Embed Size (px)
Citation preview

AMERICAN THORACIC SOCIETYDOCUMENTS
An Official American Thoracic Society Clinical Practice Guideline:Pediatric Chronic Home Invasive VentilationLaura M. Sterni, Joseph M. Collaco, Christopher D. Baker, John L. Carroll, Girish D. Sharma, Jan L. Brozek,Jonathan D. Finder, Veda L. Ackerman, Raanan Arens, Deborah S. Boroughs, Jodi Carter, Karen L. Daigle,Joan Dougherty, David Gozal, Katharine Kevill, Richard M. Kravitz, Tony Kriseman, Ian MacLusky,Katherine Rivera-Spoljaric, Alvaro J. Tori, Thomas Ferkol, and Ann C. Halbower; on behalf of the ATS PediatricChronic Home Ventilation Workgroup
THIS OFFICIAL CLINICAL PRACTICE GUIDELINE OF THE AMERICAN THORACIC SOCIETY (ATS) wAS APPROVED BY THE ATS BOARD OF DIRECTORS, JANUARY 2016
Background:Childrenwith chronic invasive ventilator dependenceliving at home are a diverse group of children with special health careneeds. Medical oversight, equipment management, and communityresources vary widely. There are no clinical practice guidelinesavailable to health care professionals for the safe hospital dischargeand home management of these complex children.
Purpose: To develop evidence-based clinical practice guidelines forthe hospital discharge and home/community management ofchildren requiring chronic invasive ventilation.
Methods: The Pediatric Assembly of the American Thoracic Societyassembled an interdisciplinary workgroup with expertise in the careof children requiring chronic invasive ventilation. The experts developedfourquestionsofclinical importanceandusedanevidence-basedstrategyto identify relevant medical evidence. Grading of RecommendationsAssessment, Development, and Evaluation (GRADE) methodologywas used to formulate and grade recommendations.
Results: Clinical practice recommendations for the management ofchildren with chronic ventilator dependence at home are provided,and the evidence supporting each recommendation is discussed.
Conclusions: Collaborative generalist and subspecialistcomanagement is the Medical Home model most likely to besuccessful for the care of children requiring chronic invasiveventilation. Standardized hospital discharge criteria are suggested.An awake, trained caregiver should be present at all times, and at leasttwo family caregivers should be trained specifically for the child’scare. Standardized equipment for monitoring, emergencypreparedness, and airway clearance are outlined. Therecommendations presented are based on the current evidence andexpert opinion and will require an update as new evidence and/ortechnologies become available.
Keywords: respiratory insufficiency; mechanical ventilators;discharge planning; medical home; children
ContentsOverviewIntroductionQuestionsMethodsClinical Questions andRecommendations
Question 1: Should the MedicalHome or Family-centeredCare Concepts Be Used in theCare of Children Requiring
Chronic Home InvasiveVentilation?
Question 2: Should StandardizedDischarge Criteria Be UsedWhen Planning the HospitalDischarge of ChildrenRequiring Chronic HomeInvasive Ventilation?
Question 3: Should HomeCaregivers Be SpecificallyTrained in the Care of Children
Requiring Chronic HomeInvasive Ventilation?
Question 4: Should StandardHome EquipmentRequirements Be AppliedWhen Planning for theEquipment Needs of ChildrenRequiring Invasive VentilatorSupport in the Home?
Research PrioritiesConclusions
An Executive Summary of this document is available at http://www.atsjournals.org/doi/suppl/10.1164/rccm.201602-0276ST
Correspondence and requests for reprints should be addressed to Laura M. Sterni, M.D., Eudowood Division of Pediatric Respiratory Sciences, The JohnsHopkins University School of Medicine, 200 North Wolfe Street, Baltimore, MD 21287. E-mail: [email protected]
This article has an online supplement, which is accessible from this issue’s table of contents at www.atsjournals.org
Am J Respir Crit Care Med Vol 193, Iss 8, pp e16–e35, Apr 15, 2016
Copyright © 2016 by the American Thoracic Society
DOI: 10.1164/rccm.201602-0276ST
Internet address: www.atsjournals.org
e16 American Journal of Respiratory and Critical Care Medicine Volume 193 Number 8 | April 15 2016

Overview
The goal of this guideline is to provide anapproach, based on the available evidenceand the consensus of the assembled groupof experts, to the hospital discharge andsubsequent management of children usinginvasive ventilation in the home. Theguideline is intended for use by pediatricpulmonologists, pediatric intensive carephysicians, pediatricians, family physicians,pediatric nurse practitioners, pediatricphysician assistants, pediatric nurses (bothin the hospital and in the home), andrespiratory therapists who care for thesepatients. The recommendations made in theguideline are not intended to impose astandard of care. Children requiring invasiveventilation are a diverse group of patientswith complex health care needs. There are awide variety of unique and important socialand medical issues that will need to beconsidered when planning for the care ofeach individual patient. It is our hope that theguideline presented can provide practitionersa basis for sound decision making and safe,effective care for this group of children.
An interdisciplinary PediatricChronic Home Ventilation Workgroup wasconvened by the Pediatric Assembly of theAmerican Thoracic Society to develop aguideline to facilitate comprehensivehome management of respiratorytechnology–dependent children andhighlight areas for future research. Four keyclinical questions were identified by theWorkgroup and addressed in the guideline.The recommendations formulated arebased on the indirect evidence in theavailable literature, which consisted ofuncontrolled studies or observations andthe consensus of the Workgroup members.Grading of Recommendations Assessment,Development and Evaluation (GRADE)methodology was used to assess the qualityof the published evidence and evaluate thestrength of the recommendations. Thefollowing recommendations were made bythe Workgroup:
1. For children requiring chronic homeinvasive ventilation, we suggest acomprehensive Medical Homecomanaged by a generalist andrespiratory subspecialist (Strength ofRecommendation: Conditional; Qualityof Evidence: Very Low).
2. For children requiring chronic invasiveventilation, we suggest the use of
standardized discharge criteria toobjectively assess readiness for care inthe home (Strength of Recommendation:Conditional; Quality of Evidence:Very Low).
3. We recommend that an awake andattentive trained caregiver be in thehome of a child requiring chronicinvasive ventilation at all times(Strength of Recommendation: Strong;Quality of Evidence: Very Low).
4. For children requiring chronic invasiveventilation, we suggest that at least twospecifically trained family caregivers areprepared to care for the child in thehome (Strength of Recommendation:Conditional; Quality of Evidence:Very Low).
5. We suggest that ongoing education toacquire, reinforce, and augment skillsrequired for patient care be providedto both the family and professionalcaregivers of children requiring chronichome invasive ventilation (Strengthof Recommendation: Conditional;Quality of Evidence: Very Low).
6. For children requiring chronic homeinvasive ventilation, we suggestmonitoring, especially when the childis asleep or unobserved, with a pulseoximeter rather than use of acardiorespiratory monitor or sole useof the ventilator alarms (Strength ofRecommendation: Conditional; Qualityof Evidence: Very Low).
7. For children requiring chronic homeinvasive ventilation, we recommendregular maintenance of home ventilatorsand all associated equipment as outlinedby the manufacturer.
8. We suggest the following pieces ofequipment for use in the home whencaring for a patient on home mechanicalventilation: the ventilator, a back-upventilator, batteries, a self-inflating bagand mask, suctioning equipment(portable), heated humidifier,supplemental oxygen for emergencyuse, nebulizer, and a pulse oximeter(nonrecording) (Strength ofRecommendation: Conditional;Quality of Evidence: Very Low).
9. We suggest that a mechanicalinsufflation–exsufflation device be usedto help maintain airway patency inpatients requiring home mechanicalventilation with ineffective cough,including, but not limited to, thosewith neuromuscular disease with poor
respiratory muscle strength (Strength ofRecommendation: Conditional; Qualityof Evidence: Very Low).
Introduction
Of the more than 9.4 million children in theUnited States with special health care needs,few present with more challenges than thosefaced by children requiring chronic homeinvasive ventilation (1–3). The shift fromcare in the pediatric intensive care unitwithin the hospital to intensive care athome requires invested families, multipletrained in-home caregivers, sophisticatedtechnology, financial support, and readyaccess to primary and subspecialty medicalcare. Despite the mandate for nationalaction by the Institute of Medicine in 2003for children with special health care needs(CSHCN), there are no evidence-basedguidelines for this complex subgroup oftechnology-dependent children (4). ThePediatric Assembly of the AmericanThoracic Society (ATS) proposed thedevelopment of an evidence-based clinicalpractice guideline for management ofchildren requiring invasive mechanicalventilation at home. An interdisciplinaryPediatric Chronic Home VentilationWorkgroup was convened to developa guideline to facilitate comprehensivehome management of respiratorytechnology–dependent children andhighlight areas for future research. Theparticipants in this guideline includeexperts in pediatric sleep medicine andpulmonary and critical care, ATS assemblychairs, and physician and nursing expertsin the inpatient and outpatient care ofchildren with advanced respiratory needs.
We recognize that children requiringinvasive ventilation are a diverse group ofpatients. These patients have advancedpulmonary disease, neuromotor disease,or defects in respiratory drive with thecommon consequence being insufficientminute ventilation to maintainnormocapnia and/or adequate oxygensaturations. They also range in severity,from children who have inadequaterespiration solely during sleep, hencerequiring nocturnal respiratory assistancealone, to those who require ventilationaround the clock for survival. Despite thisheterogeneity, common themes andchallenges are found. The Workgroupinvestigated four areas that are critical in
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents e17

the care of these patients, addressingcoordination of care, readiness for homecare, training of caregivers, and necessaryequipment, and made recommendationson the basis of available literature andconsensus of the Workgroup experts.
The goal of this guideline is to providean approach, on the basis of the availableevidence and the consensus of the assembledgroup of experts, to the hospital dischargeand subsequent management of childrenusing invasive ventilation in the home. Theguideline is intended for use by pediatricpulmonologists, pediatric intensive carephysicians, pediatricians, family physicians,pediatric nurse practitioners, pediatricphysician assistants, pediatric nurses (bothin the hospital and in the home), andrespiratory therapists who care for thesepatients. The recommendations made in theguideline are not intended to impose astandard of care. There are a wide variety ofunique and important social and medicalissues that will need to be considered whenplanning for the care of each individualpatient. It is our hope that the guidelinepresented herein can provide practitioners abasis for sound decision making and safe,effective care for this group of children.
Questions
The key clinical questions identified by theWorkgroup as important for target users are:
1. Should the Medical Home or family-centered care (FCC) concepts be used inthe care of children requiring chronichome invasive ventilation?
2. Should standardized discharge criteriabe used when planning the hospitaldischarge of children requiring chronichome invasive ventilation?
3. Should home caregivers be specificallytrained in the care of children requiringchronic home invasive ventilation?
4. Should standard home equipmentrequirements be applied when planningfor the equipment needs of childrenrequiring invasive ventilator support inthe home?
Methods
These clinical practice guidelines wereprepared according to the methods of theATS, which are described in detail in theonline supplement and summarized in
Table 1. The Patient/Population,Intervention, Comparison, and Outcome(PICO) framework was used to searchsystematically for relevant evidence.The searches identified no publishedrandomized controlled trials orcontrolled observational studies. Therecommendations are, therefore, based onuncontrolled studies and the clinicalobservations of the Workgroup members.Grading of Recommendations Assessment,Development, and Evaluation (GRADE)methodology was used to assess the qualityof the published evidence and rate thestrength of the recommendations (5). Allevidence that was selected to inform theWorkgroup’s decisions was characterizedas very low quality, indicating that theestimated effects of our suggestedinterventions are uncertain and very likelyto be affected by future research. Thestrength of one recommendation was ratedas strong, and all others were rated asconditional; the appropriate interpretationof the strength of a recommendation isprovided in Table 2 (5). Therecommendations are detailed in Table 3.
Clinical Questions andRecommendations
Question 1: Should the Medical Homeor Family-centered Care ConceptsBe Used in the Care of ChildrenRequiring Chronic Home InvasiveVentilation?
Background. The Workgroup believed thatincorporating the concepts of FCC and theMedical Home into the care of the medicallycomplex children requiring chronic homeinvasive ventilation is a priority. TheWorkgroup found no publishedexperimental or observational studiesexamining the effect of using FCC andMedical Home models on outcomes inchildren requiring invasive ventilation in thehome. There is literature describing andexamining these models in children withcomplex health care needs, and this isreviewed in the following section. On thebasis of the clinical experience of theWorkgroup and the available indirectliterature reviewed, we suggest using acomprehensive Medical Home comanagedby the generalist and respiratory subspecialistfor children requiring chronic home invasiveventilation. This recommendation places
high value on the possible medical and socialbenefits and low value on the potential risks,which may include increased resource useand provider time. Structure andcomponents of the comanaged MedicalHome are described later and in Table 4.
CSHCN. In 1998, CSHCNwere definedby the Maternal and Child Health Bureau(MCHB) of the U.S. Health Resourcesand Services Administration as follows:
CSHCN are those who have or are atincreased risk for a chronic physical,developmental, behavioral, or emotionalcondition and who also require health andrelated services of a type or amount beyondthat required by children generally (6).
The “health and related services”referenced by the above definition includephysician subspecialists, hospitalsspecialized in the care of children,therapeutic services (e.g., speech, physical,occupational, and others), home healthservices, home nursing services, familysupport services such as family counseling,comprehensive case management, carecoordination, specialized equipment andsupplies, and related services such as socialservices, transportation, special education,medical daycare, early intervention, andothers. Children with a tracheostomy onlong-term ventilatory support clearlyqualify as CSHCN and, indeed, representthe extreme end of the spectrum withrespect to their complexity, intensity of carerequirements, service needs, and risk ofadverse outcome in their daily lives.
The definition of CSHCN does notrequire a specific diagnosis or condition; itis intentionally broad and inclusive of awide spectrum of medical conditions. Theintention was to assist and guide publicprograms and other organizations in programplanning. From its inception, this definitionhas been used in program development byMCHB, U.S. Health Resources and ServicesAdministration, and state Title V programsfor needs assessment and to facilitate meetingfederal requirements when developing acommunity system of services forCSHCN (6).
Location of care: home versusinstitutional care. Home care for themajority of ventilator-dependent children isa relatively recent development. In theUnited States, long-term care of ventilator-dependent children with their family, in thehome environment, dates from the 1970s
AMERICAN THORACIC SOCIETY DOCUMENTS
e18 American Journal of Respiratory and Critical Care Medicine Volume 193 Number 8 | April 15 2016

