Embed Size (px)
Citation preview

I
“ALVEOLAR AND SYMPHYSIS REGION CHARACTERISTICS OF
PATIENTS WITH SKELETAL CLASS III MALOCCLUSION –A
CEPHALOMETRIC STUDY”
By
DR. KISHOR KUMAR
Dissertation Submitted to the
Rajiv Gandhi University of Health Sciences,
Bengaluru, Karnataka
In partial fulfillment
of the requirements for the degree of
MASTER OF DENTAL SURGERY
In
ORTHODONTICS
&
DENTOFACIAL ORTHOPAEDICS
Under the guidance of
Dr. ASHOK KUMAR TALAPANENI M.D.S
Professor & Head
DEPARTMENT OF
ORTHODONTICS & DENTOFACIAL ORTHOPAEDICS
AL-BADAR RURAL DENTAL COLLEGE AND HOSPITAL,
GULBARGA.
2015 - 2018



ACKNOWLEDGEMENT
At the very outset, I would like to thank the Almighty for making this task possible with
his blessings, providing and infusing me with enough strength to carry out this work and being
with me in all my endeavours.
My respects and deepest gratitude to my guide Dr. Ashok Kumar Talapaneni
Professor & Head,, Department of orthodontics and dentofacial orthopaedics, Al- Badar
Rural Dental College & Hospital, Kalaburagi. I have been very fortunate to have an advisor
who gave me the freedom to explore on my own and at the same time the guidance to recover
when my steps faltered.
I take this opportunity to express my gratitude to him for his keen interest and constant
encouragement during every stage of this library dissertation. He stood as pillar by me
throughout the inscription of this library dissertation and guided me throughout my work.
I cannot forget the support provided to me by, Dr.Prasad Konda, Professor, Dr.Avinash
kumar MDS Reader, Dr.Saravanan MDS, Reader, Dr Arshad MDS, Reader, Dr. Chandrika
MDS, Assistant Professor, Dr. Laeque MDS, Assistant Professor, Dr. Asma MDS, Assistant
Professor, Dr. Ayub MDS, Assistant Professor from the department of Orthodontics and
dentofacialorthopaedics, Al-Badar Rural Dental College and Hospital, Gulbarga, for whom I
remain always thankful.
I thank the librarian Mr.Jagannath Maski and the library staff for giving their valuable
support to utilize the library facility for my study.
My sincere thanks to my seniors Dr. Arifa, Dr. Meenakshi, Dr.Suresh, Dr.Rajesh,
Dr.Shreyas and Dr. Imran, Dr.Abdul Saleh, Dr.Nisar, Dr. Hajra, Dr. Samiullah
and my batchmates Dr Faiza, Dr. Kirmani, Dr. Mujeeb and Dr.Meghna who kept me aloft
during the entire course, and I am also thankful to my beloved juniors, Dr. Kamala, Dr. Rekha,
Dr. Javeria, Dr.Praveen, Dr. Mujtaba, Dr. Rony, Dr.Sujith, Dr. Fareed, Dr. Aftab, Dr.
Archana and the non-teaching staff of my department Mr.Gani, Mr.Chandru, and Mr. Noor
whose association was a source of great help.


V
LIST OF ABBREVATIONS USED
PP - Palatinal plane
MP - Mandibular plane
L1–AH - Mandibular incisor dentoalveolar height
L6–AH - Mandibular molar dentoalveolar height
U1–AH - Maxillary incisor dentoalveolar height
U6–AH - Maxillary molar dentoalveolar height
Id – Anterosuperior
Id′- Posterosuperior
B′ - Lingual projection of the B point at the lingual symphysis border

VI
LIST OF TABLES
SI.No Tables Pages
1. Landmarks and Definition 18
2. Intergroup comparison of skeletal parameters 21
3. Intergroup comparison of various maxillary parameters 22
4. Intergroup comparison of mandibular parameters 23
5. Intergroup comparison of symphysis parameters 24

VII
LIST OF FIGURES
SI.No Figures Pages
1. Dentoalveolar and Symphysis Parameters 19

Abstract
IX
ABSTRACT
Title: “Alveolar And Symphysis Region Characteristics Of Patients With Skeletal
Class
III Malocclusion – A Cephalometric Study”.”
Objectives: To investigate the differences in the properties of the alveolar and
symphysis regions of patient with skeletal class III malocclusion and a Class I control
group.
.Materials and methods: Pretreatment lateral cephalograms of 80 patients is divided
into 50 lateral cephalograms from subject of class-І malocclusion (control group) and,
30 lateral cephalograph of skeletal class-ІІІ malocclusion. The heights and widths of
the symphysis and alveolus and depth of maxillary palate is measured on the lateral
cephalograms and analyzed.
All cephalograms are traced manually by a single examiner using a protractor 0.5°
and with 0.5 mm accuracy. The data obtained will be evaluated and subjected to
statistical analysis. The cephalometric data of the control and Class III groups were
presented as a mean ± SD. The results were inferred by analysis of variance
(ANOVA) using statistical software (SPSS version 23). P < 0.05 was considered
significant.
Results: The skeletal Class III cross bite group showed a larger SNB, ANB and AO-
BO measurements compared with the control group. The maxillary incisal dento
alveolar height has an insignificant difference between the two groups. Class I control
group had a significantly lesser mandibular plane angle than the Class III. Mandibular

Abstract
X
incisal inclinations were significantly greater in Class I control group than in Class III
cross bite group (P<0.001**).
Conclusion: Mandibular incisal dento alveolar height and mandibular molar dento
alveolar height were significantly greater in the Class III cross bite group than in the
Class I control group. Symphysis height and width were significantly greater in the
Class III cross bite group than in the Class I control group.
Keywords: Lateral cephalograms, symphysis, maxillary palate

Introduction
1
INTRODUCTION
Class III malocclusion is a significant problem that can be disturbing both
socially and functionally. Many factors have been implicated in its etiology and a
strong genetic background has been established in literature. The prevalence of class
III malocclusion varies according to ethnicity; it is high among Asians of the Far East
(12%) and low in Caucasians (1-4%).1
Facial types of a multidimensional nature are derived from the combination of
anteroposterior and vertical dimensions. Teeth, muscles, and bones interact intimately
during growth, increasing or masking initial deformities.2 Disproportions and
malpositions of the structures often lead to malocclusions or facial deformities.3
In orthodontics, knowledge of mandibular growth is highly beneficial in
diagnosis and treatment planning and is critical in the development of balanced
dentofacial structures4. Mandibular rotation types have been well defined by several
authors.5,6
It was stated that some additional growth at the major growth sites
accompanied by mandibular rotation and remodeling tend to reshape the mandible.
These remodeling changes described for the inferior mandibular border have been
related to rotational changes in the mandible.7 Anterior rotation is generally associated
with deposition in the inferior aspect while posterior\ rotation is associated with
resorption.8 These remodeling processes were thought to be indirectly related to the
nature of the stresses generated by the supra-hyoid musculature.3
It is believed by some authors that the symphysis region properties could be a
good indicator of mandibular rotation.4,5,9,10
The symphysis is one of the most
important regions of the craniofacial complex for clinical orthodontists, and it serves
as a primary reference for esthetic considerations in the lower one-third of the face.7

