-
7/27/2019 Anaemia and Iron Deficiency Disease
1/10
Anaemia and iron deficiency disease inchildren
Manuel Olivares, Tomds Walter, Eva Hertrampf andFernando
PizarroInstitute of Nutrition and Food Technology (INTA),University
of Chile, Santiago, Chile
Iron deficiency is the single most common n utrition al disorder
world-wide and
the main cause of anaemia in infancy, childhood and pregnancy.
It is prevalentin most of the developing world and it is probably
the only nutritionaldeficiency of consideration in industrialised
countries. In the developing worldthe prevalence of iron deficiency
is high, and is due mainly to a low intake ofbioavailable iron.
However, in this setting, iron deficiency often co-exists withother
conditions such as, ma lnutrition , vitamin A deficiency, folate
deficiency,and in fection . In tropical regions, parasitic
infestation and haemoglobinopathiesare also a common cause of
anaemia. In the developed world iron deficiency ismainly a single n
utritional problem. The conditions previously mentioned migh
tcontribute to the development of iron deficiency or they present
difficulties inthe laboratory diagnosis of iron deficiency.
Correspondence to:Manuel Olivares,
Institute of Nutrition andFood Technology (INTA),
University of Chile, Macul5540, Casilla 138,
Santiago 11 , Chile
Iron deficiency is the single most common nutritional disorder
world-wideand the main cause of anaemia in infancy, childhood and
pregnancy. It isprevalent in most of the developing world and it is
probably the onlynutritional deficiency of consideration in
industrialised countries. Becauseof their high iron requirements,
the most commonly affected groups areinfants, children,
adolescents, and women of childbearing age andpregnancy1. In the
developing countries, the prevalence is usually greatest
in infants and to a lesser extent in women; in contrast, in
industrialisedcountries, it is present mainly in women due to the
additional ironrequirements imposed by menstruation and
pregnancy.
In the developing w orld , the prevalence of iron deficiency is
high, an d isdue mainly to a low intake in bioavailable iron.
However, in this setting,iron deficiency co-exists with other
conditions such as, protein/energymalnutrition, vitamin A
deficiency, folate deficiency, and infection2"5. Intropical
regions, parasitic infestation and haemoglobinopathies are also
The prevalence of these pathologies is higher in lessc o m m o
n3 -5
British Medical B ulletin1999; 55 (No. 3): 534-543 C The British
Council 1999
-
7/27/2019 Anaemia and Iron Deficiency Disease
2/10
Iron deficiency in children
developed countries than in areas with intermediate development.
In thedeveloped world iron deficiency is mainly a single
nutritional problem.The conditions previously mentioned might
contribute to the develop-ment of iron deficiency or they present
difficulties in the laboratory
diagnosis of iron deficiency.
Aetiology and pathogenesis of iron deficiency
Nutritional factors are the most frequent causes of iron
deficiency ininfancy and childhood. The main aetiologies of iron
deficiency at thisperiod of the life cycle are: (i) decreased iron
stores at birth (preterminfants, twins, perinatal bleeding, early
clamping of umbilical cord) (ii)inadequate iron supply (reduced
dietary iron and/or low bioavailability ofdietary iron); (iii)
increased iron requirements imposed by growth; and (iv)increased
iron losses (gastrointestinal blood loss, diarrhoea).
Ironrequirements of infants are not covered by their usual diet,
which ismainly based on milk. This problem is more severe in
children fed cows'milk, where the iron present is poorly absorbed6.
Infants who are fedcows' milk starting in early infancy and those
who are fed milk that is notiron fortified are at highest risk for
the development of iron deficiency.The situation becomes critical
when iron stores at birth are reduced. Inolder children, because of
their slower growth rate and their more varieddiet, nutritional
iron deficiency anaemia is less prevalent (when present it
is usually carry-over from earlier infancy) while other
aetiologies becomemore prevalent, gastrointestinal blood loss among
them.