and 1980s, when portable ventilatorsbecame practical for home use. A SurgeonGeneral’s Department of Health andHuman Services workshop on ventilator-dependent children, held in 1982,enumerated principles that included “thefull participation of the parents and siblingsin all the processes of medical care” and“linking up the child and the family withavailable social and medical support groupsin the community,” with a major goal ofdeveloping “strategies for providingcommunity-based services as an alternativeto acute care facilities” (2). A major shiftaway from institutional care was givennational recognition by the U.S. SurgeonGeneral’s 1987 commitment to “family-centered, community-based, coordinated
care” for CSHCN (3). The SurgeonGeneral’s report indicated that CSHCN“deserve to live with their families in theirown communities, and to share in theeveryday experiences most Americans takefor granted. We must make a commitmentto provide the kinds of health care thesechildren require, in ways that allow them toparticipate as fully as possible in all aspectsof family and community life.” The UnitedStates national objectives for improvinghealth, Healthy People 2010 and 2020,both have explicit goals of reducing thenumber of children and youth withdisabilities living in congregate careresidences (7).
Hospital pediatric intensive care units,acute-care wards, and even chronic
residential care facilities are not designedfor family-centered child development,schooling, or family and social life or to meetthe long-term developmental needs of achild. Thus, for decades U.S. governmenthealth agencies have accepted as coreprinciples that the best place for thewellbeing of a technology-dependent childis with the family/caregivers in thecommunity, and that all aspects of themedical care should be family centered,coordinated, and integrated withcommunity services (2, 3).
FCC. At its core, FCC of a child is apartnership approach to decision makingbetween health professionals and the familyin all aspects of care (8). The basic principlesof FCC shared by all current definitionsinclude 1) unbiased, open informationsharing with the patient and family; 2) aworking relationship with the family thathonors and respects differences; 3)collaborative decision making that includesfamilies as partners; 4) negotiation ofmedical care plans and desired outcomeswith the family; and 5) all decision makingand medical care within the context of thechild’s family, home, daily activities,school, and life in the community (8). FCCand the closely related patient-centered careapproach have been endorsed by multipleU.S. government health care agenciesincluding MCHB, multiple medicalsocieties, Healthy People 2020, and theInstitute of Medicine. In a 2012 PolicyStatement, the American Academyof Pediatrics (AAP) recommendedincorporation of the core concepts ofpatient- and family-centered care into allaspects of pediatric medical care anddefines the patient and family as integralmembers of the health care team (9).Numerous benefits of FCC have beendemonstrated for patients and families
Table 2. Interpretation of Strong versus Conditional Strength of Recommendation
User Group Strong Recommendation Conditional Recommendation
Patients Most individuals in this situation would want the recommendedcourse of action and only a few would not. Formal decisionaids are not likely to be needed to help individuals makedecisions consistent with their values and preferences.
The majority of individuals in this situation wouldwant the suggested course of action, but manywould not.
Clinicians Most individuals should receive the intervention. Adherenceto this recommendation according to the guideline couldbe used as a quality criterion or performance indicator.
Understand that different choices will be appropriatefor individual patients. Decision aids may be usefulin helping individuals make decisions consistentwith their values and preferences.
Policy makers The recommendation can be adopted as policy in mostsituations.
Policy making will require substantial debates andinvolvement of many stakeholders.
Table 1. Summary of Methodology
Method Yes No
Panel assemblyIncluded experts for relevant clinical disciplines XIncluded individuals who represent the views of patientsand society at large
X
Included a methodologist with appropriate expertise(documented expertise in conducting systemic reviewsto identify the evidence base and the development ofevidence-based recommendations)
X
Literature reviewPerformed in collaboration with librarian XSearched multiple electronic databases XReviewed reference lists of retrieved articles X
Evidence synthesisApplied prespecified inclusion and exclusion criteria XEvaluated included studies for sources of bias XExplicitly summarized benefits and harms XUsed PRISMA1 to report systematic review XUsed GRADE to describe quality of evidence X
Generation of recommendationsUsed GRADE to rate the strength of recommendations X
Definition of abbreviations: GRADE =Grading of Recommendations Assessment, Development, andEvaluation; PRISMA1 = Preferred Reporting Items for Systematic Reviews and Meta-Analysis 1.
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents e19

Table 3. Summary of Recommendations
Recommendation StrengthQuality ofEvidence Remarks
1. For children requiring chronic homeinvasive ventilation, we suggest acomprehensive Medical Home comanagedby the generalist and respiratorysubspecialist.
Conditional Very low The Medical Home model can provide family-centered carefor children with special health care needs, includingchildren on home invasive ventilation. This recommendationplaces a high value on the possible medical and socialbenefits to this intervention and places low value onthe potential risks, which may include increasedprovider time.
2. For children requiring chronic invasiveventilation, we suggest the use ofstandardized discharge criteria toobjectively assess readiness for care in thehome.
Conditional Very low The Workgroup believed that comprehensive standardizeddischarge criteria would encourage a complete review ofeach patient’s medical stability and home situation tofacilitate safe discharge. The goal is to identify andeliminate important barriers to care in the home beforedischarge and consider alternate care arrangements ifobstacles cannot be eliminated. Weight given to eachcomponent of the proposed criteria would vary frompatient to patient. The recommendation places high valueon the potential benefits of considering all facets of achild’s care in the home before discharge and low value onthe increased provider time and resource use that may berequired.
3a. We recommend that an awake andattentive trained caregiver be in the homeof a child requiring chronic invasiveventilation at all times.
Strong Very low Despite very low quality evidence supporting thisrecommendation, the Workgroup was confident that inthis case the desirable consequences would clearlyoutweigh the undesirable consequences of following thisrecommendation. Lack of an awake and attentive trainedcaregiver would place the child in a life-threateningsituation. Training of caregivers is irrelevant if one is notavailable to respond to an emergent situation. For mostfamilies this requires the support of a professionalappropriately trained in-home caregiver to allow familycaregivers time to sleep, work, and maintain a life balance.This recommendation places a high value on the safetyof the patient, and low value is placed on avoiding theincreased use of resources and the possible disruption tofamilies who may need to accommodate a professionalcaregiver in their home.
3b. For children requiring chronic invasiveventilation, we suggest that at least twospecifically trained family caregivers areprepared to care for the child in the home.
Conditional Very low The experience of the Workgroup and available data indicatethat a lone trained family caregiver would rarely be capableof shouldering the entire burden of care for a child usinginvasive ventilation in the home. This recommendationplaces high value on the safety of the patient and quality oflife of caregivers and low value on increased resource usefor training more than one caregiver.
3c. We suggest that ongoing education toacquire, reinforce, and augment skillsrequired for patient care be provided toboth the family and professionalcaregivers of children requiring chronichome invasive ventilation.
Conditional Very low The Workgroup believed, based on clinical experience, thatpractitioners and professional personnel agencies muststrive to provide ongoing education to family andprofessional caregivers. Continuing education wouldhelp reinforce learned skills and allow training on newtechnologies and protocols. This recommendation placesa high value on safety and on the potential clinical benefitsto the patient and a low value on increased cost andresource use.
4a. For children requiring chronic homeinvasive ventilation, we suggestmonitoring, especially when the child isasleep or unobserved, with a pulseoximeter rather than use of acardiorespiratory monitor or sole use ofthe ventilator alarms.
Conditional Very low Small indirect studies and the experience of the Workgroupsuggest that ventilator alarms may not always functioncorrectly. Furthermore, hypoxemia is most likely to be thefirst indicator of a serious issue in a child with respiratorydisease. The workgroup believes pulse oximetry is thepreferred method for monitoring patients on homemechanical ventilation. This recommendation placeshigh value on the safety of the child and low value onpossible increase in caregiver burden secondary to falsealarms.
(Continued )
AMERICAN THORACIC SOCIETY DOCUMENTS
e20 American Journal of Respiratory and Critical Care Medicine Volume 193 Number 8 | April 15 2016
and for physicians who practice patient- orfamily-centered care, including CSHCN(9–11). There are no studies to date ofpatient- or family-centered care specificallyfor children receiving long-termmechanical ventilation.
The Medical Home. The MedicalHome is the best-known model of healthcare delivery for CSHCN. It is important tonote that it is not a specific geographicallocation, medical office, or provider.The AAP describes the Medical Homeconcept as care that is 1) accessible, 2)comprehensive, 3) compassionate, 4)continuous, 5) coordinated, 6) culturallycompetent, and 7) family centered (12).Most concepts of the Medical Homefeature a primary Medical Home provider,and it is often assumed that it must be aprimary care physician. However, thereare no requirements that the primaryMedical Home provider be a primarycare physician. Similarly, there are norequirements concerning where it is based;as long as the Medical Home meets thecriteria above, it can be primary care based,tertiary care based, or a primary–tertiary
comanagement hybrid model. However, theAAP is clear and specific on the point thatMedical Home care “should be delivered ordirected by well-trained physicians whoprovide primary care and help to manageand facilitate essentially all aspects ofpediatric care” (13). Numerous state andfederal laws mandate community-based,family-centered, coordinated care programsfor CSHCN, and the AAP and MCHBstrongly endorse the Medical Homecomprehensive care model as the preferredapproach for all children, includingCSHCN (12, 14, 15).
Care models for children receivingchronic invasive mechanical ventilation. Asoutlined above, in the United States, FCC isalready mandated for CSHCN, and theMedical Home concept is the recommendedmodel of comprehensive care coordinationfor CSHCN. Given that children dependenton invasive, long-term mechanicalventilation clearly are CSHCN, theseapproaches to health care delivery andcoordination are already mandatory for thispopulation. Thus, the question for thisgroup of children, at the extreme end of the
complexity spectrum and dependent onhighly specialized, complicated life-sustaining technology, remains: What is thebest model for delivering Medical Homecare? Should primary Medical Homemanagement for the ventilator-dependentchild be provided by the primary carephysician, the tertiary care pulmonologist, ahybrid model in which both the primarycare and subspecialty physician act asCo-Medical Home providers, or a hospital-based comprehensive Medical Home clinic?The remainder of this section discussesthe evidence for a Medical Home conceptand considers possible models of MedicalHome care delivery.
Care needs of the ventilator-dependentchild: a complex mix of specialty andprimary care. The care, equipment, supply,and monitoring needs specific to theventilator-dependent child are outlined inthe following sections of this document. Therequired technology always includes thetracheostomy, ventilator, humidifier, andsuction devices and often includes addedtechnology such as airway clearance devices,mechanical insufflation–exsufflation (MI-E)
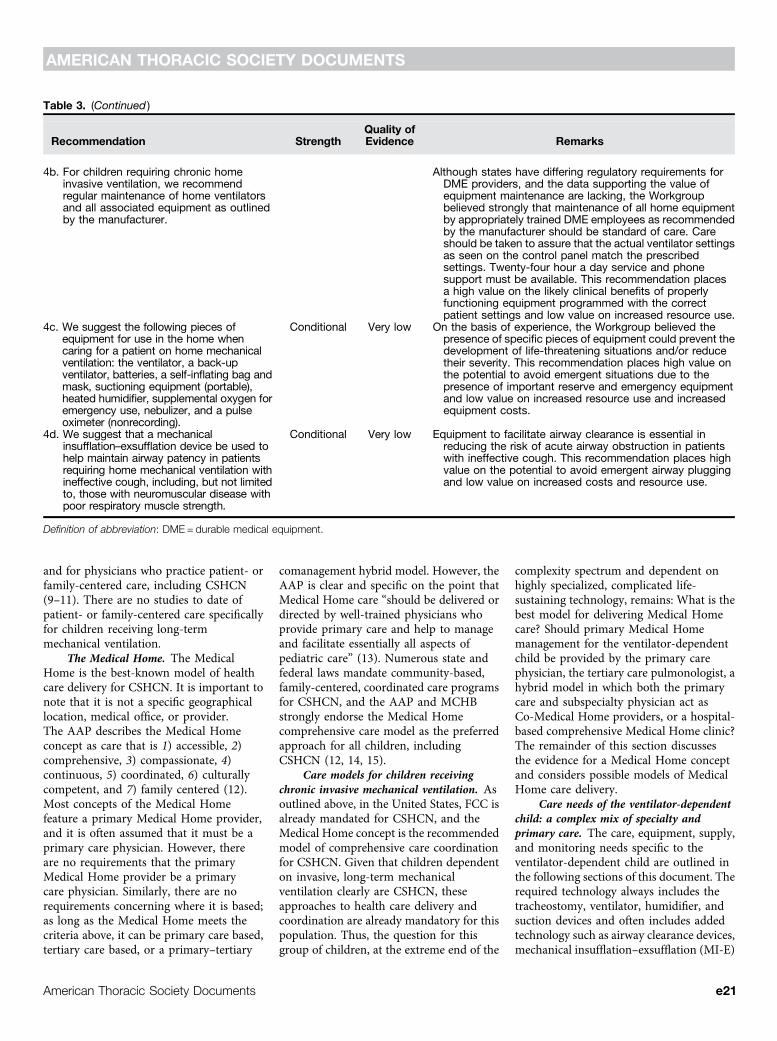
Table 3. (Continued )
Recommendation StrengthQuality ofEvidence Remarks
4b. For children requiring chronic homeinvasive ventilation, we recommendregular maintenance of home ventilatorsand all associated equipment as outlinedby the manufacturer.
Although states have differing regulatory requirements forDME providers, and the data supporting the value ofequipment maintenance are lacking, the Workgroupbelieved strongly that maintenance of all home equipmentby appropriately trained DME employees as recommendedby the manufacturer should be standard of care. Careshould be taken to assure that the actual ventilator settingsas seen on the control panel match the prescribedsettings. Twenty-four hour a day service and phonesupport must be available. This recommendation placesa high value on the likely clinical benefits of properlyfunctioning equipment programmed with the correctpatient settings and low value on increased resource use.
4c. We suggest the following pieces ofequipment for use in the home whencaring for a patient on home mechanicalventilation: the ventilator, a back-upventilator, batteries, a self-inflating bag andmask, suctioning equipment (portable),heated humidifier, supplemental oxygen foremergency use, nebulizer, and a pulseoximeter (nonrecording).
Conditional Very low On the basis of experience, the Workgroup believed thepresence of specific pieces of equipment could prevent thedevelopment of life-threatening situations and/or reducetheir severity. This recommendation places high value onthe potential to avoid emergent situations due to thepresence of important reserve and emergency equipmentand low value on increased resource use and increasedequipment costs.
4d. We suggest that a mechanicalinsufflation–exsufflation device be used tohelp maintain airway patency in patientsrequiring home mechanical ventilation withineffective cough, including, but not limitedto, those with neuromuscular disease withpoor respiratory muscle strength.
Conditional Very low Equipment to facilitate airway clearance is essential inreducing the risk of acute airway obstruction in patientswith ineffective cough. This recommendation places highvalue on the potential to avoid emergent airway pluggingand low value on increased costs and resource use.
Definition of abbreviation: DME = durable medical equipment.
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents e21

