-
8/6/2019 Anatomy for the Gynecologic Oncologist
1/70
-
8/6/2019 Anatomy for the Gynecologic Oncologist
2/70
Overview
Abdominal wall anatomy
Upper abdomen organs, vessels,
innervation Pelvic anatomy
Vulvar anatomy
-
8/6/2019 Anatomy for the Gynecologic Oncologist
3/70
Abdominal wall anatomy
Best to comprehend the anatomy as it relates to
incision types Midline, Pfannenstiel, Maylard &
Cherney
What dermatomes are affected by a midline
incision? What are affected by a pfannenstiel?
Name all the layers of the abdominal wall above
and below the arcuate line?
Describe the relationship between the incision
type and the inferior epigastric artery?
-
8/6/2019 Anatomy for the Gynecologic Oncologist
4/70
Innervation of the abdominal wall
-
8/6/2019 Anatomy for the Gynecologic Oncologist
5/70
Musculature
-
8/6/2019 Anatomy for the Gynecologic Oncologist
6/70
Rectus sheath
-
8/6/2019 Anatomy for the Gynecologic Oncologist
7/70
Rectus sheath
-
8/6/2019 Anatomy for the Gynecologic Oncologist
8/70
Course of the epigastric artery
-
8/6/2019 Anatomy for the Gynecologic Oncologist
9/70
Veins of the abdominal wall
-
8/6/2019 Anatomy for the Gynecologic Oncologist
10/70
Upper abdominal anatomy
Adequate debulking of ovarian carcinomarequires dissection of
several key organs
What vessels supply the omentum,spleen, stomach, small bowel,
colon andliver?
What are their functions?
How do you manage these organspostoperatively if they are
injured orremoved?
-
8/6/2019 Anatomy for the Gynecologic Oncologist
11/70
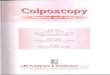
Omentum
Functions as a filter for lymphatic fluid
Lymph fluid flow in a clock-wise patternsecondary to peristalsis
of the ascending,
transverse and descending colon Brings lymph fluid to the
cisterna chyli, the
thoracic duct and then the left brachiocephalicvein
Right sided lymphatic drainage is directedthrough lymphatic
channels of the diaphragm tothe azygos system and then the IVC and
SVC
-
8/6/2019 Anatomy for the Gynecologic Oncologist
12/70
Omentum
-
8/6/2019 Anatomy for the Gynecologic Oncologist
13/70
Stomach
Second organ involved with digestion
Innervated by the vagus nerve
Blood supply from the celiac trunk: left and right
gastric arteries, right and left gastroepiploicarteries and the
short gastric arteries
Produces hydrochloric acid and pepsin to digestfood
Produces 1 to 1.5 liters of fluid each day
Injury can be controlled by primary closure Continuous NG
suctioning causes a
hyponatremic, hypokalemic metabolic alkalosis
-
8/6/2019 Anatomy for the Gynecologic Oncologist
14/70
Stomach
-
8/6/2019 Anatomy for the Gynecologic Oncologist
15/70
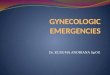
Spleen
Filter for senescent erythrocytes and circulatingpathogens
Major producer of opsonins (properdin/ tuftsin)
Hilum contains the splenic artery and vein
Extremely vascular
Splenocolic ligament must be mobilized to free thesplenic
flexure of the colon
Posterior aspect of this ligament in close proximity to thetail
of the pancreas
Splenectomies patients are at risk for pneumonia,
bacteremia, pancreatic injuries and splenic abcesses MUST BE
VACCINATED POST OPERATIVELY FOR: Streptococcus pneumoniae
Haemophilus influenzae
Nisseria meningitidis
-
8/6/2019 Anatomy for the Gynecologic Oncologist
16/70
Spleen
-
8/6/2019 Anatomy for the Gynecologic Oncologist
17/70
Small Bowel
On average 270 to 290 cm in length
Consists of the duodenum ( 20cm), jejunum (100 to110cm) and
ileum (150 to 160 cm)
Entire blood supply from the superior mesenteric artery
Both parasympathetic and sympathetic innervation Parasympathetic
