Embed Size (px)
Citation preview
Pediatric Palliative Care
An Inpatient Oncology Perspective
HPC Palliative Spring Education Event March 23, 2017 Paula MacDonald, RPh, Pediatric Oncology
Objectives
Present palliative pediatric oncology cases that illustrate symptoms such as • pain • cytopenias • bleeding • nausea/vomiting • constipation • dyspnea • secretions
Objectives
Review medications and tools used for pediatric symptom management
Highlight challenges to provision of
care in children Provide some “practical pearls” to
enhance provision of palliative care to pediatric patients
GOAL
To demonstrate that strategies for palliative symptom management in pediatric patients are not that different than those used for adult palliative patients.
Introduction Symptom management for children
with end-stage cancer presents a challenge to health care providers
Interdisciplinary family-centered care is an integral part of the symptom management for these children
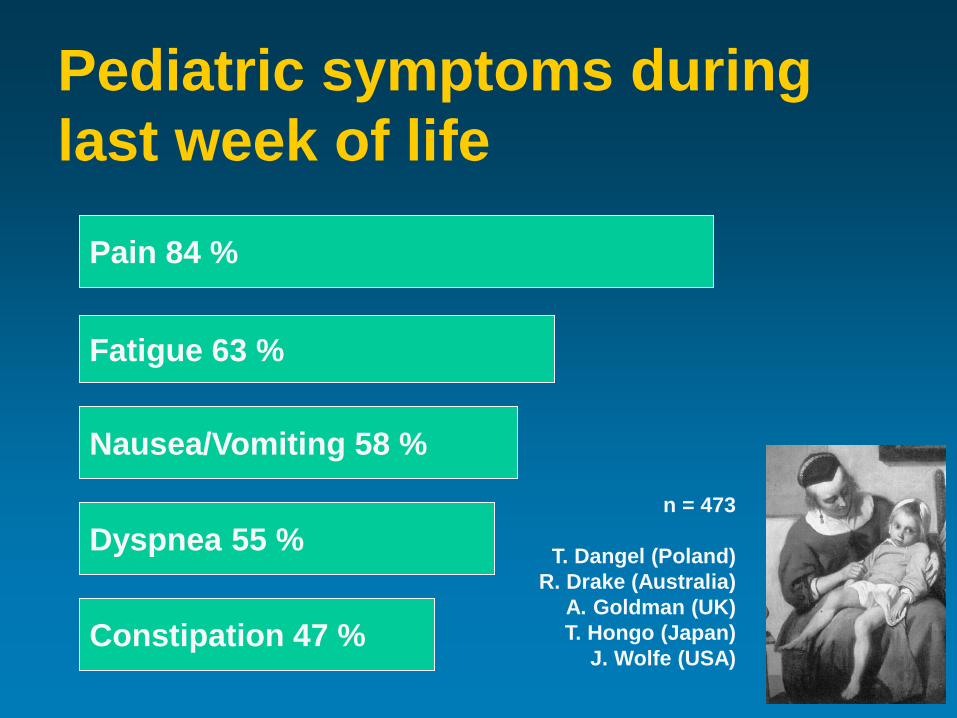
n = 473
T. Dangel (Poland) R. Drake (Australia)
A. Goldman (UK) T. Hongo (Japan)
J. Wolfe (USA)
Pain 84 %
Fatigue 63 %
Nausea/Vomiting 58 %
Dyspnea 55 %
Constipation 47 %
Pediatric symptoms during last week of life
CASE: 12 yr ♀ metastatic NBL Long-standing recurrent/refractory NBL
• Extensive progression of bony disease • Large cranial lesion with intracranial
extensions • No possibility of cure
Severe pain in legs, back, head, etc.
Overarching goal of care: Go home as much as possible for as
long as possible!!!!
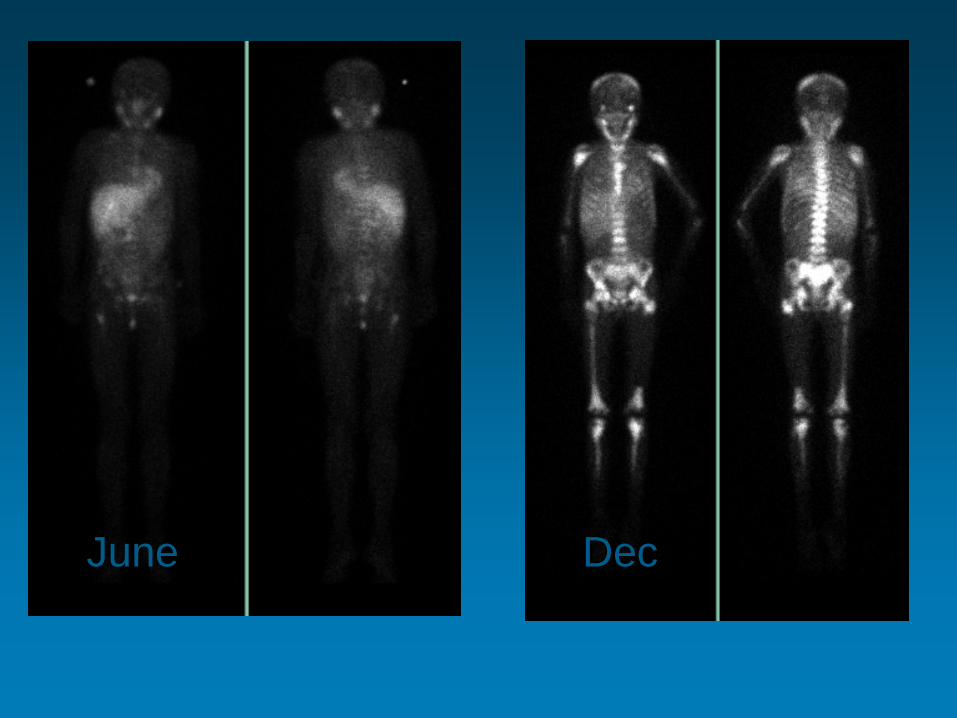
June Dec
CASE: 12 yr ♀ metastatic NBL Initial goal at disease progression: optimize pain control as outpatient as long as possible
initially requested no central IV access but