Introduction
2
Furthermore, the vertical and sagittal positions of the mandibular incisors are
important determinants in planning occlusal and skeletal relations for orthodontic
treatment and orthognathic surgical procedures.3
It is known that the facial growth pattern influences not only the morphology
of the mandibular symphysis, but also the thickness of the alveolar process in this
area, and consequently, the position of the mandibular incisors. The wider the
symphysis, the greater the possibility to tip forwards the mandibular incisors11
.
Moreover, one speculates that the negative vertical overlap is another factor
influencing the symphysis morphology.12
The region of the mandibular symphysis is involved in delicate and limited
movements, not only in esthetics, but with regard to bone and tooth resorptions.
Therefore, knowledge of the adequate limits of tooth movement and establishment of
parameters for the thickness of the alveolar process in the mandibular symphysis
region may have a significant influence on the diagnosis, and consequently, the end
result of orthodontic treatment. Previous studies have shown that individuals with a
vertical growth pattern have a longer and narrower symphysis; in those with
horizontal growth it is shorter and wider.13,14
Thus, the facial pattern may help
diagnose the shape of the symphysis.15
The morphology of mandibular symphysis is important because it serves as
the primary reference for the esthetics of the facial profile and is a determinant in
planning the lower incisor position during orthodontic and orthognathic surgery.7,16
The factors associated with the symphyseal growth and morphology include the
functional neuroskeletal balance,13
masseter muscle thickness,17
mandibular plane

Introduction
3
angle,16,18
overbite,13,15,19
lower incisor angle,20
occlusal hypofunction and its
recovery,21
inheritance.22
During orthodontic treatment, limiting incisor movement within the bone
structure is believed to be essential for achieving better results, stability, and
periodontal health, as well as for avoiding root resorption.23,24
In particular, in the case
of a severe adult skeletal Class III malocclusion, the proper amount of
decompensation including the labial inclination of the lower incisors is necessary
before orthognathic surgery.24
On the other hand, lingual inclination of the lower
incisors is needed for camouflage treatment. Either way, incisor movement confined
within the bone is recommended.25
Studies12,16
have shown morphology of the symphyseal region based on the
divergence of the mandibular plane angle and reported that the alveolar bone and
symphyseal thickness negatively correlated with the mandibular plane angle.
However Ceylan I et al19
and Nojima et al
20 from their studies have concluded Patients
with a vertical growth pattern, open bite, and high mandibular plane angle were
reported to have a similar or larger vertical dimension of the symphysis.
However substantial literature correlating and comparing the morphological
characteristics of symphysis and alveolus in brachyfacial class I and class III skeletal
subjects has not been evaluated. Therefore this study focused on the morphological
characteristics of symphysis and alveolus in Adult skeletal class III malocclusions
with cross bite and compared them with normal occlusion in brachyfacial structural
patterns.

Aims and Objectives
4
AIMS AND OBJECTIVES
The objective of this study is to measure the
1. Difference in the maxillary dentoalveolar properties of skeletal class III
cross bite malocclusion and class I control group.
2. Difference in the mandibular dentoalveolar properties of skeletal class III
cross bite malocclusion and class I control group.
3. Difference in the symphysial properties of skeletal class III cross bite
malocclusion and class I control group.

Review of Literature
5
REVIEW OF LITERATURE
Schudy F F (1963)26
conducted a cephalometric study of 400 malocclusions, in
which 19 average angles and measurements were calculated. A group of 57
malocclusions with high occluso mandibular angles (OM) were selected from the
group of 400. This group was studied and compared with other groups of 44
malocclusions with low OM angles which were selected from the group of 400 and
compared with other group. The OM angle was discussed and an attempt was made to
show its diagnostic value. This study contains documented evidence to support the
study that the relationship of the mandibular plane to the occlusal plane is very
important. The evidence strongly suggests that the OM angle is significantly related to
overbite. And by orthodontic treatment the OM angle is quite subject to change. There
is a consistency between facial type, OM angle and vertical overbite. In treated cases
attention should be given to the relationship of the incisor teeth to the occlusal plane.
The OM angle is a useful tool for describing one aspect of the morphology of the
mandible.
Robert J, et al (1977)
27 evaluated the position of the lower incisor with respect to
hard tissue references. Two samples were used for this purpose one containing 78
patients with post-treatment records having a post-retention period of at least 4 years,
and the other composed of 82 normal occlusions. They concluded that there was no
significant difference in relapse of lower incisor crowding between cases, where the
lower incisor had been moved lingually, labially, or held in the same relative position
during treatment. The position of the maxilla should be considered when placing the
lower incisor. The A-Po plane (A point to Po [Pog point]) adequately serves as a
guide to this purpose, whereas other reference lines such as mandibular plane or facial

Review of Literature
6
plane do not. The positions of the incisors with respect to popular cephalometric
reference lines such as A-Po, N-B, or mandibular plane were not correlated with the
relapse of mandibular crowding. Therefore other clinical guides might be more
successful for determining stability.
Handelman C S (1996)23
studied 107 cephalometric films which were measured to
determine the width of alveolar bone anterior and posterior to the incisor apex in each
arch. Thin alveolar widths were found both labial and lingual to the mandibular
incisors in groups of Class I, II, and III individuals with high SN-MP angle and in a
group of Class III average SN-MP individuals. Thin alveolar widths were also found
lingual to the maxillary incisors in Class II high angle group. Clinical cases were
presented showing that orthodontic tooth movement may be limited in patients with
narrow alveolar bone widths and that these patients are likely to experience increased
iatrogenic sequelae.
Bibby R E (1980)28
studied how the incisors were accommodated and whether there
is any consistent pattern operating. Sella-nasion is a stable reference plane for this
sample. Skeletal classification based on the relative prognathism of A and B points to
the cranial base indicates that Class II skeletal types, are produced due to a relatively
retruded mandible. Similarly, skeletal Class III types are due to a relatively retruded
maxilla. A compensation mechanism exists which allows upper and lower incisors ‘to
be accommodated in a normal relationship regardless of skeletal class. This
compensation is effected by both upper and lower incisors in skeletal Class III types
and mainly by the upper incisors in skeletal Class II types.
Perera P S G (1987)29
conducted a cephalometric and dental serial study of 29
untreated subjects over 9 years (11.21+/-1.1 years to 19.90+/-1.41 years), using

