Embed Size (px)
Citation preview
AANNAALLYYSSIISS OOFF RREESSUULLTTSS OOFF
IINNTTEERRTTRROOCCHHAANNTTEERRIICC
FFRRAACCTTUURREESS
BBYY
DDYYNNAAMMIICC HHIIPP SSCCRREEWW FFIIXXAATTIIOONN

C E R T I F I C A T E
This is to certify that this dissertation entitled “ANALYSIS
OF RESULTS OF INTERTROCHANTRIC FRACTURES BY
DYNAMIC HIP SCREW FIXATION” is a bonafide record of the
work doneby DDrr.. NNAARREENNDDRRAA RREEDDDDYY NELLORE in partial
fulfillment of the requirement for the award of M.C.H. Orthopedic.
D E C L A R A T I O N
I, Dr.NARENDRA REDDY, hereby declare that this dissertation
entitled “ANALYSIS OF RESULS OF INTER
TROCHANTERIC FRACTURE BY DYNAMIC HIP
SCREW FIXATION” hhaass bbeeeenn pprreeppaarreedd bbyy mmee..
Place:
Date: Dr. NARENDRA REDDY
A C K N O W L E D G E M E N T S
I am deeply indebted to DR.Y.SIVAPRASAD, Prof. DDeepp.. ooff
..oorrtthhooppaaeeddiiccss,, NNaarraayyaannaa mmeeddiiccaall ccoolllleeggee,, NNEELLLLOORREE,, for his
inspiration and encouragement in the preparation of this
dissertation.
It gives me great pleasure to express my gratitude to Dr. KIRAN
CHOWDARY, Guntur, Dr. PRASAD, M.A.V.V., Nellore
Dr. KUMAR BABU, Nellore and for their valuable guidance and
support in completion of this dissertation.
I humbly express my gratitude to all the orthopaedic faculty and
fellow postgraduates for their immense help in the completion of
this study.
Last but not the least I am grateful to all MMYY PPAATTIIEENNTTSS,, MMYY
PPAARREENNTTSS and TTHHEE AALLMMIIGGHHTTYY for the kindness and co-
operation without whom this study could not have been embarked
upon
Dr. P. NARENDRA REDDY
CONTENTS
1. INTRODUCTION
2. AIM
3. REVIEW OF LITERATURE
4. MATERIALS AND METHODS
5. PROFORMA AND MASTER CHART
6. RESULTS
7. DISCUSSION
8. CONCLUSION
9. SUMMARY
10. BIBILIOGRAPHY
INTRODUCTION

INTRODUCTION
Intertrochanteric fractures are seen with increasing frequency and
severity as the life expectancy of our population increases. The primary goal
in the treatment of an elderly patient with Intertrochanteric fracture is to
return the patient to his / her pre - fracture activity as early as possible.
Rapid mobilization of these elderly patients reduces the morbidity and
mortality rate in geriatric patients.
Before the introduction of suitable fixation devices, treatment of
intertrochanteric fractures was nonoperative, consisting of prolonged bed
rest in traction until fracture healing occurred (usually 10 – 12 weeks ),
followed by a lengthy programme of ambulation training. In elderly patients,
this approach was associated with high complication rates; typical problems
included Decubitus ulcers, Urinary tract infection, Joint contractures,
Pneumonia and Thromboembolic complications, resulting in a high
mortality rate. In addition, fracture healing was generally accompanied by
varus deformity and shortening because of the inability of traction to
effectively counteract the deforming muscular forces.
For these reasons, the treatment of intertrochanteric fracture by
reduction and internal fixation has become the standard method of
treatment.
It is important to understand the principles behind the evolution of the
multitude of implants that have been used to stabilize intertrochanteric
fractures. The first implant to be used with success was Fixed-angle Nail-

plate (e.g., Jewett nail, Holt nail) consisting of Triflanged nail fixed to a
plate at an angle between 1300 and 150
0. Although these devices provided
stabilization of the femoral head and neck fragment to the femoral shaft,
they did not allow fracture impaction. If significant impaction of the fracture
site occurred, the implant would either penetrate into the hip joint or cut out
through the superior portion of the femoral head and neck. 45
(M J Parker) If,
on the other hand, no impaction occurred, lack of bone contact would result
in either plate breakage or separation of the plate and screws from the
femoral shaft. These complications occurred much more frequently when
these devices were used to treat unstable fractures.