agreed to oral medications and radiation
Chemotherapy (irinotecan + temozolomide) stopped after 2 cycles due to prolonged neutropenia, thrombocytopenia and diarrhea
CASE: 12 yr ♀ metastatic NBL
So… what to do about her pain? oral hydromorphone PRN initially (≠ morphine, acetaminophen, NSAIDs)
1. Radiate skull, R hip and back lesions
2. REGULAR hydromorph contin + bolus: 9mg PO q12h + 2mg q2h PRN
When pain worsened, increased to 12mg PO q12h + 3mg breakthrough q2h PRN
Challenges Tolerance vs rapid disease progression Morphine allergy Lorazepam intolerance (agitation) Thrombocytopenia (≠ NSAIDs) No fentanyl infusions outside PICU No authorized methadone prescriber in
community
Myths Related to Pain and Pain Management in Children
Risk of respiratory depression Addiction Child that is sleeping or playing does not
have pain Presence of pain indicates worsening of
disease or approaching death
WHO Guidelines on the pharmacological treatment of persisting pain in children (2012)
Dosing at regular intervals: • Around the Clock
Adapting treatment to the individual child: • With the Child
Using the appropriate route of administration: • By the appropriate route
Using a two-step strategy: • By the Analgesic Ladder
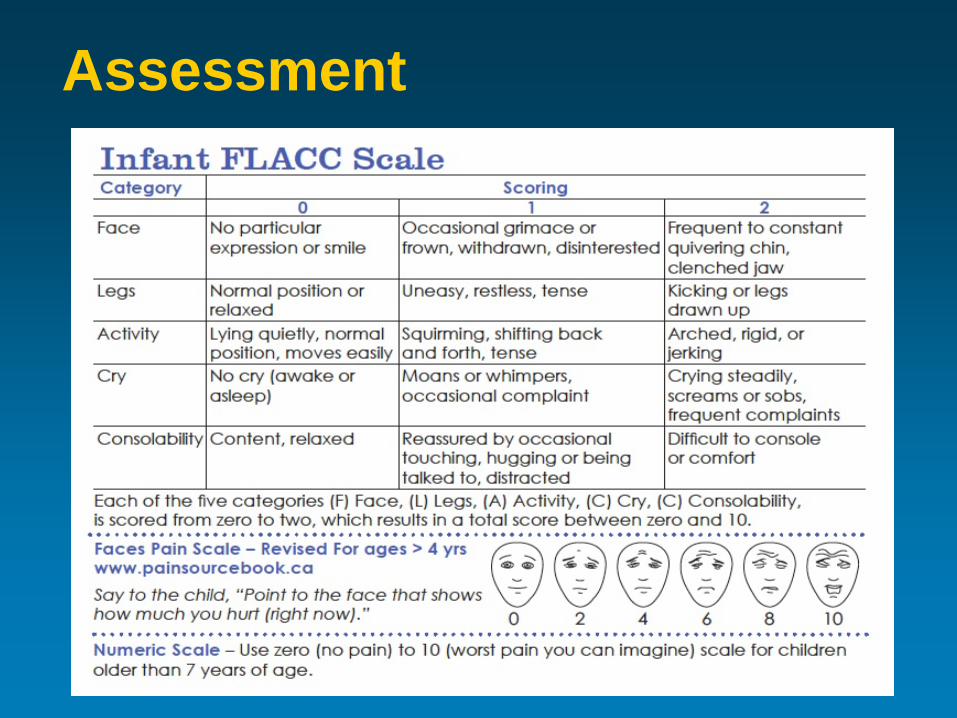
Assessment
Using the appropriate route of administration (i.e. Least traumatic)
Use oral/enteral route, when possible Alternative routes:
• Sublingual/buccal • Intranasal • Transdermal (contraindicated in acute pain) • Rectal • Intravenous (or subcutaneous) • Intramuscular = obsolete
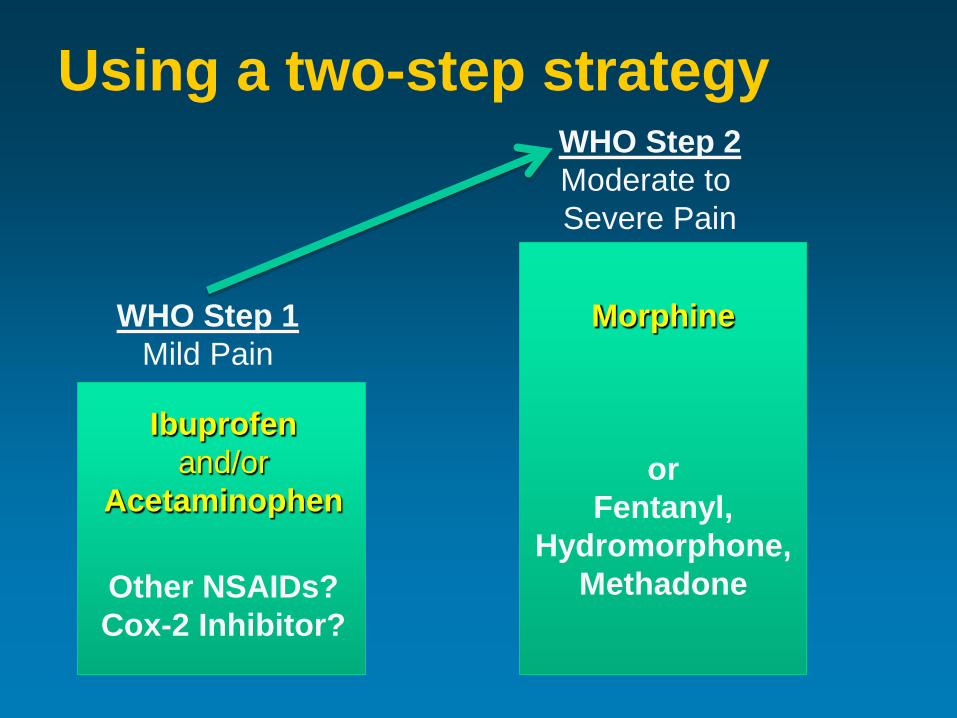
Using a two-step strategy
WHO Step 1 Mild Pain
WHO Step 2 Moderate to Severe Pain
Ibuprofen and/or
Acetaminophen
Other NSAIDs? Cox-2 Inhibitor?
