Embed Size (px)
Citation preview

Abstract of dissertation entitled
“An evidence-based guideline of nurse telephone follow-up service
in glycaemic control for Type 2 diabetic patients”
Submitted by
Ho Fung Yi
For the Degree of Master of Nursing
at The University of Hong Kong
in August 2015
Abstract
Diabetes Mellitus is one of the globally growing problems especially in the Asia-Pacific
Region. Among all the cases of diabetes, Type 2 diabetes is predominantly increased in the
prevalence and it accounted for 90% of diabetes around the world. People who suffered from Type
2 diabetes are mainly due to unhealthy lifestyle, overweight and obesity. Diabetes patients who
have not control their blood glucose satisfactorily may result in complications to heart, blood
vessels, eyes, kidneys, and nerves.
In Hong Kong, diabetes causes an increasing trend in hospital admission and death rate due to
its complications. The number of diabetics will keep on rising due to aging population and more
people who have adopted sedentary lifestyle and westernized diet. The health care system in Hong
Kong has stressed and promoted the importance of healthy lifestyle and medication adherence to
diabetic patients, however, the satisfaction of glycaemic control is still failed to achieve.

The Hospital Authority in Hong Kong promotes and supporting patients health. Healthcare
professionals empower patients to regain their health and stay healthy by offering patients support
and empowerment. To support and empower diabetes patients to control and manage their disease, a
nurse-led telephone follow-up service is necessary to implement.
The nurse-led telephone follow-up is a kind of follow-up service that aims to provide help to
diabetes patients to overcome those self-care management barriers. Nurse telephone follow-up
service is an integrated life course approach to manage the disease progression of Type 2 diabetic
patients. Telephone intervention provides a regular follow-up to Type 2 diabetic patients. Patients
will be requested to prepare the self-management diaries that the blood glucose level, any food
taken and the duration of exercise are recorded. Regular feedbacks will be given according to their
self-management diaries. Through nurse-led telephone follow-up, patients’ self-empowerment and
self-management skills will be built up. Besides, treatment satisfaction and the rapport between
patients and nurses shall also be improved.
An evidence-based guideline for providing nurse telephone follow-up service was developed
to help healthcare professionals to provide competent and effective counseling and follow up to
diabetic patients. The objective of this study is to identify the evidence and develop an evidence-
based guideline of the nurse telephone service in glycaemic control in Type 2 diabetic patients. A
systematic search was performed using three electronic databases which include PubMed, CINAHL
and Cochrane Library.
Seven randomized controlled studies were identified through comprehensive literature review.
Data were compiled into tables of evidence. Also, critical appraisal was performed. The quality of
theses studies was graded according to the Scottish Intercollegiate Guidelines Network (SIGN)
framework. An evidence-based guideline was developed based on the analyzed research findings.

The implementation potential including the transferability, feasibility and cost-benefit ratio of the
innovation was assessed. Guideline with level of evidence and recommendation grading was
developed. The implementation plan was demonstrated by communication plan between
stakeholders and potential users. Pilot test would be carried out to explore any unexpected problems
that could avoid in the full-scale implementation. An evaluation plan including patient outcomes,
healthcare provides outcomes and system outcomes would discuss in the end of the dissertation.

“An evidence-based guideline
of nurse telephone follow-up service in glycaemic control for Type 2 diabetic patients”
By
Ho Fung Yi
BNurs (HKU)
A thesis submitted in partial fulfillment of the requirements for
the Degree of Master of Nursing
at the University of Hong Kong
August 2015

I
Declaration
I declare that this thesis represents my own work, except where due acknowledgement is made, and
that it has not been previously included in a thesis, dissertation or report submitted to this
University or to any other institution for a degree, diploma or other qualifications.
Signed …………………………………..
Ho Fung Yi i

II
Acknowledgements
I would like to thank for the sincere support and guidance from my dissertation supervisor
Dr. Elizabeth Choi of Department of Nursing, the University of Hong Kong.
I would also like to thank my colleagues for their contribution to the study, in particular, my
Ward Manager, Ms. Judy Luk and Advanced Practice Nurse, Ms. Leung Siu Kuen for their
encouragement and sincere support in the past 2 years.
Besides, I would like to thank my mother, my father and my family in supporting me
throughout the study. Without their support, I would not be able to complete the study.
Finally, I would like to thank God for guiding me throughout the study. Without the
unreserved love of God, this dissertation cannot see the light of the day.
ii
III Table of Contents
Declaration
i
Acknowledgement
ii
Table of Contents
iii
Abbreviations iv Chapter 1: Introduction
1.1 Background...........................................................................................
p. 2
1.2 Affirming the need................................................................................
p. 4
1.3 Significance...........................................................................................
p.7
Chapter 2: Critical appraisal
2.1 Search and Appraisal Strategies............................................................
p. 9
2.2 Results...................................................................................................
p. 11
2.3 Summary and synthesis.........................................................................
p. 15
Chapter 3: Translation and application
3.1 Implementation potential......................................................................
p. 19
3.2 Evidence-based guideline.....................................................................
p. 29
Chapter 4: Plan for implementation and evaluation the innovation
4.1 Communication plan.............................................................................
p.31
4.2 Pilot testing........................................................................................... p.35

4.3 Evaluation plan p. 37
Chapter 5: Conclusion..............................................................................
p. 41
References..................................................................................................
p. 42
Appendices
Appendix A Search history.........................................................................
p. 45
Appendix B Table of evidence...................................................................
p. 47
Appendix C SIGN checklist of RCTs.........................................................
p. 54
Appendix D SIGN grading system (1999-2012)........................................
p. 56
Appendix E The results of quality assessment and level of evidence of the studies....................................................................................................
p. 57
Appendix F Time for implementation and evaluation................................
p. 58
Appendix G Cost of implementation innovation........................................
p. 59
Appendix H Evidence-based of guideline..................................................
p. 60
Appendix I Grades of recommendations....................................................
p. 64
Appendix J Patient satisfaction questionnaire............................................
p. 65
Appendix K Audit form on healthcare professional compliance with the nurse telephone follow-up services guideline.............................................
p. 66
Appendix L Healthcare professional satisfaction questionnaire.................
p. 67
Appendix M Effect of the diabetes nurse telephone follow-up on HbA1c levels and self-care adherence assessment form………………………….
p. 68
iii

IV
Abbreviations
ADA American Diabetes Association
APN Advanced Practice Nurse
COS Chief of Service
DOM Department Operational Manager
GMN General Manager (Nursing)
HbA1c Glycosylated hemoglobin
NC Nurse Consultant
NO Nurse Officer
OHA
Oral Hypoglycemic Agents
RCT Randomized Controlled Trial
RN Registered Nurse
SIGN Scottish Intercollegiate Guidelines Network
SMBG Self-monitoring of blood glucose
SPSS Statistical Package for the Social Sciences
WHO World Health Association
iv

Chapter 1: Introduction
Diabetes Mellitus is one of the globally growing health problems. Especially in the Asia-Pacific
Region, diabetes has become epidemic. According to estimation by World Health Association
(WHO), there will be 9% of adult aged 18 and older suffered from diabetes in 2014 (WHO, 2012).
In 2012, about 1.5 million deaths were directly caused by diabetes (WHO, 2014). Diabetes is
projected to be the one of the leading causes to death in 2030 (Mathers & Loncar, 2006). In Hong
Kong, at least one in every ten adults suffers from diabetes. The Population Health Survey 2003/04
stated that nearly 4% of people aged 15 and above are diagnosed with diabetes (Centre for Health
Protection, 2013). The number of diabetics will keep on rising with our aging population in
particular for people who have adopted sedentary lifestyle and westernized diet.
Diabetes and its complications will significantly increase the risk of morbidities and mortalities. In
the past few decades, diabetes causes an increasing trend in hospital admission and death rate.
According to the Centre for Health Protection (2013), about 23,000 hospital admissions and patient
deaths in all the hospital settings are in relation to diabetes or its complications. Diabetes was also
the tenth commonest cause of deaths and amounted to over 1% of all deaths in 2011. The exact
number of hospitalization and deaths caused by diabetes may possibly higher since many
hospitalization and deaths can be resulted to diabetes related disease or its complications.
Among all cases of diabetes, Type 2 diabetes is predominantly increased in the prevalence. About
90% of diabetics are Type 2 diabetes around the world (WHO, 1999). In Hong Kong, Type 2
diabetes is the most common form of diabetes (Chan, 2000). People who suffered from Type 2
diabetes are mainly due to unhealthy lifestyle, overweight and obesity. Diabetes patients who have
not control their blood glucose satisfactorily may result in complications to heart, blood vessels,
eyes, kidneys, and nerves. Also, early interventions such as lifestyle modification, regular
complications screening and pharmacological treatment have revealed to be effective in delaying

the onset of diabetes complications. In Hong Kong, the health care system has stressed and
promoted the importance of healthy lifestyle and medication adherence to diabetic patients,
however, the satisfaction of glycaemic control is still failed to achieve. Therefore, in order to cope
with the increasing interests, demand and expectation on public health care service from our
society, it is necessary to explore any effective intervention in order to improve the diabetic care to
patients.
1.1 Background
Diabetes is a chronic illness worldwide which causes blood glucose levels to rise higher than
normal. Type 2 diabetes is the most common type of diabetes and is normally related to either
reduction in insulin production or non-reaction of body cells to the existence of insulin (American
Diabetes Association, 2009). Type 2 diabetes is a major cause of end-stage renal failure, heart
disease, stroke, blindness, nerve damage and below knee amputation (Martinez-Castelao et al.,
2004).
Performing self-monitoring of blood glucose (SMBG) before and after meals and having regular
check on glycosylated hemoglobin (HbA1c) level will help in monitoring the disease progress. The
HbA1c test is the important index of glycaemic control. It reflects the mean blood glucose level for
the past 2 to 3 months. By measuring the HbA1c level in the blood, it can get an overview picture
of the average blood glucose level for the past few months. Also, it gives useful and meaningful
information for possible implementation/revision of diabetes management plan. For instance, based
on the results of HbA1c test, accuracy and reliability of self-testing results can be verified and
judgment on effectiveness of the treatment plan can be made. According to American Diabetes
Association (ADA) (2009), the target HbA1c level is below 7%. By lowering HbA1c level to 7%
or below has been shown to reduce macrovascular, microvascular and neuropathic complications of
diabetes.

The management goal of Type 2 diabetes is mainly controlled and reduced symptom instead of
curing. It requires a long-time change in lifestyle by eating a healthy diet, having regular physical
exercise, maintaining a normal body weight and avoiding tobacco use. Besides, performing SMBG
regularly and having insulin injection and medications on time are necessary in maintaining optimal
blood glucose level.
However, the rate of compliance to the treatment regime and healthy lifestyle were low. Since some
patients may find that the diabetic regime contain many aspects that are difficult and inconvenient
to follow. It is a burden for them to have lifestyle change and adherence to health behavior. Besides,
several studies showed that poor adherence rate to diet is the greatest self-care management barrier
in glycaemic control (Glasgow & Anderson, 1999, Chan & Molassiotis, 1999). In order to
overcome these problems, it is necessary to implement a nurse-led telephone follow-up service.
Telephones are universal available and users’ friendly. A lot of health related treatment such as
health status assessments, monitor treatment progress, provide self-care education, reinforce
adherence to treatment regime and maintain continuity of care to patients can all conduct and
achieve by telephone follow-up intervention (Funnell et al., 2007).
The nurse-led telephone follow-up is a kind of follow-up service that aims to provide help to
diabetes patients to overcome those self-care management barriers. Through the nurse-led telephone
follow-up service, monitoring the symptoms of diabetes, reinforcing healthy lifestyle behavior and
medication compliance can be achieved (Weinberger et al., 1995, Boucher et al, 2000). It provides
health education integrated with patients’ daily activities and compromised to them on
implementation of an effective diabetic care plan (Anderson et al., 1995). Nurses also empower
patients to make lifestyle modification and provide them with psychosocial support can increase the

adherence level to the treatment regime (Glasgow & Anderson, 1999). Since many patients who are
difficult to ambulate, live far away to the clinics or time constraints that make them limit to assess
to the out-patient service, the use of nurse-led telephone follow-up service to patients could provide
the opportunity to facilitate accessibility to healthcare services and thus enhance patient and nurse
relationship, decrease healthcare expenditures and reduce waiting time to get help from nurses. It
enables nurses to provide care to more patients by shorten the clinic time. Shorten waiting time and
reduced travel time may improve patients’ satisfaction with care (Funnell et al., 2007).
1.2 Affirming the Need
Patients upon diagnosis of diabetes from the primary care practitioners in Hong Kong, they will be
referred to manage their disease in hospital, specialist care or continue care in primary care
practitioners. For patients who are acutely ill, poorly diabetes control such as heavy ketonuria,
diabetic ketoacidosis or diabetic hyperosmolar non-ketotic syndrome will be emergency admitted to
hospital for further management. For the patients who are aged below 30 years, presence of
complications or women who are pregnant will be referred to specialist to further follow-up.
Clinical admission to metabolic ward for titration of medication maybe needed when blood glucose
level was not well controlled. The rest of patients who have diabetes with stabilized control will
continue care in primary care setting.
In Hong Kong, patients with diabetes have to meet doctor for follow-up at 3-4 times per year to
review medication treatment in the government setting. They will also have diabetic complication
screening yearly to detect any risk factor and presence of diabetic complication. For patients with
poor glycaemic control, they will be referred to diabetes nurse-led clinic for follow-up closely to
monitor and further titrate the medication.

