Embed Size (px)
Citation preview

ALLOPURINOL IMPROVESMYOCARDIAL REPERFUSIONINJURY IN A XANTHINE OXIDASEFREE MODELSteven B. Hopson, MD, Robert M. Lust, PhD, You Su Sun, MD, Richard S. Zeri, MD,Ron F. Morrison, Masaki Otaki, MD, and W. Randolph Chitwood, Jr, MDGreenville, North Carolina
The ability of allopurinol to protect againstreperfusion injury in the heart has usually beenattributed to its xanthine oxidase (XO)-inhibiting properties. Human myocardium how-ever, has exhibited low levels of XO activity. Toinvestigate the effects of allopurinol in anXO-free model and determine whether pretreat-ment is necessary, 12 domestic pigs (15 kg to20 kg) underwent occlusion of the left circum-flex for 8 minutes followed by reperfusion for 4hours. One group received allopurinol infusion(5 mg/kg IV) at occlusion over 45 minutes and acontrol group (n = 6) received a saline infusion(same volume). Left ventricular and aorticpressure, electrocardiograms, and regionalwall motion (sonomicrometry) were monitoredthroughout the process. Regional blood flow(microspheres) were obtained before, during,and 5, 10, and 30 minutes after ischemia.Occlusion decreased transmural flow at themidpapillary level by 75% (0.28 versus 1.10mUminute/g). The allopurinol-treated groupexhibited a mild, generalized hyperemia at 5
From the Departments of Surgery and Physiology, EastCarolina University School of Medicine, Greenville, NorthCarolina. Presented at the 97th Annual Convention andScientific Assembly of the National Medical Association, August3, 1993, San Francisco, California. Third-place winner of theDrew-Walker Competitive Forum. Requests for reprints shouldbe addressed to Dr Robert M. Lust, Division of CardiothoracicSurgery, East Carolina University School of Medicine, Green-ville, NC 27858-4354.
minutes (ischemic zone: 1.44 versus 1.10 mUmin/g, which returned to control levels at 10and 30 minutes. In contrast, the control groupwas associated with only 80% restoration ofresting blood flow at 5 minutes (0.84 versus1.10 mUmin/g), which stabilized at 63% ofcontrol levels at 10 and 30 minutes. Whenevaluated for the propensity of arrhythmiasusing an arbitrary arrhythmia score, the al-lopurinol group demonstrated no myocardialectopy when compared with the focal ectopyroutinely encountered in the control group atall time intervals. Since pigs have no detectablelevels of XO activity, allopurinol must exert itsprotectant effect during myocardial reperfu-sion by an alternative mechanism. Becauseprotection was evident without pretreatment,beneficial effects may not necessarily be theresult of allopurinol degradation products;therefore, pretreatment with allopurinol maynot be necessary. These results are clinicallyimportant when considering the use of allopuri-nol in an emergent coronary angioplasty orcoronary artery bypass grafting. (J Nati MedAssoc. 1995;87:480-484.)
Key words * pretreatment. oxypurinol * swine- myocardial shortening * microspheres
Restoration of myocardial function following globalischemia associated with cardioplegic arrest and coro-nary artery bypass surgery is a major concern to
480 JOURNAL OF THE NATIONAL MEDICAL ASSOCIATION, VOL. 87, NO. 7

ALLOPURINOL IN SWINE
cardiothoracic surgeons. Poorly contracting myocar-dium caused by reperfusion of previously ischemictissue produces an injury, or "stun," that is believed tobe a factor in the induction of fatal arrhythmias andheart failure, which ultimately may lead to death.'
In an attempt to reduce this injury, the effectivenessof several pharmacological interventions have beeninvestigated, including glucose, insulin, potassium,hyaluronidase, (3-blockers, and calcium channel antago-nists.1.2 More recently, therapies directed at reducingthe impact of reactive oxygen species, oxygen-derivedfree radicals (ODFRs), have generated much scrutiny.One such therapeutic agent is allopurinol.
