Embed Size (px)
Citation preview

for haemophilia patients
let’s talk physiotherapy
An introductory guide for physiotherapists and
haemophilia nurses
JAY LUCKEYUSAHaemophilia B with inhibitors
1
Introduction
Brief overview of haemophilia
• Inheritance of haemophilia
• Symptoms of haemophilia
• Medical treatment of haemophilia
• Inhibitors
• Comprehensive care in haemophilia
Pathophysiology of haemarthrosis and arthropathy
Importance of physiotherapy in haemophilia
Assessment of joints in people with haemophilia
Management of arthropathy in people with haemophilia
• Treatment of bleeding episodes
• Physiotherapy
• Control of arthropathic pain: analgesics
• Elective Orthopaedic Surgery (pre- and post-op physio)
Sports and haemophilia
When to refer for specialist input
Glossary of terms
Helpful resources, including online resources and suggested reading
References
contents
WALID KOBISI EgyptHaemophilia A
2
introduction brief overview of haemophilia
Haemophilia is a rare but serious inherited disorder which causes impaired blood clotting 1
Men and boys living with haemophilia are at risk of bleeds into their joints, especially knees, ankles and elbows. 2 Joint bleeds are painful and reduce mobility and, over time, multiple episodes of bleeding can result in progressive and permanent joint damage. 3
Physiotherapy has an important part to play in helping people with haemophilia recover from joint bleeds. 4, 5 A well designed exercise programme can help patients maintain healthy joints, reduce pain and reduce the risks of future bleeding episodes. 4, 6 Ideally, a specialist physiotherapist should assess the patient’s current physical condition and tailor a programme to meet their needs. 4
This booklet provides a basic introduction to the current management of haemophilia and the roles that physiotherapy can play. It is aimed at healthcare professionals, including physiotherapists who manage people with haemophilia and haemophilia nurses who collaborate with physiotherapists
to deliver musculoskeletal care. For a more in-depth consideration of the topics discussed here, please refer to the information sources listed in the ‘Helpful resources’ and ‘References’ sections.
Haemophilia is a hereditary disorder in which blood clotting is impaired.1 In normal blood clotting, thirteen different proteins – clotting factors – work together to form a blood clot. This series of events is known as the clotting cascade (Figure 1). People with haemophilia have a clotting factor that is missing or reduced, so blood clots fail to form properly. This makes bleeding last longer and be more diffi cult to control than normal. 7
Inheritance of haemophilia
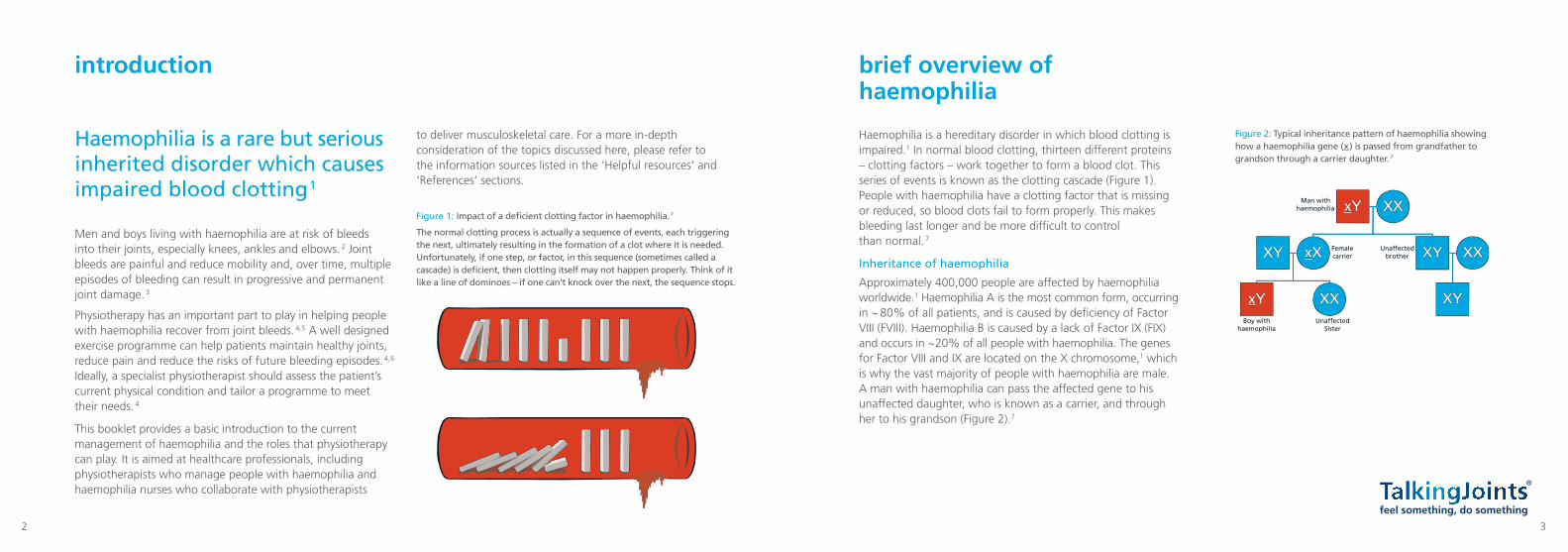
Approximately 400,000 people are affected by haemophilia worldwide.1 Haemophilia A is the most common form, occurring in ~ 80% of all patients, and is caused by defi ciency of Factor VIII (FVIII). Haemophilia B is caused by a lack of Factor IX (FIX) and occurs in ~ 20% of all people with haemophilia. The genes for Factor VIII and IX are located on the X chromosome,1 which is why the vast majority of people with haemophilia are male. A man with haemophilia can pass the affected gene to his unaffected daughter, who is known as a carrier, and through her to his grandson (Figure 2).7
xY XX
XXxX
XX
XY
xY XY
XYUnaffected brother
Unaffected Sister
Femalecarrier
Boy withhaemophilia
Man withhaemophilia
Figure 2: Typical inheritance pattern of haemophilia showing how a haemophilia gene (x ) is passed from grandfather to grandson through a carrier daughter. 7
Figure 1: Impact of a defi cient clotting factor in haemophilia. 7
The normal clotting process is actually a sequence of events, each triggering the next, ultimately resulting in the formation of a clot where it is needed. Unfortunately, if one step, or factor, in this sequence (sometimes called a cascade) is defi cient, then clotting itself may not happen properly. Think of it like a line of dominoes – if one can’t knock over the next, the sequence stops.
