Embed Size (px)
Citation preview

Support
Accepte
ReprintOrsola-M40138 B
0039-60
� 2014
http://d
512 S
Anatomic versus nonanatomicresection in cirrhotic patients withearly hepatocellular carcinomaAlessandro Cucchetti, MD,a Guo-Liang Qiao, MD,b Matteo Cescon, MD, PhD,a Jun Li, MD,b
Yong Xia, MD,b Giorgio Ercolani, MD,a Feng Shen, MD,b and Antonio Daniele Pinna, MD, PhD,a
Bologna, Italy, and Shanghai, China
Background. Whether anatomic resection (AR) for hepatocellular carcinoma (HCC) can really confer asurvival advantage over non-AR (NAR), especially for cirrhotic patients, remains unclear.Methods. Prospectively collected data of 543 cirrhotic patients in Child–Pugh class A submitted to AR(n = 228) versus NAR (n = 315) for early HCC in an Eastern (n = 269) and a Western (n = 274)surgical unit, were reviewed. To control for confounding variable distributions, a 1-to-1 propensity scorematch was applied to compare AR and NAR outcomes (n = 298).Results. The 5-year recurrence-free and overall survivals of the 543 patients were 32.3% and 60.0%,respectively, without differences between the 2 centers (P = .635 and .479, respectively). AR conferredbetter overall and recurrence-free survival than NAR (P = .009 and .041, respectively), but NAR pa-tients suffered from significantly worse hepatic dysfunction. After 1-to-1 match, AR (n = 149) and NAR(n = 149) patients had similar covariate distributions. In this matched sample, AR still conferred betterrecurrence-free survival over NAR (P = .044) but the beneficial effect of AR was limited to the reductionof early recurrence (<2 years) of poorly differentiated tumors and of tumors with microvascular invasion(P < .05), resulting in better overall survival (P = .018).Conclusion. In cirrhotic patients, AR for early HCC can lead to a lower early recurrence rate in tumorswith unfavorable tumor features, whereas NAR will not worsen the recurrence rate in well/moderatelydifferentiated tumors or in the absence of microvascular invasion. (Surgery 2014;155:512-21.)
From the Liver and Multiorgan Transplant Unit,a S. Orsola Hospital, Alma Mater Studiorum – University ofBologna, Bologna, Italy; and the Eastern Hepatobiliary Surgery Hospital,b Shanghai, China
HEPATOCELLULAR CARCINOMA (HCC) is 1 of the 5 mostcommon malignancies worldwide and the thirdmost common cause of cancer related mortality1;although more common in East Asia, the inci-dence of HCC is increasing in the Western world.2
Liver resection is widely accepted as a safe treat-ment with a low operative mortality as the resultof advances in surgical techniques and periopera-tive management.3,4 Unfortunately, the high inci-dence of recurrence remains the major challengein obtaining long-term results. Most recurrencesoccur in the liver as the consequence of subclinicalmetastases, originating from the primary tumor
ed in part by a grant from Regione Emilia Romagna.
d for publication October 8, 2013.
requests: Alessandro Cucchetti, MD, Policlinico Sant’alpighi, University of Bologna, Via Massarenti 9,ologna, Italy. E-mail: [email protected].
60/$ - see front matter
Mosby, Inc. All rights reserved.
x.doi.org/10.1016/j.surg.2013.10.009
URGERY
growth through microscopic vascular invasionand peripheral spread, and are considered themost important factors associated with poor prog-nosis.4-6 On this basis, the systematic removal of ahepatic segment, confined by tumor-bearing portaltributaries, namely anatomic resection (AR), wassuggested because it should be more effective foreradication of the intrahepatic metastases ofHCC. On the contrary, most surgeons prefer toleave a greater portion of parenchyma of this func-tional unit, such as in non-AR (NAR), focusing onthe preservation of a $1-cm tumor-free margin toreduce postoperative liver failure in patients withcirrhosis.
It remains unclear whether AR can reallyconfer a survival advantage over NAR. Someauthors have described better long-term outcomesafter AR compared with NAR, whereas others havenot been able to demonstrate these benefits, asoutlined by a recent meta-analysis.7 Discrepancieshave probably to be considered a consequence ofthe intrinsic relatively low level of evidence ofavailable literature represented by observational

SurgeryVolume 155, Number 3
Cucchetti et al 513
retrospective studies only. Meta-regression analysison this topic suggested that both overall survivaland disease-free survival after AR seem to be supe-rior to NAR because the worse liver functionreserve in the NAR group significantly affectsprognosis.7 In particular, comparative data avail-able from pertinent literature showed that pa-tients submitted to NAR were characterized by asignificantly higher prevalence of cirrhosis andmore advanced hepatic dysfunction comparedwith patients in the AR group, and that such dif-ferences are able to modify postoperative results.7
Although a randomized, controlled trial (RCT)comparing operative approaches would be ideal,a retrospective analysis using a propensity scorematching8 patients groups to reduce bias wasused herein to better determine the impact ofoperative approach on recurrence-free and overallsurvival for cirrhotic patient with HCC undergoingresection.