devices, supplemental oxygen, monitoringdevices such as pulse oximeters, and,typically, numerous medications thatrequire the use of aerosol delivery devices.As outlined in sections below, continuous24 h/d, 7 d/wk monitoring is requiredfor these children due to the high riskof morbidity and mortality (16, 17).Therefore, skilled care by trained caregivers,usually a combination of family memberswith home nursing services when available,is required.
Children dependent on long-termmechanical ventilation are at risk for severalcomplications directly related to theirchronic pulmonary condition, includingpulmonary hypertension, recurrentpulmonary infections, poor growth,developmental delay, and life-threateningemergency events such as tracheostomyplugging, accidental decannulation, andother causes of cardiorespiratory arrest.Thus, caregivers (the parents and homecareproviders) must be able to perform allroutine care, recognize and be able totroubleshoot problems, and have the skilland training to respond effectively. Oversightof the care outlined above is typicallyconsidered the primary responsibility of thepulmonologist and pulmonary care team. Thedegree of involvement of otolaryngology fortracheostomy care and airway issues or of
cardiology for issues related to pulmonaryhypertension varies between states andinstitutions.
Many ventilator-dependent childrenalso have other major medical conditionssuch as neurological disorders (e.g., cerebralpalsy, central nervous system injury,congenital central hypoventilation),neuromuscular disorders (e.g., musculardystrophy), congenital anomalies (includinga wide variety of genetic syndromes), and/orcongenital heart disease (17, 18). Thesecomorbid conditions each may have itsown set of intensive health care needs andmay involve dependence on nonrespiratorytechnologies (e.g., renal dialysis, cardiacpacemaker, ventriculoperitoneal shunt,baclofen pump) involving differentsubspecialists, such as gastroenterology,cardiology, otolaryngology, neurology, andothers. Frequently, the ventilator-dependent child also has chronic dysphagia,with limited oral intake and dependenceon liquid feedings via gastrostomy orgastrojejunal feeding tube. Some of thecomorbid conditions may interact; acommon example is dysphagia leadingto recurrent/chronic aspiration andresulting in adverse effects on respiratoryhealth.
Children on long-term ventilationshould also receive speech therapy, physical
therapy, and occupational therapy. Theymay require evaluation and therapies fordevelopmental delay and behavioral issues.In the educational sphere, the family of theventilator-dependent child interacts atmultiple levels with schools, includingschool administrators, nurses, teachers,special education teachers, and sometimestherapists. School attendance outside thehome for the child on long-term invasiveventilation is complicated. In additionto the ventilator, suction devices, othertracheostomy care supplies, and monitoringequipment, the child may be onsupplemental oxygen. Children withtracheostomy must have a trained caregiverpresent at all times, even in school. Many, ifnot most, require specialized wheelchairsand other adaptive equipment and havecomplex transportation requirements.Families must deal continuously withthe legal and financial aspects of thiscomplex, high-intensity, high-cost homecare.
In addition to all of the aboveservices, the ventilator-dependent childrequires primary care services commonto all children, including immunizations,well-child care, anticipatory guidance,and evaluation and treatment forcommon childhood infections and otherdisorders.
Table 4. Features of a Comanaged Medical Home for Children Requiring Chronic Invasive Ventilation in the Home
The care would be family/patient centered.d Recognition of patient/family preferences, social services availability, barriers to communication or medical provision is necessary.
Medical Home provider oversight would be provided by a collaborative partnership between the generalist and pediatricpulmonologist, and other necessary subspecialists.
d Keeping in mind that many children requiring mechanical ventilation are equally dependent on subspecialists, such as neurologists,gastroenterologists, physical therapists, etc., this collaborative partnership depends on the situation and will require oversight from aspecific provider most accessible to the family and identified as primarily accountable. This provider is frequently but not necessarily theprimary care provider.
The specific roles and responsibilities of each provider would be clearly delineated for each practitioner, all members of bothteams, and the patient and family.
d In practice, a written summary of responsibilities will be provided to the team and family by a social worker or nurse or primary careprovider outlining expectations and order of communication channels.
The pulmonologist and team would be responsible for management of all pulmonary and related aspects of care.The generalist would be responsible for all aspects of primary care.The comanagement collaborative would decide and delineate responsibility for comprehensive assessment, coordination, and
management of all other aspects of care.d This includes access to medical care, transportation, family care and respite, access to nutritional needs, community resources, etc. Asocial worker or local public health resource may be crucial to assist the primary care provider. Pulmonologists, medical specialists, andtheir teams will be required to assist in coordination of complex care requirements and appointments to lessen the burden on the family.Much care can be delegated to the local primary caregivers with communication from the specialist teams.
Effective communication tools would be used to ensure effective implementation of the comprehensive care plan, withoutredundancy or duplication.
d Ideally, access to the same electronic medical record system for communication between the primary care provider, specialists, nursingstaff, and social workers would allow sharing of family communications, expected appointments, and ongoing medical issues. If thiselectronic medical record system is not available to all providers, communications should be outlined in writing to the comanagementcollaborative.
AMERICAN THORACIC SOCIETY DOCUMENTS
e22 American Journal of Respiratory and Critical Care Medicine Volume 193 Number 8 | April 15 2016

Medical care for the ventilator-dependent child: family stress, frustration,and disruption. For CSHCN, carecoordination has been defined as “a processthat links children with special health careneeds and their families to services andresources in a coordinated effort tomaximize the potential of children andprovide them with optimal health care”(19). At the present time, health care for theventilator-dependent child is a complexmix of primary care and subspecialty careneeds involving multiple disciplines, withcare coordination often defaulting to thefamily. Families often cite care coordinationand navigating the complex, fragmentedhealth care system as major stressors intheir daily lives (20).
In the care of children with specialheath care needs, the specific roles andresponsibilities of the primary care andsubspecialty physicians and their teamsare often not clearly delineated. Carecoordination and communication can becomplex, confusing, and frustrating forfamilies, especially in children requiring carefrom multiple subspecialists. Where is theMedical Home based? Which health carepractitioner is the primary Medical Homeprovider? Who takes responsibility forcomprehensive care coordination? Whatare the specific responsibilities of eachsubspecialist involved in the child’s care?Who monitors communication between allinvolved services?
Medical complexity is a major factordetermining the quality of care in CSHCN.Indeed, of CSHCN, medically complexchildren (those requiring special medicalequipment such as tracheostomy orgastrostomy tubes) have higher unmetneeds in health care and community-basedservices, such as assistive devices and specialtherapies (21). Focus group discussionsconducted with regional coordinatorsof early intervention programs inMassachusetts identified significantcommon issues in medically complexchildren requiring mechanical ventilation(22). The lack of expertise of communitycaregivers leaves the training of staff tothe parents, who justifiably worry aboutchild safety. Anxiety can increase overtime with worry about sudden healthchanges (23). Families of children withrespiratory insufficiency can becomephysically and socially isolated due to thedifficulty finding family supports orsufficiently trained home-care workers
to provide respite care or time for work(24, 25).
Due to a nationwide shortage ofnursing, unfilled nursing shifts at homebecome the parent’s responsibility (26, 27).Family stress, marital problems, and sleepdeprivation are regular occurrences whencaregiving is left to an unsupported family(28–31). Travel logistics and trouble withcoordination of medical care is increased infamilies without an established MedicalHome (24). With all of the constraintsinvolved in caring for the medicallycomplex child, there is a high rate of missedwork, financial stress, and parentalunemployment (32). Parents of CSHCNhave higher rates of poor physical andemotional health and depression (33, 34).In families with a child affected by cerebralpalsy, parents report higher systemicsymptoms of illness and chronic conditions(35). Family-centered care provided via aMedical Home approach aims to reducestress by providing care coordination,resources to help navigate the health caresystem, and community support (36).
Challenges of care delivery forventilator-dependent children. As notedabove, ventilator-dependent childrenrepresent an extreme on the severe end ofthe spectrum of children with medicalcomplexity. A study of inpatient health careuse data highlights some of the differencesbetween ventilator-dependent children andother children with complex chronic healthconditions. Children dependent on long-term ventilation had longer lengths of stayin the hospital, greater total costs, higher riskof death, greater use of home health care,and a greater likelihood of transfer to anonacute facility (37). Although the numberof children dependent on long-termventilation has increased in recent years,there is a dearth of data regarding theepidemiology of these children and howthey live and receive medical care outside ofthe acute care setting (16, 22, 37, 38).
The 2012 AAP clinical report entitled“Home Care of Children and Youth withComplex Care Needs and TechnologyDependencies” delineates desirable featuresof any Medical Home for children withcomplex medical and developmental issues(18). Unfortunately, the reality of deliveringor receiving that medical care often departssharply from the coordinated and family-centered care recommended. Fragmented,uncoordinated, and inefficient care systemshave been described frequently in the
medical literature (20, 23, 39). Pilotprograms that provide Medical Homesand coordinate care have demonstratedimproved outcomes and decreased overallhealth care expenditures (39–42). However,these programs operate at financial deficitsand include children with complex chronicconditions in general, not specifically thosewho require long-term ventilation.
Information regarding the currentpatterns of health care delivery to ventilator-dependent children comes largely frominformal discussion among experts andlimited studies (22). In many cases, apediatric pulmonary group serves some ofthe Medical Home functions, providingmedical coverage and care coordination inthe ambulatory, emergency department,inpatient, and home environment, 24 hoursper day and 7 days per week. This roleis similar to that of the special needsphysician in the primary care–tertiary carepartnership model described by Gordonand colleagues (39). A number of centershave chronic ventilation programs withdedicated nurse coordinators, usuallyhoused in the pediatric pulmonarydivisions. In major tertiary care centers,ambulatory visits to a pulmonologist ofteninclude additional visits with othermembers of the health care team, such asrespiratory therapists, social workers, andnutritionists. In general, physicians spend1 hour on each ambulatory visit but areoften allotted much less time in theschedule. Physicians and their staff devotehours to each patient between visits.
Since the Institute for HealthcareImprovement’s landmark report on medicalerror in 1999, institutions have focused onimproving systems and processes withinhospitals to improve patient safety andquality of care (43). Particular emphasis hasbeen placed on the critically ill patientswithin hospital intensive care units.Children requiring long-term mechanicalventilation are chronically critically ill (44).Delivering their medical care outside theacute care hospital requires a web ofinteractions among patients and families,multiple layers of physicians and alliedhealth care professionals, and homecare companies. When surveyed, theWorkgroup members reported majorproblems with communication onmedically critical issues such as: ventilatorsettings, home care orders, identification ofwhich physician is responsible for whichorder, and medical records. Although
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents e23