Review of Literature
7
Bjork's method of superimposition, and found a statistical relationships between
rotational growth of the mandible and anterior mandibular crowding. The results
indicate that closing rotational growth in the mandible is closely related to the incisor
crowding that commonly occurs during this period of 9 years. These changes appear
to be mediated through a compensatory proclination of the mandibular incisors within
the symphysis that is associated with this rotation.
Kilpeläinen P V J (1993)30
473 parents of children being screened at an orthodontic
graduate clinic completed a self-report form about the child’s dental/facial
appearance, reasons for seeking care and referral paths. Almost all (85%) of the 313
parents of children under the age of 16 years expressed concern about the appearance
of the child’s teeth, and 44% reported the child had been teased about this. Only 14%
of the parents reported that it was the child who had first noticed the need for
treatment. The rank order of reasons for seeking treatment were appearance of teeth
(85%), advice of dentist (73%), and appearance of face (46%). Using logistic
regression, overjet and malalignment were observed to be significant predictors of the
parent report of the child being teased (odds ratios [OR] 5.5 and 2.4, respectively).
Overjet predicted citing facial appearance as the reason for seeking treatment (OR
2.9), while age predicted patient-referral (OR 2.2) and overjet predicted parental
referral (OR 3.0). Increased overjet is an important focus for early treatment and
might accordingly be expected to influence the value of early intervention.
Beckmann S H, et al (1998)
15 conducted a study to investigate whether in the maxilla
and in the mandible the structure of the anterior medial sagittal alveolar and basal
bone is related to the overbite. A total of 460 untreated adult subjects were divided
into four groups with either deep bite, normal overbite, end to-end bite, or open bite

Review of Literature
8
and were compared. The overbite, lower face height, and anterior alveolar and basal
midsagittal cross-sectional areas from the maxilla and the mandible were assessed on
lateral cephalometric radiographs. A deeper bite coincided with smaller lower face
height, larger alveolar and basal areas, and a more widened shape of the symphysis. If
the lower face height was introduced as a covariable, the open bite group showed
significantly smaller maxillary and mandibular alveolar and basal cross-sectional
areas compared with the end-to-end group, the normal overbite group, or the deep bite
group. Vertical variation of the overbite probably coincides with a relative
hyperdevelopment or hypodevelopment of the symphysis.
McIntyre GT, Millett D T (2003)31
determined whether the lateral cephalometric
crown-root shape differs among the permanent maxillary central incisor in Class I,
Class II division 1, Class II division 2 and Class III malocclusions and to identify the
nature of any differences. Of the 499 lateral cephalograms recorded at a university
orthodontic clinic during 2001, 361satisfied the inclusion criteria. Sixty cephalograms
were selected from the four malocclusion groups and were digitized in random order.
The configurations of the 10 landmarks characterizing the crown root shape of the
permanent maxillary central incisor were then the optimal superimposed using
Procrustes algorithms. Discriminant analysis of the principle components of shape
determined the incisor shape differences between the malocclusion groups. The
crown-root shape of the permanent maxillary central incisor did not differ
significantly among the Class I, Class II division 1, and Class III groups (P > .05);
however, the crown-root shape of the Class II division 2 permanent maxillary central
incisor was significantly different (P < .001) from that of the Class I, Class II division
1 and Class III. The shape discrimination involved axial bending of the Class II
division 2 incisors. Principle components 1=incisor crown tip, 2=incisor root apex,

Review of Literature
9
and 3=palatal amelocemental junction accounted for 63% of the Class II division 2
incisor shape variance, encompassing a shorter root, a longer crown, and axial
bending of the incisor, in addition to a reduced labiopalatal thickness. These shape
features could precipitate the development of a deep overbite in Class II division 2
malocclusions and may limit the amount of palatal root torque during fixed appliance
therapy.
Ochoa B K, Nanda R S (2004)32
carried a study on lateral cephalometric radiographs
to compare growth patterns of the maxilla and mandible, with hand-wrist radiographs
which are used to assess skeletal maturity. The sample comprised of 28 untreated
subjects (15 female, 13 male) who were followed from ages 6 to 20 years. All
subjects had Class I malocclusions without anterior crossbites. Absolute values and
incremental changes for linear and angular cephalometric measurements were
recorded and analyzed, and the relative growth-rate formula was used to provide an
accurate index of acceleration and deceleration of growth. The SNA angle did not
change significantly with age, but the SNB angle increased significantly in the male
subjects. The ANB angle decreased continuously until age 14. The palatal plane
descended significantly from the horizontal plane. The anterior and posterior nasal
spines moved at about the same rate. The mandible grew in length twice as much as
the maxilla from ages 6 to 20. With growth, the facial profiles of the male subjects
became straighter as the chin became more prominent. The female subjects had less
incremental growth and duration of growth of the mandible, so that the profiles
remained more convex. Overall, skeletal and chronologic ages did not differ
significantly, except at ages 10 and 16 in the female subjects. Individual variability
pointed to the need for assessing each patient's pattern in the general guidelines of the
group pattern.

Review of Literature
10
Yamada C, et al (2007)23
conducted a study to examine if there was any correlation
between the labio-lingual inclinations of the mandibular central incisor and the
associated alveolar bone, and to investigate the labio-lingual position of the
mandibular central incisor root apex in the associated cancellous bone in adults with
untreated mandibular prognathism. High-resolution computed tomography images of
the mandible were recorded in 20 adult patients with mandibular prognathism. They
concluded, in adults with untreated mandibular prognathism, when the mandibular
central incisor was more lingually inclined, the associated alveolar bone was also
more lingually inclined and thinner. The mandibular central incisor root apex was
closer to the inner contour of the labial cortical bone than to the lingual cortical bone.
Chung C J, Jun S, Baik H (2008)12
conducted a study to evaluate the relationship of
the morphological characteristics of the symphyseal region of adult Class III
malocclusion to the differences in overjet and overbite. The basal and symphyseal
widths along with the alveolar and symphyseal heights were evaluated using data
from the lateral cephalograms of skeletal Class III, divided into crossbite (n = 28) and
openbite (n = 41) groups. Male normal occlusion samples (n =32) were used as
controls. He concluded, An openbite, rather than a negative overjet, is the major
factor influencing the symphyseal morphology in an adult Class III malocclusion.
Buschang P H (2008)7 established reference data for anterior and posterior
dentoalveolar heights of growing French-Canadians with untreated normal occlusions
and malocclusions. The mixed longitudinal sample includes 227 French- Canadians,
119 male and 108 female, with cephalograms taken annually between 10-15 years of
age. Maxillary and mandibular dentoalveolar heights were measured as the
perpendicular distances of the incisor tips and first molar mesial cusp tips to the

Review of Literature
11
palatal (ANS-PNS) and mandibular (Go-Me) planes. Male dentoalveolar heights were
significantly (P < .05) greater than female heights at all ages. Dentoalveolar heights at
15 years of age were significantly larger (P < .05) than at 10 years of age, with
differences ranging from 2.1–4.2 mm in male subjects and from 2.1–3.8 mm in
female subjects. The greatest difference in dentoalveolar heights between the 10- and
15-yearold age groups was for the maxillary first molar; the maxillary central incisor
height showed the smallest age effects. The coefficients of variation were greater for
the maxillary than the mandibular dentoalveolar heights. Correlations of dentoalveolar
heights within jaws ranged from 0.53 to 0.82; correlations between jaws ranged from
0.30 to 0.44. The mandibular heights showed the strongest associations. French-
Canadian adolescents require age- and sex-specific reference data for dentoalveolar
heights.
Kim Y, Park J U, Kook Y (2009)34
conducted a study to test the hypothesis that
there is no difference in the vertical alveolar bone levels and alveolar bone thickness
around the maxillary and mandibular central incisors in surgically treated skeletal
Class III malocclusion patients. The study sample comprised patients with skeletal
Class III malocclusion with anterior crossbite and openbite. Three dimensional cone
beam computed tomography images were taken at least 1 month before the
orthognathic surgery, and sagittal slices chosen at the labio-lingually widest point of
the maxillary and mandibular right central incisor were evaluated. Measurement of
the amount of vertical alveolar bone levels and alveolar bone thickness of the labial
and lingual plate at the root apex was made using the SimPlant Pro 12.0 program. The
hypothesis was rejected. For the skeletal Class III patients undergoing orthognathic
surgery, special care should be taken to prevent or not aggravate preexisting alveolar
bone loss in the anterior teeth, especially in the mandible.