innervation is from the vagus nerve
which stems from the celiac ganglion
Parasympathetic innervation controls motility andsecretion of
enzymes
Sympathetic innervation from three sets of splanchnicnerves
oriented around the base of the SMA
Sympathetic innervation responsible for pain sensationand blood
vessel motility
-
8/6/2019 Anatomy for the Gynecologic Oncologist
18/70
Small Bowel
Majority of nutritional uptake is responsible within thejejunum
and ileum
80% to 90% of proteins reabsorbed in the jejunum
95% of lipid reabsorbed within the jejunum and ileum
8 to 10 liters of water are reabsorbed, perhaps only 500ml
actually enter the cecum
Fat soluble vitamins are reabsorbed in the terminal ileum(A, D,
E and K)
Vitamin B12 also reabsorbed in the terminal ileum KEY POINT: the
more small bowel removed expect
problems with digestion, nutrition and diarrhea
-
8/6/2019 Anatomy for the Gynecologic Oncologist
19/70
Small Bowel
Enzymes of the small bowel
Gastrin (D) promotes gastric acid and pepsinogen
production
CCK(D) promotes pancreatic enzyme secretion andgall bladder
contraction
Secretin (D,J) causes water release, secretion of bile
salts and inhibition of gastrin
Somatostatin (P) universal off switch Gastrin releasing peptide
(D,J,I) universal on switch
Motilin (D,J) stimulates upper GI motility
-
8/6/2019 Anatomy for the Gynecologic Oncologist
20/70
Small Bowel
Small Bowel Obstruction
Adhesions 60%
Malignancy 20%
Hernias 10%
Crohns disease 5%
Miscellaneous 5%
-
8/6/2019 Anatomy for the Gynecologic Oncologist
21/70
Duodenum
-
8/6/2019 Anatomy for the Gynecologic Oncologist
22/70
Small Bowel
-
8/6/2019 Anatomy for the Gynecologic Oncologist
23/70
Small Bowel
-
8/6/2019 Anatomy for the Gynecologic Oncologist
24/70
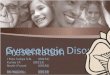
Colon
6 segments cecum and appendix,
ascending, transverse, descending,
sigmoid and rectum
On average 130 to 150 cm in length
Blood supply from the superior mesenteric
and inferior mesenteric arteries (SMA &
IMA)
-
8/6/2019 Anatomy for the Gynecologic Oncologist
25/70
Segments of the colon
-
8/6/2019 Anatomy for the Gynecologic Oncologist
26/70
Blood supply to the colon
-
8/6/2019 Anatomy for the Gynecologic Oncologist
27/70
Colonic function
Absorption
1000 to 1500ml of ileal effluent crosses the ileocecal
valve
Stool has 100 to 150 ml of water Descending colon mainly
responsible
Recycling of nutrients
Nonstarch polysaccharides
Short chain fatty acids Urea
Ascending colon responsible
-
8/6/2019 Anatomy for the Gynecologic Oncologist
28/70
Colonic innervation
Parasympathetic innervation from the vagusnerve and the pelvic
autonomic center S2-S4
Nerves are centered in plexuses along the
subserosal and muscular components of thecolon: Auerbach and
Meissner plexuses
Controls colonic motility
Sympathetic innervation is from the superior and
inferior mesenteric ganglia (found by the SMAand IMA)
Controls pain and vascular tonicity
-
8/6/2019 Anatomy for the Gynecologic Oncologist
29/70
Cecal anatomy
-
8/6/2019 Anatomy for the Gynecologic Oncologist
30/70
Appendix
No appreciable utility
Associated with carcinoid and primary
appendiceal carcinomas
Must be taken for mucinous ovarian tumors
Appendiceal artery arises from the ileocolic
artery and MUST be ligated
Primary appendiceal tumors often diagnosed bygynecologic
oncologists as a right ovarian tumor
-
8/6/2019 Anatomy for the Gynecologic Oncologist
31/70
Appendix
-
8/6/2019 Anatomy for the Gynecologic Oncologist
32/70
Portal circulation
Not essential for gynecologic malignancies;however must