When dietary iron cannot fulfil the requirements, a fall in body
storesoccurs (iron depletion), which is characterised by a drop in
serumferritin (SF) below 12 ng/1. If this negative ba lance
persists, iron tissueavailability is compromised (iron deficient
erythropoiesis). At this stage,an early progressive rise in the
concentration of serum transferrinreceptor (TfR) values occurs,
followed by an increase in free erythrocyteprotoporp hyrin (FEP), a
decrease in transferrin saturation (Sat), and theslow fall in
haemoglobin (Hb) begins7. If the iron deficit continues, the
last stage becomes evident when Hb falls below -2 standard
deviationsfor that given population,i.e. iron deficiency
anaemia.
Dietary iron absorption
The amount of iron absorbed from the diet is dependent on
threefactors: (i) the quantity of iron; (ii) the composition of the
diet; and (iii)the behaviour of the mucosa of the upper small bowel
where two major
British Medical Bulletin 1999;55 (No.3) 535
-
7/27/2019 Anaemia and Iron Deficiency Disease
3/10
Micronutrients in he alth and disease
factors that affect iron absorption occur: the body iron stores
and therate of erythropoiesis8.
The effect of the composition of the diet is based on: the type
of iron(haem or non-haem); amount of haem iron, specially as meat,
the content
of calcium in the meal, food preparation (time, temperature),
iron statusof the individual, amount of potentially available
non-haem iron(adjustment for fortification iron and con tamination
iron) and the balancebetween enhancing (ascorbic acid,
meat/poultry/fish, fermented foods)and inhibiting factors (phytate,
polyphenols, calcium, soy protein).
There are two kinds of iron in the diet with respect to the
mechanismof absorption haem iron and non-haem iron utilising two
differentreceptors on the mucosal cells. After the uptake of haem
iron into themucosal cells, the porphyrin ring is split by the
haem-oxygenase withinthe cells and its iron is released. Non-haem
and haem iron then have a
common pathway and leave the mucosal cells in the same
chemicalform, utilising the same transfer system to the serosal
side of the mucosalcells. Receptors on the luminal side probably
compete for non-haemiron with complexing luminal ligands for the
iron ions11.
Haem iron in meat and meat products constitute abou t 5-1 0% of
thedaily iron intake in most industrialised countries. In
developing coun-tries, the haem iron content of diets is usually
negligible. Its absorptionis less influenced by body iron stores
than non-haem iron12. The averageabsorption of haem iron in meat
containing meals is about 25%,calcium being the only dietary factor
that negatively influences theabsorption of haem-iron13.
Non-haem iron is the main form of dietary iron. The main sources
arecereals, vegetables, pulses, beans, fruits, etc. The absorption
of iron fromiron fortificants and contamination iron is influenced
by the same hostand dietary factors as the native iron.
Studies of iron absorption from various representative meals
havebeen done primarily in adults, but the results are also
pertinent to themixed diet in late infancy. Absorption of non-haem
iron from a mixedmeal is about 4 times greater when the major
protein source is meat, fishor chicken in comparison to the dairy
products, milk, cheese or eggs.
Term infants are protected from iron deficiency by their
endowment at
birth and the iron supply from breast milk during the first 6
months oflife. The basis for the excellent absorption of iron from
human milk isnot known. From this age on, iron status is mainly
dependent on ironsources in the diet14. The increasing use of iron
fortified formulae andiron rich weaning foods have determined a
decrease of iron deficiencyanaemia among infants in highly
developed countries15. The appropriatelevel of iron to fortify
formulae is still under discussion. Recent evidenceshows a high
iron bioavailability in these products, which is acompelling
argument for lowering the level of iron fortification in North
5 3 6 British Medical Bulletin 1999,55 (No. 3)
-
7/27/2019 Anaemia and Iron Deficiency Disease
4/10
Iron deficiency in children
260 D ie t A D ie t B
V i t . A V i t . C F o l a t e Iro n Z i n c
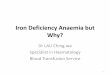
Fig. 1 White rice based diets: percentage of recommended
nutrient density per 1000kcal. Diet A composition: wh ite rice 598
g and vegetable o il 25 g. DietB composition:wh ite rice 428 g,
vegetable oil 25 g, carrots 21 g, orange 60 g, beef 35 g, spinach
raw 50
g, and lentils 45 g . Recommended nutrien t density of
micronutrients was based on th erecommendations of the
FAO/WHO".