METHODS
Patient selection was accomplished through 3levels of inclusion criteria. First, all patients sub-mitted to portosystemic shunts before or at thesame time as hepatic resection, or treated as anemergency, or submitted to preoperative portalvein embolization were excluded from the analysis.Second, we considered eligible for the presentstudy only those patients in whom no evidence ofextrahepatic metastasis was present at the time ofsurgery, and at pathologic examination did notpresent tumor invasion into a major branch of theportal or hepatic veins, direct invasion of adjacentorgans, or spread to the lymph nodes of thehepatic hilum. In addition, we retained only thosecases in which a tumor-free margin of $1 cm wasconfirmed at pathologic examination; conse-quently, no tumor enucleations were included inthe present study and all resections considered inthe present analysis were curative resections athistology. Applying these criteria, betweenFebruary 2001 and August 2010, 508 cirrhoticpatients underwent a first curative resection atthe Eastern Hepatobiliary Surgery Hospital ofShanghai, and between January 1997 andNovember 2011, 388 cirrhotic patients underwentthe same procedure at the Department of Surgeryand Transplantation of the University of Bologna:The policies of the 2 centers regarding indicationsfor hepatic resection have been published else-where.4,9 Diagnosis of cirrhosis was confirmed onhistologic specimens. To reduce potential con-founding nomenclature of AR and NAR, a thirdlevel of inclusion criteria was adopted. Patients
with large tumors were excluded from the studythat was limited to patients with a single noduleof HCC #5 cm or no more than 3 nodules none>3 cm at histologic examination. In addition, thestudy was also limited to patients belonging toChild–Pugh class A. The final study populationthus consisted of 543 cirrhotic patients, in Child–Pugh class A, resected for early HCC: A total of269 patients came from the Eastern surgical centerand 274 from the Western surgical center.
All patients underwent intraoperative hepaticultrasonography and were deemed to have resect-able tumors at the time of surgery. AR was definedas the complete removal of $1 Couinaud segmentcontaining the tumor together with the relatedportal vein branch and the corresponding hepaticterritory. The appropriate segment margins wereidentified with the discoloration of the paren-chyma after ligation of the corresponding arterialand portal venous branches and with intraoper-ative ultrasonography assistance when necessary.NAR was defined as the resection of the tumorwith a margin of $1 cm without regard tosegmental, sectional, or lobar anatomy.
Pathologic and histologic evaluations of theresected specimens were carried out for all cases.The resected tumor, with its surrounding liver, wasexamined both microscopically and macroscopi-cally for its histopathologic features. The maximaldiameter of the tumor was taken as the tumor size.Curative resection was defined as complete macro-scopic and microscopic removal of the tumor.Tumor differentiation and microscopic vascularinvasion in the resected tumor were also deter-mined.10-12
After discharge, all patients were observedperiodically at follow-up to exclude possible recur-rence of HCC: Biochemical liver function tests,serum alpha-fetoprotein level measurement andultrasonography were performed 3 and 6 monthsafter discharge and then according to an annual orsemiannual surveillance program. When any recur-rence was suspected, a computed tomography ormagnetic resonance imaging was performed forconfirmation. Recurrent lesions were managedaggressively by a multimodal approach, whichincluded re-resection, transarterial chemoemboli-zation, percutaneous radiofrequency ablation, andpercutaneous ethanol injection. The treatment wasdecided by the pattern of recurrence, liver func-tional reserve, and the general condition of thepatient at the time of recurrence. For selectedpatients with transplantable recurrence, salvageliver transplantation was also adopted. Since theend of 2008, Sorafenib (Nexavar; Bayer,

SurgeryMarch 2014
514 Cucchetti et al
Leverkusen, Germany) therapy was also adopted,either alone or in combination with percutaneousapproaches for treatment of recurrence.13,14
Follow-up data were collected until December 31,2011. The study was approved by the appropriateinstitutional review committees and met the guide-lines of their responsible governmental agencies.
Statistical analysis. Categorical variables werereported as number of cases and prevalence, anddifferences between subgroups were comparedusing the Fisher exact test Chi-square analysis.Continuous variables were initially explored fortheir normal distribution using the Kolmogorov-Smirnov test. Because normal distribution couldnot be confirmed for most variables, all wereexpressed as median and range and differencesbetween subgroups were explored by the Mann-Whitney test. All analyses were 2-tailed. Overallsurvival was computed from the day of operationuntil the most recent follow-up or until patientdeath; recurrence-free survival was computed fromthe day of operation until the most recent follow-up visit or until clinical evidence of tumor recur-rence. Patients transplanted for postoperative liverfailure or tumor recurrence were censored on theday before transplantation. In particular, at theend of follow-up, in the whole study group of 543patients, salvage transplantation was performed in18 cases (3.3%; 11 of them underwent NAR).Survival estimates were obtained with the Kaplan-Meier method and compared using the log-ranktest.
