Embed Size (px)
Citation preview

ARTHRITIS & RHEUMATISMVol. 43, No. 6, June 2000, pp 1421–1429© 2000, American College of Rheumatology
LETTERS
Poly(ADP)-ribose polymerase and susceptibility tosystemic lupus erythematosus and primaryantiphospholipid syndrome: comment on the article byDelrieu et al
To the Editor:Several genome-wide scans for systemic lupus ery-
thematosus (SLE) susceptibility genes have shown linkage to aregion on human chromosome lq41-42 (1–3). Poly(ADP-ribose) polymerase (PARP) is one of the candidates in thisregion implicated by a transmission disequilibrium study of 124multiethnic (primarily Caucasian) SLE families, suggestingthat PARP alleles may be (or be close to) the SLE suscepti-bility gene within lq41-q42 (4). Therefore, we read withinterest the article by Delrieu et al (5) reporting a lack ofassociation of PARP alleles with SLE among French Cauca-sians. Our data described below suggest that PARP alleles maybe in linkage disequilibrium with an SLE susceptibility gene.
The incidence of SLE in African Americans is 2–4times greater than that in Caucasians (6). Our study usedbanked DNA obtained from consecutive African AmericanSLE patients (n 5 91) at the Division of Rheumatologyand Immunogenetics, University of Texas–Houston MedicalSchool and from normal controls (n 5 53) recruited fromamong medical center personnel. All SLE patients fulfilledthe American College of Rheumatology criteria for thedisease (7).
Consistent with the findings reported by Delrieu et al(5), no specific PARP promoter allele was found to besignificantly associated with SLE or with any subset of SLE(patients stratified by the presence of lupus nephritis, anti–double-stranded DNA [by Crithidia luciliae assay], or HLAclass II alleles) (data not shown). However, the overall distri-bution of PARP alleles among the SLE patients was signifi-cantly skewed compared with that among controls (P 5 0.0185by Monte Carlo test [8]) (Table 1). In addition, PARP allelesin the SLE patients demonstrated significant deviation fromHardy-Weinberg equilibrium (HWE [9,10]) (P , 0.00001 byFisher’s exact test) (Table 1), but this was not found in thecontrols. Deviation from HWE at a marker locus has beenused in the fine localization of disease susceptibility loci, asdemonstrated in identification of the susceptibility gene forhereditary hemochromatosis (11,12). In that heterogeneousrecessive disease, deviation from HWE (due to excess homozy-gosity) of the marker loci among affected individuals peakedwith increased linkage disequilibrium between the test markerand the disease gene. Thus, departure from HWE can provideevidence both for linkage disequilibrium between marker andsusceptibility loci and for heterogeneity of disease susceptibil-ity (11,12).
In this study, both the SLE patients and the controlshad African American maternal and paternal grandparents.The 2 groups were drawn from the same geographic area andmatched for sex distribution (90% female). Because this studydesign is sensitive to population admixture, all subjects weregenotyped at 3 forensic loci: D5S818, D7S820, and D13S317.In contrast to the results with PARP, none of the 3 forensic
markers demonstrated skewed allele distribution in the SLEpatients compared with the controls. One forensic locus(D5S818) showed deviation from HWE in the SLE patients,while another (D13S317) demonstrated the HWE deviation inthe controls. Potential differences in population admixturebetween the 2 groups are difficult to exclude. Recent studiesestimate that genome-wide analysis of 2,000 biallelic markerswill be required to extract 70–90% of ancestry information fora given locus (13). This may only be possible when a compre-hensive genome map of single-nucleotide polymorphisms be-comes available.
Our observations suggest that PARP alleles may be inlinkage disequilibrium with a disease locus in this AfricanAmerican cohort. The seemingly different association resultsfor PARP and SLE in our study and that by Delrieu et al (5)are not unexpected in the genetic analysis of complex diseases,and may be attributed to genetic heterogeneity and populationhistory (whether cumulative recombination events have oc-curred in the studied populations to cause diminished linkageand diluted association with disease).
In summary, linkage of the human chromosome lq41-q42 region to SLE has been supported in independent data setssince our earlier report (1–3). Fine mapping near PARP allelesmay help in the identification of the putative susceptibilitygene within this region (11,12).
Supported by grants from the RGK Foundation, theUniversity of Texas LASR 2000 Research Fund, the NIH (GM-41399, GM-58545, AR-43814, and AI-45916), the SouthernCalifornia Chapter of the Arthritis Foundation, and the PaxsonFamily Foundation.
Filemon K. Tan, MD, PhDJohn D. Reveille, MDFrank C. Arnett, MDThe University of Texas–Houston Medical SchoolDavid N. Stivers, PhDThe University of Texas Health Science Center–HoustonSchool of Public HealthBetty P. Tsao, PhDUniversity of California, Los AngelesSchool of Medicine
Table 1. Comparison of PARP allele frequencies in AfricanAmerican SLE patients and controls*
Disease locus P†
P, deviation from HWE‡
SLE patients Controls
PARP 0.0185 ,1/10,000 0.170Noncoding forensic loci
D5S818 0.985 ,1/10,000 0.172D7S820 0.933 0.145 0.423D13S317 0.593 0.623 0.021
* PARP 5 poly(ADP)-ribose polymerase; SLE 5 systemic lupuserythematosus; HWE 5 Hardy-Weinberg equilibrium.† Based on 104 Monte Carlo simulations (8).‡ Fisher’s exact test for HWE within each group (9,10).
