Embed Size (px)
Citation preview

rxcc \'01. 4, No.3September 1984:601-10
DIAGNOSTIC TECHNIQUES
601
Anatomic and Electrophysiologic Substrate of the Permanent Form ofJunctional Reciprocating Tachycardia
GILSEPPE CRITELLI, MD, FACC, JOHN J. GALLAGHER, MD, FACC,* VITTORIO MONDA, MD,
FERNANDO COLTORTI, MD, MARINO SCHERILLO, MD, LINO ROSSI, MDt
Naples and Milan, Italy and Durham, North Carolina
Data are reported on three patients with the permanentform of junctional reciprocating tachycardia, in whomconduction over a slow accessory pathway was observedafter His bundle ablation. Tachycardia was almost incessant and showed a retrograde P wave (PI) and RP'interval longer than P'R interval in all patients; duringsinus rhythm, the PR interval was normal and there wasno evidence of a delta wave. An accessory pathway witha longconduction time located in the posterior pyramidalspace provided the retrograde limb of the reentry circuit. After His bundle ablation, the accessory pathwaywas capable of conducting in both anterograde and ret-
The permanent form of junctional reciprocating tachycardia,as defined by Coumel et al. in 1967 (1), presents the following clinical and electrocardiographic findings: 1) it occurs predominantly in infants and children; 2) it is nearlyincessant and usually unresponsive to conventional treatment: 3) initiation is commonly related to a critical shortening of the atrial cycle length (PP) without PR prolongation: 4) during tachycardia there is a 1:1 atrioventricular(AY) relation with a retrograde P wave (PI) negative inleads II, III and aYF and an RP' interval that is longer thanthe P'R interval.
The underlying mechanism of this arrhythmia is not knownand IwO hypotheses have been advanced: 1) an unusual (thatis, fast-slow) variety of intranodal reentry (2-5); and 2)reentry utilizing a concealed accessory pathway with a longconduction time (2,6-10).
In this study, we present data on three patients with the
From the Istituto di I Clinica Medica, II Facolta di Medicina e Chirurgia . Universita di Napoli, Naples, Italy. *Duke University MedicalCenter, Durham, North Carolina and the tIstituto di Anatomia Patologica,Universita di Milano, Milan, Italy. This study was supported in part byGram 8L01718.11 from the Consiglio Nazionale delle Ricerche, Rome,Italy Manuscript received December 9, 1983; revised manuscript receivedMarch 28, 1984, accepted April 13, 1984.
Address for reprints: Giuseppe Critelli, MD, Istituto di I Clinica Medica, II Policlinico Via Sergio Pansini, 5-80131 Napoli, Italy.
© 198,' by the American College of Cardiology
rograde directions with decremental properties in allpatients.
Postmortem documentation of the accessory pathwaywas achieved in one patient. Serial sections revealed anaccessory atrioventricular connection composed of ordinary myocardium joining the lower rim of the coronary sinus outlet to the uppermost ventricular muscle.This anomalous atrioventricular connection pursued asinuous, tortuous path. As a result of changing crosssectional area, such an accessory pathway might exhibitslow conduction, thus explaining its decrementalcharacteristics.
permanent form of junctional reciprocating tachycardia, inwhom conduction over a slow accessory pathway was observed in both anterograde and retrograde directions afterHis bundle ablation. In one of these patients, the presenceof the accessory pathway was demonstrated postmortem,providing certain anatomic-physiologic correlations.
Methods
Cfinical Data
Patient J was a 36 year old woman with no evidence oforganic heart disease, who had had supraventricular tachycardia for 14 years. Heart rate ranged between 130 and 180beats/min during tachycardia.
Patient 2 was a 52 year old man with a recent myocardialinfarction and a 15 year history of supraventricular tachycardia (130 to 160 beats/min).
Patient 3 was an 18 year old youth with obesity andtachycardia since birth. The tachycardia rate ranged between160 and 200 beats/min. He developed repetitive episodesof congestive heart failure in the last 2 years; physical examination of the heart showed marked cardiomegaly witha ventricular gallop and a grade 2/6 holosystolic murmuraudible at the apex. Slight peripheral edema was present.
In all patients, the tachycardia was almost incessant andunresponsive to pharmacologic treatment.
0735-1097/84/$3.00
602 CRITELLI ET AL.JUNCTIONAL RECIPROCATING TACHYCARDIA
JACC Vol. 4, No.3September 1984:601-10
Electrocardiographic Findings
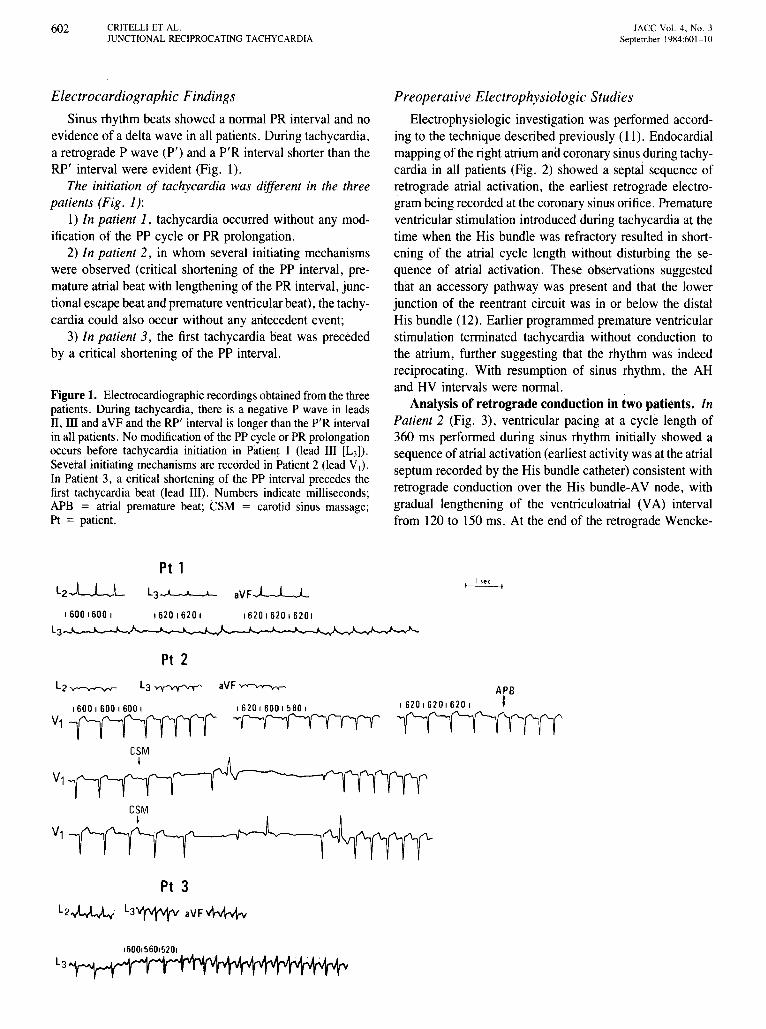
Sinus rhythm beats showed a normal PR interval and noevidence of a delta wave in all patients. During tachycardia,a retrograde P wave (Pi) and a P'R interval shorter than theRP' interval were evident (Fig. 1).
The initiation of tachycardia was different in the threepatients (Fig. 1):
I) In patient 1, tachycardia occurred without any modification of the PP cycle or PR prolongation.
