Embed Size (px)
Citation preview

An Unusual Finding NACNS Conference
March 2, 2018
Heidi Shafland, MSN, APRN, CCRN-K, ACCNS-P

2 | © 2015

3 | © 2015
Disclosures
• I have nothing to disclose

4 | © 2015
• Define osteopenia and it’s significance in the pediatric population
• Review evidence-based problem solving strategies
• Discuss current trends in the identification and management of osteopenia
• Summarize one institution’s protocol
Objectives

5 | © 2015
• JD was a 6 month old patient with: dextrocardia, malposition of the great vessels, hypoplastic pulmonary valve, tricuspid atresia, bilateral Superior Vena Cavae, right aortic arch, with heterotaxy , s/p:
− Right sided bidirectional cavopulmonary anastamosis
− Clot in the lower Superior Vena Cava
− Left modified Blalock Taussig shunt
− Cardiac catheterization
− Small bowel obstruction – s/p exploratory laparotomy
− Chylous effusions
− Gastrostomy tube placement
− Presumed asplenia
− Hypercoaguable state
PATIENT’S H&P

6 | © 2015

7 | © 2015
• 9/9/15 CXR demonstrated irregularity and sclerosis indicating a healed rib fracture
• 9/10/15 CXR - Irregularity of bone ends bilaterally noted
• Questioned rickets
• Parathyroid and Vitamin D levels checked
• 9/11/15 Additional healing rib fractures noted
• POC changed to gentle handling
• 9/15/15 Lab results
• Parathyroid level low
• Vitamin D level low and supplementation started
• 9/21/15 RN reports, “The patient is more irritable with movement today.”
• L femoral X-ray showed – fracture 1-2 weeks old.
• Fracture precautions ordered
A devastating finding…

8 | © 2015
Diagnosis: Osteopenia in a Pediatric Patient

9 | © 2015
2008 2015
Patients with incidental fractures
7 Patients with
multiple fractures 3 Extremely
premature patients with ELBW
-24-25 weeks -380-750 grams
4
Background at Children’s MN

10 | © 2015
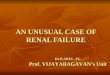
0
1
2
3
4
5
6
7
8
2008 2009 2010 2011 2012 2013 2014 2015
Fractures in Cardiac Population Prior to Protocol

11 | © 2015
• Osteopenia
− Decrease in the amount of organic bone matrix
• Osteomalacia
− Lack of mineralization of the organic bone matrix
• Rickets
− When loss of mineralization involves the growth plate
• Osteoporosis
− Decrease in bone mineral density >2.5 SD below the norm (not defined for infants)
• Metabolic bone disease
− Preferred term for osteopenia
Definitions

12 | © 2015
• Incidence
• Causes:
− Low nutrient stores/inadequate provision of Ca & Ph
− Medications
− Increased nutrient losses
− Vitamin D deficiency
− Immobility
• Screening
− Alkaline Phosphatase: <500 U/L
− Calcium: <8
− Serum phosphorus: < 5 mg
− Vitamin D < 32 ng/ml
− Radiographic evidence of demineralization
Quick Overview

13 | © 2015 13 | © 2015
Author, Year Title Level of
Evidence
Highlights
Cheng, H., Carmona,
F., & McDavitt, E. et.
Al., 2015
Fractures Related to
Metabolic Bone
Disease in Children
with Congenital Heart
Disease
Strong 1. Hyperparathyroidism
present in 77%, Low
Vit D present in 40%.
2. Increased exposure
to risk factors for
MBD
3. Increased mortality
rate
4. Protocol to identify
and treat patients
decreased fractures.
Uziel, Y., Zifman, E., &
Hashkes, P., 2009
Osteoporosis in
children: pediatric and
pediatric rheumatology
perspective: a review
Case Studies 1. Definitions
2. Etiology
3. Bisphosphonate use
Cross, B., & Vasquez,
E., 1999
Osteopenia of
Prematurity Prevention
and Treatment
Case Study 1. Pathophysiology
2. Prevention
3. Treatment
4. Nursing Implications
Step #1 – Literature Review