3
5
Symptoms of haemophilia
People with haemophilia do not bleed more than normal, but bleeding is prolonged and takes longer to stop.7 The severity of symptoms depends on the patient’s clotting factor levels: less than 1% of normal levels of FVIII or FIX is associated with severe disease, whereas higher levels are associated with moderate (1– 5%) or mild (> 5%) symptoms.1 People with severe haemophilia experience bruising, spontaneous bleeds and excessive bleeding following surgery or injury.1 People with haemophilia are prone to bleeds into their joints, with the majority of bleeds occurring in joints and known as haemarthrosis.8 Over time, cumulative bleeding into joints can cause long-term damage to the structure and function of the joint, known as haemophilic arthropathy (discussed later).1
Medical treatment of haemophilia
Treatment options include replacement of the missing clotting factor, FVIII or FIX, which can be administered when a bleeding episode occurs (on-demand treatment) or at regular intervals to proactively prevent bleeding (prophylactic therapy).1 Prophylaxis is considered to be the ‘gold-standard’ treatment but it is not always available or suitable for the individual patient.9 Replacement clotting factor can be recombinant (manufactured using genetic engineering) or derived from blood products (plasma-derived).1 Many patients with haemophilia are trained to administer clotting factor themselves, at home.1
Inhibitors
Development of inhibitors (antibodies) to clotting factor therapy is an uncommon but serious complication that reduces the efficacy of haemophilia treatment.1 Risk factors for inhibitors include severity and type of haemophilia, family history, genetic and environmental factors as well as the clotting factor treatment exposure.10 Bleeding episodes are harder to manage in patients with inhibitors; management options include: higher doses of clotting Factors VIII or IX, immune tolerance therapy* and so-called bypassing agents.1
Comprehensive care in haemophilia
People with haemophilia should ideally be managed in specialist comprehensive care centres.1 These centres should be staffed by haematologists, specialist nurses and physiotherapists, and social workers. They have access to laboratory services and clotting factor treatment, and can draw on specialist expertise when needed (e.g. orthopaedic surgeons, dentists, occupational therapists and infectious disease specialists).1
SERIOUS BLEEDS SHOULD ALWAYS BE TREATED IN HOSPITAL1
ANIL ÖZCAN TurkeyHaemophilia A
*Immune tolerance induction therapy (ITI) is used to get rid of high-titre inhibitors to clotting factor. It involves giving the patient repeated doses of Factor VIII or IX over a length of time (a few months to several years). If successful, the process reduces the immune reaction to administered clotting factor and eliminates the inhibitor. 54
4
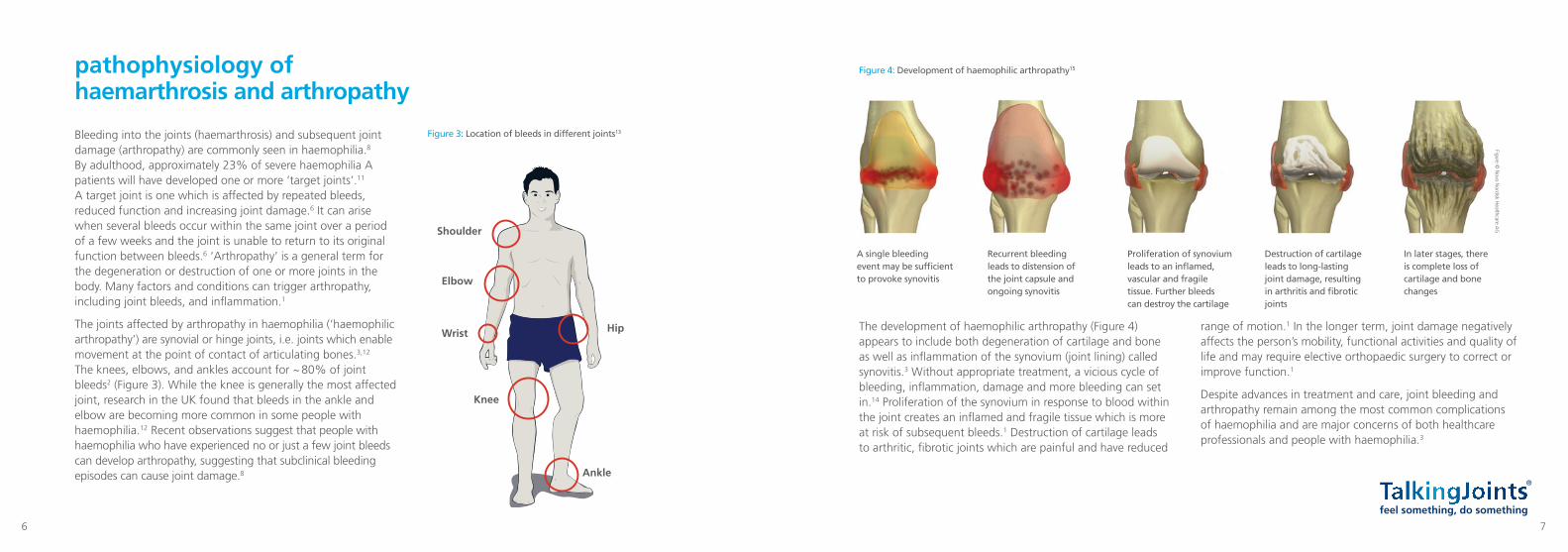
The development of haemophilic arthropathy (Figure 4) appears to include both degeneration of cartilage and bone as well as infl ammation of the synovium (joint lining) called synovitis.3 Without appropriate treatment, a vicious cycle of bleeding, infl ammation, damage and more bleeding can set in.14 Proliferation of the synovium in response to blood within the joint creates an infl amed and fragile tissue which is more at risk of subsequent bleeds.1 Destruction of cartilage leads to arthritic, fi brotic joints which are painful and have reduced
range of motion.1 In the longer term, joint damage negatively affects the person’s mobility, functional activities and quality of life and may require elective orthopaedic surgery to correct or improve function.1
Despite advances in treatment and care, joint bleeding and arthropathy remain among the most common complications of haemophilia and are major concerns of both healthcare professionals and people with haemophilia.3
Bleeding into the joints (haemarthrosis) and subsequent joint damage (arthropathy) are commonly seen in haemophilia.8 By adulthood, approximately 23% of severe haemophilia A patients will have developed one or more ‘target joints’.11 A target joint is one which is affected by repeated bleeds, reduced function and increasing joint damage.6 It can arise when several bleeds occur within the same joint over a period of a few weeks and the joint is unable to return to its original function between bleeds.6 ‘Arthropathy’ is a general term for the degeneration or destruction of one or more joints in the body. Many factors and conditions can trigger arthropathy, including joint bleeds, and infl ammation.1
The joints affected by arthropathy in haemophilia (‘haemophilic arthropathy’) are synovial or hinge joints, i.e. joints which enable movement at the point of contact of articulating bones.3,12 The knees, elbows, and ankles account for ~ 80% of joint bleeds2 (Figure 3). While the knee is generally the most affected joint, research in the UK found that bleeds in the ankle and elbow are becoming more common in some people with haemophilia.12 Recent observations suggest that people with haemophilia who have experienced no or just a few joint bleeds can develop arthropathy, suggesting that subclinical bleeding episodes can cause joint damage.8
pathophysiology of haemarthrosis and arthropathy
Figure 3: Location of bleeds in different joints13
Figure 4: Development of haemophilic arthropathy15
Shoulder
Elbow
Wrist
Knee
Hip
Ankle
A single bleeding event may be suffi cient to provoke synovitis
Recurrent bleeding leads to distension of the joint capsule and ongoing synovitis
Proliferation of synovium leads to an infl amed, vascular and fragile tissue. Further bleeds can destroy the cartilage
Destruction of cartilage leads to long-lasting joint damage, resulting in arthritis and fi brotic joints
In later stages, there is complete loss of cartilage and bone changes
Figure © N
ovo Nordisk H
ealthcare AG
6 7
assessment of joints in patients with haemophilia
Patients with haemophilia undergo regular (annual) joint assessment. Ongoing evaluation allows the physiotherapist to:20
• Detect deterioration in joint condition
• Detect failure of current treatment regimen
• Determine whether alternative management options are required.