The experience with fixed-angle nail plate devices indicated the need
for a device that allowed controlled fracture impaction. This gave rise to
Sliding Nail-Plate devices (e.g., Massie nail, Clawson Ken-Pugh nail), which
consisted of a nail that provided proximal fragment fixation a sideplate that
allowed the ―telescope‖ within a barrel35
Impaction provided bone-on-bone
contact, which promoted fracture union; implant sliding also decreased the
moment arm and stress on the implant, thereby lowering the risk of implant
failure.
The Sliding Nail-Plate devices gave rise to Sliding Hip Screw devices.
The nail portion was replaced by a blunt-ended screw with a large outside
thread diameter. The first author to describe a sliding hip screw device was
Schumpulick W.48
One early modification to the Sliding Hip Screw maximized fracture
impaction by allowing the proximal lag screw to telescope within the plate
barrel and the plate to slide axially along the femoral shaft. To accomplish
this bi-directional sliding, the plate was modified by replacing the round
screw holes with slotted screw holes (Egger’s plate). More recently, a two-
component plate device was introduced (Medoff plate, Medpac, Culver City,
CA)1 in which a central vertical channel constrains an internal sliding
component. Both devices have been used successfully for the treatment of
stable and unstable intertrochanteric fractures.
Intramedullary Sliding Hip Screw devices have recently been
developed for stabilization of pertrochanteric fractures (Gamma nail).3,17
These devices couple a sliding hip screw with a locked intramedullary nail.
However, patients treated with these devices are at increased risk for femoral
shaft fracture at the nail tip and the insertion sites of the distal locking
screws.
Hence, for these various complications associated with other
fixation devices in the treatment of unstable intertrochanteric fractures,
Dynamic Hip Screw Fixation has become the Gold standard treatment.
AIM
AIM
To analyse the results of the intertrochanteric fractures treated by
Dynamic Hip Screw fixation

