Embed Size (px)
Citation preview

Case ReportAcute Osteomyelitis of the Symphysis Pubis after InguinalHernia Surgery
Recep Tekin,1 Rojbin Ceylan Tekin,2 Figen Ceylan Cevik,3 and Remzi Cevik4
1Department of Infectious Disease and Clinical Microbiology, Dicle University School of Medicine, Yenisehir, 21280 Diyarbakir, Turkey2Department of Radiology, Genesis Hospital, Diyarbakir, Turkey3Department of Physical Medicine and Rehabilitation, Diyarbakir State Hospital, Diyarbakir, Turkey4Department of Physical Medicine and Rehabilitation, Dicle University School of Medicine, Yenisehir, 21280 Diyarbakir, Turkey
Correspondence should be addressed to Remzi Cevik; [email protected]
Received 25 January 2015; Revised 1 April 2015; Accepted 2 April 2015
Academic Editor: Mario Salazar-Paramo
Copyright © 2015 Recep Tekin et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Osteomyelitis of pubic symphysis is infectious inflammatory condition of the symphysis pubis and rare complication of surgeryaround inguinal and groin region. It should be kept in mind in the differential diagnosis of lower pelvic pain and should be soughtin cases of pelvic insufficiency fractures. Herein, we present a case of a 55-year-old man with osteomyelitis of the symphysis pubisfollowing inguinal hernia surgery for diagnosis and management of this rare condition.
1. Introduction
Osteomyelitis of the symphysis pubis is a rarely describedentity. Osteomyelitis pubis is a term used to describe anentity characterised by severe pelvic pain, a wide-basedgait, and bony destruction of the margins of the pubicsymphysis [1]. Osteomyelitis of the symphysis pubis is veryunusual and the clinical presentation can resemble osteitispubis. Both entities commonly confused with each other.Rarity of condition nonspecific signs and symptoms has ledto misdiagnosed, undiagnosed and delay in the manage-ment [2, 3]. Osteomyelitis of the symphysis pubis followinginguinal hernia repair is extremely rare. We reported a rarelyencountered case of osteomyelitis of the symphysis pubis.
2. Case
A 55-year-old man visited our hospital, because of feverand left inguinal pain that appeared at ten days after oper-ation with disturbance of gait. On physical examination,his temperature was 39∘C, pulse 102 beats/min, and bloodpressure 120/80mmHg. The locomotor system examinationpelvic compression test and bitrochanteric compression testwere positive. Investigation revealed white blood cell (WBC)
count 14000mm3, erythrocyte sedimentation rate 42mm/h,and C-reactive protein (CRP) 9mg/dL (normal range 0–5mg/dL). The rheumatoid factor (RF), anti-nuclear anti-body (ANA), HLAB-27, and standard tube agglutination forBrucella were negative. Anteroposterior plain radiograph ofthe pelvis is normal (Figure 1). Pelvic magnetic resonanceimaging (MRI) demonstrated inflammatory change in leftpubic bone, adductor muscle, which suggested the diagnosisof osteomyelitis of the pubis (Figure 2). The diagnosis ofosteomyelitis of the symphysis pubis was based on reviewof the patient’s history, clinical findings, and radiologicalabnormalities. Treatment was started with a combination ofampicillin/sulbactam 6 g/day and ciprofloxacin 1500mg/day.After ten days of medical treatment, inguinal pain hadreduced progressively.The therapy was stopped after 6 weeks;he was very healthy, inflammatory manifestation in leftpubic bone in MRI regressed (Figure 3), and there was norecurrence of osteomyelitis of the symphysis pubis at one yearafter operation.
3. Discussion
Osteomyelitis of the symphysis pubis is a rarely describedentity. The etiologies of pubic osteomyelitis include
Hindawi Publishing CorporationCase Reports in RheumatologyVolume 2015, Article ID 845867, 3 pageshttp://dx.doi.org/10.1155/2015/845867