It is important to assess disease progression by evaluating markers including bleeding frequency, pain, degree of swelling/synovitis, range of motion, crepitus, muscle power, balance and gait.20 Indeed, the Hemophilia Joint Health Score (HJHS) – one of the main tools used to assess joint status in children – is designed to be used by specially-trained physiotherapists.22,23 The HJHS was recently shown to be 74% more efficient than the World Federation of Hemophilia (WFH) physical examination scale in differentiating boys receiving prophylactic treatment from those treated on-demand.23 Because it prevents bleeds, boys receiving prophylaxis generally have better joint status than boys who treat bleeds on-demand.1
Physiotherapy forms a vital component of the management of patients with haemophilia 5
Exercise programmes help to manage recovery from a muscle bleed or joint bleed and help prevent future bleeding episodes.4
The overall aim of physiotherapy in haemophilia is to restore normal motor function. Specific goals include:
• Maintaining healthy joints and avoiding deformity 6,16
• Reducing pain 6
• Increasing function by maintaining range of motion (ROM)6
• Increasing muscle strength to minimise potential for bleeding 6
• Improving balance and proprioception which help to avoid injury 4,6
• Helping the person remain fit/active and maintain a healthy weight.1,6
Physiotherapists should be specially trained to manage patients with haemophilia.4 Special care must be taken in order to avoid causing a bleed or exacerbating symptoms during assessment or exercise. For example, the physiotherapist should handle the patient carefully and confirm factor replacement therapy has been administered before the session, if needed.17,18
Physiotherapy is also used to support recovery from surgical procedures, especially elective orthopaedic surgery (EOS).19 Pre- and post-operative physiotherapy are essential to optimise the outcomes of EOS.19 – 21
importance of physiotherapy in haemophilia
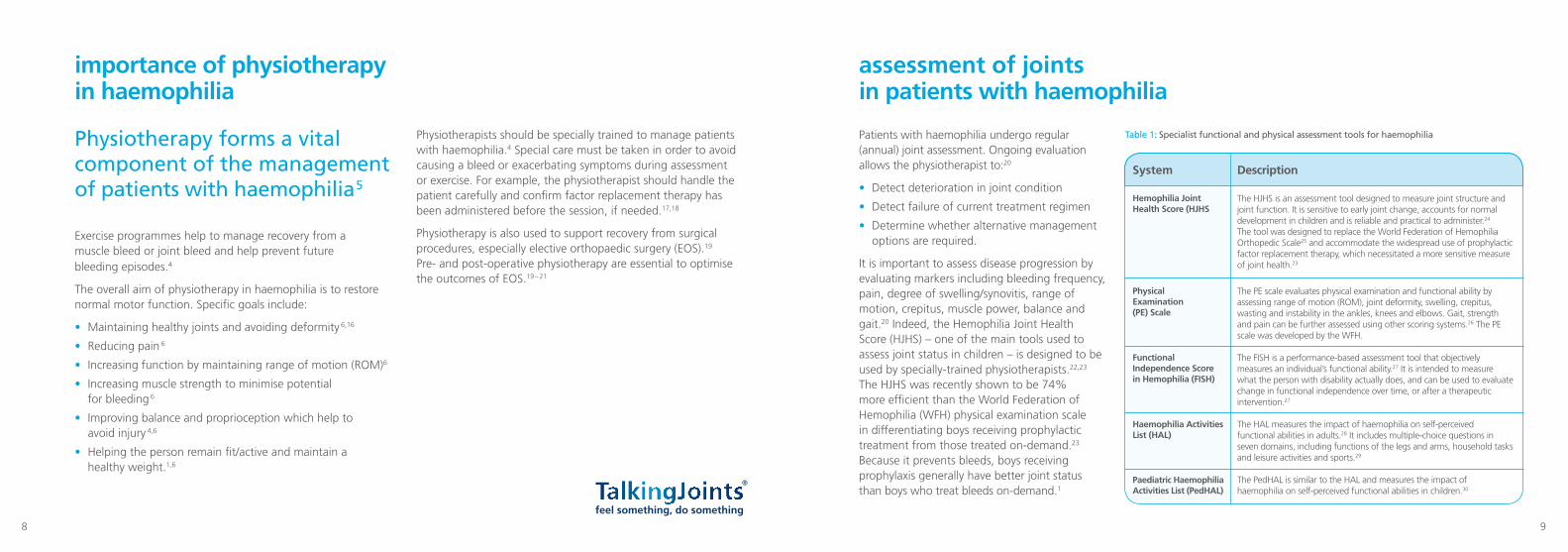
Table 1: Specialist functional and physical assessment tools for haemophilia
System
Hemophilia Joint Health Score (HJHS
Physical Examination (PE) Scale
Functional Independence Score in Hemophilia (FISH)
Haemophilia Activities List (HAL)
Paediatric Haemophilia Activities List (PedHAL)
Description
The HJHS is an assessment tool designed to measure joint structure and joint function. It is sensitive to early joint change, accounts for normal development in children and is reliable and practical to administer.24 The tool was designed to replace the World Federation of Hemophilia Orthopedic Scale25 and accommodate the widespread use of prophylactic factor replacement therapy, which necessitated a more sensitive measure of joint health.23
The PE scale evaluates physical examination and functional ability by assessing range of motion (ROM), joint deformity, swelling, crepitus, wasting and instability in the ankles, knees and elbows. Gait, strength and pain can be further assessed using other scoring systems.26 The PE scale was developed by the WFH.
The FISH is a performance-based assessment tool that objectively measures an individual’s functional ability.27 It is intended to measure what the person with disability actually does, and can be used to evaluate change in functional independence over time, or after a therapeutic intervention.27
The HAL measures the impact of haemophilia on self-perceived functional abilities in adults.28 It includes multiple-choice questions in seven domains, including functions of the legs and arms, household tasks and leisure activities and sports.29
The PedHAL is similar to the HAL and measures the impact of haemophilia on self-perceived functional abilities in children.30
8 9
Available functional and physical scoring systems that can be used to assess joint status in haemophilia are summarised in Table 1. These specialist scales should be used by physiotherapists and other healthcare professionals who regularly see haemophilia patients and who are experienced in the use of these assessments.
