Embed Size (px)
Citation preview
ORIGINAL ARTICLE
Anatomical versus nonanatomical resection of colorectalliver metastases: a meta-analysis
Cheng-Jun Sui & Lu Cao & Bin Li & Jia-Mei Yang &
Shuang-Jia Wang & Xu Su & Yan-Ming Zhou
Accepted: 22 December 2011 /Published online: 4 January 2012# Springer-Verlag 2012
AbstractPurpose The purpose of the study was to compare anatomicalresection (AR) versus nonanatomical resection (NAR) forcolorectal liver metastases (CLM) with respect to periopera-tive and oncological outcomes.Methods Literature search was performed to identifycomparative studies reporting outcomes for both AR andNAR for CLM. Pooled odds ratios (OR) and weighted meandifferences (WMD with 95% confidence intervals (95% CI)were calculated using either the fixed effects model or randomeffects model.Results Seven nonrandomized controlled studies matchedthe selection criteria and reported on 1,662 subjects, ofwhom 989 underwent AR, and 673 underwent NAR forCLM. Compared with the perioperative results, NAR reduced
the operation time (WMD, 0.39; 95% CI, 1.97–79.17)and blood transfusion requirement (OR, 2.98; 95% CI,1.87–4.74), whereas postoperative morbidity and mortalitywere similar between the two groups. With respect to onco-logic outcomes, there was no significant difference in surgicalmargins, overall survival and disease-free survival betweenthe two groups.Conclusions NAR is a safe procedure for CLM and doesnot compromise oncological outcomes. However, thefindings have to be carefully interpreted due to the lower levelof evidence.
Keywords Anatomical resection . Liver surgery . Colorectalliver metastases . Meta-analysis . Prognosis
Introduction
Colorectal cancer remains to be one of the most commonhuman malignancies, afflicting nearly one million peopleworldwide every year [1]. Approximately 50% patients withcolorectal cancer develop hepatic metastases during thecourse of disease. Patients with colorectal liver metastases(CLM) have a dismal prognosis. The median survival rangesfrom 6 to 9 months, and the 5-year survival is between 0%and 3% [2]. Hepatic resection is the only chance of cure forpatients with CLM, and the 5-year survival rate after radicalresection is about 37–58% [2].
A tumor-free resection margin is known to positivelyaffect local recurrences and long-term survival of CLMpatients [3–5]. Improved knowledge of hepatic anatomyand advances in imaging technologies have facilitated anapproach based on the resection of individual hepatic segments.Anatomic resection (AR) is systematic removal of a hepaticsegment confined by tumor-bearing portal tributaries with an
C.-J. Sui : J.-M. YangDepartment of Special Treatment and Liver transplantation,Eastern Hepatobiliary Surgery Hospital,Second Military Medical University,Shanghai, China
L. CaoDepartment of Molecular Oncology,Eastern Hepatobiliary Surgery Hospital,Second Military Medical University,Shanghai, China
B. Li : S.-J. Wang :X. Su :Y.-M. ZhouDepartment of Hepato-Biliary-Pancreato-Vascular Surgery,The First Affiliated Hospital of Xiamen University,Xiamen, China
Y.-M. Zhou (*)Department of Hepatobiliary & Pancreatovascular Surgery,The First Affiliated Hospital of Xiamen University,55 Zhenhai Road,Xiamen 361003, FJ, Chinae-mail: [email protected]
Int J Colorectal Dis (2012) 27:939–946DOI 10.1007/s00384-011-1403-5

adequate margin [6]. Although the potential superiority of ARfor hepatocellular carcinoma (HCC) has been indicated [7], thedata about CLM are conflicting [8–10]. DeMatteo et al. [8]reported better 5-year (49% vs 37%) and overall mediansurvival (55 vs 38 months) for AR versus nonanatomicalresection (NAR), whereas Kokudo et al. [9] reported anequivalent 5-year overall survival rate (45.7% vs 40.4%)between AR and NAR groups
Meta-analysis can be used to evaluate the existing literaturein both a qualitative and quantitative way by comparing andintegrating the results of different studies and taking intoaccount variations in characteristics that can influence theoverall estimate of the outcome of interest [11]. Therefore,we used meta-analysis to evaluate the evidence available bycomparing the clinical efficacy of AR and NAR for thetreatment of CLM.
Methods
Study selection
A MEDLINE, EMBASE, Ovid, and Cochrane databasesearch was performed on all studies that compared AR andNAR for CLM from the time of inception to April 2011. Thefollowing Mesh search headings were used: “wedgeresection,” “anatomic resection,” “nonanatomic resection,”“limited resection,” and “colorectal liver metastases.” Onlystudies on humans and in the English language wereconsidered for inclusion. Reference lists of all retrievedarticles were manually searched for additional studies.
Data extraction
Two reviewers (LC and CS) independently extracted thefollowing parameters from each study: (1) the first authorand year of publication, (2) study population characteristics,(3) study design, inclusion, and exclusion criteria, (4) thenumber of subjects operated on each technique, and (5) treat-ment outcome. All relevant texts, tables, and figures werereviewed for data extraction. Discrepancies between the tworeviewers were resolved by discussion and consensus.