Review of Literature
12
Gracco A (2009)
35 studied the correlations between the morphology of the upper jaw,
the position of the upper incisors, and facial type. From a sample of 191 patients, the
FMA angle was used to select 20 short face type, 20 normal face type, and 20 long
face type patients, aged 12 to 40 years. Using cone-beam computed tomography
(CBCT); tomography was carried out on sagittal sections corresponding to the four
upper incisors. Some parameters defining the dentoskeletal relationships, the alveolar
thickness, the alveolar height, and the dental movement were measured. The
measurements were processed using analysis of variance and Tukey'stest. At the
upper central incisors, short face type patients presented a greater alveolar bone
thickness than long face type patients. In short face type and normal face type subjects
the root apex of the upper incisors was farther away from the lingual cortex than in
the long face type patients. At the central incisors the alveolar thickness was greater
and the lingual cortex was higher with respect to the lateral incisors in all three facial
types. With respect to the upper incisors, facial types are correlated statistically
significantly with both alveolar bone thickness and distance between the root apex
and lingual cortex.
Esenlik E, Sabuncuoglu F A (2012)
3 conducted a study to investigate the alveolar
and symphysis region properties in hyper-, hypo-, and normodivergent Class II
division 1 anomalies. Pretreatment lateral cephalograms of 111 young adult female
patients with skeletal Class II division 1 anomalies were compared to those of 54
Class I normal subjects (control group). Class II cases were divided into
hyperdivergent (n = 58), hypodivergent (n = 19), and normodivergent groups (n = 34).
The heights and widths of the symphysis and alveolus and the depth of maxillary
palate were measured on the lateral cephalograms. He concluded that Symphysis
width is the main factor in the differential diagnosis of Class II division 1 anomaly

Review of Literature
13
rather than symphysis height and hypodivergent Class II Division 1 anomaly is more
suitable for mandibular incisors movements.
Baysal A, Ucar F I , BuyukS K, Ozer T , Uysal T (2013)
36 study was conducted
to evaluate lower incisor position and bony support between patients with Class II
average- and high-angle malocclusions and compare with the patients presenting
Class I malocclusions. CBCT records of 79 patients were divided into 2 groups
according to sagittal jaw relationships: Class I and II. Each group was further divided
into average- and high-angle subgroups. Six angular and 6 linear measurements were
performed. They concluded that Mandibular anterior bony support and lower incisor
position were different between average- and high-angle Class II patients. Range of
lower incisor movement in high-angle Class II patients is limited compared to average
angle class II patients.
Krishana N, Shetty A, Girija M. P, Nayak R (2013)37
Conducted a study to
Evauated change in alveolar bone as a result of maxillary and mandibular incisor
retraction in patients with bimaxillary protrusion by means of using lateral
cephalogram and computed tomography (CT)scans and to investigate any occurance
of bony defect like dehiscence and fenestration. Ten patients (age 15 ± 3 years) with
bimaxillary protrusion treated by extraction of four first premolars were investigated
by lateral cephalograms and CT scans during pre‑ treatment (T1) and after 3 months
of completion of incisor retraction (T2). In the mandibular arch, after lingual
movement of the incisors, the bone labial to the anterior teeth decreased in thickness
at the coronal level of the left lateral and left central incisors. In the maxilla the
change in the labial bone thickness was not statistically significant.He concluded,
when incisors are retracted, the risk of adverse effect is present. This must be
carefully monitored to avoid negative iatrogenic effects.

Review of Literature
14
Nahás-Scocate A C (2014)38
evaluated the amount of buccal and lingual supporting
bone tissue of 60 upper central incisors and the relationship with their inclination.
Thirty healthy adult patients with no previous orthodontic treatment were evaluated
using cone-beam computed tomography. Cross-sectional views were analyzed to
check the amount of the bone tissue on the cervical (cervical buccal thickness/CBT;
lingual/CLT), middle (middle buccal thickness/MBT; lingual/MLT), and apical
regions (apical buccal thickness/ABT; lingual/ALT). The Pearson correlation, linear
regression, and analysis of variance tests were used (P < .05). For both surfaces
(buccal and lingual), the amount of bone tissue in the apical region was significantly
higher than the middle and cervical regions, and the middle region was significantly
higher than the cervical region. In relation to the upper central incisor's inclination,
the higher the U1/PP the higher was ABT. However, the coefficient values for both
upper central incisors were low.
Gutermanna C (2014)39
reassessed the inclination of lower incisors and evaluated
possible associations with gender, age, symphyseal parameters, and skeletal pattern.
Twelve hundred and seventy-two (605 females, 667 males) cephalograms of untreated
subjects of a craniofacial growth study (8–16 years) were evaluated. Correlations
between the angulation of the lower incisors and age, symphyseal distances (height,
width, and depth), symphyseal ratios (height-width, height-depth), and skeletal angles
(divergence of the jaws and gonial angle) were investigated for all ages separately and
for both sexes independently. Lower incisor inclination was linked to the subject’s
sex, age, and skeletal pattern. The inclination of lower incisors increased over age,
correlated with the divergence of the jaws for all ages significantly or highly
significantly, except for boys and girls 9 years of age and girls 11 and 12 years of age,
for which only a tendency was observed. Similarly, a strong correlation to gonial

Review of Literature
15
angle was observed. No correlation was found between the inclination of lower
incisors and any symphyseal parameters (absolute measurements and ratios), except
for symphyseal depth. The inclination of lower incisor was not associated with
symphyseal dimensions, except symphyseal depth. Factors related to natural
inclination of lower incisors should be respected when establishing a treatment plan.
Dayoub N S, Al- Sabbagh R (2015)40
conducted a study to assess the supporting
bone tissue thickness of 68 lower central incisors and to investigate the impact of
gender on the alveolar bone thickness. Thirtyfour healthy patients with no previous
orthodontic were evaluated by Cone Beam Computed Tomography. Sagittal sections
views were analyzed to check the thickness of supporting bone on the cervical, middle
of the root and apical for both surfaces buccal and lingual. The results showed that
buccal apical and lingual apical regions had the greatest values of bone tissue
thickness, and the lowest values were in lingual cervical, buccal cervical and buccal
middle of the root for both lower central incisors. There was no significant effect of
gender on supporting bone thickness.
Arriola-Guille´n L E, Flores-Mir C (2015)
41 conducted a study to compare the
anterior dentoalveolar and skeletal maxillary cephalometric factors involved in
excessive upper incisor crown exposure (UICE) in subjects with skeletal open bite
Class II (SOBCIIG) and Class III (SOBCIIIG) against an untreated control group
(CG). Seventy pretreatment lateral cephalograms of orthodontic young adult patients
(34 men, 36 women) were examined. The sample was divided into three groups
according to both sagittal and vertical growth pattern and occlusion. Several
cephalometric measurements were considered (skeletal and dental). Princicipal
component analysis (PCA) showed that a nondental component—including vertical