REVIEW OF LITERATURE
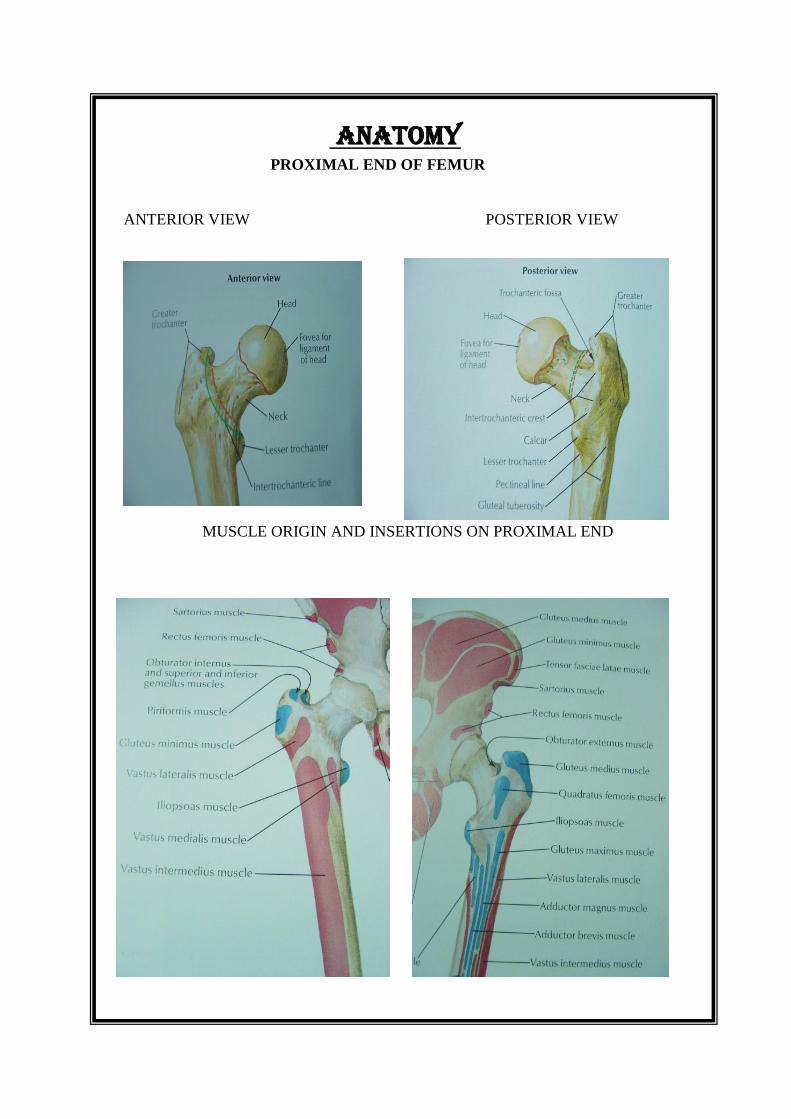
PROXIMAL END OF FEMUR
ANTERIOR VIEW POSTERIOR VIEW
MUSCLE ORIGIN AND INSERTIONS ON PROXIMAL END
ANATOMY

ANATOMY
The upper end of femur includes the head, neck, greater trochanter,
lesser trochanter, intertrochanteric line and intertrochanteric crest.
The femur is the second long bone in the body to start ossifying. The
primary center appears in the shaft during 7th
fetal week. Four secondary
centers, one for lower end appears at the end of ninth month of intrauterine
life, one for head appears during first six months of life and fuses at around
16yrs , one for greater trochanter appears during fourth year and fuses at
around 14yrs, one for lesser trochanter appears during 12 yrs and fuses at
around 13yrs.
HEAD OF THE FEMUR:
It forms more than half of a sphere and is directed medially, upwards
and slightly forward. It articulates with the acetabulam to form the hip
joint. The roughened pit, situated just below and behind
its centre is called the fovea. It provides attachment to the ligament of
head of femur (the round ligament or ligamentum teres).
NECK OF THE FEMUR:
Its about 5 cm long; connects the head of the femur and the shaft with
which it forms an angle of about 1250
and an anteversion of 150 in adults.
The neck shaft angle is less in females due to their wider pelvis.
The neck of the femur is strengthened by calcar femorale along its concave
surface

ANATOMY
LATERAL ASPECT FEMORAL NERVE
LIGAMENTS OF HIP JOINT
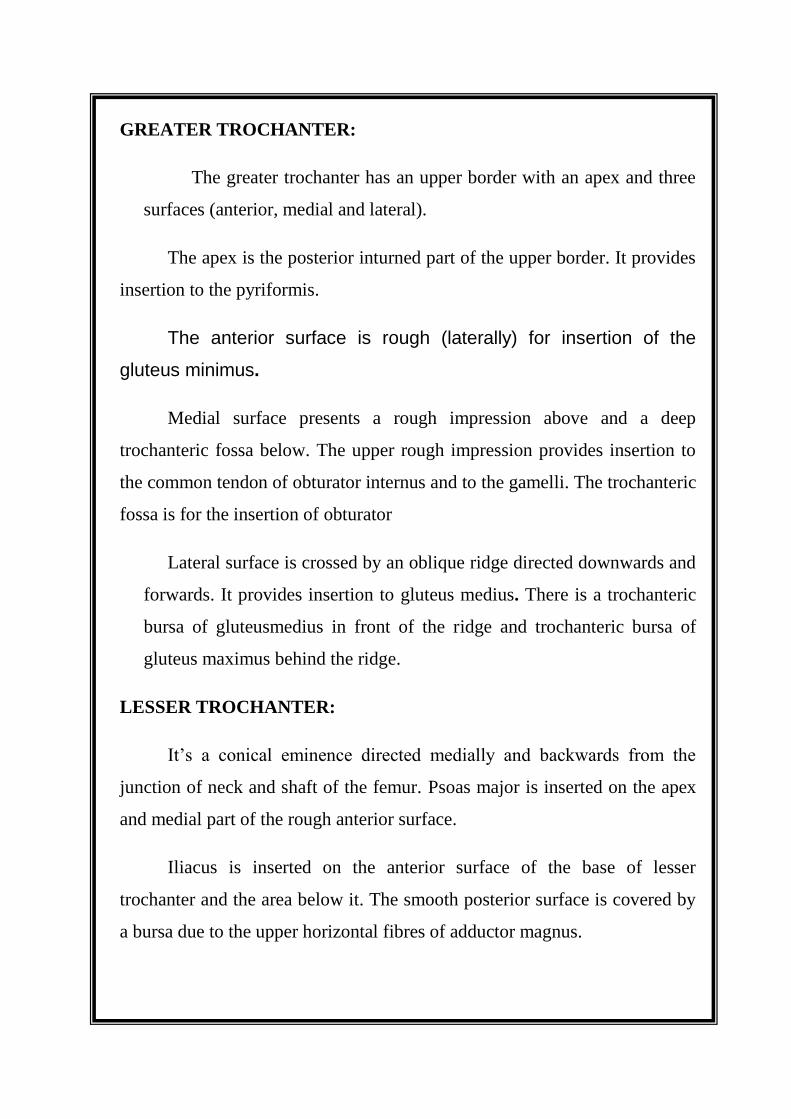
GREATER TROCHANTER:
The greater trochanter has an upper border with an apex and three
surfaces (anterior, medial and lateral).
The apex is the posterior inturned part of the upper border. It provides
insertion to the pyriformis.
The anterior surface is rough (laterally) for insertion of the
gluteus minimus.
Medial surface presents a rough impression above and a deep
trochanteric fossa below. The upper rough impression provides insertion to
the common tendon of obturator internus and to the gamelli. The trochanteric
