Embed Size (px)
Citation preview

Anaphylaxis
Jesse Sturm, MD
PEM Fellow
October 3, 2007

2
This is a Test
It is ONLY a Test

3
A 16 y/o girl just passed out after receiving her penicillin shot for strep throat (“doesn’t swallow pills”). Which of the following will be most useful to know in treating her:
A Her Blood Pressure
B Her Glucose level
C Her Heart Rate
D Your Heart Rate

4
Which of the following is the safest and most efficient route to administer epinephrine in an allergy emergency:
A IV
B Sub Q
C IM
D PR

5
When advising parents/patients on how to administer an “epi-pen” you should tell them to:
A. hold it against the triceps and squeeze the trigger
B. “stab” it into the anterior thigh
C. hold it against the lateral thigh and push

6
Which is NOT a clinical presentation of anaphylaxis:
A. Vomiting and Diarrhea
B. Syncope
C. Altered Mental Status
D. Itchy Tongue

7
In counseling a 50kg 15 year old after a severe episode of anaphylaxis to a bee sting your best advice is that if they get stung again they first should take
A. (2) 25mg diphenhydramine capsules PO
B. (5) tsp diphenhydramine elixir PO
C. .5mg epinephrine SQ
D. 60mg prednisone PO

8
Which of the following treatments has been shown to decrease the incidence of biphasic reactions:
A. Corticosteroids
B. Epinephrine
C. Diphenhydramine
D. Ranitidine

9
Objectives
Definition of anaphylaxis Epidemiology Presenting signs and symptoms What is the management algorithm
• Supporting evidence for medication usage• Biphasic reactions

10
History
First recorded case in Egyptian hieroglyphics 2641 B.C. – Pharaoh Menes died after wasp sting
Modern times – named by French scientists investigating anemone stings on dogs• “aphylaxis”
a – contrary phylaxis – protection
• Changed to anaphylaxis because sounded better

11
Definition
Anaphylactic: allergic, IgE-mediated, immediate hypersensitivity reactions to protein substances • Requires previous exposure to antigen to form IgE
Anaphylactoid: clinically indistinguishable, NOT IgE-mediated i.e. contrast media• Does not require previous antigen exposure• Unknown mechanism
Anaphylaxis: clinical syndrome, regardless of mechanism

12
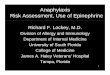
Mechanism
IgE antibodies form upon initial Ag exposure• IgE binds to high-affinity Fc receptor on mast cell• Re-exposure, Ag bridges IgE → mast cell
degranulation → release of preformed mediators (histamine, prostaglandin D2, leukotrienes)
Direct complement cascade activation by Ag resulting in anaphylatoxins C3a and C5a • Directly degranulate mast cells
Non-IgE and non-complement mechanism• Direct activity on mast cells• Hyperosmolar solutions (mannitol, radiocontrast)

13

14
Epidemiology
Incidence varies – lack of consensus definition• ~ 10.5 per 100,000 person-years
1% of all ED visits in both children and adults Fatality rate: ~ 1% 1500 deaths per year in all ages
• 1300 drug induced• 100 food and sting induced
Children with atopy and asthma at higher risk One study – males < 15yo, OR 1.9 for anaphylaxis
compared to girls

15
Clinical Criteria
Anaphylaxis is highly likely when any one of the following 3 criteria are met.
1. Acute onset of an illness with involvement of skin, mucosal tissue, or both and at least one of the following:
a. Respiratory compromiseb. Reduced BP or end-organ dysfunction.
2. Two or more of the following that occur rapidly after exposure to a likely allergen for that patient:
a. Involvement of the skin mucosal tissueb. Respiratory compromisec. Reduced BP or associated symptomsd. Persistent GI symptoms
3. Reduced BP after exposure to known allergen for that patient.
Sampson et al Annals of Emerg Med Apr 2006

16
Anaphylaxis TriggersReaction to previously known antigen: 21.1%
1. FOOD: 56%
-Peanut, egg, dairy, seafood, food additives/dyes
2. DRUGS: 5%
-Penicillins, cephalosporins, NSAIDs, other
3. INSECTS: 5%
-Bees, wasps, ants
4. NO cause identified: 18%Braganza et al. Arch Dis Child 2006 N=57
Others: Blood products, Immunotherapy, Latex, Vaccines, Radiocontrast media