In Hong Kong, diabetes nurses provide care for people with diabetes in hospitals and community.
Diabetes nursing services include clinical management, diabetes self-management education and
community health promotion.
For clinical management, diabetes nurses provide complication screening, education service to the
individuals and their significant others, stabilize glycaemic control by adjusting anti-diabetic
medications specified in the organization approved protocols, arrange early medical review where
appropriate, refer to other health care professionals accordingly, and formulate discharge plans and
collaborate with multidisciplinary team members to ensure continuity of care (Hospital Authority
Head Office, 2014).
For diabetes self-management education, diabetes nurses assess the learning needs and abilities of
the individual and their significant others, plan and conduct education programs appropriate to
them, and evaluate their effectiveness so as to empower them on self-care management (Hospital
Authority Head Office, 2014). The self-management education includes SMBG, insulin injection
technique, symptoms and its managements of hypoglycaemia and hyperglycaemia, advice on
traveling, diabetic foot care and gestational diabetes mellitus. Diabetes nurses also provide hotline
service to answer disease management issues.
For community health promotion, diabetes nurses will collaborate with local or international
organizations to conduct health education out-reach programs or seminars to promote diabetes
health and awareness for the community (Hospital Authority Head Office, 2014).
However, the hospital environment is not a real life environment to monitor the blood glucose level.
Patients in the hospital seldom do exercise and their meals are all well planned by the dietitian. The
frequency of blood glucose checking and the time of insulin injection are all planned by doctor’s

prescription and followed by the ward routines. Therefore, during the hospitalization, patients are
often having an optimal glycaemic control in the ward, however, when they are discharged home
and back to a less stringent environment, their blood glucose level will be less easy to control well.
Nowadays, mostly all diabetes managements take place at physicians’ clinics or nurse-led clinic by
face-to-face counseling. Besides, group-based structured diabetes education and hotline services to
manage self-management problems are not enough to sustain and maintain the adherence to the
diabetes control recommendations in patients. Therefore, the admission and death rate was in an
increasing trend in the past few decades as mentioned before.
Implementation of diabetes nurse-led telephone follow-up service can act as an alternative strategy
to deliver diabetic managements and knowledge to patients’ home and monitor their treatment
progress. It also improves patients’ self-empowerment, quality of life, self-management skills and
treatment satisfaction based on the needs of different people.
Nurse telephone follow-up service is an integrated life course approach to manage the disease
progression of Type 2 diabetic patients. Telephone follow-up service in diabetes showed
improvement in glycemic control. Monitor patients blood glucose level, reinforce their health
behavior, review their drugs compliance and adjust their medication can all be achieved and
conducted by the nurse telephone follow-up (Kim & Oh, 2003). Telephone intervention provides a
regular follow-up to Type 2 diabetic patients. Patients will be requested to prepare the self-
management diaries that the blood glucose level, any food taken and the duration of exercise are
recorded. Regular feedbacks will be given according to their self-management diaries. Through
nurse-led telephone follow-up, patients’ self-empowerment and self-management skills will be built
up. Besides, treatment satisfaction and the rapport between patients and nurses shall also be
improved.

1.3 Significance
As mentioned before, there were about 23,000 hospital admissions and patient deaths in all the
hospital settings. The exact number of hospitalization and deaths caused by diabetes may possibly
higher due to diabetic complications (Centre for Health Protection, 2013). Considered that diabetes
was one of the commonest causes of deaths and formed a major part of expenditures in health care
settings, the importance of good glycaemic control should be promoted in order to reduce the rate of
deterioration of the disease. Studies consistently showed that patients with adequate control of
blood glucose level could prevent or delay the complications of diabetes. Stratton et al. (2000)
proved that for every 1% reduction in HbA1c level could have an associated reduction in the risk of
deaths, risk of suffering form myocardial infarction and risk of suffering from microvascular
complications respectively by 21%, 14% and 37%. By reducing the risk of deaths and
complications, the hospitalization and deaths caused by diabetes can be reduced. Therefore, the
expenditures of diabetic care will also be decreased.
In the current practice, diabetes nurse-led clinic only provide education and ambulatory dosage
adjustment of insulin to diabetic patients by face to face counseling instead of telephone follow-up
service. It is necessary to setup the nurse-led telephone follow-up service to provide a feasible and
effective care to diabetic patients and reduce the healthcare expenditure. By implementation of
nurse-led telephone follow-up service, patients can have more frequent follow-up to monitor their
disease progression, obtain feedback and receive updated knowledge and management of diabetes
form healthcare providers. Besides, by using nurse telephone follow-up, patients can participate in
the diabetic managements and treatments, and thus can improve patients’ self-empowerment, self-
management skills and treatment satisfaction. In addition, the waiting time and the appointment
making to see diabetes nurse will be decreased. Therefore, the relationship between patients and
diabetes nurses will also be improved and good rapports and interactions between patients and

diabetes nurses can be established. In a long run, better glycaemic control can be achieved and the
hospital admission rate will be decreased. Thus, the bed occupancy rate due to poor glycaemic
control will be decreased ultimately.
In order to have a better understanding of the effectiveness and efficiency of nurse-led telephone
follow-up intervention, the research question proposed is as follow.
“In the healthcare setting, how effective is a nurse telephone follow-up intervention in
comparison to the routine follow-up care in improvement of blood glucose level in Type 2
diabetic patients?”
The objective of this study is “to evaluate the effect of nurse telephone follow-up service in
glycaemic control for Type 2 diabetic patients”.
The hypothesis is:
The glycaemic level in Type 2 diabetic patients would be reduced by an effective nurse telephone
follow-up intervention.

Chapter 2: Critical Appraisal
2.1 Search and Appraisal Strategies
In order to investigate the impact on the nurse-led telephone follow-up in glycaemic control, a
systematic review of relevant studies was performed through the three electronic databases which
were PubMed, CINHAL and Cochrane Library. The keywords used for searching were ‘diabetes’ or
‘diabetes mellitus’ or ‘Type 2 diabetes’ and ‘telephone’ or ‘telephone follow-up’ and ‘glycaemic
control’ or ‘adherence’ or ‘nurse’.
Systematic search was done between 15th April 2014 and 15th September 2014. Without setting any
limitation to the publication years or language in order to obtain as many as relevant studies as
possible. Total 813 studies were yielded, in which 683 studies from PubMed, 113 from CINHAL,
and 17 from Cochrane Library. After screening those titles and abstracts of the studies, 32 studies
were obtained. After reading those full texts, 15 studies were identified. Besides, manual search to
the reference lists of relevant papers was performed, 4 more studies were identified. After removal
of the duplication copies, 7 studies were obtained finally. The search history was shown in
flowchart in Appendix A.
The searching criterion is limited to the randomized controlled trail (RCT) studies. The inclusion
and exclusion criteria are as follow:
Inclusion criteria:
Type 2 diabetes
Nurse-led telephone follow-up
The main outcome of the studies is HbA1c level
Participants are able to communicate by phone

Exclusion criteria:
Children
Unstable in general medical condition
Mental illness
Poor cognitive state
Being admitted to hospital
Appraisal strategies
The quality of the seven identified articles was assessed by the Scottish Intercollegiate Guidelines
Network (SIGN) and the level of evidence was assessed by the SIGN grading system (1999-2012).
The RCTs checklist developed by the SIGN is used to assess the internal validity and overall
assessment of study. The SIGN checklist reviews and assesses the appropriate and clearly focused
questions, randomization, concealment method, blinding of allocation between subjects and
investigators, similarity of baseline data between the intervention and comparison group, group
difference between group under treatment investigation, validity and reliability of outcomes
measurement, dropout rate, intention to treat analysis, comparable for all sites, minimize bias,
statistical power and generalizability of the result. The SIGN checklist for RCTs is shown in
Appendix C.
The SIGN grading system (1999-2012) is used to assess the level of evidence of the study. High
quality RCTs with a very low risk of bias is graded as ‘1++’. Well-conducted RCTs with a low risk
of bias are graded as ‘1+’. RCTs with a high risk of bias are grades as ‘1-‘. The SIGN grading
system (1999-2012) is shown in Appendix D. The results of the quality assessment and the level of
evidence of the studies are shown in Appendix E.

2.2 Results
The publication years of the study were between 2003 and 2013. The studies were conducted in
South Korea, Iran, California and Italy. Three studies recruited participants from the endocrinology
outpatient department (Kim & Oh, 2003, Oh et al., 2003 and Kim, Oh & Lee, 2004), one study from
Diabetes Society (Nesari et al., 2010), one study form diabetes clinic (Aliha et al., 2013), one study
from medical center (Taylor et al., 2003) and one study from three diabetes outpatient clinics
(Franciosi et al., 2011). The length of follow-up in the reviewed studies ranged from 12 weeks to 1
year. The intervention of all studies was nurse-led telephone follow-up and the control was usual
care. The HbA1c level was the main outcome measure.
Total seven studies were identified and those data were extracted to form the table of evidence. A
table of evidence provides a good summary of relevant articles for the synthesis of results. The
seven table of evidence extracted from identified articles are shown in Appendix B.
Summarize study characteristics
All of the seven identified studies were randomized controlled trial. Three studies were conducted
in South Korea (Kim & Oh, 2003, Oh et al., 2003 and Kim, Oh & Lee, 2004), one from Iran
(Franciosiet al., 2011), one form California (Taylor et al., 2003) and two from Iran (Nesari, 2010,
Aliha et al., 2013).
The sample size of participants was varied from 25 to 169 with mean age from 49 to 62. All of the
participants from seven studies were diagnosed with Type 2 diabetes.
Four studies (Kim & Oh, 2003, Oh et al., 2003, Nesariet al., 2010 and Kim, Oh & Lee, 2004)
required their participants to have diagnosis with Type 2 diabetes according to the ADA criteria and
with HbA1c level > 7%. Subjects should be able to perform SMBG, self-injection of insulin or

taking oral hypoglycemic agents (OHA), understand the treatment procedure and have access to a
telephone.
For the study of Aliha et al. (2013), they specified no requirement on HbA1c level and did not
mention whether participants needed to perform SMBG or self -injection of insulin. From the study
of Tayloret al. (2003), they required the participants to have HbA1c level > 10% and with one or
more medical comorbid conditions such as hypertension, hyperlipidemia or cardiovascular disease.
The intervention and comparison group of the seven identified studies were similar and easy for
comparison. Before implementation of the intervention, education was provided to all participants
about the knowledge of diabetes, risk factors, diet control, exercise, medication, hypoglycemia and
hyperglycemia symptoms by diabetic care booklet (Kim & Oh, 2003, Oh et al., 2003, and Kim, Oh
& Lee, 2004); 3 day diabetes self-care education program (Nesari et al., 2010); two educational
sessions (Aliha et al., 2013) or individual nurse consultation, weekly group class and educational
program (Franciosi et al., 2011).
In the intervention group, the participants from all the seven studies were then received telephone
follow-up to monitor the glycaemic control, reinforce the diabetic treatment regime and answer
participants’ questions. From the studies of Kim & Oh (2003), Oh et al. (2003), and Kim, Oh & Lee
(2004), telephone calls will be provided at least twice a week for the first month and then weekly
for the second and third month. The frequency of the telephone calls was an average of 16 times for
each participants and the duration of each call was an average of 25 minutes. From the studies of
Nesari et al. (2010), the telephone intervention was same as above while the duration of each call
was an average of 20 minutes. From the study of Aliha et al. (2013), the frequency of telephone call
was same as above but they did not mention about the duration of telephone call. From the study of
Taylor et al. (2003), the telephone intervention was depended on the participant’s goals, Beck

Depression Inventory and alcohol problems. 8 subsequent calls were made between 44 weeks and
the duration of each call was an average of 15 minutes. For the study of Franciosi et al. (2011),
monthly telephone call was provided.
To sum up, it is necessary to educate the diabetic knowledge and management to patients before
implementation of the nurse-led telephone follow-up intervention. Besides, the participants should
be able to perform SMBG and insulin injection in order to monitor and report their blood-glucose
reading to the nurse via the telephone follow-up.
In the control group, from the studies of Kim & Oh (2003), Oh et al. (2003), Taylor et al. (2003)
and Kim, Oh & Lee (2004), the participants were follow up by physician every 3 months. Form the
Nesari et al. (2010), participants received the 3 day diabetes education program plus physician
follow-up every 3 months. From the study of Aliha et al. (2013), participants were received routine
care and usual diabetic education. From the study of Franciosi et al. (2011), participants were
received education session that stressed on diet and lifestyle modification, and follow-up visits
every 3 months.
All of these studies include measurement and study on HbA1c level. Some studies (Kim & Oh,
2003, Nesari et al., 2010) also measured the adherence of lifestyle modification such as diet,
exercise, blood-glucose testing and self-insulin injection and medication taking. Some studies (Oh
et al., 2003, Aliha et al., 2013, Kim, Oh & Lee, 2004) measured the 2-hour postprandial glucose
level. Three studies (Taylor et al., 2003, Kim, Oh & Lee, 2004, Franciosi et al., 2011) measured the
blood pressure and cholesterol levels.
Summarize methodological issues
The methodological issues summary will be illustrated by SIGN checklist. All of the seven

identified studies were clearly stated that how the nurse telephone follow-up intervention affect the
outcome of glycaemic control.
Randomization was included in all studies. Different randomization methods such as by toss of a
coin (Kim & Oh, 2003, Oh et al., 2003, Nesari et al., 2010), by a random number table (Kim, Oh &
Lee, 2004) or by the basis of random permuted block computer-generated randomization tables
(Franciosi et al., 2011) were also clearly stated in some studies. All of the seven studies did not
mention their concealment method and only Taylor et al. (2003) has mentioned blinding test was
used in the studies.
All of the studies described the intervention components clearly in order to compare to the control
group. Therefore, the only difference between groups was due to intervention treatments.
The main outcome measure of HbA1c level was determined by a high-performance liquid
chromatography technique using the Variant II (Bio-Rad, Hercules, CA, USA). Therefore, a
standard, valid and reliable way of outcome measures was maintained.
The dropout rates all the studies were mentioned except the study of Aliha et al. (2013). The
dropout rate varied from 0% to 25% in the intervention group, and 3.2% to 36% in the control
group. The reasons of dropping out included missing of participants before completing the test,
moved to other area, change their mind to refuse to continue the test or death.
Overall, the results of quality assessment and level of evidence of the studies were shown in
Appendix E. And, all studies were rated as 1+ only as one to two items were not achieved from the
SIGN checklist (Appendix D).