fossa is for the insertion of obturator
Lateral surface is crossed by an oblique ridge directed downwards and
forwards. It provides insertion to gluteus medius. There is a trochanteric
bursa of gluteusmedius in front of the ridge and trochanteric bursa of
gluteus maximus behind the ridge.
LESSER TROCHANTER:
It’s a conical eminence directed medially and backwards from the
junction of neck and shaft of the femur. Psoas major is inserted on the apex
and medial part of the rough anterior surface.
Iliacus is inserted on the anterior surface of the base of lesser
trochanter and the area below it. The smooth posterior surface is covered by
a bursa due to the upper horizontal fibres of adductor magnus.

INTERTROCHANTERIC LINE:
It marks the junction of anterior surface of the neck with shaft of
femur. It begins above at the antero - superior angle of the greater trochanter
and is continuous below with the spiral line in front of the lesser trochanter.
It provides attachment to,
1. Capsular ligament of the hip joint.
2. Upper band of iliofemoral ligament in upper part.
3. Lower band of iliofemoral ligament in lower part; origin to the
highest fibres of the vastus lateralis from the upper end and the origin
to the highest fibres of vastus medialis from the lower end of the line.
INTERTROCHANTERIC CREST:
This marks the junction of posterior part of neck with shaft of femur.
It begins above at the postero - superior angle of greater trochanter and
ends at the lesser trochanter. The rounded elevation, a little above its
middle is called the QUADRATE TUBERCLE, which provides insertion
to quadratus femoris extending to the area below it
BLOOD SUPPLY:
An extracapsular arterial ring is formed anteriorly by ascending
branch of lateral femoral circumflex artery and posteriorly by medial
circumflex femoral artery. The ascending cervical branch from this ring
pierce the hip capsule near its distal insertion, becoming the retinacular
arteries supply the femoral head. A subsynovial intracapsular arterial ring
enter the femoral head and unite to form the lateral epiphysial arteries.

