,CE., Smith,E.E.: Effect of allopurinol on hemorrhagic shock. Amer. J.
Physiol. 216, 744-748 (1969) Cunningham,S.K., Keaveny,T.V., Fitzgerald,P.: Effect of allopurinol on tissue ATP, ADP, and
AMP concentrations in renal ischaemia. Brit. J. Surg. 61, 562-565 (1974) Davis,P. S., Deller,D.J.: Effect of a xanthine oxidase inhibitor (allopurinol) on radio-iron absorp
tion in man. Lancet 1966 II, 470-472 Dean, B. M., Perrett, D., Simmonds, H. A., Grahame,R.: Thiopurinol: comparative enzyme inhibi
tion and protein binding studies with allopurinol, oxipurinol and 6-mercaptopurine. Brit. J. clin. Pharmacol.1, 119-127 (1974)
Delbarre,F., Auscher,C, De Gery,A., Brouilhet,H., Olivier,J.-L.: Le traitement de la dyspurinurie goutteuse par la mercapto-pyrazolopyrimidine (M.P.P.: thiopurinol). Presse med. 76, 2329-2332 (1968)
Delbarre,F., Auscher, C., Thang, K. V., Brouilhet,H., De Gery,A.: Effet de retro-action de certaines pyrazolopyrimidines sur Ie metabolisme de l'acide urique. CR. Acad. Sci. (Paris) 267, 2231-2234 (1968 a)
Delbarre, F., Cartier, P., Auscher, C, De Gery,A., Hamet, M.: Dyspurinies par deficit en hypoxanthine-guanine-phosphoribosyl-transferase. Frequence et caracteres cliniques de l'anenzymose. Presse med. 78, 729-734 (1970)
De Vries, A., Frank,M.: Prophylaxis of idiopathic and gouty uric acid lithiasis by allopurinol. Urol. int. 22, 505-516 (1967)
De Vries, A., Frank,M., Libermon, u.A., Sperling, 0.: Allopurinol in the prophylaxis of uric acid stones. Ann. rheum. Dis. 25, 691---693 (1966)
De Vries, A., Sperling,O.: Recent data on uric acid lithiasis. Adv. Nephrol. 3, 89-116 (1974) De Wall,R.A., Vasko, K. A., Stanley,E.L., Kezdi,P.: The responses of the ischemic myocardium
to allopurinol. Amer. Heart J. 82, 362-370 (1971) Duggan,D.E., Noll,R.M., Baer,J.E., Novello,F.C, Baldwin,J.J.: 3,5-Disubstituted-l,2,4-tria
zoles, a new class of xanthine oxidase inhibitor. J. med. Chern. 18, 900-905 (1975) Edmondson, D., Massey, V., Palmer, G., Beacham, L. M., III, Elion, G. B.: The resolution of active
and inactive xanthine oxidase by affinity chromatography. J. bioI. Chern. 247, 1597-1604 (1972)
Elion, G. B.: Unpublished

508 GERTRUDE B. ELION
Elion,G.B.: Enzymatic and metabolic studies with allopurinol. Ann. rheum. Dis. 25, 608-614 (1966)
Elion,G.B.: Interaction of anticancer drugs with enzymes. In: Pharmacological Basis of Cancer Chemotherapy, pp. 547-564. Baltimore Maryland: Williams and Wilkins Co. 1975
Elion, G. B., Benezra, F. M., Canellas, I., Carrington, L. 0., Hitchings, G. H.: Effects of xanthine oxidase inhibitors on purine catabolism. Israel J. Chern. 6, 787-796 (1968)
Elion,G.B., Bieber,S., Hitchings,G.H.: The fate of 6-mercaptopurine in mice. Ann. N.Y. Acad. Sci. 60, 297-303 (1954)
Elion, G. B., Callahan, S. W., Hitchings, G. H., Rundles,R. W., Laszlo,J.: Experimental, clinical, and metabolic studies of thiopurines. Cancer Chern other. Rep. 16, 197-202 (1962)
Elion,G.B., Callahan,S., Nathan, H., Bieber,S., Rundles,R.W., Hitchings,G.H.: Potentiation by inhibition of drug degradation: 6-substituted purines and xanthine oxidase. Biochem. Pharmacol. 12, 85-93 (1963)
Elion, G. B., Callahan, S., Rundles,R. W., Hitchings, G. H.: Relationship between metabolic fates and antitumor activities of thiopurines. Cancer Res. 23, 1207-1217 (1963 a)
Elion,G.B., Hitchings,G.H.: Azathioprine. In: Sartorelli,A.C., Johns,D.G. (Eds.): Handbook of experimental pharmacology, New Series, Vol. 38, Pt. 2, pp. 404--425. Berlin-Heidelberg-New York: Springer 1975
Elion,G.B., Kovensky,A., Hitchings,G.H., Metz,E., Rundles,R.W.: Metabolic studies of allopurinol, an inhibitor ofxanthine oxidase. Biochem. Pharmacol. 15, 863-880 (1966)