17
Causes of Anaphylaxis: All Ages
Retrospective review 601 patients with anaphylaxis Excluded hymenoptera stings Causes:
Idiopathic: 59%
Food: 22%
Meds: 11%
Exercise: 5% – rare in children
Latex: 1%
Webb M. Ann Allergy Asthma Immunol. 2006

18
Foods
Peanut and Tree nuts: 1% Americans (3 million) allergic
Legumes: 25-35% also allergic to tree nuts
Shellfish Fish Milk Eggs Food additives: sulfites

19
Foods That May Contain Peanut Oil
Arachis oil (peanut oil) Baked Goods and
mixes Biscuits, cookies,
pastries Candy Cereals Chocolate Emulsifiers, flavorings Ethnic foods: African,
Chinese, Mexican, Thai, Vietnamese
Ice Cream Margarine Milk formula Satay Sauce (thai
sauce) Soft drinks Soups Sunflower seeds Vegetable fats and oils

20
Medication Triggers: All Ages
69 anaphylactic events Causes:
Aspirin: 35%
NSAID: 22%
B-Lactam: 20%
Insulin: 10%
Protamine: 3%
PCN and cephalosporins cross react in 4-10% Penicillin and NSAIDs most common in children
• PCN IgE mediated 1:40,000 in children

21
Venoms/Antivenins
5 major stinging insects in the US:• honeybees• wasps• yellow jackets• hornets• fire ants

22
Latex
Incidence low, except for risk groups:• Medically complex, multiple procedures
>1000 episodes and 15 deaths attributed Surgical and dental procedures highest risk RAST testing available

23
Vaccinations
Rare event < 1.5 events per million Most common MMR and Influenza
• Both chick-derived cellular vaccines MMR safe to give in egg allergy Influenza contraindicated in egg allergy

24
Anaphylaxis: Signs and Symptoms
Cutaneous 90%
Urticaria and angioedema 90%
Flushing 50%
Pruritus without rash 5% Respiratory 60%
Throat pruritis/tingling 50%
Dyspnea, wheeze 50%
Upper airway angioedema 60%
Rhinitis 20% Dizziness, syncope, hypotension 35% Abdominal 30%
Nausea, vomiting, diarrhea, cramping pain
Lieberman et al. American Academy of Allergy, Asthma and Immunology 2005

25
Other Symptoms to Look For
Sense of impending doom Uterine cramps Visual disturbances Metallic taste Increased lacrimation Seizure

26
Anaphylaxis Boy

27
Timing and Route of Exposure
Most symptoms occur within 5-30 minutes Parentally injected medication and hymenoptera
envenomation –more rapid Oral ingestion – may be rapid or delayed
Food ingestions more often associated with GI symptoms

28
Differential Diagnosis
Vasovagal reaction Hereditary angioedema Panic Attack Urticarial disorders Seizure Vocal cord dysfunction Systemic mastocytosis Status asthmaticus, croup, tracheitis Upper airway obstruction, foreign body

29
Management of Anaphylaxis
Medications:• Epinephrine
• H1 and H2 antagonists
• Vasopressors• Glucagon • Corticosteroids• Albuterol
Supportive measures:• Oxygen• Positioning• Fluid Resuscitation
Observation period Outpatient follow-up

30
Immediate Assessment
CR Monitor, pulseox Supine positioning with Trendelenberg if shock Assessment of ABC’s Oxygen by NRB, wean as tolerated
Early elective intubation for significant hoarseness and/or lingual or oropharyngeal edema• Consider sedated intubation without paralysis

31
Epinephrine
α1: promote vasoconstriction and decrease edema β1: increase inotropy and chronotropy Β2: bronchodilation and decreased mast cell
degranulation
Dose: 0.01mg/kg: 0.1-0.5mg (0.5mL) of Epi 1:1000 IM anterolateral thigh superior to SQ Repeat dose at 5-10min intervals as needed Persistent hypotension may reflect volume
depletion and not failure of Epinephrine

32
IM vs. SQ2 studies by Simons et al
Patients NOT experiencing anaphylaxis
Single blind study in children, n=17 MMEC= mean max epi concentration Location of injections not described
SQ: n=9. MMEC=1802pg/ml, @ 34min
IM: n=8. MMEC=2136pg/ml, @ 8min
Simons F. J Allergy Clin Immunol 1998
Simons F. J Allergy Clin Immunol 2001