Morphine
or Fentanyl,
Hydromorphone, Methadone
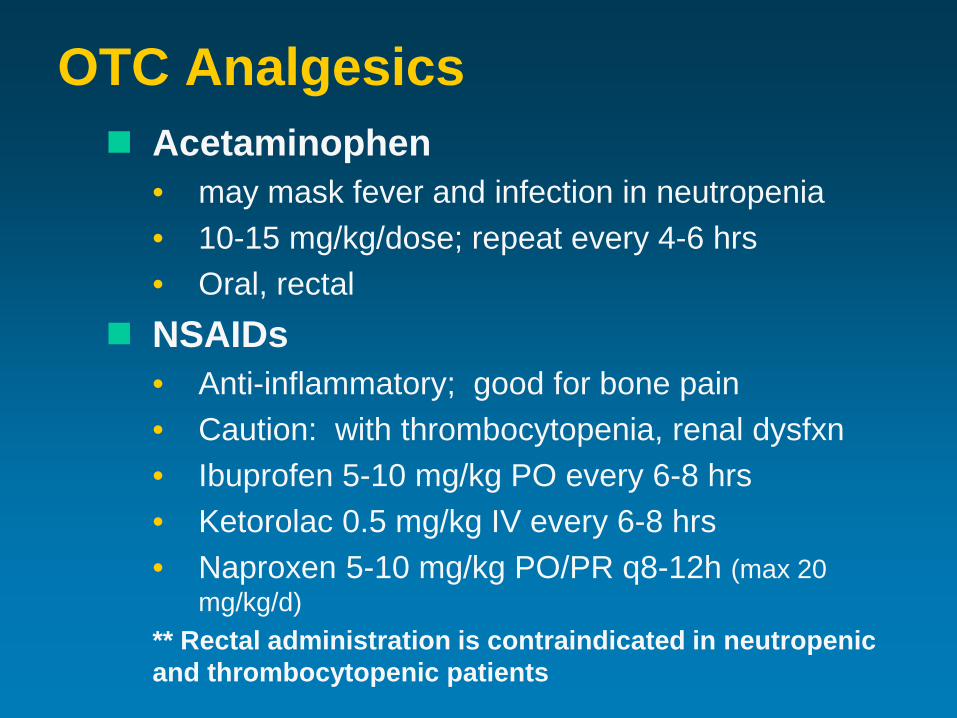
OTC Analgesics Acetaminophen
• may mask fever and infection in neutropenia • 10-15 mg/kg/dose; repeat every 4-6 hrs • Oral, rectal
NSAIDs • Anti-inflammatory; good for bone pain • Caution: with thrombocytopenia, renal dysfxn • Ibuprofen 5-10 mg/kg PO every 6-8 hrs • Ketorolac 0.5 mg/kg IV every 6-8 hrs • Naproxen 5-10 mg/kg PO/PR q8-12h (max 20
mg/kg/d) ** Rectal administration is contraindicated in neutropenic and thrombocytopenic patients
Opioid drug options Phenanthrene derivatives
• Morphine: Gold Standard • Hydromorphone • Oxycodone (not recommended) • Codeine (not recommended)
Phenylpiperidine derivatives • Fentanyl
Diphenylheptane derivatives • Methadone
Intranasal Fentanyl Rapid and effective minimization of pain Indicated for Moderate to Severe Acute
Pain when IV access not available or necessary
Contraindicated if allergy to fentanyl or other opiates, altered conscious state, occluded nasal passages, intubated pts, URTI with nasal secretions, epistaxis
Intranasal Fentanyl Dose: 1.5 mcg/kg/dose Repeat q5mins, PRN Onset: 2-5 minutes Duration: ~ 30 minutes to 2 hours Administration via Mucosal Atomization
Device (MAD):
Tool kits at www.caphc.org
Intranasal Fentanyl Adverse Effects
• Bitter taste • Nasal irritation • Respiratory depression • Dyspnea/cough • Hypotension • Excessive sedation • Pruritus • Chest wall rigidity (with large doses) Monitoring same as with IV opioids
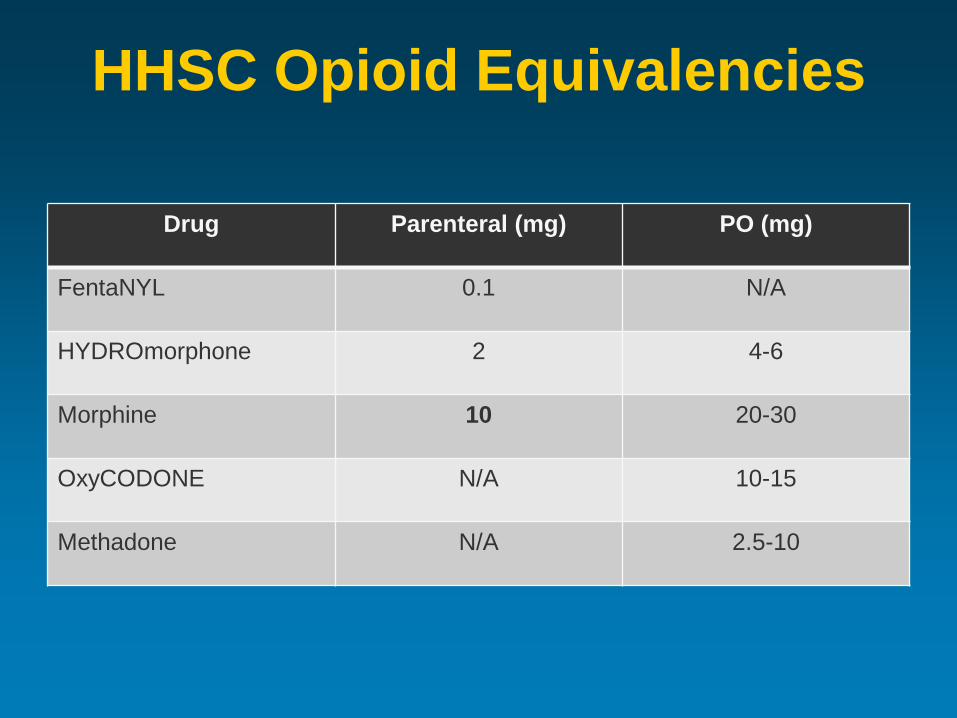
HHSC Opioid Equivalencies
Drug Parenteral (mg) PO (mg)
FentaNYL 0.1 N/A
HYDROmorphone 2 4-6
Morphine 10 20-30
OxyCODONE N/A 10-15
Methadone N/A 2.5-10
Opioid Rotation
Morphine is gold standard first line • BUT, it is not always best for every child
≥10% of children have inadequate pain control with intolerable side effects • May respond to opioid rotation! • If in renal failure consider: fentanyl, methadone • Premature infants: fentanyl • Equianalgesic dosing
Side effects
Analgesia
What about neuropathic pain? Multiple causes of neuropathic pain
in childhood cancer: Tumor infiltration (nerve compression) Phantom limb pain Spinal cord compression ↑ intracranial pressure Neuropathy (e.g. from chemotherapy) *Currently no validated neuropathic pain scales for children < 18 years of age.