2.3 Summary and Synthesis
All of the seven identified studies showed that the nurse-led telephone follow-up had an
improvement on glycaemic control as evidenced by lowering the HbA1c level. The decrease in
HbA1c level was varied from -1.14% to -1.86% in the intervention group compared to -1% to 0.6%
in the control group form the identified studies.
From the study of Kim & Oh (2003), Oh et al. (2003), and Kim, Oh & Lee (2004), they all provided
a diabetic care booklet as diabetic knowledge education and management to participant prior the
telephone follow-up intervention. From the study of Nesari et al. (2010), Aliha et al. (2013) and
Franciosi et al. (2011), the diabetic self-education program were provided before the telephone
intervention. From the study of Taylor et al. (2003), they also provided an individual counseling by
a registered nurse and group education class before the telephone intervention. Although different
program or education sessions were provided from different studies, the contents of the program or
sessions were more or less the same.
Besides, the study of Kim & Oh (2003) showed that the nurse-led telephone intervention had a good
impact on diet and SMBG adherence. Study of Nesari et al. (2010) showed that the nurse-led
telephone follow-up had a good impact on improving the level of diabetic diet adherence, physical
exercise, SMBG, medication-taking and foot care. From the study of Franciosi et al. (2011), the
results showed that the nurse-led telephone intervention had a positive effect in controlling body
weight and waist circumference. From the study of Taylor et al. (2003), it showed that the
intervention had impact on lowering the cholesterol level. From the study of Kim, Oh & Lee
(2004), the result showed that the satisfaction with the care was improved.
Study of Nesari et al. (2010) showed that nurse-led telephone follow-up significantly improved the
level of drug compliance. However, the medication regime adherence in other studies (Kim & Oh,

2003) was not shown improvement. There maybe due to medication adherence level in both
intervention and control group in study of Kim & Oh (2003) was in a high proportion to the total
score, therefore significant change was difficult to detect. Besides, the score of the adherence to
exercise was in the low side in both intervention and control groups before the treatment, this is
quite agreed with the finding by Kim & Oh (2003) that lower adherence to diet and exercise aspects
was observed. Therefore, more effort is needed to initiate the lifestyle changes in exercise and diet
aspects.
From the study of Kim, Oh & Lee (2004), the result showed that the satisfaction with the nurse care
was improved after the intervention. Therefore, it is confirmed that the use of nurse-led telephone
follow-up showed a positive impact on improving patients’ satisfaction. However, this study had no
significant impact on cholesterol level while compare to the study of Taylor et al. (2003). It may
due to the 12 weeks intervention period in the study of Kim, Oh & Lee (2003) was too short in
comparing to 1 year intervention period in Taylor et al. (2003) study.
There were some limitations in the studies. Most of the studies participants were recruited from the
outpatient department, diabetes society or medical centre. They are not suitable to represent the
society as a whole due to their limited sample size.
With reference to the above studies, some evidence-based recommendations are made to the target
and the innovation group.
Evidence-based recommendations in target group
Diabetes is a chronic disease requiring lifelong treatment and lifestyle modification. The non-
adherence to treatment regime is the common cause resulted in poor glycaemic control (Toljamo &
Hentinen, 2001). There was a discrepancy between the knowledge and actions in diabetic patients

(Chan & Molassiotis, 1999). Non-compliance to diabetic diet is the major self-care problem
(Glasgow & Anderson, 1999) than the self-medication in diabetic patients (Chan & Molassiotis,
1999). Therefore, it recommends that an intervention should be implemented to improve the non-
adherence to treatment regime especially to the diabetic diet in diabetic patients.
Evidence-based recommendations in intervention group
Poor control in diabetes may result in complication to renal, eye and cardiovascular system. The
lifestyle change and health behavior adherence are the burden to diabetic patients (Cox & Gonder-
Frederick, 1992). In order to increase the adherence rate in treatment regime, heath care providers
should empower patients to change the lifestyle and provide psychosocial support to them (Glasgow
& Anderson, 1999). Therefore, it recommends that healthcare provider should empower and
provide psychosocial support to patients to make lifestyle modification and adherence to the
treatment regime in order to reduce the complication.
Besides, increase patients participation into treatment planning and provide a continue follow-up
are importance in improving health lifestyle adherence (Norris et al. 2002). The nurse-led
telephones follow up act as an alternative method for transferring the diabetic managements into
patients’ home (Aubert et al., 1998). Therefore, it recommends that a nurse-led telephone follow-up
should be implemented to increase patients participation into treatment planning and provide a
continue follow-up into patients’ home.
All in all, the nurse-led telephone follow-up intervention plays an important role in the decrease
HbA1c level by reinforcing and monitoring the adherence to diabetic treatment regime to patients.
The result of the above studies can be generalized to the Hong Kong healthcare setting since most
of the situations from the selected studies are similar to Hong Kong situation. Besides, the
Department of Health and the Hospital Authority should collaborate with each other to implement

the nurse-led telephone follow-up to improve and support glycaemic control to all the Hong Kong
citizens. The healthcare providers should play more effort to promote the lifestyle behavior
adherence especially the diet and exercise aspects. Besides, provision of sponsorship to the
healthcare providers for participation of diabetic management training can be adopted as incentive
to promote glycaemic control.

Chapter 3: Translation and Application
The nurse telephone follow-up service showed to be effective in glycaemic control in Type 2
diabetic patients (Kim & Oh, 2003; Oh et al, 2003; Nesari et al, 2010; Taylor et al, 2003; Kim, Oh
& Lee, 2004; Franciosi et al., 2011; Aliha et al, 2013). It provides an alternate route for nurses to
monitor patient’s blood glucose level, reinforce healthy lifestyle, review drug compliance and
medication adjustment, thereby optimizing the blood glucose level and reducing the risk of
complications by increase the adherence to the diabetes control recommendations. In this chapter,
the implementation potential and the evidence-based guideline of the nurse telephone follow-up
service in diabetes nurse clinic of the Hospital Authority in Hong Kong will be examined and
developed.
3.1 Implementation potential
Diabetes management requires life-long lifestyle modification and adherence to medication and
treatment regime. In Hong Kong, patients with diabetes have to visit doctors, endocrinologists and
diabetes nurses for follow-up frequently in order to manage and monitor their progress. In diabetes
nurse clinic, patients learn about the nature of diabetes and its complications, importance of meal
planning, smoking cessation, weight control, regular exercise and complication screening. Patients
normally receive medication, relative knowledge on diabetes and methods to manage the disease
through regular meeting with doctors or nurses. Even though patents are having regular follow-up
on their disease, glycaemic control is still unsatisfactory and the admission rate to the hospital due
to poor glycaemic control is not uncommon. It is necessary to implement the nurse telephone
follow-up service to improve the glycaemic control in Type 2 diabetic patients.
Target audience
The target audiences are Type 2 diabetic patients who are under care and follow-up by the Hospital
Authority. They are being treated by oral hypoglycaemic agents (OHA) and/ or insulin therapy and

their HbA1c level are higher than 7%. The target audiences will be recruited from the outpatient
clinics or diabetes nurse clinics during their follow-up visits.
Transferability of the finding
To assess the transferability of the nurse telephone follow-up service, it is necessary to compare the
setting, target population and philosophy of care of the current healthcare setting with the previous
seven reviewed studies.
Setting
The settings of the reviewed studies were outpatient departments, diabetes clinics or medical
centers, and the setting of the proposed innovation will be the diabetes nurse clinic. As all the
settings of the reviewed studies and the proposed innovation are outpatient clinics, and all the
purpose of the reviewed studies and the proposed innovation are to achieve optimal glycaemic
control, therefore, it is reasonably to believe that there is no significant difference among them.
Patients learnt about the nature of disease, meal planning, exercise, drug therapy, signs and
symptoms of hypoglycaemia and hyperglycaemia and its management from diabetic care booklet
(Kim & Oh, 2003 and Oh et al., 2003) or education sessions (Nesari et al., 2010, Franciosi et al.,
2011 and Aliha et al., 2013). Patients will then have follow-up by nurse telephone calls. In Hong
Kong, patients leant about diabetic care through structured education including individual meetings,
education sessions and information pamphlets in diabetes nurse clinics or outpatient clinics. Patients
will then follow-up by diabetes nurse telephone calls instead of face-to-face diabetes nurse clinic
visits. Although there were some differences in the education strategies among the reviewed studies
and the current practice, all of the education contents were similar and were all prepared or
provided by Nurse Consultant (NC), Advanced Practice Nurses (APNs) and Registered Nurses
(RNs), who are specialized in diabetic care.

Target population
The target populations of the seven reviewed studies were patients who suffered from Type 2
diabetes with HbA1c level > 7%. Similarly, patients who referred to diabetes nurse clinic usually
have suboptimal glycaemic control including those patients with HbA1c level > 7%.
Some participants in the reviewed studies were having insulin therapy (Kim & Oh, 2003; Oh, Kim
and Yoon, 2003; Kim, Oh & Lee, 2004) while some participants were taking OHA only (Nesari et
al, 2010 and Franciosi et al, 2011). Although there were differences between patient characteristics
of the seven reviewed studies, the overall characteristics of the participants in the reviewed studies
are similar to Hong Kong situation. Most of the Type 2 diabetic patients in Hong Kong are having
insulin injection or taking OHA. They acquire the knowledge of diabetes, HBGM, insulin injection
technique in diabetes nurse clinic.
Philosophy of care
“Helping people stay healthy” is the mission of Hospital Authority (2014). It states that healthcare
professionals play an important role in supporting patients health. Healthcare professionals not only
saving patients’ life, but also empower patients to regain their health and stay healthy by offering
patients support and empowerment.
The proposed nurse telephone follow-up service in glycaemic control is in a close connection to
help people stay healthy. The nurse telephone follow-up services empower patients to regain their
health by providing them knowledge and skills. It also support and encourage patients in drug
compliance, meal planning and regular exercise.
Benefiting sufficient clients

Patients who suffer from Type 2 diabetes with HbA1c level > 7% and receive care from the
Hospital Authority can be benefit from the proposed innovation. The proposed innovation will be
conducted in a regional diabetes nurse clinic of acute hospital in Hong Kong. According to the
statistics of the designated diabetes nurse clinic, in the past years, there were about 5000 patients
per year requiring medical follow-up on glycaemic control (Hospital Authority, 2014). Therefore,
an estimation of around 5000 patients can be benefit from this innovation per year. And for the pilot
program, only 1000 participants will be recruited.
Time for implementation and evaluation
The nurse telephone support service will take 22 months to implement. This innovation includes
four phases that are preparation phase, implementation of intervention phase, data collection phase,
and result analysis and dissemination phase.
Preparation phase will take around eight months. Proposal preparation and application of approval
of the program will be carried out in this phase. And some adjustments will be made during the
preparation phase to improve the feasibility of the innovation. Implementation of intervention
phases will be then carried out in the next six months. Diabetes education sessions and disease
control recommendations will be provide to participants at diabetes nurse clinic in the first two
months of this phase. Besides, baseline HbA1c level of the participants will then be obtained. For
the following three months, diabetes nurse will follow up participants through telephone regularly
to reinforce the importance of treatment adherence and medication adjustments will be made if
necessary. Post intervention HbA1c level will be collected in the following one month after the
intervention. Finally, result analysis and dissemination phase will takes around five months. Data
analysis, evaluation and report preparation will be done in this phase. The details refer to Appendix
F.