33
Serum Levels: Adults

34
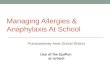
IM vs SQ: Adults
Adults:6 way crossover study, n=13
SQ deltoid: 2,877 pg/ml
IM deltoid: 1,821 pg/ml
Epipen thigh: 12,222 pg/ml
IM thigh: 9,722 pg/ml
Saline IM: 1458 pg/ml
Saline SQ: 1495 pg/ml

35
Epipen

36
IV Epinephrine
Indicated for persistent hypotension after IM Epi, IVF, and positioning OR shock• IV/IO: Epi 1:10,000 at 0.01mg/kg (0.1mL/kg), max 1mg
• Continuous infusion may be needed: 0.1-1μg/kg/min Evidence based on a few adult studies Can cause lethal arrhythmias
• Requires careful continuous monitoring, especially in the elderly

37
Epinephrine: Other Routes
Sublingual epinephrine vs. IM• Current study in rabbit model shows SL may be
similar in efficacy• Not definitive
Inhaled Epi from MDI-type system shown to be ineffective

38
Vasopressors
First line: intravenous epinephrine Second line: Vasopressin
2 adult case reports of anaphylaxis with shock
-42y/o s/p hornet sting, no improvement with 1mg Epi IV, improved with vasopressin (10 IU)
-47y/o s/p wasp sting improved with vasopressin (40 IU)
Other vasopressors: dopamine or norepinephrine Glucagon in persistently hypotensive pt taking beta-
blockers
Kill C, Int Arch Allergy Immunol, 2004.

39
Glucagon
Theoretical utility and case reports of efficacy:• Activates adenylate cyclase independent of
Beta receptor• May reverse refractory hypotension and
bronchospasm• Particularly helpful if taking beta-blocker
Adults: 1-5 mg IV Children 20-30 mcg/kg (max 1mg)
Followed by infusion 5-15mcg/min Significant SE of emesis
Javeed N. Cath & Card Diag, 1996.

40
Anti-histaminesFor symptomatic treatment of urticaria-angioedema and pruritus
H1 antagonists (Diphenhydramine):
• 25-50mg for adults• 1mg/kg for children (max 50mg)• IV route preferred for significant reactions
With H2 antagonists (Ranitidine, Cimetidine):
-Double blind controlled trial demonstrated efficacy
Claritin and other second generation antihistamines may have more efficacy than diphenhydramine but lack IV formulation
Lin R, Ann Emerg Med 2000.

41
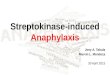
Primary Outcomes at 2 hours
N = 91 adults
Diphenhydramine+ Ranitidine
Diphenydramine + Placebo
Urticaria 4 11
Erythema 13 20
Angioedema 11 14
Lin R, Ann Emerg Med 2000.
Anaphylaxis symptoms at 2 hours with and without Zantac

42
Corticosteroids
No placebo-controlled trials supporting efficacy Theoretical utility
• May reduce late phase reaction based on results with asthma
• Some studies have found them to be ineffective Dosage:
• methylprednisolone 1-2mg/kg IV Q6 up to 125mg• prednisone 1-2mg/kg (max=50mg)• No data on dexamethasone
Duration for 72hrs for latent reactionsBiphasic reactions will be discussed in a few slides….

43
Supportive Measures
Supplemental oxygen Inhaled β2 agonists for wheezing
• No data on inhaled Atrovent in anaphylaxis Positioning in recumbent position Fluid resuscitation
• Vasodilatation and extravasation cause distributive shock
• Circulating volume can drop 35% within 10min• May require multiple boluses of crystalloid and/or
colloid (up to 60-80 mL/kg)Pumphrey R. J Allergy Clin Immunol 2003Boulain T. Chest 2002

44
Biphasic Reactions
Delayed reactions – up to 72 hours• Largest review in children - 6% incidence• Asymptomatic intervals 1.3 hrs to 28.4 hrs
Failure to administer prompt adequate doses of Epi increases risk of biphasic reaction
Route, quantity, and type of antigen NOT correlated with latent reaction
Symptoms and severity during initial reaction NOT predictive of latent reaction

45
Observation PeriodCan we predict biphasic reactions?
Study Number Frequency Time (hr)
Brazil 6/34 18% 4.5-29.5
Douglas 6/103 6% 1-72
Lee 6/105 5% 5-47.6
Stark 5/25 20% 1-8
Brady 2/67 3% 24-28
Smit 15/282 5% 1-23
Ellis 20/103 19.4% 2-38

46
Predictors of biphasic reactions?
Delayed administration of epinephrine Suspected but not proven
• Patient requiring high doses of epinephrine• Lower doses of corticosteroids given• Ingested antigen
There are NO reliable clinical predictors of biphasic reactions
Observation period individualized, but at least 6 hours

47
Laryngoscopy?
Consider early elective intubation in severe cases Endotracheal intubation for all children with orofacial
bee stings AND any airway compromise• Not all facial swelling requires intubation
Ditto A. Ann of All, Asthma and Immunol, 1995.
Tome R. Am J of Otolaryng, 2005.

