-
8/12/2019 An Indian Tragedy, An Indian Solution - Perspective of
Managing Service Quality in Emergency Medical Services in India
1/9
-
8/12/2019 An Indian Tragedy, An Indian Solution - Perspective of
Managing Service Quality in Emergency Medical Services in India
2/9
!" $"%&'" ()'*+%,- '" $"%&'" ./012&/"345$"2/67 +2 '0
G
"""#$%&'(#)*+, [ISSN 2159-6743 (Online)] 9:; :? @>:A!>
BC!>(B D!;4C G- =;4AC< 8- GH8G
!" $"%&'" ()'*+%,- '" $"%&'" ./012&/"3
4+)56+72&8+ /9 :'"'*&"* .+)8&7+ ;1'0&2,
&"
-
8/12/2019 An Indian Tragedy, An Indian Solution - Perspective of
Managing Service Quality in Emergency Medical Services in India
3/9
!" $"%&'" ()'*+%,- '" $"%&'" ./012&/"345$"2/67 +2 '0
I
"""#$%&'(#)*+, [ISSN 2159-6743 (Online)] 9:; :? @>:A!>
BC!>(B D!;4C G- =;4AC< 8- GH8G
care should typically be provided by an emergency medical team
consisting of doctors trained tointernational standards on trauma
life-support techniques, nurses, trained ambulance personnel
andparamedic units requiring highly advanced skills and specialized
equipment. Improving service qualityin emergency medical care will
help to save lives and minimize disabilities in patients after
recovery(Rehberg, 2007). More important however, is to ensure that
people are aware of the existence of theemergency medical service.
Garg, (2012) noted an EMS that people are not aware of is as good
as
nonexistent (para. 7). Gargs notion is particularly relevant to
the poor, indigent and illiterate.The increasing rates of
urbanization and industrialization in India suggest that providing
efficient
post trauma care is an important area of concern in India.
Current statistics are difficult to obtain but theNational Crime
Records Bureau in India reported that in 2010, at least 10.1% of
deaths were due toaccidents and injuries. A total of 678,326 cases
of Un-Natural Accidents caused 359,583 deaths andrendered 503,932
people injured during 2010 with a male to female victim ratio of
78:22. Most of thevictims of accidents were in the economically
active group aged between 15 and 44 years. This group ofpeople
accounted 60.7% of all persons killed in accidents in the country
during the year. This is a majorarea of concern and hence efforts
need to be made effectively to prevent accidents, and secondly,
toincrease the service quality of emergency medical services in
India (NCRB, 2011). These statistics shouldbe treated with caution,
however, because they underrepresent to reality on the ground; they
do notreveal the true picture. A Report of the Committee on Crime
Statistics by the Social Statistics Divisionof the Central
Statistics Office in 2011, revealed Minimisation and Suppression of
Statistics , Favours to High
Ups, Monetary Considerations, Under Pressure from goons, gangs,
mafias or other influential sectionsas someof the reasons for
under-, or non-reporting accidents and injuries in India (CSS,
2011, p. 18-19).
Government policy focuses on the prevention of communicable
diseases rather prevention of trauma.There are no government
agencies to plan, finance, or draft legislation to establish an
efficient nationalintegrated trauma care system in the country.
This is specifically lacking in rural areas where
accuratestatistics may be limited and under reporting common
(Joshipura et al., 2003). Furthermore, there islimited provision of
accident and emergency care unit systems in the major cities and
towns (Garg, 2012;Wegman, 1996). Meeting the golden hour goal
(first hour after injury) and the platinum hour goal (firstten
minutes after injury) determines the effectiveness of treatment in
the trauma patients that isfrequently missed in India (Medindia,
2012). Delayed pre-hospital care such as delayed
first-aidtreatment, delayed inefficient transfer of the victim to
the hospital from the accident site and medico-legalissues can lead
to deterioration of the patients conditions leading to complication
(Gururaj, 2005).