Feasibility
To facilitate the implementation of the nurse telephone support service in glycaemic control, some
barriers and difficulties from organization, administrators and frontline staff should be overcome.
Nurse’s autonomy
According to the guidelines for specialty nursing service of diabetes care (Hospital Authority,
2010), diabetes nurses empower patients with knowledge and skills to make informed choices
concerning their diabetic management, and support them emotionally. Besides, diabetes nurse
facilitate behavioral changes in diabetic patients and promote a healthy life-style through education
to enhance quality of life. As diabetes nurse facilitate behavioral changes and promote a healthy
life-style in patients, it is necessary to implement the proposed innovation so as to provide an
alternate route for them to exercise their judgment and make decision under their knowledge and
skills when counseling and educating the patients.
Interference with current staff functions
In order to avoid and minimize the interference with the current staff functions, the orientation and
training program of the innovation will be provided to the involved diabetes nurses during the
Saturday afternoon or Sunday after the office hour. Therefore, it can avoid making disturbance to
the normal function of the services and the manpower.
All diabetes nurses in the diabetes nurse clinic will be involved in this innovation. Three diabetes
nurses will be assigned to perform the telephone follow-up to patients. All the diabetes nurses are
well trained. They all well equip with diabetes management, knowledge and counseling technique.
Therefore, implementation of the innovation will not cause any disturbance to the current staff.
Administration support and organization climate

Hospital Authority mission is to empower patients to stay healthy by providing them support and
encouragement in the disease treatments and care. Diabetes nurses help patients and their partners
to achieve optimal glycaemic control and improve their quality of life by manage the skills of
lifestyle modification and prevent diabetic complication (Hospital Authority, 2010). The nurse
telephone support follow-up is in line with the Hospital Authority mission and the diabetes nurses
works. Besides, all nurse in diabetes clinic have supported and received specialty training in
diabetes care and management to enhance and their competence in diabetes care.
Consensus among administrators and staff
Before implementation of the innovation, it is necessary to get consensus among administrators and
staff. Administrators may concern and worry about the extra cost and manpower of the new
innovation implementation. They may be worried about any risk and disadvantage of the innovation
to patients and staff. The nursing staff may concern about the increased workload, shortage of
manpower and time constraints. In order to minimize the concerns and worries, one designated
APN in diabetes center will be assigned to be in-charge in this proposed innovation. The APN will
then work with the professionalism bodies in diabetes care at regional academic institution in
working out the protocol and contents of the innovation. Besides, administrators and frontline staff
will be invited to give comments on the protocol and contents of the innovation. Monthly meeting
and review between administrators and frontline staff will be held to facilitate communication in
order to improve the quality of service.
Support and cooperation with other department
To gain the support and cooperation with endocrinologists are importance in implementation of this
innovation. Adjustment of the insulin or mediation is the part of the job of diabetes nurses in the
telephone support follow-up service. By having weekly meeting with endocrinologists to assess and
review the dosage of insulin and medication adjusted by diabetes nurses is the way to maintain

better and quality decision outcome. Besides, it also can increase the confidence and gain the
support from the endocrinologists to the proposed innovation.
Skills needed to carry out the innovation
The skills of diabetes care, management and counseling are all available as these are all daily jobs
of diabetes nurse in nurse clinic. All the diabetes nurses are familiar and confidence in diabetes
counseling and education. In the past, endocrinologists did all referrals to diabetes nurses clinic for
education or management. But, now the nurse telephone follow-up is governed by the protocol.
Diabetes nurses have autonomy to decide the education and counseling content according to
patients needs. To provide quality service, nurses need to acquire up-to-date knowledge by
attending seminars and lessons.
Equipment and facilities
Most of the equipment and facilities such as information leaflets, education videos, meeting rooms,
stationaries and furniture are available in the diabetes nurse clinic. However, the clinic needs to
apply extra installation of telephone lines for implementation of the innovation.
Staff training
As mentioned before, the orientation and training sessions will be held during the Saturday
afternoon or Sunday. The orientation session will be arranged to nursing and medical staffs to
introduce the innovation and explain the rationale of implementation of this innovation. Three
subsequence refreshment-training sessions will be arranged to diabetes nurses to refresh their
knowledge and counseling skills and to reinforce the staff to follow the guidelines.
Clinical evaluation
In order to assess the proposed innovation success or not, evaluation of the innovation must be
needed. The outcome measurement will focus on the changes in HbA1c level after the nurse
telephone follow-up. The laboratory in a localized hospital under Hospital Authority will provide
the HbA1c level checking.
Cost-benefit ratio of the innovation
Potential risks
In face-to face follow-up, any suspicious blood glucose reporting can be verified by a blood sample
for glucose level checking. Besides, SMBG skills and self-insulin injection techniques can all be
reviewed and assessed during the face-to face follow-up. However, in phone interview, these cannot
be done and there will be the risks in this. Telephone follow-up depends on patients’ own
assessment and reports, thus patients’ creditability are very importance.
Potential benefits
The benefits of nurse telephone follow-up service in glycaemic control for Type 2 diabetes patients
are well acknowledged. Nurse telephone support follow-up in glycaemic control has been shown to
be effective in decrease HbA1c level in real-life situations in different countries (Kim & Oh, 2003,
Oh et al., 2003, Nesari et al., 2010, Taylor et al., 2003, Kim, Oh & Lee, 2004, Franciosi et al., 2011
and Aliha et al., 2013). Participants seem to have greater adherence to diet control and blood
glucose monitoring and medication treatments (Kim & Oh, 2003, Nesari et al., 2010 and Aliha et
al., 2013). Continuous support and counseling can empower and strengthen patient’s confidence in
decision-making. Patients and health care professionals will also gain benefits form the innovation.
Since, the glycaemic education and promotion will be run more effectively in the nurse clinic. More
patients can achieve the optimal glycaemic control and the complication risks will also decrease.
Finally, the patients require hospitalizations due to poor glycaemic control will decrease.

Risk of maintaining current practice
The risks of continue current practice means exposing diabetic patients to suboptimal glycaemic
control and resulted in increasing risk of complications. As mentioned before, studies consistently
showed that patients with adequate control of blood glucose level could prevent or delay the
complications of diabetes. Stratton et al. (2000) proved that for every 1% reduction in HbA1c level
could have an associated reduction in the risk of deaths, risk of suffering form myocardial infarction
and risk of suffering from microvascular complications respectively by 21%, 14% and 37%. With
the increasing evidences and advantages to support the nurse telephone follow-up innovation in
effective glycaemic control, the nurse telephone follow-up service will become popular in patients
care. The Hospital Authority should pay more resources to implement this innovation.
Material costs of implementing innovation
Set-up cost
Application of installation of telephone lines will be the set-up cost of the nurse telephone support
service. For other parts of necessary materials such as holding orientation program, furniture and
extra rooms for providing the postposed service, all are available in the nurse-led clinic.
Operational cost
The operation cost of implementing innovation will include telephone service maintenance and
repair of telephone service, staff training, salaries of extra manpower, additional furniture, extra
brochures and pamphlets, and stationeries refill. The details of cost of implementing innovation
refer to Appendix G.
Costs to benefit ratio
A preliminary cost breakdown was proposed in this study for establishment of nurse telephone
follow-up service. Details on setup & operation costs for necessary resources can be referred to

Appendix G. The estimated establishment cost for nurse telephone follow-up service was then
compared with the normal medical cost as shown below.
-The total cost of implementing the postposed innovation is:
$10400 + $1266250= $1276650
i.e. The estimated set-up costs of implementing innovation for 1000 patients together with the
estimated operational costs implementing innovation for 1000 patients
-The cost of implementing the postposed innovation per clients:
$1276650/1000= ~$1277
According to the cost of Type 2 diabetes in Hong Kong Chinese study (Chan et al., 2007):
-Annual total direct medical cost per patient: $ 11638
-Expenditure in a diabetic patient suffers from both microvascular and macrovascular
complications: 1.3 fold higher than in patients without complication
$11638 x 1.3= $15129.4
If the postposed innovation successfully implemented, it can risk the risk of the diabetes related
complications.
-The cost to benefit ratio of implementing the postposed innovation:
$15129.4 / ($11683+ $1277) = ~ 1.17
This shows that the nurse telephone support follow-up in glycaemic control is cost effective.
Costs associated with the convention care

Increasing healthcare cost and expenditure will be needed if continue the convention practice. Poor
glycaemic control resulted in increasing risk of complications. Thus, diabetic related complications
including diabetic retinopathy, neuropathy and nephropathy will cost inevitably increase in
expenditure and heavier burden to the healthcare system.
Potential nonmaterial costs and benefits of implementing the innovation
Evaluation and data analysis, low staff morale due to extra workload, time constraint and poor
recognition from the public are the potential nonmaterial costs of implementing the innovation.
Thus, the staff turnover rate, absenteeism and the conflicts between frontline staff and
administrators will increase.
Increase nurses’ autonomy, jobs satisfaction, and patient’s satisfaction are the potential benefits of
implementing the innovation. The nurse telephone support follow-up provides a chance for nurses
to make own judgment based on their knowledge and patient’s needs. Thus, increase job
satisfaction and autonomy from nurses. Through implementing the nurse telephone support follow-
up service, the readmission rate due to poor glycaemic control may reduce. It also helps patients to
achieve optimal blood glucose control and improve their quality of life.
3.2 Evidence-based guideline
The nurse support telephone follow-up service provides a chance to diabetes nurse to assist patients
in applying the knowledge and skills learned to day-to-day self-care practice. It also educates and
empowers patients to have better lifestyle modification and diabetic management. An evidence-
based guideline of the nurse telephone support service will be made based on the findings of
previous reviewed studies (Appendix H).
Recommendations and evidence

The recommendations of the evidence-based guideline are based on findings from previous studies
conducted by different academics/ professional bodies (Kim & Oh, 2003; Oh et al., 2003; Nesari et
al., 2010; Taylor et al., 2003; Kim, Oh & Lee, 2004; Franciosi et al., 2011; Aliha et al, 2013). Total
seven recommendations of guideline (Appendix H) based on the Grade of Recommendation of
Scottish Intercollegiate Guideline Network (SIGN) (Appendix I) are developed.

Chapter 4: Plan for implementation and evaluating the innovation
Implementation plan together with communication plan and pilot testing will be illustrated and
discussed in this Chapter. Effective communication plan, stakeholders and communication process
with potential users will be worked out. Pilot testing will be implemented as a preliminary trial of
the proposed innovation to try out the guidelines before implementing the innovation in other
clinical units. At last, the evaluation plan that evaluates the effectiveness of the proposed innovation
will be discussed.
4.1 Communication plan
Identification of stakeholders
The stakeholders play an important role to make the implementation of the proposed innovation to
be succeeded or failed as they can support, facilitate, hinder or oppose the implementation of the
innovation. Therefore, identify the relevant stakeholders of the proposed innovation and gain their
support are important in implementing the proposed innovation.
In this proposed innovation, the relevant stakeholders are the service providers and the service
users. The service providers include Chief of Service (COS) and Department Operational Manager
(DOM) of Medicine Department, General Manager (Nursing) (GMN), Physicians of Metabolism
and Endocrine service, NC, and diabetes nurses in the diabetes center such as Nurse Officers (NOs),
APN and RNs. The service users are patients with Type 2 diabetes who attend the diabetes clinic.
The administrators including COS and DOM of Medicine Department, GMN, Physicians of
Metabolism and Endocrine service and NC are responsible for decision-making, budgeting and
managing of manpower and resources in clinical services. It is important to gain their approval and
support before implementation of new proposal. The main service providers that support and
implement the proposed innovation are the diabetes nurses in the diabetes center. The designated

APN in diabetes center will be chosen to take the lead of the implementing the proposed innovation.
She will work with the professionalism bodies in diabetes care at regional academic institution in
working out the protocol and contents of the innovation. She will also take part in the orientation
program of the proposed innovation.
Communication process with the potential users
The communication processes with the potential users divide into three parties that include
administrators, frontline diabetes nurses and the service users. In order to maximize the
supportability among the there parties, a mutual relationship with two-way communications should
be established in the communication process.
Communication with the administrators
Prior to implementation of communication process with the administrators, a comprehensive and
integrated search and review of relevant information and studies about nurse telephone follow-up
service should be conducted. Based on gathered information from available statistic in literatures,
transferability, feasibility, potential benefits, risks and possible barriers for implementation of
nurse-led telephone follow-up service will be identified. After detailed review/study, necessary
changes on current practice shall be proposed. Besides, a budget planning including potential
benefits, risks and cost-benefit ratio of the proposed innovation will be prepared and submitted to
the DOM and NC. The proposal and budget planning will present separately to the administrators
including DOM of Medicine Department and NC by the APN in-charge to introduce the purpose
and service provided of the proposed innovation in a formal meeting. The purpose of increasing
adherence to diabetes control recommendations to improve the HbA1c level will be discussed. The
APN in-charge acts as the leader and the communication person to bridge with the NC and DOM in
the communication process. Further meeting and discussion sessions will be held to obtain further

suggestions and improvements of the proposed innovation. Adjustments and modifications of the
services will be made afterwards.
After obtaining support and approval of the proposed innovation from the DOM and NC, the
innovation will then be introduced to COS of Medicine Department, GMN and physicians of
Metabolism and Endocrine service through the presentation and discussion in the department
meeting in order to obtain the support and budgeting. Consensus among different administrative
parties will then be obtained after the series discussions and meetings. After consensuses from
different administrative parties were obtained, a working group including 1 endocrinologist, 1 APN
and 3 diabetes RNs in diabetes center will be formed to work as a connection with other frontline
staffs. The APN in-charge will take part as the leader in the working group to introduce the
proposed innovation to all diabetes nurses and physicians in diabetes center.
Communication with the frontline diabetes nurses
The APN in-charge will hold the orientation program and meetings to introduce and explain the
proposed innovation to all the staff in diabetes clinic. The success of implementation of innovative
idea is relied on the participating of frontline diabetes nurses. Therefore, active participation of the
frontline diabetes nurses is important. Maintaining effective communication by two-way
communications, active listening, open discussion and sharing should be established in the
communication process. By introducing previous successful cases to frontline nurses shall
definitely increase their interests and determination to initiate the changes. Besides, weekly sharing
meetings will be held to obtain the feedbacks and comments of difficulties in implementing the
proposed innovation.
Communication with the service users