Criteria for inclusion and exclusion
For inclusion in the meta-analysis, a study had to fulfill thefollowing criteria: (1) comparing the results of AR versus NARfor CLM; (2) reporting at least one of the outcome measuresmentioned below, and the mean standard deviation forcontinuous outcomes of interest was reported or can be calcu-lated; and (3) reporting dual (or multiple) studies by the sameinstitution and/or authors, and either one of higher quality or themost recent publications was included in the analysis.
Abstracts, letters, editorials and expert opinions, reviewswithout original data, case reports, and studies lacking controlgroups were excluded.
Outcomes of interest
The following outcomes were used to compare the twooperative techniques: operative outcomes, which includedoperation time, intra-operative blood loss, the number ofpatients requiring blood transfusion; postoperative outcomes,which includedmorbidity, mortality, and the length of hospitalstay; and oncological results, which included pathologicresection margins, overall survival, and disease-free survival.
Statistical analysis
The meta-analysis was performed using the Review Manager(RevMan) software, version 4.2.7. Dichotomous variables wereanalyzed using estimation of odds ratios (OR) with a 95%confidence interval (95% CI), and continuous variables wereanalyzed using weighted mean difference (WMD) with a 95%CI. Pooled effect was calculated using either the fixed effectsmodel or random effects model. Heterogeneity was evaluatedby χ2 and I2. Heterogeneity was considered present if the I2
statistic was >50%. P<0.05 was considered statistically signif-icant. Publication bias was assessed visually using a funnel plot.
Results
Selection of studies
The literature search identified nine studies that compared theresults of AR and NAR for CLM. Of them, one study wasexcluded from the analysis because it did not provide the out-comes of NAR group [12], and another was excluded becauseit was a review [13]. Finally, a total of seven nonrandomizedstudies published between 2000 and 2011 matched theinclusion criteria and were therefore included [8–10, 14–17].
The characteristics of the seven studies are summarizedin Table 1. They included a total of 1,662 patients, of whom989 were in AR group and 673 in NAR group. Two studieswere conducted in the USA [8, 16], one in Japan [9], one inmultiple centers [10], one in the UK [14], one in Italy [15],and one in The Netherlands [17]. The sample size of eachstudy varied from 174 to 376 patients.
In these studies, patients in the two groups were matched forage [8–10, 14–17], gender [8–10, 14–17], the number of tumors[8–10, 15, 17], tumor distribution [9, 15, 17], the primary tumorsite (colon versus rectum) [8–10, 15–17], the primary nodalstatus [8, 10, 15, 17], preoperative carcinoembryonic antigenlevel [8, 10, 14, 15, 17], synchronous disease [10, 14, 16, 17],and disease-free interval [15–17].
940 Int J Colorectal Dis (2012) 27:939–946
Meta-analysis of operative outcomes
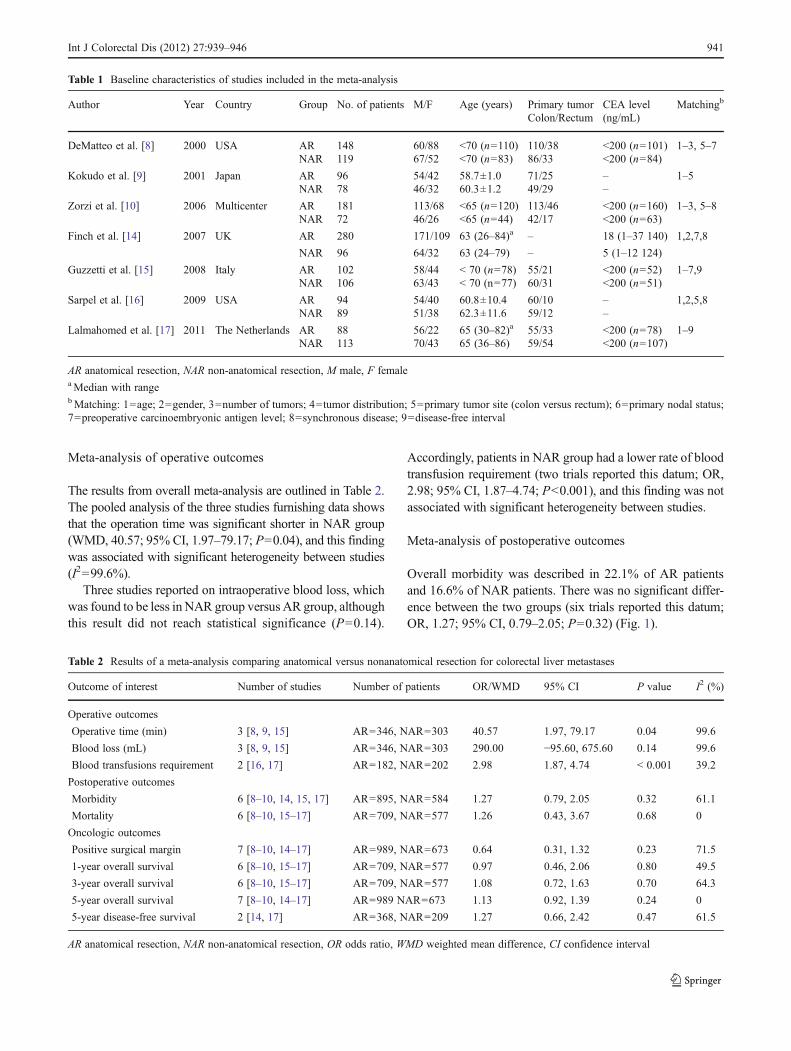
The results from overall meta-analysis are outlined in Table 2.The pooled analysis of the three studies furnishing data showsthat the operation time was significant shorter in NAR group(WMD, 40.57; 95% CI, 1.97–79.17; P00.04), and this findingwas associated with significant heterogeneity between studies(I2099.6%).