What about neuropathic pain? Start with opioids Consider addition of adjuvant agents Tricyclic antidepressants*
– Amitriptyline, Nortriptyline – Side effects: sedation, anticholinergic effects,
prolonged QTc. Wean over 1 week
Gabapentinoids* – Gabapentin, pregabalin – Mechanism: calcium-channel blocker, decrease
release of pain transmitters – Side effects: nystagmus, thought disorder,
hallucinations, headache, and myalgia. Wean 1-2 wks
Pediatric doses of adjuvant agents Amitriptyline (or Nortriptyline) Dose same for both
– Starting dose: 0.1 mg/kg po qhs – Slowly titrate up to 1 mg/kg/day (usually 5-10 mg to start, then max 50-75 mg/day)
Gabapentin – Starting dose: 5-10 mg/kg/dose (max 100 mg/dose);
start QHS, then BID, then TID-QID – Titrate by 5 mg/kg/day every 3-4 days based on
response (max 50 mg/kg/day OR 3600 mg/day) – May titrate more rapidly for severe pain
Adjuvant agents
NMDA receptor channel blockers: – Ketamine (low-dose infusion)
– Dissociative anesthetic, analgesic at low doses – Side effects: intracranial hypertension, tachycardia,
psychomimetic phenomena (give lorazepam) – 1-2 mcg/kg/min IV continuous infusion
– Methadone – Mu-opioid receptor agonist and NMDA receptor
antagonist – Also serotonin and norepinephrine reuptake
inhibitor
CASE: 12 yr ♀ metastatic NBL
Her pain worsens – PO not fast enough: 1. Switch to hydromorphone IV (CADD):
– 8mcg/kg/hr plus boluses 4mcg/kg – Titrate increases: by 50% of dose – Her max reached: 620mcg/kg/hr!!!! (gradual increase
over months; good efficacy; manageable side effects)
2. Amitriptyline added: 10mg PO qhs
3. Ketorolac added: 10mg q6h IV
4. Methadone added: – Started 0.5mg PO BID 2mg PO TID
CASE: 12 yr ♀ metastatic NBL
Other symptoms:
Cytopenias; bleeding risk Anxiety/ OCD-like behaviour Anorexia/Cachexia/Dehydration Nausea/Vomiting Constipation
Cytopenias Caused by:
• Decreased production (chemo, radiation, bone marrow infiltration of malignant cells)
• Destruction, Sequestration Management: (symptom focused!) * Reduce risks (i.e. no rectal meds, ↓ invasive procedures)
• Anemia – fatigue, respiratory compromise - PRBCs • Neutropenia – infection risk – antibiotics/ G-CSF • Thrombocytopenia – transfuse; no NSAIDs
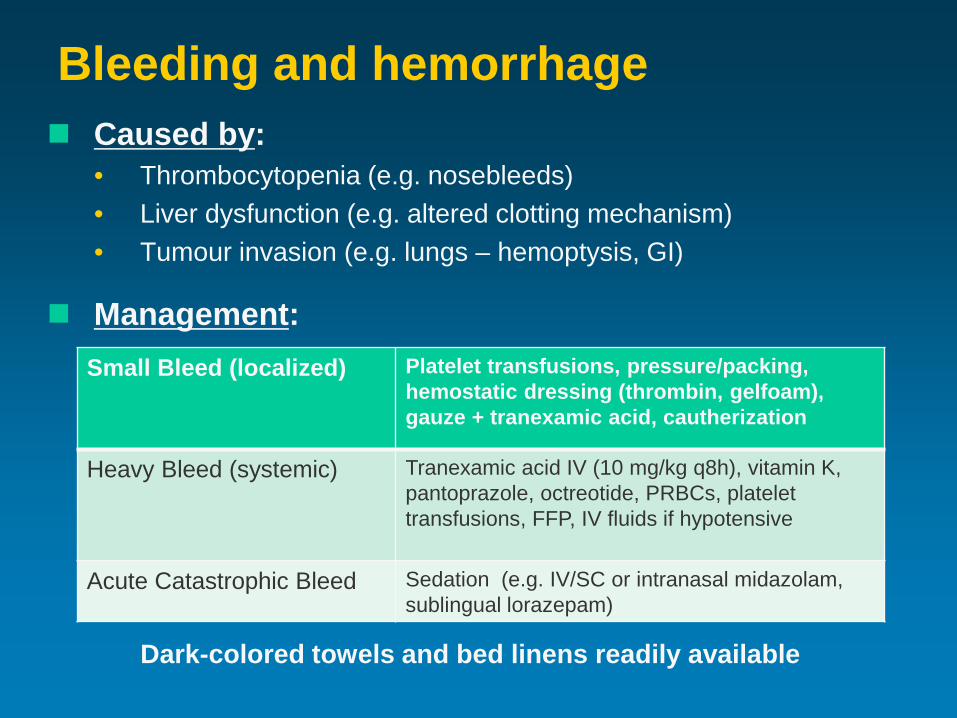
Bleeding and hemorrhage Caused by:
• Thrombocytopenia (e.g. nosebleeds) • Liver dysfunction (e.g. altered clotting mechanism) • Tumour invasion (e.g. lungs – hemoptysis, GI)
Management:
*
Dark-colored towels and bed linens readily available
Small Bleed (localized) Platelet transfusions, pressure/packing, hemostatic dressing (thrombin, gelfoam), gauze + tranexamic acid, cautherization
Heavy Bleed (systemic) Tranexamic acid IV (10 mg/kg q8h), vitamin K, pantoprazole, octreotide, PRBCs, platelet transfusions, FFP, IV fluids if hypotensive
Acute Catastrophic Bleed Sedation (e.g. IV/SC or intranasal midazolam, sublingual lorazepam)
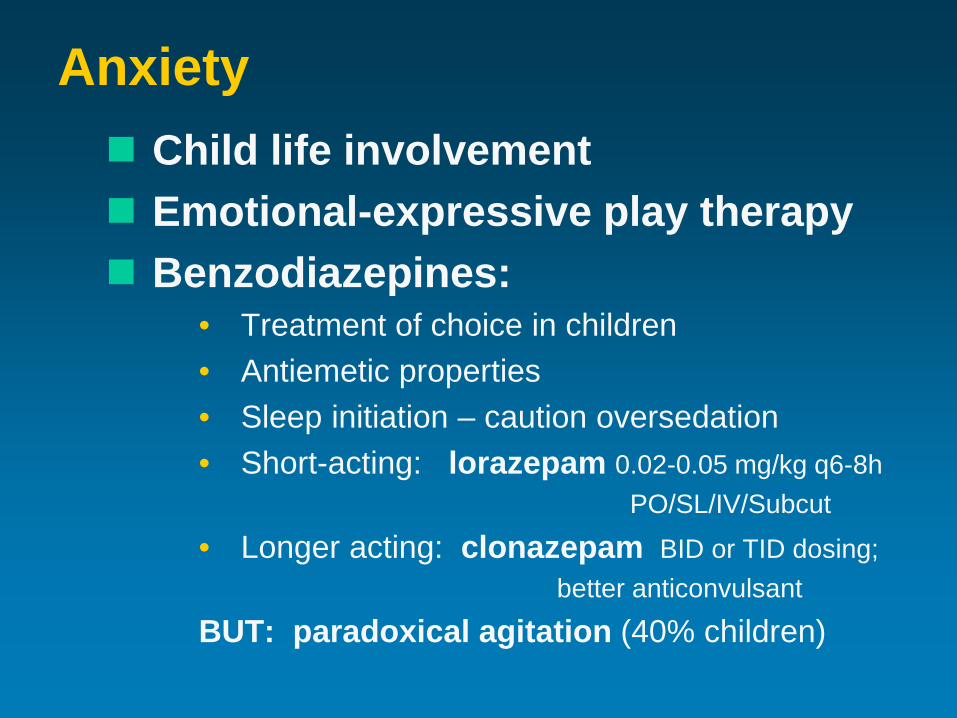
Anxiety Child life involvement Emotional-expressive play therapy Benzodiazepines:
• Treatment of choice in children • Antiemetic properties • Sleep initiation – caution oversedation • Short-acting: lorazepam 0.02-0.05 mg/kg q6-8h
PO/SL/IV/Subcut
• Longer acting: clonazepam BID or TID dosing; better anticonvulsant
BUT: paradoxical agitation (40% children)
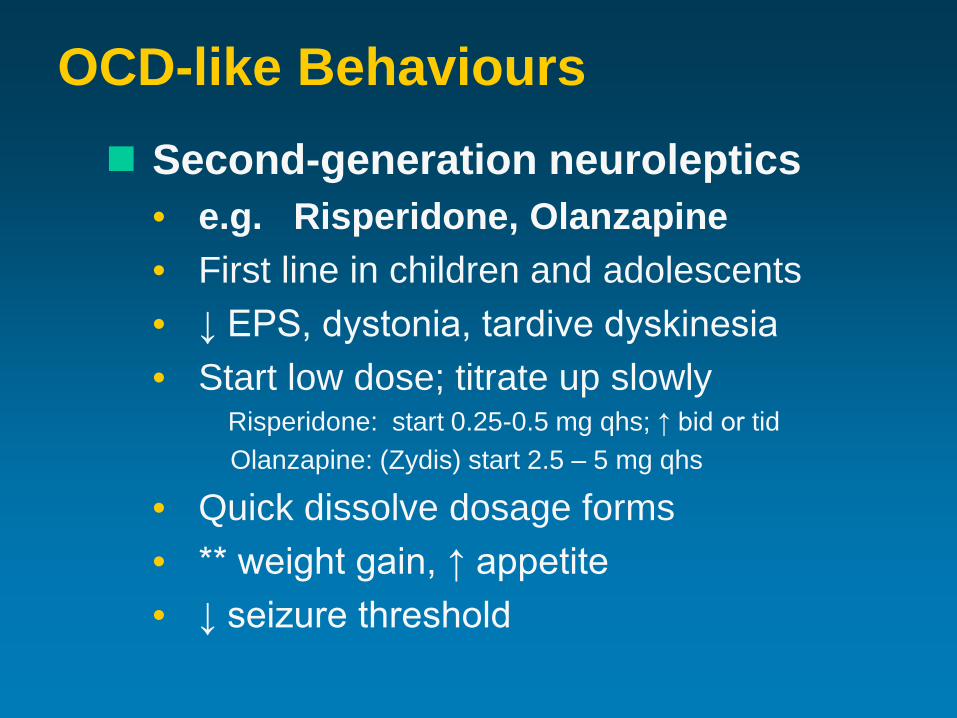
OCD-like Behaviours Second-generation neuroleptics
• e.g. Risperidone, Olanzapine • First line in children and adolescents • ↓ EPS, dystonia, tardive dyskinesia • Start low dose; titrate up slowly
Risperidone: start 0.25-0.5 mg qhs; ↑ bid or tid Olanzapine: (Zydis) start 2.5 – 5 mg qhs
• Quick dissolve dosage forms • ** weight gain, ↑ appetite • ↓ seizure threshold
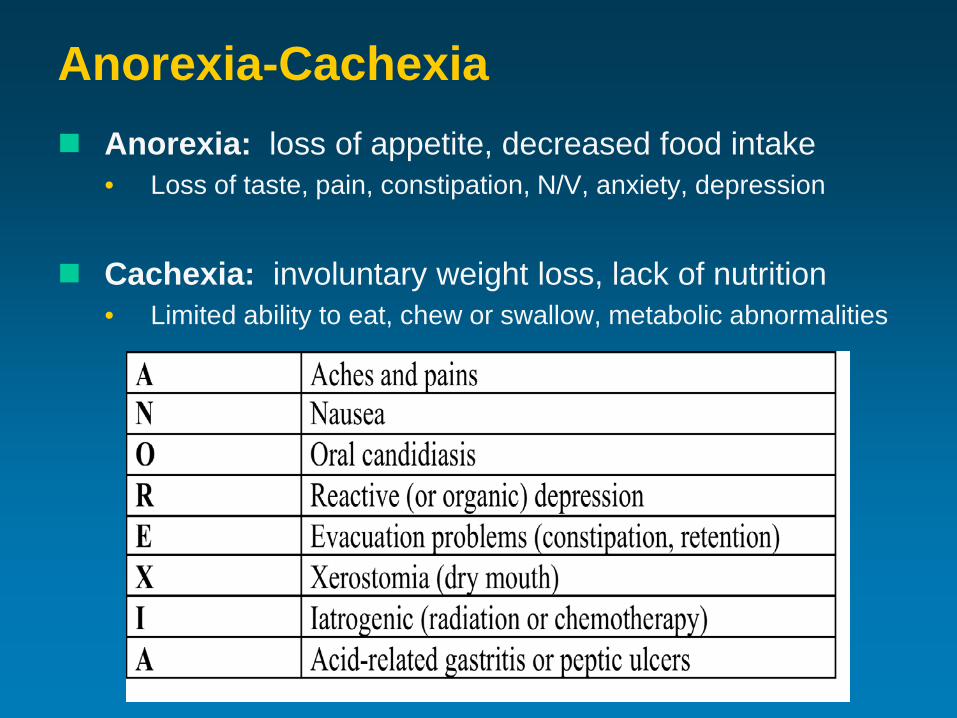
Anorexia-Cachexia Anorexia: loss of appetite, decreased food intake
• Loss of taste, pain, constipation, N/V, anxiety, depression
Cachexia: involuntary weight loss, lack of nutrition
• Limited ability to eat, chew or swallow, metabolic abnormalities
Anorexia-Cachexia Goal of Care: ↑ appetite → promote wt gain ** slow rate of weight loss **
• favourite high-calorie foods, soft foods • Nutritional supplementation – enteral vs parenteral • Appetite stimulants (e.g. Cyproheptadine, steroids) • Treat underlying causes of ↓ appetite: - constipation - N/V - pain - anxiety - thrush
Dehydration excessive loss of water
• limited ability to consume sufficient fluids • increased losses
Hydration intervention – controversial; individualized • Goal: ↓ thirst for comfort help maintain renal function • Caution: peripheral edema • ≠ evidence that hydration ↑ terminal secretions
Goals of Nutrition and Fluid Management in the Dying Child
Alleviate any hunger and thirst