Posters and leaflets with the information and details of the diabetes nurse telephone follow-up
services and its benefits will be distributed to the target patients in the diabetes clinic. Comments
from the users will be obtained through patients’ interview during their follow-up visits.
Initiate the change
In order to facilitate the implementation of the proposed innovation, the working group that is led
by the APN in-charge will initiate the change. The current face-to-face follow up and the evidence
form the seven reviewed studies about the innovation will be discusses in focus group meetings.
The pros and cons of the innovation will also be thoroughly discussed. The needs and important of
change will be introduced, explained and supported by statistic mentioned before. Posters and
website introducing the innovation will also be made.
Guiding of change
A pilot testing will be carried out after the orientation program. The members of the working group
will act as the role models to the frontline diabetes nurses in implementing the evidence-based
guideline of the proposed innovation. Besides, the members of the working group will provide
ongoing clinical guidance and support to the frontline diabetes nurses in order to cultivate the
positive attitude towards the proposed innovation. Moreover, a pocket guide will be distributed to
the frontline diabetes nurses and the updated resource manual will be kept in the clinic as an
additional support for the staff. Feedback and opinions from the frontline diabetes nurses will be
obtained and reviewed from regular meetings. Further, a platform shall be established to allow
nurses to share their experience and new method in different case management via nurse-led
telephone service.
Sustaining the change

To sustain the change, monthly regular meeting will be held to obtain frontline diabetes nurses’
feedback. Sharing success stories to the staff to build up and enhance their confidence in the
proposed innovation. Performing compliance audit to nursing staff by designated APN in order to
assess nurses’ level of understanding and compliance with the new guideline. Monitoring patients’
HbA1c level are also the main methods to sustain the innovation. Besides, the new guideline will be
reviewed and updated if necessary based on evidence collected.
4.2 Pilot testing
Before implementing the full-scale of proposed innovation, a pilot testing will be carried out to
determine the feasibility of the innovation, prevent the unexpected difficulties and evaluate the
proposed change. Besides, the pilot test provides a chance to let the frontline staff to get familiar
with the proposed innovation and make them to get ready for change.
Objective of pilot testing
1. To assess the counseling skills of the diabetes nurses
2. To test the staff’s acceptance, confidence and their satisfaction
3. To test the feasibility and look for unexpected difficulties of the nurse telephone follow-up
services in the real clinical setting
Pilot test setting, design and sample
The pilot test will be conducted in the designated diabetes clinic. Approximately 50 patients will be
recruited during their follow-up visits. There will be 10 diabetes nurses in the diabetes clinic
participate in this pilot test. Therefore, each diabetes nurse will responsible for 5 patients and
adequate cases to practice the counseling intervention can be achieved.

The participant criteria are patients with Type 2 diabetes with HbA1c level >7%. The materials
required are extra installation of telephone lines for implementation of the innovation. Other
materials such as information leaflets, education videos, meeting rooms, stationaries and furniture
are available in the diabetes nurse clinic.
The pilot test will last for total eight months in which the preparation, implementing the innovation,
data collection and the evaluation of the pilot test will take two months, three months, one month
and two months respectively.
In the preparation of the pilot test, the APN in-charge will provide an orientation program and two
training sessions to the diabetes nurses to explain the new guideline in designated diabetes clinic.
Frontline diabetes nurses should undergo the basic counseling training to review their counseling
skills.
Pilot test evaluation
In order to test the feasibility of implementing the innovation, the APN in-charge will evaluate the
pilot test. The workflow of the nurse telephone follow-up services in the targeted diabetes clinic
will be assessed and evaluated. Any unexpected difficulties will also be discovered and tackled. The
normal functionality of the targeted diabetes clinic is maintained and not affected. Besides, the
materials such as brochures, pamphlets, leaflets and stationaries will also be assessed and recorded
to determine the enough stocks for implementation of the innovation. Technical support will be
provided in the pilot test to tackle the technical problems such as telephone service and computer
program in implementing the telephone follow-up services.
To maintain the standard of the content of nurse telephone follow-up services, the competence of
counseling skills, time management and knowledge of diabetes and its managements of the diabetes

nurses will be assessed and evaluated by competency audit by the APN in-charge (Appendix K).
Besides, monthly meeting will be held to allow an open discussion to staff to sharing their
experiences and encountered difficulties. Healthcare providers’ satisfaction and their suggestions
will be collected through a self-reported questionnaire (Appendix L). Further adjustments of the
innovation will be made.
To assess the effectiveness of the nurse telephone follow-up services in glycaemic control,
reviewing the HbA1c level and their self-care adherence (Appendix M) from the participants before
and after the innovation are important. Besides, questionnaires (Appendix J) will be distributed to
the participants after the innovation to obtain their feedback, opinions and suggestion of them.
4.3 Evaluation plan
An evaluation plan aims to assess and measure the clinical benefits and effectiveness of the
proposed innovation by collecting and analyzing the identify outcomes form patients, healthcare
providers and system.
Identifying outcomes
Patient outcomes
To assess the clinical benefits of the nurse telephone follow-up services in Type 2 diabetic patients,
HbA1c control and the level of patients’ satisfaction about the innovation will be included. The
HbA1c control will be the primary and long-term outcome of the proposed innovation. And the
level of patients’ satisfaction about the innovation will be the short-term outcome.
For the HbA1c control, the proposed innovation aims to improve the HbA1c control in Type 2
diabetic patients by increasing the adherence to diabetes control recommendations thorough nurse
telephone follow-up service in three months after the innovation. The HbA1c level and a self-report

questionnaire about the adherence to the diabetes control recommendations (Appendix M) will be
checked and distributed before the innovation and three months after the innovation.
For the outcome of the level of patients’ satisfaction about the innovation, a simple questionnaire
(Appendix J) that reflects the satisfaction of the diabetes nurses and the innovation will be
distributed to the participants after the nurse telephone follow-up services.
Healthcare provider outcomes
To assess the acceptance and compliance level of the healthcare providers, the level of healthcare
providers’ satisfaction and knowledge about the innovation will be evaluated.
For the acceptance level of healthcare providers, a self-reported questionnaire (Appendix L) that
assesses the level of satisfaction and confidence in the nurse telephone follow-up services for
glycaemic control will be distributed in the sharing meeting after the innovation process.
For the compliance level of the healthcare providers, an audit (Appendix K) for assessing the
performance in counseling technique, diabetes knowledge and the compliance of the guideline will
be held. The auditor will be the APN in-charge of this innovation and the audit will be performed
during the innovation process.
System outcomes
To assess the system effectiveness, the utilization and cost of the innovation will be evaluated. The
utilization of the services will be assessed annually. Resources including application of telephone
lines and its maintenance, brochures, pamphlets, stationeries and the evaluation forms will be
evaluated annually.

Participants’ eligibility
Patients with type 2 diabetes who are attend diabetes clinic due to poor glycaemic control with
HbA1c level >7% are eligible to participate in the services. They should be able to perform SMBG,
self-insulin injection or taking oral hypoglycaemic agents, and understand the goals, methods and
procedures of treatment. The diabetes nurses who work in diabetes clinic will responsible for the
recruitment and the screening.
Determining the number of clients to be involved
To determine the number of clients to be involved, a computer software ‘Java Applets’ was used for
power and sample size calculation. By comparing a single proportion to a known proportion with
the significant level = 0.05 and power = 80%, the estimate sample size is 139 patients. Assume the
drop out rate of 20%, the sample size will then be 170 patients.
Measurement
Patients with Type 2 diabetes who attend diabetes nurse clinic follow-up due to poor glycaemic
control will be assessed. The patients who wish to receive nurse telephone follow-up service will
then be interviewed. The HbA1c level and body mass index will be recorded and calculated. The
baseline data of self-care adherence (Appendix M) of patients will be assessed afterward. The self-
care adherence assessment includes diet, exercise, SMBG, medication and hypoglycaemia
management. Patients will then receive education session to review and update their diabetes
knowledge, SMBG and self-insulin injection techniques. Afterwards, the diabetes nurses will
provide 12 weeks of telephone follow-up to them. After the 12 weeks nurse telephone follow-up
services, the HbA1c level and the self-care adherence (Appendix M) will also be assessed again.
Besides, the level of patient satisfaction and suggestion about the innovation will be measured by a
simple questionnaire (Appendix J).

For healthcare professionals, the level of satisfaction with the innovation of healthcare professionals
will be assessed by the self-reported questionnaire (Appendix L) at the end of the implementation
period. Their knowledge, confidence, autonomy and duration of the innovation will be assessed and
suggestions will be collected. Besides, an audit on compliance with the innovation guideline
(Appendix K) will perform during the innovation implementation period.
Data analysis
For data analysis, the data will be analyzed by using the Statistical Package for the Social Sciences
(SPSS). The primary outcome of the proposed innovation is HbA1c control. The data will be
analyzed and compared by paired t test for the changes before and after the innovation. The level of
patient and healthcare professional satisfaction will be analyzed by one sample t-test by SPSS.
Basis for an effective change of practice
The proposed innovation determines to be effective based on the defined outcomes. According to
the seven reviewed studies, the HbA1c level will be decreased by at least 1% after the 12 weeks of
innovation. Patients reported to increase the adherence to diabetes treatment recommendations.
Besides, patients’ and healthcare professionals’ satisfaction are important in determining the
effectiveness of the innovation. The proposed innovation is considered to be effective if 70% of the
patients and healthcare professionals agree on the overall satisfaction level.

Chapter 5: Conclusion
To conclude, the evidence-based guideline of nurse telephone follow-up service for Type 2 diabetic
patients is effective in glycaemic control by lowering the HbA1c level. It is necessary to implement
the nurse telephone follow-up service for Type 2 diabetic patients in the healthcare setting. The
guideline is well supported and developed by various evidences from the reviewed studies. It will
be successfully implemented through the comprehensive plan which include communication plan
between the service providers and the users and pilot test. Also, a comprehensive outcome
evaluation plan is needed to assess the level of lowering HbA1c level and the satisfaction rate of the
patients and healthcare professionals with the program.