These lateral epiphyseal arteries supply the majority of femoral head. The
artery of ligamentum teres , a branch of obturator artery supply a small
portion of femoral head around the fovea capitis
BLOOD SUPPLY TO HEAD OF THE FEMUR
TRABECULAR PATTERN

NUTRIENT ARTERY
This is derived from second perforating artery. In case of absence it is
replaced by two nutrient arteries derived from first and third perforating
arterie . The nutrient foramen is located on the medial side of the linea
aspera and is directed upwards.
TRABECULAR PATTERN:
The trabecular architecture of the proximal end of femur
comprises of 5 distinct groups
1) Principal compression trabeculae- there run from the weight
bearing portion of the femoral head to the region of the calcar
femoris and the medial cortex.
2) Principal tension trabeculae - there begin in the inferior portion of
the head and arch across the superior portion ,terminating in the
lateral cortex
3) Trochanteric trabeculae- these begin in the greater trochanter and
end in the lateral cortex
4) Secondary compression trabeculae
5) Secondary tension trabeculae - these are found between primary
trabeculae and act as tie beams.
The primary tensile and compression trabeculae, resist tensile and
compression stress respectively. Trabecular bone is concentrated as
thin layer deep to the subchondral bone
CLASSIFICATION
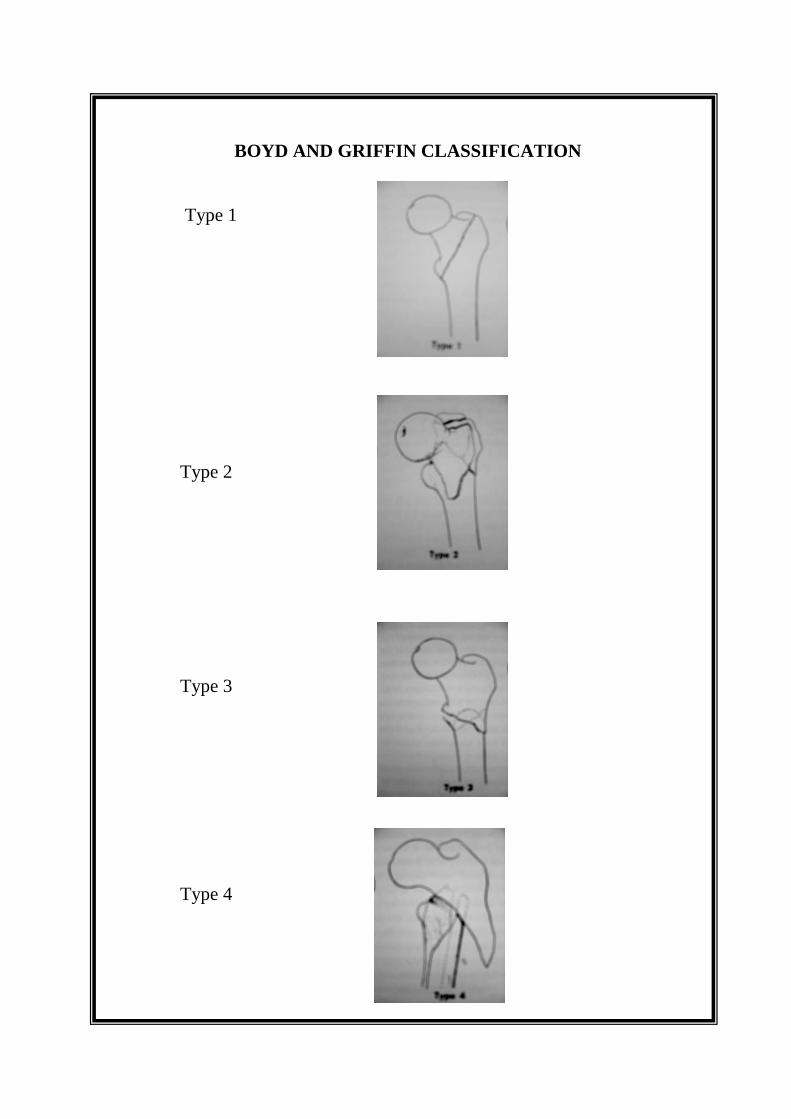
BOYD AND GRIFFIN CLASSIFICATION
Type 1
Type 2
Type 3
Type 4
CLASSIFICATION
A number of classifications of trochanteric fractures are recorded in the
literature. No standard classification is universally accepted. Stuck,(using
Boehler’s classification) Moore, Brigg’s and Keats and others classified
trochanteric fractures primarily from an anatomical standpoint.