1421

1. Tsao BP, Cantor RM, Kalunian KC, Chen CJ, Badsha H, Singh R,et al. Evidence for linkage of a candidate chromosome 1 region tohuman systemic lupus erythematosus. J Clin Invest 1997;99:725–31.
2. Gaffney PM, Kearns GM, Shark KB, Ortmann WA, Selby SA,Malmgren ML, et al. A genome-wide search for susceptibilitygenes in human systemic lupus erythematosus sib-pair families.Proc Natl Acad Sci U S A 1998;95:14875–9.
3. Moser KL, Neas BR, Salmon JE, Yu H, Gray-McGuire C, AsundiN, et al. Genome scan of human systemic lupus erythematosus:evidence for linkage on chromosome 1q in African-Americanpedigrees. Proc Natl Acad Sci U S A 1998;95:14869–74.
4. Tsao BP, Cantor RM, Grossman JM, Shen N, Teophilov NT,Wallace DJ, et al. PARP alleles within the linked chromosomalregion are associated with systemic lupus erythematosus. J ClinInvest 1999;103:1135–40.
5. Delrieu O, Michel M, Frances C, Meyer O, Michel C, Wittke F, etal. Poly(ADP-ribose) polymerase alleles in French Caucasians areassociated neither with lupus nor with primary antiphospholipidsyndrome. Arthritis Rheum 1999;42:2194–7.
6. Hochberg MC. The epidemiology of systemic lupus erythemato-sus. In: Wallace DJ, Hahn BH, editors. Dubois’ lupus erythema-tosus. Baltimore: Williams and Wilkins; 1996. p. 49–65.
7. Tan EM, Cohen AS, Fries JF, Masi AT, McShane DJ, RothfieldNF, et al. The 1982 revised criteria for the classification of systemiclupus erythematosus. Arthritis Rheum 1982;25:1271–7.
8. Sham PC, Curtis D. Monte Carlo tests for associations betweendisease and alleles at highly polymorphic loci. Ann Hum Genet1995;59:97–105.
9. Agresti A. Categorical data analysis. New York: John Wiley &Sons; 1990.
10. Guo SW, Thompson EA. Performing the exact test of Hardy-Weinberg proportion of multiple alleles. Biometrics 1992;48:361–72.
11. Feder JN, Gnirke A, Thomas W, Tsuchihaski Z, Ruddy DA,Basava A, et al. A novel MHC class I-like gene is mutated inpatients with hereditary hemochromatosis. Nat Genet 1996;13:399–408.
12. Nielsen DM, Ehm MG, Weir BS. Detecting marker-disease asso-ciation by testing for Hardy-Weinberg disequilibrium at a markerlocus. Am J Hum Genet 1999;63:1531–40.
13. McKeigue PM. Mapping genes that underlie ethnic differences indisease risk: methods for detecting linkage in admixed popula-tions, by conditioning on parental admixture. Am J Hum Genet1998;63:241–51.
Reply
To the Editor:The contribution of the PARP gene or a close locus to
susceptibility to SLE is still unclear. Using a multiallelictransmission-disequilibrium test, Tsao et al previously foundsignificant skewing of transmission of PARP alleles to affectedoffspring, preferential transmission of 1 of the PARP alleles toaffected offspring, and lack of transmission to unaffectedoffspring in 124 multiethnic families (1). Results remainedsignificant, though less strong, in the subset of 75 Caucasianfamilies (1). In contrast, using an association study approach,we did not observe any significant difference in the distributionof PARP alleles between French Caucasian controls and SLEpatients (n 5 193 healthy controls, 89 patients with sporadicSLE, 82 patients with familial SLE, 171 total SLE patients).
The study described in the letter by Tan et al included91 African American SLE patients and 53 normal AfricanAmerican controls from the same area. Consistent with ourfindings in French Caucasians, Tan and colleagues found no
significant association of any specific PARP allele with SLE.Interestingly, the overall distribution of PARP alleles amongSLE patients was significantly skewed compared with controlsby the Monte Carlo test. When testing for deviation fromHWE, Tan et al found significant deviation at the PARP locusamong African American SLE patients, but not among con-trols.
Within our French Caucasian SLE cohort, Monte-Carlo analysis did not show any skewing in the overall distri-bution of PARP alleles (105 simulations for each group:sporadic SLE P 5 0.44, familial SLE P 5 0.98, total SLE P 50.83). There was no significant deviation from HWE either incontrols (P 5 0.47) or in patients (sporadic SLE P 5 0.33,familial SLE P 5 0.64, total SLE P 5 0.60).
Taken together, these data can be interpreted indifferent ways. One conclusion could be that PARP alleles maybe in linkage disequilibrium with an SLE locus in the AfricanAmerican cohort studied by Tan et al and not in FrenchCaucasians. However, we would like to emphasize that strongcaution would be needed in making this interpretation forseveral reasons, including the small size of the cohorts and thedramatic effect of potentially overlooked population admix-ture. In addition, as noted recently by Nielsen et al (2), “careis needed in the drawing of inference from marker Hardy-Weinberg disequilibrium for disease-susceptibility loci withmore than two alleles.”