References Aliha, J.M., Asgari, M., Khayeri, K., Ramazani, M, Farajzadegan, Z. & Javaheri, J.(2013), Group education and nurse-telephone follow-up effects on blood glucose control and adherence to treatment in type 2 diabetes patients. Int J Prev Med 4(7), 797-802 American Diabetes Association (2009). Retrieved July 1, 2004 from http://www.diabetes.org/diabetes-basics/type-2/?loc=hottopics Anderson, R.M., Funnell, M.M., Butler, P.M., Arnold, M.S., Fitzgerald, J.T. & Geste, C.C. (1995), Patient empowerment. Diabetes Care 18, 943–949.
Aubert, R., Herman, W., Waters, J., Moore, W., Sutton D., Peterson, B., Bailey, C. & Koplan, J.P. (1998) Nurse case management to improve glycemic control in diabetic patients in a health main- tenance organization: a randomized, controlled trial. Annals of Internal Medicine 129, 605–612.
Boucher, J.L., Pronk, N.P. & Gehling, E.M. (2000), Telephone-based lifestyle counseling. Diabetes Spectrum 13, 190–194.
Centre for Health Protection (2013). Retrieved July 1, 2014 from http://www.chp.gov.hk/en/content/9/25/59.html Chan, B. S., Tsang, M. W., Lee, V. W. & Lee, K. K. (2007) Cost of Type 2 Diabetes mellitus in Hong Kong Chinese. Int J Clin Pharmocol Ther. 45(8):455-68. Chan, J. C. (2000). Heterogeneity of diabetes mellitus in the Hong Kong Chinese population. The Chinese University of Hong Kong-Prince of Wales Hospital Diabetes Research and Care Group. Hong Kong Med J. 6:77-84 Chan, Y.M. & Molassiotis, A. (1999), The relationship between diabetes knowledge and compliance among Chinese with non-insulin dependent diabetes mellitus in Hong Kong. Journal of Advanced Nursing 30, 431–438.
Cox, D.J. & Gonder-Frederick, L. (1992), Major developments in behavioural diabetes research. Journal of Consulting and Clinical Psychology 60, 682–638.
Franciosi, M., Lucisano, G., Pellegrini, F., Cantarello, A., Consoli, A., Cucco, L., Ghidelli, R., Sartore, G., Sciangula, L. &Nicolucci, A. (2011) ROSES: role of self-monitoring of blood glucose and intensive education in patients with type 2 diabetes not receiving insulin. A pilot randomized clinical trial. Diabetic Medicine 28, 789-796 Funnell, M.M., Tang, T.S. & Anderson, R. (2007). From DSME to DSMS: Developing empowerment-based diabetes self-management support. Diabetes Spectr, 20, 221–6. Glasgow, R.E. & Anderson, R.M. (1999) In diabetes care, moving from compliance to adherence. Diabetes Care 22, 2090–2094. Hospital Authority (2010). Guidelines for Specialty Nursing Service: Diabetes Care. (3rd edition). Hong Kong: Hospital Authority. Hospital Authority (2014). Hospital Authority: Vision, mission and values. Retrieved December 24, 2014 from http://www.ha.org.hk/visitor/ha_visitor_index.asp?Content_ID=10009&Lang=ENG&Dimension=100&Parent_ID=10004&Ver=HTML

Hospital Authority (2014). Retrieved December 24, 2014 from http://www3.ha.org.hk/qmh/department/Special%20Services/K%20K%20Leung%20Diabetes%20Centre/kkleung_main.htm Hospital Authority Head Office (2014). Guidelines for Specialty Nursing Service: Diabetes Care. (4th edition). Hong Kong: Hospital Authority. Kim, H. S. & Oh, J. A. (2003). Adherence to diabetes control recommendations: impact of nurse telephone calls. Journal of Advanced Nursing 44(3), 256-261.
Kim, H. S., Oh, J. A. & Lee, H. O. (2004). Effects of nurse-coordinated intervention on patients with type 2 diabetes in Korea. J Nurs Care Qual 20(2), 154-160 Mathers, C.D. & Loncar, D. (2006). Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med, 3(11):e442. Martinez-Castelao, A., Gorriz, J.L., Garcia-Lopez, F., Lopez-Revuelta, K., De Alvaro, F. & Cruzado, J.M. (2004). Perceived health related QOL and co morbidity in diabetic patients starting dialysis (CALVIDIA study) J Nephrol, 17,544–51. Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med 6(6): e1000097. doi:10.1371/journal.pmed1000097 Nesari, M., Zakerimoghadam, M., Rajab, A., Bassampour, S.& Faghihzadeh, S. (2010) Effect of telephone follow-up on adherence to a diabetes therapeutic regimen. Japan Journal of Nursing Science 7, 121-128. Oh, J. A., Kim, H. S., Yoon, K. H., & Choi, E. S. (2003). A Telephone-Delivered Intervention to Improve Glycemic Control in Type 2 Diabetic Patients. Yonsei Medical Journal 44(1), 1-8. SIGN (2012). The Grade of Recommendation of Scottish Intercollegiate Guideline Network. Retrieved December, 28, 2014 from http://www.sign.ac.uk/guidelines/fulltext/50/annexoldb.html Stratton, I.M., Adler, A.I., Neil, H.A., Matthews, D.R., Manley, S.E. & Cull, C.A., (2000), Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ, 321(7258), 405–412. Taylor, C. B., Cunning, D., Miller, N. H., Deeter, A, Reilly, K. R., Abascal, L., &Greenwald, G. (2003), Evaluation of a nurse-care management system to improve outcomes in patients with complicated diabetes. Diabetes Care 26, 1058-1063 Toljamo, M. & Hentinen, M. (2001), Adherence to self-care and glycaemic control among people with insulin-dependent diabetes mellitus. Journal of Advanced Nursing 34, 780–786.
Weinberger, M., Kirkman, S., Samsa, G.P., Shortliffe, E.A., Landsman, P.B., Cowper, P.A., Simel, D.L. & Feussner, J.R. (1995), A nurse- coordinated intervention for primary care patients with non- insulin-dependent diabetes mellitus: Impact on glycemic control and health-related quality of life. Journal of General Internal Medicine 10, 59–66.

WHO (1999). Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: Diagnosis and classification of diabetes mellitus. Geneva, World Health Organization, (WHO/NCD/NCS/99.2).
WHO (2012). Global status report on noncommunicable diseases 2014. Geneva, World Health Organization
WHO (2014). Global Health Estimates: Deaths by Cause, Age, Sex and Country, 2000-2012. Geneva, WHO

Appendix A: search history
CINAHL PubMed Cochrane Library
By keyword search: 1. diabetic OR diabetic mellitus OR type 2 diabetic 2. telephone OR telephone follow-up OR glycaemic control 3. adherence OR nurse
CINAHL 113 articles
PubMed 683 articles
Cochrane Library 17 articles
Reviewed by titles
65 articles s
321 articles 5 articles
Reviewed by abstracts
10 articles 18 articles 4 articles
Reviewed by full texts and reference lists
5 articles 12 articles 2 articles
Total articles for review after elimination of duplication: 7

From: Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med 6(6): e1000097.
doi:10.1371/journal.pmed1000097
Iden
tification+ Records(identified(through(
database(searching(from(CINAHL,(
PubMed(and(Cochrane(Library(
(n(=((813()(
Additional(records(identified(
through(reference(lists(
(n(=(19(()(
Screen
ing+
Records(after(duplicates(removed(
(n(=(820(()(
Records(screened(
(n(=((51()(
Records(excluded(after(
review(by(titles(and(
abstracts(
(n(=((769()(
FullOtext(articles(assessed(
for(eligibility(
(n(=(20((()(
FullOtext(articles(excluded,(
with(reasons(
(n(=((31()(
Studies(included(in(
qualitative(synthesis(
(n(=((0()(
Studies(included(in(
quantitative(synthesis(
(metaOanalysis)(
(n(=(7)(
Eligibility+
Includ
ed+

Kim, H. S. & Oh, J. A. (2003). Adherence to diabetes control recommendations: impact of nurse telephone calls. Journal of Advanced Nursing 44(3), 256-261.
Citation Study design Patient Characteristics Intervention(s) Comparison Length of follow- up
Outcome measures Effect size
Kim & Oh, 2003
South Korea
Randomized controlled trail
36 participants were recruited from the endocrinology outpatient department Diagnose with diabetes according to the ADA criteria HbA1c > 7% Able to perform blood glucose self-testing and self-injection of medication
Provide diabetic care booklet : z nature of the disease z risk factors z diet therapy z exercise z drug therapy z hypoglycemia and
hyperglycaemia management Participants needed to log blood glucose levels more than twice a day and also to keep daily diet and exercise logs 12 weeks of telephone intervention z continuing education z reinforcement of diet, exercise z medication adjustment z frequent self-monitoring of
blood glucose levels Frequency of telephone intervention: z at least twice a week for the first
month z then weekly for the second and
third month z averaged 16 times for each
individual z averaged 25 minutes for each
session (n=20)
Visiting a physician every 3 months (n=16)
12 weeks 1. HbA1c (%) 2. Self-reported adherence by six components questionnaire (VAS: ‘0=never do at all’-‘100=always do as prescribed’) (i) diet (five items) (ii) exercise (one item) (iii) blood glucose testing( four items) (iv) medication taking (two items) (v) hypoglycemia management (two items) (vi) foot care (six items) The mean for each component was calculated by: sum of component score/ number of items)
1. Intervention: -1.2 Control: 0.6 (p=0.0001) 2. (i) Intervention: 13.6 Control: 0.4 (p=0.006) (ii) Intervention: -9.7 Control: -13.6 (p=0.754) (iii) Intervention: 10.8 Control: -3.4 (p=0.024) (iv) Intervention: 16 Control: 6.8 (p=0.334) (v) Intervention: 14.6 Control: -5.7 (p=0.149) (vi) Intervention: 5.3 Control: 0.8 (p=0.362)
Appendix B: Table of evidence

Oh, J. A., Kim, H. S., Yoon, K. H., & Choi, E. S. (2003). A Telephone-Delivered Intervention to Improve Glycemic Control in Type 2 Diabetic Patients. Yonsei Medical Journal 44(1), 1-8. Citation Study design Patient characteristics Intervention(s) Comparison Length of
follow-up Outcome measures
Effect size
Oh, Kim, Yoon & Choi, 2003 South Korea
Randomized controlled trial
38 participants were recruited from the endocrinology outpatient department Participants with age range between 45-73 years Diagnose with diabetes according to the ADA criteria HbA1c > 7% Able to perform blood glucose self-testing and self-injection of medication
Provide diabetic care booklet: z nature of the disease z risk factors z diet therapy z exercise z drug therapy z hypoglycemia management z sick day management The participants were required to log blood glucose levels more than twice a day, and to keep daily diet and exercise logs. 12 weeks of telephone intervention: z continuous education z reinforcement of diet, exercise z medication adjustment z frequent self-monitoring of
blood glucose levels Frequency of telephone intervention: z at least twice a week for the first
month z then weekly for the second and
third months z total frequency of telephone
counseling averaged sixteen times per subject
(n=20)
Visiting a physician every 3 months (n=18)
12 weeks 1. HbA1c (%) 2. FBG
(mg/dl) 3. PP2h
(mg/dl) 4. BMI
(kg/m2)
1. Intervention: -1.2 (p=0.002) Control: 0.6 (p=0.005) 2. Intervention: -15.7 (p=0.193) Control: -6.9 (p=0.657) 3. Intervention: -42.6 (p= 0.114) Control: 19.6 (p=0.315) 4. Intervention: 0.3 (p=0.068) Control: 0.2 (p=0.278)

Nesari, M., Zakerimoghadam, M., Rajab, A., Bassampour, S. & Faghihzadeh, S. (2010) Effect of telephone follow-up on adherence to a diabetes therapeutic regimen. Japan Journal of Nursing Science 7, 121-128. Citation Study
design Patient characteristics
Intervention(s) Comparison Length of follow-up
Outcome measures Effect size
Nesari, Zakerimoghadam, Rajab, Bassampour & Faghihzadeh, 2010 Iran
Randomized controlled trial
61 participants who attended the Iranian Diabetes Society < 65 years of age diagnosis of type 2 diabetes HbA1c measurement of > 7 % Stable in general medical condition taking blood glucose-lowering tablets and not insulin
3 day diabetes self-care education program: z nature of diabetes z diabetic complication z risk factors z self-care skills in relation to
diet, exercise, foot care z medication-taking z hypoglycemia management z blood glucose self-
monitoring z recording the results 12 weeks of telephone follow-up: z health behaviors z diet, exercise, medication-
taking z foot care z regular monitoring of blood
glucose z answer participants’
questions Frequency of telephone intervention: z twice per week for the first
month z then weekly for the second
and third months z average of 20 min a session z received 16 phone calls for
each individual (n=30)
Same as 3 day diabetes self-care education program provided to intervention group Participants were visited by one endocrinologist every 3 months. (n=31)
12 weeks 1.HbA1c (%) 2. Self-reported questionnaire (Five-point Likert scale, the total score of each domain was the sum of the scores of the items, which was expressed out of 100.) (i) diet (ii) exercise (iii) foot care (iv) medication (v) duration of
blood glucose testing
1.Intervention: -1.86 (p<0.001) Control: -1(p=0.150) 2.(i) Intervention: 17.62 (p<0.001) Control: 5.31 (p<0.001) (ii) Intervention: 44.86 (p<0.001) Control: 8.98(p=0.070) (iii) Intervention: 21.11 (p<0.001) Control: 5.39 (p=0.080) (iv) Intervention: 28.44 (p<0.001) Control: 2.9 (p=0.360)

Aliha, J.M., Asgari, M., Khayeri, K., Ramazani, M, Farajzadegan, Z. & Javaheri, J. (2013), Group education and nurse-telephone follow-up effects on blood glucose control and adherence to treatment in type 2 diabetes patients. Int J Prev Med 4(7), 797-802 Citation Study design Patient
characteristics Intervention(s) Comparison Length of
follow-up Outcome measures Effect size
Aliha, Asgari, Khayeri, Ramazani, Farajzadegan & Javaheri, 2013 Iran
Randomized controlled clinical trial
Participants with type 2 diabetes recruited from Khomein’s diabetes clinic
Two educational session (lasting 60 min two consecutive day) z diabetes and its complications z importance and ways of self-
care in diabetes z correct insulin injection z self-monitoring blood glucose z emergent measure in
hypoglycemic z regular use of drugs z diet in diabetes z significance of exercise and
physical activity 12 weeks of telephone follow-up: z asked about adherence to diet,
drug usage, exercise, SMBG at home possible questions raised on behalf of participants
Frequency of telephone intervention: z total 16 times telephone
follow-up z two calls per week for first
four weeks z one call per week for the
remaining eight weeks z participants were followed up
for 3 months (n=31)
Conventional care and usual education for diabetic patients were provided. (n=31)
12 weeks 1. FBS 2. 2 hpp BS 3. HbA1c (%) 4. Patient’s adherence
to treatment programs questionnaires (scores classified as unfavorable, some favorable, favorable and very favorable)
1. Intervention: -38 Control: -23 (p=0.000) 2. Intervention: -66 Control: -17 (p=0.000) 3. Intervention: -1.4 Control: -0.1 (p=0.000) 4. Intervention: some favorable: 22.7 favorable: -16.2 very favorable: 3.6 Control: some favorable: -16.1 favorable: -74.2 very favorable: 90.3