Simple checklist for assessing joint status
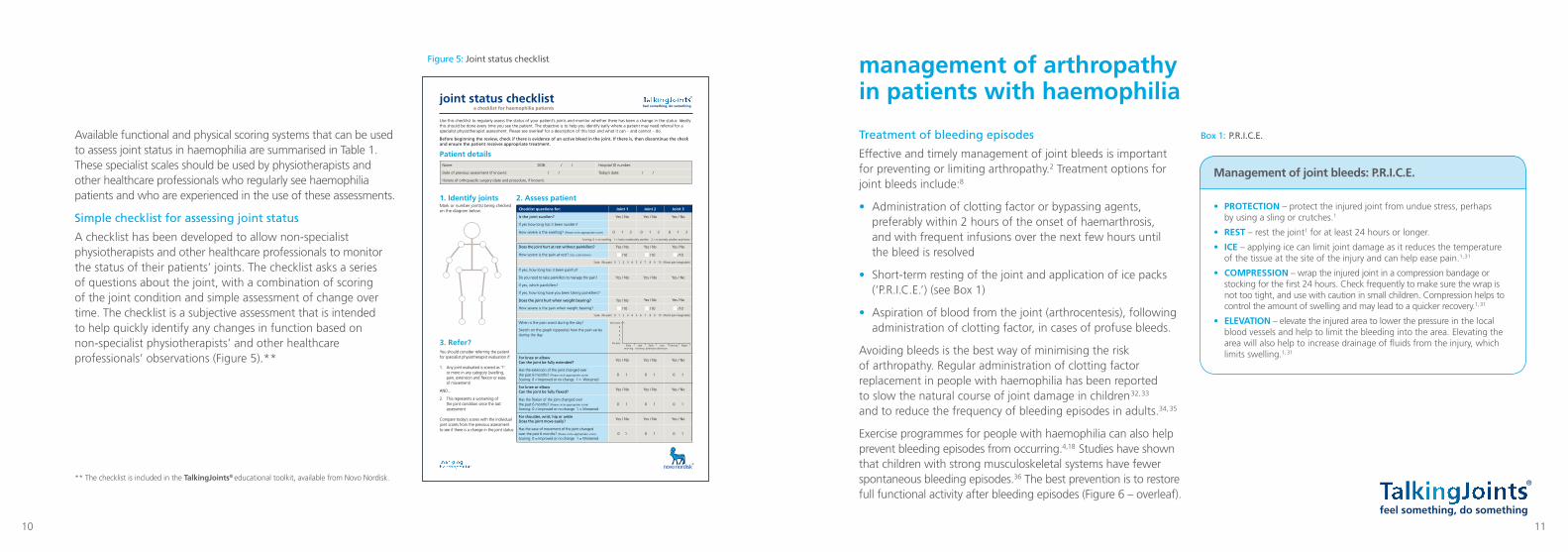
A checklist has been developed to allow non-specialist physiotherapists and other healthcare professionals to monitor the status of their patients’ joints. The checklist asks a series of questions about the joint, with a combination of scoring of the joint condition and simple assessment of change over time. The checklist is a subjective assessment that is intended to help quickly identify any changes in function based on non-specialist physiotherapists’ and other healthcare professionals’ observations (Figure 5).**
** The checklist is included in the TalkingJoints® educational toolkit, available from Novo Nordisk.
management of arthropathy in patients with haemophilia
Treatment of bleeding episodes
Effective and timely management of joint bleeds is important for preventing or limiting arthropathy.2 Treatment options for joint bleeds include:8
• Administration of clotting factor or bypassing agents, preferably within 2 hours of the onset of haemarthrosis, and with frequent infusions over the next few hours until the bleed is resolved
• Short-term resting of the joint and application of ice packs (‘P.R.I.C.E.’) (see Box 1)
• Aspiration of blood from the joint (arthrocentesis), following administration of clotting factor, in cases of profuse bleeds.
Avoiding bleeds is the best way of minimising the risk of arthropathy. Regular administration of clotting factor replacement in people with haemophilia has been reported to slow the natural course of joint damage in children 32, 33 and to reduce the frequency of bleeding episodes in adults.34, 35
Exercise programmes for people with haemophilia can also help prevent bleeding episodes from occurring.4,18 Studies have shown that children with strong musculoskeletal systems have fewer spontaneous bleeding episodes.36 The best prevention is to restore full functional activity after bleeding episodes (Figure 6 – overleaf).
Joint checklist to come
Patient details
Use this checklist to regularly assess the status of your patient’s joints and monitor whether there has been a change in the status. Ideally this should be done every time you see the patient. The objective is to help you identify early where a patient may need referral for a specialist physiotherapist assessment. Please see overleaf for a description of this tool and what it can – and cannot – do.
Before beginning the review, check if there is evidence of an active bleed in the joint. If there is, then discontinue the check and ensure the patient receives appropriate treatment.
Mark or number joint(s) being checked on the diagram below.
1. Identify joints
Name: DOB: / / Hospital ID number:
Date of previous assessment (if known): / / Today’s date: / /
History of orthopaedic surgery (date and procedure, if known):
You should consider referring the patient for specialist physiotherapist evaluation if: 1. Any joint evaluated is scored as ‘1’ or more in any category (swelling, pain, extension and flexion or ease of movement)
AND...
2. This represents a worsening of the joint condition since the last assessment Compare today’s scores with the individual joint scores from the previous assessment to see if there is a change in the joint status.
3. Refer?
2. Assess patientChecklist questions for: Joint 1 Joint 2 Joint 3
Is the joint swollen? Yes / No Yes / No Yes / No
If yes how long has it been swollen?
How severe is the swelling? (Please circle appropriate score) 0 1 2 0 1 2 0 1 2
Scoring: 0 = no swelling 1 = looks moderately swollen 2 = is severely swollen and tense
Does the joint hurt at rest without painkillers? Yes / No Yes / No Yes / No
How severe is the pain at rest? (Use scale below) /10 /10 /10
Scale: (No pain) 0 1 2 3 4 5 6 7 8 9 10 (Worst pain imaginable)
If yes, how long has it been painful?
Do you need to take painkillers to manage the pain? Yes / No Yes / No Yes / No
If yes, which painkillers?
If yes, how long have you been taking painkillers?
Does the joint hurt when weight bearing? Yes / No Yes / No Yes / No
How severe is the pain when weight bearing? /10 /10 /10
Scale: (No pain) 0 1 2 3 4 5 6 7 8 9 10 (Worst pain imaginable)
When is the pain worst during the day?
Sketch on the graph (opposite) how the pain varies during the day
For knee or elbow Can the joint be fully extended?
Yes / No Yes / No Yes / No
Has the extension of the joint changed over the past 6 months? (Please circle appropriate score) Scoring: 0 = Improved or no change 1 = Worsened
0 1 0 1 0 1
For knee or elbow Can the joint be fully flexed?
Yes / No Yes / No Yes / No
Has the flexion of the joint changed over the past 6 months? (Please circle appropriate score) Scoring: 0 = Improved or no change 1 = Worsened
0 1 0 1 0 1
For shoulder, wrist, hip or ankle Does the joint move easily?
Yes / No Yes / No Yes / No
Has the ease of movement of the joint changed over the past 6 months? (Please circle appropriate score) Scoring: 0 = Improved or no change 1 = Worsened
0 1 0 1 0 1
joint status checklista checklist for haemophilia patients
Worst pain
No painEarly
morningLate
morningEarly
afternoonLate
afternoonEvening Night
2
4
6
8
Figure 5: Joint status checklist
Box 1: P.R.I.C.E.
Management of joint bleeds: P.R.I.C.E.
• PROTECTION – protect the injured joint from undue stress, perhaps by using a sling or crutches.1
• REST – rest the joint1 for at least 24 hours or longer.
• ICE – applying ice can limit joint damage as it reduces the temperature of the tissue at the site of the injury and can help ease pain.1, 31
• COMPRESSION – wrap the injured joint in a compression bandage or stocking for the first 24 hours. Check frequently to make sure the wrap is not too tight, and use with caution in small children. Compression helps to control the amount of swelling and may lead to a quicker recovery.1, 31
• ELEVATION – elevate the injured area to lower the pressure in the local blood vessels and help to limit the bleeding into the area. Elevating the area will also help to increase drainage of fluids from the injury, which limits swelling.1, 31
10 11
13
Physiotherapy management of haemophilia
Physiotherapy exercise programmes form a vital part of the management of people with haemophilia.5 Physical benefits of exercise include improved strength, proprioception, joint range of motion and lean body mass, as well as reduced frequency of bleeding.18 Exercise strengthens muscle, and strong muscle protects joints.37 Proprioceptive (balance) training may promote joint stability and function.4 Weight-bearing exercise can improve bone health in children with severe haemophilia who have reduced bone mineral density.38 Exercise programmes for people with haemophilia are designed and implemented for a number of reasons, including: 4,18,19
• Reactive management of recovery after a muscle bleed, a joint bleed (haemarthrosis) or surgery
• Proactive prevention of future bleeding episodes
• General health and psychosocial well-being.