Alternatively, the observed skewing of the overalldistribution of PARP alleles could reflect differences betweencontrols and patients in genetic background. The deviationfrom HWE observed by Tan and colleagues for one forensiclocus in SLE cases and for another in controls could suggestthat both their African American patient group and theircontrol group are not indeed homogenous populations, butmay comprise mixed populations with distinct ethnic back-grounds. It should be remembered that African Americanscomprise a highly complex and heterogenous population orig-inating from many countries or areas (3), and this might havemajor implications given that subtle ethnic heterogeneity, suchas Anglo Saxon versus French descent, affects genetic suscep-tibility to SLE among Canadian Caucasian patients (4).
For all of these reasons, additional work is needed toelucidate the putative role of the PARP region in susceptibilityto SLE.
O. DelrieuE. Tournier-Lasserve, MDINSERM U25Faculte de Medecine Necker ParisJ. C. Piette, MDHopital de la Pitie Parisfor the Group for Researchon Auto-Immune DisordersParis, France
1. Tsao BP, Cantor RM, Grossman JM, Shen N, Teophilov NT,Wallace DJ, et al. PARP alleles within the linked chromosomalregion are associated with systemic lupus erythematosus. J ClinInvest 1999;103:1135–40.
2. Nielsen DM, Ehm MG, Weir BS. Detecting marker-disease asso-ciation by testing for Hardy-Weinberg disequilibrium at a markerlocus. Am J Hum Genet 1999;63:1531–40.
3. Bae S-C, Fraser P, Liang MH. The epidemiology of systemic lupuserythematosus in populations of African ancestry: a critical review
1422 LETTERS

of the “prevalence gradient hypothesis.” Arthritis Rheum 1998;41:2091–9.
4. Goldstein R, Sengar DPS. Comparative studies of the majorhistocompatibility complex in French Canadian and non–FrenchCanadian Caucasians with systemic lupus erythematosus. ArthritisRheum 1993;36:1121–7.
Analysis of the association of the matrillin-1 gene(CRTM) with osteoarthritis: comment on the articleby Meulenbelt et al
To the Editor:Meulenbelt et al (1) have reported a significant asso-
ciation between the microsatellite polymorphism in the 39-untranslated region of the matrillin 1 gene (CRTM, 1p35) andradiographically evident hip osteoarthritis (OA) in DutchCaucasian males. The 110-basepair allele of this polymorphismwas found at an increased frequency in their male hip OAcases (frequency 0.66; n 5 37) compared with their malecontrols (frequency 0.51; n 5 63), and this increase wassignificant (P 5 0.04). To test this association, we havegenotyped the CRTM microsatellite in a proband–spousecase–control cohort.
The cohort was composed of 338 OA cases (probands)and 338 controls (spouses of the cases), all Caucasians fromthe UK. Of the 338 cases, 199 were female and 139 were male.All cases were ascertained through the Nuffield OrthopaedicCentre in Oxford, and all had undergone total joint replace-ment (TJR) of the hip, knee, or hip and knee, for idiopathicOA. Patients who underwent TJR secondary to other factorswere excluded. Controls had not undergone any joint replace-ment surgery and had not required or sought clinical treatmentfor OA. The average age of the cases and controls whenrecruited into the study was 73. The average age of the cases atTJR was 65 (64 for females and 67 for males). The CRTMmicrosatellite was amplified as described previously (2), butwith the forward polymerase chain reaction primer fluores-cently labeled. The amplification products were electropho-resed through 5% LongRanger acrylamide (FMC BioProd-ucts, Rockland, ME) using a DNA sequencer (ABI model 377;Applied Biosystems, Foster City, CA).
Table 1 lists the allele frequencies of the CRTMmicrosatellite in the cases and controls. Also listed are thefrequencies following stratification of the cases and controlsfor sex, and of the cases for joint replaced (hip or knee) and forsex combined with joint replaced. A hip-only case is anindividual who has undergone either unilateral or bilateral hipreplacement without knee replacement. Similarly, a knee-onlycase refers to an individual who has had either unilateral orbilateral knee replacement but not hip replacement. In previ-ous analyses of the CRTM microsatellite (1,3), 4 alleles weredetected (102 bp, 106 bp, 108 bp, and 110 bp). In our analysisof a larger number of individuals, we detected a rare fifth alleleof 112 bp in size.
We compared the allele frequencies using contingencytable analysis. P values, under the null hypothesis of no genefrequency differences between groups, were calculated usingasymptotic chi-square. Since we were specifically testing allele1, we combined alleles 2, 3, 4, and 5 and performed a 2 3 2analysis. There was no significant difference (at P , 0.05) inthe frequency of alleles between the unstratified cases and theunstratified controls, nor was there a significant difference
between the male cases and the female cases. When the caseswere stratified according to joint replaced (hip-only or knee-only), there was an elevated frequency of allele 1 in knee-onlycases compared with hip-only cases (0.65 versus 0.58). Amongthe hip-only cases, there was no significant difference in thefrequency of allele 1 between males and females. Furthermore,allele 1 was found at a lower frequency in the 92 male hip-onlycases compared with the 199 male controls (0.59 versus 0.61).Overall, these observations were opposite to those of Meulen-belt et al (1).