2) In patient 2, in whom several initiating mechanismswere observed (critical shortening of the PP interval, premature atrial beat with lengthening of the PR interval, junctional escape beat and premature ventricular beat), the tachycardia could also occur without any antecedent event;
3) In patient 3, the first tachycardia beat was precededby a critical shortening of the PP interval.
Figure1. Electrocardiographic recordings obtained from the threepatients. During tachycardia, there is a negative P wave in leadsII, III and aVF and the RP' interval is longer than the P'R intervalin all patients. No modification of the PP cycle or PR prolongationoccurs before tachycardia initiation in Patient I (lead III [L3]) .
Several initiating mechanisms are recorded in Patient 2 (lead V,).In Patient 3, a critical shortening of the PP interval precedes thefirst tachycardia beat (lead III). Numbers indicate milliseconds;APB = atrial premature beat; CSM = carotid sinus massage;Pt = patient.
Preoperative Electrophysiologic Studies
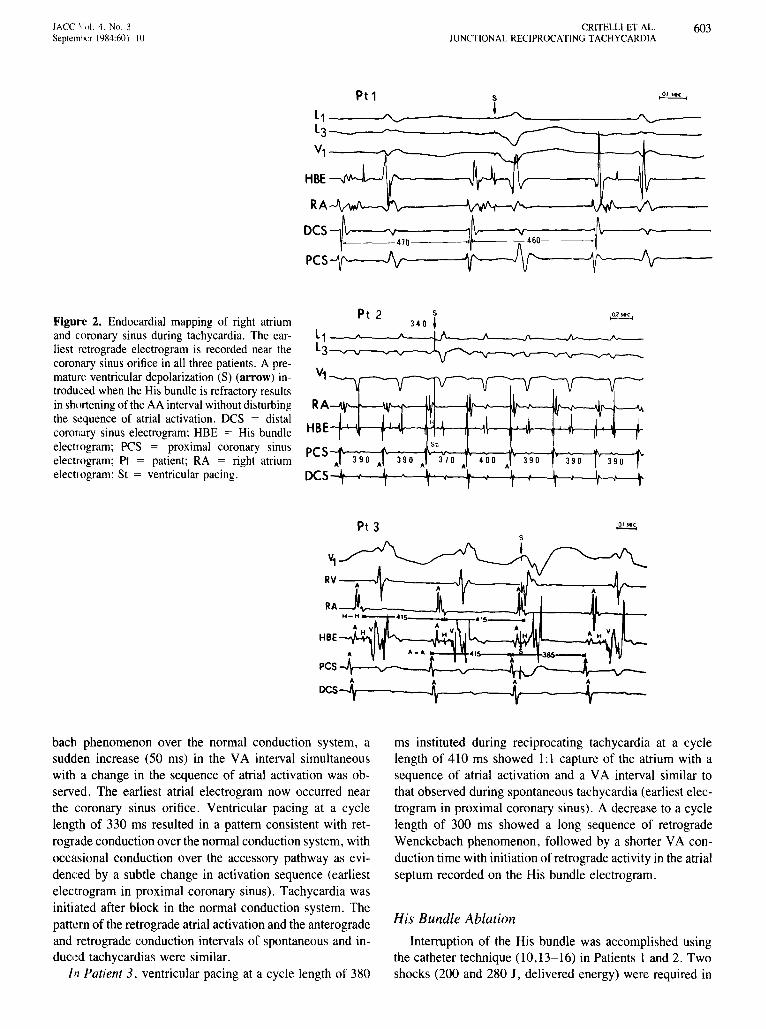
Electrophysiologic investigation was performed according to the technique described previously (11), Endocardialmapping of the right atrium and coronary sinus during tachycardia in all patients (Fig. 2) showed a septal sequence ofretrograde atrial activation, the earliest retrograde electrogram being recorded at the coronary sinus orifice. Prematureventricular stimulation introduced during tachycardia at thetime when the His bundle was refractory resulted in shortening of the atrial cycle length without disturbing the sequence of atrial activation. These observations suggestedthat an accessory pathway was present and that the lowerjunction of the reentrant circuit was in or below the distalHis bundle (12). Earlier programmed premature ventricularstimulation terminated tachycardia without conduction tothe atrium, further suggesting that the rhythm was indeedreciprocating. With resumption of sinus rhythm, the AHand HV intervals were normal.
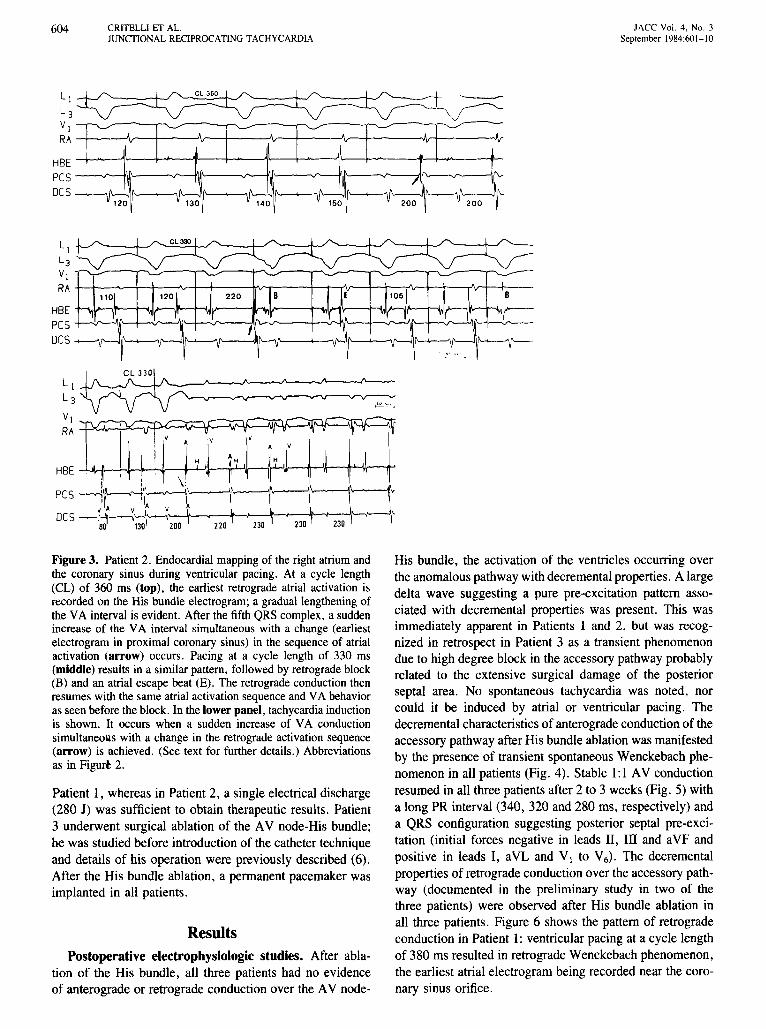
Analysis of retrograde conduction in two patients. InPatient 2 (Fig. 3), ventricular pacing at a cycle length of360 ms performed during sinus rhythm initially showed asequence of atrial activation (earliest activity was at the atrialseptum recorded by the His bundle catheter) consistent withretrograde conduction over the His bundle-A V node, withgradual lengthening of the ventriculoatrial (VA) intervalfrom 120 to 150 ms. At the end of the retrograde Wencke-
Pt 1
l3~ aVF..l-L.-.J....