Beneficial effects observed with allopurinol in thesetting of ischemia and reperfusion injury in themyocardium have been attributed to its ability to reducethe formation of ODFRs by inhibiting the enzymeXO.3-6 However, these data largely have been generatedfrom animal models (dogs and rats), which havedemonstrated substantial XO enzyme activity. How-ever, allopurinol also has been reported as therapeutic inanimal systems with no detectable XO activity.7-8Human myocardial biopsies have demonstrated verylittle XO enzymatic activity.6 Therefore, the exact roleof allopurinol in limiting the effects of ODFRs andmyocardial reperfusion injury remains uncertain.Clearly, the data suggest that allopurinol reducesmyocardial reperfusion injury by mechanisms otherthan inhibition of XO-generated ODFRs. At least onesuggestion is that pretreatment with allopurinol leads toaccumulation of the degradation product oxypurinol,which has ODFR-scavenging effects.8 To furtherevaluate the efficacy of allopurinol and/or pretreatment,a "stun" paradigm was investigated in a pig modelwhich has been shown to exhibit no XO activity.6,8
METHODSTwelve domestic pigs (15 kg to 20 kg) were
anesthetized using sodium pentobarbital (10 mg/kgbolus; 7 mg/kg/hour infusion), intubated, and venti-lated with positive pressure and room air. A mediansternotomy was performed. Left atrial, left ventricu-lar, arterial, and venous cannulas were placed. Pairsof sonomicrometry crystals were placed in thedistribution of the circumflex (ischemic, posterior)and the anterior (control) descending coronary arter-ies. Segment length was measured according toelectrocardiogram (ECG)-gated times for end-systoleand end-diastole, and relative shortening was calcu-lated as an index of myocardial function in eachregion.
2.000
1.7500
1.500 ~~~~~~~~(pe-O5) vs Control
-' 150
1.250
0 1.000 ~~~~~~~~~~Ailopurinol
0 .000 _
-j
a 5075500-J
0.500 Saline
0.250
0.0000 10 30
CONTROL ISCHEMIA REPERFUSION (min)
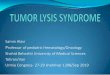
Figure 1. Mean transmural blood flow in theposterior papillary region. Note that bothgroups showed significant decreases duringocclusion, as expected, while only the al-lopurinol-treated group demonstrated remark-able hyperemia and restoration of baselineflows during reperfusion.
The left circumflex artery was gently dissected freeof interstitial connections, and a snare was placed.The animal was then allowed to stabilize. Followingstabilization, local occlusion of the left circumflexartery was accomplished and maintained for 8minutes. After the 8-minute ischemic period, the leftcircumflex artery was reopened and allowed toreperfuse the ischemic myocardium for a period of 4hours. One group (n = 6) received an intravenousallopurinol infusion (5 mg/kg) beginning at the timeof occlusion and continuing for 45 minutes (37thminute of reperfusion). A second group (n = 6)received a comparable saline infusion (vehicle con-trol) over the same period. Left ventricular and aorticpressure, ECG (lead II), and regional wall motion(sonomicrometry) were monitored and recordedthroughout the experiment.
Regional myocardial blood flow, using the refer-ence withdrawal method as established in ourlaboratory,9 was determined using microspheresbefore, during, and 5, 10, and 30 minutes afterischemia was produced. At the end of the experiment,the animal was killed by lethal overdose, and theheart was removed. After formalin fixation for 5days, the myocardium was sectioned, and tissue wasanalyzed for radioactivity, which was then convertedto flow by computer analysis and normalized forsample weight. This produced final blood flowmeasurements expressed in mL/minutes/g.An arrhythmia score was developed: 0= no ectopy,
JOURNAL OF THE NATIONAL MEDICAL ASSOCIATION, VOL. 87, NO. 7 481

ALLOPURINOL IN SWINE
1.500
l1 l' (p<.O5) vs Control
B., k ~~~~~~~~~~Allopurinolo 1.000 l
U.a00-j
0.5005 10 30
CONTROL ISCHEMIA REPERFUSION (min)
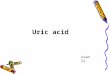
Figure 2. Mean transmural flow in the anteriorpapillary region. Note that the allopurinol-treated group displayed a significant hypere-mia during the occlusive episode in the adja-cent region, which was sustained early duringreperfusion. Blood flow patterns later duringreperfusion were not significantly different.
