Embed Size (px)
Citation preview
An Uncommon Mimicker
Nachiketh Soodana Prakash MD MS1, Sanoj Punnen
MD1 and Leonardo Kayat Bittencourt, MD, PhD2
1Depatment of Urology, University of Miami, Miami, FL, USA.2Department of Radiology, Fluminense Federal University, Rio de Janeiro, Brazil.
Case
• 64 year old male.
• Follow-up of serial PSA elevation: 10ng/ml
• DRE: abnormal firmness on the right lobe.
• Previous negative biopsy with right mid core showing
focus of high grade PIN with adjacent small atypical
glands.
• H/O Renal transplant on immunosuppression drugs.
Episode of UTI 3 months back urine culture showing
E.coli and was treated for the same.
• mpMRI was ordered for biopsy planning.
Imaging findings
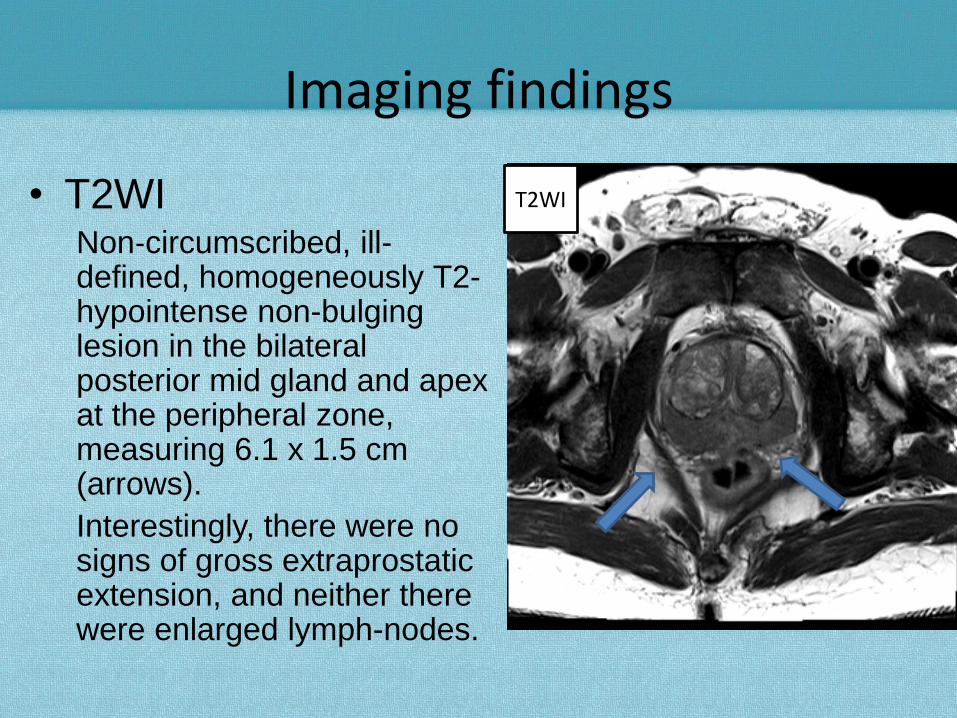
• T2WINon‐circumscribed, ill-defined, homogeneously T2-hypointense non-bulging lesion in the bilateral posterior mid gland and apex at the peripheral zone, measuring 6.1 x 1.5 cm (arrows).
Interestingly, there were no signs of gross extraprostatic extension, and neither there were enlarged lymph-nodes.
T2WI

ADC map
High B-valueDWI
Imaging Findings
• DWI
High signal intensities on
high b-value DWI, as well
as markedly impeded
diffusion on the ADC map
(arrows).
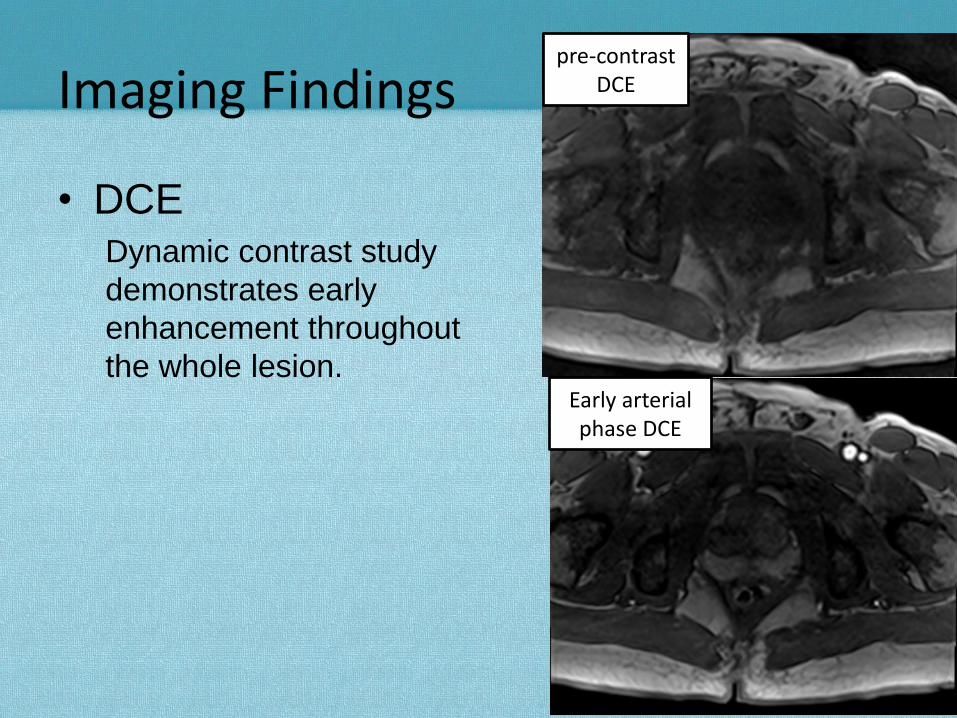
pre-contrast DCE
Early arterial phase DCE
Imaging Findings
• DCEDynamic contrast study
demonstrates early
enhancement throughout
the whole lesion.