D ie t A D ie t B
Vi t . A V i t . C F o l a te I r o n Z i n c
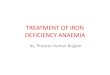
Fig. 2 Corn -tortilla based diets: percentage of recommended
nutrien t density per 1000kcal. Diet A composition: corn -tortilla
368 g and vegetable oil 25 g. DietB composition:corn-tortilla 266
g, vegetable oil 20 g, carrots21 g, orange 60 g, beef 55 g, spinach
raw 50g, and black beans 45 g. Recommended nutrient density of
micronutrients was based onthe recommendations of the FAO/WHO".
American formulae1617. Home prepared complementary foods, based
on
cereals and legumes fed to weanlings in the less developed world
wheremost of the children younger than 2 years reside, contain
relatively highlevels of phytic acid and negligible amounts of
ascorbic acid or meat.
School-age children and adolescents at a global level are
affected byseveral micronutrient deficiencies, because at presently
staple foods suchas wheat, rice, corn or potatoes make up the
largest proportion of thefood supply. Uauy and Oyarzun explored the
adequacy of food patternsbased predominantly in rice and corn18.
Theoretical d iets were developedand complemented with low cost
micronutrient rich foods. The foodportion size considered in this
exercise represent the usual amount eaten
British Medical B ulletin1999;55 (No. 3) 537
-
7/27/2019 Anaemia and Iron Deficiency Disease
5/10
Micronutrien ts in hea lth and disease
in a meal or provided by a 1000 kcal food tray. Vitamin A,
vitamin C,folate, iron and zinc were selected. The nutrient density
of plain rice andcorn plus a regular portion of vegetable oil as a
fat source was analysed.The content of selected micronutrients was
computed per 1000 kcal. As
shown in Figures 1 and 2 in terms of percentage recommended
nutrientdensity, both diets provide no vitamins A or C, and very
low levels offolates, iron and zinc. Following a food based
approach to improve themicronutrient content of the diets, small
portions of carrots, orange,beef,spinach, and lentils or black
beans were added. In both cases, allmicronutrient needs were
covered (Figs 1 & 2).
Interactions b etween iron and vitamin A
Vitamin A is important not only for visual function but also for
normaldifferentiation of various tissues. Early reports
demonstrated anaemia andreduction in haemopoietic tissue in severe
vitamin A deficiency.Thereafter, an array of epidemiological
studies have shown that vitamin Adeficiency and anaemia often
co-exist and that there is significant assoc-iation between retinol
and biochemical indicators of iron deficiency20"21.
The re are several hypotheses to explain this interrelation: (i)
that impro v-ing vitamin A status improves mobilisation of iron
from the tissue stores;(ii) that vitamin A decreases infection and
thus improves iron status; and(iii) that vitamin A improves iron
absorption.
It is of interest to note that interactions are found only in
vitamin Adeficient populations and no demonstration of these
effects has beenshown in vitamin A sufficient subjects.
Animal experiments show that supplemental vitamin A enhances
therecovery from iron deficiency in rats with chronic vitamin A
deficiency.Vitamin A supplemen tation during the period of iron
treatme nt produce da depletion of spleen and tibia iron
concentration22. Other authors foundalso decreased liver iron in a
similar experiment. Supplemental vitaminA also produced a reduction
of Hb probably explained by a decrease inthe degree of
haemoconcentration seen in vitamin A deficiency. Thesestudies in
experimental animals suggest that supplemental vitamin Aduring iron
repletion contributes to optimum erythropoeisis and
ironmobilisation when baseline vitamin A status is impaired.
Several studies in anaemic children and pregnant women in
endemicvitamin A deficient regions have shown a beneficial effect
on iron statuswith vitamin A supplementation21-23"25.