14 | © 2015 14 | © 2015
Author, year Title Level of
Evidence
Highlights
Marrani, E., Giani, T.,
Simonini, G, & Cimaz,
R. 2017
Pediatric Osteoporosis:
Diagnosis and
Treatment
Considerations
Mod 1. Great definitions
2. Making the
diagnosis (after
fracture)
3. Treatment options
Bachrach, L, 2014 Diagnosis and
treatment of pediatric
osteoporosis
Mod 1. Comprehensive
bone health screen:
DEXA, labs, bone
biopsy, X-ray
Khosla, S., Bilezikian,
J., Dempster, D.,
Lewiecki, E., Miller, P.,
Neer, R., Recker, R.,
Shane, E. Shoback, D.,
& Potts, J., 2012
Benefits and Risks of
Bisphosphonate
Therapy for
Osteoporosis
Mod 1. Benefits and risks of
bisphosphonates.
Lit Review cont

15 | © 2015 15 | © 2015
• Multi-disciplinary team formation
• Nutrition
• OT/PT
• Pharmacy
• Nursing
• Intensive Care
• Radiology
• Endocrine
• IT
Step #2: Question the Experts

16 | © 2015 16 | © 2015
Risk Factors
• Hx long bone/vertebral fracture (12)
• Rickets (12)
• Osteogenesis Imperfecta (12)
• Previous osteopenia diagnosis (4)
• >5 days of hydrocortisone (4)
• TPN > 4 weeks (4)
• Muscle relaxed ≥14 days (4)
• Severe malnutrition due to malabsorption malabsorption issues (4)
Precautions/ Preventative Treatment
• RN/Provider/Parent education regarding careful handling (RN to educate parents)
• https://www.childrensmn.org/educationmaterials/childrensmn/article/17174/osteopenia/
• Post "Careful Handling" sign on bed (see dietitian)
• Dietitian to note Osteopenia Risk on the "CVICU Nutrition Goals" (copy in workroom)
• RN to ensure staff outside unit are aware of risk when applicable (MRI, off-unit procedures)
• PT/OT consults (ROM exercises, use of Z-flo to create resistance boundaries, Joint Compression Protocol)
Screening Tests
• Alkaline Phosphatase: <668 males <12mo. and <610 females <12mo.
• Serum Phosphorus: >5mg
• Serum Calcium: >8mg/dl
• If low, check iCa and PTH. Always check PTH if DiGeorge or VACTERL
• Vitamin D (25-OH): >32ng/ml
• Urine Calcium/Creatinine Ratio: <7mo <0.86; 7-18m < 0.6, 19m - 6y <0.42, adult < 0.21
• Skeletal Survey
Protocol at a Glance

17 | © 2015 17 | © 2015
If all labs are normal
•Dietitian to evaluate risk level weekly. If still ≥ 12 in 4 weeks, repeat screening tests. Alter treatment as indicated by screening tests. If <12, patient is removed from "Osteopenia-Risk" list and precaution signage removed from room
Low Vitamin D
•Try to correct via nutritional supplementation for 1 week
• If calcium deficiency persists, order PTH. If concern for hypoparathyroidism, check serum1,25 OH Vit. D
•Repeat serum calcium/phosphorus labs q. day until stablilzation, then q. Monday/Thursday
•Repeat alkaline phosphatase, urine calcium/creatinine ratio, and vitamin D labs monthly
• If Ca++ persistently low or additional labs become abnormal, order Endocrinology Consult
Low/High Serum Ca
•Follow the Vitamin D Supplemental Guidelines (dietitian to manage)
•Repeat serum calcium/phosphorus labs q. day until stablilzation, then q. Monday/Thursday
•Repeat alkaline phosphatase, urine calcium/creatinine ratio, and vitamin D labs monthly
• If all labs are normal, proceed to that treatment (route to getting off risk list). If abnormalities persist, proceed to needed treatment
Continued

18 | © 2015 18 | © 2015
Low/High Serum Phos
• Order PTH
• Endocrinology Consult (evaluate calcitriol, bisphosponate need. If hypoparathyroid or on calcitriol, renal ultrasound q. month)
• Repeat serum calcium/phosphorus labs q. day until stablilzation, then q. Monday/Thursday
• Repeat alkaline phosphatase, urine calcium/creatinine ratio, vitamin D labs monthly
• If Phosphorus is elevated and tolerating feeds, consider adding a Phosphorous binder to feeds
Elevated Ca/Cr Ratio
• Endocrinology Consult (evaluate calcitriol, bisphosponate need. If hypoparathyroid or on calcitriol, renal ultrasound monthly)
• Renal ultrasound
• If abnormal, nephrology consult
• Repeat urine calcium/creatinine ratio and renal ultrasound weekly
• Repeat alkaline phosphatase, serum calcium and phosphorus, and vitamin D labs monthly
• Consider diuretic change (hydrochlorathizoid)
Long Term Follow up
• For patients who recieved an endocrinlogy consult during their stay, an outpatient endocrinology follow-up visit should be scheduled before discharge. At follow-up, patients ≥ 2 years should be considered for a DXA scan
Continued