Elion, G. B., Mueller, S., Hitchings, G. H.: Studies on condensed pyrimidine systems XXI. The isolation of synthesis of 6-mercapto-2,8-purinediol (6-thiouric acid). J. Amer. chern. Soc. 81, 3042-3045 (1959)
Elion, G. B., Nelson,D. J.: Ribonucleotides of allopurinol and oxipurinol in rat tissues and their significance in purine metabolism. Advanc. expo Med. BioI. 41 B, 639-652 (1974)
Elion,G.B., Yu,T.-F., Gutman,A.B., Hitchings,G.H.: Renal clearance of oxipurinol, the chief metabolite of allopurinol. Amer. J. Med. 45, 69-77 (1968)
Ellis,C.H., Touw,K.B., Dickerson,S.W.: Some acute hemodynamic effects of large doses of sodium allopurinol in open-chested dogs. Arch. int. Pharmacodyn. Therap. 205, 355-367 (1973)
Emmerson, B. T.: Effect of allopurinol on iron metabolism in man. Ann. rheum. Dis. 25, 700---703 (1966)
Engelman, K., Watts,R. W. E., Klineberg,J.R., Sjoerdsma,A., Seegmiller,J. E.: Clinical, physiological and biochemical studies of a patient with xanthinuria and pheochromocytoma. Amer. J. Med.37,839-861 (1964)
Fox,1. H., Kelley, W. N.: Phosphoribosylpyrophosphate in man: biochemical and clinical significance. Ann. intern. Med. 74, 424--433 (1971)
Fox, 1. H., Wyngaarden, J. B., Kelley, W. N.: Depletion of erythrocyte phosphoribosylpyrophosphate in man-a newly observed effect of allopurinol. New Engl. J. Med. 283,117-1182 (1970)
Fox,R.M., Royse-Smith,D., O'Sullivan, W.l.: Orotidinuria induced by allopurinol. Science 168, 861-862 (1970)
Fox,R.M., Wood,M.H., O'Sullivan,W.J.: Studies on the coordinate activity and lability of orotidylate phosphoribosyl transferase and decarboxylase in human erythrocytes, and the effects of allopurinol administration. J. clin. Invest. 50,1050-1060 (1971)
Fyfe,J. A., Miller,R. L., Krenitsky, T. A.: Kinetic properties and inhibition of orotidine 5' -phosphate decarboxylase. J. bioI. Chern. 248, 3801-3809 (1973)
Fyfe,J.A., Nelson,D.J., Hitchings,G.H.: The molecular basis of the effects of allopurinol on pyrimidine metabolism. Adv. expo Med. BioI. 41B, 621-628 (1974)
Gevirtz, N. R.: Allopurinol and iron metabolism. Lancet 1967 11,715 Glogner,P.: Metabolism of tolbutamide and cyclamate. Hum. Genet. 9, 230-232 (1970) Goldfinger, S., Klinenberg, J. R., Seegmiller,J. E. : The renal excretion of oxypurines. J. clin. Invest.
44,623-628 (1965) Grace, N. D., Greenwald, M. A., Greenberg, M. S.: Effect of allopurinol on iron mobilization. Gas
troenterology 59, 103-108 (1970) Grahame,R., Simmonds,H.A., Cadenhead,A., Dean,B.M.: Metabolic studies of thiopurinol in
man and pig. Advanc. expo BioI. Med. 41B, 597-605 (1974)

Allopurinol and Other Inhibitors of Urate Synthesis 509
Grahame,R., Simmonds, H. A., Cameron,J. S., Cadenhead, A. : Thiopurinol: dose related effect on urinary oxypurine excretion. 1. clin. Chern. clin. Biochem. 14,291 (1976)
Grayzel,A., SeegmiIIer,J.E., Lane,E.: Suppression of uric acid synthesis in the gouty human by the use of 6-diazo-5-oxo-L-norieucine. J. clin. Invest. 39,447-454 (1960)
Green, A. R., Curzon, G.: Decrease of 5-hydroxytryptamine in the brain provoked by hydrocortisone and its prevention by allopurinol. Nature (Lond.) 220,1095-1097 (1968)
Green,R., Levin,N. W., Samassa,D., Charlton,R. W., Bothwell, T. H.: The effect of allopurinol on iron metabolism. S. Afr. med. 1. 42, 776-779 (1968)
Green,A.R., Woods,H.F., Joseph,M.H.: Tryptophan metabolism in the isolated perfused liver of the rat: effects of tryptophan concentration, hydrocortisone and allopurinol on tryptophan concentration, hydrocortisone and allopurinol on tryptophan pyrrolase activity and kynurenine formation. Brit. J. Pharmacol. 57, 103-114 (1976)