The increase in frequency of allele 1 in our knee OAcases was restricted to males (frequency 0.75, versus 0.56 infemales with knee OA). This increase was significant when themale knee OA cases were compared with the female knee OAcases (x2 5 6.3 with 1 degree of freedom [df], 0.02 . P . 0.01)and with the male controls (x2 with 1 df 5 5.6, 0.02 . P .0.01).
To test this potential association between CRTM allele1 and knee OA in males, we typed an additional 107 unrelatedmales with knee OA (Table 1). These individuals were alsoCaucasians from the UK and were ascertained using the sameclinical criteria as for the initial cases (average age at TJR was65). Twelve of the 107 were ascertained as part of thecase–control cohort but were not included in that cohortbecause the original typing of the CRTM microsatellite hadbegun. The remaining 95 were from families identified as partof our OA linkage analysis program (4). The frequency ofallele 1 in these additional 107 male knee OA cases was 0.61.When these cases were combined with the original 42 maleknee OA cases, the combined frequency of allele 1 was 0.65.There was no significant difference in allele frequencies whenthe combined male knee OA cases were compared with themale controls (x2 with 1 df 5 1.3, 0.3 . P . 0.2). Increasing thenumber of male knee OA cases had therefore reduced theevidence of association.
Meulenbelt et al (1) rightly point out that theassociation with allele 1 that they observed in males with hipOA needed confirmation in additional male hip OA cohortsif it were to be considered a true as opposed to a false-positive association. In the present study we compared thefrequency of this allele between 92 males with OA who hadundergone hip replacement and 199 male controls, andobserved no association. We would therefore argue that theassociation reported by Meulenbelt et al (1) is probably afalse-positive one, although one must bear in mind theunknown underlying differences in structure of the UK andDutch populations. We did observe a significant increase inthe frequency of allele 1 in our male knee OA cases initiallystudied. However, an examination of a larger cohort of maleknee OA cases demonstrated that this increase also repre-sented a false-positive association.
John Loughlin, PhDBarbara Dowling, BScZehra Mustafa, BScAnne Smith, BScBryan Sykes, DScKay Chapman, PhDUniversity of OxfordOxford, UK
LETTERS 1423

1. Meulenbelt I, Bijkerk C, de Wildt SCM, Miedema HS, Valkenburg HA,Breedveld FC, et al. Investigation of the association of the CRTM andCRTL1 genes with radiographically evident osteoarthritis in subjects fromthe Rotterdam study. Arthritis Rheum 1997;40:1760–5.
2. Loughlin J, Irven C, Fergusson C, Sykes B. Sibling pair analysisshows no linkage of generalised osteoarthritis to the loci encodingtype II collagen (COL2A1), cartilage link protein (CRTL1) orcartilage matrix protein (CRTM). Br J Rheumat 1994;33:1103–6.
3. Wang Y, Sadler L, Hecht JT. Polymorphic dinucleotide repeat in acartilage matrix protein (CRTM) gene. Hum Mol Genet 1992;1:780.
4. Chapman K, Mustafa Z, Irven CM, Carr AJ, Clipsham K, Smith A,et al. Osteoarthritis-susceptibility locus on chromosome 11q, de-tected by linkage. Am J Hum Genet 1999;65:167–74.
Reply
To the Editor:Loughlin et al tested for an association between poly-
morphism in the 39-untranslated region of the matrillin 1 gene(CRTM) and joint replacement at the hip and/or knee. Theabsence of association in their study suggests that the CRTMlocus does not contribute to this clinical end point of knee andhip OA. In view of these results, they mention the possibilitythat the association of the same CRTM polymorphism andradiographically evident hip OA in Dutch men observed in ourstudy may be a false-positive association. As discussed in our
Table 1. Allele frequencies in the 338 cases and 338 controls (unstratified and stratified) and in 107additional males with knee osteoarthritis
Allele (length in bp)
1 (110) 2 (108) 3 (106) 4 (102) 5 (112)
Initial study groupUnstratified cases (n 5 338)
No. 403 241 30 0 2Frequency 0.60 0.36 0.04 0.00 0.00
Unstratified controls (n 5 338)No. 418 227 28 1 2Frequency 0.62 0.34 0.04 0.00 0.00
Male cases (n 5 139)No. 178 90 10 0 0Frequency 0.64 0.32 0.04 0.00 0.00
Female cases (n 5 199)No. 225 151 20 0 2Frequency 0.57 0.38 0.05 0.00 0.00
Male controls (n 5 199)No. 241 137 17 1 2Frequency 0.61 0.34 0.04 0.00 0.01
Female controls (n 5 139)No. 177 90 11 0 0Frequency 0.64 0.32 0.04 0.00 0.00
Hip-only cases (n 5 233)No. 270 174 21 0 1Frequency 0.58 0.37 0.05 0.00 0.00
Male hip-only cases (n 5 92)No. 108 69 7 0 0Frequency 0.59 0.37 0.04 0.00 0.00
Female hip-only cases (n 5 141)No. 162 105 14 0 1Frequency 0.57 0.37 0.05 0.00 0.00
Knee-only cases (n 5 91)No. 118 56 8 0 0Frequency 0.65 0.31 0.04 0.00 0.00
Male knee-only cases (n 5 42)No. 63 18 3 0 0Frequency 0.75 0.21 0.04 0.00 0.00
Female knee-only cases (n 5 49)No. 55 38 5 0 0Frequency 0.56 0.39 0.05 0.00 0.00
Additional study group (male knee cases; n 5 107)No. 131 78 5 0 0Frequency 0.61 0.37 0.02 0.00 0.00
Male knee cases: initial study group 1 additionalstudy group (n 5 149)
No. 194 96 8 0 0Frequency 0.65 0.32 0.03 0.00 0.00
1424 LETTERS

report, association studies in general are indeed subject tofalse-positive findings, which prompted us to advocate thenecessity of confirmation of findings in an additionalpopulation-based sample. However, we would argue that thedifferences in design and population structure between Lough-lin’s study and ours may explain the inconsistent results.