Review of Literature
16
maxillary height (VMH) and upper lip height (ULH)—was the only component
significantly associated with upper incisor crown exposure (UICE). Although the
upper incisor crown exposure (UICE) was statistically different in skeletal open bite
Class II (SOBCIIG), the values were within the esthetic standards. The upper incisor
crown exposure (UICE) was mainly influenced by vertical maxillary height (VMH)
and upper lip height (ULH).

Methodology
17
MATERIAL AND METHODS
Material required:
In this study a total of 80 lateral cephalograms of adult patients over the age of
18years (50 of patients with skeletal class I malocclusions and 30 lateral
cephalograph of patients with skeletal class-ІІІ malocclusion) referred to the
department of orthodontics and dentofacial orthopedics, Al-Badar dental college and
hospital, Gulbarga were evaluated.
The skeletal Class III sample was selected in accordance with the following
inclusion criteria
Class III intermaxillary jaw base relationship (ANB below 0O, AO – BO ≤ -
0.5mm)
Class III molar relationship, negative overjet, positive overbite and deep
vertical incisal overlap.
Brachyfacial pattern with low mandibular plane angle (angular value of FMA
< 20o and SN GO-GN < 29
o)
The skeletal Class I control group exhibited normal ANB angle, normal
overjet and acceptable occlusion.
Cephalometric Analysis:
The lateral cephalograms were taken with the head locked in position by ear
rods and nasal support. The Frankfort horizontal plane was set parallel to the floor
and teeth were in centric occlusion. The x-rays were taken with a focus coronal plane
distance of 200cm and an enlargement of 7.5 %.

Methodology
18
All cephalograms were traced manually by a single examiner using a
protractor with 0.5° and 0.5 mm accuracy as described in, (Table 1 and fig.1).
Duplicate tracings of 30 landmarks on 15 randomly chosen cephalograms were done
at a 2month interval by the same examiner. The systematic error was evaluated with a
paired t Test at P < 0.05. No significance was noted in the measurements of the first
and second evaluation.
The cephalometric data of the control, Class III cross bite groups were
presented as a mean ± SD. The results were inferred by analysis of variance
(ANOVA) using statistical software (SPSS version 23). P < 0.05 was considered
significant.
Table.1 and fig.1
No Landmarks Definition
1. 1/PP (°) The angle from the maxillary central Incisor’s axis to
the palatinal plane (ANS–PNS).
2. 1/MP (°) The angle from the mandibular central incisor’s axis
to the mandibular plane (Go – Me).
3. Mandibular incisor
dentoalveolar
height (L1–AH)
The perpendicular distance between the lower incisor
tip and mandibular plane.
4. Mandibular molar
dentoalveolar
height (L6–AH)
The perpendicular distance between the lower first
molar mesial cusp tip and mandibular plane.
5. Maxillary incisor
dentoalveolar
height (U1–AH)
The perpendicular distance from the upper incisor tip
to the palatal plane.
6. Maxillary molar
dentoalveolar
height (U6–AH)
The perpendicular distance from the upper first molar
mesial cusp tip to the palatal plane.

Methodology
19
7. Id–Id′ width The distance between the most anterosuperior (Id) and
most posterosuperior (Id′) points on the mandibular
alveolus.
8. B–B′ width The distance between the B and B′ (the lingual
projection of the B point at the lingual symphysis
border) points.
9. Symphysis
height
The distance from the midpoint of the anterior
alveolus to the Menton point. The symphysis ratio
was calculated by dividing the symphysis height by
the symphysis width.
10. Symphysis
width
The perpendicular distance from the pogonion to the
most convex point of the lingual curvature of the
symphysis.
11. Maxillary depth The distance from the deepest point on the palatal
bone curvature to the A point.
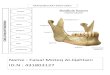
Figure 1. Dentoalveolar and Symphysis Parameters. 1: 1/PP, 2: 1/MP,
3:L1/AH, 4:L6/AH, 5:U1/AH, 6:U6/AH, 7:Id-Id' width, 8:B-B' width, 9:
Symphysis height, 10: Symphysis width, 11: maxillary depth.

Sample size Estimation
20
SAMPLE SIZE ESTIMATION
The formula for sample size determination for t test is
n=(Z*Z*SD*SD)/ME*ME
Z = z value for 85% power = 1.44
SD= SD of SNB = (3+3.6)/2 = 3.3 (table no 2)
ME= Margin of error = SD/(SQRT of N) = 3.3/ (SQRT32)=0.58
substituting the above we get the total sample size of
(1.44*1.44*3.3*3.3)/0.58*0.58 = 68.4 = 70
the minimum total sample size will be 70.

Results
21
RESULTS
Table 2 provide a summary of the skeletal characteristics of the Class III cross
bite and Class I control groups. The skeletal Class III cross bite group showed a larger
SNB, ANB and AO-BO measurements compared with the control group. The values
for the above parameters were significantly different between the control and class III
cross bite groups. Class I control group had a significantly lesser mandibular plane
angle than the Class III cross bite group (p <0.001).
Table 2: Intergroup comparison of skeletal parameters
Parameter Class III Class I Mean
Difference
P value
N Mean Std.
Deviation
N Mean Std.
Deviation
SNA (o) 30 82.033 5.1158 50 81.960 2.8569 0.073 0.935 NS
SNB (o) 30 85.700 4.4346 50 78.600 5.4210 7.1 <0.001**
ANB (o) 30 -3.667 2.7834 50 2.880 .9179 -6.54 <0.001**
AO-BO
(mm)
30 -7.733 4.1100 50 .680 .4712 -8.41 <0.001**
GO-GN-
SN(o)
30 26.800
4.5768 50 23.867 1.6288 -2.93 0.002*
NS- Not significant (p>0.05), *-Significant (p<0.05), **-Highly significant (p<0.001)
COMPARISON OF MAXILLARY PARAMETERS
Table 3 shows an increased maxillary incisor inclination in Class III cross bite
group (128.5 ± 8.3; Mean ± SD) compared to class I subjects (123.6 ± 7.7; Mean ±
SD) with a significant difference between the two groups (p<0.05). The maxillary