Conservative management, such as serial casting, bracing and orthotics (e.g. shoe inserts, crutches) may be used to correct deformities and support painful and unstable joints.1 Patients may need clotting factor administration prior to undertaking physiotherapy.17,18 It is important that the physiotherapist discusses this with the Haemophilia Treatment Centre (HTC), not just with the patient. The factor replacement guidelines set by the HTC should be followed before undertaking any physiotherapy or exercise programme, with infusion ideally before activity.18 Regular replacement therapy may not completely prevent bleeds, so it is important to monitor for any bleeding or other injuries, and follow HTC guidelines to manage these.18 It is especially important to monitor for any bleeding or injury in patients with inhibitors, as they are more likely to have musculoskeletal problems than people without inhibitors.39
Table 2 lists lists some ‘do’s’ and ‘don’ts’ that should be kept in mind by healthcare professionals and patients.
ÖMER GÜVERCI.N
TurkeyHaemophilia B
Figure 6: Stages of recovery from a bleeding episode 1
Effective treatment, proper recovery and appropriate rehabilitation give the best chance of full functional recovery. If any of these stages are inadequate, the risk of further bleeding and subsequent loss of function increases.
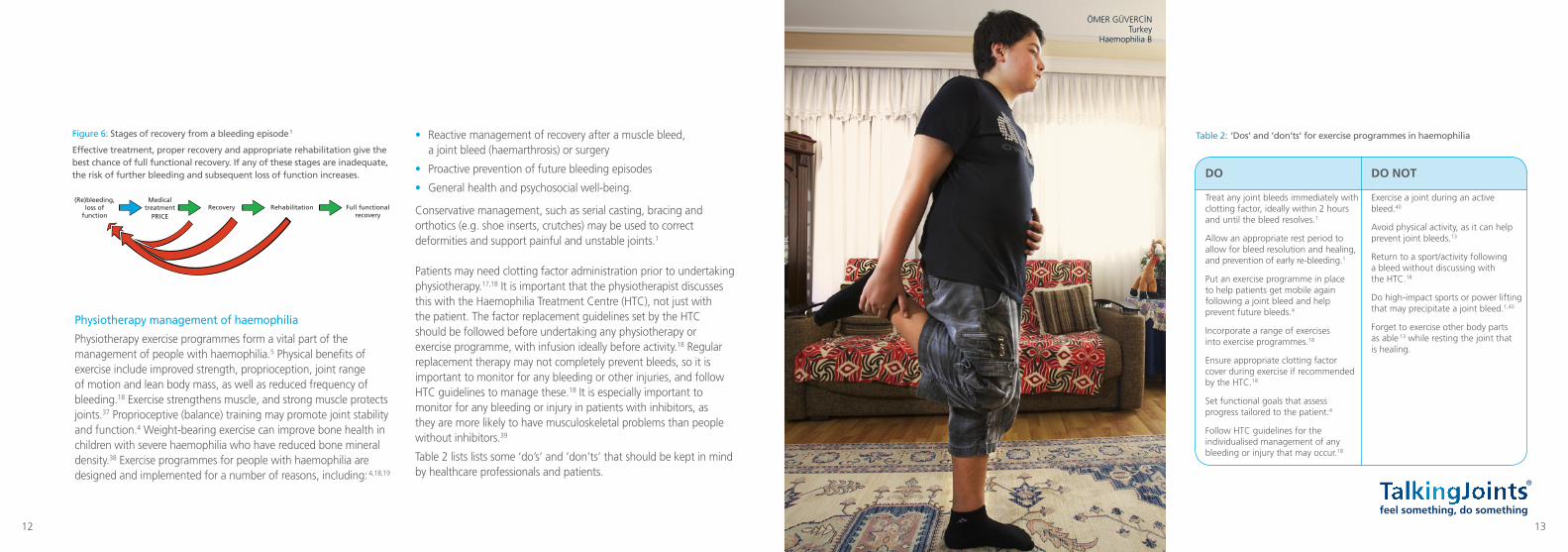
Table 2: ‘Dos’ and ‘don’ts’ for exercise programmes in haemophilia
(Re)bleeding, loss of
functionRecovery Rehabilitation Full functional
recovery
Medical treatment
PRICE
DO NOT
Exercise a joint during an active bleed.40
Avoid physical activity, as it can help prevent joint bleeds.13
Return to a sport/activity following a bleed without discussing with the HTC.18
Do high-impact sports or power lifting that may precipitate a joint bleed.1,40
Forget to exercise other body parts as able 13 while resting the joint that is healing.
DO
Treat any joint bleeds immediately with clotting factor, ideally within 2 hours and until the bleed resolves.1
Allow an appropriate rest period to allow for bleed resolution and healing, and prevention of early re-bleeding.1
Put an exercise programme in place to help patients get mobile again following a joint bleed and help prevent future bleeds.4
Incorporate a range of exercises into exercise programmes.18
Ensure appropriate clotting factor cover during exercise if recommended by the HTC.18
Set functional goals that assess progress tailored to the patient.4
Follow HTC guidelines for the individualised management of any bleeding or injury that may occur.18
12
Elective Orthopaedic Surgery (pre- and post-op physiotherapy)
When carried out by an experienced and well-equipped multidisciplinary team, with appropriate physiotherapy support, elective orthopaedic surgery (EOS) can be safely performed in patients with haemophilia, even those with inhibitors.43
EOS procedures can offer a number of benefits to patients with haemophilia:14, 44 – 47
• Significantly improve joint function
• Reduce pain due to chronic arthropathy • Improve mobility
• Reduce the frequency of bleeding episodes
• Improve quality of life.
There is a trend towards a more aggressive approach to surgery in younger patients based on the rationale that these patients can benefit from optimal physical health. In addition, the musculature of these younger patients is still in a good condition and thus can usually be more easily rehabilitated following orthopaedic surgery than that of older patients.48
Table 3 lists important considerations for developing an exercise programme that is tailored to the individual needs of the person with haemophilia.13 Specialist physiotherapy input should always be sought when establishing a new programme for a patient with haemophilia, especially if the patient has inhibitors.
It is important that any exercise programme for a person with haemophilia is designed with their functional goals in mind.41 Functional goals can include returning to work or school, participating fully in social activities or taking up a new sporting activity. Specific exercises and physical activities should be recommended to help patients reach their goals, with progress assessed by how much these goals have been achieved.41
Control of arthropathic pain: analgesics
People with haemophilia need to be able to distinguish between pain from arthropathy and pain that could indicate an active bleed19 (see callout box). It is important that physiotherapists listen to the individual when he reports pain during exercise and do not encourage patients to over-exert themselves.13 The patient knows their condition best. For the control of arthropathic pain, analgesics are commonly used.
Characteristics of pain associated with a bleed 42
• Does not reduce when the joint is rested
• Is accompanied by one or more of:
– Palpable swelling of the joint
– Warmth of the skin over the joint
– Sensation of tingling (‘aura’)
– Progressive loss of range of motion
• Reduces with appropriate clotting factor treatment.
Non-steroidal anti-inflammatory drugs should be used with caution.1 A combination of analgesics (with their different mechanisms of action) may be the most effective way of relieving pain.8 As discussed above, protection, rest, ice and compression can also help reduce the pain of a bleeding episode.