Reduce anxiety about intake
Preserve the social aspects of mealtimes
Constipation Causes:
• Disease-related (e.g. obstruction, neurologic, hypercalcemia, inactivity)
• Treatment-related (e.g. opioids, vincristine)
• Change in diet Management:
• Diet (high fiber) and fluids • Activity • Toileting • Medications
Medications to treat Constipation Osmotic – PEG 3350, lactulose, Citromag
Bulk forming (fibre) - Metamucil Stimulants – senna, bisacodyl, PicoSalax
Stool softeners - docusate Lubricants - mineral oil, glycerine Opioid reversal - methylnaltrexone Motility agents – domperidone, metoclopramide
Caution: thrombocytopenia, neutropenia, obstruction
Nausea and Vomiting Causes
• GI – infection, obstruction, ileus, constipation • Metabolic – hypoglycemia, electrolyte imbalance • CNS - ↑ ICP, anxiety; brain tumour location • Treatment – opioids, chemo, radiation
Management
• Distraction • Dietary • Small meals + slow feeding • Medications
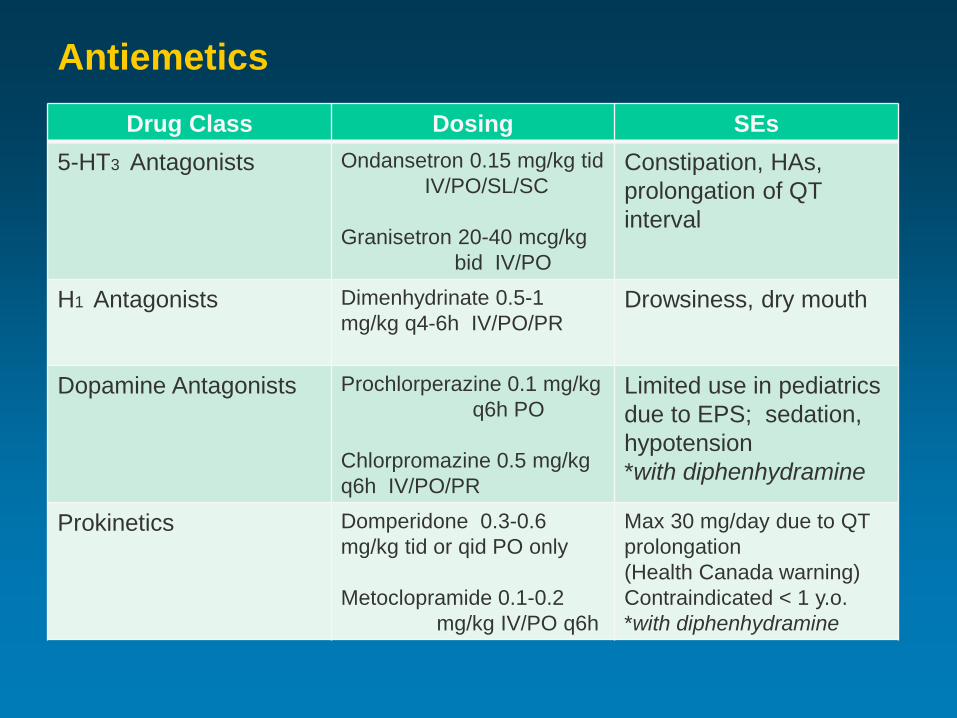
Antiemetics Drug Class Dosing SEs
5-HT3 Antagonists Ondansetron 0.15 mg/kg tid IV/PO/SL/SC Granisetron 20-40 mcg/kg bid IV/PO
Constipation, HAs, prolongation of QT interval
H1 Antagonists Dimenhydrinate 0.5-1 mg/kg q4-6h IV/PO/PR
Drowsiness, dry mouth
Dopamine Antagonists Prochlorperazine 0.1 mg/kg q6h PO Chlorpromazine 0.5 mg/kg q6h IV/PO/PR
Limited use in pediatrics due to EPS; sedation, hypotension *with diphenhydramine
Prokinetics Domperidone 0.3-0.6 mg/kg tid or qid PO only Metoclopramide 0.1-0.2 mg/kg IV/PO q6h
Max 30 mg/day due to QT prolongation (Health Canada warning) Contraindicated < 1 y.o. *with diphenhydramine
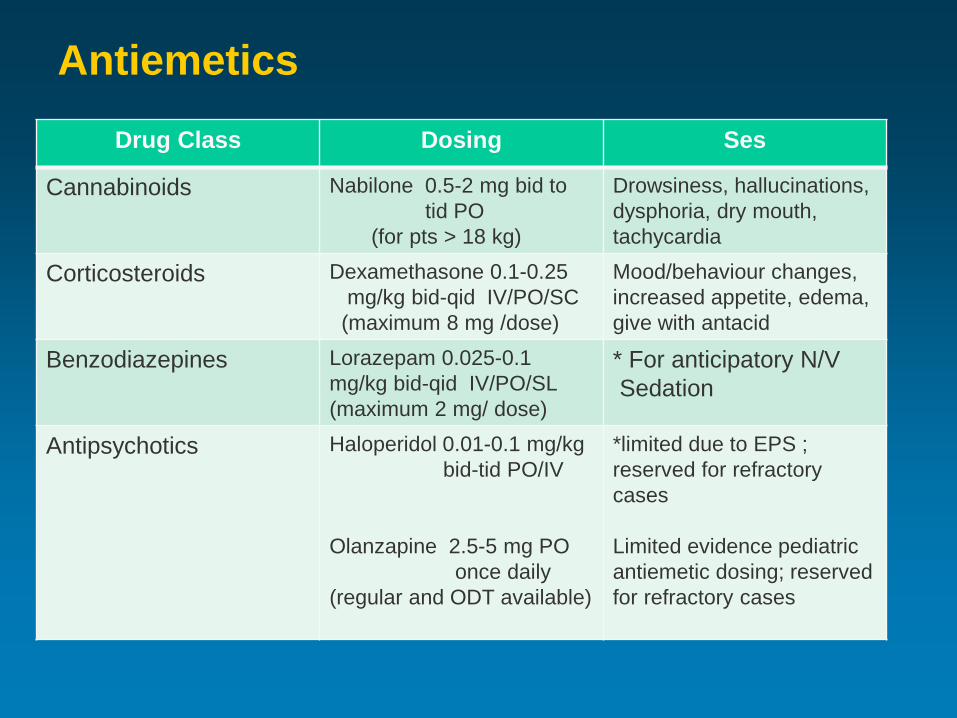
Antiemetics Drug Class Dosing Ses
Cannabinoids Nabilone 0.5-2 mg bid to tid PO (for pts > 18 kg)
Drowsiness, hallucinations, dysphoria, dry mouth, tachycardia
Corticosteroids Dexamethasone 0.1-0.25 mg/kg bid-qid IV/PO/SC (maximum 8 mg /dose)
Mood/behaviour changes, increased appetite, edema, give with antacid
Benzodiazepines Lorazepam 0.025-0.1 mg/kg bid-qid IV/PO/SL (maximum 2 mg/ dose)
* For anticipatory N/V Sedation
Antipsychotics Haloperidol 0.01-0.1 mg/kg bid-tid PO/IV Olanzapine 2.5-5 mg PO once daily (regular and ODT available)
*limited due to EPS ; reserved for refractory cases Limited evidence pediatric antiemetic dosing; reserved for refractory cases