adverse medical and/or safety-related eventswithin health care delivery systems are oftentracked, there is no system to track or reportsuch incidents in ventilator-dependentchildren once they leave the hospital.
Care model for family-centered MedicalHome care of ventilator-dependentchildren. The complexity of the carerequired for a child dependent onchronic mechanical ventilation cannot beoverstated. Regardless of the venue of care,a myriad of providers contribute to thedevelopment and implementation of thecare plan. To achieve optimum functioning,this care plan must be comprehensive andaddress the child’s medical, educational,psychosocial, and, often, behavioral needs.Care of this complexity is potentially highcost and draws on many communityresources. Each specific area typicallyinvolves multiple providers ordisciplines, and there is often overlap inresponsibilities. What is the best, mostpractical and feasible way to providefamily-centered, Medical Home care forthe ventilator-dependent child?
Several models of shared care have beendescribed. The first model, endorsed bythe AAP for routine care, is the MedicalHome with generalist as primary providerand input from specialists only occasionallyas needed. Another model proposescomanagement by the generalist andsubspecialist, both as Medical Homeproviders, each with clearly delineated roles.In a third model, the subspecialist is theprimary Medical Home provider, with thegeneralist playing a limited role as needed(45). In a fourth proposed model, thehospital-based comprehensive care MedicalHome clinic, all primary and specialty careand care coordination is provided in thetertiary care setting by a multidisciplinaryteam (40). As outlined by Antonelli andcolleagues, the choice of model dependson 1) the medical complexity and severityof the medical condition(s), 2) theexpertise of each type of provider, 3)family/patient access to each type ofprovider, and 4) the comfort level offamilies and involved providers indifferent care scenarios (45).
Regardless of the model, the MedicalHome for the ventilator-dependent childmust provide:
d Subspecialty management of the child’schronic respiratory failure and itstreatment, including all aspects of
ventilator management and associatedtherapies
d Support for technical aspects of theventilator and tracheostomy
d Appropriate training of family caregiversd Access to care 24 h/d, 7 d/wkd Community-based primary cared Coordination of all aspects of the child’s
cared Guidance to patient/family on all aspects
of the child’s medical cared Providers responsible for comprehensive
care assessment and management of allaspects of the child’s health care
Given the extreme level of medicalcomplexity of the child on long-termmechanical ventilation, with highlyspecialized care and medical technology,the generalist as primary Medical Homeprovider model is unlikely to be successful.This model would require the generalistprovide and be responsible for acomprehensive care plan and management,with limited input from the subspecialist(45). Similarly, in view of the extensivenonpulmonary care coordination needsoutlined above, the subspecialist as primaryMedical Home provider model may alsoprove difficult to implement. This modelwould require the subspecialist to providecomprehensive care assessment andmanagement of all aspects of the child’scare, including nonpulmonary problems. Itis unlikely that a pediatric pulmonologistwould be comfortable, have the expertise,and have time or resources to oversee theprimary care and other, nonpulmonaryaspects of the child’s care. The hospital-based comprehensive care Medical Homeclinic model has been demonstrated to besuccessful (40), but this model of care existsonly in a few locations; it assumes thatpediatric pulmonologists, respiratorytherapists, and related services are part ofthe multidisciplinary team caring for thepatient; and it assumes that the family haseasy access to the tertiary care medical center.
The model most likely to be successfulfor providing comprehensiveMedical Homecare to the ventilator-dependent child isthe collaborative generalist and subspecialistcomanagement model (39, 46, 47). In thismodel, the generalist and pulmonologistform a team that requires a goodrelationship, with open and effectivecommunication with each other and withhome care and nursing agencies, medicalequipment companies, and all other
services involved. Delineation of who isresponsible for what aspects of care, andcommunication of the specifics to allinvolved, is critically important. Familiesneed to know who to call for each aspectof the child’s care. For example, thepulmonology team would be accessed forhelp with acute respiratory problems andhave a prominent, if not coordinating, rolefor hospital admissions. The generalistand team would be responsible for allaspects of primary care. For aspects of carethat are not respiratory or primary care, thecomanagement team would decide whowould be responsible. For example, thepulmonology team may take responsibilityfor interacting with the dysphagia specialistand overseeing feeding management, due tothe risk for aspiration. The generalist mayassume oversight of the child’s gastrointestinal,neurological, rehabilitation, and other care.Both components of the team should beattuned to integration of the child’s medicalcare plan in nonmedical settings outsidethe home, notably in school. Directcommunication and engagement of schoolstaff on an enhanced level may be needed ifmore complicated elements of the child’s careare to be delivered in that setting (i.e., airwayclearance sessions, monitoring during anyweaning process, behavioral interventions fora medical issue). It is also incumbent on themedical provider to review and adapt aspecific plan able to accommodateadvancement in other areas of the child’sdevelopment (altering medication schedulesor ventilator weaning for rehabilitativetherapies sessions).
Families often need advice and supportas they work to attain other, nonmedicalservices for their children. These will likelyinclude optimum insurance coverage;transportation; and educational, vocational,and recreational services. A family, as a groupor for an individual member, may also needsupport for their own optimal functioning(i.e., recognizing and treating stress ordepression associated with care demands).Ideally, the child’s care team includes one ormore members adept at identifying, or betteryet anticipating, these needs, with theknowledge and skills to help.
Recommendation.
1. For children requiring chronic homeinvasive ventilation, we suggest acomprehensive Medical Home
AMERICAN THORACIC SOCIETY DOCUMENTS
e24 American Journal of Respiratory and Critical Care Medicine Volume 193 Number 8 | April 15 2016

comanaged by a generalist andrespiratory subspecialist (Strength ofRecommendation: Conditional; Qualityof Evidence: Very Low). The features ofthis Medical Home are summarized inTable 4.
Question 2: Should StandardizedDischarge Criteria Be Used WhenPlanning the Hospital Discharge ofChildren Requiring Chronic HomeInvasive Ventilation?
Background. Care in the home for childrenrequiring chronic invasive ventilation ispossible and preferred to care in aninstitution. Yet discharging a patientdependent on invasive ventilation can takemany months or even years to arrange(48, 49). The decision to pursue chronicmechanical ventilation in the home settingwill be influenced by the comfort level ofthe family and medical team caring for thechild and the availability of resources in thechild’s home and community. It should benoted that many of the risks of chronicventilation in children are present regardlessof whether the child is cared for at home, in along-term facility, or in the hospital setting(50, 51). The heterogeneity of insurancecoverage and community availability ofprofessional home care providers fornecessary services and equipment makescomprehensive guidance difficult. The bestjudgment of the provider, after candiddiscussion with caregivers and review ofavailable resources outside of the hospital, isessential for designing a customizeddischarge plan for each child.
The Workgroup found no publishedexperimental or observational studiesexamining the use of standardized dischargecriteria for children on chronic homemechanical ventilation. The effect of applyingstandardized discharge criteria on importantoutcomes in these children, such as death,rehospitalization, and quality of life, is notknown. Guidelines designed to facilitate thesafe discharge and home care of mechanicallyventilated children were provided by theATS in 1990, and subsequently pediatricguidelines have been published in the UnitedKingdom and Australia (52–54). ThePediatric Chronic Home VentilationWorkgroup compared existing dischargecriteria from the chronic ventilationprograms of seven children’s hospitalswithin the United States and a compositedocument was generated. The Workgroup
reviewed the composite document andcompared it to other consensus statementsaddressing pediatric home invasiveventilation in an effort to developgeneralizable criteria for an ideal discharge(53, 54). When appropriate, aspects of carefrom adult guidelines for home mechanicalventilation were incorporated into therecommendations (55–57). On the basis ofthe extensive clinical experience of theWorkgroup, we suggest the use ofstandardized discharge criteria to objectivelyassess readiness of an invasively ventilatedpediatric patient for care in the home. Thepossible benefit of standardized dischargecriteria would be to identify and eliminateimportant barriers to care in the homebefore discharge and consider alternate carearrangements if obstacles cannot beeliminated. Weight given to each componentof the proposed criteria would vary betweencenters and patients. The recommendationplaces high value on the potential benefits ofconsidering all facets of a child’s care in thehome before discharge and low value tothe increased provider time and resource usethat may be required.
Table 5 lists proposed standard criteriafor discharge home from the hospital ofchildren with invasive mechanicalventilation. All required services must becovered by insurance or other definedmeans, and a home care supplier must beidentified to provide the necessary durablemedical equipment (DME). In Table 5,section 1 describes the readiness of thechild. Assessing the child’s medical stabilityincludes evaluating respiratory stability;ideally, ventilator settings have not requiredadjustment for weeks before discharge (54).Thresholds for delivered oxygenconcentration or prescribed ventilatorsettings are often set by local home carecompany limitations and should be definedbefore discharge. Evaluation of homeoxygen delivery systems should beperformed to ensure the FIO2
delivered byhome equipment is sufficient to meet thechild’s needs. Section 2 addresses the familycaregivers. Families must have the ability toprovide for the child’s basic needs (safety,food, clothing, stimulation) while alsomanaging the complex medical needs oftheir child. Caregivers should demonstratecompetence with the provision of alltherapies required by the patient beforedischarge. The Workgroup agreed that aminimum of two family caregivers shouldbe trained in the care of the complex child
at home. One caregiver (including availableprofessionals) should be awake and alert torespond to emergencies at all times. Therequirement for number of caregivers in thehome and the training of these caregivers isdiscussed in the following section of thisdocument. Section 3 describes the basicrequirements for a DME company, whichwill be needed to partner with the familiesand their health care team. In-homeprofessionals are required for assistance tothe family caregivers and, as described insection 4 and later in this document,must be appropriately trained. Theseprofessionals might include nurses,respiratory therapists, or other homepersonnel specifically trained in the careand management of the ventilated child.Section 5 addresses the important aspectsof the home environment. The homeenvironment must meet basic safetyrequirements and provide provisions foremergencies.
Advance care planning, including thedevelopment of written care directives,should be addressed before the child’s initialhospital discharge. Anticipatory guidancethat includes information about thepatient’s diagnosis and prognosis, potentialemergency situations that may be faced,and the expectations for and limitations ofavailable therapies should be provided.Decisions regarding resuscitation and life-sustaining treatments should be discussedwith the family and, when appropriate, thepatient. Patients and families should alsounderstand that directives and goals of carecan be modified at any time.
Recommendation.
2. For children requiring chronicinvasive ventilation, we suggest theuse of standardized discharge criteriato objectively assess readiness forcare in the home (Strength ofRecommendation: Conditional; Qualityof Evidence: Very Low). Suggestedcomponents of these criteria are listed inTable 5.
Question 3: Should Home CaregiversBe Specifically Trained in the Care ofChildren Requiring Chronic HomeInvasive Ventilation?
Background. Children on home invasiveventilation are typically cared for by a
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents e25
combination of family and professionalcaregivers. In the ideal situation, the child’scaregivers understand the patient’s diseaseand the role invasive ventilation plays in itsmanagement, the mechanics of providinginvasive ventilation including the features
and limitations of the specific ventilatorused, and tracheostomy care with a focuson preventing tracheostomy-specificcomplications. Caregivers must providecomprehensive care in all eventualities,particularly in emergencies. Accidental
deaths remain a significant cause ofmorbidity in this population, and hospitalreadmissions are common. During the pastthree decades, the overall mortality rate of atotal of 1,008 children enrolled in thePennsylvania Ventilator Assisted Children’s
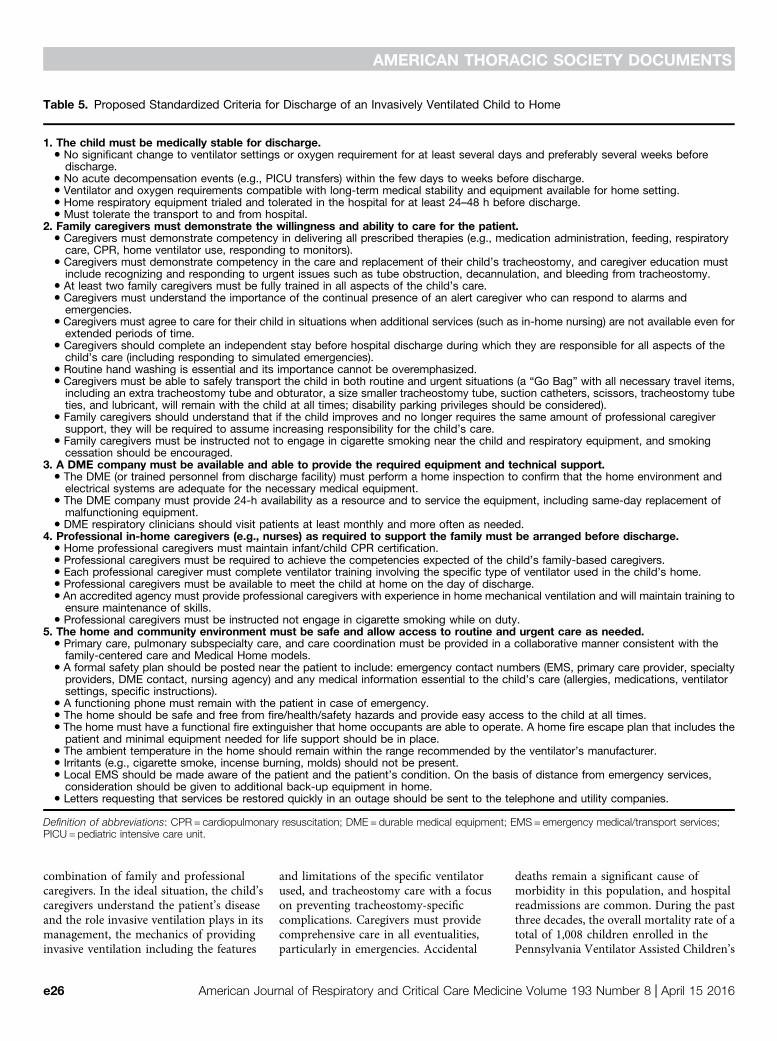
Table 5. Proposed Standardized Criteria for Discharge of an Invasively Ventilated Child to Home
1. The child must be medically stable for discharge.d No significant change to ventilator settings or oxygen requirement for at least several days and preferably several weeks beforedischarge.
d No acute decompensation events (e.g., PICU transfers) within the few days to weeks before discharge.d Ventilator and oxygen requirements compatible with long-term medical stability and equipment available for home setting.d Home respiratory equipment trialed and tolerated in the hospital for at least 24–48 h before discharge.d Must tolerate the transport to and from hospital.
2. Family caregivers must demonstrate the willingness and ability to care for the patient.d Caregivers must demonstrate competency in delivering all prescribed therapies (e.g., medication administration, feeding, respiratorycare, CPR, home ventilator use, responding to monitors).
d Caregivers must demonstrate competency in the care and replacement of their child’s tracheostomy, and caregiver education mustinclude recognizing and responding to urgent issues such as tube obstruction, decannulation, and bleeding from tracheostomy.
d At least two family caregivers must be fully trained in all aspects of the child’s care.d Caregivers must understand the importance of the continual presence of an alert caregiver who can respond to alarms andemergencies.
d Caregivers must agree to care for their child in situations when additional services (such as in-home nursing) are not available even forextended periods of time.
d Caregivers should complete an independent stay before hospital discharge during which they are responsible for all aspects of thechild’s care (including responding to simulated emergencies).
d Routine hand washing is essential and its importance cannot be overemphasized.d Caregivers must be able to safely transport the child in both routine and urgent situations (a “Go Bag” with all necessary travel items,including an extra tracheostomy tube and obturator, a size smaller tracheostomy tube, suction catheters, scissors, tracheostomy tubeties, and lubricant, will remain with the child at all times; disability parking privileges should be considered).
d Family caregivers should understand that if the child improves and no longer requires the same amount of professional caregiversupport, they will be required to assume increasing responsibility for the child’s care.
d Family caregivers must be instructed not to engage in cigarette smoking near the child and respiratory equipment, and smokingcessation should be encouraged.
3. A DME company must be available and able to provide the required equipment and technical support.d The DME (or trained personnel from discharge facility) must perform a home inspection to confirm that the home environment andelectrical systems are adequate for the necessary medical equipment.
d The DME company must provide 24-h availability as a resource and to service the equipment, including same-day replacement ofmalfunctioning equipment.
d DME respiratory clinicians should visit patients at least monthly and more often as needed.4. Professional in-home caregivers (e.g., nurses) as required to support the family must be arranged before discharge.
d Home professional caregivers must maintain infant/child CPR certification.d Professional caregivers must be required to achieve the competencies expected of the child’s family-based caregivers.d Each professional caregiver must complete ventilator training involving the specific type of ventilator used in the child’s home.d Professional caregivers must be available to meet the child at home on the day of discharge.d An accredited agency must provide professional caregivers with experience in home mechanical ventilation and will maintain training toensure maintenance of skills.
d Professional caregivers must be instructed not engage in cigarette smoking while on duty.5. The home and community environment must be safe and allow access to routine and urgent care as needed.
d Primary care, pulmonary subspecialty care, and care coordination must be provided in a collaborative manner consistent with thefamily-centered care and Medical Home models.
d A formal safety plan should be posted near the patient to include: emergency contact numbers (EMS, primary care provider, specialtyproviders, DME contact, nursing agency) and any medical information essential to the child’s care (allergies, medications, ventilatorsettings, specific instructions).
d A functioning phone must remain with the patient in case of emergency.d The home should be safe and free from fire/health/safety hazards and provide easy access to the child at all times.d The home must have a functional fire extinguisher that home occupants are able to operate. A home fire escape plan that includes thepatient and minimal equipment needed for life support should be in place.
d The ambient temperature in the home should remain within the range recommended by the ventilator’s manufacturer.d Irritants (e.g., cigarette smoke, incense burning, molds) should not be present.d Local EMS should be made aware of the patient and the patient’s condition. On the basis of distance from emergency services,consideration should be given to additional back-up equipment in home.
d Letters requesting that services be restored quickly in an outage should be sent to the telephone and utility companies.
Definition of abbreviations: CPR = cardiopulmonary resuscitation; DME = durable medical equipment; EMS = emergency medical/transport services;PICU = pediatric intensive care unit.
AMERICAN THORACIC SOCIETY DOCUMENTS
e26 American Journal of Respiratory and Critical Care Medicine Volume 193 Number 8 | April 15 2016