Additionally a systematic triage system to evaluate the trauma
victim is followed only by fifty-fourpercent of the hospitals. This
is compounded by resource shortages because state public health
carepolicy falls short for the majority of trauma cases that leads
to inefficient trauma-care service to thosepeople who cannot afford
the cost of investigations and the admission costs in specialized
hospitals(Joshipura et. al., 2003). Consequently, the poor and
indigent are deprived of necessary post trauma careand treatment
because they cannot afford the treatment cost. Often the hospital
where the patient may beadmitted depends on the hospital fees that
the patients family can afford and not on the type of
injury(Joshipura et. al., 2003). The mortality rate among
low-income group is as high as 63%, compared to 55%among the
middle-income group and 35% among high-income groups (Mock et
al.,1998).
The better survival and functional outcome among injured
patients in developed countries can bepartly attributed to
high-cost equipment and technology (Narayan, 2011). Much of this
high-endtechnology is unaffordable and unavailable to victims to
the poor. Improvement in the outcome oftrauma patients can result
from improvements in the organization of trauma care services in
the form of
focused systems in specific geographical areas (Sasser et al.,
2006). Better organization of systems mayreduce the time between
injury and the definitive treatment thereby reducing morbidity and
mortality. InIndia, such a trauma system is almost non-existent and
even if present in some urban areas, lacks thecohesive effort
required (Joshipura, 2006).
Framework of Service Quality Model of Emergency Medical
Service
Services tend to be intangible, inseparable from their provider,
perishable and inconsistent in their delivery(Walker & Baker,
2001, p. 2). These qualities make services high in experience and
credence qualities.Patients therefore have greater difficulty in
evaluating medical services generally and trauma services
-
8/12/2019 An Indian Tragedy, An Indian Solution - Perspective of
Managing Service Quality in Emergency Medical Services in India
4/9
!" $"%&'" ()'*+%,- '" $"%&'" ./012&/"345$"2/67 +2 '0
J
"""#$%&'(#)*+, [ISSN 2159-6743 (Online)] 9:; :? @>:A!>
BC!>(B D!;4C G- =;4AC< 8- GH8G
specifically. Noting the unique nature of services, Levitt
(cited in Gronroos, 2001) describes a service as apromise of
satisfaction (p. 3). As such, trauma services promise both implicit
and explicit influencepatient expectations. Brown, Fisk and Bitners
(1994) seminal work in clearly allied service satisfactionwith
service quality, although the two do not share common definitions
of terms nor is there clearunderstanding in the literature of how
the two relate.
Parasuraman (cited in Walker & Baker 2000), whose research
has provided a framework for
measuring service quality in this paper, defines service quality
as the gap between the consumersexpectations and their perceptions
of how the service is performed(p. 1). Quality is therefore likely
to be valueled in terms of perceived quality and availability of
service to patients. It therefore follows that perceivedvalue in a
trauma unit is a measure of the extent to which the medical service
delivered meets thepatients expectations. The nature of a service
means that the patient is physically present throughout thecare
delivery process. Both the service outcome, as well as the service
process influences the perception ofvalue. The perceived quality
can be aligned with a continuum of unacceptable quality at one end
andideal quality at the other with graduations of quality in
between. This implies that prior expectations arecompared with
actual service delivery and the service outcome and it is this
comparison that leads toperceived value. Thus, it is important that
the management of the care service process occurs throughmanagement
of standards and controls be they regulatory or provider specific
(Dorrian, 1996; Ghobadian,Speller & Jones, 1994).
Quality is not a singular but a multi-dimensional phenomenon. It
is not possible to ensure
organization specific quality without determining the salient
determinants of quality specific to a service.There are a number of
models including those of Gronroos (1983), Lehtinen and Lehtinen
(1991), andParasuraman (2002). Gronroos (2001) argues that service
quality comprises three dimensions namely: thetechnical quality of
the outcome, the functional quality of the service encounter and
the corporate image.Lehtinen and Lehtinen also identify three
dimensions namely physical quality, corporate quality
andinteractive quality. They argue that it is necessary to
differentiate between the quality of the process ofdelivery and the
quality of the outcome of the service (Ghobadian, Speller &
Jones, 1994; Martin, 1999,Walker & Baker, 2000). Garg (2012)
further suggested that the reputation of a hospital often
dependsupon the quality and promptness of its emergency medical
services.