Greenberg,R.: Discussion. In: Wolstenholme,G.E.W., O'Conner,C.M. (Eds.): Chemistry and Biology of Purines, Ciba Foundation Symposium, May 1956, p. 267. Boston: Little Brown 1957
Greene,M. L., Fujimoto, W. Y., Seegmiller,J. E.: Urinary xanthine stones-a rare complication of allopurinol therapy. New Engl. J. Med. 280, 426-427 (1969)
Grindey,G.B., Moran,R.G.: Effects of allopurinol on the therapeutic efficacy of methotrexate. Cancer Res. 35,1702-1705 (1975)
Grobner, W., Kelley, W. N.: Effect on allopurinol and its metabolic derivatives on the configuration of human orotate phosphoribosyltransferase and orotidine 5' -phosphate decarboxylase. Biochem. Pharmacol. 24, 379-384 (1975)
Gutman, A. B., Yii,T.-F.: Uric acid nephrolithiasis. Amer. J. Med. 45, 756-779 (1968) Hamilton, L., Elion, G. B.: The fate of 6-mercaptopurine in man. Ann. N.Y. Acad. Sci. 60, 304-
314 (1954) Haskovec, L., Dostal, T., Jirak, R.: The action of allopurinol as an inhibitor of liver tryptophan
pyrrolase in depressions. Activ. nerv. sup. (Praha) 14,131-132 (1972) Hatfield, D., Wyngaarden,1. B.: 3-ribosylpurines. I. Synthesis (3-ribosyluric acid)5'-phosphate
and (3-ribosylxanthine)5' -phosphate by a pyrimidine ribonucleotide pyrophosphorylase of beef erythrocytes. J. bioI. Chern. 239, 2580-2586 (1964)
Hatfield, D., Wyngaarden,J. B.: II. Studies on (3-ribosylxanthine)-5' -phosphate and on ribonucleotide derivatives of certain uracil analogues. J. bioI. Chern. 239, 2587-2592 (1964a)
Hayes,C.P.,Jr., Metz,E.N., Robinson,R.R., Rundles,R.W.: The use of allopurinol (HPP) to control hyperuricemia in patients on chronic intermittent hemodialysis. Trans. Amer. Soc. artif. internal Org. 11,247-251 (1965)
Hillier,J., Hillier,J.G., Redfern,P.H.: Liver tryptophan pyrrolase activity and metabolism of brain 5-HT in rat. Nature (Lond.) 253,566-567 (1975)
Hitchings, G. H.: Effects of allopurinol in relation to purine biosynthesis. Ann. rheum. Dis. 25, 601---607 (1966)
Hitchings,G.H.: Allopurinol, an inhibitor of xanthine oxidase; physiological and biochemical studies. In: Shugar,D. (Ed.): FEBS Symposium, Biochemical Aspects of Antimetabolites and of Drug Hydroxylation, Vol. 16, pp. 11-22. London-New York: Academic Press 1969
Hitchings,G.H.: Crystals in skeletal muscle. Brit. med. 1. 1971IV, 555 (1971) Hitchings, G. H.: Indications for control mechanisms in purine and pyrimidine biosynthesis as
revealed by studies with inhibitors. In: Advances in enzyme regulation, Vol. 12, pp. 121-129. Oxford: Pergamon 1974
Hitchings, G. H.: Pharmacology of allopurinol. Arthr. and Rheum. 18, 863-870 (1975) Hitchings, G. H., Elion, G. B.: Mechanisms of action of purine and pyrimidine analogues. In:
Brodsky,!., Kahn,S.B., Moyer,J.H. (Eds.): Cancer Chemotherapy II, 22nd Hahnemann Symposium, pp. 23-32. New York: Grune and Stratton 1972
Hoenig, V., Brodanonva,M., Strejcek,J., Kordac,V.: Allopurinol and iron metabolism. Lancet 19671,387
Holmes,E.W., Mason,D.H., Goldstein,L.I., Blount,R.E., Kelley,W.N.: Xanthine oxidase deficiency: studies of a previously unreported case. Clin. Chern. 20, 1076-1079 (1974)
Hopkins,R.W., Abraham,J., Simeone,F.A., Damewood,C.A.: Effect of allopurinol on hepatic adenosine nucleotides in hemhorrhagic shock. J. Surg. Res. 19,381-390 (1975)

510 GERTRUDE B.EuON
Imai, S., Riley, A. L., Berne, R. M.: Effect of ischemia on adenine nucleotides in cardiac and skeletal muscle. Circulat. Res. 15,443---450 (1964)
Iwata,H., Yamamoto,!., Huh,K.: Sex differences in allopurinol oxidizing enzyme activity in mouse liver supernatant fraction. Biochem. Pharmacol. 23, 1144-1146 (1974)