Three studies reported on intraoperative blood loss, whichwas found to be less in NAR group versus AR group, althoughthis result did not reach statistical significance (P00.14).
Accordingly, patients in NAR group had a lower rate of bloodtransfusion requirement (two trials reported this datum; OR,2.98; 95% CI, 1.87–4.74; P<0.001), and this finding was notassociated with significant heterogeneity between studies.
Meta-analysis of postoperative outcomes
Overall morbidity was described in 22.1% of AR patientsand 16.6% of NAR patients. There was no significant differ-ence between the two groups (six trials reported this datum;OR, 1.27; 95% CI, 0.79–2.05; P00.32) (Fig. 1).
Table 1 Baseline characteristics of studies included in the meta-analysis
Author Year Country Group No. of patients M/F Age (years) Primary tumorColon/Rectum
CEA level(ng/mL)
Matchingb
DeMatteo et al. [8] 2000 USA AR 148 60/88 <70 (n0110) 110/38 <200 (n0101) 1–3, 5–7NAR 119 67/52 <70 (n083) 86/33 <200 (n084)
Kokudo et al. [9] 2001 Japan AR 96 54/42 58.7±1.0 71/25 – 1–5NAR 78 46/32 60.3±1.2 49/29 –
Zorzi et al. [10] 2006 Multicenter AR 181 113/68 <65 (n0120) 113/46 <200 (n0160) 1–3, 5–8NAR 72 46/26 <65 (n044) 42/17 <200 (n063)
Finch et al. [14] 2007 UK AR 280 171/109 63 (26–84)a – 18 (1–37 140) 1,2,7,8
NAR 96 64/32 63 (24–79) – 5 (1–12 124)
Guzzetti et al. [15] 2008 Italy AR 102 58/44 < 70 (n078) 55/21 <200 (n052) 1–7,9NAR 106 63/43 < 70 (n077) 60/31 <200 (n051)
Sarpel et al. [16] 2009 USA AR 94 54/40 60.8±10.4 60/10 – 1,2,5,8NAR 89 51/38 62.3±11.6 59/12 –
Lalmahomed et al. [17] 2011 The Netherlands AR 88 56/22 65 (30–82)a 55/33 <200 (n078) 1–9NAR 113 70/43 65 (36–86) 59/54 <200 (n0107)
AR anatomical resection, NAR non-anatomical resection, M male, F femaleaMedian with rangebMatching: 10age; 20gender, 30number of tumors; 40tumor distribution; 50primary tumor site (colon versus rectum); 60primary nodal status;70preoperative carcinoembryonic antigen level; 80synchronous disease; 90disease-free interval