understand the different source ofvenous drainage
Splenic vein, SMV, IMV, gastric veins involved inthe portal
system
Portal hypertension can therefore cause,gastroesophageal
varices, rectal varices andmedusae caput
Acute bleeding has 25-30% mortality rate
Patients with cirrhosis have a 50% mortality rate
-
8/6/2019 Anatomy for the Gynecologic Oncologist
33/70
Portal circulation
-
8/6/2019 Anatomy for the Gynecologic Oncologist
34/70
Pelvic Anatomy
The home of the gynecologic oncologist
Focus on blood supply, nerves of thepelvis, musculature and
rectal anatomy
Must understand the boundaries of pelviclymph node
dissection
Lateral: genitofemoral nerve
Medial: ureter
Inferior: deep iliac circumflex vein
Superior: inferior mesenteric artery
P l i bl d l
-
8/6/2019 Anatomy for the Gynecologic Oncologist
35/70
Pelvic blood supply Aorta
Middle sacral artery
Common iliac artery External iliac artery
Inferior epigastric artery
Deep circumflex iliac artery
Posterior division of internal iliac artery Superior gluteal
artery
Iliolumbar artery
Lateral sacral
Anterior division of internal iliac artery Obturator artery
Uterine artery
Superior vesical artery
Inferior vesical artery
Umbilical ligament
Middle rectal artery Internal pudendal artery
Inferior rectal artery
Labial arteries
Dorsal artery of the clitoris
-
8/6/2019 Anatomy for the Gynecologic Oncologist
36/70
Pelvic blood supply
-
8/6/2019 Anatomy for the Gynecologic Oncologist
37/70
Pelvic blood supply
-
8/6/2019 Anatomy for the Gynecologic Oncologist
38/70
Common iliac artery
-
8/6/2019 Anatomy for the Gynecologic Oncologist
39/70
External iliac artery & vein
-
8/6/2019 Anatomy for the Gynecologic Oncologist
40/70
Superior vesical artery
-
8/6/2019 Anatomy for the Gynecologic Oncologist
41/70
Obturator space
-
8/6/2019 Anatomy for the Gynecologic Oncologist
42/70
Obturator nerve
-
8/6/2019 Anatomy for the Gynecologic Oncologist
43/70
Obturator artery
-
8/6/2019 Anatomy for the Gynecologic Oncologist
44/70
Obturator venous plexus
Pelvic nerves
-
8/6/2019 Anatomy for the Gynecologic Oncologist
45/70
Pelvic nerves Femoral nerve
Nerve roots L2, L3, L4
Provides motor function to the extensor muscles Provides
sensation to the thigh
Sciatic nerve Nerve roots L4, L5, S1, S2, S3
Largest nerve in the body
It divides into the tibial and peroneal nerves
Provides motor function to the distal extremity Obturator
nerve
Nerve roots L2, L3, L4
Provides motor function to the adductor muscles
Pudendal nerve Nerve roots S2, S3, S4
Provides motor functions to the muscles of the pelvis and
external analsphincter
Provides sensation to the vulva and clitoris
Genitofemoral nerve Nerve roots L1, L2
Provides sensation to the thigh and vulva
P l i
-
8/6/2019 Anatomy for the Gynecologic Oncologist
46/70
Pelvic nerves
Pelvic nerves
-
8/6/2019 Anatomy for the Gynecologic Oncologist
47/70
Pelvic nerves
-
8/6/2019 Anatomy for the Gynecologic Oncologist
48/70
Muscles of the pelvis
Psoas L2, L3, L4 flexes thigh
Piriformis S1, S2 rotates thigh laterally
Obturator internus L5, S1, S2 rotates thigh laterally
Levator Ani Pubococcygeus S3, S4 raise pelvic floor
Iliococcygeus
Puborectalis
Coccygeus S4, S5 raise pelvic floor
Muscles of the pelvis
-
8/6/2019 Anatomy for the Gynecologic Oncologist
49/70
Muscles of the pelvis
M l f th l i
-
8/6/2019 Anatomy for the Gynecologic Oncologist
50/70
Muscles of the pelvis
-
8/6/2019 Anatomy for the Gynecologic Oncologist
51/70
Bladder
Muscular structure which functions as a reservoir forurine