These attempts to identify the service quality determinants lack
sufficient detail but are useful in theseparation of measuring both
process and outcome in terms of quality. Other researchers such
asParasuraman and Ghobadian, Speller and Jones have proposed more
detailed quality determinants (e.g.,see Ghobadian, Speller &
Jones, 1994; Zeithhaml, 2000) wherein the importance and utility
value of eachdeterminant is dependent on the nature of the service.
Technical quality, functional quality and serviceimage form
components of a service quality. Technical quality is the quality
received by the patient whenthe patient interacts with the service
that leads to an evaluation of the service by that patient.
Thetechnical outcome determines the functional quality that
reflects the views of the actual service itself. Thetechnical and
the functional quality of the service lead to building up of a
service image in a broaderstakeholder context including those with
no experience of the service delivery. Tradition, ideology, wordof
mouth, pricing and public relation also contribute towards the
building of that image (Gronroos, 1984).Thus service quality is
subjective and interpretative in the context of emergency medical
services ratherthan having an absolute clinical perspective.
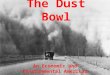
An analysis in terms of the current state of emergency medical
services, using the general model ofservice quality structure as
proposed by Parasuraman, et al. (1988), is shown as Figure 1.
Emergencymedical services quality has impact on all the three
phases of its interaction with patients. RATER and
the three phases of emergency care have been chosen for this
review because of its simplicity andappropriateness to the
characteristic demands from emergency medical services. The
dimensions of theRATER Model include reliability, assurance,
tangibles, empathy, and responsiveness (Nitin Seth, et
al.,2004).
-
8/12/2019 An Indian Tragedy, An Indian Solution - Perspective of
Managing Service Quality in Emergency Medical Services in India
5/9
!" $"%&'" ()'*+%,- '" $"%&'" ./012&/"345$"2/67 +2 '0
K
"""#$%&'(#)*+, [ISSN 2159-6743 (Online)] 9:; :? @>:A!>
BC!>(B D!;4C G- =;4AC< 8- GH8G
Figure 1.The RATER Model- Service Quality Dimensions Applied to
Emergency Medical Services.Note. Adapted from Parasuraman et al.
(1988) and Nitin Seth, S. G. Deshmukh and Prem Vrat (2005).
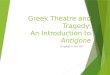
Figure 2 illustrates the emphasis in managing service quality at
each phase of emergency medicalservices: Phase One being the
awareness, trust and initial accessing the care, Phase Two being
the inhospital care and Phase Three discharge and
rehabilitation.
-
8/12/2019 An Indian Tragedy, An Indian Solution - Perspective of
Managing Service Quality in Emergency Medical Services in India
6/9
-
8/12/2019 An Indian Tragedy, An Indian Solution - Perspective of
Managing Service Quality in Emergency Medical Services in India
7/9
!" $"%&'" ()'*+%,- '" $"%&'" ./012&/"345$"2/67 +2 '0
M
"""#$%&'(#)*+, [ISSN 2159-6743 (Online)] 9:; :? @>:A!>
BC!>(B D!;4C G- =;4AC< 8- GH8G
public trust, reliability and awareness of access is to be
achieved. It follows that a regulated skill-basedtraining program
for doctors as well as paramedical staff in emergency medical
services procedures isimplemented to organize and integrate
pre-hospital services with definitive care facilities (hospital)
sothat a patient is shifted to an appropriate facility in the
shortest possible time, regardless of the ability topay. A
systematic triage protocol should be made mandatory in all trauma
units (Joshipura, 2008).
Conclusion
From the above review, it has been highlighted that in India
there is significant work to be done in thefields of medical
treatment and quality of patient care. The field of trauma care and
emergency medicinehas not progressed uniformly in the country and
it is still at a primitive stage. The importance of
reliableemergency medical services cannot be over emphasized,
especially where the government has theresponsibility of caring for
a majority of the population.