162016201620,'6201620,I 600 1600 I
L3_."--.A.__k-,,J'-o..-_J-....,..-"................I'-_.Jo-..---"__~-.J.......;-........~..,,......-v"........."-
Pt 2
1600 I 600 I 600 I
V1~
l2~ l3~ aVF~
1620160015801
~
APB1620162016201 I
ilf-l'--'ifffi
CSMI
Pt 3
l2~ l3"'r"'rtv aVF~
1600156015201
JACC \',,1. 4. No.3Septemncr 1984:601-10
CRITELLIET AL.JUNCTIONAL RECIPROCATING TACHYCARDIA
603
Pt1 s ~
l1 ---""--"------,-'"'-~ ""_---l3-_-/'-'--- _
V1----V'-__--~
H8E --.r~I'v-J I ,'----"\11
390390400370
A~ •
S
340 I
390
Pt 2
l1 -~--,/'--_IJ''----J'--_.l'---.../'v'_~'''__l3---...--v--v~-~
V1
RA---w'-f'---IM'--ilIl---W--./'---ilf'-"'-~f--_\If'.+_---'t>.
H8E-Tl-1t----Ir+-J,\r---lH-\~f_'_n--4-'--'o\-_}_wJr_____l\...4_.Il____lr
Figure 2. Endocardial mapping of right atriumand coronary sinus during tachycardia. The earliest retrograde electrogram is recorded near thecoronary sinus orifice in all three patients. A premature ventricular depolarization (S) (arrow) introduced when the His bundle is refractory resultsin shortening of the AA interval without disturbingthe sequence of atrial activation. DCS = distalcoronary sinus electrogram; HBE = His bundleelectrogram; PCS = proximal coronary sinuselectrogram; Pt = patient; RA = right atriumelectrogram; St = ventricular pacing.
Aj~v
Pt 3
HBE
DCS-4---~~----t------I\.-----
bach phenomenon over the normal conduction system, asudden increase (50 ms) in the VA interval simultaneouswith a change in the sequence of atrial activation was observed. The earliest atrial electrogram now occurred nearthe coronary sinus orifice. Ventricular pacing at a cyclelength of 330 ms resulted in a pattern consistent with retrograde conduction over the normal conduction system, withoccasional conduction over the accessory pathway as evidenced by a subtle change in activation sequence (earliestelectrogram in proximal coronary sinus). Tachycardia wasinitiated after block in the normal conduction system. Thepattern of the retrograde atrial activation and the anterogradeand retrograde conduction intervals of spontaneous and induced tachycardias were similar.
In Patient 3, ventricular pacing at a cycle length of 380
ms instituted during reciprocating tachycardia at a cyclelength of 410 ms showed 1:1 capture of the atrium with asequence of atrial activation and a VA interval similar tothat observed during spontaneous tachycardia (earliest electrogram in proximal coronary sinus). A decrease to a cyclelength of 300 ms showed a long sequence of retrogradeWenckebach phenomenon, followed by a shorter VA conduction time with initiation of retrograde activity in the atrialseptum recorded on the His bundle electrogram.
His Bundle Ablation
Interruption of the His bundle was accomplished usingthe catheter technique (10,13-16) in Patients 1 and 2. Twoshocks (200 and 280 J, delivered energy) were required in
604
HBEpesDes
CRITELLI ET AL.JUNCTIONAL RECIPROCATING TACHYCARDIA
- i'---'" ~ '-' '--'
A -v
j,
iI t,
V 120 V 130 V 140 V 150 V 200 '~ V 200 .~
JACC Vol. 4, No.3September 1984:601-10
LjL
3
VI ••r--._':.---.,.-..,
RA +-+--'-'-+-+---"v-+-+----Irv...---_+__+-"T'Ir-_+__+----,JIr--+--+-----..Jv--+--_+__-
HBE +--<IJI.t-~-HJI.t--~____lrl..lv--......,IL.--j,JLr---_+.,w[,.....,IIr---l-\JI .....___,j~-H,JI .......__,II~Hpes -I--:.r----'j,''--+-.;.r..--'llY-:.r---!l{\.--.r----+-.-v'4\/\---l---.r-'-'lf'..-+--v-----'-'IHe-..:.r--
Des -<----.r~II'-'O""--4,...-III'--'--'lf'----1IlII'--~1'----+----'\f'-i1I'---<--'lr'--,IIf\--<.--_4I'-~\1'__~41'_-
Figure 3. Patient 2. Endocardial mapping of the right atriumandthe coronary sinus during ventricular pacing. At a cycle length(CL) of 360 ms (top), the earliest retrograde atrial activation isrecordedon the His bundle electrogram; a graduallengthening ofthe VA interval is evident. After the fifth QRS complex,a suddenincrease of the VA interval simultaneous with a change (earliestelectrogram in proximal coronary sinus) in the sequence of atrialactivation (arrow) occurs. Pacing at a cycle length of 330 ms(middle) results in a similarpattern, followed by retrograde block(8) and an atrial escape beat (E), The retrograde conduction thenresumeswith the same atrial activation sequence and VA behavioras seen beforethe block, In the lower panel, tachycardia inductionis shown. It occurs when a sudden increase of VA conductionsimultaneous with a change in the retrograde activation sequence(arrow) is achieved. (See text for further details.) Abbreviationsas in Figur. 2.
Patient 1, whereas in Patient 2, a single electrical discharge(280 J) was sufficient to obtain therapeutic results. Patient3 underwent surgical ablation of the AV node-His bundle;he was studied before introduction of the catheter techniqueand details of his operation were previously described (6).After the His bundle ablation, a permanent pacemaker wasimplanted in all patients.