Home Program (VACHP) was 27.5%.Despite technological advances in homemonitoring, 18 to 20% of the overallmortality rate was attributed to preventabledeaths related to tracheostomy accidentsthat included undetected decannulationand mucous plugging of the tracheostomytube (58). In a retrospective observationalcohort analysis of 228 children enrolled in ahome mechanical ventilation program insouthern California over a 22-year period(990 person-years), there was a 21%mortality rate. Progression of underlyingconditions accounted for only 34% of thedeaths, whereas 49% of the deaths wereunexpected. Of the unexpected deaths,19% were related to airway issues, includingacute airway obstruction, trachealhemorrhage, and accidental decannulation(51). A study from the same program inCalifornia found that 40% of newlydischarged pediatric patients requiringhome mechanical ventilation requirednonelective readmission to the hospitalin their first year home; half of theseadmissions occurred in the first 3 months(59). Pneumonia and tracheitis were themost common causes of readmission, andthe authors postulate that this may be,in part, related to inadequate caregivertraining on airway clearance and care.A study from Germany examining severeemergencies in a group of ventilator-dependent children found an incidenceof 0.27 emergencies per patient-yearand also found that the majority wererelated to respiratory problems, suchas infection, atelectasis, and increasedsecretions and tracheostomycomplications (60).
Authors reviewing outcomes in thispopulation have suggested that improvedcaregiver training may help reducemorbidity and mortality on the basis of theirclinical experience (58, 59). Consensusstatements by the ATS and the AmericanAcademy of Otolaryngology–Head andNeck Surgery that describe the care ofchildren with tracheostomies emphasize theimportance of home caregiver education,which includes both family members andhome nurses (61, 62). The Workgroupfound no experimental or observationalstudies directly addressing the question ofthe effect of training caregivers or thepresence of a trained caregiver onimportant outcomes, such as death orrecurrent hospitalization, for childrenrequiring chronic home invasive
ventilation. Despite the very low qualityevidence available, the Workgroup, onthe basis of consensus opinion andunsystematic observations, stronglyrecommends that an awake and alerttrained caregiver be always present andimmediately available in the home ofa child requiring chronic invasiveventilation.
In making this strongrecommendation, the Workgroup believesthat the desirable consequences wouldclearly outweigh the undesirableconsequences, which include increased useof resources and a possible disruption tofamilies, of following this recommendation.Lack of an awake and attentive trainedcaregiver would place the child in a life-threatening situation. Training isirrelevant if a caregiver cannot respond to anurgent situation secondary to sleepiness orfatigue. To provide an awake and alerttrained caregiver at all times generallyrequires the involvement of bothprofessional and nonprofessional (family)caregivers.
Previous guidelines released by the ATSon the care of a child with a tracheostomy inthe home recommended that two adultcaregivers be trained in the care andreplacement of a tracheostomy tube (61).A small retrospective study surveyedcaregivers of infants discharged from thehospital with a tracheostomy. Mostcaregivers (70%) reported that the secondcaregiver participated in the child’s medicalcare often or very often (63). Fifty percentof the respondents believed they could nothave cared for the infant in the homewithout another trained caregiver. On thebasis of the experience of the Workgroupand these limited survey data, we suggestthat at least two family caregivers aretrained to provide care for the child in thehome. This recommendation places ahigh value on the safety of the patient andthe quality of life of the caregivers andlow value in the increased resource userequired for training more than onecaregiver.
Limited literature describing training ofboth family and professional caregivers wasavailable and is reviewed below. Dataexamining to what extent level of trainingaffects the outcomes of these patients are notavailable.
Family caregivers. Single-centerobservational studies have outlinedrecommended training for caregivers
(64–68). Recommendations include acomprehensive and staged educationalapproach that begins even before placementof the tracheostomy and spans until thetime of the child’s discharge from thehospital. These approaches have appliedvarious aids that involve individualizedinstruction, audiovisual and writtenmaterials, supervised practice using homeequipment, and use of dolls or mannequinsfor skill demonstration. Programs haveincluded written objectives and validationof acquired skills and knowledge.Structured educational programs have beenshown to reduce the length of the initialhospital stay after tracheostomyplacement in children (69, 70). Trainingis designed to ensure parental familiarityand understanding of the role and useof devices and equipment; comfortwith routine tracheostomy and ventilatorcare, day-to-day respiratorymanagement, and troubleshooting; aswell as emergency care. A study by Kunand colleagues demonstrated, throughthe use of a 25-question survey, thatfamily caregivers once trained have agood understanding of how to respond toventilator or tracheostomy emergencies,with no difference in scores notedbetween lay caregivers and licensednurses (71). Some deficits in knowledgewere found, however, with theauthors recommending more in-deptheducation on the limitations of ventilatoralarms.
Professional caregivers. Care of achronically ventilated child in the home canrarely be accomplished without the use ofprofessional caregivers. As noted previously,safe care of a child with a tracheostomy andhome mechanical ventilator relies not onlyon caregiver training but also on thepresence of an awake and alert trainedcaregiver. Professional caregivers arecommonly used to meet this standard andprovide the needed respite for families tosleep, work, and attempt to maintain lifebalance. In a survey of families caringfor ventilator-dependent children, 25%reported providing direct patient care totheir child for more than 16 h/d, and 40%reported an unmet need for skilled nursingin the home (72). A significant portion offamily caregiver respondents reportedfrequent depressive symptoms, and, in thiscohort, screening positive for a likelydepressive disorder was associated withreporting unmet needs for care. In
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents e27

another small study of caregivers ofventilator-dependent children, symptomsof clinical depression and sleep deprivationwere significantly associated with a lack ofnighttime nursing (73). Guidelinesaddressing the use of professional homenursing care for children with atracheostomy or tracheostomy withventilator have stressed the use of homenursing care during the transition fromhospital to home and supported that manychildren will have an ongoing need for homeprofessional care (53, 61). The number ofhours of professional care required will bebased on multiple factors (for example,complexity of the child’s care, the child’sdependence on the ventilator, the family’sability to provide safe care, and the otherdemands on the family’s time, includingother children) and must be evaluated andreevaluated as situations change on a case-by-case basis.
In Pennsylvania, a care assessmentsurvey was administered to 107 randomlyselected families enrolled in VACHP. Thesefamilies reported that home care wasfrequently disrupted by 1) the lack ofavailable nurses, and 2) an inadequate levelof skill demonstrated by the homecarenurses (74). In response to the surveyresults, the organization assessed the skilllevels of 21 experienced home care nurses(16 registered nurses and 5 licensedpractical nurses) who were providing careto the VACHP children. The assessmentsrevealed a knowledge deficit in manyareas of care. The deficient areas were:respiratory assessment (71%), tracheostomycare (43%), tracheostomy string change(90%), suctioning of the tracheostomy(95%), tracheostomy tube change (90%),tracheostomy emergencies (86%),cardiopulmonary resuscitation with atracheostomy (47%), ventilator care andmanagement (86%), and troubleshootingventilator alarms (100%). Individualtraining included pretraining evaluation,individual skill level validation, simulation,return demonstration, and post-trainingevaluation to all the nurses over a 7- to13-hour period. At the conclusion, eachnurse was able to demonstrate mastery of theskills with the patient. Parents reportedan overall increase in satisfaction with thecare provided by their nurses post-training (74).
From 2003 to 2012, VACHP providedtraining to 600 home care nurses fromacross the United States caring for
ventilator-assisted children. Of the nurseswho identified themselves as experienced intracheostomy and ventilator home care, theaverage pretest score was only 60%, withsome nurses scoring as low as 20%. Post-training evaluation was conducted with eachof the nurses to assure skill acquisition toprovide proficient care in the home (58).Kun and colleagues used home mechanicalventilator emergency scenarios provided byan online survey to evaluate the knowledgeof practicing pediatric home health nurses(75). Regardless of years of experience, thenurses scored poorly, and those surveyedoverwhelmingly favored more training inhome mechanical ventilation. The authorsrecommend enhancing nurse educationthrough the use of simulation, “teach back”methods, and return demonstrations andsimulations in the home where the nurse isproviding care. It is unknown, however,whether periodic assessment andreeducation of professional caregiversreduces the frequency of adverse events inthe home.
On the basis of the literature reviewedand the unsystematic observations of theWorkgroup, we suggest that ongoingeducation to allow acquisition of and thenreinforce and augment the skills requiredfor patient care be provided to both familyand professional caregivers of childrenrequiring chronic home invasive ventilation.Ongoing education after the initial trainingperiod would help reinforce learned skillsand allow training on new protocols andtechnology. Education should be providedby the involved medical professionals in theclinic or hospital, professional personnelagencies, and DME companies. Thisrecommendation places a high value onsafety and the potential clinical benefits tothe patient and a low value on potentialincreased cost and resource use.
Paraprofessional caregivers.Nonprofessional caregivers are rarelyemployed in the home care of chronicallyventilated children in the United States,and research literature is limited. AnAustralian study of 168 ventilator-dependent children at home evaluatedcare provided by alternative caregivers inplace of skilled nurses (76). The studyreported that the trained lay caregiversprovided adequate care and did notcorrelate negative patient outcomes withcare provided by nonprofessionals.However, the study did not describe thetraining curriculum or methodology. Most
of the children in the study requirednoninvasive ventilation; therefore, furtherinvestigation of the use of paraprofessionalcaregivers for children who requireconventional mechanical ventilator supportis warranted.
Recommendation.
3a. We recommend that an awake andattentive trained caregiver be in thehome of a child requiring chronicinvasive ventilation at all times(Strength of Recommendation: Strong;Quality of Evidence: Very Low).
3b. For children requiring chronic invasiveventilation, we suggest that at least twospecifically trained family caregiversare prepared to care for the child in thehome (Strength of Recommendation:Conditional; Quality of Evidence:Very Low).
3c. We suggest that ongoing education toacquire, reinforce, and augment skillsrequired for patient care be providedto both the family and professionalcaregivers of children requiringchronic home invasive ventilation(Strength of Recommendation:Conditional; Quality of Evidence: VeryLow). Suggested educational objectivesare provided in Table 6.
Question 4: Should Standard HomeEquipment Requirements Be AppliedWhen Planning for the EquipmentNeeds of Children Requiring InvasiveVentilator Support in the Home?
Background. The Workgroup found noexperimental or observational studiesdirectly addressing the question of whetherthe availability of certain equipment in thehome of a child dependent on invasiveventilation would lead to improvedoutcomes and therefore be considered arequired component of care. We foundseveral studies examining the performanceof equipment in the home and oneevaluating the performance of ventilatoralarms in a setting designed to simulateaccidental decannulation, and these aredescribed in the following paragraphs. Noneof the literature reviewed addressed theeffect of providing specific home equipmentor of maintaining home equipment onoutcomes such as death, morbidity, or qualityof life. The indirect evidence described below,
AMERICAN THORACIC SOCIETY DOCUMENTS
e28 American Journal of Respiratory and Critical Care Medicine Volume 193 Number 8 | April 15 2016