Boyd and Griffin (1949) classified fractures in the trochanteric area
of femur into 4 types13
. Their classification included all fractures from
extracapsular part of the neck to a point 5 cm distal to the lesser trochanter.
Their classification is useful in planning treatment and estimating prognosis.
TYPE-1:
Fractures extending along the intertrochanteric line from the greater to
lesser trochanter
TYPE - 2 :
Comminuted fractures, the main fracture being along the
intertrochanteric line but with multiple fractures in the cortex
TYPE - 3 :
Fractures that are basically sub -trochanteric with at least one fracture
passing across the proximal end of the shaft just distal to or at the lesser
trochanter; Varying degrees of comminution are associated.
TYPE - 4 :
Fractures of the trochanteric region and proximal shaft with fractures
in at least 2 planes
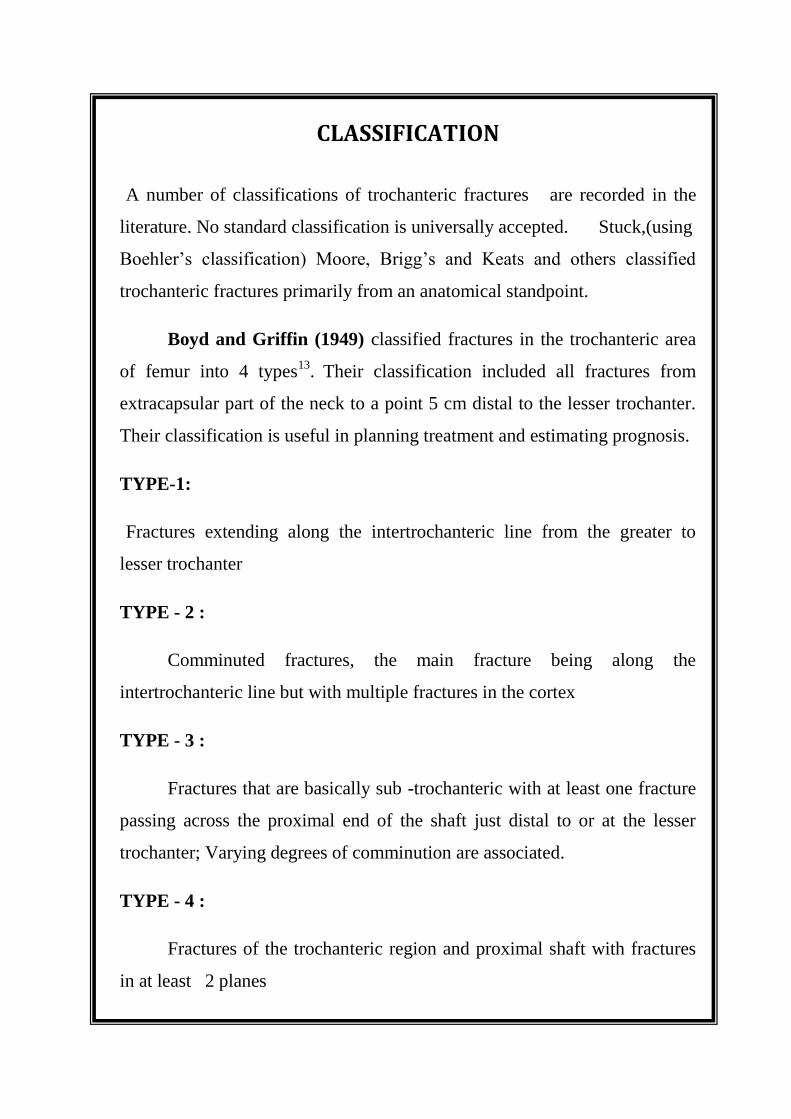
EVAN’S CLASSIFICATION
STABLE
UNSTABLE
EVAN’S CLASSIFICATION:
Evan presented a simpler classification based on dividing fractures
into stable and unstable groups.21
He further divided the unstable into those
in which stability could be restored by anatomic or near anatomic reduction
and in those in which anatomic reduction would not create stability.