Mejfa and Chew in Guatemala studied 99 children, 1-8 years of
age,divided in 4 groups2 3. Each group was supplemented for 2
months with:(i) vitamin A; (ii) iron; (iii) vitamin A plus iron; or
(iv) placebo. Vitamin
5 3 8 British M e d i a l Bulletin 1999;55 (No. 3)
-
7/27/2019 Anaemia and Iron Deficiency Disease
6/10
Iron deficiency in children
A elevated retinol, Hb, serum iron (Fe) and Sat. Iron alone did
not affectretinol but improved haematological and iron nutrition
indicatorsincluding total iron binding capacity (TIBC) and SF. The
conco mitantsupplementation of vitamin A and iron resulted in a
better response of
Fe and Sat saturation than either alone. This study suggested
thatvitamin A benefits haematological condition and iron
metabolism.
Two studies showed the effect of a single oral massive dose of
vitaminA on iron metabolism21-24. Kahn et al studied a group
Pakistani children,of whom 16% had low serum vitamin A and 2% were
deficient21: 42children were supplemented with a single oral
vitamin A dose and 53children received p lacebo. After 6 weeks,
there were significant differ-ences between the 2 groups for
retinol, retinol binding protein andhaematocrit (Htc). However, no
significant difference could be found forH b, red blood cell count,
mean corpuscular volume, mean corpuscular
haemoglobin concentration, Fe, transferrin, andSF. In the ano
ther study,a group of 134 school children, with signs of
conjunctival xerosis, fromThailand were selected for a controlled
study on the short-term effect ofa single, oral high dose of
vitamin A on iron metabolism24. Childrenwithin villages were
randomly assigned to receive the vitamin A or serveas control
subjects. Two weeks after supplementation, significantincreases of
retinol, retinol binding protein, Hb, Htc, Fe, and Sat werefound in
the supplemented group. SF concentrations did not
changesignificantly. These two studies provide further evidence of
a causalassociation between vitamin A and iron metabolism.
The anti-infective properties of vitamin A are well know n, and
there issome suggestion that the benefits of vitamin A on iron
status may be doto reduced level of infection26.
Garci'a-Casal et al have shown the enhancer effect of vitamin A
and P-carotene on non-haem iron absorption from Venezuelan
cereal-baseddiets27. Vitamin A increased iron absorption up to
2-fold for rice, 0.8-fold for wheat and 1.4-fold for corn;
|3-carotene increased absorptionmore than 3-fold for rice
and1.8-fold for wheat and corn. The authorssuggested that both
compounds prevented the inhibitory effect ofphytates and
polyphenols on iron absorption, because both compoundsmay form a
complex with iron , keeping it soluble in the intestinal lum
en.
Pathological blood loss
The digestive tract is the most frequent source of occult
bleeding.Gastrointestinal blood loss may occur during the first
months of lifewhen infants are fed fresh or pasteurised cows' milk,
or during repeatedepisodes of acute diarrhoea, or less frequently,
in cows' milk proteinallergy28-29. Alaskan natives have shown a
high prevalence of iron
British M e d i a l Bulletin 1999;55 (No. 3) 5 39
-
7/27/2019 Anaemia and Iron Deficiency Disease
7/10
Micro nutrien ts in hea lth and disease
deficiency anaemia despite an adequate iron intake. This
population hasan increased frequency of elevated stool haem
concentration30-31 . Thegastrointestinal blood loss has been
attributed to an altered plateletfunction due probably a high
intake of (n-3) fatty acid from marine
mammals and f ish30, or caused by chronic active gastritis
associatedHelicobacter pylori infection31 .
In tropical areas, pathologic bleeding due to infestation with
parasites isa contributing factor to nutritional iron
deficiency3"5. Hookworms(Necator atnericanus and Ancylostoma
duodenale) are the most prevalentparasites related to iron
deficiency32. These haematophagous intestinalparasites produce
intestinal blood loss that is proportional to the parasiticload.
When faeces contain 1000 eggs/g, daily blood loss is 2 ml (1 mg
ofiron) if the infection is du e toN. atnericanus, the
corresponding figures forA. duodenale and Trichiuris trichiura
infestations are 4 ml and 0.25 ml,
respectively33
. In areas endemic for u rinary schistosomiasis, blood loss
dueto haematuria is a cofactor to the development of iron
deficiency34.