We studied the association of the CRTM gene within apopulation-based cohort (the Rotterdam study) (1), in whichradiographs of knee, hip, hand, and spine in subjects between55 and 65 years of age were scored for the presence ofradiographic signs of OA (Kellgren-Lawrence scale) (2). Casesfrom this cohort were selected for the presence of radiographicOA in the hip joint, whereas controls in our study were subjectswithout any radiographic OA (only 13% of the cohort of 1,040subjects). The association observed in our study was due to anincreased frequency of allele 1 in cases (0.66) and a decreasedfrequency in controls (0.51), as compared with the populationfrequency (0.59). The relatively strict selection criteria for ourcontrols may have attenuated the association. In contrast, casesin the study by Loughlin and colleagues had total jointreplacement at an average age of 65 years, which is a muchmore severe clinical end point of OA than the radiographicOA of the hip present in our cases. Furthermore, controls inthe study by Loughlin et al were not selected based on theabsence of radiographic OA, but were spouses (of the cases)without clinical joint disease. Indeed, the frequency of allele 1differed considerably between our study and the one byLoughlin for male controls (0.51 and 0.61, respectively) as wellas for male cases (0.64 and 0.59, respectively).
The findings reported by Loughlin et al indicate lim-ited relevance of the CRTM locus in relation to OA leading tojoint replacement. The contrasting outcome of the 2 studiesmay be either the result of a different definition of cases andcontrols and the low concordance of radiographic OA andclinical OA, or proof of a false-positive association in ourstudy.
As pointed out by Loughlin, it may also be that thereare underlying differences in structure of the UK and Dutchpopulations that hamper true replication of the associationbeing tested. This may especially be the case when testingpolymorphisms instead of the functional variation that under-lies the association. Different allele frequencies were alsoobserved for a Mae II polymorphism at the 39-untranslatedregion of COL2A1, as described by Loughlin and colleagues ina 1995 report (3). The frequency of the Mae II allele in ourstudy group (0.08) (4) was significantly higher than in theBritish group (0.03) (3). In addition, the association of this rareMae II allele with increased susceptibility to generalized OA inthe British population (3) was not observed in the Dutch (4).
The absence of confirmation of the CRTM andCOL2A1 associations with OA may indicate that we shouldreconsider whether UK and Dutch patients are suitable pop-ulations for association studies testing for replication of find-ings with nonfunctional polymorphisms. To confirm associa-tions, it may be important to conduct large population-basedstudies that are able to provide their own replication sample.Findings regarding COL2A1 and CRTM underscore the factthat functional followup of genetic association studies is cru-cial.
Ingrid Meulenbelt, PhDP. Eline Slagboom, PhDTNO Prevention and HealthGaubius LaboratoryLeiden, The NetherlandsCornelia van Duijn, PhDErasmus University Medical SchoolRotterdam, The Netherlands
1. Hofman A, Grobbee DE, de Jong PTVW, van Den Ouweland FA.Determinants of disease and disability in the elderly: the RotterdamElderly Study. Eur J Epidemiol 1991;7:403–22.
2. Kellgren JH, Lawrence JS. Radiological assessment of osteoarthro-sis. Ann Rheum Dis 1957;16:494–501.
3. Loughlin J, Irven C, Athanasou N, Carr A, Sykes B. Differentialallelic expression of the type II collagen gene (COL2A1) inosteoarthritic cartilage. Am J Hum Genet 1995;56:1186–93.
4. Meulenbelt I, Bijkerk C, de Wildt SCM, Miedema HS, BreedveldFC, Pols HAP, et al. Haplotype analysis of three polymorphisms ofthe COL2A1 gene and associations with generalised radiologicalosteoarthritis. Ann Hum Genet. In press.
Diagnosis of osteoarthritis in relation to molecularprocesses in cartilage: comment on the article byClark et al
To the Editor:In a recent well-performed study by Clark and cowork-
ers (1), serum concentrations of cartilage oligomeric matrixprotein (COMP) were shown to reflect both the presence andthe severity of osteoarthritis (OA). Interestingly, althoughserum levels of COMP were higher in patients with radio-graphic knee/hip OA in all age groups studied, these levelsincreased with age both in the OA group and in the controlgroup. We have previously demonstrated that serum levels ofCOMP relate to presence and progression of OA (2,3), and theresults of the study by Clark and coworkers support the notionof the utility of COMP as a biologic marker of the OA process.
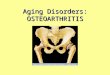
Data on age-related variations in serum COMP levelshave not been published before, other than in the report byClark et al. In support of their findings, we report herein asimilar relationship between serum COMP levels and age inblood donors (Figure 1). Although we examined only 74individuals, the results closely resemble those in the US study.To facilitate comparisons, we present the data using the samearbitrary age groups as in the report by Clark and coworkers.We also include individuals of younger age, which enables us toshow that serum COMP levels remain stable until ;50 years ofage.