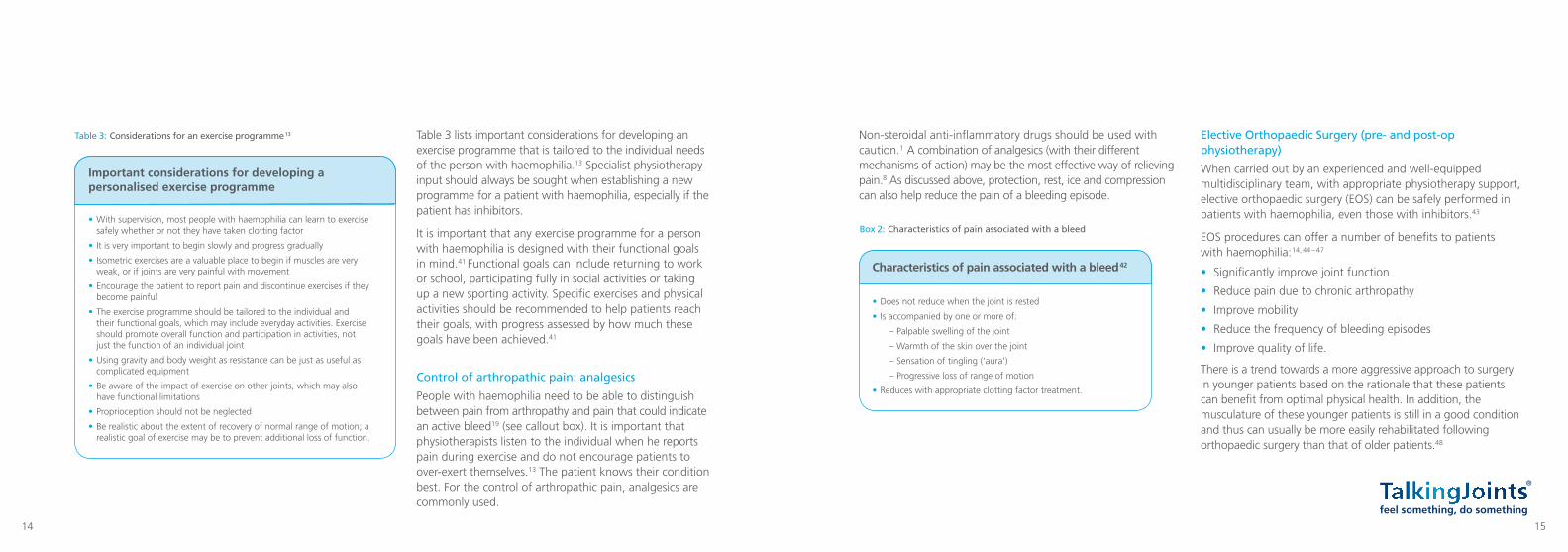
Table 3: Considerations for an exercise programme 13
Important considerations for developing a personalised exercise programme
• With supervision, most people with haemophilia can learn to exercise safely whether or not they have taken clotting factor
• It is very important to begin slowly and progress gradually
• Isometric exercises are a valuable place to begin if muscles are very weak, or if joints are very painful with movement
• Encourage the patient to report pain and discontinue exercises if they become painful
• The exercise programme should be tailored to the individual and their functional goals, which may include everyday activities. Exercise should promote overall function and participation in activities, not just the function of an individual joint
• Using gravity and body weight as resistance can be just as useful as complicated equipment
• Be aware of the impact of exercise on other joints, which may also have functional limitations
• Proprioception should not be neglected
• Be realistic about the extent of recovery of normal range of motion; a realistic goal of exercise may be to prevent additional loss of function.
Box 2: Characteristics of pain associated with a bleed
14 15
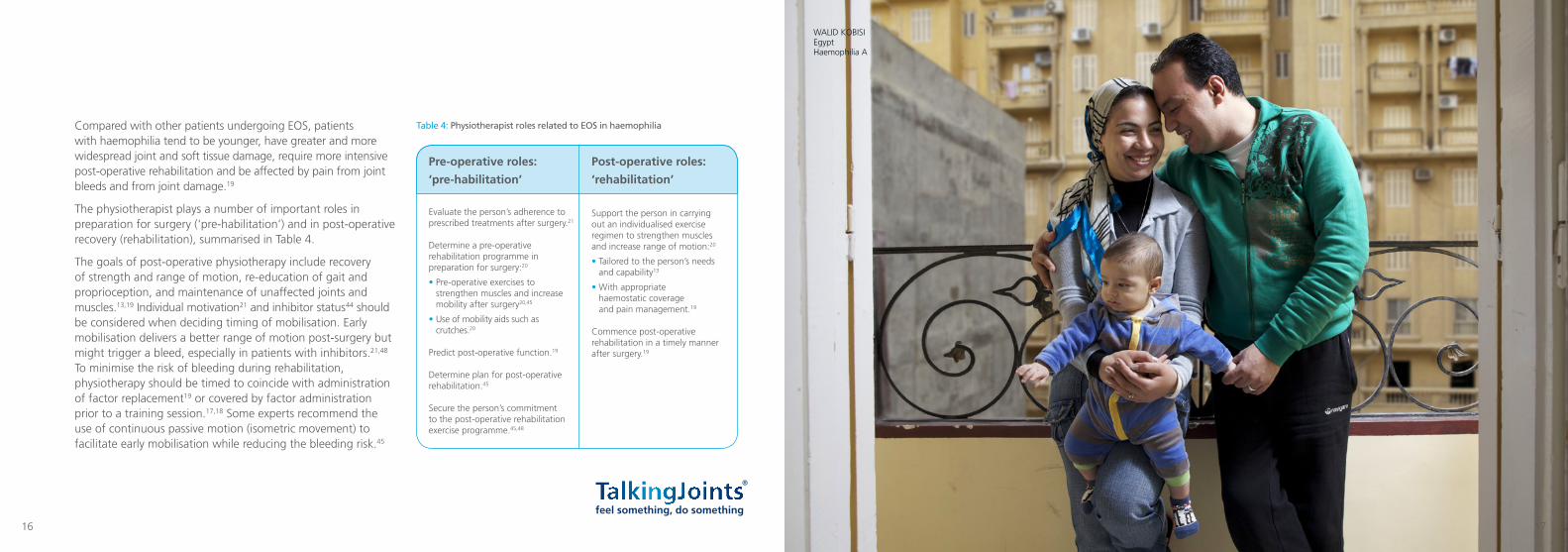
Table 4: Physiotherapist roles related to EOS in haemophilia
WALID KOBISI EgyptHaemophilia A
Compared with other patients undergoing EOS, patients with haemophilia tend to be younger, have greater and more widespread joint and soft tissue damage, require more intensive post-operative rehabilitation and be affected by pain from joint bleeds and from joint damage.19
The physiotherapist plays a number of important roles in preparation for surgery (‘pre-habilitation’) and in post-operative recovery (rehabilitation), summarised in Table 4.