Iron, inflammation and infection
Acute or chronic inflammatory diseases are a well-recognised
cause ofmild to moderate anaemia35 . This reduction in haem oglob
in level is due toseveral factors36 : (i) a block in iron release
from the reticuloendothelialsystem and a reduction in iron
intestinal absorption, with the consequent
reduction on iron available for erythropoiesis; (ii) inhibition
oferythropoiesis; (iii) inappropriate erythropoietin production;
and (iv)reduction of erythrocyte survival.
Immunoactivation releases cytokines that are mainly responsible
for thechanges on iron metabolism, inhibition of eythropoiesis and
lowererytropoietin production observed in inflammation or
infection36.
Acute infections are very frequent in childhood, especially in
subjects oflow socio-economic strata of developing countries. Even
mild infectionsthat do not warrant medical consultation induce a
significant decrease inH b , Fe, TIBC, and Sat, whereas, FEP and SF
increase significantly37-38.
Most of the changes in iron laboratory indices persist for 2-3
weeks afterthe appearance of fever, and some measures may become
abnormal evenduring the incubation period of the illness37-39. The
modifications oflaboratory indicators of iron status are related to
the severity of theinflammatory process40 . Changes in iron status
parameters are moreprominent in subjects with increased C reactive
protein, high band counts,or fever above 38C38-40.
Proper diagnosis of iron status is based primarily on multiple
laboratorymeasures. However, in populations where infections are
prevalent, classic
5 40 British Medical B ulletin1999;55 (No. 3)
-
7/27/2019 Anaemia and Iron Deficiency Disease
8/10
Iron deficiency in children
Eum
Inflammation/infection (-)
IV(6-11 mo.) (12 mo.) (1 2- 69 mo.)
Studies
References
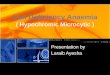
Fig. 3 Prevalence of anaemia in children with and with ou t
inflamm ations/infections.Data of studies I, II, III, and IV were
taken from Olivareset al 3 *, Jansonn et al*\ Reeves etat* 2 , and
Freire e t a/*3, respectively.
iron measures might underestimate or overestimate the prevalence
of irondeficiency depending on the measure used. Figure 3 shows the
results ofseveral studies in which the prevalence of anaemia in
subjects with andwithout inflammation/infection was studied. The
prevalence of anaemiawas overestimated in subjects with clinical
and/or laboratory evidence ofinflammatory or infectious processes38
'41"43. TfR assay has been shown tobe useful in evaluating iron
status in these populations, since acute orchronic infection or
inflammation does not affect it44-45. In the absence ofthis
indicator, the interpretation of iron status measures should be
madewith caution in populations or individuals during or shortly
after aninflammatory process.
1 DeM acyer E, Adiels-Tegman M. The prevalence of anaemia in the
world.World Health Stat Q1985; 38: 302-16
2 Florentino RF, Guirriec RM . Prevalence of nu tritional anemia
in infancy and childhoo d withemphasis on developing countries. In:
Stekel A (Ed)Iron nutrition in infancy and childhood.Vevey/New
York: Nestle/Raven Press, 1984: 61-74
3 Fleming AF. Iron deficiency in the tropics.Clin Haematol 1982;
2: 365-884 Masawe AEJ. Nutritional anaemias. Part 1. Tropical
Africa.Clin Haematol1981; 3: 815-425 Baker SJ. Nutritional
anaemias. Pan 2. Tropical Asia.Clin Haematol1981; 3: 843-716 Stekel
A, Olivares M, Pizarro F, Chadud P, Lopez I, Amar M . Absorption of
fortification iron
from milk formulas in infants.Am J Clin tiutr 1986; 43: 91 7-227
Skikne BS, Flowers CH, Cook JD . Serum transferrin receptor: a
quantitative measure of tissue
iron deficiency. Blood 1990; 75: 1870-68 Charlton RW, Bothwell
TH . Iron absorption.Annu Rev Med1983; 34: 55-6 8
British Medical Bu lletin1999;55 (N o. 3) 54 1
-
7/27/2019 Anaemia and Iron Deficiency Disease
9/10
Micro nutrien ts in health and disease
9 Rossander-H ulthen L, Hallberg L. Dietary factors influencing