Table 2 Results of a meta-analysis comparing anatomical versus nonanatomical resection for colorectal liver metastases
Outcome of interest Number of studies Number of patients OR/WMD 95% CI P value I2 (%)
Operative outcomes
Operative time (min) 3 [8, 9, 15] AR0346, NAR0303 40.57 1.97, 79.17 0.04 99.6
Blood loss (mL) 3 [8, 9, 15] AR0346, NAR0303 290.00 −95.60, 675.60 0.14 99.6
Blood transfusions requirement 2 [16, 17] AR0182, NAR0202 2.98 1.87, 4.74 < 0.001 39.2
Postoperative outcomes
Morbidity 6 [8–10, 14, 15, 17] AR0895, NAR0584 1.27 0.79, 2.05 0.32 61.1
Mortality 6 [8–10, 15–17] AR0709, NAR0577 1.26 0.43, 3.67 0.68 0
Oncologic outcomes
Positive surgical margin 7 [8–10, 14–17] AR0989, NAR0673 0.64 0.31, 1.32 0.23 71.5
1-year overall survival 6 [8–10, 15–17] AR0709, NAR0577 0.97 0.46, 2.06 0.80 49.5
3-year overall survival 6 [8–10, 15–17] AR0709, NAR0577 1.08 0.72, 1.63 0.70 64.3
5-year overall survival 7 [8–10, 14–17] AR0989 NAR0673 1.13 0.92, 1.39 0.24 0
5-year disease-free survival 2 [14, 17] AR0368, NAR0209 1.27 0.66, 2.42 0.47 61.5
AR anatomical resection, NAR non-anatomical resection, OR odds ratio, WMD weighted mean difference, CI confidence interval
Int J Colorectal Dis (2012) 27:939–946 941
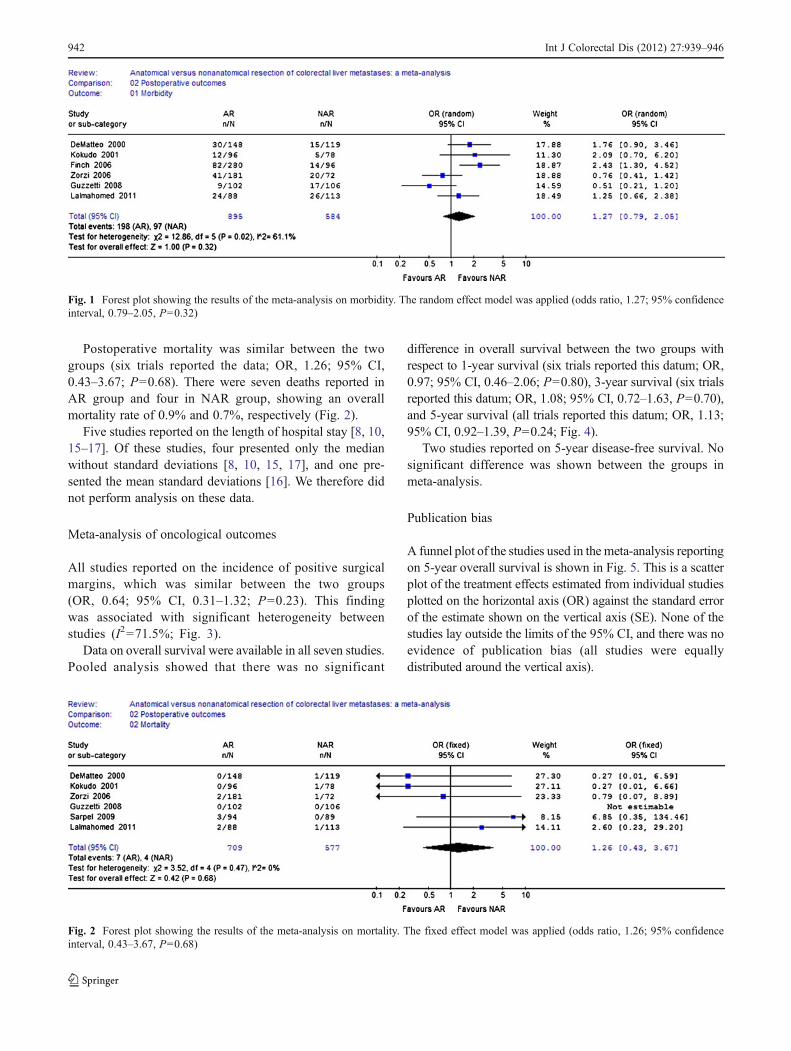
Postoperative mortality was similar between the twogroups (six trials reported the data; OR, 1.26; 95% CI,0.43–3.67; P00.68). There were seven deaths reported inAR group and four in NAR group, showing an overallmortality rate of 0.9% and 0.7%, respectively (Fig. 2).
Five studies reported on the length of hospital stay [8, 10,15–17]. Of these studies, four presented only the medianwithout standard deviations [8, 10, 15, 17], and one pre-sented the mean standard deviations [16]. We therefore didnot perform analysis on these data.
Meta-analysis of oncological outcomes
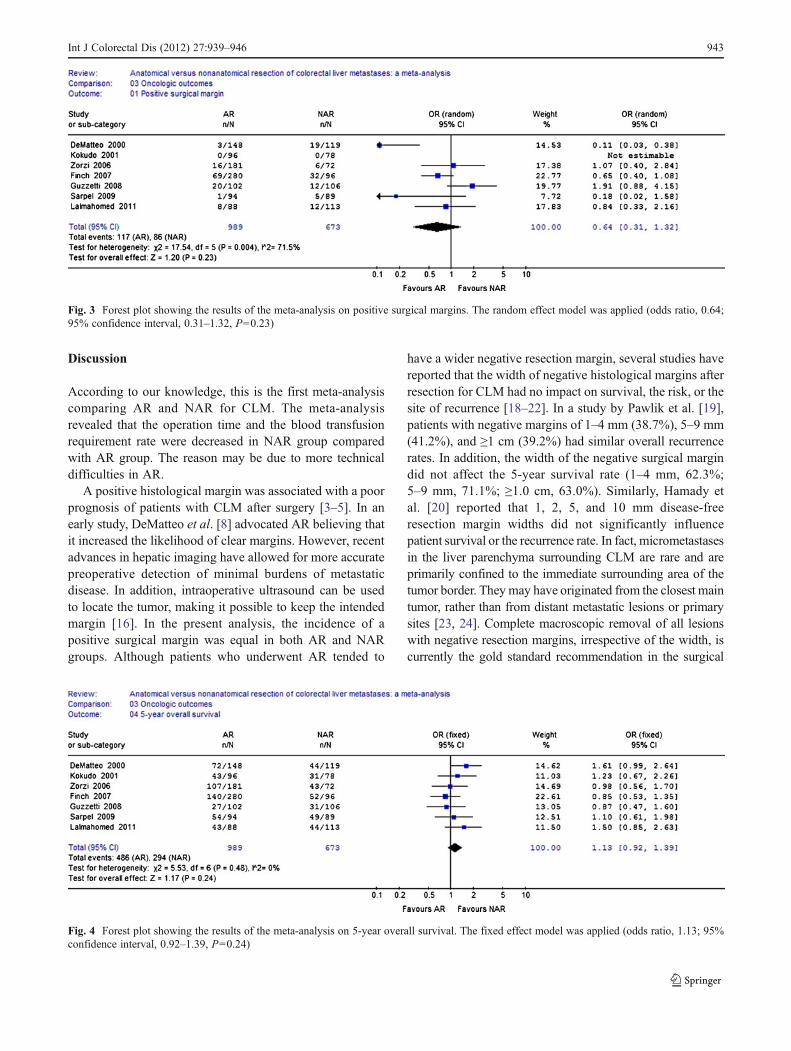
All studies reported on the incidence of positive surgicalmargins, which was similar between the two groups(OR, 0.64; 95% CI, 0.31–1.32; P00.23). This findingwas associated with significant heterogeneity betweenstudies (I2071.5%; Fig. 3).