To overcome biases owing to the differentdistribution of covariates among patients submit-ted to AR and those submitted to NAR, a 1-to-1match was created using propensity score analysis:The propensity score represents the probability ofeach individual patient being assigned to a partic-ular condition in a study given a set of knowncovariates.8 Propensity scores are used to reduceselection bias by equating groups on the basis ofthese covariates and are used to adjust for selectionbias in observational studies through matching. Amultivariate logistic regression was built to predictthe probability of each individual patient beingsubmitted to AR or NAR (predictive values) onthe basis of covariates that showed a different dis-tribution in the 2 groups and taking into accounthistologic variables that are known to be able toaffect postoperative survival or recurrence. Thepredictive values were then used to obtain a 1-to-1 match by using the nearest neighbor matchingmethod: Matching to 5 decimal points was initiallyperformed, followed by 4-, 3-, 2-, and 1-pointmatching, and cases whose propensity score
deviated >0.10 were considered unmatched.Thus, patients for whom the propensity score wasnot matchable were excluded from further anal-ysis. The Cox proportional hazard model wasfinally applied in the matched sample to identifyindependent predictors of tumor recurrence andoverall survival. Effect size was also calculated foreach covariate. Effect size is a measure that is inde-pendent of the sample size and can give a morerobust estimation of a difference in means or pro-portions: Values <j0.1j indicate very small differ-ences between means; values between j0.1j andj0.3j indicate small differences; values betweenj0.3j and j0.5j indicate moderate differences; andvalues >j0.5j indicate considerable differences.An effect size value of <j0.1j in propensity scoreanalyses means that the 2 groups are well matchedfor covariates.8,15 The statistical analysis was per-formed using SPSS Version 10.0 software for PCcomputer (SPSS, Inc, Chicago, IL).
RESULTS
Baseline characteristics of the whole study pop-ulation of 543 cirrhotic patients are reported inTable I: 228 patients were submitted to AR (42.0%)and 315 to NAR (58.0%). In the 228 patients sub-mitted to AR, a segmentectomy was performed in170 (74.6%), a bisegmentectomy in 46 (20.2%)and a trisegmentectomy or a major hepatectomyin 9 (4.0%). The 30- and 90-day postoperative mor-tality rates were 0.9% and 2.0%, respectively. Dur-ing a median follow-up of 38 months (range, 10days–12 years), 321 patients developed recurrence(59.1%) and 212 patients died (39.0%). In partic-ular, 171 patients died after tumor recurrence(31.5%). The 1-, 3-, and 5-year recurrence-free sur-vival rates were 79.6%, 52.5%, and 32.3%, respec-tively, and the corresponding overall survivalswere 93.4%, 74.3%, and 60.0%. Overall andrecurrence-free survivals did not significantly differbetween the 2 surgical units (P = .479 and .635,respectively); further details regarding clinicaland tumoral characteristics and outcome betweenthe 2 Centers can be found in SupplementaryTable I.
Comparison between AR and NAR patients. Ascan be observed in Table I, AR and NAR patients,of the whole study population, significantly differwith regard to clinical covariates. In particular,AR were more frequently performed in the Easternsurgical center (P = .009), and, as a consequence,hepatitis B surface antigen positivity was morefrequent in these patients (P = .019), whereas hep-atitis C virus positivity was more frequent in theNAR patients (P = .025). Even if all patients

Table I. Baseline characteristics of the cirrhotic patients, belonging to Child–Pugh class A, submitted tosurgery for early hepatocellular carcinoma in relationship with anatomic resection (AR) and nonanatomicresection (NAR)
Variable All patients (n = 543) AR (n = 228) NAR (n = 315) P value Effect size
Eastern Surgical Centre 269 (49.5%) 128 (56.1%) 141 (44.8%) .009 0.226Western Surgical Centre 274 (50.5%) 100 (43.9%) 174 (55.2%) — —Age (y) 58 (48–66) 57 (48–65) 59 (49–67) .115 0.134Male gender 449 (82.7%) 192 (84.2%) 257 (81.6%) .491 0.059HCV positive serology 204 (37.6%) 73 (32.0%) 131 (41.6%) .025 0.193HBsAg positive serology 291 (53.6%) 136 (59.6%) 155 (49.2%) .019 0.202Serum albumin (g/dL) 4.0 (3.6–4.3) 4.1 (3.7–4.3) 3.9 (3.5–4.2) .035 0.182Platelet count (3103/mm3) 118 (86–162) 120 (87–167) 115 (84–149) .179 0.163Serum bilirubin (mg/dL) 0.85 (0.64–1.16) 0.84 (0.64–1.12) 0.85 (0.64–1.18) .521 0.078ALT (IU) 53 (33–84) 55 (34–85) 53 (33–84) .983 0.009INR 1.07 (0.98–1.16) 1.05 (0.90–1.13) 1.09 (1.00–1.17) .001 0.298MELD score 8 (7–9) 7 (7–8) 8 (7–9) .001 0.283Histologic solitary tumor 501 (92.3%) 216 (94.7%) 285 (90.5%) .074 0.154Histologic size of largest tumor (cm) 3.0 (2.0–4.0) 3.0 (2.0–4.0) 3.0 (2.0–4.0) .409 0.070Histologic tumor size <2 cm 104 (19.2%) 48 (21.1%) 56 (17.8%) .377 0.076Histologic tumor size >3 cm 230 (42.4%) 105 (46.1%) 125 (39.7%) .159 0.121Tumor grading G3–G4 366 (67.4%) 149 (65.4%) 217 (68.9%) .405 0.072Presence of MVI 310 (57.1%) 124 (54.4%) 186 (59.0%) .293 0.090
Continuous variables are reported as median values and interquartile ranges (25th and 75th percentiles) because normal distribution cannot beconfirmed for most variables. Comparisons were performed with Mann-Whitney U test for continuous variables and Fisher exact test for categorical vari-ables. For continuous variables, the effect size was measured after log10 transformation. The following variables, significantly different between the 2groups and/or known to be able to affect postoperative survival or recurrence, were selected for propensity score calculation: Age, HCV serology, HBsAgserology, albumin, MELD score (INR was not included because it was already present in the MELD formula), solitary tumor, tumor size, tumor gradingand MVI.ALT, Alanine aminotransferase; HBsAg, hepatitis B surface antigen; HCV, hepatitis C virus; INR, International Normalized Ratio; MELD, Model forEnd-Stage Liver Disease; MVI, microvascular invasion.