19 | © 2015 19 | © 2015
Step #3: Algorithm Formation – Patient Identification

20 | © 2015 20 | © 2015
Step #4 Preventative Measures

21 | © 2015

22 | © 2015

23 | © 2015
RN Bedside Education Tool

24 | © 2015 24 | © 2015
Step #5 Screening Tests

25 | © 2015 25 | © 2015
Step #6: Treatment

26 | © 2015
Results: n = 14

27 | © 2015
n = 14
2017-2018 Gender Prevalence
n = 6 n = 8

28 | © 2015
SUCCESSES

29 | © 2015
n=3
Nephrocalcinosis

30 | © 2015
n = 1
Nephrocalcinosis
Fracture before admission

31 | © 2015
n = 1
Nephrocalcinosis
Fracture before admission
Fracture after discharge

32 | © 2015
n = 14
Nephrocalcinosis
Fracture before admission
Fracture after discharge
14 patients had electrolytes closely
monitored, targeted PT/OT, and careful
handling

33 | © 2015
OPPORTUNITIES FOR IMPROVEMENT

34 | © 2015
n = 2
Fractures

35 | © 2015
Next Steps
• Re-evaluate the protocol and adjust as necessary
• Sustainability
− Continue to work with unit champions
− Discuss fractures and protocol with unit council
− Educate about the osteopenia protocol
Conferences
New Hires

36 | © 2015
Questions

37 | © 2015
• Bachrach, L. (2014). Diagnosis and treatment of pediatric osteoporosis. Endocrinology. 21:6, 454-460.
• Cheng, H., Carmona, F., McDavitt, E., Wigmore, D., Perez-Rossello, J., Gordon, C., Pigula, F., Laussen, P., & Rajagopal, S. (2015). Fractures related to metabolic bone disease in children with congenital heart disease. Congenital Heart Disease.
• Christodoulou, s., Goula, T., Ververidis, A., & Drosos, G. (2013). Vitamin D and Bone Disease. Hindawi Publishing Corporation. Retrieved from: http://dx.doi.org/10.1155/2013/396541.
• Gajic-Veljanoski, O., Phua, C., Shah, P., & Cheung, A. (2016). Effects of long-term low-molecular –weight heparin on fractures and bone density in non-pregnant adults: a systematic review with meta-analysis. Journal of General Internal Medicine. 31(8). 947-957.
• Khosla, S., Bilezikian, J., Dempster, D., Lewiecki, E., Miller, P., Neer, R., Recker, R., Shane, E., Shoback, D., Potts, J. (2012). Benefits and Risks of Bisphosphonate Therapy for Osteoporosis. Journal of Clinical Endocrinology and Metabolism. 97(7): 2272-2282.
• Marrani, E., Giani, T., Simonini, G., & Cimaz, R. (2017). Pediatric Osteoporosis: Diagnosis and Treatment Considerations. Drugs. 77, 679-695.
• Rastogi, S., (2013). Using an Assessment Tool to Identify Risk of Osteopenia in Infants and Prevent Fractures. The Joint Commission. 39, 5, 228-232.
• Rodgers, C., & Monroe, R. (2007). Osteopenia and Osteoporosis in Pediatric Patients After Stem Cell Transplant. Journal of Pediatric Oncology Nursing. 24(4). 184-189.
• Sheridan, K. (2010). Assessing Bone Health in Children. A Pediatric Perspective. 19, 1, 1-3.
• Smeltzer, S. (2014). Practical implications for nurses caring for patients being treated for osteoporosis. Dovepress.
4, 19-33. • Uziel, Y., Zifman, E., Hashkes, P. (2009). Osteoporosis in children: pediatric and pediatric rheumatology
perspective: a review. Pediatric Rheumatology. 7, 16. 1-8.
References