Data on overall survival were available in all seven studies.Pooled analysis showed that there was no significant
difference in overall survival between the two groups withrespect to 1-year survival (six trials reported this datum; OR,0.97; 95% CI, 0.46–2.06; P00.80), 3-year survival (six trialsreported this datum; OR, 1.08; 95% CI, 0.72–1.63, P00.70),and 5-year survival (all trials reported this datum; OR, 1.13;95% CI, 0.92–1.39, P00.24; Fig. 4).
Two studies reported on 5-year disease-free survival. Nosignificant difference was shown between the groups inmeta-analysis.
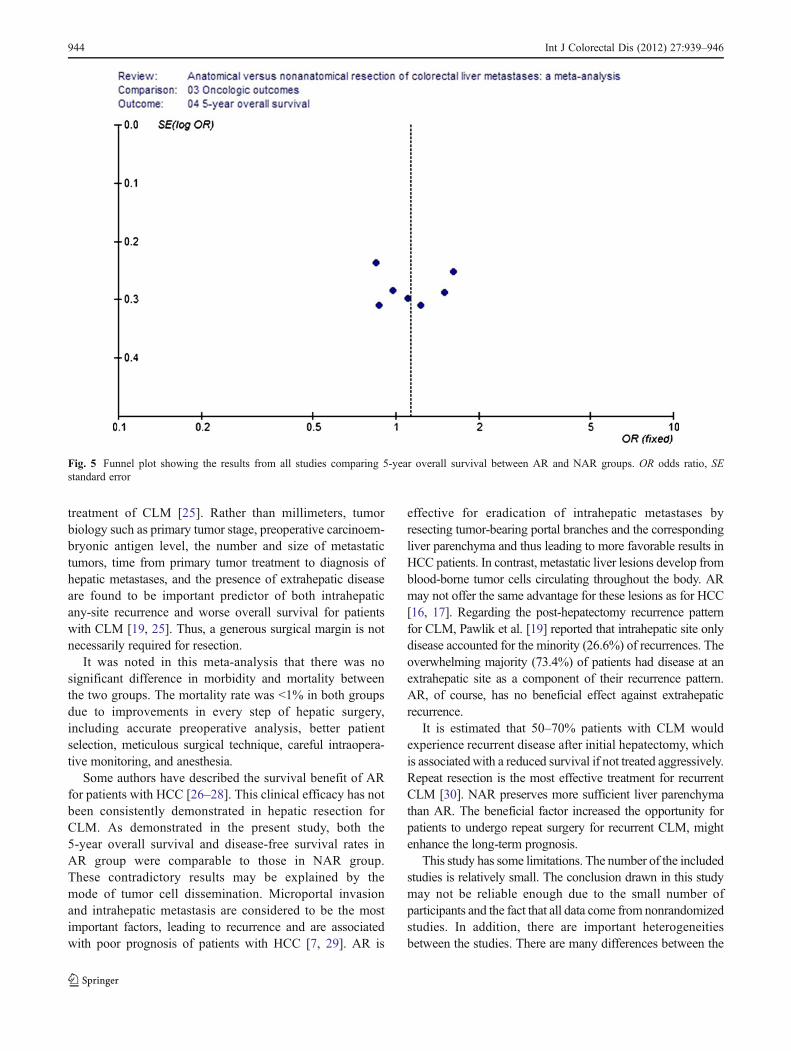
Publication bias
A funnel plot of the studies used in the meta-analysis reportingon 5-year overall survival is shown in Fig. 5. This is a scatterplot of the treatment effects estimated from individual studiesplotted on the horizontal axis (OR) against the standard errorof the estimate shown on the vertical axis (SE). None of thestudies lay outside the limits of the 95% CI, and there was noevidence of publication bias (all studies were equallydistributed around the vertical axis).