Table 6. Suggested Educational Objectives for Family and Professional Caregivers of Children Requiring Home MechanicalVentilation
Pulmonary care and assessmentCaregivers should be able to:d Obtain basic vital signs, including pulse rate, breath rate, and oxygen saturationd Recognize and state the child’s usual breath rate, pulse rate, oxygen saturation, respiratory effort, and colord Identify type of ventilator used in home and ventilator settingsd Identify type of tracheostomy tube and whether it is cuffed or uncuffed and, if cuffed, instructions for inflation of the cuff (manufacturerrecommendation for cuff inflation [air vs. water], amount of air/water used to inflate cuff, hours per day spent with cuff inflated)
d Identify type of “back-up” tracheostomy tube to be used if primary tube cannot be replacedd Know that an additional tracheostomy tube, the back-up tracheostomy tube, and the supplies needed to change the tracheostomyshould be with the child at all times (the “Go Bag”)
d Identify signs of respiratory distress and describe proper intervention. (Signs of respiratory distress to review may include: increasedtracheal secretions or change in color of secretions, retractions, increased work of breathing, cough, color changes, nasal flaring,increased or decreased heart rate, increased or decreased respiratory rate, desaturation, anxiety, abnormal breath sounds.)
Tracheostomy careGuidelines for tracheostomy education are provided in Reference 61
Emergency responseCaregivers should be able to:d Verbalize criteria for calling emergency services (such as 911 in the United States)d Be certified in CPRd Be able to access a list of numbers for emergencies or problems not requiring emergency services (physicians, DME, etc.) and knowwho to contact on the basis of the type of emergency
d Demonstrate use of self-inflating bag and mask in routine and emergency care proceduresd List signs of tracheostomy obstructiond Demonstrate appropriate suctioning techniques to remove tracheostomy obstructiond Demonstrate an emergency tracheostomy tube change (change done by one caregiver without assistance)d Demonstrate knowledge of emergency medications (if applicable)d Verbalize plans for loss of electricity, fire, tornado, or other natural disaster
Ventilator trainingCaregivers should be able to:d Identify electrical power sourcesd Assemble ventilator circuit and humidification systemd Describe routine cleaning of equipmentd Add oxygen to circuit if indicatedd Verbalize that ventilator alarms must be audible throughout the homed Demonstrate how to properly turn the ventilator on, test the ventilator before use, and view and verify settingsd Demonstrate an understanding of ventilator alarms and how to troubleshoot the alarmsd Demonstrate the appropriate technique for draining tubing in the ventilator circuit, down and away from childd Demonstrate the ability to keep battery-operated back-up equipment charged and ready for used Demonstrate how to charge batteries for ventilatorsd Demonstrate how to connect and use the external battery for the ventilator if applicabled Verbalize understanding of the approximate battery life for each piece of equipment
Infection control practicesCaregivers should be able to:d Demonstrate infection control practices as they relate to the plan of cared Demonstrate proper hand-washing techniqued Demonstrate proper disposal of contaminated materiald Demonstrate how to clean and disinfect reusable medical supplies
MedicationsCaregivers should be able to:d Identify the dosage and frequency of all medications required by the childd Explain the indications and side effects of medicationsd Demonstrate the ability to prepare and administer medications correctly
OxygenCaregivers should be able to:d Demonstrate the proper care and use of home oxygen delivery equipment (e.g., cylinders, concentrators)d Verbalize the safety issues related to use of oxygen in the home (risk of fire with smoking, open flames, flammable products near theoxygen, or close proximity to heat sources)Demonstrate understanding of when and how oxygen should be used for the patient
Oximetry monitoringCaregivers should be able to:d Demonstrate the proper and secure placement of the oximeter probed Demonstrate the ability to differentiate true from false oximeter readingsd Verbalize steps for responding to an oximeter alarmd Verbalize an understanding of normal oxygen saturations and a plan for responding to saturations that fall below the normal range
(Continued )
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents e29

coupled with the unsystematic observationsof the Workgroup experts, was used toformulate the recommendations.
Children requiring invasive homeventilation have diverse underlyingetiologies for their chronic respiratoryfailure and often have significant associatedcomorbidities. They are at high risk of deathand require significant medical andtechnological support in the communitysetting. Although most of the deaths seen inpatients requiring chronic home invasiveventilation are related to the progression oftheir underlying disease or their associatedcomorbidities, a significant number of thesedeaths are caused by tracheostomy-relatedaccidents or complications, many of whichmay be preventable (51).
Although many of these tracheostomy-related deaths may be due to problemsregarding caregiver training and their abilityto appropriately respond to emergencysituations, there may be equipment-basedstrategies available to avoid or reducetracheostomy-related mortality. One meansmay be through using appropriatemonitoring strategies in the home. Althoughpositive-pressure ventilators are equippedwith various alarms, these may not provideadequate protection. A study by Kun andcolleagues found that low inspiratorypressure alarms failed to alarm duringsimulated decannulation when tested withthe smaller-diameter tracheostomy tubesoften used in pediatric patients (77). Thissuggests the need for alternate monitoringstrategies. In a separate study examiningthe performance of ventilators in the homeenvironment, poor functioning of ventilatoralarms was also noted, with 18.6% of thebuilt-in alarms for disconnection and 5.1%
of the alarms for obstruction in the homeventilators found to be nonfunctional wheninvestigated by the examiners (78). Limitedavailable data suggest that pulse oximetry isthe preferred monitoring method, althoughthis is not provided for every patient, asreported in a 2007 study of home ventilatedpatients in Massachusetts (22). Standardhome cardiorespiratory monitors thatmonitor heart rate and chest wallmovement will only alert caregivers if thereis absence of respiratory effort and/orassociated bradycardia. In infants andchildren, hypoxemia is likely to be an earlyindicator of airway obstruction orequipment malfunction leading toinadequate ventilation, whereas bradycardiaand central apnea are later complicationsof a serious event, which make patientresuscitation more difficult. For childrenrequiring chronic home ventilation, wesuggest monitoring, especially when thechild is asleep or unobserved, with a pulseoximeter. In making this recommendation,we place high value on the potentialbenefits of monitoring with a pulseoximeter and low value on the potentialrisks, which may include false alarms(which can lead to caregiverdesensitization) as well as difficultymaintaining the pulse oximeter probein place.
Unlike tracheostomy-related issues,deaths secondary to ventilator failure arerare. Equipment malfunction and/or failure,however, can lead to significant overuse ofresources by patients. Equipment failuremay be related to age of the equipment,longer intervals between equipmentservicing, longer ventilator use by thepatient, failure of caregivers to care for
equipment appropriately, and failure of thecaregivers to recognize poor equipmentperformance (e.g., leaks in the circuit) (79).Interestingly, equipment failure was alsoassociated with “very new” ventilators,suggesting issues are uncovered after releaseof newer models (79). Strategies foraddressing potential equipment failureinclude regular maintenance and servicingof home equipment as well as regularreeducation of the patients and caregivers.A study by Farre and colleagues examiningquality-control procedures in Europe foundthat medical centers prescribing homemechanical ventilation were generally notinvolved in the care and maintenance of theventilator and that ventilator companieswere servicing equipment with a frequencythat ranged from 3 to 12 months (80). Mostprescribing centers were unaware of thequality-control procedures followed by theventilator companies, with communicationbetween the two entities limited. Theprovision of appropriate back-up supplieswas found to decrease the risk of ventilatormalfunction and associated mortality.A 2011 German study of 54 children andadolescents receiving ventilation in thehome setting reported only three acuteemergencies associated with ventilatorfailure without resulting mortality,subsequent hospitalization, or persistentadverse event (60). Authors of this studypostulated that the low incidence ofadverse events associated with equipmentmalfunction in their patient populationmay have been related to the provision ofback-up ventilators, self-inflating bag andmasks, and emergency oxygen for all of theventilator-dependent patients. Providers inthe United States should be aware of the
Table 6. (Continued )
Suctioning equipmentCaregivers should be able to:d Demonstrate the correct catheter size to use for the patientd Demonstrate the correct suction pressure and catheter depth to use to clear tracheostomyd Demonstrate how to test for suction pressured Demonstrate a clean suction technique
Nebulizer/metered dose inhaler (if ordered)Caregivers should be able to:d Verbalize when the prescribed inhaled medications are requiredd Demonstrate how to deliver inhaled medications in ventilator circuit if applicable
Definition of abbreviations: CPR = cardiopulmonary resuscitation; DME = durable medical equipment.Further instruction and competency assessment will be required if patient requires equipment/therapy beyond those listed above (e.g., pulmonaryclearance therapies, cardiorespiratory monitors, end-tidal CO2 monitors, etc.). The goal should be to ensure that all caregivers are fully versed in allaspects of the child’s care.
AMERICAN THORACIC SOCIETY DOCUMENTS
e30 American Journal of Respiratory and Critical Care Medicine Volume 193 Number 8 | April 15 2016

requirement to report medical devicefailures or defects to the Federal DrugAdministration (81).
Even in the absence of ventilatormalfunction or failure, patients may be atrisk for underventilation or overventilationin the home setting. Studies in adult patientshave suggested that performance ofventilators in the home may varyconsiderably and that there is often adifference between the set and theprescribed ventilator settings on theseventilators. This places patients at riskfor hypoventilation and associatedcomplications (78). In addition, intransitioning a patient from an internalpositive end-expiratory pressure ventilatorto an external positive end-expiratorypressure ventilator (or vice versa), theclinician must recognize that the requiredsettings on the ventilator may be differentso as to achieve the same ventilatorysupport. Home ventilators have beenshown to vary in their ability to reliablydeliver a specified tidal volume andcompensate for air leaks (82, 83).Pediatric patients should demonstratestability on their chosen home devicebefore discharge and may requirereadmission or increased monitoring inthe home if transition from one homeventilator type to another is required.
For children requiring invasive homeventilation, we recommend regularmaintenance of ventilators and associatedequipment in the home as outlined by themanufacturer. Care should be taken toassure that the actual ventilator settingsas seen on the control panel match theprescribed settings. Twenty-four hour a dayservice and phone support for mechanicalfailure or malfunctions must be availableand is generally provided by the DMEcompany. This recommendation supportsthe safe and appropriate use of allequipment chosen by the provider for usein the home.
A 1998 consensus statement from theUnited Kingdom recommended thatequipment chosen for the home for childrenrequiring long-term ventilation be“portable, durable and simple to use” (53).A second ventilator was believed to berequired for any child who cannot be offthe ventilator for 6 continuous hours. It wasalso recommended that alternative powersources be supplied (battery or generator).Last, it was recommended that clear plansshould be in place for the maintenance and
replacement of equipment in the case ofmechanical failure. Given the limited dataavailable to the clinician when choosingappropriate equipment for the home andthe absence of any randomized controlledtrials, our expert panel was surveyed toformulate equipment recommendations.Each pediatric tertiary center withrepresentatives in the working group wasasked to provide their written protocol forstandard equipment prescribed at initialdischarge for home ventilated infants orchildren. These lists were then mergedinto a single list containing only DME;disposable items were not included. Thefinal list included 21 items. Allparticipants were then e-mailed a surveyasking them to 1) rank-order the 21 itemsfrom most important to least important;and 2) rate whether each item wasabsolutely required, required, stronglyrecommended but not required, oroptional. A total of 15 experts in chronichome ventilation from 15 different centersresponded to the survey. Participants wereencouraged to discuss the survey withtheir colleagues and/or hospital dischargeplanner. Survey results are summarized inTable 7. Equipment believed to beabsolutely required by 70% or more of theexperts surveyed included: the ventilator,a back-up ventilator, batteries for theventilator, self-inflating bag and mask,suctioning equipment (portable), heatedhumidifier, supplemental oxygen foremergency use, nebulizer, and a pulseoximeter (nonrecording). The remainderof the survey results can be found inTable 7. We suggest that the “absolutelyrequired” equipment identified in oursurvey of expert clinicians be available inthe home. On the basis of experience, theWorkgroup believed the presence ofspecific pieces of equipment could preventthe development of life-threateningsituations and/or reduce their severity.This recommendation places high value onthe potential to avoid emergent situations dueto the presence of important reserve andemergency equipment and low value toincreased resource use and increasedequipment costs.
Another possible strategy to avoidcomplications for patients dependent oninvasive ventilation is to decrease the riskof tracheostomy plugging through theoptimization of airway clearance. Therecent Canadian Thoracic Societystatement on home ventilation, which
focused on the adult population, stronglyrecommended manually assisted coughtechniques or the use of the cough assist inpatients with tracheostomy, regardless ofthe underlying etiology of the chronicrespiratory failure (57). Methods foraugmenting cough, including MI-E devices,are strongly recommended for use in patientswith neuromuscular disease with anineffective cough so as to help maintainairway patency and avoid respiratorycomplications, such as atelectasis andinfection (84–86). We suggest that an MI-Edevice be used to help maintain airwaypatency in patients requiring homemechanical ventilation with ineffectivecough, including, but not limited to, thosewith neuromuscular disease with poorrespiratory muscle strength. Thisrecommendation places high value on thepotential to avoid airway plugging and lowvalue on increased costs and resource use.
Recommendation.
4a. For children requiring chronic homeinvasive ventilation, we suggestmonitoring, especially when the childis asleep or unobserved, with a pulseoximeter rather than use of acardiorespiratory monitor or sole useof the ventilator alarms (Strengthof Recommendation: Conditional;Quality of Evidence: Very Low).
4b. For children requiring chronic homeinvasive ventilation, we recommendregular maintenance of homeventilators and all associatedequipment as outlined by themanufacturer.
4c. We suggest the following pieces ofequipment for use in the home whencaring for a patient on homemechanical ventilation: the ventilator,a back-up ventilator, batteries, a self-inflating bag and mask, suctioningequipment (portable), heatedhumidifier, supplemental oxygen foremergency use, nebulizer, and a pulseoximeter (nonrecording) (Strengthof Recommendation: Conditional;Quality of Evidence: Very Low).
4d. We suggest that an MI-E device beused to help maintain airway patencyin patients requiring homemechanical ventilation withineffective cough, including, but notlimited to, those with neuromuscular
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents e31