PI-RADS Scoring
• T2WI = 5
• DWI = 5
• DCE = + (positive)
• PI-RADS Score = 5
Dominant parameter for PZ lesions
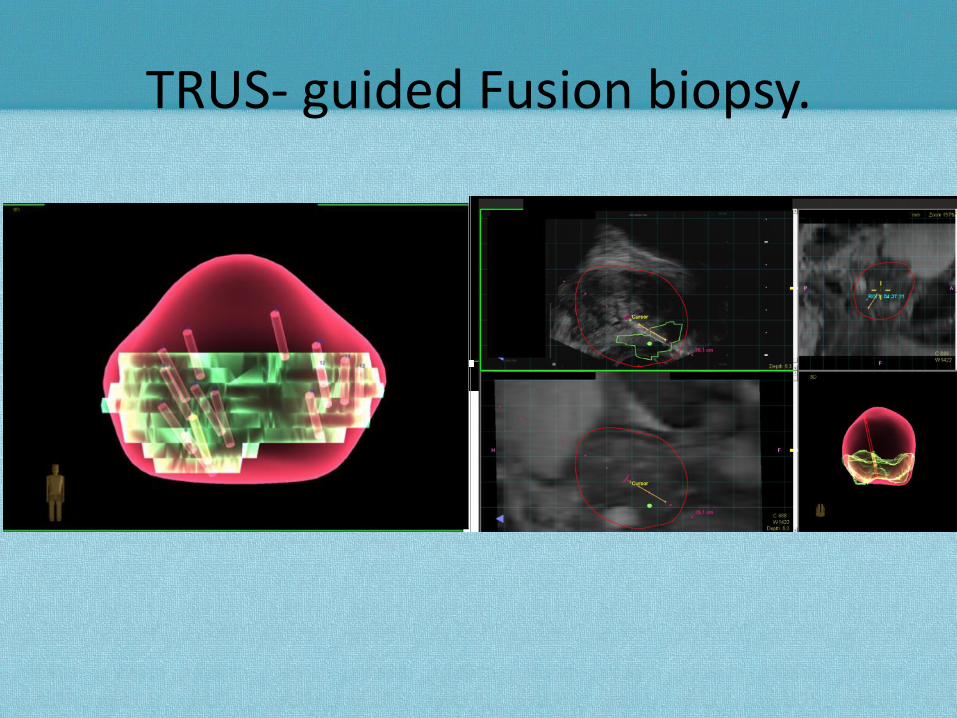
TRUS- guided Fusion biopsy.

Discussion
• Extensive highly-suspicious lesion in the whole PZ.
PI-RADS Score = 5.
• No signs of gross extraprostatic extension or enlarged
lymph-nodes.
• No evidence of bone metastases.
• PSA levels around 10 ng/ml.
• History of immunosuppression and UTI.
• Therefore, an alternative hypothesis of
chronic/granulomatous prostatitis was included in the
differential diagnoses.
• MR-TRUS fusion guided biopsy revealed prostatic
malakoplakia.

Pathology: Malakoplakia
• Pathology: Atrophic Prostate Glands with Chronic Inflammation with
significant amount of Histiocytes. (20x).

Pathology: Malakoplakia• Pathology: 60x - high power magnification showing Michaelis–Gutmann
bodies(MG bodies) which are pathognomic feature of Malakoplakia.

Malakoplakia• A form of chronic inflammation thought to be associated
with E. coli or K. pneumoniae infection.
• Association with immunosuppression has also been hypothesized.
• Most commonly found in the Bladder. Extra-genital sites have also been rarely described.
• Malakoplakia of the prostate is an extremely rare condition, and is known to mimic prostate cancer in terms of imaging findings.
• Patients can be treated with antibiotic therapy.
• There are no pathognomonic imaging findings. However, this condition should be suspected in patients with a typical clinical history, associated to mpMRI findings that resemble those of chronic/granulomatous prostatitis.
M. Niemierko, B. Kuzaka. Malacoplakia of the prostatePrzegl Lek, 62 (2005), pp. 825–826
Acknowledgements
• Oleksandr Kryvenko MD : University of Miami, Department of
Pathology.