Iwata, H., Yamamoto, 1., Muraki, K., Goda,E.: Sex differences of acute toxicity in rats and mice. In: 1st Symp. on Drug Metabolism and Action, Chiba, Japan, Nov. 1969, pp. 124-129
Jones, C. E., Crowell,J. W., Smith, E. E.: Significance of increased blood uric acid following extensive hemhorrage. Amer. J. Physiol. 214,1374-1377 (1968)
J ulian,J., Chytil, E.: Participation of xanthine oxidase in the activation of liver tryptophan pyrrolase. J. bioI. Chern. 245,1161-1168 (1970)
Kann, H. E., Jr., Wells,J. H., Galleli,J. F., Schein,P. S., Cooney,D. A., Smith, E. R., Seegmiller,J. E., Carbone,P. P.: The development and use of an intravenous preparation of allopurinol. Amer. J. med. Sci. 256, 53---63 (1968)
Kelley, W. N., Beardmore, T. D.: Allopurinol: Alteration in pyrimidine metabolism in man. Both allopurinol and oxypurinol inhibit de novo pyrimidine biosynthesis. Science 169, 388-390 (1970)
Kelley,W.N., Beardmore,T.D., Fox,1.H., Meade,J.C.: Effects of allopurinol and oxipurinol on pyrimidine synthesis in cultured human fibroblasts. Biochem. Pharmacol. 20, 1471-1478 (1971)
Kelley, W. M., Wyngaarden, J. B.: Effects of allopurinol and oxipurinol on purine synthesis in cultured human cells. J. clin. Invest. 49, 602---609 (1970)
Klinenberg,J. R., Goldfinger, S. E., Seegmiller,J. E.: Effectiveness of the xanthine oxidase inhibitor allopurinol in the treatment of gout. Ann. intern. Med. 62, 639---647 (1965)
Kozma, c., Salvador,R.A., Elion,G.B.: Allopurinol and iron storage. Lancet 196711,1040-1041 Kozma, c., Salvador, R. A., Elion, G. B.: Chronic allopurinol administration and iron storage in
mice. Life Sci. 7, 341-348 (1968) Krakoff,1.H., Meyer,R.L.: Prevention of hyperuricemia in leukemia and lymphoma. Use of
allopurinol, a xanthine oxidase inhibitor. J. Amer. med. Ass. 193,89-94 (1965) Krakoff,1.H., Murphy,M.L.: Hyperuricemia in neoplastic disease in children: prevention with
allopurinol, a xanthine oxidase inhibitor. Pediatrics 41, 52-56 (1968) Krenitsky, T.A.: Purine nucleoside phosphorylase: kinetics, mechanism, and specificity. Molec.
Pharmacol. 3, 526-536 (1967) Krenitsky, T. A.: Tissue distribution of purine ribosyl and phosphoribosyl-transferase in the
Rhesus monkey. Biochim. biophys. Acta (Arnst.) 179, 506-509 (1969) Krenitsky, T. A., Elion, G. B., Henderson, A. M., Hitchings, G. H.: Inhibition of human purine nu
cleoside phosphorylase. J. bioI. Chern. 243, 2876-2881 (1968) Krenitsky, T. A., Elion, G. B., Strelitz,R. A., Hitchings, G. H.: Ribonucleosides of allopurinol and
oxoallopurinol. J. bioI. Chern. 242, 2675-2682 (1967) Krenitsky, T. A., Mellors,J. W., Barclay,R. K.: Pyrimidine nucleosidases. Their classification and
relationship to uric acid ribonucleoside phosphorylase. J. bioI. Chern. 240,1281-1286 (1965) Krenitsky, T. A., Neil, S. M., Elion, G. B., Hitchings, G. H.: A comparison of the specificities of
xanthine oxidase and aldehyde oxidase. Arch. Biochem. Biophys. 150,585-599 (1972) Krenitsky, T. A., Papaioannau,R., Elion, G. B.: Human hypoxanthine phosphoribosyltransferase.
1. purification, properties, and specificity. J. bioI. Chern. 244, 1263-1270 (1969) Landgrebe,A.R., Nyhan, W.L., Coleman,M.: Urinary-tract stones resulting from the excretion of
oxipurinol. New Eng!. J. Med. 292, 626---627 (1975) Lazarus,H. M., Owens,M. L., Hopfenbeck,A.: Allopurinol protection of hepatic nuclear function
during hemorrhagic shock. Surg. Forum 25,10-12 (1974) Lefer,A.M., Daw,C.F., Berne,Q.M.: Cardiac and skeletal muscle metabolic energy stores in
hemorrhagic shock. Amer. J. Physio!. 216,483---486 (1969) Levin, N. W., Abrahams, O. L.: Allopurinol in patients with impaired renal function. Ann. rheum.