ResultsPostoperative electrophysiologic studies. After abla
tion of the His bundle, all three patients had no evidenceof anterograde or retrograde conduction over the AV node-
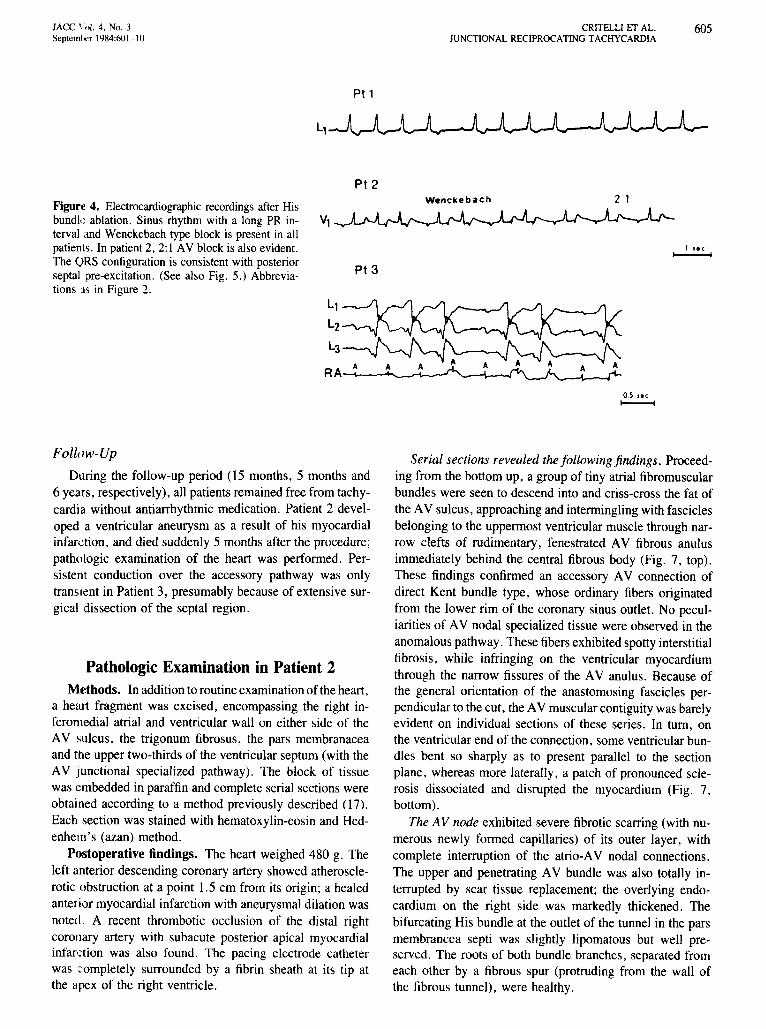
His bundle, the activation of the ventricles occurring overthe anomalous pathway with decremental properties. A largedelta wave suggesting a pure pre-excitation pattern associated with decremental properties was present. This wasimmediately apparent in Patients 1 and 2, but was recognized in retrospect in Patient 3 as a transient phenomenondue to high degree block in the accessory pathway probablyrelated to the extensive surgical damage of the posteriorseptal area. No spontaneous tachycardia was noted, norcould it be induced by atrial or ventricular pacing. Thedecremental characteristics of anterograde conduction of theaccessory pathway after His bundle ablation was manifestedby the presence of transient spontaneous Wenckebach phenomenon in all patients (Fig. 4). Stable 1:1 AV conductionresumed in all three patients after 2 to 3 weeks (Fig. 5) witha long PR interval (340, 320 and 280 ms, respectively) anda QRS configuration suggesting posterior septal pre-excitation (initial forces negative in leads II, III and aVF andpositive in leads I, aVL and V j to V6) . The decrementalproperties of retrograde conduction over the accessory pathway (documented in the preliminary study in two of thethree patients) were observed after His bundle ablation inall three patients. Figure 6 shows the pattern of retrogradeconduction in Patient 1: ventricular pacing at a cycle lengthof 380 ms resulted in retrograde Wenckebach phenomenon,the earliest atrial electrogram being recorded near the coronary sinus orifice.
lAC C \ ..1.4. No. 3Septerntvr 1984:601-10
Pt1
CRITELLI ET AL.JUNCTIONAL RECIPROCATING TACHYCARDIA
605
Pt2
Figure 4. Electrocardiographic recordings after Hisbundle ablation. Sinus rhythm with a long PR in- Vlterval and Wenckebach type block is present in allpatients . In patient 2, 2: I AV block is also evident.The ORS configuration is consistent with posteriorseptal pre-excitation . (See also Fig. 5.) Abbrevia-tions :IS in Figure 2.
Pt 3
Wenckebach
I se c~
Ll
L2
L3
RA_--,-~~ ......
05 lee-Follow-Up
During the follow-up period (15 months,S months and6 years, respectively), all patients remained free from tachycardia without antiarrhythmic medication. Patient 2 developed a ventricular aneurysm as a result of his myocardialinfarction , and died suddenl y 5 months after the procedure ;pathologic examination of the heart was performed. Persistent conduction over the accessory pathway was onlytransient in Patient 3, presumably because of extensive surgical dissection of the septal region .
Pathologic Examination in Patient 2Methods. In addition to routine examination of the heart ,
a heart fragment was excised, encompassing the right inferomedial atrial and ventricular wall on either side of theAV sulcus, the trigonum fibrosus, the pars membranac eaand the upper two-thirds of the ventricular septum (with theAV junctional specialized pathway). The block of tissuewas embedded in paraffin and complete serial sections wereobtained according to a method previously described (17).Each section was stained with hematoxylin-eosin and Hedenhein's (azan) method .
Postoperative findings. The heart weighed 480 g. Theleft anterior descending coronary artery showed atherosclerotic obstruction at a point 1.5 em from its origin; a healedanterior myocardial infarction with aneurysmal dilation wasnoted . A recent thrombotic occlusion of the distal rightCOrollary artery with subacute posterior apical myocardialinfarction was also found . The pacing electrode catheterwas completely surrounded by a fibrin sheath at its tip atthe apex of the right ventricle .
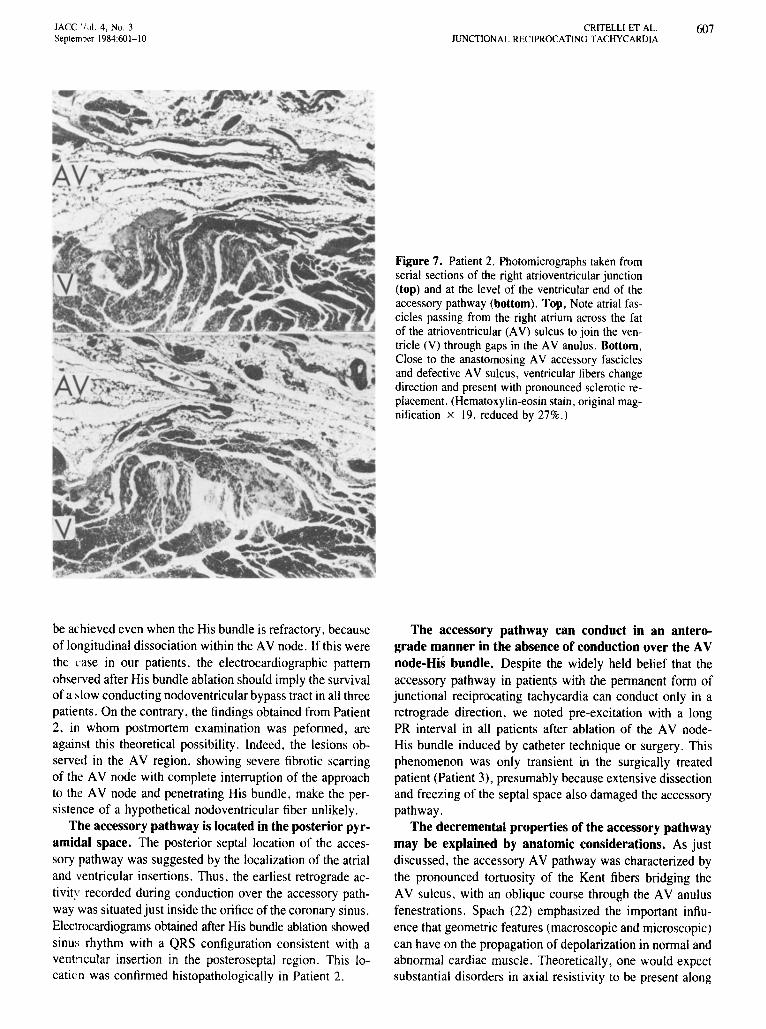
Serial sections revealed the follo wing findings. Proceeding from the bottom up, a group of tiny atrial fibromuscularbundle s were seen to descend into and criss-cross the fat ofthe AV sulcus, approaching and intermingling with fasciclesbelonging to the uppermost ventricular muscle through narrow clefts of rudimentary , fenestrated AV fibrous anulusimmediately behind the central fibrous body (Fig. 7, top).These findings confirmed an accessory AV connection ofdirect Kent bundle type , whose ordinary fibers originatedfrom the lower rim of the coronary sinus outlet. No peculiarities of AV nodal specialized tissue were observed in theanomalous pathway. These fibers exhibited spotty interstitialfibrosis, while infringing on the ventricular myocard iumthrough the narrow fissures of the AV anulus . Because ofthe general orientation of the anastomosing fascicles perpend icular to the cut, the AV muscular contiguity was barelyevident on individual sections of these series. In tum , onthe ventricular end of the connection , some ventricular bundles bent so sharply as to present parallel to the sectionplane, whereas more laterally, a patch of pronounced sclerosis dissociated and disrupted the myocardium (Fig. 7,bottom ).