The goals of post-operative physiotherapy include recovery of strength and range of motion, re-education of gait and proprioception, and maintenance of unaffected joints and muscles.13,19 Individual motivation21 and inhibitor status 44 should be considered when deciding timing of mobilisation. Early mobilisation delivers a better range of motion post-surgery but might trigger a bleed, especially in patients with inhibitors.21,48 To minimise the risk of bleeding during rehabilitation, physiotherapy should be timed to coincide with administration of factor replacement19 or covered by factor administration prior to a training session.17,18 Some experts recommend the use of continuous passive motion (isometric movement) to facilitate early mobilisation while reducing the bleeding risk.45
Pre-operative roles:
‘pre-habilitation’
Evaluate the person’s adherence to prescribed treatments after surgery.21
Determine a pre-operative rehabilitation programme in preparation for surgery:20
• Pre-operative exercises to strengthen muscles and increase mobility after surgery20,45
• Use of mobility aids such as crutches.20
Predict post-operative function.19
Determine plan for post-operative rehabilitation.45
Secure the person’s commitment to the post-operative rehabilitation exercise programme.45,48
Post-operative roles:
‘rehabilitation’
Support the person in carrying out an individualised exercise regimen to strengthen muscles and increase range of motion:20
• Tailored to the person’s needs and capability13
• With appropriate haemostatic coverage and pain management.19
Commence post-operative rehabilitation in a timely manner after surgery.19
16 17
sports and haemophilia
Exercise can improve not only physical well-being, but also the emotional and social well-being of people with haemophilia18, 49
Physical activity helps children develop socially and emotionally. In competitive sports, they learn teamwork.40 When people choose to participate in a sport they enjoy, it offers a number of benefits including better physical and mental health and improved bone and joint health and function.40
Several components make up a well-rounded, complete fitness programme, including endurance or cardiovascular activities, muscle strengthening and flexibility exercises, and balance and stability exercises.18 Starting exercise at an early age can build a strong routine that will be beneficial throughout life.40
When selecting sports activities for people with haemophilia, safety is an important consideration: activities must be age-appropriate and properly supervised.40 Ideally activity should take place soon after clotting factor treatment, although exercise can be safe even in the absence of replacement factor.18 Other safety considerations include appropriate warm-up and cool-down exercises, the using of protective gear, and choosing organised, supervised sports programmes rather than unstructured activities.1,18
The National Hemophilia Foundation book ‘Playing it Safe’ lists a number of sports activities graded by whether they can or cannot be recommended for people with haemophilia when carried out at an appropriate intensity for the individual’s level of fitness and experience.40 Less risky sports include archery, stationary bike, fishing, golf, hiking, tai chi and swimming. Recent evidence shows the benefits for people with haemophilia of a range of activities, including sports, aquatic exercise and resistance training.50 – 53
There are risks and benefits to all activities, and advice should be sought from the Haemophilia Treatment Centre before recommending a new or changed activity.18
when to refer for specialist input
Specialist input should be sought whenever there is doubt about the patient’s treatment or prognosis. Specific circumstances include:
• Initiating a physiotherapy regime 4
• Assessing the patient’s baseline function 20
• Poor recovery in response to a physiotherapy programme 20
• Inadequate pain management 1
• When starting or choosing a sport or exercise programme. 18
VICTOR DA SILVA MELCUNASBrazilVictor has severe haemophilia A
18 19
Reference listHelpful resources
• Guidelines for the Management of Hemophilia (2013) – World Federation of Hemophilia. Available from www.wfh.org or published as Srivastava A, Brewer AK, Mauser-Bunschoten EP, Key NS, Kitchen S, Llinas A, et al., Guidelines for the management of hemophilia. Haemophilia, 2013; 19(1): e1– 47.
• Management of acute soft tissue injury using Protection Rest Ice Compression and Elevation. Recommendations from the Association of Chartered Physiotherapists in Sports and Exercise Medicine (ACPSM). Available from http://www.physiosinsport.org/media/wysiwyg/ACPSM_Physio_Price_A4.pdf
• Negrier C, Seuser A, Forsyth A, Lobet S, Llinas A, Rosas M, et al., The benefits of exercise for patients with haemophilia and recommendations for safe and effective physical activity. Haemophilia, 2013; 19(4): 487– 98.
• Blamey G et al. Comprehensive elements of a physio-therapy exercise programme in haemophilia – a global perspective. Haemophilia, 2010; 16 Suppl 5: 136 – 45
• Mulder K. (2006) World Federation of Haemophilia: Exercises for people with haemophilia. Available from www.wfh.org [under Resources > Search the Library]
• Compendium of Assessment Tools, World Federation of Hemophilia. Available from www.wfh.org [under Resources]
• National Hemophilia Foundation Playing It Safe: Bleeding Disorders, Sports and Exercise 2005, New York: National Hemophilia Foundation. Available from https://www.hemophilia.org/sites/default/files/document/files/PlayingItSafe.pdf
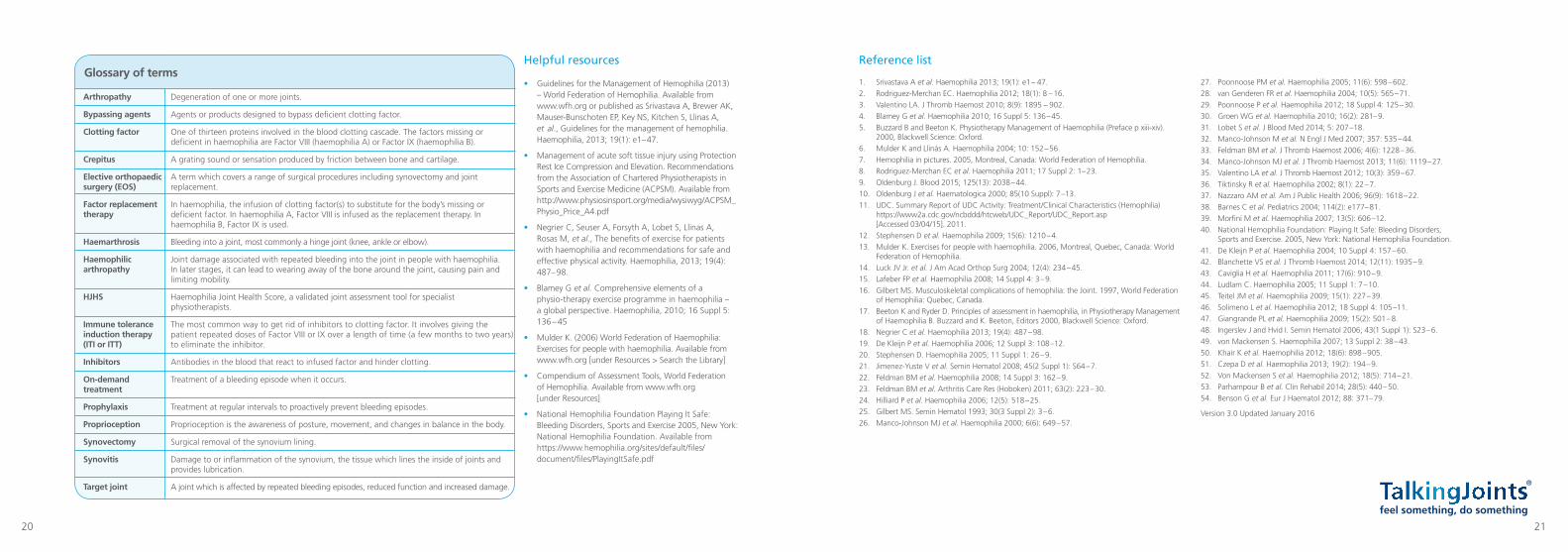
Glossary of terms
Degeneration of one or more joints.
Agents or products designed to bypass deficient clotting factor.
One of thirteen proteins involved in the blood clotting cascade. The factors missing or deficient in haemophilia are Factor VIII (haemophilia A) or Factor IX (haemophilia B).
A grating sound or sensation produced by friction between bone and cartilage.
A term which covers a range of surgical procedures including synovectomy and joint replacement.
In haemophilia, the infusion of clotting factor(s) to substitute for the body’s missing or deficient factor. In haemophilia A, Factor VIII is infused as the replacement therapy. In haemophilia B, Factor IX is used.