Service quality of the trauma care system in India can be
improved by increasing resources availablefor the treatment of the
trauma victims. The technical quality should meet the functional
quality ofhospital services thus enhancing image of the trauma care
system and trust from citizens (Nitin Seth etal., 2004). The United
Nations General Assembly and the WHO have implemented an action
plan ADecade of Action for Road Safety 2011-2020 by member nations
and thus the quality of emergencymedical services generally rather
than road safety specifically, should be considered a high priority
and
different mechanisms for its implementation throughout the
country needs to be devised.
-
8/12/2019 An Indian Tragedy, An Indian Solution - Perspective of
Managing Service Quality in Emergency Medical Services in India
8/9
!" $"%&'" ()'*+%,- '" $"%&'" ./012&/"345$"2/67 +2 '0
N
"""#$%&'(#)*+, [ISSN 2159-6743 (Online)] 9:; :? @>:A!>
BC!>(B D!;4C G- =;4AC< 8- GH8G
References
A)/O"- .P QP- ?&6R-
412).8
I J/2)1K)2).8 91*1%/:/*.?FFUVW- JI\LLP
@)/")//6- DP U8VNJWP ! 6+)X&5+ d1'0&2, Z/%+0 '"% &26
Z')R+2&"* &ZY0&5'2&/"6P G40,L/1* 3,40*12 ,+
910H/.)*%- FMUJW-
IL\JJ
@)/")//6- DP UGHH8WP (7+ Y+)5+&X+% 6+)X&5+ d1'0&2,
5/"5+Y2_ ! Z&62'R+c 91*1%)*% 5/06)'/ >412).8-
FFUIW-8KH`8KGP
@1)1)'e- @P UGHHKWP -*$40)/( )* -*7)1N O *1.),*12 L/0(L/'.)6/?
-* P1'H%0,4*7 Q1L/0(N P407/* ,+ B)(/1(/? =+O ^+07&_(7+
='2&/"'0 D/ZZ&66&/" /" 4'5)/+5/"/Z&56 '"% B+'027-
4&"&62), /[ B+'027 '"% ?'Z&0, Q+0[')+P
B&"%162'" (&Z+6P UGH8HWP 91* 7)/( 1( R &,(L).12(
0/+4(/ &): .0/1.:/*.#+72&"+"- ;P- T >+72&"+"- 9P
U8VV8WP (O/ !YY)/'57+6 2/ .+)X&5+ g1'0&2,
&Z+"6&/"6P P UGH8HWP ./Z+ &"6&*726 /"
5/"5+Y21'0&h&"* '"% Z+'61)&"* 6+)X&5+
d1'0&2,-3,40*12 ,+
J/.1)2)*% 1*7 C,*(4:/0 5/06)'/(?FVU8W GV\JGP
4')2&"- DP >P U8VVVWP (7+ B&62/),- CX/012&/" '"%
S)&"5&Y0+6 /[ .+)X&5+ 4')R+2&"*- 910H/.)*%
-*./22)%/*'/ 1*7
Q21**)*%- FVUMW IGJ`IGNP
4+%&"%&'P UGH8GWP P >P U8VNNWP .C_ !
Z102&Y0+\&2+Z 65'0+ [/) Z+'61)&"* 5/"61Z+)
Y+)5+Y2&/"6 /[ 6+)X&5+ d1'0&2,P3,40*12 ,+ J/.1)2)*%-
.Y)&"*- 8G\JHP
-
8/12/2019 An Indian Tragedy, An Indian Solution - Perspective of
Managing Service Quality in Emergency Medical Services in India
9/9
!" $"%&'" ()'*+%,- '" $"%&'" ./012&/"345$"2/67 +2 '0
V
"""#$%&'(#)*+, [ISSN 2159-6743 (Online)] 9:; :? @>:A!>
BC!>(B D!;4C G- =;4AC< 8- GH8G
S+%+" 4P- .51)[&+0%