disease with poor respiratory musclestrength (Strength ofRecommendation: Conditional;Quality of Evidence: Very Low).
Research Priorities
These guidelines are based largely on theextensive clinical experience of theWorkgroup members. Published data arelimited and experimental, and evenobservational clinical studies are absent. Thefollowing future directions were identifiedby the Workgroup in hopes that studyof this population will lead to improvedcare. We anticipate that updates to theseguidelines will be required as our knowledgeincreases and home equipment changes. Werecognize that what works in one center maynot work well in another. Regular reviewand revision of these guidelines withindividual patients and their communitypartners (primary care providers, homenursing agencies, DME companies,emergency medical services) is needed toensure the guidelines remain relevant in thelocal setting.
1. A national registry of patients onhome invasive ventilation should beestablished to monitor the epidemiologyof children requiring chronic invasiveventilation in the home, track outcomes,and facilitate multicenter research.A learning network associated withthe registry could be developed andregularly bring together stakeholders toshare knowledge and develop andimplement research projects and clinicalprograms.
2. A national safety reporting system ofsevere events in the home that wouldenable tracking of poor outcomes ordangerous situations due to problems inthe health care delivery system shouldbe developed. Analysis of these eventswill help to alert caregivers to practicesor equipment that place patients atrisk and support important quality-assurance efforts, which can be used totailor the guidelines. We also proposestandardization of nomenclature forventilator modes and settings to avoiderrors leading to inappropriate settingsor ventilator support. Proprietarynaming of ventilator modes by
manufacturers results in different termsbeing used for the same or similarventilator modes and leads to confusionamong medical staff.
3. Evaluation of the efficacy of formalizedfamily caregiver training programs andprofessional caregiver training programsis needed. The role of simulationprograms and other media should beinvestigated. To possibly expand theavailable home care workforce andprovide needed support to families,research examining the role andrequired training of paraprofessionalcaregivers for children requiring chronichome invasive ventilation should beperformed.
4. Studies examining the role oftelemedicine and remote monitoringin the care of chronically ventilatedchildren should be undertaken,specifically investigating the usefulnessregarding patient outcomes andequipment troubleshooting.
5. Further research is needed on themost effective models of primarycare–specialist partnerships. Researchregarding the delivery of health care to
Table 7. Survey of Expert Opinion on the Necessary Equipment for Care of Children Requiring Invasive Home Ventilation
Equipment“Absolutely Required” or“Required” (% of Experts)
“Strongly Recommended”(% of Experts)
“Optional”(% of Experts)
No. ofRespondents*
Battery (long) 100.0 0 0 15Heated humidifier 100.0 0 0 15Suction (portable) 100.0 0 0 15Ventilator (primary) 100.0 0 0 14Oxygen 93.3 6.7 0 15Pulse oximeter (nonrecording) 93.3 6.7 0 15Self-inflating bag and mask 93.3 6.7 0 15Battery (short) 78.6 7.1 14.3 14Nebulizer 73.3 20.0 6.7 15Ventilator (back-up) 71.4 28.6 0 14Suction (stationary) 64.3 28.6 7.1 14Stethoscope 53.3 33.3 13.3 15Mechanical insufflation–exsufflationdevice
33.3 26.7 40.0 15
Car adapter 26.7 73.3 0 15Cardiorespiratory monitor (recording) 21.4 28.6 50.0 14Pulse oximeter (recording) 21.4 42.9 35.7 14Test lung 21.4 21.4 57.1 14Cardiorespiratory monitor(nonrecording)
13.3 26.7 60.0 15
Tool chest 7.7 46.2 46.2 13Capnograph 7.1 35.7 57.1 14
*Pediatric tertiary care centers surveyed include: Arkansas Children’s Hospital (AR), Lucille Packard Children’s Hospital at Stanford (CA), Children’sHospital Colorado (CO), All Children’s Hospital (FL), Rush Children’s Hospital (IL), The University of Chicago Medicine Comer Children’s Hospital (IL), RileyHospital for Children (IN), Johns Hopkins Children’s Center (MD), St. Louis Children’s Hospital (MO), Duke Children’s Hospital & Health Center (NC), StonyBrook Children’s Hospital (NY), Nationwide Children’s Hospital (OH), Children’s Hospital of Pittsburgh (PA), Ventilator Assisted Children’s Home Program(PA), and Hasbro Children’s Hospital (RI).
AMERICAN THORACIC SOCIETY DOCUMENTS
e32 American Journal of Respiratory and Critical Care Medicine Volume 193 Number 8 | April 15 2016

children dependent on long-termmechanical ventilation will requiredevelopment of innovative models ofhealth care efficiency that includemetrics that reflect: quality; medicaloutcomes; overall health care cost,including both dollars paid and time
invested by all members of the healthcare team; and patient/family experience.
Conclusions
There are many barriers to caring for theventilator-dependent child outside of the
hospital, but practitioners, families, andpatients see the benefits of care in a homesetting daily. The Workgroup hopes thatcontinued research and efforts to shareexperiences will lead to improved careand enhanced quality of life for thesepatients. n
This official clinical practice guideline of the American Thoracic Society was prepared by an ad hoc subcommittee of the Assembly on Pediatrics.
Members of the subcommittee are asfollows:
LAURA M. STERNI, M.D. (Chair)ANN C. HALBOWER, M.D. (Chair)JOSEPH M. COLLACO, M.D.CHRISTOPHER D. BAKER, M.D.JOHN L. CARROLL, M.D.GIRISH D. SHARMA, M.D.JAN L. BROZEK, M.D., PH.D.JONATHAN D. FINDER, M.D.
VEDA L. ACKERMAN, M.D.RAANAN ARENS, M.D.DEBORAH S. BOROUGHS, R.N., M.S.N.JODI CARTER, R.N., M.S.N., C.P.N.P.KAREN L. DAIGLE, M.D.JOAN DOUGHERTY, B.S.N., C.P.N., C.S.N.DAVID GOZAL, M.D.KATHARINE KEVILL, M.D.RICHARD M. KRAVITZ, M.D.TONY KRISEMAN, M.B. B.CH.
IAN MACLUSKY, M.B. B.S.KATHERINE RIVERA-SPOLJARIC, M.D.ALVARO J. TORI, M.D.THOMAS FERKOL, M.D.
Author Disclosures: L.M.S., J.M.C., C.D.B.,J.L.C., G.D.S., J.L.B., J.D.F., V.L.A., R.A.,D.S.B., J.C., K.L.D., J.D., D.G., K.K., R.M.K.,T.K., I.M., K.R.-S., A.J.T., T.F., and A.C.H.report no relevant commercial interest.
References
1. U.S. Department of Health and Human Services. The national survey ofchildren with special health care needs: chartbook 2001. 2004[accessed 2016 Mar 4]. Available from: http://mchb.hrsa.gov/chscn/pages/prevalence.htm
2. U.S. Department of Health and Human Services. Report of the SurgeonGeneral’s workshop on children with handicaps and their families.Case example: the ventilator-dependent child. 1983 [accessed 2016Mar 4]. Available from: http://profiles.nlm.nih.gov/NN/B/C/G/M/
3. U.S. Department of Health and Human Services. Surgeon General’sReport. Campaign ’87: commitment to family-centered, coordinatedcare for children with special health care needs. 1987 [accessed 2016Mar 4]. Available from: http://profiles.nlm.nih.gov/ps/access/NNBCFP.pdf
4. Adams K, Corrigan JM, editors; Institute of Medicine. Priority areas fornational action: transforming health care quality. 2003 [accessed 2016Mar 4]. Available from: http://www.nap.edu/read/10593/chapter/1
5. Schunemann HJ, Jaeschke R, Cook DJ, Bria WF, El-Solh AA, Ernst A,Fahy BF, Gould MK, Horan KL, Krishnan JA, et al.; ATS DocumentsDevelopment and Implementation Committee. An official ATSstatement: grading the quality of evidence and strength ofrecommendations in ATS guidelines and recommendations. Am JRespir Crit Care Med 2006;174:605–614.
6. McPherson M, Arango P, Fox H, Lauver C, McManus M, NewacheckPW, Perrin JM, Shonkoff JP, Strickland B. A new definition of childrenwith special health care needs. Pediatrics 1998;102:137–140.
7. Office of Disease Prevention and Health Promotion. Healthy people 2020[accessed 2016 Mar 4]. Available from: http://www.healthypeople.gov/2020/default.aspx
8. Kuo DZ, Houtrow AJ, Arango P, Kuhlthau KA, Simmons JM, Neff JM.Family-centered care: current applications and future directions inpediatric health care. Matern Child Health J 2012;16:297–305.
9. Committee on Hospital Care and Institute for Patient- and Family-Centered Care. Patient- and family-centered care and thepediatrician’s role. Pediatrics 2012;129:394–404.
10. Kuo DZ, Bird TM, Tilford JM. Associations of family-centered care withhealth care outcomes for children with special health care needs.Matern Child Health J 2011;15:794–805.
11. Kuo DZ, Frick KD, Minkovitz CS. Association of family-centered carewith improved anticipatory guidance delivery and reduced unmetneeds in child health care. Matern Child Health J 2011;15:1228–1237.
12. Medical Home Initiatives for Children With Special Needs ProjectAdvisory Committee. American Academy of Pediatrics. The medicalhome. Pediatrics 2002;110:184–186.
13. American Academy of Pediatrics Medical Home Initiatives for ChildrenWith Special Needs Project Advisory Committee. Policy statement:organizational principles to guide and define the child health caresystem and/or improve the health of all children. Pediatrics 2004;113:1545–1547.
14. American Academy of Pediatrics. National Center for Medical HomeImplementation [accessed 2016 Mar 4]. Available from: http://www.medicalhomeinfo.org/
15. Health Resources and Services Administration. Implementation ofthe medical home program [accessed 2016 Mar 4]. Available from:http://mchb.hrsa.gov/programs/medicalhome/
16. Cristea AI, Carroll AE, Davis SD, Swigonski NL, Ackerman VL.Outcomes of children with severe bronchopulmonary dysplasiawho were ventilator dependent at home. Pediatrics 2013;132:e727–e734.
17. Overman AE, Liu M, Kurachek SC, Shreve MR, Maynard RC, MammelMC, Moore BM. Tracheostomy for infants requiring prolongedmechanical ventilation: 10 years’ experience. Pediatrics 2013;131:e1491–e1496.
18. Elias ER, Murphy NA; Council on Children with Disabilities.Home care of children and youth with complex health careneeds and technology dependencies. Pediatrics 2012;129:996–1005.
19. Ziring PR, Brazdziunas D, Cooley WC, Kastner TA, Kummer ME,Gonzalez de Pijem L, Quint RD, Ruppert ES, Sandler AD, AndersonWC, et al. American Academy of Pediatrics. Committee on Childrenwith Disabilities. Care coordination: integrating health and relatedsystems of care for children with special health care needs.Pediatrics 1999;104:978–981.
20. Berry JG, Goldmann DA, Mandl KD, Putney H, Helm D, O’Brien J,Antonelli R, Weinick RM. Health information management andperceptions of the quality of care for children with tracheotomy: aqualitative study. BMC Health Serv Res 2011;11:117.
21. Dusing SC, Skinner AC, Mayer ML. Unmet need for therapy services,assistive devices, and related services: data from the national surveyof children with special health care needs. Ambul Pediatr 2004;4:448–454.
22. Graham RJ, Fleegler EW, Robinson WM. Chronic ventilator need in thecommunity: a 2005 pediatric census of Massachusetts. Pediatrics2007;119:e1280–e1287.
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents e33