Bleeding into a joint, most commonly a hinge joint (knee, ankle or elbow).
Joint damage associated with repeated bleeding into the joint in people with haemophilia. In later stages, it can lead to wearing away of the bone around the joint, causing pain and limiting mobility.
Haemophilia Joint Health Score, a validated joint assessment tool for specialist physiotherapists.
The most common way to get rid of inhibitors to clotting factor. It involves giving the patient repeated doses of Factor VIII or IX over a length of time (a few months to two years) to eliminate the inhibitor.
Antibodies in the blood that react to infused factor and hinder clotting.
Treatment of a bleeding episode when it occurs.
Treatment at regular intervals to proactively prevent bleeding episodes.
Proprioception is the awareness of posture, movement, and changes in balance in the body.
Surgical removal of the synovium lining.
Damage to or inflammation of the synovium, the tissue which lines the inside of joints and provides lubrication.
A joint which is affected by repeated bleeding episodes, reduced function and increased damage.
Arthropathy
Bypassing agents
Clotting factor
Crepitus
Elective orthopaedic surgery (EOS)
Factor replacement therapy
Haemarthrosis
Haemophilic arthropathy
HJHS
Immune tolerance induction therapy (ITI or ITT)
Inhibitors
On-demand treatment
Prophylaxis
Proprioception
Synovectomy
Synovitis
Target joint
1. Srivastava A et al. Haemophilia 2013; 19(1): e1 – 47.2. Rodriguez-Merchan EC. Haemophilia 2012; 18(1): 8 – 16.3. Valentino LA. J Thromb Haemost 2010; 8(9): 1895 – 902.4. Blamey G et al. Haemophilia 2010; 16 Suppl 5: 136 – 45.5. Buzzard B and Beeton K. Physiotherapy Management of Haemophilia (Preface p xiii-xiv).
2000, Blackwell Science: Oxford.6. Mulder K and Llinás A. Haemophilia 2004; 10: 152 – 56.7. Hemophilia in pictures. 2005, Montreal, Canada: World Federation of Hemophilia.8. Rodriguez-Merchan EC et al. Haemophilia 2011; 17 Suppl 2: 1– 23.9. Oldenburg J. Blood 2015; 125(13): 2038 – 44.10. Oldenburg J et al. Haematologica 2000; 85(10 Suppl): 7 –13.11. UDC. Summary Report of UDC Activity: Treatment/Clinical Characteristics (Hemophilia)
https://www2a.cdc.gov/ncbddd/htcweb/UDC_Report/UDC_Report.asp [Accessed 03/04/15]. 2011.
12. Stephensen D et al. Haemophilia 2009; 15(6): 1210 – 4.13. Mulder K. Exercises for people with haemophilia. 2006, Montreal, Quebec, Canada: World
Federation of Hemophilia.14. Luck JV Jr. et al. J Am Acad Orthop Surg 2004; 12(4): 234 – 45.15. Lafeber FP et al. Haemophilia 2008; 14 Suppl 4: 3 – 9.16. Gilbert MS. Musculoskeletal complications of hemophilia: the Joint. 1997, World Federation
of Hemophilia: Quebec, Canada.17. Beeton K and Ryder D. Principles of assessment in haemophilia, in Physiotherapy Management
of Haemophilia B. Buzzard and K. Beeton, Editors 2000, Blackwell Science: Oxford.18. Negrier C et al. Haemophilia 2013; 19(4): 487 – 98.19. De Kleijn P et al. Haemophilia 2006; 12 Suppl 3: 108 –12.20. Stephensen D. Haemophilia 2005; 11 Suppl 1: 26 – 9.21. Jimenez-Yuste V et al. Semin Hematol 2008; 45(2 Suppl 1): S64 – 7.22. Feldman BM et al. Haemophilia 2008; 14 Suppl 3: 162 – 9.23. Feldman BM et al. Arthritis Care Res (Hoboken) 2011; 63(2): 223 – 30.24. Hilliard P et al. Haemophilia 2006; 12(5): 518 – 25.25. Gilbert MS. Semin Hematol 1993; 30(3 Suppl 2): 3 – 6.26. Manco-Johnson MJ et al. Haemophilia 2000; 6(6): 649 – 57.
27. Poonnoose PM et al. Haemophilia 2005; 11(6): 598 – 602.28. van Genderen FR et al. Haemophilia 2004; 10(5): 565 – 71.29. Poonnoose P et al. Haemophilia 2012; 18 Suppl 4: 125 – 30.30. Groen WG et al. Haemophilia 2010; 16(2): 281– 9.31. Lobet S et al. J Blood Med 2014; 5: 207 –18.32. Manco-Johnson M et al. N Engl J Med 2007; 357: 535 – 44.33. Feldman BM et al. J Thromb Haemost 2006; 4(6): 1228 – 36.34. Manco-Johnson MJ et al. J Thromb Haemost 2013; 11(6): 1119 – 27.35. Valentino LA et al. J Thromb Haemost 2012; 10(3): 359 – 67.36. Tiktinsky R et al. Haemophilia 2002; 8(1): 22 – 7.37. Nazzaro AM et al. Am J Public Health 2006; 96(9): 1618 – 22.38. Barnes C et al. Pediatrics 2004; 114(2): e177– 81.39. Morfini M et al. Haemophilia 2007; 13(5): 606 –12.40. National Hemophilia Foundation: Playing It Safe: Bleeding Disorders,
Sports and Exercise. 2005, New York: National Hemophilia Foundation.41. De Kleijn P et al. Haemophilia 2004; 10 Suppl 4: 157 – 60.42. Blanchette VS et al. J Thromb Haemost 2014; 12(11): 1935 – 9.43. Caviglia H et al. Haemophilia 2011; 17(6): 910 – 9.44. Ludlam C. Haemophilia 2005; 11 Suppl 1: 7 – 10.45. Teitel JM et al. Haemophilia 2009; 15(1): 227 – 39.46. Solimeno L et al. Haemophilia 2012; 18 Suppl 4: 105 –11.47. Giangrande PL et al. Haemophilia 2009; 15(2): 501 – 8.48. Ingerslev J and Hvid I. Semin Hematol 2006; 43(1 Suppl 1): S23 – 6.49. von Mackensen S. Haemophilia 2007; 13 Suppl 2: 38 – 43.50. Khair K et al. Haemophilia 2012; 18(6): 898 – 905.51. Czepa D et al. Haemophilia 2013; 19(2): 194 – 9.52. Von Mackensen S et al. Haemophilia 2012; 18(5): 714 – 21.53. Parhampour B et al. Clin Rehabil 2014; 28(5): 440 – 50.54. Benson G et al. Eur J Haematol 2012; 88: 371– 79.
Version 3.0 Updated January 2016
20 21
“ let’s talk physiotherapy” is part of the TalkingJoints® programme to encourage better understanding of how physiotherapy can help look after the body and joints of patients with haemophilia.
TalkingJoints® is a programme of information, education and support that talks to healthcare professionals, patients and carers about haemophilia and its impact on joint function. TalkingJoints® aims to help individuals detect changes early (feel something) and act accordingly (do something). We hope that by helping people with their joint function we can help improve the way they live with haemophilia, for the better.
Changing H
aemophilia™
is a registered trademark ow
ned by Novo N
ordisk Health C
are AG
and the Apis bull logo is a registered tradem
ark of Novo N
ordisk A/SDate of preparation: January 2016 HQMMA/CH/0215/0043(1)





























