Embed Size (px)
Citation preview

CMAJ • January 31, 2006 • 174(3) | 302© 2006 CMA Media Inc. or its licensors
AnalysisIn developed countries, rates of
maternal death from infection,pre-eclampsia, cardiovascular dis-
ease, intracranial hemorrhage andembolism have fallen to low and sta-ble rates.1 A recent report from thePublic Health Agency of Canada notesthat the 1997–2000 rate for Canada(excluding Quebec) was 6.1 maternaldeaths for every 100 000 live births. Incontrast, the world rate is 400; inAfrica, over 900 (Table 1).1 Solutionsto lowering these rates in underdevel-oped countries are no mystery; they in-clude improving access to care, redu-cing poverty and improving othersociodemographic factors. But is thereroom for improvement in reducingmaternal mortality in Canada andother developed countries?
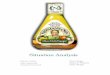
Perhaps we should look at othercountries with low maternal mortalityfor ideas. In the United Kingdom, theConfidential Enquiries into MaternalDeaths (CEMD) has reported on theserates since 1952. Their most recent edi-
tion used data from linked nationaldatabases, which allowed for improvedcase identification and evaluation ofthe factors playing a role in maternaldeaths (Fig. 1). The report revealed thatwomen from the most disadvantagedgroups of society were more than 20 times more likely to die thanwomen in the highest 2 socioeconomicclasses. Moreover, women from non-white ethnic groups were twice aslikely to die as white women. TheCEMD also showed that 12% ofwomen who died had previously de-clared that they were subject to violence in the home and that 20% had booked for maternity care after 24 weeks of gestation or missed over 4routine antenatal visits. Other factorsassociated with an increased risk ofdeath were age less than 18 years, ahigher maternal age, increasing parity,obesity, and multiple pregnancies(largely due to in vitro fertilization).Most importantly, for the first time thereport revealed that more deaths werecaused by pre-existing medical condi-tions that were exacerbated by preg-nancy (indirect deaths) than werecaused by conditions specific to preg-nancy (direct deaths).
The causes of the deaths werestriking. Over 40 deaths resulted fromsuicide or other violent causes and 11,accidental drug overdoses. When allmaternal deaths within 1 year after de-livery were considered, suicide wasone of the 3 leading causes of mater-nal deaths overall. Given that highrates of depression exist among non-pregnant women aged 18–44 years, itis not surprising that it is frequentlyseen among pregnant and recentlypregnant women.2 Depression andsuicide are underdiagnosed and diffi-cult to ascertain, but rates of depres-sion during and after pregnancy rangefrom 10% to 20%.2 The CEMD reportsthat maternal mental illness is morecommon than nearly all the condi-tions that we routinely ask obstetricand postpartum patients about andreport.
Depression during pregnancy is dis-tinguished by its context and conseq-uences. The depressed pregnant wo-man is less likely than others to eat andsleep well, seek prenatal care or adhereto medical recommendations. In addi-tion to personal suffering, disability,self-harm and suicide, depressed wo-men can undergo perturbed hypothala-mic pituitary axes and β-endorphin lev-els, which may result in harmful fetaleffects such as prematurity, low birthweight, and slower fetal activity and de-velopment.2 Infants of depressed wo-men may receive suboptimal physicaland psychological care; their older chil-dren and the marital partner may alsoexperience secondary effects of mater-nal depression.2
In Canada, maternal death rates arebased on causes of death directly at-tributable to classic obstetric indica-tors. If we want to lower rates in this
DO
I:10
.150
3/cm
aj.0
5077
5
A broader context
for maternal mortality Thrombo-embolism
Cardiac event
Suicide
Sepsis
Ectopicpregnancy
Hypertension
Amniotic-fluidembolism
Hemorrhage
Cause
Maternal deathsper million pregnancies
205 10 150
Fig. 1: Main causes of maternal deathper million pregnancies in the UnitedKingdom, 1997–1999. Source: WhyMothers Die 1997–1999: The Fifth Re-port of the Confidential Enquiries intoMaternal Deaths in the United King-dom. London: Royal College of Obstet-rics and Gynaecologists Press; 2001.
Table 1: Maternal death rates in 2000
Region or countryDeaths
per 100 000*
World (total) 400
Sub-Saharan Africa 920
Asia 330
Latin America, Caribbean 190
United States 17
United Kingdom 13
Canada 6
Denmark, Ireland,Portugal, Italy, Kuwait 5
Spain, Austria, Slovakia 4
Sweden 2
Iceland 0
Source: World Health Organization. MaternalMortality in 2000: Estimates Developed by WHO,UNICEF, UNFPA. Geneva: WHO Department ofReproductive Health and Research; 2004.*Adjusted maternal deaths per 100 000population.

country, the first step would be to takea broader conceptualization of mater-nal morbidity and mortality and in-clude deaths attributable to mentalhealth conditions and violence. To bet-ter understand the effects of poverty,nutrition, education and mental healthindicators on pregnancy outcomes, thePublic Health Agency of Canadashould link national databases thatrecord social indicators as well as ma-ternal health outcomes. Furthermore,by extending the period of maternalsurveillance beyond 42 days, as theUnited Kingdom has done and othershave advocated, we will be better ableto study the effects of these “nonob-stetric” indicators.
At the practice level, we need to askabout and intervene in maternal de-pression, substance abuse and vio-lence in the home and to consider thespecial needs of women with low in-come, poor social support, communi-cation problems and irregular atten-dence at prenatal care classes.3 Theroutine use of national guidelines fordiagnosis and treatment also im-proves outcomes.
Six deaths per 100 000 live birthsare still too many, and likely to be anundercount. A broader conceptualiza-tion of health in future Canadian ma-ternal and child health reports willenable us to further reduce our mater-nal death rate.
Donna E. Stewart Professor and ChairWomen’s Health University HealthNetwork
University of TorontoToronto, Ont.
REFERENCES1. Public Health Agency of Canada. Make every moth-
er and child count: report on maternal and childhealth in Canada. Available: www.phac-aspc.gc.ca/rhs-ssg/whd05_e.html (accessed 2005 Dec 6).
2. Stewart D. Depression during pregnancy. Can FamPhysician 2005;51:1061-7.
3. Carroll JC, Reid AJ, Biringer D, et al. Effectiveness ofthe Antenatal Psychosocial Health Assessment (AL-PHA) form in detecting psychosocial concerns: a ran-domized controlled trial [published erratum appearsin CMAJ 2005;173(4):345]. CMAJ 2005;173(3):253-9.
CMAJ • January 31, 2006 • 174(3) | 303
Analysis
Competing interests: None declared.
2006 AMA/CMAInternational Conference on Physician HealthFairmont Château LaurierOttawa, Ontario, Canada30 November–2 December 2006
Mark your calendar now …and watch cma.ca for further details!
Abstracts due 1 May 2006
For more information on the Call for Papers or the conference, please contact Susan Yungblut at 800 663-7336 or 613 731-8610 x2877 or [email protected] or visitcma.ca/physicianhealth&well-being












![Job Analysis Step by Step Guide - bnhexpertsoft.com · model. [Mission Analysis, Competency Analysis, System Analysis, Job Task Analysis and Knowledge/Skill Gap Analysis]. Module](https://img.pdfslide.net/doc/110x75/5e6efaea7135b4624d2ba2da/job-analysis-step-by-step-guide-model-mission-analysis-competency-analysis.jpg)