Dis. 25, 681---687 (1966) Levine,A.S., Sharp, H. L., Mitchell,J., Krewit,W., Nesbit,M.E.: Combination therapy with
6-mercaptopurine (NSC-755) and allopurinol (NSC-1390) during induction and maintenance of remission of acute leukemia in children. Cancer Chemother. Rep. 53, 53-57 (1969)
Lyon,G.M.: Allopurinol and cytotoxic agents. J. Amer. med. Ass. 228,1371 (1974)

Allopurinol and Other Inhibitors of Urate Synthesis 511
Manzke,H., Dorner,K.: Effect of allopurinol on erythrocyte ATP and a 2,3-diphosphoglycerate levels and hemoglobin oxygen affinity in man. Arch. clin. Pharmacol. Ther. 3, 107 (1975)
Massey,V., Komai,H., Palmer, G., Elion,G.B.: On the mechanism of inactivation of xanthine oxidase by allopurinol and other pyrazolo(3,4-d)pyrimidines. 1. bioI. Chern. 245, 2837-2844 (1970)
Massey, V., Komai, H., Palmer, G., Elion, G. B.: The existence of nonfunctional active sites in milk xanthine oxidase; reaction with functional active site inhibitors. Vitam. Horm. 28, 505-531 (1970a)
Mazur,A., Carleton, A. : Hepatic xanthine oxidase and ferritin iron in the developing rat. Blood 26,317-322 (1965)
Mazur, A., Green, S., Saha, A., Carleton, A.: Mechanism of release of ferritin in vivo by xanthine oxidase. l. clin. Invest. 37,1809-1817 (1958)
McCollister,R.l., Gilbert,W.R., Ashton,D.M., Wyngaarden,l.B.: Pseudofeedback inhibition of purine synthesis by 6-mercaptopurine ribonucleotide and other purine analogues. 1. bioI. Chern. 239,1560-1563 (1964)
McDaniel, H. G., Podgainy,H., Bressler,R.: The metabolism of tolbutamide in rat liver. l. Pharmacol. expo Ther. 167,91-97 (1969)
Miller, R. L., Adamczyk, D. L.: Inosine S -monophosphate dehydrogenase from sarcoma 180 cells-substrate and inhibitory specificity. Biochem. Pharmacoi. 25, 883-888 (1976)
Moon,R. l.: Tryptophan oxygenase and tryptophan metabolism in endotoxin-poisoned andallopurinol treated mice. Biochim. biophys. Acta (Arnst.) 230,342-348 (1971)
Morita,M., FeIIer,D.R., Gillette,l.R.: Reduction of niridazole by rat liver xanthine oxidase. Biochem. Pharmacol. 20, 217-226 (1971)
Nelson,D.l.: Unpublished Nelson,D.l., Bugge, c.1. L., Krasny,H. c., Elion,G.B.: Formation of nucleotides of 6_ 14C oxipu
rinol in rat tissues and effects on uridine nucleotide pools. Biochem. Pharmacol. 22, 2003-2033 (1973)
Nelson,D.l., Elion,G.B.: Metabolism of [6_ 14C] allopurinol-lack of incorporation of allopurinol into nucleic acids. Biochem. Pharmacol. 24,1235-1237 (1975)
Oster, K. A.: Treatment of angina pectoris according to a new theory of its origin. Cardiol. Dig. 3, 29-34 (1968)
Oster, K. A.: Plasmalogen diseases: a new concept of the etiology of the atherosclerotic process. Am. l. CIin. Res. 2, 30--35 (1971)
Owens, M. L., Lazarus, H. M., Wolcott, M. W., Maxwell,l. G., Taylor,l. B.: Allopurinol and hypoxanthine pretreatment of canine kidney donors. Transplantation 17,224-227 (1974)
Pak, C. Y. c., Arnold, L. H.: Heterogeneous nucleation of calcium oxalate by seeds of monosodium urate. Proc. Soc. expo BioI. (N.Y.) 149,930--932 (1975)
Parker,l.C., Smith,E.E.: Effects of xanthine oxidase inhibition in cardiac arrest. Surgery 71, 339-344 (1972)
Payne,M.R., Dancis,l., Berman,P.H., Balis,M.E.: Inosine kinase in leucocytes of Lesch-Nyhan patients. Exp. Cell Res. 59, 489---490 (1970)
Pomales,R., Bieber,S., Friedman,R., Hitchings,G.H.: Augmentation of the incorporation of hypoxanthine into nucleic acids by the administration of an inhibitor of xanthine oxidase. Biochim. biophys. Acta (Arnst.) 72, 119-120 (1963)
Pomales,R., Elion,G.B., Hitchings,G.H.: Xanthine as a precursor of nucleic acid purines in the mouse. Biochim. biophys. Acta (Arnst.) 95, 505-506 (1965)
Powell, L. W.: Effects of allopurinol in iron storage in the rat. Ann. rheum. Dis. 25, 697-699 (1966)
Powell, L. W., Emmerson, B. T.: Haemosiderosis associated with xanthine oxidase inhibition. Lancet 19661,239-240
Prien, E. L., Prien, E. L.: Composition and structure of urinary stone. Amer. l. Med. 45, 654-672 (1968)