Fig. 1 Forest plot showing the results of the meta-analysis on morbidity. The random effect model was applied (odds ratio, 1.27; 95% confidenceinterval, 0.79–2.05, P00.32)
Fig. 2 Forest plot showing the results of the meta-analysis on mortality. The fixed effect model was applied (odds ratio, 1.26; 95% confidenceinterval, 0.43–3.67, P00.68)
942 Int J Colorectal Dis (2012) 27:939–946
Discussion
According to our knowledge, this is the first meta-analysiscomparing AR and NAR for CLM. The meta-analysisrevealed that the operation time and the blood transfusionrequirement rate were decreased in NAR group comparedwith AR group. The reason may be due to more technicaldifficulties in AR.
A positive histological margin was associated with a poorprognosis of patients with CLM after surgery [3–5]. In anearly study, DeMatteo et al. [8] advocated AR believing thatit increased the likelihood of clear margins. However, recentadvances in hepatic imaging have allowed for more accuratepreoperative detection of minimal burdens of metastaticdisease. In addition, intraoperative ultrasound can be usedto locate the tumor, making it possible to keep the intendedmargin [16]. In the present analysis, the incidence of apositive surgical margin was equal in both AR and NARgroups. Although patients who underwent AR tended to
have a wider negative resection margin, several studies havereported that the width of negative histological margins afterresection for CLM had no impact on survival, the risk, or thesite of recurrence [18–22]. In a study by Pawlik et al. [19],patients with negative margins of 1–4 mm (38.7%), 5–9 mm(41.2%), and ≥1 cm (39.2%) had similar overall recurrencerates. In addition, the width of the negative surgical margindid not affect the 5-year survival rate (1–4 mm, 62.3%;5–9 mm, 71.1%; ≥1.0 cm, 63.0%). Similarly, Hamady etal. [20] reported that 1, 2, 5, and 10 mm disease-freeresection margin widths did not significantly influencepatient survival or the recurrence rate. In fact, micrometastasesin the liver parenchyma surrounding CLM are rare and areprimarily confined to the immediate surrounding area of thetumor border. They may have originated from the closest maintumor, rather than from distant metastatic lesions or primarysites [23, 24]. Complete macroscopic removal of all lesionswith negative resection margins, irrespective of the width, iscurrently the gold standard recommendation in the surgical
Fig. 3 Forest plot showing the results of the meta-analysis on positive surgical margins. The random effect model was applied (odds ratio, 0.64;95% confidence interval, 0.31–1.32, P00.23)
Fig. 4 Forest plot showing the results of the meta-analysis on 5-year overall survival. The fixed effect model was applied (odds ratio, 1.13; 95%confidence interval, 0.92–1.39, P00.24)
Int J Colorectal Dis (2012) 27:939–946 943
treatment of CLM [25]. Rather than millimeters, tumorbiology such as primary tumor stage, preoperative carcinoem-bryonic antigen level, the number and size of metastatictumors, time from primary tumor treatment to diagnosis ofhepatic metastases, and the presence of extrahepatic diseaseare found to be important predictor of both intrahepaticany-site recurrence and worse overall survival for patientswith CLM [19, 25]. Thus, a generous surgical margin is notnecessarily required for resection.
It was noted in this meta-analysis that there was nosignificant difference in morbidity and mortality betweenthe two groups. The mortality rate was <1% in both groupsdue to improvements in every step of hepatic surgery,including accurate preoperative analysis, better patientselection, meticulous surgical technique, careful intraopera-tive monitoring, and anesthesia.
Some authors have described the survival benefit of ARfor patients with HCC [26–28]. This clinical efficacy has notbeen consistently demonstrated in hepatic resection forCLM. As demonstrated in the present study, both the5-year overall survival and disease-free survival rates inAR group were comparable to those in NAR group.These contradictory results may be explained by themode of tumor cell dissemination. Microportal invasionand intrahepatic metastasis are considered to be the mostimportant factors, leading to recurrence and are associatedwith poor prognosis of patients with HCC [7, 29]. AR is
effective for eradication of intrahepatic metastases byresecting tumor-bearing portal branches and the correspondingliver parenchyma and thus leading to more favorable results inHCC patients. In contrast, metastatic liver lesions develop fromblood-borne tumor cells circulating throughout the body. ARmay not offer the same advantage for these lesions as for HCC[16, 17]. Regarding the post-hepatectomy recurrence patternfor CLM, Pawlik et al. [19] reported that intrahepatic site onlydisease accounted for the minority (26.6%) of recurrences. Theoverwhelming majority (73.4%) of patients had disease at anextrahepatic site as a component of their recurrence pattern.AR, of course, has no beneficial effect against extrahepaticrecurrence.
It is estimated that 50–70% patients with CLM wouldexperience recurrent disease after initial hepatectomy, whichis associatedwith a reduced survival if not treated aggressively.Repeat resection is the most effective treatment for recurrentCLM [30]. NAR preserves more sufficient liver parenchymathan AR. The beneficial factor increased the opportunity forpatients to undergo repeat surgery for recurrent CLM, mightenhance the long-term prognosis.