Results
22
incisal dento alveolar height has an insignificant difference between the two groups.
The maxillary molar dento alveolar height and maxillary depth were significantly
greater in the Class III cross bite group, than in the control group (p<0.001).
Table 3: Intergroup comparison of various maxillary parameters
Parameter Class III Class I Mean
Difference
P value
N Class
III
Std.
Deviation
N Class I Std.
Deviation
1/ PP(o) 30 128.533 8.3490 50 123.660 7.7739 4.87 0.010*
U1-
AH(mm)
30 26.333 4.9434 50 25.720 2.5638 .6133 0.467 NS
U6-
AH(mm)
30 23.900 3.0777 50 20.780 2.2704 3.1200 <0.001**
Max
Depth
(mm)
30 16.200 3.2206 50 12.460 2.4596 3.7400 <0.001**
NS- Not significant (p>0.05), *-Significant (p<0.05), **-Highly significant (p<0.001)
COMPARISON OF MANDIBULAR PARAMETERS
Table 4 shows Mandibular incisal inclinations were significantly greater in
Class I control group than in Class III cross bite group (P<0.001**). Mandibular
insisal dento alveolar height and mandibular molar dento alveolar height were
significantly greater in the Class III cross bite group than in the Class I control group
(p<0.001).

Results
23
Table 4: Intergroup comparison of mandibular parameters
Parameter Class III Class I Mean
Difference
P value
N Class
III
Std.
Deviation
N Class I Std.
Deviation
1/MP(o) 30 92.533 8.5892 50 105.120 7.2016 -12.5867 <0.001**
L1-
AH(mm)
30 41.267 4.2906 50 36.840 2.7207 4.4267 0.001*
L6-
AH(mm)
30 31.733 3.7040 50 28.800 2.3561 2.9333 <0.001**
**-Highly significant (p<0.001)
COMPARISON OF SYMPHYSIS PARAMETERS
Table 5 shows symphysis height and width were significantly greater in Class
III cross bite group than in the control group, while symphysis ratio was similar in
both the groups.

Results
24
Table 5: Intergroup comparison of symphysis parameters
Parameter Class III Class I Mean
Difference
P value
N Class
III
Std.
Deviation
N Class I Std.
Deviation
Id-IdI
(mm)
30 6.600 .8137 50 5.900 .6776 .7000 <0.001**
B-BI
(mm)
30 8.367 1.0981 50 9.460 1.4316 -1.0933 0.001*
Sym Ht
(mm)
30 32.200 3.9339 50 28.920 2.2663 3.2800 <0.001**
Sym
Width
(mm)
30 13.800 1.7499 50 12.620 1.4270 1.1800 0.002*
Sym h/w 30 2.3567 .36073 50 2.2752 .28403 .08147 0.266 NS
NS- Not significant (p>0.05), *-Significant (p<0.05), **-Highly significant (p<0.001)

Discussion
25
DISCUSSION
The mandibular bone is strongly influenced by the masticatory function.42-45
Maxillofacial region contains essentially membranous bone and is more susceptible to
environmental factors such as the stimulating influence of muscles and extra
functional forces.17,46
During the power stroke of mastication, the middle and lower third of the
labial aspect of the symphysis is predominantly sheared dorsoventrally, twisted and
bent according to the magnitude and position of the bite force.42-44
Therefore it was hypothesized that due to differences in the bite force direction
of mandibular incisors, the morphological characteristics of mandibular symphysis
and premaxillary alveolus can vary between normal Class I and Class III cross bite
brachyfacial subjects.
The results showed a significant increase in the maxillary incisal inclination,
depth and dento alveolar molar height in the Class III cross bite groups than in the
control groups. In the lower jaw the mandibular incisor showed a significant
retroclination in Class III cross bite group and the mandibular molar dento alveolar
height and incisal dento alveolar height was greater in the Class III cross bite group
than in the control group.
Maxillary incisal proclination and mandibular incisal retroclinaton in Class III
cross bite group probably resulted from a dento alveolar compensation, to Class III
skeletal discrepancies.
The maxillary alveolar process, mandibular condyle and alveolar process were
defined as major sites of bony additions.10
The Class III cross bite subjects in the

Discussion
26
present study showed an increased gonial angle compared to the control group. This
downward and backward rotation of the mandible is associated with excessive
extrusion of posterior maxillary and mandibular alveolar processes contributing to
vertical development. This also explains the increased lower anterior dental height in
Class III cross bite subjects. The increased depth of the maxillary alveolus in Class III
cross bite subjects could be possibly due to remodeling changes associated with
premaxillary alveolus as a part of dento alveolar compensations seen with Class III
skeletal patterns.
Karlsen10
stated that alveolar process growth demonstrated compliance with
mandibular rotation. He also stated that dentoalveolar mechanisms have great
potential for compensating for vertical skeletal deviations. Overdevelopment of the
anterior lower facial height was compensated by marked growth of the incisal heights
in both jaws. In his study evaluating low and high angles in patients 6-12 years of age,
he found great increases in the upper and lower incisor heights in the high angle cases.
As the mandible is displaced downward and forward, supraeruption of the incisors
fills the created space.6 Mandibular rotation also interacts with vertical growth, and
anterior or counterclockwise rotation might be expected to limit vertical change in the
anterior region.
Baumrind et al47
investigated the amount of modeling at the apices of the
mandibular and maxillary incisors and molars associated with remodeling changes in
the mandible from 8.5 to 15.5 years of age. They observed statistically significant
tooth displacements associated with surface remodeling in the maxilla at all
timepoints, whereas significant differences in the mandible were observed only in the
vertical direction in the incisors.

Discussion
27
Janson et al48
stated that the lower anterior dental height was significantly
different in each facial type. When we compared anterior alveolar heights in the
present study, we found that the upper and lower incisor heights were increased
slightly but significantly in the Class III cross bite group as seen in Karlsen’s10
study.
Clinicians classify the growth pattern of the mandible anteriorly or posteriorly
according to the symphysis shape and size.10
Symphysis ratio in particular was found
to be strongly related to the direction of mandibular growth4.
Noh et al49
found that a high symphysis ratio presented high correlations with
the hyperdivergent pattern and increased gonial angle. In contrast, Kim and Son50
found no statistically significant difference in symphysis ratio to mandibular plane
between forward and backward rotational growth patterns.
Morphological differences in the symphyseal region between Class III cross
bite and Class I normal occlusion were found in the present study. Symphyseal height
and width; Id–Id and B-B widths were significantly greater in Class III cross bite
subjects compared to Class I controls.
The findings of the present study indicate a large symphysis allows a greater
sagittal but also vertical mandibular tooth movements, particularly required during
decompensation of anterior dental segments during the phase of pre surgical
orthodontics.
Bone is a dynamic tissue that constantly undergoes remodeling, but it has been
reported that remodeling can remove or conserve the bone but not add to it. New bone
formation at the labial side after incisal movements could be expected in growing
patients but not in nongrowing patients.3 It is suggested that rapid tipping tooth

Discussion
28
movements contribute to bone dehiscence and root resorption.51
Sufficient alveolar
bone thickness in the lower incisor region is critical in the case of Class III skeletal
malocclusions requiring orthognathic surgery.
Studies have shown a narrow symphysis is detrimental in surgical treatment of
Class III malocclusions since the lower incisors would be limited in their antero
posterior tooth movements thus compromising on the antero posterior segments
during surgical intervention.
Hence a wider and thicker symphysis is accommodative of all incisal
movements in the labiolingual direction in Class III skeletal subjects requiring
camouflage treatment or orthognathic surgery. The clinical implications from the
above findings imply iatrogenic damage of orthodontic treatment like dehiscence,
fenestration and root resorption are minimal in brachyfacial skeletal Class III
malocclusions compared to hyperdivergent skeletal Class III malocclusions.