no tachycardia; 1 = isolated ventricular ectopy orperiods of sinus tachycardia; 2 =interrupted runs ofventricular tachycardia (V-tach); 3 = sustained V-tach (continuously for 10 seconds); and 4 = ventricu-lar fibrillation. Arrhythmogenicity during ischemicand reperfusion periods was evaluated.
All experiments were conducted under protocolsapproved by the institutional animal care and usecommittee, and methods of anesthesia and euthanasiawere consistent with National Institutes of Healthguidelines. All data were analyzed using multivariateanalysis of variance for repeated measures, usingDunnett's multiple range test as appropriate. Signifi-cance was determined when P<.05.
RESULTSBlood Flow
Occlusion of the left circumflex artery decreasedtransmural blood flow 75% in both groups (0.28versus 1.10 mL/minutes/g; P<.01). During reperfu-sion, the allopurinol-treated group demonstrated amild, generalized hyperemia at 5 minutes that wassignificantly greater than baseline (1.44 versus 1.10mL/minutes/g; P<.01). In addition, the allopurinol-treated group sustained baseline blood flow levels at10 and 30 minutes of reperfusion. In contrast, thesaline group exhibited a defective reperfusion. At 5minutes of reperfusion, flow remained 20% belowbaseline (0.84 versus 1.10 mL/minutes/g; P<.05). At10 and 30 minutes, the untreated group showed afurther decrease in adequate reperfusion. Blood flow
stabilized at only 63% of baseline levels. In sum-mary, allopurinol was associated with preservation ofphysiologic reactive hyperemia and preservation ofnormal flow distribution during reperfusion. Bothwere defective in comparable controls (Figure 1). Inaddition, allopurinol treatment was associated withimproved perfusion to the nonischemia anteriorsegments during occlusion (Figure 2). The improvedhyperemia in the nonischemic segments may haveimportant ramifications in supporting compensatoryrecruitable wall motion adjacent to the ischemictissue.
ArrhythmogenicityUsing the defined arrhythmia score, the propensity of
the reperfused myocardium to develop arrhythmias wasevaluated. The allopurinol-treated group demonstratedno myocardial ectopy, while dramatic, focal, andmyocardial ectopy was routinely encountered in theuntreated group at all time intervals (P<.05).
Wall MotionIn general, allopurinol treatment did not have a
significant effect on wall motion in the nonischemicmyocardium, except during the immediate occlusion,when there was a remarkable retention of shorteningcompared with saline-treated groups (Figure 3).Thus, in the nonoccluded region, the effect ofallopurinol is manifest during ischemia in theadjacent region, but little effect was observed duringreperfusion. In contrast, wall motion in the occludedregion was not preserved in the allopurinol-treatedgroup; however, with reperfusion, allopurinol treat-ment was associated with a much stronger, sustainedrecovery of myocardial shortening (Figure 4). To-gether, both wall motion data and perfusion datasuggest a bimodal efficacy for allopurinol treatment,with a beneficial effect during occlusion manifest inthe nonischemic tissue beds, and a beneficial effectduring reperfusion in the previously ischemic tissuebut not the nonischemic tissue.
DISCUSSIONAllopurinol has been suggested to improve myocar-
dial reperfusion injury by reducing the number ofODFRs secondary to competitive inhibition of XO.3-5Xanthine oxidase uses molecular oxygen as an electronacceptor.5 These ODFRs are able to produce myocar-dial alterations characteristic of ischemic-reperfusioninjury, including disruption of plasma membranes andlysosomes, damage to mitochondria and sarcoplasmic
482 JOURNAL OF THE NATIONAL MEDICAL ASSOCIATION, VOL. 87, NO. 7

ALLOPURINOL IN SWINE
130
110
90D.