A crucial issue is how to interpret the finding ofincreasing serum COMP levels in individuals in the older agegroups, be they radiographically “unaffected controls” orblood donors not examined radiographically. Clark et al con-clude that “the explanation for this phenomenon is currentlyunknown.” This implies that they consider radiographic find-ings to be the “gold standard,” which is understandable butmay not be correct from a biologic standpoint. We would arguethat molecular markers such as COMP reflect ongoing pro-cesses in the tissue and that measurements of cartilage com-ponents in body fluids reflect changes in the tissue turnover injoint disease before any changes are visible radiographically(4). Radiographic features, in contrast, reflect the conse-
LETTERS 1425

quences of processes that may have occurred over a longperiod, i.e., radiographic results depict biologically advanceddisease. Thus, the biochemical process in the tissue that isreflected by release of tissue proteins or their fragments by farprecedes the gross morphologic changes that are reflected withthe use of currently available imaging techniques, such asconventional radiography.
Consequently, we suggest that the individuals in the“control” groups in the 2 studies who show increased serumCOMP levels might be ones in whom an OA process is ongoingbut still at a stage where symptoms (as in our Swedish study) orradiographic changes (as in the US study) have not appeared.We realize that this is as yet speculative, and prospectivestudies should be performed to confirm the hypothesis.
We believe there is a need for an approach to theinvestigation of OA pathophysiology that is not dependentonly on a radiographic definition of the disease. In fact,defining patient groups strictly according to radiographic fea-tures may hamper research progress since primarily severecases will be studied. Thus, the evaluation of novel tools forresearch and clinical use, such as molecular markers, shouldnot rely on a crude “gold standard” which does not identify theprocesses that can be monitored by the marker (e.g., serumCOMP). In other words, we don’t need molecular markers thatconfirm what we see on radiographs; we need markers thatidentify changes before any changes are apparent radiograph-ically. An approach that focuses on detailed prospective stud-ies of biochemical events in early phases of OA, identified bychanges in molecular marker patterns, would, in our opinion,facilitate the understanding and treatment of this enigmaticcondition. Radiography undoubtedly still has a role as anoutcome measure in these studies.
In conclusion, we very much agree with the conclusionby Clark and coworkers that serum COMP may be useful as amarker for OA. We suggest that the future development of thisand other potential cartilage markers would benefit from anapproach that examines the OA process from the perspectiveof the early tissue events, rather than from the perspective ofradiographic features indicating advanced tissue events.
Bengt Månsson, MD, PhDDick Heinegård, MD, PhDTore Saxne, MD, PhDLund UniversityLund, Sweden
1. Clark AG, Jordan JM, Vilim V, Renner JB, Dragomir AD, Luta G,et al. Serum cartilage oligomeric matrix protein reflects osteoarthri-tis presence and severity: the Johnston County OsteoarthritisProject. Arthritis Rheum 1999;42:2356–64.
2. Petersson IF, Boegård T, Svensson B, Heinegård D, Saxne T.Changes in cartilage and bone metabolism identified by serummarkers in early osteoarthritis of the knee joint. Br J Rheumatol1998;37:46–50.
3. Conrozier T, Saxne T, Fan CS, Mathieu P, Tron AM, Heinegård D,et al. Serum concentrations of cartilage oligomeric matrix proteinand bone sialoprotein in hip osteoarthritis: a one year prospectivestudy. Ann Rheum Dis 1998;57:527–32.
4. Månsson B, Geborek P, Saxne T. Cartilage and bone macro-molecules in knee joint synovial fluid in rheumatoid arthritis:relation to development of knee or hip joint destruction. AnnRheum Dis 1997;56:91–6.
Reply
To the Editor:We would like to thank Drs. Mansson and colleagues
for presenting their results on serum COMP levels in blooddonors, corroborating our finding of an increase starting in thefifth decade of life. They raise the very important and as-yet-unresolved issue of the cause of this phenomenon. Theysuggest the possibility that the older “control” individualsshowing an increase in serum COMP levels might be develop-ing OA in joints other than those specifically evaluated in thestudy. From our models, we have seen a similar effect of age incases and controls after controlling for demographics. We havework in progress suggesting that the age effect on COMP isvirtually unchanged even after controlling further for variableswhich address pain in remaining joints not assessed radio-graphically. Thus, although we certainly concur with the sug-gestion that the joint burden of OA may be increasing with ageand may be one cause for increasing serum COMP levels withage, we also favor a hypothesis that there is some phenomenonworking to raise serum COMP levels systematically with age.Possibilities for such an age-related phenomenon might in-clude changes in cartilage or other joint tissue metabolism, orchanges in blood clearance of COMP.
We share the enthusiasm expressed by Mansson et alfor identifying surrogate markers of early, preradiographicOA. For now, however, OA markers must by necessity bevalidated in the context of the existing “gold standards,”namely, imaging modalities. We would ideally recommendevaluation of promising OA biologic markers for age, race, sex,and body mass index effects and ultimately, evaluation of theirability to detect early pathologic changes in joint tissues.Validation in longitudinal studies will be necessary to ensurethat levels of a biologic marker, or a change in levels of abiologic marker, will predict the entity we know as OA in thelong term. We compliment the authors for having originallyidentified the COMP marker, which currently appears to beone of the most promising for OA research.