Conclusion
29
CONCLUSIONS
Maxillary incisor inclination, Max molar dento alveolar height and maxillary
depth were significantly greater in the Class III cross bite group than in the
Class I control group.
Mandibular incisal dento alveolar height and mandibular molar dento alveolar
height were significantly greater in the Class III cross bite group than in the
Class I control group.
Symphysis height and width were significantly greater in the Class III cross
bite group than in the Class I control group.

Summary
30
SUMMARY
The prevalence of class III malocclusion varies according to ethnicity. In
orthodontics, knowledge of mandibular growth is highly beneficial in diagnosis and
treatment planning and is critical in the development of balanced dentofacial
structures.
The symphysis is one of the most important regions of the craniofacial
complex for clinical orthodontists, and it serves as a primary reference for esthetic
considerations in the lower one-third of the face. Vertical and sagittal positions of the
mandibular incisors are important determinants in planning occlusal and skeletal
relations for orthodontic treatment and orthognathic surgical procedures.
The region of the mandibular symphysis is involved in delicate and limited
movements, not only in esthetics, but with regard to bone and tooth resorptions.
Therefore, knowledge of the adequate limits of tooth movement and establishment of
parameters for the thickness of the alveolar process in the mandibular symphysis
region may have a significant influence on the diagnosis, and consequently, the end
result of orthodontic treatment.
Therefore the present study focused on the morphological characteristics of
symphysis and alveolus in Adult skeletal class III malocclusions with cross bite and
compared them with normal occlusion in brachyfacial structural patterns.
In this study a total of 80 lateral cephalograms of adult patients over the age of
18years (50 of patients with skeletal class I malocclusions and 30 lateral
cephalograph of patients with skeletal class-ІІІ malocclusion were evaluated. The

Summary
31
cephalometric data of the control class I group and Class III cross bite groups were
presented.
Thus the study concluded that Maxillary incisor inclination, Max molar dento
alveolar height and maxillary depth were significantly greater in the Class III cross
bite group than in the Class I control group.
Mandibular incisal dento alveolar height and mandibular molar dento alveolar
height were significantly greater in the Class III cross bite group than in the Class I
control group. Symphysis height and width were significantly greater in the Class III
cross bite group than in the Class I control group.

Bibliography
32
BIBLIOGRAPHY
1. Mehboob B, Rasool G, Amin M, Characteristics of skeletal class III
malocclusion and its associated dento alveolar compensation, JKCD
December 2011, Vol. 2, No. 1.
2. Sassouni V. The Class II syndrome: Differential diagnosis and treatment.
Angle Orthod 1970;40:334-341.
3. Esenlik E, Sabuncuoglu F A. Alveolar and symphysis regions of patients with
skeletal class II division 1 anomalies with different vertical growth patterns.
European Journal of Dentistry 2012; 6.
4. Aki T, Nanda RS, Currier GF, Nanda SK. Assessment of the symphysis
morphology as a predictor of the direction of mandibular growth. Am J Orthod
1994;106:60-69.
5. Bjork A. Prediction of mandibular growth rotation. Am J Orthod 1969;55:585
599.
6. Isaacson JR, Isaacson RJ, Speidel TM, Worms FW. Extreme variation in
vertical facial growth and associated variation in skeletal and dental relations.
Angle Orthod 1971;41:219-229.
7. Buschang PH, Julien K, Sachdeva R, Demirjian A. Childhood pubertal
growth changes of the human symphysis. Angle Orthod 1992;62:203-210.
8. Enlow DH, Harris DB. A study of the postnatal growth of the human
mandible. Am J Orthod 1964;75:25-50.
9. Skieller V, Bjork A, Linde-Hansen T. Prediction of mandibular growth
rotation evaluated from a longitudinal sample. Am J Orthod 1984;86:359-370.
10. Karlsen AT. Craniofacial growth differences between low and high MP-SN
angle males: a longitudinal study. Angle Orthod 1995;65:341-350.

Bibliography
33
11. Perera PSG. Rotational growth and incisor compensation. Angle Orthod
1987;57:39-49.
12. Chung CJ, Jung S, Baik HS. Morphological characteristics of the symphyseal
region in adult skeletal Class III crossbite and openbite malocclusions. Angle
Orthod 2008;78:38-43.
13. Haskell BS. The human chin and its relationship to mandibular morphology.
Angle Orthod 1979;49:153-66.
14. Wehrbein H, Bauer W, Diedrich P. Mandibular incisors, alveolar bone, and
symphysis after orthodontic treatment. A retrospective study. Am J Orthod
Dentofacial Orthop 1996;110:239-46.
15. Beckmann SH, Kuitert RB, Prahl-Andersen B, Segner D, The RPS, Tuinzing
DB. Alveolar and skeletal dimensions associated with overbite. Am J Orthod
Dentofacial Orthop 1998;113:443-52.
16. Tanaka R, Suzuki H, Maeda H, Kobayashi K. Relationship between an
inclination of mandibular plane and a morphology of symphysis [in Japanese].
Nippon Kyosei Shika Gakkai Zasshi. 1989;48:7–20.
17. Kubota M, Nakano H, Sanjo I, Satoh K, Sanjo T, Kamegai T, Ishikawa F.
Maxillofacial morphology and masseter muscle thickness in adults. Eur J
Orthod. 1998;20:535–542.
18. Eroz UB, Ceylan I, Aydemir S. An investigation of mandibular morphology in
subjects with different vertical facial growth patterns. Aust Orthod J.
2000;16:16–22
19. Ceylan I, Eroz UB. The effects of overbite on the maxillary and mandibular
morphology. Angle Orthod. 2001;71:110–115.