2 Case Reports in Rheumatology
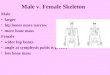
Figure 1: Anteroposterior plain radiograph of the pubis is normal.
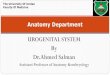
Figure 2: Pelvic MRI demonstrated inflammatory change in leftpubic bone (arrow) and adductor muscle.
hematogenous, traumatic, and iatrogenic (after urologicalor gynecological surgery) factors, and the influence ofother adjacent infection foci (e.g., prostate abscess, softtissue infection) [3]. The pathogenesis is still not clear.Pubic osteomyelitis is an entity characterized by pelvic pain,wide-based gait, and bony destruction of the margins of thepubic symphysis. It is difficult clinically to identify infectionof the pubis symphysis, as the symptoms are very nonspecificand do not present like a typical septic arthritis of a joint.However, we recommend having a high level of suspicion forpatients presenting with pubic, groin, and hip pain, especiallyin patients who have undergone inguinal hernia surgery. RossandHu reviewed 100 cases of pubic symphysis septic arthritis[4]. They demonstrated that this condition is not specificto any age group and can range from 7 to 86 years of age.Most common presenting signs and symptoms include fever,pubic tenderness, antalgic gait, and pain with active/passiverange of motion of hip. They identified several predisposingfactors including urological, gynecological procedures,pregnancy, athletes, malignancy, and intravenous druguse, as well as other invasive procedures. Osteomyelitis ofpubis should be considered in patients with pelvic pain,pubic tenderness, fever, and painful hip abduction. Pain
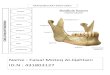
Figure 3: Pelvic MRI two months after completion of antibiotictherapy reveals no inflammatory change.
specially occurred by gait and spread to the perineal,testicular, suprapubic, and inguinal area. However, pain alsoaggravated by Valsalva maneuver and occurred in scrotumafter ejaculation [1]. C-reactive protein level, erythrocytesedimentation rate, and white blood cell count are eitherelevated in osteomyelitis pubis, while they are usually normalor slightly elevated in osteitis pubis [5]. Osteomyelitis of thepubis frequently begins unilaterally and then expands tothe other side of the pubic ramus. Symmetrical involvementis mostly present and bone destruction is progressive.Because radiographic imaging may be normal in acutepubic osteomyelitis, advanced imaging modalities shouldbe considered in clinical suspicion. In the present case,radiographic examination was normal while inflammatorychanges suggesting osteomyelitis were detected in MRI.Aspiration or open biopsy should be performed in thepatients who do not respond to conservative treatmentby means of clinical, laboratory, and radiological findings.However, most of the clinicians suggest taking directbiopsy without following conservative treatment responsein patients who have inguinal pain increasing by gait andsupporting laboratory and radiological findings after surgicalprocedure [1–3]. Because the present case did not acceptbiopsy, we diagnosed acute osteomyelitis pubis by clinicallyhaving fever and pelvic pain and elevations in CRP andWBC and demonstrating changes for osteomyelitis in MRI.The histological features of acute osteomyelitis pubis includegranulation tissue, areas of necrosis (sequestra), exudates,lymphocytic infiltration, and plasma cells. In chronicosteomyelitis pubis similar features are noted, but in additiondecreased vascularity and sclerotic new bone formation canbe observed. [5]. In present case there was no need for thebiopsy because of inguinal and pelvic pain increasing bygait, and laboratory and radiological findings supportingosteomyelitis of the symphysis pubis, and response to theconservative treatment.
Differential diagnosis of osteomyelitis of pubis shouldbe made from tuberculosis, brucellosis, primer or metastaticbone neoplasms, pubic osteolysis, subluxation of symphysispubis after delivery,muscle injury of pelvic girdle or sacroiliac

Case Reports in Rheumatology 3
joint, pelvic inflammatory disease, and ankylosing spondyli-tis. Histopathologic examination is an important diagnostictool for differentiation from primer bone tumours rarelyinvolving pubis such as multiple myeloma, reticular cell sar-coma, fibrosarcoma, and chondrosarcoma [3]. We excludedbrucellosis by negative Rose Bengal test and inappropriateclinical and laboratory findings. In differential diagnosis,spondyloarthropathies should be taken into consideration.Because clinical and laboratory findings are absent, involvedarea is not usual place of enthesitis, and radiological finding isnot resembled we excluded spondyloarthropathies includingankylosing spondylitis.
The treatment of osteomyelitis pubis is based on theintravenous administration of antibiotics. If the disease isprogressive in spite of specific antibiotic therapy, surgicaldebridement with curettage and jet lavage is indicated.Invasive surgical procedures seem not to be necessary inmost cases, due to the often spectacular response to simpleantibiotherapy in arthritis and in discitis [6]. We recommendstarting antibiotic immediately after culture is obtained formicrobiology. Thus, it is important that these infections areidentified early before the development of abscesses as surgi-cal or radiological intervention might then be warranted. Weopted for a treatment by high doses of ampicillin/sulbactamand ciprofloxacin for a duration of 6 weeks without surgicalintervention, with a good clinical, laboratory, and radiologicresponse (Figure 3).
In conclusion, osteomyelitis of the pubic symphysiscan have serious complications. The diagnosis should beconsidered in postoperative patients with disturbance ofgait, particularly in elderly patients who have undergonean operation for inguinal hernia. It can be treated withantibiotic medication and early administration of it shallprevent developing of complication.
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper.
References
[1] R. Mader and E. Yeromenco, “Pseudomonas osteomyelitisof the symphysis pubis after inguinal hernia repair,” ClinicalRheumatology, vol. 18, no. 2, pp. 167–169, 1999.
[2] O. P. Lakhwani, U. Ojha, P. Lakhwani, and N. Nagaich,“Osteomyelitis of pubis unusual complication and dilemma,”WebmedCentral Orthopaedics, vol. 4, no. 2, Article IDWMC004030, pp. 1–5, 2013.
[3] T. Koakutsu,M.Kawamura, K. Takada, andE. Itoi, “Osteomyeli-tis of the pubic symphysis as a complication of bladder necksuspension procedure with use of bone anchors: a case report,”Rheumatology: Current Research, vol. s16, no. 2, pp. 1–3, 2014.
[4] J. J. Ross and L. T. Hu, “Septic arthritis of the pubic symphysis:review of 100 cases,”Medicine, vol. 82, no. 5, pp. 340–345, 2003.
[5] S. M. Knoeller, M. Uhl, and G. W. Herget, “Osteitis orosteomyelitis of the pubis? A diagnostic and therapeutic chal-lenge: report of 9 cases and review of the literature,” ActaOrthopaedica Belgica, vol. 72, no. 5, pp. 541–548, 2006.
[6] D. Wilmes, P. Omoumi, J. Squifflet, O. Cornu, H. Rodriguez-Villalobos, and J. C. Yombi, “Osteomyelitis pubis caused byKingella kingae in an adult patient: report of the first case,” BMCInfectious Diseases, vol. 12, article 236, 2012.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com