iron absorption - an overview.In: Hallberg L, Asp N-G (Eds)Iron
Nutrition in Health and Disease. London: John Libbey,1996;
105-15
10 Hallberg L, Brunt M, Rossander L. Iron absorption in man:
ascorbic acid and dose dependentinhibition by phytate.Am J Clin
Nutr 1989; 49: 140-4
11 Wood JR, Han O. Recently identified molecular aspects of
intestinal iron absorp tion. /Nutr1998; 128: 1841-4
12 Olivares M, Hertramp f E , Pizarro F. Effect of iron stores
on heme iron absorptio n.Nutr Res1993; 13: 633-8
13 Hallberg L, Bjorn-Rasmussen E, Howard L. Dietary haem iron
abso rption. A discussion ofpossible mechanisms for the
absorption-promoting effect of meat and for the regulation of
ironabsorption. Scand ] Gastroenterol 1979; 14: 769-7 9
14 Pizarro F, Yip R, Dallman PR, Olivares M, Hertramp f E,
Walter T. Iron status with differentfeeding regimens: relevance to
screening and prevention of iron deficiency. /Pediatr 1991;
118:687-92
15 Yip R, Walsh KM , Goldfarb MG , Binkin NJ. Declining
prevalence of anemia in childhood in amiddle-class setting: a
pediatnc success story?Pediatrics 1987; 80: 330-4
16 Her tramp f E, Olivares M, Pizarro F, Walter T. High
absorption of fortification iron from
current infant formulas. /Pediatr Gastroenterol Nutr 1998; 27:
425-3017 Walter T, Pino P, Pizarro F, Lozoff B. Prevention of
iron-deficiency anemia: comp arison of high-and low-iron formulas
in term healthy infants after six months of life. /Pediatr 1998;
132:635^*0
18 Uauy R, Oyarziin M T. Food based approaches to meet vitamin
and mineral needs: possibilitiesand limitations. Background paper
to Joint FAO/WHO consultation on human vitamin andmineral
requirements. Bangkok, Thailand, September 21-30, 1998
19 FAO/WHO. Preparation and use of food-based dietary
guidelines.Report of a JointFAO/WHO consultation. Nicosia, Cyprus:
WHO, 1996
20 Suharno D, West CE, Muh ilalB et al. Cross-sectional study on
the iron and vitamin A statusof pregnan t wom en in West Java,
Indonesia.Am ] Clin Nutr 1992; 56: 988 -93
21 Khan I, Baseer A. Hematologic effect of vitamin A supplem
entation in anemic Pakistanichildren. / Pak Med Assoc1996; 46: 3
4-8
22 Rooden burg AJ, West CE, Hovenier R, Beynen AC. Supplemental
vitamin A enhances therecovery from iron deficiency in rats with
chronic vitamin A deficiency.Br J Nutr 1996; 75:623-36
23 Mejia LA, Chew F. Hematological effect of supplementing
anemic children with vitamin Aalone and in combination with iron.Am
J Cltn Nutr 1988; 48: 595-600
24 Bloem MW, Wedel M , van Agtmaal EJet al. Vitamin A
intervention: short-term effects of asingle, oral, massive dose on
iron metabolism.Am ] Clin Nutr 1990; 51 : 76-9
25 Suharno D , West CE, Mu hilal, Karyadi D, Hautvast JG.
Supplementation with vitamin A andiron for nutritional anaemia in
pregnant women in West Java, Indonesia.Lancet 1993; 342:1325-8
26 Northrop-Clewes CA, Paracha PI, McLoone UJ, Thurnham DI.
Effect of improved vitamin Astatus on response to iron
supplementation in Pakistani infants.Am J Clin Nutr 1996; 64 :
6949
27 Garria-Casal M N, Layrisse M , Solano L, etal. Vitamin A and
[}-carotene can improve nonhemeiron absorption from rice, wheat and
corn by humans. /Nutr 1998; 128: 646-50
28 Ziegler EE, Fomon SJ, Nelson SEet al. Cow milk feeding in
infancy: further observations onblood loss from the
gastrointestinal tract./Pediatr 1990; 116: 11-8
29 Walter T, Hertrampf E, Arredondo M. Gastrointestinal iron
losses in infancy: effect of the diet.In: Hercberg S, Galan P,
Dupin H (Eds)Recent Knowledge on Iron and Folate Deficiencies inthe
World. Colloque INSERM Vol 197, Paris: INSERM, 1990; 283-90
30 Petersen KM , Parkinson AJ, Nobmann ED, Bulkow L, Tip R,
Mokdad A. Iron deficiencyanemia among Alaska natives may be due to
fecal loss rather than inadequate intake. /Nutr1996; 126:
2774-83
31 Yip R, Limburg PJ, Ahlquist DAet al. Pervasive occult
gastrointestinal bleeding in an Alaskanative population with
prevalent iron deficiency. Role ofHelicobacter pylori gastritis.