The AV node exhibited severe fibrotic scarring (with numerous newly formed capillaries) of its outer layer, withcomplete interruption of the atrio-AV nodal connections.The upper and penetrating AV bundle was also totally interrupted by scar tissue replacement; the overlying endocardium on the right side was markedly thickened. Thebifurcating His bundle at the outlet of the tunnel in the parsmembrancea septi was slightly lipomatous but well preserved . The roots of both bundle branches, separated fromeach other by a fibrous spur (protruding from the wall ofthe fibrous tunnel), were healthy.
606 CRITELLI ET AL.JUNCTIONAL RECIPROCATING TACHYCARDI A
JACC Vol. 4 . No.3September 1984:601-10
Ll~ V,~ Ll~ Vl~L,A.AA... V,mV
L2~ V2JvJ)v L2~ V2rl-U L2'YYY'V
2W0JV3JrlJIyL31l1 ~Yff V3~ ~Yff V3/tM
aVR~ v.~LW aVR_V.~
aVR----- v.IVvV
J, Gl aVL~ Vs~aVLAJvl.
VSMJ"V5~aVL ..... .-..r---
aVF-V-yy V6~
aVF~aVFYff v6MA.
V6~
Pt 1 Pt 2 Pt 3
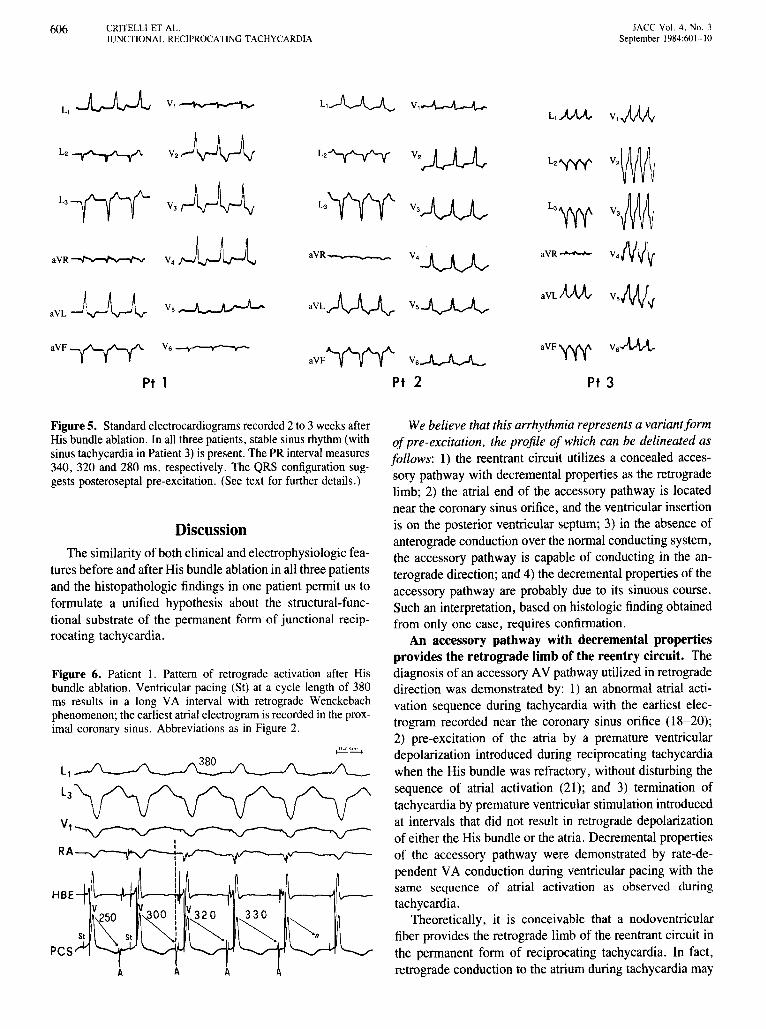
Figure 6. Patient 1. Pattern of retrograde activation after Hisbundle ablation. Ventricular pacing (St) at a cycle length of 380ms results in a long VA interval with retrograde Wenckebachphenomenon; the earliest atrialelectrogram is recorded in the proximal coronary sinus. Abbreviations as in Figure 2.
Figure 5. Standardelectrocardiograms recorded 2 to 3 weeks afterHis bundle ablation. In all three patients, stablesinus rhythm(withsinus tachycardiain Patient3) is present.The PR interval measures340, 320 and 280 rns, respectively. The QRS configuration suggests posteroscptal pre-excitation. (See text for further details.)
DiscussionThe similarity of both clinical and electrophysiologic fea
tures before and after His bundle ablation in all three patientsand the histopathologic findings in one patient permit us toformulate a unified hypothesis about the structural-functional substrate of the perm anent fonn of junctional reciprocating tachycardia.
We believe that this arrhythmia represents a variant formof pre -excitation. the profile of which can be delineated asfollows: 1) the reentrant circuit utilizes a concealed accessory pathway with decremental properties as the retrogradelimb; 2) the atrial end of the accessory pathway is locatednear the coronary sinus orifice , and the ventricular insertionis on the posterior ventricular septum; 3) in the absence ofanterograde conduction over the normal conducting system,the accessory pathway is capable of conducting in the anterograde direction; and 4) the decremental properties of theaccessory pathway are probably due to its sinuous course.Such an interpretation, based on histologic finding obtainedfrom only one case , requ ires confirmation .
An accessory pathway with decremental propertiesprovides the retrograde limb of the reentry circuit. Thediagnosis of an accessory AV pathway utilized in retrogradedirection was demonstrated by: 1) an abnormal atrial activation sequence during tachycardia with the earliest electrogram recorded near the coronary sinus orifice (18-20);2) pre-excitation of the atria by a premature ventriculardepolarization introduced during reciprocating tachycardiawhen the His bundle was refractory, without disturbing thesequence of atrial activation (21); and 3) termination oftachycardia by premature ventricular stimulation introducedat intervals that did not result in retrograde depolarizationof either the His bundle or the atria. Decremental propertiesof the accessory pathway were demonstrated by rate-dependent VA conduction during ventricular pacing with thesame sequence of atrial activation as observed duringtachycardia .
Theoretically, it is conceivable that a nodoventricularfiber provides the retrograde limb of the reentrant circuit inthe permanent form of reciprocating tachycardia. In fact,retrograde conduction to the atrium during tachycardia mayAAA
IACC 'IJI. 4. No.3Septemoer 1984:601-10
CRITELLI ET AL.JUNCTIONAL RECIPROCATING TACHYCARDIA
Figure 7, Patient 2. Photomicrographs taken fromserial sections of the right atrioventricular junction(top) and at the level of the ventricular endof theaccessory pathway (bottom). Top, Note atrial fascicles passing from the right atrium across the fatof the atrioventricular (AV) sulcus to join the ventricle (V) through gaps in the AV anulus. Bottom.Close to the anastomosing AV accessory fasciclesand defective AV sulcus, ventricular fibers changedirection andpresent with pronounced sclerotic replacement. (Hematoxylin-eosinstain, original magnification x 19, reduced by 27%.)