SurgeryVolume 155, Number 3
Cucchetti et al 515
belonged to Child–Pugh class A, NAR patientsshowed lower serum albumin levels (P = .035),higher International Normalized Ratio values(P = .001), and worse Model for End-stage LiverDisease scores (P = .001) than AR patients. Histo-logic characteristics were similar. The 1-, 3-, and5-year recurrence-free rates were 83.4%, 57.0%,and 37.2%, respectively, after AR, and 76.8%,49.2%, and 28.4%, respectively, after NAR (P =.041). The 1-, 3-, and 5-year overall survival rateswere 93.7%, 82.2%, and 65.1%, respectively, afterAR, and 93.1%, 68.4%, and 56.1%, respectively,after NAR (P = .009).
Analysis of the matched sample. After the 1-to-1propensity score match, 298 patients were selectedfor comparison: 149 were submitted to AR and anequal number to NAR; details regarding propen-sity score calculation can be found inSupplementary Table II. As can be observed inTable II, clinical and histologic variables had verysimilar distributions as confirmed by the effectsize of <0.1 in all cases. In this matched sample,the 30- and 90-day postoperative mortality rateswere 0.3% and 1.3%, respectively. The 1-, 3-, and5-year recurrence-free survivals were 78.5%,
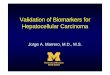
52.9%, and 34.6%, respectively, and the corre-sponding overall survivals were 93.1%, 74.9% and59.2% (Fig 1). As can be noted, recurrence-freesurvival changed its slope from the second year on-ward. In particular, the annual incidence rate ofrecurrence within 2 years of surgery (early recur-rence) was 24.0% (95% confidence interval[CI],19.5–28.6) and the annual incidence of recur-rence 2 years after surgery (late recurrence) was19.6% (95% CI, 15.0–24.1).
In this matched sample, patients submitted toAR still showed an overall better recurrence-freesurvival than NAR patients (P = .044). Results fromthe Cox regression are reported in Table III andshowed that when tumor recurrence was stratifiedinto early and late recurrence, the type of surgerysignificantly affected early recurrence (P = .015)together with tumor diameter (P = .016) and tu-mor grading (P = .006), but late recurrence wasnot significantly affected by AR (ExpB = 1.032;95% CI, 0.644–1.652; P = .896) or the other avail-able variables (full data not reported). Thesedata were confirmed when patients were stratifiedon the basis of tumor invasiveness to further inves-tigate how type of surgery could influence early

Table II. Baseline characteristics of the matched cohort in relationship with anatomic resection (AR) andnonanatomic resection (NAR)
Variable All patients (n = 298) AR (n = 149) NAR (n = 149) P value Effect size
Age, y (range) 56 (48–66) 57 (48–66) 56 (47–66) .507 0.034Male gender 245 (82.2%) 124 (83.2%) 121 (81.3%) .560 0.076HCV-positive serology 107 (35.9%) 54 (36.2%) 53 (35.6%) .860 0.016HBsAg-positive serology 169 (56.7%) 84 (56.4%) 85 (57.0%) .868 0.015Serum albumin (g/dL) 4.0 (3.6–4.3) 4.0 (3.7–4.3) 4.0 (3.6–4.4) .784 0.041Platelet count (3103/mm3) 124 (91–165) 124 (91–160) 124 (93–169) .892 0.074Serum bilirubin, mg/dL (range) 0.84 (0.63–1.12) 0.84 (0.64–1.11) 0.82 (0.62–1.15) .909 0.022ALT, IU/L (range) 55 (35–85) 58 (36–89) 54 (34–81) .399 0.078INR 1.07 (0.97–1.14) 1.06 (0.97–1.14) 1.07 (0.97–1.15) .996 0.033MELD score 8 (7–9) 8 (7–9) 8 (7–8) .702 0.011Histologic solitary tumor 286 (96.0%) 143 (96.0%) 143 (96.0%) 1.000 0.000Histologic size of largest tumor (cm) 3.0 (2.0–4.1) 3.0 (2.0–4.0) 3.0 (2.0–4.1) .870 0.085Tumor grading G3–G4 196 (65.8%) 98 (65.8%) 98 (65.8%) 1.000 0.000Presence of MVI 153 (51.3%) 77 (51.7%) 76 (51.0%) .903 0.015
Continuous variables are reported as median values and interquartile range (25th and 75th percentiles). Comparisons were performed with Wilcoxonsigned-rank test for continuous variables and McNemar for categorical variables. For continuous variables, effect size was measured after log10 transfor-mation. Effect size < 0.1 indicates very small differences.ALT, Alanine aminotransferase; HBsAg, hepatitis B surface antigen; HCV, hepatitis C virus; INR, International Normalized Ratio; MELD, Model forEnd-Stage Liver Disease; MVI, microvascular invasion.