Ragab,A. H., Gilkerson, E., Myers, M.: The effect of 6-mercaptopurine and allopurinol on granulopoiesis. Cancer Res. 34, 2246-2249 (1974)
Rawlins,M.D., Smith,S.E.: Influence ofaIIopurinol on drug metabolism in man. Brit. 1. Pharmacol. 48, 693-698 (1973)

512 GERTRUDE B. EUON
Rodnan, G. P., Robin,J. A., Tolchin, S. F., Elion, G. B.: Allopurinol and gouty hyperuricemia. Efficacy of a single daily dose. J. Amer. med. Ass. 231,1143-1147 (1975)
Romas, N., Fingerhut, B., Feigelson, P., Veenema, R.: Apparent inhibition of bladder carcinogenesis in the rat by allopurinol. Proc. Amer. Ass. Cancer Res. 14,95 (1973)
Rosenbloom,F.M., Kelley,W.N., Miller,J.M., Seegmiller,J.E.: An enzymatic biochemical basis for variation in response to allopurinol. Arthr. and Rheum. 10,307 (1967)
Rundles,R. W.: Allopurinol in gouty nephropathy and renal dialysis. Ann. rheum. Dis. 25, 694-696 (1966)
Rundles,R. W.: Metabolic effects of allopurinol and alloxanthine. Ann. rheum. Dis. 25, 615---620 (1966 a)
Rundles,R.W., Elion,G.B.: Unpublished Rundles,R. W., Elion, G. B., Hitchings, G. H.: Allopurinol in the treatment of gout and secondary
hyperuricemia. Bull. rheum. Dis. 161,400----403 (1966a) Rundles,R. W., Metz, E., Silberman,H. R.: Allopurinol in the treatment of gout. Ann. intern. Med.
64,229-258(1966) Rundles,R.W., Wyngaarden,J.B., Hitchings,G.H., Elion,G.B.: Drugs and uric acid. Ann. Rev.
Pharmacol. 9, 345-362 (1969) Rundles,R. W., Wyngaarden,J.B., Hitchings,G.H., Elion,G.B., Silberman,H.R.: Effects of a x an
thine oxidase inhibitor on thiopurine metabolism, hyperuricemia and gout. Trans. Ass. Amer. Phycns 76,126-140 (1963)
Ryckewaert,A.: Les indications du traitement de fond de la goutte. Cah. Med. 11, 669---673 (1970)
Scott,J. T. (Ed.): Symposium on allopurinol. Ann. rheum. Dis. 25(6), 599-718 (1966) Scott,J.T., Hall,A.P., Grahame,R.: Allopurinol in the treatment of gout. Brit. med. J. 196611,
321-327 Seegmiller,J.E., Engelman,K., Klinenberg,J.R., Watts,R.W.E., Sjoerdsma,A.: Xanthine oxidase
and iron. New Engl. J. Med. 270, 534-535 (1964) Seegmiller,J.E., Rosenbloom,F.M., Kelley,W.N.: Enzyme defect associated with a sex-linked
human neurological disorder and excess purine synthesis. Science 155, 1682-1684 (1967) Serre, H., Simon, L., Claustre,J.: Les urico-freinateurs dans Ie traitement de la goutte: a propos de
126 cas. Sem. Hop. Paris 46, 3295-3301 (1970) Shatney, C. H., MacCarter,D. J., Lillehei,R. c.: Effect of allopurinol, propanolol, and methylpred
nisolone on infarct size in experimental myocardial infarction. Amer. J. Cardiol. 37,572-580 (1976)
Simmonds, H. A.: Urinary excretion of purines, pyrimidines, pyrazolopyrimidines in patients treated with allopurinol or oxipurinol. Clin. chim. Acta 23(2),353-364 (1969)
Simmonds, H. A., Cadenhead, A., Cameron, J. S., Rising, T. J., Grahame,R., Dean, B. M.: Thiopurinol and purine metabolism. Metabolic and radioisotope studies. Ann. rheum. Dis. 33, 548-553 (1974)
Simmonds,H.A., Levin,B., Cameron,J.S.: Variations in allopurinol metabolism by xanthin uric subjects. Clin. Sci. molec. Med. 47, 173-178 (1974 a)
Simmonds, H. A., Van Acker, K.J., Cameron,J. S., McBurney,A., Snedden, W.: Purine excretion in complete adenine phosphoribosyltransferase deficiency: effect of diet and allopurinol therapy. J. din. Chern. din. Biochem. 14,321 (1976)
Sjoberg,K.-H.: Allopurinol therapy of gout with renal complications. Ann. rheum. Dis. 14,688-690 (1966)
Skipper, H. E., Robins,R. K., Thomson, J. R., Cheng, C. c., Brockman, R. W., Schabel, F. M. J r.: Structure activity relationships observed on screening a series ofpyrazalopyrimidines against experimental neoplasms. Cancer Res. 17,579-596 (1957)
Smith, M. J. V.: Placebo vs. allopurinol for renal calculi. J. Urol. (in press) (1977) Smith, M. J. V., Boyce, W. H.: Allopurinol and urolithiasis. J. Urol. 102,750-753 (1969) Sorensen,L.: Seminars on the Lesch-Nyhan syndrome; management and treatment, discussion.