Case: 16 yr ♂ – High-grade brain stem glioma
Diagnosed with DIPG • High grade brain stem glioma • 10-20% of childhood brain tumours • Very aggressive, poor prognosis • No surgical removal; no chemotherapy • Radiation = temporary response (~ 6-9 months) • Post radiation inflammation = Radiation Necrosis • Dexamethasone for symptom control
Case: 16 yr ♂ – High-grade brain stem glioma
Palliative care initiated in community
episode of coughing, difficulty swallowing → Panic Attack → Admit • Unable to stand, walk or speak • Extreme hunger (dexamethasone) but
coughing with liquids, secretions • Tongue numbness • Dyspnea
Case: 16 yr ♂ – High-grade brain stem glioma Overarching goal of care:
• Comfort, surrounded by loved ones • End-of-life in hospital
• Issues: – Hunger : NG tube + feeds for satiety – Communication: IPAD + eye movements – Restlessness: lorazepam sublingually – Secretions: scopolamine (Intima – SC) – Dyspnea: O2 by nasal prongs – Legacy-building: organ donation
Secretions ↓ ability to swallow and clear oral secretions
Contributing factors: • Pulmonary malignancy • Pulmonary edema • Dysphagia • Generalized weakness • Altered consciousness
Interventions: • Humidified air • Suctioning (may ↑ secretions) • Medications
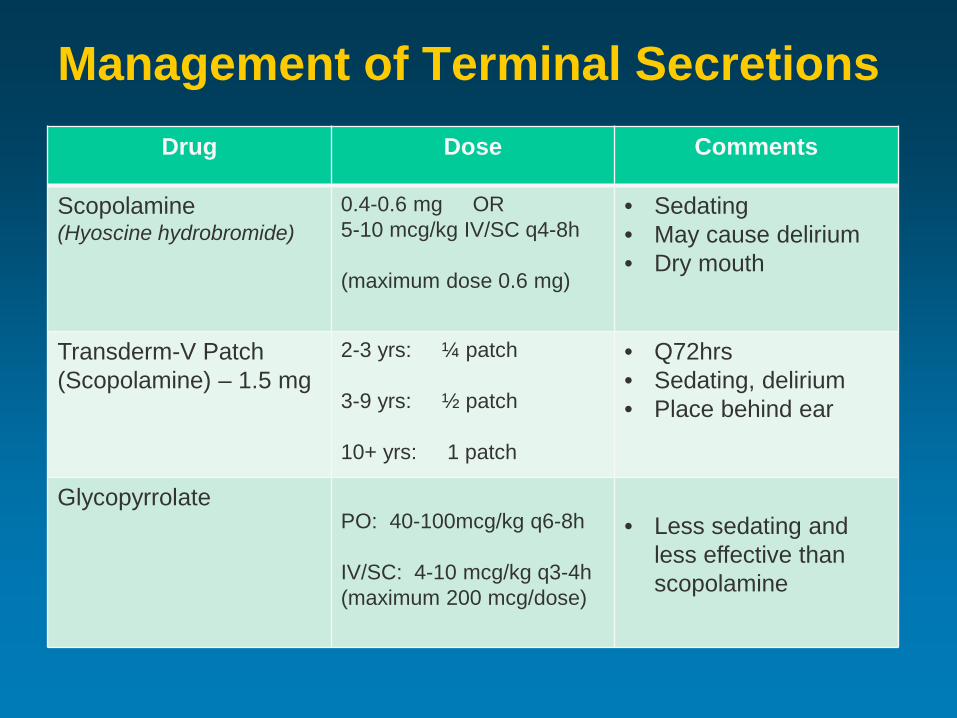
Management of Terminal Secretions Drug Dose Comments
Scopolamine (Hyoscine hydrobromide)
0.4-0.6 mg OR 5-10 mcg/kg IV/SC q4-8h (maximum dose 0.6 mg)
• Sedating • May cause delirium • Dry mouth
Transderm-V Patch (Scopolamine) – 1.5 mg
2-3 yrs: ¼ patch 3-9 yrs: ½ patch 10+ yrs: 1 patch
• Q72hrs • Sedating, delirium • Place behind ear
Glycopyrrolate PO: 40-100mcg/kg q6-8h IV/SC: 4-10 mcg/kg q3-4h (maximum 200 mcg/dose)
• Less sedating and
less effective than scopolamine
Dyspnea = distressing SOB; breathlessness Causes in cancer patients: Respiratory
• Metastatic lung disease - obstruction • Pleural effusion, pulmonary edema, ascites • Pulmonary embolism • Pneumonia
Cardiac • CHF, superior vena cava obstruction, anemia
Treatment related • Radiation pneumonitis, chemotherapy induced
cardiomyopathy or pulmonary fibrosis
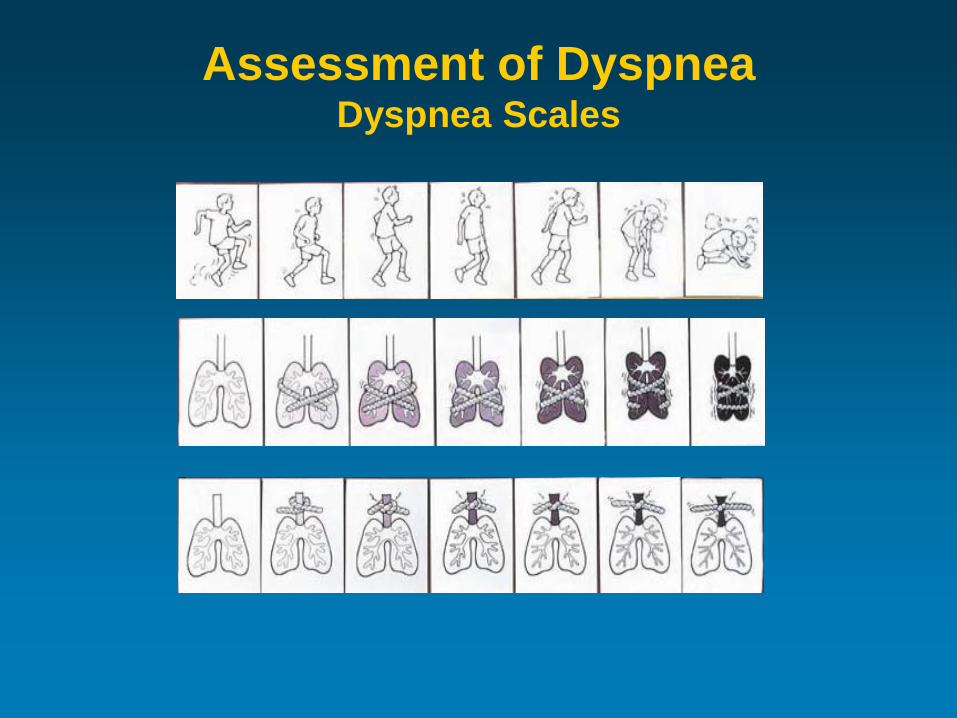
Assessment of Dyspnea Dyspnea Scales
Treatment of Dyspnea
Non-pharmacological: • Oxygen • Fan, open window • Sit upright • Calm reassurance • Relaxation and distraction • Cool temperature • Humidifier • Pursed-lip breathing exercises