Fig 1. Overall (upper plot) and recurrence-free (lowerplot) survivals of the matched cohort of 298 cirrhotic pa-tients. Recurrence-free survival changes its slope fromyear 2 after surgery onward, dividing early from late re-currences. Linear interpolation for early recurrence:Constant = 0.977; b1 = �0.016; r2 = 0.984. For late recur-rence: constant = 0.801; b1 = �0.008; r2 = 0.988.
SurgeryMarch 2014
516 Cucchetti et al
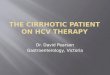
and late recurrence. As can be noted from Figure 2and Table IV, AR lost its prognostic significance inimproving the recurrence-free survival in G1–G2tumors and in the absence of microvascular inva-sion (MVI). In these 2 categories neither the over-all recurrence rate nor the early recurrence ratewere affected by the type of operative procedure(P > .05 in all cases). The benefit obtainable with
AR was narrowed to G3–G4 tumors and in tumorswith MVI: In these 2 categories, AR provided betterearly recurrence rates (P = .003 and .017, respec-tively) even if late recurrence rates remained sub-stantially unaffected (P > .05 in both cases).Similar findings were observed for tumor size(Fig 2 and Table IV). The 1-, 3-, and 5-year patientsurvivals after AR were 93.1%, 83.3%, and 65.8%,respectively, and after NAR were 93.1%, 66.8%,and 52.9% (P = .018). In particular, the overall sur-vival was similar, between AR and NAR patients, inG1–G2 tumors (P = .388), in tumors without MVI(P = .197) and in tumors <2 cm (P = .113), whereasAR was related to better overall survival in G3–G4tumors (P = .014); when MVI was present (P =.016) and in tumor sized $2 cm (P = .043).
Cox regression results on overall survival areprovided in Supplementary Table III. Regardingdata from the 245 patients excluded from thematch, 79 patients were submitted to AR and 166to NAR. Patients submitted to AR had a medianModel for End-stage Liver Disease score of 7(range, 6–8) and a tumor diameter of 3.3 (range,2.0–4.0) whereas those submitted to NAR had amedian Model for End-stage Liver Disease of 8(range, 7–10) and a tumor diameter of 2.8 (range,2.0–3.7; P = .001 and .041, respectively), confirm-ing that outliers were excluded from the match.
DISCUSSION
Surgery is the most important therapeuticapproach for patients with HCC, offering a

Table III. Uni- and multivariate Cox regression model on early recurrence-free survival in the matchedcohort of 298 cirrhotic patients
Variable
Univariate regression model Multivariate regression model
Exp(B) 95% CI P Exp(B) 95% CI P
Western (vs Eastern) Surgical Centre 1.013 0.689–1.490 .949 - - -Non-anatomic resection (vs Anatomic) 1.629 1.104–2.405 .014 1.625 1.100–2.401 .015Age (per year increase) 0.992 0.975–1.008 .311 - - -Male (vs female) 0.876 0.539–1.426 .595 - - -HCV positive (vs negative) 0.900 0.600–1.350 .611 - - -HBsAg positive (vs negative) 1.396 0.939–2.077 .103 - - -Serum albumin (per g/dL increase) 1.078 0.754–1.541 .681 - - -Platelet count (3103/mm3 increase) 1.001 0.996–1.003 .785 - - -Serum bilirubin (per mg/dL increase) 1.951 0.898–3.203 .218 - - -ALT (per IU/L increase) 0.997 0.993–1.002 .214 - - -INR (per unit increase) 0.961 0.236–3.916 .995 - - -Solitary tumor (vs multiple) 0.515 0.225–1.175 .115 - - -Size of largest tumor (per cm increase) 1.253 1.063–1.478 .007 1.229 1.040–1.451 .016Tumor grading G3–G4 (vs G1–G2) 1.875 1.197–2.936 .005 1.889 1.205–2.961 .006Presence of MVI (vs absent) 1.291 0.880–1.895 .092 1.142 0.826–1.577 .422
The annual incidence rate of early recurrence (<2 years from surgery) was 24.0% (95% CI, 19.5–28.6). P < .10 at univariate Cox regression were enteredin the multivariate backward proportional hazard model.ALT, Alanine aminotransferase; HBsAg, hepatitis B surface antigen; HCV, hepatitis C virus; INR, International Normalized Ratio; MELD, Model forEnd-Stage Liver Disease; MVI, microvascular invasion.
SurgeryVolume 155, Number 3
Cucchetti et al 517
possibility of cure. Unfortunately, the long-termprognosis remains undermined by the high recur-rence rate that is among the most importantfactors affecting the survival of HCC patients.4-6
The main problem that surgeons have to facewhile operating on cirrhotic patients is the balancebetween achieving a radical intervention and, atthe same time, preventing the development ofpostoperative liver failure that could ensue fromremoval of too much liver parenchyma. This prob-lem is at the basis of the dispute between AR, thatshould be theoretically more radical from an onco-logic point of view, and NAR, which should reducethe risk of postoperative hepatic failure. In theabsence of RCTs, results reported in the literatureare still conflicting.7 In particular, different pro-portions of cirrhotic patients, analyzed togetherwith noncirrhotic patients in previous studies,bias the differences observed between AR andNAR outcomes, because AR was mostly performedin noncirrhotic subjects that already have a favor-able clinical outcome. The present study showsthat even when restrictive criteria were applied toidentify a homogeneous study population, namelycirrhotic patients only, belonging to Child–Pughclass A, differences between patients submitted toAR or NAR still exist, because patients submittedto NAR still show more advanced hepatic dysfunc-tion. Thus, the present initial analysis required anin-depth evaluation of outcomes related to the 2different operative procedures, in which the
potential confounding impact of covariates, typicalof previous observational studies, was appropri-ately dealt with by means of a meticulous statisticalapproach.