Figure 1. Serum concentrations of cartilage oligomeric matrix protein(COMP) in blood donors of different ages (n 5 74). The significanceof group differences was calculated by Mann-Whitney U test (2-tailed).N.S. 5 not significant (P $ 0.05).
1426 LETTERS

Virginia B. Kraus, MD, PhDAmy G. Clark, BSJoanne M. Jordan, MD, MPHAnca D. DragomirGheorghe Luta, MSVladimir Vilim, PhDDuke University Medical CenterDurham, NC
Trends in the inflammatory response in biopsy-provengiant cell arteritis: comment on the article by Cid etal, and the letters by Nesher and Sonnenblick andLiozon et al
To the Editor:There has recently been much controversy about the
relationship between severe cranial ischemic complicationsand the intensity of the inflammatory response in giant cell(temporal) arteritis (GCA). Cid et al observed a negativecorrelation between inflammatory response and the presenceof severe ischemic complications, mainly related to permanentvisual loss (1). In keeping with these findings, Liozon et al alsodescribed a negative correlation between the hemoglobinlevels/erythrocyte sedimentation rate values and the develop-ment of cranial ischemic complications (2). In a collaborativemulticenter study with investigators at 2 other hospitals inSpain, we found a negative correlation between fever/weightloss and the occurrence of permanent visual loss (3). Incontrast, Nesher and Sonnenblick did not demonstrate anycorrelation between the degree of inflammatory response andthe risk of irreversible ischemic complications in GCA (4).Liozon and colleagues suggested that the intensity of thebiologic inflammatory response might correlate indirectly withthe development of irreversible ischemic complications ofGCA (2).
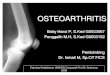
To further investigate this question, we analyzed therelationship between anemia (defined as hemoglobin value,12 gm/dl) and the occurrence of ischemic visual complica-tions (permanent or transient visual loss and/or diplopia) ofGCA in a well-defined area of northwestern Spain (Lugo),where Xeral-Calde Hospital (Lugo) is the single hospital for astable population of ;250,000. We examined the relationshipbetween the hemoglobin value at the time of admission and itscorrelation with the development of visual manifestations inGCA. Between 1981 and 1998, 161 cases of biopsy-provenGCA were diagnosed in Lugo. We have observed a progressiveincrease in the incidence of GCA, especially during the lastdecade (5,6). Therefore, we analyzed the possible correlationbetween hemoglobin and visual manifestations during differ-ent time periods. We considered 4 time periods, with ;40patients with GCA in each period. As shown in Figure 1, therewas a progressive decrease over time in the risk of visualmanifestations in GCA patients with anemia in the Lugo area.According to our data, whereas in the 1980s there was no clearcorrelation between hemoglobin level and the development ofvisual manifestations, in the last 10 years it has been moreevident that the risk of ischemic visual manifestations isnegatively correlated with the presence of anemia. Such atrend was clearer during the last time period (1997–1998; 37cases), when the risk of visual complications was very low: only
2 of 21 patients with hemoglobin values ,12 gm/dl developedocular ischemic manifestations, and none developed perma-nent visual loss. In this 1997–1998 period, 7 of the 9 patientswho had visual complications had hemoglobin values .12gm/dl. Based on these data, we are tempted to speculate thatthe occurrence of anemia may now be a protective factoragainst the development of visual manifestations of GCA.
Although at present it is difficult to identify patients athigh risk for severe ischemic complications based only on thepresence of a high inflammatory response, the similaritybetween these observations and those recently reported byother authors may support a possible change in the clinicalspectrum of the disease. Multicenter prospective studiesshould be undertaken to further delineate clinical diseasepatterns associated with high or low risk of severe ischemiccomplications.
Miguel A. Gonzalez-Gay, MD, PhDCarlos Garcıa-Porrua, MD, PhDPilar Rodrıguez-Ledo, MDHospital Xeral-CaldeLugo, SpainJavier Llorca, MD, PhDUniversity of CantabriaSantander, Spain
1. Cid MC, Font C, Oristrell J, de la Sierra A, Coll-Vinent B,Lopez-Soto A, et al. Association between strong inflammatoryresponse and low risk of developing visual loss and other cranialischemic complications in giant cell (temporal) arteritis. ArthritisRheum 1998;41:26–32.
2. Liozon E, Jauberteau MO, Loustaud V, Vidal E. Associationbetween the inflammatory response and the risk of developingirreversible cranial ischemic complications: comment on the articleby Cid et al and the letter by Nesher and Sonnenblick [letter].Arthritis Rheum 1999;42:2256–7.
Figure 1. Trends in the relationship between anemia (hemoglobin,12 gm/dl) and visual complications in 161 patients with biopsy-proven giant cell arteritis in northwestern Spain. Horizontal bars showthe odds ratios; vertical bars show the 95% confidence intervals.
LETTERS 1427

3. Gonzalez-Gay MA, Blanco R, Rodrıguez-Valverde V, Martınez-Taboada VM, Delgado-Rodrıguez M, Figueroa M, et al. Permanentvisual loss and cerebrovascular accidents in giant cell arteritis:predictors and response to treatment. Arthritis Rheum 1998;41:1497–504.