Taylor, C. B., Cunning, D., Miller, N. H., Deeter, A, Reilly, K. R., Abascal, L., & Greenwald, G. (2003), Evaluation of a nurse-care management system to improve outcomes in patients with complicated diabetes. Diabetes Care 26, 1058-1063 Citation Study
design Patient characteristics
Intervention(s) Comparison
Length of follow-up
Outcome measures
Effect size
Taylor, Cunning, Miller, Deeter, Reilly, Abascal & Greenwald, 2003 California
Randomized controlled trial
169 participants were recruited from Kaiser Permanente Medical Center with longstanding diabetes HbA1c > 10% one or major medical comorbid conditions such as hypertension, dyslipidemia, or CVD
Initial individual meeting with an registered nurse: (90-min consultation) z review the participant’s medical, lifestyle, and psychosocial
status z foot exam z checked and record blood pressure and pulse z initial self-management plan was developed. Group class: 1to 2-h group class and met once a week for 4 weeks) z follow a workbook which included some diabetic material z focus was on group discussion, participation, and problem-
solving Telephone follow-up calls: z participant’s goals z medication use z symptoms z glucose monitoring z blood pressure monitoring z self-management/care activities -with a Beck Depression Inventory (BDI) score >10 were reassessed or referred for psychopharmacology therapy
-with alcohol problems were also monitored and referred
Frequency of telephone intervention: z received an initial telephone call before the fourth group
session z subsequent calls were scheduled for 5, 8, 12, 16, 20, 28, 36,
and 44 weeks into the program and were designed to average 15 min.
z additional calls were provided to participants as needed (n=84)
Under treatment of primary care physician (n=85)
One year
1. HbA1c (%) 2. Total cholesterol (mg/dl) 3. LDL cholesterol (mg/dl) 4. HDL cholesterol (mg/dl) 5. Triglycerides (mg/dl) 6. Glucose (fasting) (mg/dl) 7. Systolic blood pressure (mmHg) 8. Diastolic blood pressure (mmHg) 9. BMI (kg/m2)
1.Intervention: -1.14 Control: -0.35 (Effect size: 0.37) 2. Intervention: -20.6 Control: -11.5 (Effect size: 0.18) 3. Intervention: -19.4 Control: -6.5 (effect size: 0.33) 4. Intervention: 0.2 Control: -0.7 (Effect size: 0.07) 5. Intervention: -11.0 Control: -10.5 (Effect size:0) 6. Intervention: -25.0 Control: -13.4 (Effect size:0.16) 7. Intervention: 4.4 Control: 8.6 (Effect size:0.28) 8. Intervention: 2.2 Control: 1.9 (Effect size:0.03) 9.Intervention: 0.5 Control: -0.3 (Effect size:0.11)

Kim, H. S., Oh, J. A. & Lee, H. O. (2004) Effects of nurse-coordinated intervention on patients with type 2 diabetes in Korea. J Nurs Care Qual 20(2), 154-160 Citation Study design Patient
characteristics Intervention(s) Comparison Length of
follow-up Outcome measures Effect size
Kim, Oh & Lee, 2004 South Korea
Randomized controlled trial
25 participants recruited from the endocrinology outpatient department of a tertiary care hospital diagnosed diabetes according to the ADA criteria HbA1c > 7% able to perform blood glucose self-testing and self-injection of medication
Provide diabetic care booklet: the nature of the disease risk factors medical regimen (diet, exercise, medications) hypoglycemia management illness management 12 weeks of telephone intervention: z counseling on the importance of
maintaining blood glucose levels within a near-normal range
z continuing education z reinforcement of diet, exercise z medication adjustment z frequent self-monitoring of blood
glucose levels The participants were required to log blood glucose levels more than twice a day and also to keep daily diet and exercise logs. The frequency of telephone counseling: z at least twice a week for the first
month then weekly for the second and third month
z averaged 16 times per subject of each average of 25 minutes per each session
(n=15)
Visiting a physician every 3 months (n=10)
12 weeks 1. HbA1c (%) 2. FBG (mg/dL) 3. PP2h (mg/dL) 4. Triglycerides (mg/dL) 5. HDLC (mg/dL) 6. Care satisfaction (scores)
1. Intervention: -1.2 (p=0.011) Control: 0.5 (p=0.193) 2.Intervention: -23.2 (p=0.113) Control: -14.7 (p=0.613) 3.Intervention: -52.6 (p=0.138) Control: -1.9 (p=0.958) 4.Intervention: -1.8 (p=0.811) Control: -4.8 (p=0.767) 5.Intervention: -2.5 (p=0.450) Control: -1.7 (p=0.333) 6.Posttest: Intervention: 74.3 Control: 45.7 (p=0.023)

Franciosi, M., Lucisano, G., Pellegrini, F., Cantarello, A., Consoli, A., Cucco, L., Ghidelli, R., Sartore, G., Sciangula, L. & Nicolucci, A. (2011) ROSES: role of self-monitoring of blood glucose and intensive education in patients with type 2 diabetes not receiving insulin. A pilot randomized clinical trial. Diabetic Medicine 28, 789-796 Citation Study deign Patient
characteristics Intervention(s) Comparison Length
of follow-up
Outcome measures Effect size
Franciosi, Lucisano, Pellegrini, Cantarello, Consoli, Cucco, Ghidelli, Sartore, Sciangula, & Nicolucci, 2011 Italy
Randomized controlled trial
62 participants recruited by three diabetes outpatient clinics aged between 45 and 65 years with type 2 diabetes HbA1c values between 7% and 9% treated with oral hypoglycemic agents monotherapy with no experience of self-monitoring in the previous 12 months seen for the first time in the diabetes outpatients clinic
Face to face educational programme: (held every 3 months) z addressing how to perform
self-monitoring of blood glucose
z how to modify diet and level of physical activity according to blood glucose levels
z the actions to undertake in case of abnormal values (hypoglycaemia or hyperglycaemia)
z 12 weeks of telephone intervention: z discuss the mean fasting and
postprandial blood glucose levels with the participant following a structured interview
z the reasons for elevated values and their relationship with quality and quantity of foods and exercise
The frequency of telephone counseling: z telephone contact every month (n=46)
Standard counseling with focus on diet and lifestyle, and follow-up visits were scheduled every 3 months (n=16)
6 months 1. HbA1c (%) 2. Weight (kg) 3. BMI 4. Waist
circumference (cm) 5. Systolic blood
pressure (mmHg) 6. Diastolic blood
pressure (mmHg) 7. Total cholesterol
(mmol/l) 8. HDL cholesterol
(mmol/l) 9. Triglycerides
(mmol/l)
1. Intervention: -1.3 (95% CI -1 to -1.3) Control: -0.7 (95% CI -0.9 to -0.4) 2. Intervention: -4.5 Control: -0.5 3. Intervention: -1 Control: -0.1 4. Intervention: -4.4 Control: -1.1 5. Intervention: -4 Control: -7 6. Intervention: -3 Control: -1 7. Intervention: —0.41 Control: -4.2 8. Intervention: -0.03 Control: -0.01 9. Intervention: -2.5 Control: -0.15

_
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Guideline topic: Key Question No: Reviewer:
Before completing this checklist, consider:
1. Is the paper a randomised controlled trial or a controlled clinical trial? If in doubt, check the study design algorithm
available from SIGN and make sure you have the correct checklist. If it is a controlled clinical trial questions 1.2, 1.3,
and 1.4 are not relevant, and the study cannot be rated higher than 1+
2. Is the paper relevant to key question? Analyse using PICO (Patient or Population Intervention Comparison Outcome). IF
NO REJECT (give reason below). IF YES complete the checklist.
Reason for rejection: 1. Paper not relevant to key question ! 2. Other reason ! (please specify):
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.i
Yes !
Can’t say !
No !
1.2 The assignment of subjects to treatment groups is randomised.ii
Yes !
Can’t say !
No !
1.3 An adequate concealment method is used.iii
Yes !
Can’t say !
No !
1.4 Subjects and investigators are kept ‘blind’ about treatment allocation.iv Yes !
Can’t say !
No !
1.5 The treatment and control groups are similar at the start of the trial.v Yes !
Can’t say □
No !
1.6 The only difference between groups is the treatment under investigation.vi Yes !
Can’t say !
No !
1.7 All relevant outcomes are measured in a standard, valid and reliable way.vii Yes !
Can’t say !
No !
1.8 What percentage of the individuals or clusters recruited into each treatment arm
of the study dropped out before the study was completed?viii
Appendix C: SIGN checklist for RCTs

_
1.9 All the subjects are analysed in the groups to which they were randomly allocated
(often referred to as intention to treat analysis).ix
Yes !
Can’t say !
No !
Does not apply !
1.10 Where the study is carried out at more than one site, results are comparable for all
sites.x
Yes !
Can’t say !
No !
Does not apply !
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias?
Code as follows:xi
High quality (++)!
Acceptable (+)!
Unacceptable – reject 0 !
2.2 Taking into account clinical considerations, your
evaluation of the methodology used, and the statistical
power of the study, are you certain that the overall effect
is due to the study intervention?
2.3 Are the results of this study directly applicable to the
patient group targeted by this guideline?
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the extent to
which it answers your question and mention any areas of uncertainty raised above.
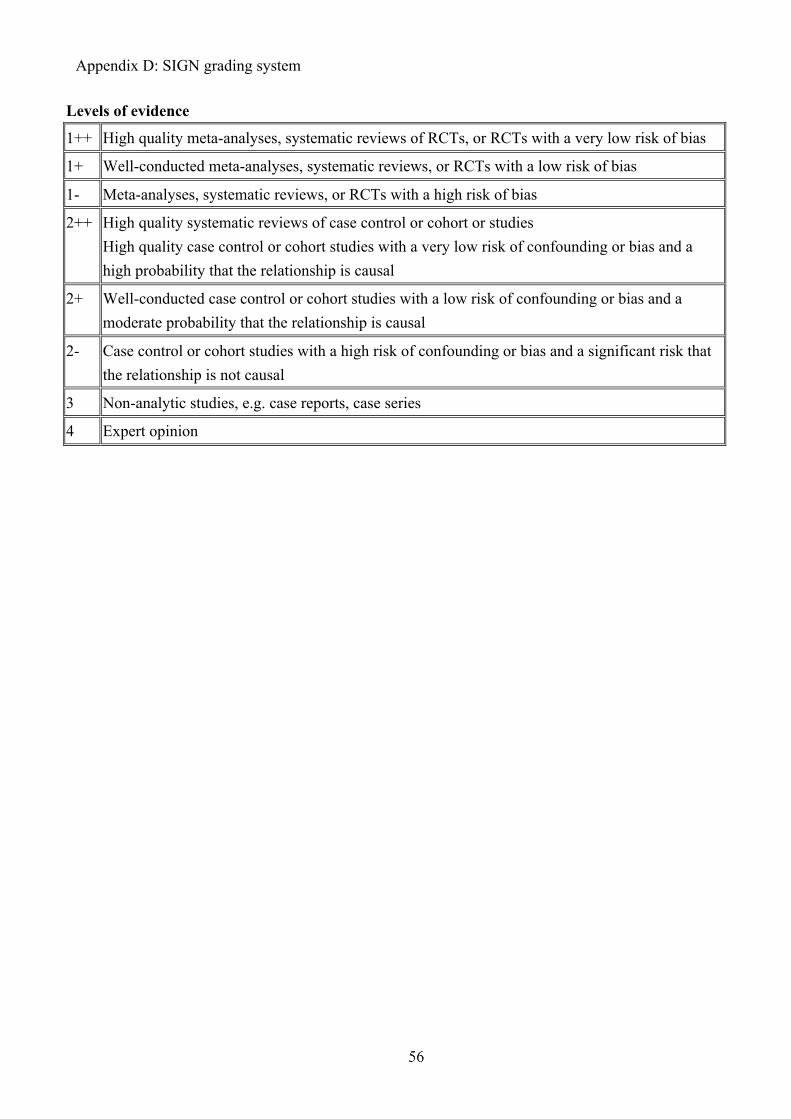
p
!
Levels of evidence
1++ High quality meta-analyses, systematic reviews of RCTs, or RCTs with a very low risk of bias
1+ Well-conducted meta-analyses, systematic reviews, or RCTs with a low risk of bias
1- Meta-analyses, systematic reviews, or RCTs with a high risk of bias
2++ High quality systematic reviews of case control or cohort or studies High quality case control or cohort studies with a very low risk of confounding or bias and a high probability that the relationship is causal
2+ Well-conducted case control or cohort studies with a low risk of confounding or bias and a moderate probability that the relationship is causal
2- Case control or cohort studies with a high risk of confounding or bias and a significant risk that the relationship is not causal
3 Non-analytic studies, e.g. case reports, case series
4 Expert opinion
!
!
!
!
Appendix D: SIGN grading system (1999-2012)

! ! !
!
RCTs
Kim et al.,
2003
Oh et al.,
2003
Nesari
et al.,
2010
Aliha et
al., 2013
Taylor et
al.,
2003
Kim et
al., 2004
Franciosi et al.,
2011
Section 1: Internal Validity
1.1 Appropriate and clearly
focused question
Yes Yes Yes Yes Yes Yes Yes
1.2 Randomization Yes (Poor
method: a
toss of a
coin)
Yes (Poor
method: a
toss of a
coin)
Yes (Poor
method: a
toss of a
coin)
Can’t say Can’t say Yes (a
random
number
table)
Yes (a basis of
random permuted
block
computer-generat
ed randomization
tables)
1.3 Concealment method No No No No No No No
1.4 Blinding Can’t say Can’t say Can’t say Can’t say Yes Can’t
say
Can’t say
1.5 Similarity between
intervention and control
group
Yes Yes Yes Yes Yes Yes Yes
1.6 Only difference in
treatment
Yes Yes Yes Yes Yes Yes Yes
1.7 Valid and reliable
outcome measures
Yes Yes Yes Yes Yes Yes Yes
1.8 Dropout rate
-Intervention:
-Control:
-20%
-36%
:-20%
-28%
-0
-3.2%
Can’t say
-20.2%
-16.5%
-25%
-33.3%
-8.7%
-6.25%
1.9 Intention to treat Yes Yes Yes Yes Yes Yes Yes
1.10 Comparable results Dose not
apply
Dose not
apply
Dose not
apply
Dose not
apply
Dose not
apply
Dose
not
apply
Dose not apply
Section 2: Overall Assessment of the Study
2.1 Minimize bias (+) (+) (+) (+) (+) (+) (+)
Appendix!E:!The!results!of!quality!assessment!and!level!of!evidence!of!the!studies!