When patients were adequately matchedthrough propensity score, the results from thepresent study show that AR might be consideredthe preferred operative procedure for early HCCbecause of the lower recurrence rate and, conse-quently, greater patient survival. Nevertheless, thistype of resection did not determine an absoluteadvantage compared with NAR because the benefitseems to be limited to the reduction of earlyrecurrences and depends on tumor features. Earlyrecurrences are defined as subclinical metastasesoriginating from the primary tumor and missedduring staging and treatment; thus, the presentfinding that AR could reduce such an inauspiciousevent well supports its oncologic rationale. How-ever, there is a peculiar finding of the presentanalysis that deserves particular attention. ARproved superior to NAR, in determining earlyrecurrence-free survival, only in early HCC withunfavorable tumor features such as poorly orundifferentiated grade or in the presence ofmicroscopic vascular invasion. In other words,the present results suggest that the higher theinvasiveness of the tumor, the greater the need forthe removal of the entire liver functional unit. Thisis an important aspect that acquires particularclinical interest since tumor grade can be assessed

Fig 2. Recurrence-free survival in relationship with type of surgery and histologic findings. Number of patients at risk,and distinction between early and late recurrence, are reported in Table IV. (A) G1–G2 tumor. (B) G3–G4 tumor. (C)Microscopic vascular invasion absent. (D) Microscopic vascular invasion present. (E) Tumor size <2 cm. (F) Tumor size$2 cm.
SurgeryMarch 2014
518 Cucchetti et al

Table IV. Overall, early, and late recurrence-free survival in relationship with anatomic resection (AR),nonanatomic resection (NAR), and tumor histologic features in the matched population of 298 patients
Survival (y) At risk AR, % (95% CI) At risk NAR, % (95% CI) P value
All patients (n = 298) 149 149 .0441 113 84.5 (77.4–89.5) 105 72.7 (64.7–79.3)2 79 68.7 (59.9–75.8) 72 55.3 (46.7–63.0) .0133 61 57.7 (48.4–65.9) 49 48.2 (39.5–56.4)5 25 37.2 (27.6–46.7) 20 32.2 (23.2–41.5) .896
G1–G2 tumors (n = 102) 51 51 .6271 36 81.6 (67.5–90.0) 42 83.9 (70.4–91.6)2 29 74.5 (64.0–82.3) 33 73.4 (58.6–83.6) .9743 25 69.1 (53.2–80.6) 25 68.5 (53.0–79.7)5 11 45.5 (34.0–56.3) 11 46.1 (29.1–61.6) .527
G3–G4 tumors (n = 196) 98 98 .0201 77 86.1 (77.3–91.7) 63 65.9 (55.5 –74.4)2 51 65.7 (49.9–77.6) 39 45.8 (35.4–55.6) .0033 35 50.3 (33.5–64.9) 26 37.6 (27.4–47.7)5 18 33.5 (22.6–44.8) 11 25.2 (15.3–36.3) .845
MVI absent (n = 145) 72 73 .1781 56 82.7 (71.6–89.8) 56 81.9 (70.8–89.1)2 40 67.9 (55.0–77.9) 42 65.8 (53.4–75.6) .2753 31 58.3 (44.7–69.6) 29 55.4 (42.5–66.5)5 11 38.5 (23.9–52.9) 10 35.2 (21.8–48.9) .427
MVI present (n = 153) 77 76 .1201 60 84.8 (74.2–91.3) 49 65.4 (53.5–75.0)2 40 64.7 (51.7–74.3) 33 51.4 (38.3–62.9) .0173 30 55.2 (42.0–66.5) 22 41.3 (29.5–52.6)5 12 32.2 (20.7–43.8) 13 31.9 (20.3–44.1) .586
Size <2 cm (n = 56) 32 24 .2701 28 90.2 (72.5–96.7) 18 78.3 (55.4–90.3)2 21 72.0 (51.5–84.9) 13 64.9 (41.9–80.7) .2833 15 68.0 (47.2–82.0) 6 56.8 (31.7–75.7)5 3 55.8 (32.7–73.7) 2 47.3 (21.6–69.4) .733
Size $2 cm (n = 242) 117 125 .2581 85 81.9 (73.3–87.9) 87 71.7 (62.9–78.8)2 58 66.4 (56.4–74.7) 58 53.5 (44.2–62.0) .0343 45 53.5 (42.9–63.0) 43 48.6 (39.2–57.3)5 19 34.2 (24.3–44.4) 17 31.2 (21.8–31.0) .296
For each subgroup, P values are reported for the entire time interval, for early recurrence (<2 years) and for late recurrence assuming 2 years as thestarting point. To obtain late recurrence-free survival (RFS) rates from actuarial data, survival can be calculated as follows: 3-year late RFS = 5-yearRFS/2-year RFS.CI, Confidence interval; MVI, microvascular invasion.