Fed. Proc. 27, 1097(1968) Spector,T.: Inhibition of urate production by allopurinol. Biochem. Pharmacol. 26,355-358
(1977) Spector, T., Johns, D. G.: Stoichiometric inhibition of reduced xanthine oxidase by hydroxypyra
zoI0[3,4-dJpyrimidines. J. bioI. Chern. 245, 5079-5085 (1970)

Allopurinol and Other Inhibitors of Urate Synthesis 513
Spector,T., Johns,D.G.: 4-Hydroxypyrazolo(3,4-d)pyrimidine as a substrate for xanthine oxidase: loss of conventional substrate activity with catalytic cycling of the enzyme. Biochem. Biophys. Res. Commun. 38, 583-589 (1970a)
Stanley,E.L.: Allopurinol, a generalized coronary vasodilator. Circulation 43-44, 229 (1971) Sweetman,L.: Urinary and cerebrospinal fluid oxypurine levels and allopurinol metabolism in
the Lesch-Nyhan syndrome. Fed. Proc. 27, 1055-1058 (1968) Tatsumi,K., Yamaguchi,T., Yoshimura,H.: Metabolsm of drugs. LXXX. The metabolic fate of
nitrofuran derivatives. (3) Studies on enzymes in small intestinal mucosa of rat catalyzing degradation of nitrofuran derivatives. Chern. Pharm. Bull. (Tokyo) 21, 622---628 (1973)
Tax,W.lM., Veerkamp,J.H., Trijbels,F.J.M., SchretIen,E.D.A.M.: Mechanism of allopurinolmediated inhibition and stabilization of human orotate phosphoribosyltransferase and orQtidine phosphate decarboxylase. Biochem. Pharmacol. 25, 2025-2032 (1976)
Tersigni,R., Toledo-Pereyra,L.H., Najarian,J.S.: Effects of methylprednisolone, glucagon, and allopurinol in the protection of pancreaticoduodenal allografts perfused for twenty-four hours. Surgery 78, 599---607 (1975)
Tjandramaga,T.B., Cucinell,S.A, Iscaili,Z.H., Perel,J.M., Dayton,P.G., Yii,T.-F., Gutman,A.B.: Observations on the disposition of probenecid in patients receiving allopurinol. Pharmacology 8(4---6), 259-272 (1972)
Toledo-Pereyra, L. H., Najarian, J. S. : Total recovery of ischemic kidneys treated with allopurinol before transplantation. Surg. Forum 24, 302-304 (1973)
Toledo-Pereyra,L.H., Najarian,J.S.: Allopurinol on renal preservation. Transplantation 20, 256 (1975)
Toledo-Pereyra,L.H., Simmons,R.L., Najarian,J.S.: Protection of the ischemic liver by donor pretreatment before transplantation. Amer. J. Surg. 129,513-517 (1975)
Toledo-Pereyra,L.H., Simmons,R.L., Olson,L.C., Najarian,J.S.: Clinical effect of allopurinol on preserved kidney. A randomized double blind study. Ann. Surg. 185, 128-131 (1977)
Udall, V.: Hepatic iron storage. Ann. Rheum. Dis. 25, 704 (1966) Utter,M.F.: Guanosine and inosine nucleotides. In: Boyer,P.D., Lardy,H., Myrback,K. (Eds.):
The Enzymes, Vol. 2, pp. 75-88. New York: Academic Press 1960 Vasko,K.A, De Wall,R.A, Riley,AM.: Effect of allopurinol in renal ischemia. Surgery 71,
787-790 (1972) Vesell, E. S., Passanti, G. T., Greene, F. E.: Impairment of drug metabolism in man by allopurinol
and nortryptyline. New Engl. J. Med. 283,1484-1488 (1970) Vogler,W.R., Bain,lA, Huguley,C.M., Palmer,H.G.Jr., Lowrey,M.E.: Metabolic and thera
peutic effects of allopurinol in patients with leukemia and gout. Amer. l Med. 40, 548-549 (1966)
Walker,R.I., Horvath, W. L., Rule, W. S., Herion,J. c., Palmer,J. G.: The failure of allopurinol to enhance 6-mercaptopurine toxicity in rabbits. Cancer Res. 33, 755-758 (1973)