48

49
Laboratory tests
Useful in uncertain cases• Prick skin tests: best screening test
high false positives; very few false negatives may require food challenge
• RAST: measures specific IgE less sensitive than skin prick
• Plasma Histamine: increases in 5-10 min, elevated for only 30-60min – not clinically useful
• Serum Tryptase: peak 1-1.5 hrs, inc for up to 5hrs Alpha: secreted constitutively Beta: released during degranulation, ratio helpful
• C1 inhibitor assay in hereditary angioedema• These tests have only limited utility in setting of
acute severe anaphylaxisLaRoche D. Anethesiology 1991.

50
Disposition(after appropriate observation period)
Severe reactions require observation for minimum 6-24hrs Observation time based on: severity of initial reaction,
home supervision, reliability of parent, access to care High risk patients:
• History of biphasic reaction, asthma, possibility of continued Ag absorption
Prescriptions for steroids and antihistamines for 72 hours
Three key components of disposition:
1. Self-injectable epi-pen
2. Education about avoidance of triggers and return of symptoms
3. Follow-up evaluation with allergist

51
Physician compliance
Study of patients with food related anaphylaxis from ED:• 35% patients given instructions for return symptoms• 22% given prescription for epi-pen• 13% referred to allergy specialist
Only 2% received all three!
Clark S. J Clin Immunol 2004
Clark S. J Clin Immunol 2005

52
Epipen dosing
2 fixed doses available (1:1000)• Epipen JR: 0.15mg (10kg-25kg)• Epipen: 0.3mg (>25kg)• <10kg – can be given Epi ampule and syringe
needle Parents studied took several minutes to draw
up doses, were inaccurate, and uncomfortable drawing up medication
Weigh risk and benefit with parents
Simons FE, J All and Clin Imm. 2002

53
Epipen
2 doses available at all times• Second injections necessary in 36% of patients
Childcare facilities and other caregivers must be familiar with indications for use and technique
Epi degrades over time and heat/cold will hasten degradation• Refill prescriptions at least annually

54
Summary
Give Epi IM in the thigh, dose early in course IV Epi reserved for persistently hypotensive patients Observation periods must be tailored to the
individual since biphasic reactions are unpredictable• Minimum of 6 hrs
Disposition requires:• Return precautions and trigger avoidance• Epipen prescriptions• Verbal referral to allergist
Ongoing multicenter studies:• Predictors of biphasic reactions

55
A 16 y/o girl just passed out after receiving her penicillin shot for strep throat (“doesn’t swallow pills”). Which of the following will be most useful to know in treating her:
A Her Blood Pressure
B Her Glucose level
C Her Heart Rate
D Your Heart Rate

56
Which of the following is the safest and most efficient route to administer epinephrine in an allergy emergency:
A IV
B Sub Q
C IM
D PR

57
When advising parents/patients on how to administer an “epi-pen” you should tell them to:
A. hold it against the triceps and squeeze the trigger
B. “stab” it into the anterior thigh
C. hold it against the lateral thigh and push

58
Which is NOT a clinical presentation of anaphylaxis:
A. Vomiting and Diarrhea
B. Syncope
C. Altered Mental Status
D. Itchy Tongue

59
In counseling a 50kg 15 year old after a severe episode of anaphylaxis to a bee sting your best advice is that if they get stung again they first should take
A. (2) 25mg diphenhydramine capsules PO
B. (5) tsp diphenhydramine elixer PO
C. .5mg epinephrine SQ
D. 60mg prednisone PO

60
Which of the following treatments has been shown to decrease the incidence of biphasic reactions:
A. Corticosteroids
B. Epinephrine
C. Diphenhydramine
D. Ranitidine

61
QUESTIONS?

62
END OF SHOW