SurgeryVolume 155, Number 3
Cucchetti et al 519
preoperatively with reasonable accuracy.16-23 Tu-mor grade can be evaluated before surgery with tu-mor biopsy17,18 and there is recent evidence thatdiffusion-weighted magnetic resonance imagingcan identify degrees of tumor differentiation.21-23
In the presence of a preoperative diagnosis ofpoor differentiation, 1 suggestion could be tostudy candidates for hepatic resection to plan anAR. On the other hand, in patients without thesefeatures, a NAR could be performed withoutaffecting recurrence-free survival. This latter aspectis of particular importance in those patients inwhom the future remnant liver volume will beinadequate if an AR will be pursued. These
considerations must be made with caution,because the risks of a liver biopsy can overshadowpotential benefits. In particular, the risk of seedingis reported to range around 2–3%, when not asso-ciated with percutaneous therapies, but some Au-thors reported seeding #10%.24 It is clear thatliver biopsy cannot be suggested as a routine pre-operative tool. In addition, data on the accuracyof modern imaging techniques in predicting tu-mor differentiation are still scarce. Consequently,preoperative information regarding tumor inva-siveness should probably still be based on tumorsize. In the present study, and in the largest pub-lished experience from Eguchi et al,25 the benefit

SurgeryMarch 2014
520 Cucchetti et al
from AR over NAR, in terms of recurrence-freeand disease-free survivals, was not observed inHCC <2 cm. Thus, it can be suggested that whenan anatomic approach cannot be pursued owingto inadequate remnant liver volume, NAR forsmall HCCs will not affect tumor recurrence.That is because tumor size is known to be strictlyrelated to tumor differentiation and presence ofMVI.16,19,20
We are aware that the present study is not anRCT, and the present statistical approach is notaimed at replacing one; however, we believe thatthese results acquire particular strength for 3 mainreasons. First, matched patients had similar, oreven identical, clinical and tumor features knownto influence prognosis, the match was achievedwith a statistical approach and not made a priorion the basis of preselected covariates. Thisapproach excluded outlier patients that are moreprone to develop postoperative liver failure or,conversely, bring a null risk for postoperativecomplications. In these patients, the uncertaintyof the best operative approach is absent, inparticular for patients at high risk for postopera-tive liver failure, where NAR will be the onlyapproach that can be attempted. Second, theoperative procedures were not selected by apredetermined algorithm, but were left to thesurgeon’s choice because the superiority of oneor the other type of resection was unclear at thetime of the study. This aspect could apparentlyrepresent a possible bias right at the start, and itshould be observed that other features may haveaffected the operative choice, such as the attemptto obtain greater tumor-free margins, presence ofcomorbidities, or transplant eligibility. However,the proportion of patients that were suitable formatching was quite large (298/543), suggestingthat surgeons preferred AR or NAR approachindependent of clinical circumstances and tumorcharacteristics, providing comparable cases to beanalyzed. This second aspect is further highlightedby the fact that the study population derived from2 surgical centers that provide a good representa-tion of both Eastern and Western HCC epidemi-ology and surgical perspectives. Third, to the bestof our knowledge, this is the largest and most well-defined study conducted on exclusively cirrhoticpatients; in fact, most of previous literature resultsderived from mixed cohorts of cirrhotic and non-cirrhotic patients.7 This feature assumes particularimportance because cirrhosis represents the prin-cipal clinical impasse in the selection of the opera-tive procedure to adopt. Nevertheless, an RCTconducted to clarify the debate is warranted, but
unfortunately, to the best of our knowledge, only1 RCT has been designed and at present is notyet open for participant recruitment.26
In conclusion, the present analysis suggests thatanatomic resection of early HCC can reduce theearly recurrence-rate after hepatic resection, andthis is true for patients having poorly differentiatedHCC orMVI. Nevertheless, AR cannot be applied toall patients with cirrhosis because of the risk ofpostoperative insufficiency; in this regard, NAR canprovide similar results to that of AR in the absenceof unfavorable tumor features or for small tumors.
A. Cucchetti and G-L. Qiao equally contributed to thepresent work. The authors thank Ms. Susan West forwriting assistance.
SUPPLEMENTARY DATA
Supplementary data associated with this article can befound in the online version at http://dx.doi.org/10.1016/j.surg.2013.10.009.
REFERENCES
1. El-Serag HB. Hepatocellular carcinoma: an epidemiologicview. J Clin Gastroenterol 2002;35:S72-8.
2. Parkin D. Global cancer statistics in the year 2000. LancetOncol 2001;2:533-43.
3. Fan ST, Lo CM, Liu CL, et al. Hepatectomy for hepatocellu-lar carcinoma: toward zero hospital deaths. Ann Surg 1999;229:322-30.
4. Cucchetti A, Zanello M, Cescon M, Ercolani G, Del GaudioM, Ravaioli M, et al. Improved diagnostic imaging and inter-ventional therapies prolong survival after resection for he-patocellular carcinoma in cirrhosis: the university ofbologna experience over 10 years. Ann Surg Oncol 2011;18:1630-7.
5. Park JH, Koh KC, Choi MS, Lee JH, Yoo BC, Paik SW, et al.Analysis of risk factors associated with early multinodularrecurrences after hepatic resection for hepatocellular carci-noma. Am J Surg 2006;192:29-33.
6. Kamiyama T, Nakanishi K, Yokoo H, Kamachi H, Tahara M,Kakisaka T, et al. Analysis of the risk factors for early deathdue to disease recurrence or progression within 1 year afterhepatectomy in patients with hepatocellular carcinoma.World J Surg Oncol 2012;10:107.