607
be achieved even when the His bundle is refractory, becauseoflongitudinal dissociation within the AV node. If this werethe case in our patients, the electrocardiographic patternobserved after His bundle ablation should imply the survivalof a slow conducting nodoventricularbypass tract in all threepatients. On the contrary, the findings obtained from Patient2, in whom postmortem examination was peformed, areagainst this theoretical possibility. Indeed, the lesions observed in the AV region, showing severe fibrotic scarringof the AV node with complete interruption of the approachto the AV node and penetrating His bundle, make the persistence of a hypothetical nodoventricular fiber unlikely.
The accessory pathway is located in the posterior pyramidal space. The posterior septal location of the accessory pathway was suggested by the localization of the atrialand ventricular insertions. Thus, the earliest retrograde activity recorded during conduction over the accessory pathway was situated just inside the orificeof the coronary sinus.Electrocardiograms obtained after His bundle ablation showedsinus rhythm with a QRS configuration consistent with aventricular insertion in the posteroseptal region. This location was confirmed histopathologically in Patient 2.
The accessory pathway can conduct in an anterograde manner in the absence of conduction over the AVnode-His bundle. Despite the widely held belief that theaccessory pathway in patients with the permanent form ofjunctional reciprocating tachycardia can conduct only in aretrograde direction, we noted pre-excitation with a longPR interval in all patients after ablation of the AV nodeHis bundle induced by catheter technique or surgery. Thisphenomenon was only transient in the surgically treatedpatient (Patient 3), presumably because extensive dissectionand freezing of the septal space also damaged the accessorypathway.
The decremental properties of the accessory pathwaymay be explained by anatomic considerations. As justdiscussed, the accessory AV pathway was characterized bythe pronounced tortuosity of the Kent fibers bridging theAV sulcus, with an oblique course through the AV anulusfenestrations. Spach (22) emphasized the important influence that geometric features (macroscopic and microscopic)can have on the propagation of depolarization in normal andabnormal cardiac muscle. Theoretically, one would expectsubstantial disorders in axial resistivity to be present along
608 CRITELLI ET AL.JUNCTIONAL RECIPROCATING TACHYCARDIA
JACC Vol. 4. No.3September 1984:601-10
the course of a fiber that pursued a sinuous, tortuous path.As a result of changing cross-sectional area, such a fibermight predictably exhibit slow conduction similar to thatobserved in the AV node. The structural and geometricasymmetry of the accessory pathway, as found in Patient2, may be critical to decremental conduction. Although thiscase is not representative of all patients with the permanentform of junctional reciprocating tachycardia, one can speculate that directional distortion and partial fibrotic thinningof the accessory pathway may have a significantbearing onimpairment in impulse propagation along the accessorypathway itself.
On the basis of our data, it appears reasonable to modifysome currently accepted concepts.
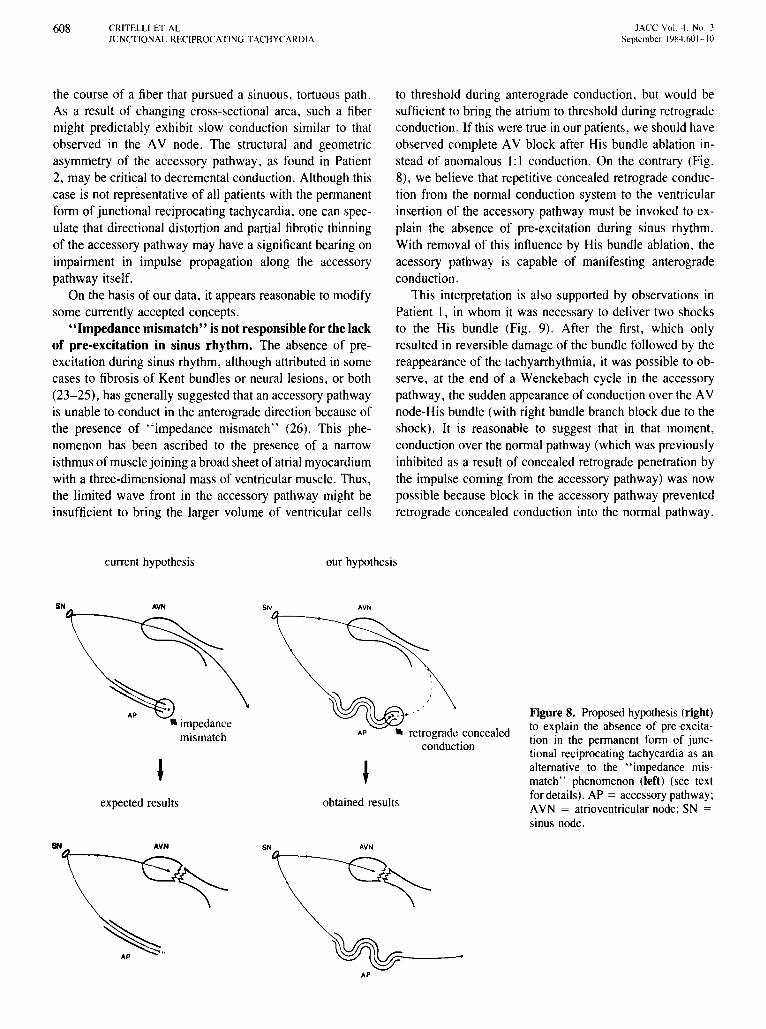
"Impedance mismatch" is not responsible for the lackof pre-excitation in sinus rhythm. The absence of preexcitation during sinus rhythm, although attributed in somecases to fibrosis of Kent bundles or neural lesions, or both(23-25), has generally suggested that an accessory pathwayis unable to conduct in the anterograde direction because ofthe presence of "impedance mismatch" (26). This phenomenon has been ascribed to the presence of a narrowisthmusof musclejoining a broad sheetof atrial myocardiumwith a three-dimensional mass of ventricular muscle. Thus,the limited wave front in the accessory pathway might beinsufficient to bring the larger volume of ventricular cells
to threshold during anterograde conduction, but would besufficient to bring the atrium to threshold during retrogradeconduction. If this were true in our patients, we should haveobserved complete AV block after His bundle ablation instead of anomalous I: I conduction. On the contrary (Fig.8), we believe that repetitive concealed retrograde conduction from the normal conduction system to the ventricularinsertion of the accessory pathway must be invoked to explain the absence of pre-excitation during sinus rhythm.With removal of this influence by His bundle ablation, theacessory pathway is capable of manifesting anterogradeconduction.