Treatment of Dyspnea Pharmacological:
• *Opioids* – treatment of choice! Low dose morphine (30-50% pain dose) Already on opioid – titrate dose up to effect
• Benzodiazepines - adjunct Lorazepam – for anxiety/panic with dyspnea
0.05-1 mg/kg/dose q6-24h Midazolam – infusion for acute resp distress
1-5 mcg/kg/min – titrate to effect Children require higher doses
Disease-specific Medications for Dyspnea
• Diuretics (e.g. furosemide) – CHF, ascites • Corticosteroids – obstruction, pneumonitis • Antibiotics – pneumonia
• Anticoagulants - pulmonary embolism
• Transfusion – anemia
• Chemotherapy/radiation – metastases
Treat underlying cause!
Pediatric Pearls Multidisciplinary – “it takes a village”
Define overall goals of care – patient & family
Adapt treatment to individual child
Child that is sleeping, playing or quiet can still have pain
Rotate opioids if ineffective or intolerable SEs
Use consistent pain assessment scales
Children with cancer can require extremely high doses of opioids at end of life (e.g. solid tumours, NBL)
Pediatric Pearls Alternative routes of administration are safe and
effective (e.g. intranasal, subcutaneous, SL) – insuflons, Intima devices, MAD, CADD pumps
Opioids = drugs of choice for pain, dyspnea but Ø codeine or meperidine in children
Topical tranexamic acid ↓ localized bleeding
Caution with chlorpromazine, haloperidol, metoclopramide and prochlorperazine in children due to ↑ risk of EPS, dystonias, tardive dyskinesia
(give with IV diphenhydramine if benefits > risk)
Inpatient End-of-Life Care Advantages:
• Access to multidisciplinary team & specialists • Quick access to IV blood products, IV medications, cardioresp
monitors • Emotional support from staff, other parents • Medical personnel close for emergencies (ICU)
Disadvantages: • Not home-like environment • Limited room for family and friends • Medical, sterile • Lack of quiet and privacy • Medical learners on weekends/evenings – inexperienced • Difficult to transition from “active treatment” to “comfort care”
Goals for the Future
Continue to develop a collaborative relationship between McMaster Children’s Hospital and our colleagues in the community so that we can create more opportunities for our pediatric oncology patients to receive end-of-life care in their home communities.
Questions? Comments?
Thank you!