JAMA1997; 277: 1135-9
5 42 British Medical Bulletin 1999;55 (No. 3)
-
7/27/2019 Anaemia and Iron Deficiency Disease
10/10
Iron deficiency in children
32 Stoltzfus RJ, Dreyfuss ML, Chwaya HM , Albonico M. Hook worm
control as a strategy toprevent iron deficiency.Nutr Rev 1997; 55:
223-32
33 Roche M, Layrisse M. The nature and causes of 'hookw orm anem
ia'.Am } Trop Med Hyg1966; 15: 1029-102
34 Prual A, Daouda A, Develoux M , Sellin B, Galan P, Hercberg
S. Consequences ofScbistosoma
haematobium infection on the iron status of school children in
Niger.Am J Trop Med Hyg1992; 47: 291 -7
35 Yip R, Dallman PR. The roles of inflammation and iron
deficiency as causes of anem ia.Am JClin Nutr 1988; 48:
1295-1300
36 Means RT, Krantz SB. Progress in understanding the
pathogenesis of the anemia of chronicdisease. Blood 1992; 80:
1639-47
37 Olivares M , WalterT, Osono M , ChadudP, Schlesinger L.
Anemia ofa mild viral infection: themeasles vaccine as a
model.Pediatrics 1989; 84: 851-5
38 Olivares M , Walter T, Llaguno Set al. Modificaciones del
hemograma y de los parametrosindicadores del metabolismo de hierro
en infecaones virales leves (Changes of blood eel] countsand
laboratory indices related to iron metabolism in mild viral
infections).Sangre 1993; 38:211-6
39 Hulthen L, Lindstedt G, Lundberg P-A, Hallberg L. Effect of a
mild infection on serum ferritin
concentration clinical and epidemiological implications.Eur J
Clin Nutr 1998; 52: 376940 Olivares M, Walter T, Oso rio M , Chadu
d P, Schlesinger L. Effect of a mild viral infection on
laboratory measures of iron nutriture. The measles vaccine as a
model. In: Hercberg S, GalanP, Dupin H (Eds) Recent Knowledge on
Iron andFolate Deficiencies in the World. ColloqueINSERM Vol 197,
Paris: INSERM, 1990; 209-15
41 Janso nn LT, Kling S, Dallman PR . Anemia in children with
acu te infections seen in a prim arycare pediatric ou tpatient
clinic.Pediatr Infect Dts 1986; 5: 424- 7
42 Reeves JD, Yip R, Kiley VA, Dallman PR. Iron deficiency in
infants: the influence of m ildantecedent infection. / Pediatr
1984; 105: 874-9
43 Freire WB, Dirren H, Barclay D. The influence of infection
and inflammation on the estimationof the prevalence of iron
deficiency anemia. In: Hercberg S, Galan P, Dupin H
(Eds)RecentKnowledge on Iron andFolate Deficiencies in the World.
Colloque INSERM Vol 197, Paris:INSERM, 1990; 205-8
44 Ferguson BJ, Skikne BS, Simpson K M, Baynes RD , Cook JD .
Serum transferrin receptordistinguishes the anemia of chronic
disease from iron deficiency anemia.J Lab Clin M ed 1992;19:
385-90
45 Olivares M , Walter T, Cook JD , Llaguno S. Effect of acute
infection on measurem ent of ironstatus: usefulness of the serum
transferrin receptor.Int] Pediatr Hematol Oncol1995; 2:31-3
British Medical Bulletin 1999;55 (No. 3) 54 3