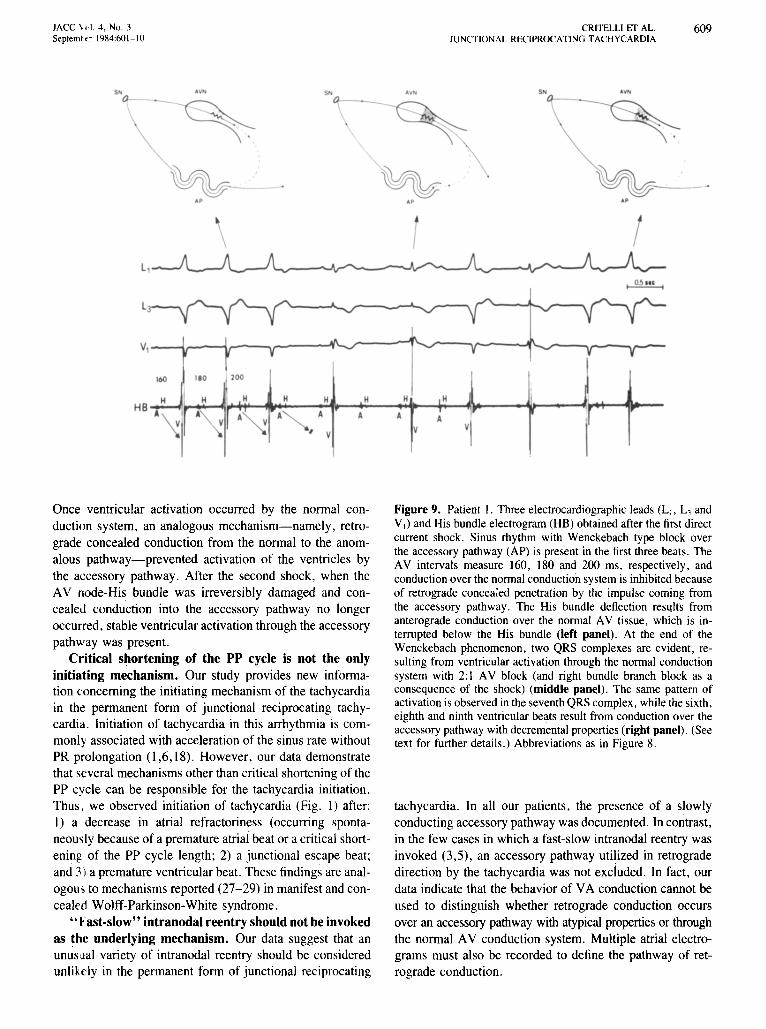
This interpretation is also supported by observations inPatient I, in whom it was necessary to deliver two shocksto the His bundle (Fig. 9). After the first, which onlyresulted in reversible damage of the bundle followed by thereappearance of the tachyarrhythmia, it was possible to observe, at the end of a Wenckebach cycle in the accessorypathway, the sudden appearance of conduction over the AVnode-His bundle (with right bundle branch block due to theshock). It is reasonable to suggest that in that moment,conduction over the normal pathway (which was previouslyinhibited as a result of concealed retrograde penetration bythe impulse coming from the accessory pathway) was nowpossible because block in the accessory pathway preventedretrograde concealed conduction into the normal pathway.
current hypothesis our hypothesis
AVN
obtained results
Figure8. Proposed hypothesis (right)to explain the absence of pre-excitation in the permanent form of junctional reciprocating tachycardia as analternative to the "impedance mismatch" phenomenon (left) (see textfor details). AP = accessory pathway;AVN = atrioventricular node; SN =sinus node.
AP ... retrograde concealedconduction
SN
"impedancemismatch
expected results
SN AVN SN AVN
~---AP
JACC \ d. 4, No.3September 1984:601-10
CRITELLI ET AL.JUNCTIONAL RECIPROCATING TACHYCARDIA
609
....
~-••
5..
H
Av
AV'
H
A
~.A'
H
A
500--_
S. AV'
0 - -
~
~A'
t.
\L,
L)
V,
HB
Once ventricular activation occurred by the normal conduction system, an analogous mechanism-namely, retrograde concealed conduction from the normal to the anomalous pathway-prevented activation of the ventricles bythe accessory pathway. After the second shock, when theAV node-His bundle was irreversibly damaged and concealed conduction into the accessory pathway no longeroccurred, stable ventricular activation through the accessorypathway was present.
Critical shortening of the PP cycle is not the onlyinitiating mechanism. Our study provides new information concerning the initiating mechanism of the tachycardiain the permanent form of junctional reciprocating tachycardia. Initiation of tachycardia in this arrhythmia is commonly associated with acceleration of the sinus rate withoutPR prolongation (1,6,18). However, our data demonstratethat several mechanisms other than critical shortening of thePP cycle can be responsible for the tachycardia initiation.Thus, we observed initiation of tachycardia (Fig. 1) after:1) a decrease in atrial refractoriness (occurring spontaneously because of a premature atrial beat or a critical shortening of the PP cycle length; 2) a junctional escape beat;and 3) a premature ventricular beat. These findings are analOgOU5 to mechanisms reported (27-29) in manifest and concealed Wolff-Parkinson-White syndrome.
"Fast-slow" intranodal reentry should not be invokedas the underlying mechanism. Our data suggest that anunusual variety of intranodal reentry should be consideredunlikely in the permanent form of junctional reciprocating
Figure 9. Patient 1. Three electrocardiographic leads (LI. L) andVI) and His bundle electrogram (HB) obtained after the first directcurrent shock. Sinus rhythm with Wenckebach type block overthe accessory pathway (AP) is present in the first three beats. TheAV intervals measure 160, 180 and 200 ms, respectively, andconduction over the normal conduction system is inhibited becauseof retrograde concealed penetration by the impulse coming fromthe accessory pathway. The His bundle deflection reslilts fromanterograde conduction over the normal AV tissue, which is interrupted below the His bundle (left panel). At the end of theWenckebach phenomenon, two QRS complexes are evident, resulting from ventricular activation through the nonnal conductionsystem with 2:1 AV block (and right bundle branch block as aconsequence of the shock) (middle panel), The same pattern ofactivation is observed in the seventh QRS complex, while the sixth,eighth and ninth ventricular beats result from conduction over theaccessory pathway with decremental properties (right panel). (Seetext for further details.) Abbreviations as in Figure 8.
tachycardia. In all our patients, the presence of a slowlyconducting accessory pathway was documented. In contrast,in the few cases in which a fast-slow intranodal reentry wasinvoked (3,5), an accessory pathway utilized in retrogradedirection by the tachycardia was not excluded. In fact, ourdata indicate that the behavior of VA conduction cannot beused to distinguish whether retrograde conduction occursover an accessory pathway with atypical propertiesor throughthe normal AV conduction system. Multiple atrial electrograms must also be recorded to define the pathway of retrograde conduction.

610 CRITELLI ET AL.JUNCTIONAL RECIPROCATING TACHYCARDIA
lACC Vol. 4. No. }September 1984:60I-I 0
Therapeutic implications. The presence of an accessory pathway with decremental properties as the substrateof the permanent form of junctional reciprocating tachycardia provides two potential therapeutic possibilities: ablation of the normal or the accessory pathway. AV node-Hisbundle ablation can be accomplished by the closed chestcatheter technique, as was performed in two of our patients.Because of the latent capability of the accessory pathwayto conduct anterogradely, pacemaker dependence will notnecessarily occur. In addition, the decremental propertiesof the accessory pathway will prevent a rapid ventricularresponse in the event of atrial fibrillation. Alternatively,surgical dissection of the posterior septal accessory pathwayhas been reported (30) in cases of the permanent form ofjunctional reciprocating tachycardia, leaving the AV nodeHis bundle intact. This possibility has been realized onlyby open chest surgery to date, but the possible use of theclosed chest catheter technique to accomplish the same purpose seems feasible.