Can hold 1000 ml however most females have a strongurge to void
at 400 ml
Supplied by the superior vesical and inferior
vesicalarteries
Innervation is both parasympathetic and sympathetic
Parasympathetic (S2, S3, S4) controls detrusorcontraction while
inhibiting the internal sphincter
Sympathetic (T11, T12, L1, L2) transmit sensation
Bladder innervation
-
8/6/2019 Anatomy for the Gynecologic Oncologist
52/70
Bladder innervation
-
8/6/2019 Anatomy for the Gynecologic Oncologist
53/70
Rectum
Last portion of the colon, rich blood supply, relativelymobile
below the peritoneum
Multiple layers which control continence 1st it follows the
contour of the sacrum
2nd
the valves of houston produce sharp turns for the feces
tonavigate
3rd the puborectalis muscles forms a sling around the
rectumcalled the anorectal angle
All these layers close off the lumen with valsalva
The pectinate line marks the transformation fromsquamous
epithelium to columnar epithelium
Blood supply stems from both the IMA and the internaliliac
arteries (superior, middle, inferior rectal arteries)
Rectum
-
8/6/2019 Anatomy for the Gynecologic Oncologist
54/70
Rectum
Rectum
-
8/6/2019 Anatomy for the Gynecologic Oncologist
55/70
Rectum
-
8/6/2019 Anatomy for the Gynecologic Oncologist
56/70
Vulvar anatomy
Layers of support to the pelvic floor
Blood supply to the vulva Internal pudendal artery
Inferior rectal artery
Labial/ perineal arteries
Dorsal artery of the clitoris External pudendal artery
Nervous supply to the vulva Ilioinguinal nerve
Pudendal nerve Labial/ perineal nerves
Dorsal nerve of the clitoris
Posterior femoral cutaneous nerve
Points of interest with a inguinal lymphadenectomy
Vulva: deep to superficial
-
8/6/2019 Anatomy for the Gynecologic Oncologist
57/70
Vulva: deep to superficial
Vulva: deep to superficial
-
8/6/2019 Anatomy for the Gynecologic Oncologist
58/70
Vulva: deep to superficial
V l d t fi i l
-
8/6/2019 Anatomy for the Gynecologic Oncologist
59/70
Vulva: deep to superficial
Vulva: deep to superficial
-
8/6/2019 Anatomy for the Gynecologic Oncologist
60/70
Vulva: deep to superficial
Vulva: deep to superficial
-
8/6/2019 Anatomy for the Gynecologic Oncologist
61/70
Vulva: deep to superficial
Vulvar blood supply
-
8/6/2019 Anatomy for the Gynecologic Oncologist
62/70
Vulvar blood supply
Vulvar blood supply
-
8/6/2019 Anatomy for the Gynecologic Oncologist
63/70
pp y
Vulvar blood supply
-
8/6/2019 Anatomy for the Gynecologic Oncologist
64/70
pp y
Lymphatic drainage of the vulva
-
8/6/2019 Anatomy for the Gynecologic Oncologist
65/70
Lymphatic drainage of the vulva
Innervation of the vulva
-
8/6/2019 Anatomy for the Gynecologic Oncologist
66/70
Femoral Triangle
-
8/6/2019 Anatomy for the Gynecologic Oncologist
67/70
Femoral Triangle
Borders: Inguinal ligament superiorly, sartoriusmuscle laterally
and adductor longus medially
Superficial inguinal lymph nodes above thecribriform fascia
(6-8)
Femoral nerve, artery, and vein are found belowthe cribriform
fascia
Deep inguinal lymph nodes (2-3)
Cloquets node deepest most superior lymphnode before crossing
inguinal ligament andthereby external iliac lymph nodes
Femoral Triangle
-
8/6/2019 Anatomy for the Gynecologic Oncologist
68/70
g
Muscles of the thigh
-
8/6/2019 Anatomy for the Gynecologic Oncologist
69/70
Muscles of the thigh
Sartorius
L2, L3 (F) Flexes, abducts and
laterally rotates thigh
Gracilus L2, L3 (O) Flexes, adducts and
medially rotates thigh
Adductor longus L2, L3 (O) Adducts thigh
Femoral and Obturator Nerves
-
8/6/2019 Anatomy for the Gynecologic Oncologist
70/70