Wang, C. Y., Hayashida, S., Pamukcu,A M., Brian, G. T.: Enhancing effect of allopurinol on the induction of bladder cancer in rats by N-[4-(5-nitro-2-furyl)-2-thiazolyIJformamide. Cancer Res. 36,1551-1555 (1976)
Watts,R.W.E., Engelman,K., Klinenberg,J.R., Sjoerdsma,A, Seegmiller,J.E.: Enzyme defect in a case ofxanthinuria. Nature (Lond.) 201, 395-396 (1964)
Watts,R. W. E., Snedden, W., Parker,R.A: A quantitative study of skeletal-muscle purines and pyrazolo(3,4-d)pyrimidines in gout patients treated with allopurinol. Clin. Sci. 41, 153-158 (1971)
Watts,R. W. E., Watts,J. E. M., Seegmiller,J. E.: Xanthine oxidase activity in human tissues and its inhibition by allopurinol (4-hydroxypyrazolo-[3,4-dJpyrimidine). J. Lab. clin. Invest. 66, 688---698 (1965)
Way,J. L., Parks,R. E., Jr.: Enzymatic synthesis of 5' -phosphate nucleotides of purine analogs. J. bioI. Chern. 231, 467--480 (1958)
WeIch, R. M.: Drug-protein binding: A method for studying the interaction of drugs with bishydroxycoumarin (dicoumarol) in dogs. Ann. N.Y. Acad. Sci. 226, 259-266 (1973)
Wenzel ides, K., Guski, H., Seidler, E., Meyer, R. : The infl uence of allopurinol on the alterations in the myocardium and the frequency of myocardial infarction in the hearts of rats under various experimental conditions. Dtsch. Gesundh.-Wes. 30,183 (1975)

514 GERTRUDE B. EUON
Wenzelides, K., Meyer, R.: The influence of allopurinol upon the size of the experimental myocardial infarction in the rat. Dtsch. Gesundh.-Wes. 30, 229 (1975)
Westerfeld,W.W., Richert,D.A., Bloom,R.J.: Inhibition of xanthine and succinic oxidases by carbonyl reagents. J. bioI. Chern. 234,1889-1896 (1959)
Wood,M.H., O'Sullivan, W.J., Wilson,M., Tiller,D.J.: Potentiation of an effect of allopurinol on pyrimidine metabolism by chlorothiazide in man. Clin. expo Pharmacol. Physiol. 1, 53-58 (1974)
Wood,M. H., Sebel, E., O'Sullivan, W.J.: Allopurinol and thiazides. Lancet 1972 1,751 Worthy, T. E., Grobner, W., Kelley, W. N.: Hereditary orotic aciduria: evidence for structural
gene mutation. Proc. nat. Acad. Sci. (Wash.) 71, 3031-3035 (1974) Yii, T.-F., Balis, M. E., Krenitsky, T. A., Dancis,J., Silvers, D. N., Elion, G. B., Gutman, A. B.: Rarity
of X-linked partial hypoxanthine-guanine phosphoribosyltransferase deficiency in a large gouty population. Ann. intern. Med. 76, 255-264 (1972)
Yii, T.-F., Gutman,A. B.: Study of the paradoxical effects of salicylate in low, intermediate, and high dosage on the renal mechanisms for excretion of urate in man. J. clin. Invest. 38, 1298-1315 (1959)
Yii, T.-F., Gutman, A. B.: Effect of allopurinol (4-hydroxypyrazolo(3,4-d)pyrimidine) on serum and urinary uric acid in primary and secondary gout. Amer. 1. Med. 37, 885-898 (1964)
Zuckerman,R., Drell, W., Levin, M. H.: Urinary purines in gout: effect of azaserine. Arthr. and Rheum. 2, 46--47 (1959)

![Comparative Efficacy and Safety of Febuxostat and ... · a serum urate (sUA) ... solution of tophaceous deposits [4]. Allopurinol, ... safety at the final visit. We quantified the](https://img.pdfslide.net/doc/110x75/5b81c23c7f8b9a32738d1cd3/comparative-efficacy-and-safety-of-febuxostat-and-a-serum-urate-sua-.jpg)