0' 30 60 120 180 240.REPERFUSION.(miii
Figure 3. Change from baseline in shorteningfraction in the anterior region. Note that whileshortening was generally comparablethroughout the experiment, during the occlu-sion of the adjacent region, allopurinol wasassociated with wall motion preservation thatwas 10% better than the control group. Whilethis may not be a factor in otherwise-normalmyocardium, as in these experiments, thisdifference may be important in diseased myo-cardium.
reticulum, increases in vascular permeability, and theinitiation of ventricular arrhythmias.1
Despite this observation, the involvement of XO andallopurinol in myocardial preservation during ischemic-reperfusion remains unclear. The activity of XO hasvaried from one study to another, as well as fromspecies to species, which is also confusing. No XOactivity has been reported in pig myocardium. Simi-larly, rabbit and human myocardial biopsies haveexhibited little XO enzymatic activity. However,moderate to high levels of XO have been detected inboth dogs and guinea pigs.6
Using the pig model, our results demonstrate thatallopurinol does have beneficial and protectiveeffects during myocardial reperfusion after an acute,non-necrosing ischemic period. Since no XO enzymeactivity was present in this model, the beneficialeffects observed with allopurinol administrationmust be attributed to a mechanism other thaninhibition of XO.The allopurinol-treated group exhibited superior resto-
ration of blood flow during the reperfusion period whencompared to the untreated group. Myocardial ectopy alsowas reduced dramatically in the allopurinol-treated group.Our data are consistent with other investigations whichhave shown allopurinol to exert beneficial effects in
o 1 L1_ 1 {(p<.05) vs Control0 1.ous~~~~~~~~~~~~o
0-.
Fiur 4.Canefombseie inshrenin
Z 0
60Mi
0 .30 60-. 120. 180 '240-REPERFUSION (min)
Figure 4. Change from baseline in shorteningfraction in the posterior region. Note that, incontrast to the anterior region, no effect ofallopurinol treatment could be demonstratedduring ischemic occlusion. However, onreperfusion, a sustained recovery in shorten-ing was observed. Allopurinol was associatedwith a full recovery of wall motion in thepreviously ischemic tissue within 30 minutes,while saline control had recovered only 75% ofbaseline function as late as 4 hours afterreperfusion had been established.
rabbit hearts, the rabbit being an animal that also isreported to have little XO activity.'Many factors are believed to contribute to the
generation of reperfusion injury. In general, these factorsmay be categorized into three groups: injuries related toultrastructural damage and the inability to regulatecalcium flux, injuries related to the production of ODFRs,and injuries that result from acute inflammatory re-sponses in the previously ischemic region.7 Das et al8used biochemical analysis to demonstrate that bothoxypurinol and allopurinol may salvage myocardialfunction during ischemia and reperfusion by scavengingODFRs rather than by inhibiting XO. Together, these datasuggest that xanthine oxidase probably is not the principalsource of ODFRs and that allopurinol has a directscavenging effect on ODFRs.
Certain protective actions of allopurinol, such as thepreservation of cellular adenosine triphosphate (ATP)levels and of mitochondrial ATP-generating capacity,have been shown to be exerted predominantly during theischemic phase of injury. Other beneficial actions, such aspreventing a decrease in left ventricular pressure,decreasing sodium and calcium accumulation, andpreserving sarcolemmal and sarcoplasmic reticularATPases, are greater during the reperfusion phase ofinjury. This would imply that the molecular processes
JOURNAL OF THE NATIONAL MEDICAL ASSOCIATION, VOL. 87, NO. 7 483

ALLOPURINOL IN SWINE
determining cellular injury are mechanistically differentduring these two phases.' Beneficial effects observedwith allopurinol may be exerted at different phases ofinjury.
In addition, our data clearly show that the protectiveeffects do not depend on pretreatment, suggesting thatimproved recovery may not require allopurinol degra-dation to oxypurinol. Therefore, pretreatment withallopurinol may not be necessary, as was the case in ourstudy. This is an important clinical consideration whentreating a patient suffering from an acute ischemic event.