Timeframe (Month)
1 2 3 4 5 6 7 8 9 1
0
1
1
1
2
1
3
1
4
1
5
1
6
1
7
1
8
1
9
2
0
2
1
2
2
2
3
Communication with stakeholders * *
Proposal preparation and application for approval * * *
Initiating the change (Introduce, explain the innovation to staffs) * *
Guiding of change * * * *
Pilot test
Preparation * *
Data collection *
Implementation * * *
Data collection *
Evaluation * *
Sustaining the change (Amendment on guideline and evaluation
plan)
* * * * *
Full-scale
implementation
Preparation (Training workshop for staffs) * * * * *
Diabetes education provide to participants * *
Data collection *
Implementation (12 weeks Nurse telephone
follow-up)
* * *
Data collection *
Data analysis and dissemination * * * * *
Appendix F: Time for implementation and evaluation

! !
!
Estimated set-up costs of implementing innovation for 1000 patients
Details Cost
Application of telephone
line
Three extra telephone
lines
$ 300 @ x 3= $900
Orientation program Introduce the innovation 2 hours @ x 20 nurses=40
hours
($187.5 x 40= $ 7500)
Furniture Tables and chairs $2000
Extra rooms Available in clinic -
Total $10400
Estimated operational costs of implementing innovation for 1000 patients
Cost
Telephone service
maintenance and repair
Maintenance and repair of
telephone service per year
$2000
Staff training Renew the diabetes
management and
knowledge
3 hours x 20 nurses= 60
hours
($ 187.5 x 60= $11250)
Telephone follow-up Diabetes nurses follow-up 25 mins x 16 times x 1000
patients = 400000 mins
($187.5 x 400000/60=
$1250000)
Brochures and pamphlets Diabetes management and
care
$3000
Stationeries Available in clinic -
Total $ 1266250
*Mid-point hourly salary of registered nurse $187.5
Appendix G: Cost of implementing innovation

! !
Title
An evidence-based guideline of nurse telephone follow-up service in glycaemic
control for Type 2 diabetic patients
Objectives
1. To educate and support the Type 2 diabetic patients by telephone follow-up
2. To reinforce the adherence of treatment regime and lifestyle modification
3. To provide medication adjustment according to individual patient’s condition
4. To reduce the risk of diabetic related complications for patients
Intended users
Intended users are trained nurses working in diabetes nurse-led clinic.
Target population
The target population is Type 2 diabetic patients with HbA1c level >7
Setting
The innovation will be implemented in local diabetes nurse-led clinic
Interventions
The interventions include the diabetes knowledge education and counseling,
treatments and regimens reinforcement and medications adjustments through
telephone calls by diabetes nurse.
Recommendations of guideline:
1. Patients with suboptimal glycaemic control should be provided nurse
telephone support follow-up service by diabetes nurses. (Grade A)
A telephone intervention by a nurse could improve HbA1c in patients with Type 2
diabetes mellitus and the HbA1c decreased 1.2 percentage points in the
intervention group after 12 weeks (Kim & Oh, 2003) (1+), (Oh et al., 2003) (1+).
Appendix H: Evidence-based guideline

! !
2. Patients should have basic knowledge of the disease, understand the signs
and symptoms of hypoglycaemia and hyperglycaemia and its managements,
learn SMBG and self–insulin injection technique if necessary through two
educational session lasting 60 minutes in two consecutive days and booklet
before recruit to innovation (Grade A).
Each participant was educated about the nature of the disease, risk factors, diet,
exercise, drug therapy, hypoglycaemia and hyperglycaemia management, and how
to record a daily log through a booklet (Kim & Oh, 2003) (1+), (Oh et al., 2003).
All the participants attended a 3 days diabetes self-care education program before
the innovation (Nesari et al., 2010) (1+).
Patients received 1 day education session addressing the basic knowledge of
diabetes and SMBG before the initiation of the innovation (Franciosi et al., 2011).
Two educational session lasting 60 minutes in two consecutive days about
diabetes nature and its complications, insulin injection technique, SMBG and
hypoglycaemia and hyperglycaemia management were provided to participants
before the initiation of the innovation (Aliha et al., 2013).
3. Diabetes nurses should provide health education on diabetic care and
reinforcement of diabetic regime to patients during the nurse telephone
follow-up. The contents should include the following:
! Education of diabetic care
! Reinforcement of diet and exercise
! Medication adjustment recommendations (Grade A)
Participants’ daily food intakes were analyzed and recommendations were made
for appropriate diabetic dietary control according to their diet and exercise
patterns. Medications adjustments were made after reviewing the blood glucose

! !
log and the results were discussed to the patients (Kim & Oh, 2003) (1+), (Oh et
al., 2003), (Nesari et al., 2010) (1+).
4. The nurse telephone follow-up intervention lasts for 12 weeks. The frequency
of telephone calls provided by the diabetes nurses to patients is around 16
times with twice a week for the first month and then weekly for the second
and third month. The duration of each session should last for 20-25 minutes.
(Grade A)
The nurses contacted the participants twice a week for the first month and then
weekly for the second and third month. An average 16 times of telephone calls
and average 25 minutes for each session were provided (Kim & Oh, 2003) (1+),
(Oh et al., 2003).
A Master’s nursing degree student contacted the participants twice per week for
the first month and then weekly for the second and third month. Each participant
received 16 calls and the duration of each call was an average of 20 minutes
(Nesari et al., 2010) (1+).
Patients followed up 16 times by trained diabetes nurse through telephone (2 calls
per week in the first 4 week, 1 call per week for the remaining 8 weeks) (Aliha et
al., 2013).
5. Patients will be asked to have regular checking on their blood glucose level
more than twice a day and record the food intake and exercise pattern (Grade
A).
Participants were asked to record blood glucose levels more than twice a day and
also to keep daily diet and exercise logs (Kim & Oh, 2003) (1+).

! !
6. All the medication and insulin adjustments by the nurse telephone follow-up
intervention will be discussed with the endocrinologist (Grade A).
Adjustments of medications were communicated to the participants’ doctors (Kim
& Oh, 2003) (1+), (Nesari et al., 2010) (1+).

! !
!
The Grade of Recommendation of Scottish Intercollegiate Guideline Network
(SIGN) (SIGN, 2012)
Grade& & Statements
A At least one meta-analysis, systematic review, or RCT rated as 1++, and
directly applicable to the target population; or
A body of evidence consisting principally of studies rated as 1+, directly
applicable to the target population, and demonstrating overall consistency of
results
B! A body of evidence including studies rated as 2++, directly applicable to the
target population, and demonstrating overall consistency of results; or
Extrapolated evidence from studies rated as 1++ or 1+
C! A body of evidence including studies rated as 2+, directly applicable to the
target population and demonstrating overall consistency of results; or
Extrapolated evidence from studies rated as 2++
D! Evidence level 3 or 4; or
Extrapolated evidence from studies rated as 2+
!
Appendix I: Grades of recommendations

! ! ! !!
!
Patient satisfaction questionnaire
(Please!circle!the!appropriate!answer)! Strongly
Disagree
Disagree Neutral Agree Strongly
Agree
1. The diabetes nurses are knowledgeable about diabetes management.
1 2 3 4 5
2. The diabetes nurses provide help and support in diabetes management.
1 2 3 4 5
3. The diabetes nurses help to resolve the management problems.
1 2 3 4 5
4. The diabetes nurses have encouraged and reinforced me to adherence the treatment recommendations.
1 2 3 4 5
5. The duration of telephone counseling is adequate.
1 2 3 4 5
6. The frequency of telephone counseling is adequate.
1 2 3 4 5
7. Overall, the diabetes nurse follow-up is satisfactory.
1 2 3 4 5
8. Any other suggestions: ________________________________________________________________________________________________________________________________________________________________________________________________________________________
Appendix J: Patient satisfaction questionnaire

!
!
Audit form on healthcare professional compliance with the
nurse telephone follow-up services guideline
(Please “! “ in appropriate column)
Standard criteria Sources of
information
Yes No N/A Remarks
1. Conduct health education on diabetic care O / CR / NA
Reinforce diabetic regime
2. - Diet
3. - Exercise
4. - Self-monitoring blood glucose (SMBG)
5. - Medication
6. -Hypoglycaemia management
Medication adjustment
7. -Medication and insulin adjustments were
reviewed by the endocrinologist
Duration of the service
8. - Total 12 weeks of nurse telephone follow-up
intervention was provided
9. - 16 times of telephone calls with twice a
week for the first month and then weekly for
the second and third month was provided
10. - The duration of each session last for 20-25
minutes
11. Appropriate counseling skills was used
Score: Total
O = Observe; CR = Check Record; NA = Not Applicable
(Please circle the appropriate sources of information)
Compliance Percentage of standard criteria: _______________________________________
Appendix K: Audit form on healthcare professional compliance with
the nurse telephone follow-up services guideline

!
!
Healthcare professional satisfaction questionnaire
(Please!circle!the!appropriate!answer)! Strongly
disagree
Disagree Neutral Agree Strongly
agree
1. The program is properly briefed.
(Orientation program)
1 2 3 4 5
2. The guideline is concise and clear. 1 2 3 4 5
3. The guideline of the program is clear
and easy to follow.
1 2 3 4 5
4. The working group provides help and
support when necessary.
1 2 3 4 5
5. The program can update the
knowledge and managements of
diabetes care.
1 2 3 4 5
6. I feel confident in counseling and
supporting the patients with type 2
diabetes via telephone.
1 2 3 4 5
7. The program can increase my
autonomy in diabetes care.
1 2 3 4 5
8. The duration of the telephone
counseling is adequate.
1 2 3 4 5
9. The frequency of telephone counseling
is adequate.
1 2 3 4 5
10. The diabetes self-care adherence
assessment form is simple to use.
1 2 3 4 5
11. Overall, the program is satisfactory. 1 2 3 4 5
12. Any other suggestions:
___________________________________________________________________________________
___________________________________________________________________________________
___________________________________________________________________________________
Appendix L: Healthcare professional satisfaction questionnaire

!
Effect of the diabetes nurse telephone follow-up on HbA1c
levels and self-care adherence assessment form !Body weight (kg): ___________________
Body height (m): ___________________
Body mass index: ___________________
HbA1c level (%): ___________________
!(Please!circle!the!appropriate!answer)!1. Diet Rarely Occasionally Somewhat
frequently
Very frequently
-Eat recommended food
portions
0 1 2 3
-Eat meals/snacks on time 0 1 2 3
-Read food labels 0 1 2 3
!!
2. Exercise No regular exercise Perform one or
two times of
exercise per
week
Perform exercise
three or more
times per week
-20-30 minutes of exercise at
least two to three times per week
0 1 2
!!
3. Self-monitoring blood glucose
(SMBG)
Non-adherence
Adherence
-Perform SMBG four points a day and
two days per week
0
1
!
Appendix M: Effect of the diabetes nurse telephone follow-up on
HbA1c levels and self-care adherence assessment form

!
!4. Medication Rarely Occasionally Somewhat
frequently
Very
frequently
-Take OHA or insulin at the
right time
0 1 2 3
-Take correct dose of diabetes
pills or insulin
0 1 2 3
!5. Hypoglycaemia management Not achieved Achieved
-Treat low blood glucose appropriately 0 1
!
Ho Fung Yi (2008943820)