This study has some limitations. The number of the includedstudies is relatively small. The conclusion drawn in this studymay not be reliable enough due to the small number ofparticipants and the fact that all data come from nonrandomizedstudies. In addition, there are important heterogeneitiesbetween the studies. There are many differences between the
Fig. 5 Funnel plot showing the results from all studies comparing 5-year overall survival between AR and NAR groups. OR odds ratio, SEstandard error
944 Int J Colorectal Dis (2012) 27:939–946

studies that serve as sources of heterogeneity, includingvariations in patient characteristics and surgical skills anddifferent neoadjuvant chemotherapy regimens in perioperativeand postoperative care. Although we used a random effectmodel to take into consideration the variation between thestudies, this may not necessarily rule out the effect ofheterogeneity between the studies, though the influence maybe very limited.
In conclusion, the results of this meta-analysis of 1,662patients have shown that NAR is a safe procedure for CLMand does not compromise oncological outcomes. However,the findings have to be carefully interpreted due to the lowerlevel of evidence. Future multicenter and high-quality trialsare needed.
Acknowledgments The authors thank Umut Sarpel, MD for kindlyproviding details about their reported cases.
References
1. El-Tawil AM (2010) Colorectal cancer and pollution. World JGastroenterol 16:3475–3477. doi:10.3748/wjg.v16.i28.3475
2. Mohammad WM, Balaa FK (2009) Surgical management ofcolorectal liver metastases. Clin Colon Rectal Surg 22:225–232.doi:10.1055/s-0029-1242462
3. Nordlinger B, Guiguet M, Vaillant JC, Balladur P, Boudjema K,Bachellier P, Jaeck D (1996) Surgical resection of colorectalcarcinoma metastases to the liver. A prognostic scoring system toimprove case selection, based on 1568 patients. AssociationFrançaise de Chirurgie. Cancer 77:1254–1262. doi:10.1002/(SICI)1097-0142(19960401
4. Fong Y, Fortner J, Sun RL, Brennan MF, Blumgart LH (1999)Clinical score for predicting recurrence after hepatic resection formetastatic colorectal cancer: analysis of 1001 consecutive cases.Ann Surg 230:309–318
5. Rees M, Tekkis PP, Welsh FK, O’Rourke T, John TG (2008)Evaluation of long-term survival after hepatic resection for meta-static colorectal cancer: a multifactorial model of 929 patients. AnnSurg 247:125–135. doi:10.1097/SLA.0b013e31815aa2c2
6. Makuuchi M, Hasegawa H, Yamazaki S (1985) Ultrasonicallyguided subsegmentectomy. Surg Gynecol Obstet 161:346–350
7. Zhou Y, Xu D, Wu L, Li B (2011) Meta-analysis of anatomicresection versus nonanatomic resection for hepatocellular carcinoma.Langenbecks Arch Surg 396:1109–1117. doi:10.1007/s00423-011-0784-9
8. DeMatteo RP, Palese C, Jarnagin WR, Sun RL, Blumgart LH,Fong Y (2000) Anatomic segmental hepatic resection is superiorto wedge resection as an oncologic operation for colorectal livermetastases. J Gastrointest Surg 4:178–184
9. Kokudo N, Tada K, Seki M, Ohta H, Azekura K, Ueno M,Matsubara T, Takahashi T, Nakajima T, Muto T (2001) Anatomicalmajor resection versus nonanatomical limited resection for livermetastases from colorectal carcinoma. Am J Surg 181:153–159
10. Zorzi D, Mullen JT, Abdalla EK, Pawlik TM, Andres A, MuratoreA, Curley SA, Mentha G, Capussotti L, Vauthey JN (2006)Comparison between hepatic wedge resection and anatomicresection for colorectal liver metastases. J Gastrointest Surg10:86–94. doi:10.1016/j.gassur.2005.07.022
11. Aziz O, Constantinides V, Tekkis PP, Athanasiou T, Purkayastha S,Paraskeva P, Darzi AW, Heriot AG (2006) Laparoscopic versus
open surgery for rectal cancer: a meta-analysis. Ann Surg Oncol13:413–424. doi:10.1245/ASO.2006.05.045
12. Stewart GD, O’Súilleabháin CB, Madhavan KK, Wigmore SJ,Parks RW, Garden OJ (2004) The extent of resection influencesoutcome following hepatectomy for colorectal liver metastases.Eur J Surg Oncol 30:370–376. doi:10.1016/j.ejso.2004.01.011
13. Yasui K, Shimizu Y (2005) Surgical treatment for metastaticmalignancies. Anatomical resection of liver metastasis: indicationsand outcomes. Int J Clin Oncol 10:86–96. doi:10.1007/s10147-005-0475-z