We are very grateful to Officine Toscane Elettromeccaniche Biomedica inFlorence, Italy for providing technical assistance in carrying oUlthis study.
ReferencesI. Coumel P, Cabrol C, Fabiato A, Gourgon R, Slama R. Tachycardie
permanente par rhythme reciproque. Arch Mal Coeur 1967;60:1830-64.
2. Brugada P, Bar FW, Vanagt EJ, Friedman PL. Wellens H11. Observations on patients showing AV junctional echoes with a shorter P-Rthan R-P interval. Distinction between intranodal reentry or reentryusing an accessory pathway with a long conduction time. Am J Cardiol1981;48:611-22.
3. Strasberg B. Swiryn S, Bauernfeind R, et al. Retrograde dual atrioventricular nodal pathways. Am J Cardiol 1981;48:639-46.
4. Gallagher 11. Smith WM. Kerr CR. German LD, Sterba R, SealyWe. Etiology of long R-P tachycardia in 33 cases of supraventriculartachycardia (abstr). Circulation 1981;64(suppl IV):IV-145.
5. Wu D. Denes P, Arnat-y-Leon F, Wyndham CRC, Dhingra R, RosenKM. An unusual variety of atrioventricular nodal reentry due to retrograde dual atrioventricular nodal pathways. Circulation 1977;56:50-9.
6. Gallagher 11, Sealy We. The permanent form of junctional reciprocating tachycardia. Further elucidation of the underlying mechanism.Eur J Cardiol 1978;8:413-30.
7. Gallagher 11, Sealy WC, Kasell 1, Klein GJ, Pritchett ELC, Davis D.The permanent form of junctional reciprocating tachycardia: evidencefor an accessory ventriculo-atrial pathway as the underlying substrate(abstr). PACE 1979;2:21.
8. Epstein ML, Stone FM, Benditt DG. Incessant atrial tachycardia inchildhood: association with rate-dependent conduction in accessoryatrioventricular pathway. Am 1 Cardiol 1979;44:498-504.
9. Brugada P, Vanagt El, Bar FW, Wellens H11. Incessant reciprocatingatrioventricular tachycardia. Factors playing a role in the mechanismof the arrhythmia. PACE 1980;3:670-7.
10. Critelli G. Perticone F. Coltorti F, Monda V. Gallagher 11. Antegradeslow bypass conduction after closed-chest ablation of the His bundlein permanent junctional reciprocating tachycardia. Circulation1983;67:687-92.
II. Gallagher 11, Pritchett ELC, Sealy WC, Kasell J. Wallace AG. Thepreexcitation syndromes. Prog Cardiovasc Dis 1978;20:285-327.
12. Coumel P, Attuel P, Motte G, Slama R. Bouvrain Y. Les tachycardiesjonctionelles paroxystiques. Evaluation du point de jonction inferieurdu circuit de reentree. Demembrement des "rhythmes" reciproquesintra-nodaux. Arch Mal Coeur 1975;68:1255-77.
13. Gallagher 11. Svenson RH, Kasell J, et al. Catheter technique forclosed-chest ablation of the atrioventricular conduction system: a therapeutic alternative for the treatment of refractory supraventriculartachycardia. N Engl 1 Med 1982;306:194-200.
14. Gallagher 11, Svenson RH. Kasell 1, German LD. Bardy GH. Broughton A. Catheter technique for closed chest ablation of the atrioventricular conduction system in man (abstr), Am J Cardiol 1982;49:1012.
15. Scheinman M, Morady F, Hess D, Gonzales R. Catheter inducedablation of the atrioventricular junction to control refractory supraventricular arrhythmias. lAMA 1982;243:851-5.
16. Critelli G. Perticone F, Coltorti F, Monda V, Gallagher 11. Closedchest modification of the atrioventricular conduction system in manfor treatment of refractory supraventricular tachycardia. Br Heart 11983;49:544-9.
17. Rossi L, Thiene G. Arrhythmologic Pathology of Sudden CardiacDeath. Milan: Casa Editrice Ambrosiana, 1983:150.
18. Wellens H1J. Durrer D. Patterns ofventriculo-atrial conduction in theWolff-Parkinson-White syndrome. Circulation 1974;40;22-41.
19. Svenson RH, Miller RH. Gallagher 11, Wallace AG. Electrophysiologic evaluation of the Wolff-Parkinson-White syndrome. Problemsin assessing antegrade and retrograde conduction over the accessorypathway. Circulation 1975;52:552-62.
20. Arnat-y-Leon F, Dhingra RC. Wu D. Denes P, Wyndham C, RosenKM. Catheter mapping of retrograde atrial activation. Observationsduring ventricular pacing and AV nodal re-entrant paroxysmal tachycardia. Br Heart 1 1976;38;355-62.
21. Sellers TD, Gallagher 11, Cope GD, Tonkin AM, Wallace AG. Retrograde atrial preexcitation following premature ventricular beats during reciprocating tachycardia. Eur 1 Cardiol 1976;4:283-94.
22. Spach MS. The electrical representation of cardiac muscle based ondiscontinuities of atrial resistivity at a microscopic and macroscopiclevel. A basis for saltatory propagation in cardiac muscle. In: deCarvalho AP, Hoffman BF, Liebermann M, eds. Normal and Abnormal Conduction in the Heart. Biophysics, Physiology. Pharmacology and Ultrastructure. Mount Kisko, NY: Futura, 1982:145-53.
23. Klein GJ. Hackel DB. Gallagher 11. Anatomic substrate of impairedantegrade conduction over an accessory pathway in the Wolff-Parkinson-White syndrome. Circulation 1980;61:1249-56.
24. Prystowsky EN, Heger 11. lackman WM, Naccarelli GV, Zipes DP.Post-myocardial infarction incessant supraventricular tachycardia dueto concealed accessory pathway. Am Heart 1 1982;103:426--33.
25. Rossi L. The pathologic basis of cardiac arrhythmias. Cardiol Clin1983;1:13-37.
26. De La Fuente D. Sasyniuk B, Moe GK. Conduction through a narrowisthmus in isolated canine atrial tissue. A model of the WPW syndrome. Circulation 1971;44:803-9.
27. Coumel P, Fidelle J, Cloup M, Toumieux ML, Atteul P. Les tachycardies reciproques a evolution prolongee chez l'enfant, Arch MalCoeur 1974;67:23-44.
28. Krikler DM, Curry P, Attuel P, Coumel P. "Incessant" tachycardiasin Wolf-Parkinson-White syndrome. I: Initiation without antecedentextrastimulus or PR lengthening, with reference to reciprocation aftershortening of cycle length. Br Heart 1 1976;38:885-96.
29. Coumel P. Attuel P, Slama R, Curry P, Krikler DM. "Incessant"tachycardias in Wolff-Parkinson-White syndrome. II: Role of atypicalcycle length dependence and nodal-His escape beats in initiation ofreciprocating tachycardias. Br Heart 1 1976;38:897-906.
30. Gallagher lJ. German LD. Broughton A. Guarnieri T. Trantam JL.Variants of the preexcitation syndromes. In: Rosenbaum MB, ElizariMV, eds. Frontiers of Cardiac Electrophysiology. The Hague: Martinus Nijhoff, 1983:724-72.





