Bibliography
34
20. Nojima K, Nakakawaji K, Sakamoto T, Isshiki Y. Relationships between
mandibular symphysis morphology and lower incisor inclination in skeletal
class III malocclusion requiring orthognathic surgery. Bull Tokyo Dent Coll.
1998;39:175–181.
21. Shimomoto Y, Iwasaki Y, Chung CY, Muramoto T, Soma K. Effects of
occlusal stimuli on alveolar/jaw bone formation. J Dent Res. 2007;86:47–51.
22. Garn SM, Lewis B, Vicinus JH. The inheritance of symphyseal size during
growth. Angle Orthod. 1963;33:222–231.
23. Handelman CS. The anterior alveolus: its importance in limiting orthodontic
treatment and its influence on the occurrence of iatrogenic sequelae. Angle
Orthod. 1996;66:95–110.
24. Proffit WR, Whilte RPJ, Sarver DM. Contemporary Treat ment of Dentofacial
Deformity. New York, NY: Elsevier Inc; 2003.
25. Mulie RM, Hoeve AT. The limitations of tooth movement within the
symphysis studied with laminagraphy and standardized occlusal films. J Clin
Orthod. 1976;10:882–893,886–889.
26. Schudy F F. Cant of the Occlusal Plane and Axial Inclinations of Teeth. Angle
Orthod 1963; 33( 2):69-82.
27. Robert J. Sci-Iuli-Iof, A.B, M.A. Robert W. Allen, Roland D. Walters and
Michael Dreskin. The Mandibular Dental Arch: Part 1, Lower Incisor
Position. Angle Orthod. 1974, ;47( 4): 280- 87.
28. Bibby R E. Incisor relationships in different skeletofacial patterns. Angle
Orthod: 1980; 50(1): 41-44.
29. Perera P S G. Rotational Growth and Incisor Compensation. Angle Orthod.
1987; 57(1):39-49.

Bibliography
35
30. Kilpeläinen P V J, Phillips C, Tulloch J F C. Anterior tooth position and
motivation for early treatment. Angle Orthod. 1993;63(3):171-174 .
31. McIntyre G T, Millett D T. Crown-root shape of the permanent maxillary
central incisor. Angle Orthod. 2003; 73(6):710-5.
32. Ochoa B K and Nanda R S. Comparison of maxillary and mandibular growth
.Am J Orthod Dentofacial Orthop. 2004;125:148-59.
33. Yamada C, ‘et al’, SpatiaRelationships between the Mandibular Central
Incisor and Associated Alveolar Bone in Adults with Mandibular
Prognathism. Angle Orthodontist 2007; 77( 5)
34. Kim Y, Park J U, Kook Y. Alveolar Bone Loss around Incisors in Surgical
Skeletal Class III Patients. Angle Orthod 2009; 79:676–682.
35. Gracco A, Lombardo L, Mancuso G, Gravina V, Siciliani G. Upper incisor
position and bony support in untreated patients as seen on CBCT. Angle
Orthod. 2009; 79(4):692-702.
36. Baysal A, Ucar F I, Buyuk S K, Ozer T , Uysal T . Alveolar bone thickness and
lower incisor position in skeletal Class I and Class II malocclusions assessed
with cone-beam computed tomography. Korean J Orthod 2013; 43(3):134-140
37. Krishna N, Shetty A, Girija MP, Nayak R. Changes in alveolar bone thickness
due to retraction of anterior teeth during orthodontic treatment: A
cephalometric and computed tomography comparative study. Indian J Dent
Res 2013; 24:736-41.
38. Nahás-Scocate A. C, De Siqueira Brandão A, Patel MP, Lipiec -Ximeneme,
Chilvarquer I, DoValle - Corottickm. Bone tissue amount related to upper
incisors inclination. Angle Orthod. 2014; 84(2):279-85.

Bibliography
36
39. Gutermanna C, Peltomakib T, Markicc M, Hanggia M, Schatzlec M ,
Signorellia L and Patcas R. The inclination of mandibular incisors revisited.
Angle Orthod.2014; 84:109-119.
40. Dayoub N S T et al. Assessment of Supporting Bone Thicknesses Related to
Lower Incisors -A CBCTStudy Int.J. PharmTech Res. 2015; 8(1):53-62.
41. Arriola-Guille´n L E, Flores-Mir C. Anterior maxillary dentoalveolar and
skeletal cephalometric factors involved in upper incisor crown exposure in
subjects with Class II and III skeletal open bite. Angle Orthod 2015; 85:72–79.
42. Hylander WL. In vivo bone strain in the mandible of Galago crassicaudatus.
Am J Phys Anthropol. 1977;46:309–326.
43. Hylander WL. Stress and strain in the mandibular symphysis of primates: a
test of competing hypotheses. Am J Phys Anthropol. 1984;64:1–46.
44. Korioth TW, Hannam AG. Deformation of the human mandible during
simulated tooth clenching. J Dent Res. 1994; 73:56–66.
45. Korioth TW, Hannam AG. Mandibular forces during simulated tooth
clenching. J Orofac Pain. 1994;8:178–189.
46. Dulkin J. Secondary cartilage: a misnomer? Am J Orthod. 1972;62:15–41.
47. Baumrind S, Bravo LA, Ben-Bassat Y, Curry S, Korn EL. Lower molar and
incisor displacement associated with mandibular remodeling. Angle Orthod
1997;67:93-102.
48. Janson GRP, Metaxas A, Woodside DG. Variation in maxillary and
mandibular molar incisor vertical dimension in 12-year old subjects with
excess, normal and short lower anterior face height. Am J Orthod
1994;106:409-418.

Bibliography
37
49. Noh SH, Lee KS, Park YK. A cephalometric study on correlation between
mandibular symphysis and craniofacial skeleton. Korean J Orthod
1997;27:119-127.
50. Kim SJ, Son WS. A study on the relationship of the mandibular symphysis
and anterior alveolar and skeletal morphology according to the rotational
growth pattern of mandible in skeletal Class III malocclusion Korean J Orthod
1999;29:303-315.
51. Diedrich P. Problems and risks in the movement of the mandibular anterior
teeth. Fortschr Kieferorthop 1995;56:148-156.

Consent Form
38
AL - BADAR
RURAL DENTAL COLLEGE & HOSPITAL, GULBARGA
CONSENT FORM
I ………………………………………. OPD No…...... undergoing Orthodontic
treatment in the Department of Orthodontics and Dentofacial Orthopedics, Al Badar
Rural Dental College and Hospital, have been explained about the research study, and
I hereby give my consent for taking my lateral cephalogram.
Signature of patient

Ethical Clearance
39

Proforma Prototype
40
PROFORMA PROTOTYPE
The skeletal Class III sample was selected in accordance with the
following inclusion criteria
Class III intermaxillary jaw base relationship (ANB below 0O, AO – BO ≤
-0.5mm)
Class III molar relationship, negative overjet, positive overbite and deep
vertical incisal overlap.
Brachyfacial pattern with low mandibular plane angle (angular value of
FMA < 20o and SN GO-GN < 29
o)
The skeletal Class I control group exhibited normal ANB angle, normal
overjet and acceptable occlusion.
Exclusion criteria
Patient with
1. Congenital anomalies and
Hypodontia are excluded from study.
Lateral cephalogram evaluation parameters;

Proforma Prototype
41
Dentoalveolar and Symphysis Parameters. 1: 1/PP, 2: 1/MP, 3:L1/AH, 4:L6/AH,
5:U1/AH, 6:U6/AH, 7:Id-Id' width, 8:B-B' width, 9: Symphysis height, 10:
Symphysis width, 11: maxillary depth.



Annexures
44
ANNEXURES
Digital Panoramic and Cephalometric Extra oral Imaging System
– Cephalostat (Kodak 8000C).

Annexures
45
The lateral cephalograms were taken with the head locked position.

Annexures
46

Annexures
47