Xanthine oxidase catalyzes the irreversible oxidationof hypoxanthine to xanthine and to uric acid, possiblyaccelerating the ischemic breakdown of purine nucleo-sides and bases that are needed for the resynthesis of ATPduring reperfusion.6,"0 DeWall et al2l' have suggestedthat XO inhibition might be protective by facilitatingpurine salvage, thereby enabling ischemic tissues tomaintain their ATP scores. However, others havesuggested that this mechanism is unlikely because thewashout of nucleotide degradation products is too rapid. 12
SUMMARYDespite controversy, there is a growing body of
evidence to support the theory that allopurinol exhibitsits beneficial effects by more than one mechanism andpathway. The results of this study demonstrate clearlythat allopurinol exerts a significant protective effectduring myocardial reperfusion injury by mechanisms orpathways other than the inhibition of XO, and pretreat-ment with allopurinol is not required. Future studies tospecifically identify these mechanisms and pathways,as well as dosage strategies, are needed.
AcknowledgmentsThe authors thank Roshanak Etemad-Moghadam for techni-
cal assistance and Mike Dulude for the illustrations.
Literature Cited1. Godin DV, Bhimji S. Effects of allopurinol on myocardial
ischemic injury induced by coronary artery ligation and reperfu-sion. Biochem Pharmacol. 1987;34:2101-2107.
2. Arnold WL, Dewall RA, Kezdi P, Zwart HH. The effect ofallopurinol on the degree of early myocardial ischemia. AmHeart J. 1980;99:614-624.
3. Werns SW, Shea MJ, Mitsos SE, Dysko RC, FantoneJC, Schork MA, et al. Reduction of the size of infarction byallopurinol in the ischemic-reperfused canine heart. Circulation.1 986;73:51 8-524.
4. Stewart JR, Blackwell WH, Crute SL, Loughlin V,Greenfield LJ, Hess ML. Inhibition of surgically inducedischemia/reperfusion injury by oxygen free radical scavengers.J Thorac Cardiovasc Surg. 1983;86:262-272.
5. Stewart JR, Crute SL, Loughlin V, Hess ML, GreenfieldLJ. Prevention of free radical-induced myocardial reperfusioninjury with allopurinol. J Thorac Cardiovasc Surg. 1985;90:68-72.
6. Muxfeldt M, Schaper W. The activity of xanthine oxidasein heart of pigs, guinea pigs, rabbits, rats, and humans. BasicRes Cardiol. 1987;82:486-492.
7. Lust RM. Physiologic influences of alterations in coro-nary anatomy on cardioplegia and reperfusion. Cardiac Sur-gery: State of the Art Reviews. 1988;2:351-381.
8. Das DK, Engelman RM, Clement R, Otani H, PrasadMR, Rao PS. Role of xanthine oxidase inhibitor as free radicalscavenger: a novel mechanism of action of allopurinol andoxypurinol in myocardial salvage. Biochem Biophys ResCommun. 1987;148:314-319.
9. Lust RM, Beggerly CE, Morrison RF, Austin EH,Chitwood WR, Jr. Improved protection of chronically inflow-limited myocardium with retrograde coronary sinus cardiople-gia. Circulation. 1 988;78(suppl 3):217-223.
10. Wexler BC, McMurtry JP. Allopurinol amelioration of thepathophysiology of acute myocardial infarction in rats. Athero-sclerosis. 1981;39:71-87.
11. DeWall RA, Vasko KA, Stanley EL, Kezdi P. Responsesof the ischemic myocardium to allopurinol. Am Heart J.1971;82:362-370.
12. Chambers DE, Parks DA, Patterson G, Roy R, McGrodJM, Yoshida S, et al. Xanthine oxidase as a source of freeradical damage in myocardial ischemia. J Mol Cell Cardiol.1985;17:145-152.
484 JOURNAL OF THE NATIONAL MEDICAL ASSOCIATION, VOL. 87, NO. 7