4. Nesher G, Sonnenblick M. No association between the inflamma-tory response and the risk of developing irreversible cranial isch-emic complications: comment on the article by Cid et al [letter].Arthritis Rheum 1998;41:2088.
5. Gonzalez-Gay MA, Blanco R, Sanchez-Andrade A, Vazquez-Caruncho M. Giant cell arteritis in Lugo, Spain: a more frequentdisease with fewer classic features. J Rheumatol 1997;24:2166–70.
6. Gonzalez-Gay MA, Garcıa-Porrua C. Systemic vasculitis in adults inNorthwestern Spain, 1988–1997: clinical and epidemiologic aspects.Medicine (Baltimore) 1999;78:292–308.
Reply
To the Editor:As Dr. Gonzalez-Gay et al note, our article reporting
an association between a strong inflammatory response (de-fined by clinical [fever and weight loss] and biochemical[erythrocyte sedimentation rate and hemoglobin concentra-tion] parameters) and a low risk of developing cranial ischemiccomplications in GCA has generated some discussion (1–3). Ingeneral, although the study designs and the sets of parametersevaluated by different groups are heterogeneous, a similartrend has been observed by the majority of authors who haveaddressed this (1,2,4). In a previous study, Gonzalez-Gay et alalso reported a negative correlation between fever/weight lossand the risk of permanent visual impairment in GCA (4).Consistent with our data, in their present letter they describe asignificantly reduced risk of visual impairment in GCA patientswith hemoglobin levels of ,120 gm/liter. However, this corre-lation was observed only in patients diagnosed in recent years.They conclude that since no clear correlation between hemo-globin levels and visual manifestations was observed in patientsdiagnosed in the 1980s or early 1990s, a change in the clinicalspectrum of disease may be occurring.
In our study, the risk of ischemic events was definitivelylower in patients with anemia, and this continues to beobserved in our present extended series of 250 patients (oddsratio [OR] 0.38, 95% confidence interval [95% CI] 0.18–0.82).We believe that the data presented by Gonzalez-Gay andcolleagues are very similar to ours, and there are just somemethodologic differences that reduce the sensitivity of theirevaluation. First, they refer to visual manifestations, not topermanent cranial ischemic events. When we considered allkinds of visual events together, regardless of whether they weretransient or irreversible, we obtained virtually the same results,but the association was much weaker. This may be becausetransient visual phenomena are subjective and sometimesdifficult to evaluate in elderly people who not infrequentlyhave visual impairment associated with other diseases. Second,we calculated the risk in association with hemoglobin values,110 gm/liter whereas the threshold chosen by Gonzalez-Gay
et al was 120 gm/liter. A hemoglobin value ,110 gm/liter ismuch more discriminative in a population in which elderlywomen predominate. In fact, we did not find significantdifferences in the risk for ischemic events in patients withhemoglobin values .120 gm/liter versus those with values,120 gm/liter in our complete series (OR 0.68, 95% CI0.32–1.44).
Gonzalez-Gay et al have found the negative correla-tion between anemia and ischemic events to be more evident inrecent years. We have also found that the strength of thiscorrelation fluctuates among different periods of time, but wehave not observed a tendency toward an increase in recentyears in our series. In fact, variations in OR over the years aremostly related to small fluctuations in the number of patientswith ischemic events at a given time point since this num-ber is, fortunately, low. The periods of time examined byGonzalez-Gay are very variable (9, 4, 3, and 2 years), and thecriteria used to define these periods are not clear. According tothe data presented in their figure, if the OR had beencalculated for homogeneous periods of 5 or 10 years, theputative tendency to increase would have been less evident.
We agree that a definitive identification of parameterswith predictive value in identifying patients at high or low riskof developing ischemic complications and the definition ofclinically useful thresholds requires prospective multicenterstudies. A prospective multicenter study with the collaborationof the International Network for the Study of Systemic Vas-culitis is now ongoing, and we would be very pleased ifGonzalez-Gay et al would join their efforts with ours.
Maria C. Cid, MDCarme Font, MDJose Hernandez-Rodrıguez, MDAlejandro de la Sierra, MDBlanca Coll-Vinent, MDAlfons Lopez-Soto, MDAlvaro Urbano-Marquez, MDJosep M. Grau, MDUniversity of Barcelona Medical SchoolBarcelona, Spain
1. Nesher G, Sonnenblick M. No association between the inflamma-tory response and the risk of developing irreversible cranial isch-emic complications: comment on the article by Cid et al [letter].Arthritis Rheum 1998;41:2088.
2. Liozon E, Jauberteau MO, Loustaud V, Vidal E. Associationbetween the inflammatory response and the risk of developingirreversible cranial ischemic complications: comment on the articleby Cid et al and the letter by Nesher and Sonnenblick [letter].Arthritis Rheum 1999;42:2256–7.
3. Schmidt D, Vaith P. Acute-phase response and the risk of devel-oping ischemic complications in giant cell arteritis: comment on thearticle by Cid et al [letter]. Arthritis Rheum 2000;43:234–5.
4. Gonzalez-Gay MA, Blanco R, Rodrıguez-Valverde V, Martınez-TaboadaVM, Delgado-Rodrıguez M, Figueroa M, et al. Permanent visual loss andcerebrovascular accidents in giant cell arteritis: predictors and response totreatment. Arthritis Rheum 1998;41:1497–504.
1428 LETTERS