14. Finch RJ, Malik HZ, Hamady ZZ, Al-Mukhtar A, Adair R, PrasadKR, Lodge JP, Toogood GJ (2007) Effect of type of resection onoutcome of hepatic resection for colorectal metastases. Br J Surg94:1242–1248. doi:10.1002/bjs.5640
15. Guzzetti E, Pulitanò C, Catena M, Arru M, Ratti F, Finazzi R,Aldrighetti L, Ferla G (2008) Impact of type of liver resection onthe outcome of colorectal liver metastases: a case-matched analysis. JSurg Oncol 97:503–507. doi:10.1002/jso.20979
16. Sarpel U, Bonavia AS, Grucela A, Roayaie S, Schwartz ME,Labow DM (2009) Does anatomic versus nonanatomic resectionaffect recurrence and survival in patients undergoing surgery forcolorectal liver metastasis? Ann Surg Oncol 16:379–384.doi:10.1245/s10434-008-0218-2
17. Lalmahomed ZS, Ayez N, van der Pool AE, Verheij J, IJzermansJN, Verhoef C (2011) Anatomical versus nonanatomical resectionof colorectal liver metastases: is there a difference in surgical andoncological outcome? World J Surg 35:656–661. doi:10.1007/s00268-010-0890-9
18. Shirabe K, Takenaka K, Gion T, Fujiwara Y, Shimada M, YanagaK, Maeda T, Kajiyama K, Sugimachi K (1997) Analysis ofprognostic risk factors in hepatic resection for metastatic colorectalcarcinoma with special reference to the surgical margin. Br J Surg84:1077–1080
19. Pawlik TM, Scoggins CR, Zorzi D, Abdalla EK, Andres A, Eng C,Curley SA, Loyer EM, Muratore A, Mentha G, Capussotti L,Vauthey JN (2005) Effect of surgical margin status on survivaland site of recurrence after hepatic resection for colorectal metastases.Ann Surg 241:715–722
20. Hamady ZZ, Cameron IC, Wyatt J, Prasad RK, Toogood GJ,Lodge JP (2006) Resection margin in patients undergoinghepatectomy for colorectal liver metastasis: a critical appraisalof the 1 cm rule. Eur J Surg Oncol 32:557–563. doi:10.1016/j.ejso.2006.02.001
21. Figueras J, Burdio F, Ramos E, Torras J, Llado L, Lopez-Ben S,Codina-Barreras A, Mojal S (2007) Effect of subcentimeternonpositive resection margin on hepatic recurrence in patientsundergoing hepatectomy for colorectal liver metastases. Evidencesfrom 663 liver resections. Ann Oncol 18:1190–1195. doi:10.1093/annonc/mdm106
22. Muratore A, Ribero D, Zimmitti G, Mellano A, Langella S,Capussotti L (2010) Resection margin and recurrence-free survivalafter liver resection of colorectal metastases. Ann Surg Oncol17:1324–1329. doi:10.1245/s10434-009-0770-4
23. Yamamoto J, Sugihara K, Kosuge T, Takayama T, Shimada K,Yamasaki S, Sakamoto M, Hirohashi S (1995) Pathologic supportfor limited hepatectomy in the treatment of liver metastases fromcolorectal cancer. Ann Surg 221:74–78
24. Kokudo N, Miki Y, Sugai S, Yanagisawa A, Kato Y, Sakamoto Y,Yamamoto J, Yamaguchi T, Muto T, Makuuchi M (2002) Geneticand histological assessment of surgical margins in resected livermetastases from colorectal carcinoma: minimum surgical marginsfor successful resection. Arch Surg 137:833–840
25. de Haas RJ, Wicherts DA, Flores E, Azoulay D, Castaing D, AdamR (2008) R1 resection by necessity for colorectal liver metastases:is it still a contraindication to surgery? Ann Surg 248:626–637.doi:10.1097/SLA.0b013e31818a07f1
Int J Colorectal Dis (2012) 27:939–946 945

26. Cho YB, Lee KU, Lee HW, Cho EH, Yang SH, Cho JY, Yi NJ, SuhKS (2007) Anatomic versus non-anatomic resection for small singlehepatocellular carcinomas. Hepatogastroenterology 54:1766–1769
27. Hasegawa K, Kokudo N, Imamura H, Matsuyama Y, Aoki T,Minagawa M, Sano K, Sugawara Y, Takayama T, Makuuchi M(2005) Prognostic impact of anatomic resection for hepatocel-lular carcinoma. Ann Surg 242:252–259. doi:10.1097/01.sla.0000171307.37401.db
28. Kamiyama T, Nakanishi K, Yokoo H, Kamachi H, Matsushita M,Todo S (2010) The impact of anatomical resection for hepatocellular
carcinoma that meets the Milan criteria. J Surg Oncol 101:54–60.doi:10.1002/jso.21414
29. Zhou YM, Yang JM, Li B, Yin ZF, Xu F, Wang B, Xu W, Kan T(2010) Risk factors for early recurrence of small hepatocellularcarcinoma after curative resection. Hepatobiliary Pancreat Dis Int9:33–37
30. Yan TD, Sim J, Black D, Niu R, Morris DL (2007) Systematicreview on safety and efficacy of repeat hepatectomy for recurrentliver metastases from colorectal carcinoma. Ann Surg Oncol14:2069–2077. doi:10.1245/s10434-007-9388-6
946 Int J Colorectal Dis (2012) 27:939–946