7. Cucchetti A, Cescon M, Ercolani G, Bigonzi E, Torzilli G,Pinna AD. A comprehensive meta-regression analysis onoutcome of anatomic resection versus non-anatomic resec-tion for hepatocellular carcinoma. Ann Surg Oncol 2012;19:3697-705.
8. Austin PC. A critical appraisal of propensity-score matchingin the medical literature between 1996 and 2003. Stat Med2008;27:2037-49.
9. Huang G, Lai EC, Lau WY, Zhou WP, Shen F, Pan ZY, et al.Posthepatectomy HBV reactivation in hepatitis B-related he-patocellular carcinoma influences postoperative survival inpatients with preoperative low HBV-DNA levels. Ann Surg2013;257:490-505.
10. Edmondson HA, Steiner PE. Primary carcinoma of the liver:a study of 100 cases among 48,900 necropsies. Cancer 1954;7:462-503.

SurgeryVolume 155, Number 3
Cucchetti et al 521
11. Nzeako UC, Goodman ZD, Ishak KG. Comparison of tumorpathologywithdurationof survival ofNorthAmericanpatientswith hepatocellular carcinoma. Cancer 1995;76:579-88.
12. Vauthey JN, Lauwers GY, Esnaola NF, Do KA, Belghiti J,Mirza N, et al. Simplified staging for hepatocellular carci-noma. J Clin Oncol 2002;20:1527-36.
13. Cheng AL, Kang YK, Chen Z, Tsao CJ, Qin S, Kim JS, et al.Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: aphase III randomised, double-blind, placebo-controlledtrial. Lancet Oncol 2009;10:25-34.
14. Llovet JM, Ricci S, Mazzaferro V, Hilgard P, Gane E, BlancJF, et al. Sorafenib in advanced hepatocellular carcinoma.N Engl J Med 2008;359:378-90.
15. Normand ST, Landrum MB, Guadagnoli E, Ayanian JZ,Ryan TJ, Cleary PD, et al. Validating recommendations forcoronary angiography following acute myocardial infarctionin the elderly: a matched analysis using propensity scores.J Clin Epidemiol 2001;54:387-98.
16. Cucchetti A, Piscaglia F, Grigioni AD, Ravaioli M, Cescon M,Zanello M, et al. Preoperative prediction of hepatocellularcarcinoma tumour grade and micro-vascular invasion bymeans of artificial neural network: a pilot study. J Hepatol2010;52:880-8.
17. Colecchia A, Scaioli E, Montrone L, Vestito A, Di Biase AR,Pieri M, et al. Pre-operative liver biopsy in cirrhotic patientswith early hepatocellular carcinoma represents a safe andaccurate diagnostic tool for tumour grading assessment.J Hepatol 2011;54:300-5.
18. Pawlik TM, Gleisner AL, Anders RA, Assumpcao L, Maley W,Choti MA. Preoperative assessment of hepatocellular carci-noma tumour grade using needle biopsy: implications fortransplant eligibility. Ann Surg 2007;245:435-42.
19. Kim BK, Han KH, Park YN, Park MS, Kim KS, Choi JS, et al.Predictionofmicrovascular invasionbefore curative resectionof hepatocellular carcinoma. J Surg Oncol 2008;97:246-52.
20. Pawlik TM, Delman KA, Vauthey JN, Nagorney DM, Ng IO,Ikai I, et al. Tumour size predicts vascular invasion and his-tologic grade: implications for selection of surgical treat-ment for hepatocellular carcinoma. Liver Transpl 2005;11:1086-92.
21. Nasu K, Kuroki Y, Tsukamoto T, Nakajima H, Mori K, Min-ami M. Diffusion-weighted imaging of surgically resectedhepatocellular carcinoma: imaging characteristics and rela-tionship among signal intensity, apparent diffusion coeffi-cient, and histopathologic grade. AJR Am J Roentgenol2009;193:438-44.
22. Saito K,Moriyasu F, Sugimoto K, Nishio R, Saguchi T, Akata S,et al. Histological grade of differentiation of hepatocellularcarcinoma: comparison of the efficacy of diffusion-weightedMRI with T2-weighted imaging and angiography-assisted CT.J Med Imaging Radiat Oncol 2012;56:261-9.
23. Witjes CD, Willemssen FE, Verheij J, van der Veer SJ, Han-sen BE, Verhoef C, et al. Histological differentiation gradeand microvascular invasion of hepatocellular carcinomapredicted by dynamic contrast-enhanced MRI. J MagnReson Imaging 2012;36:641-7.
24. Stigliano R, Marelli L, Yu D, Davies N, Patch D, Bur-roughs AK. Seeding following percutaneous diagnosticand therapeutic approaches for hepatocellular carci-noma. What is the risk and the outcome? Seeding riskfor percutaneous approach of HCC. Cancer Treat Rev2007;33:437-47.
25. Eguchi S, Kanematsu T, Arii S, Okazaki M, Okita K, OmataM, et al. Comparison of the outcomes between an anatom-ical subsegmentectomy and a non-anatomical minor hepa-tectomy for single hepatocellular carcinomas based on aJapanese nationwide survey. Surgery 2008;143:469-75.
26. Prognostic impact of anatomical resection vs. non-anatomical resection for HCC (ARversusNAR) [cited 2013May 31]. Available from: http://clinicaltrials.gov/ct2/show/NCT01236989.