23. van Kesteren RG, Velthuis B, van Leyden LW. Psychosocial problemsarising from home ventilation. Am J Phys Med Rehabil 2001;80:439–446.
24. Graham RJ, Pemstein DM, Palfrey JS. Included but isolated: earlyintervention programmes provision for children and families withchronic respiratory support needs. Child Care Health Dev 2008;34:373–379.
25. Noyes J, Hartmann H, Samuels M, Southall D. The experiences andviews of parents who care for ventilator-dependent children. J ClinNurs 1999;8:440–450.
26. Kirk S, Glendinning C. Developing services to support parents caringfor a technology-dependent child at home. Child Care Health Dev2004;30:209–218. [Discussion, p. 219.]
27. Dybwik K, Tollali T, Nielsen EW, Brinchmann BS. “Fighting the system”:families caring for ventilator-dependent children and adults withcomplex health care needs at home. BMC Health Serv Res 2011;11:156.
28. Wallander JL, Varni JW. Effects of pediatric chronic physical disorderson child and family adjustment. J Child Psychol Psychiatry 1998;39:29–46.
29. Sabbeth BF, Leventhal JM. Marital adjustment to chronic childhoodillness: a critique of the literature. Pediatrics 1984;73:762–768.
30. Meltzer LJ, Mindell JA. Impact of a child’s chronic illness on maternalsleep and daytime functioning. Arch Intern Med 2006;166:1749–1755.
31. Heaton J, Noyes J, Sloper P, Shah R. Families’ experiences of caringfor technology-dependent children: a temporal perspective. HealthSoc Care Community 2005;13:441–450.
32. DeRigne L. The employment and financial effects on families raisingchildren with special health care needs: an examination of theevidence. J Pediatr Health Care 2012;26:283–290.
33. Murphy NA, Christian B, Caplin DA, Young PC. The health of caregiversfor children with disabilities: caregiver perspectives. Child CareHealth Dev 2007;33:180–187.
34. Kuster PA, Badr LK. Mental health of mothers caring for ventilator-assisted children at home. Issues Ment Health Nurs 2006;27:817–835.
35. Brehaut JC, Kohen DE, Raina P, Walter SD, Russell DJ, Swinton M,O’Donnell M, Rosenbaum P. The health of primary caregivers ofchildren with cerebral palsy: how does it compare with that of otherCanadian caregivers? Pediatrics 2004;114:e182–e191.
36. Carnevale FA, Alexander E, Davis M, Rennick J, Troini R. Daily livingwith distress and enrichment: the moral experience of families withventilator-assisted children at home. Pediatrics 2006;117:e48–e60.
37. Benneyworth BD, Gebremariam A, Clark SJ, Shanley TP, Davis MM.Inpatient health care utilization for children dependent on long-termmechanical ventilation. Pediatrics 2011;127:e1533–1541.
38. Paulides FM, Plotz FB, Verweij-van den Oudenrijn LP, van Gestel JP,Kampelmacher MJ. Thirty years of home mechanical ventilation inchildren: escalating need for pediatric intensive care beds. IntensiveCare Med 2012;38:847–852.
39. Gordon JB, Colby HH, Bartelt T, Jablonski D, Krauthoefer ML, HavensP. A tertiary care-primary care partnership model for medicallycomplex and fragile children and youth with special health careneeds. Arch Pediatr Adolesc Med 2007;161:937–944.
40. Casey PH, Lyle RE, Bird TM, Robbins JM, Kuo DZ, Brown C, Lal A,Tanios A, Burns K. Effect of hospital-based comprehensive careclinic on health costs for Medicaid-insured medically complexchildren. Arch Pediatr Adolesc Med 2011;165:392–398.
41. DeVries A, Li CH, Sridhar G, Hummel JR, Breidbart S, Barron JJ. Impactof medical homes on quality, healthcare utilization, and costs. Am JManag Care 2012;18:534–544.
42. Romaire MA, Bell JF, Grossman DC. Health care use and expendituresassociated with access to the medical home for children and youth.Med Care 2012;50:262–269.
43. Frankel A, Leonard M, Simmonds T, Haraden C, Vega K, editors. Theessential guide for patient safely officers. Oakbrook Terrace, IL: TheJoint Commission on Accreditation of Healthcare Organizations andInstitute for Healthcare Improvement; 2009.
44. Peterson-Carmichael SL, Cheifetz IM. The chronically critically illpatient: pediatric considerations. Respir Care 2012;57:993–1002.[Discussion, pp. 1002–1003.]
45. Antonelli R, Stille C, Freeman L. Enhancing collaboration betweenprimary and subspeciality care providers for children and youth withspecial health care needs. Washington, DC: Georgetown UniversityCenter for Child and Human Development. 2005.
46. Cohen E, Lacombe-Duncan A, Spalding K, MacInnis J, Nicholas D,Narayanan UG, Gordon M, Margolis I, Friedman JN. Integratedcomplex care coordination for children with medical complexity: amixed-methods evaluation of tertiary care-community collaboration.BMC Health Serv Res 2012;12:366.
47. Cohen E, Bruce-Barrett C, Kingsnorth S, Keilty K, Cooper A, Daub S.Integrated complex care model: lessons learned from inter-organizational partnership. Healthc Q 2011;14:64–70.
48. Edwards EA, O’Toole M, Wallis C. Sending children home ontracheostomy dependent ventilation: pitfalls and outcomes. Arch DisChild 2004;89:251–255.
49. Margolan H, Fraser J, Lenton S. Parental experience of services whentheir child requires long-term ventilation: implications forcommissioning and providing services. Child Care Health Dev 2004;30:257–264.
50. Ambrosio IU, Woo MS, Jansen MT, Keens TG. Safety of hospitalizedventilator-dependent children outside of the intensive care unit.Pediatrics 1998;101:257–259.
51. Edwards JD, Kun SS, Keens TG. Outcomes and causes of death inchildren on home mechanical ventilation via tracheostomy: aninstitutional and literature review. J Pediatr 2010;157:955–959.e2.
52. Eigen H, Zander J; American Thoracic Society. Home mechanicalventilation of pediatric patients. Am Rev Respir Dis 1990;141:258–259.
53. Jardine E, Wallis C; UK Working Party on Paediatric Long TermVentilation. Core guidelines for the discharge home of the child onlong-term assisted ventilation in the United Kingdom. Thorax 1998;53:762–767.
54. Nixon GM, Edwards EA, Cooper DM, Fitzgerald DA, Harris M, Martin J,Massie RJ, Suresh S, Waters KA, Wilson A. Ventilatory support athome for children: a consensus statement from the Australasianpaediatric respiratory group. 2008 [accessed 2016 Mar 4]. Availablefrom: http://www.thoracic.org.au/journal-publishing/command/download_file/id/10/filename/Ventilatory_Support_at_Home_for_Children._A_Consensus_Statement_from_the_Australasian_Paediatric_Respiratory_Group.pdf
55. AARC; Respiratory Home Care Focus Group. AARC clinical practiceguideline. Long-term invasive mechanical ventilation in the home:2007 revision & update. Respir Care 2007;52:1056–1062.
56. Windisch W, Walterspacher S, Siemon K, Geiseler J, Sitter H; GermanSociety for Pneumology; Published by the German Society forPneumology (DGP). Guidelines for non-invasive and invasivemechanical ventilation for treatment of chronic respiratory failure.Pneumologie 2010;64:640–652.
57. McKim DA, Road J, Avendano M, Abdool S, Cote F, Duguid N, FraserJ, Maltais F, Morrison DL, O’Connell C, et al.; Canadian ThoracicSociety Home Mechanical Ventilation Committee. Home mechanicalventilation: a Canadian Thoracic Society clinical practice guideline.Can Respir J 2011;18:197–215.
58. Boroughs D, Dougherty JA. Decreasing accidental mortality ofventilator-dependent children at home: a call to action. HomeHealthc Nurse 2012;30:103–111; quiz 112–113.
59. Kun SS, Edwards JD, Ward SL, Keens TG. Hospital readmissions fornewly discharged pediatric home mechanical ventilation patients.Pediatr Pulmonol 2012;47:409–414.
60. Reiter K, Pernath N, Pagel P, Hiedi S, Hoffmann F, Schoen C, Nicolai T.Risk factors for morbidity and mortality in pediatric home mechanicalventilation. Clin Pediatr (Phila) 2011;50:237–243.
61. Sherman JM, Davis S, Albamonte-Petrick S, Chatburn RL, Fitton C,Green C, Johnston J, Lyrene RK, Myer C III, Othersen HB, et al.Care of the child with a chronic tracheostomy: this officialstatement of the American Thoracic Society was adopted by theATS Board of Directors, July 1999. Am J Respir Crit Care Med2000;161:297–308.
AMERICAN THORACIC SOCIETY DOCUMENTS
e34 American Journal of Respiratory and Critical Care Medicine Volume 193 Number 8 | April 15 2016

62. Mitchell RB, Hussey HM, Setzen G, Jacobs IN, Nussenbaum B,Dawson C, Brown CA III, Brandt C, Deakins K, Hartnick C, et al.Clinical consensus statement: tracheostomy care. Otolaryngol HeadNeck Surg 2013;148:6–20.
63. Tolomeo C, Bazzy-Asaad A. Utilization of a second caregiver in thecare of a child with a tracheostomy in the homecare setting. PediatrPulmonol 2010;45:656–660.
64. Ronczy NM, Beddome MA. Preparing the family for home tracheotomycare. AACN Clin Issues Crit Care Nurs 1990;1:367–377.
65. Oberwaldner B, Eber E. Tracheostomy care in the home. PaediatrRespir Rev 2006;7:185–190.
66. Rouault S. Education of the families of patients receiving domiciliaryventilation [in French]. Rev Mal Respir 2005;22:461–465.
67. Salvesen RS, Mostad U, Aadahl P. Care for children with tracheostomy[in Norwegian]. Tidsskr Nor Laegeforen 2005;125:907–909.
68. Barnes LP. Tracheostomy care: preparing parents for discharge. MCNAm J Matern Child Nurs 1992;17:293.
69. Graf JM, Montagnino BA, Hueckel R, McPherson ML. Children withnew tracheostomies: planning for family education and commonimpediments to discharge. Pediatr Pulmonol 2008;43:788–794.
70. Tearl DK, Cox TJ, Hertzog JH. Hospital discharge of respiratory-technology-dependent children: role of a dedicated respiratory caredischarge coordinator. Respir Care 2006;51:744–749.
71. Kun SS, Davidson-Ward SL, Hulse LM, Keens TG. How much doprimary care givers know about tracheostomy and home ventilatoremergency care? Pediatr Pulmonol 2010;45:270–274.
72. Hefner JL, Tsai WC. Ventilator-dependent children and the healthservices system: unmet needs and coordination of care. Ann AmThorac Soc 2013;10:482–489.
73. Meltzer LJ, Boroughs DS, Downes JJ. The relationship between homenursing coverage, sleep, and daytime functioning in parents ofventilator-assisted children. J Pediatr Nurs 2010;25:250–257.
74. Dougherty JM, Parrish JM, Parra M, Kinney ZA, Kandrak G. Part 2:using a competency-based curriculum to train experienced nurses inventilator care. Pediatr Nurs 1996;22:47–50.
75. Kun SS, Beas VN, Keens TG, Ward SS, Gold JI. Examining pediatricemergency home ventilation practices in home health nurses:opportunities for improved care. Pediatr Pulmonol 2015;50:691–697.
76. Tibballs J, Henning R, Robertson CF, Massie J, Hochmann M, Carter B,Osborne A, Stephens RA, Scoble M, Jones SE, et al. A homerespiratory support programme for children by parents andlayperson carers. J Paediatr Child Health 2010;46:57–62.
77. Kun SS, Nakamura CT, Ripka JF, Davidson Ward SL, Keens TG. Homeventilator low-pressure alarms fail to detect accidental decannulationwith pediatric tracheostomy tubes. Chest 2001;119:562–564.
78. Farre R, Navajas D, Prats E, Marti S, Guell R, Montserrat JM, Tebe C,Escarrabill J. Performance of mechanical ventilators at the patient’shome: a multicentre quality control study. Thorax 2006;61:400–404.
79. Chatwin M, Heather S, Hanak A, Polkey MI, Simonds AK. Analysis ofhome support and ventilator malfunction in 1,211 ventilator-dependent patients. Eur Respir J 2010;35:310–316.
80. Farre R, Lloyd-Owen SJ, Ambrosino N, Donaldson G, Escarrabill J,Fauroux B, Robert D, Schoenhofer B, Simonds A, Wedzicha JA.Quality control of equipment in home mechanical ventilation: aEuropean survey. Eur Respir J 2005;26:86–94.
81. US Food and Drug Administration. How consumers can report anadverse event or serious problem to FDA [accessed 2016 Mar 4].Available from: http://www.fda.gov/Safety/MedWatch/HowToReport/ucm053074.htm
82. Lujan M, Sogo A, Pomares X, Monso E, Sales B, Blanch L. Effect ofleak and breathing pattern on the accuracy of tidal volume estimationby commercial home ventilators: a bench study. Respir Care 2013;58:770–777.
83. Blakeman TC, Rodriquez D Jr, Hanseman D, Branson RD. Benchevaluation of 7 home-care ventilators. Respir Care 2011;56:1791–1798.
84. Birnkrant DJ, Bushby KM, Amin RS, Bach JR, Benditt JO, Eagle M,Finder JD, Kalra MS, Kissel JT, Koumbourlis AC, et al. Therespiratory management of patients with Duchenne musculardystrophy: a DMD care considerations working group specialtyarticle. Pediatr Pulmonol 2010;45:739–748.
85. Finder JD, Birnkrant D, Carl J, Farber HJ, Gozal D, Iannaccone ST,Kovesi T, Kravitz RM, Panitch H, Schramm C, et al.; AmericanThoracic Society. Respiratory care of the patient with Duchennemuscular dystrophy: ATS consensus statement. Am J Respir CritCare Med 2004;170:456–465.
86. Wang CH, Finkel RS, Bertini ES, Schroth M, Simonds A, Wong B,Aloysius A, Morrison L, Main M, Crawford TO, et al.; Participants ofthe International Conference on SMA Standard of Care. Consensusstatement for standard of care in spinal muscular atrophy. J ChildNeurol 2007;22:1027–1049.
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents e35





