TYPE - 1 :
The fracture line extends upwards and outwards from the lesser
trochanter and there are 4 sub divisions.
In the first group, comprising 65% of all cases, the inner cortical
buttress has never been disturbed. There is no displacement and fractures
unite in perfect position.
In the second group, simple overlap of the inner cortical buttress can
be reduced by manipulation and the fracture thus becomes stable.
In the third and fourth group, there is unreduced overlap or destruction
of this cortical buttress and coxa vara deformity is to be expected.
TYPE - 2 :
The obliquity of major fracture line is reversed, that is it extends
outward and downward from the lesser trochanter. There is marked tendency
to inward displacement of the femoral shaft but this does not affect the
ultimate function.
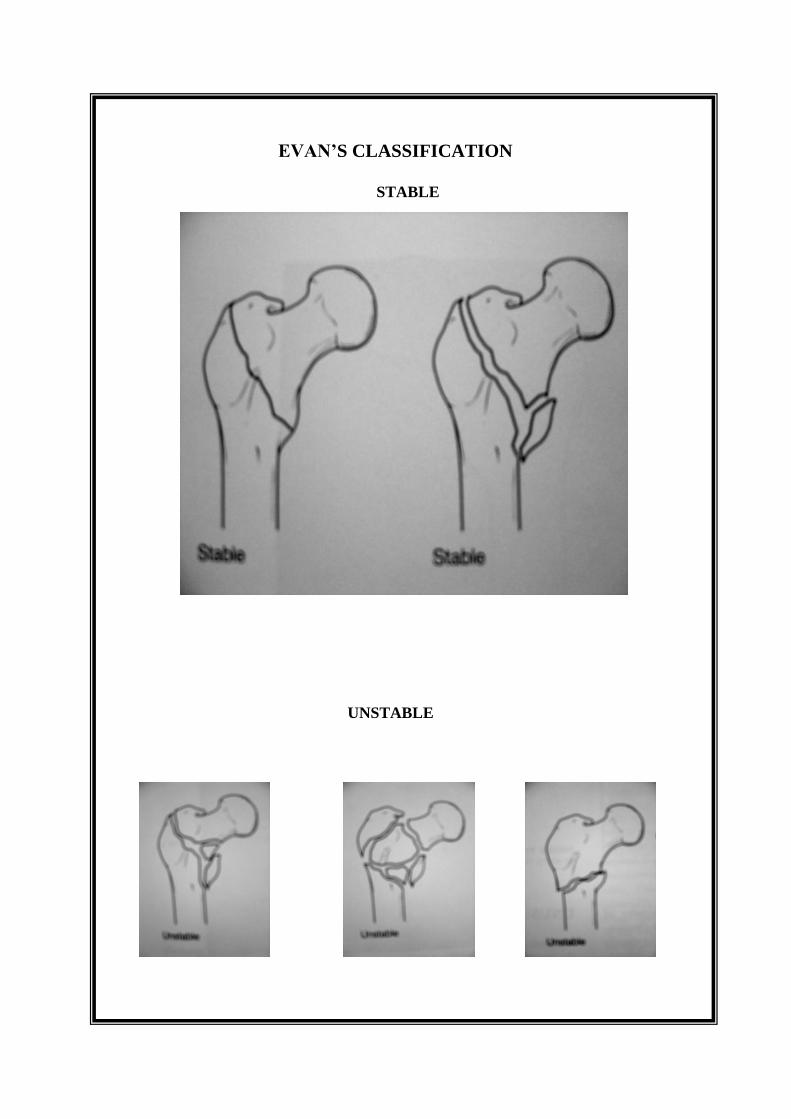
KYLE CLASSIFICATION
TYPE 1 TYPE 2
TYPE 3 TYPE 4
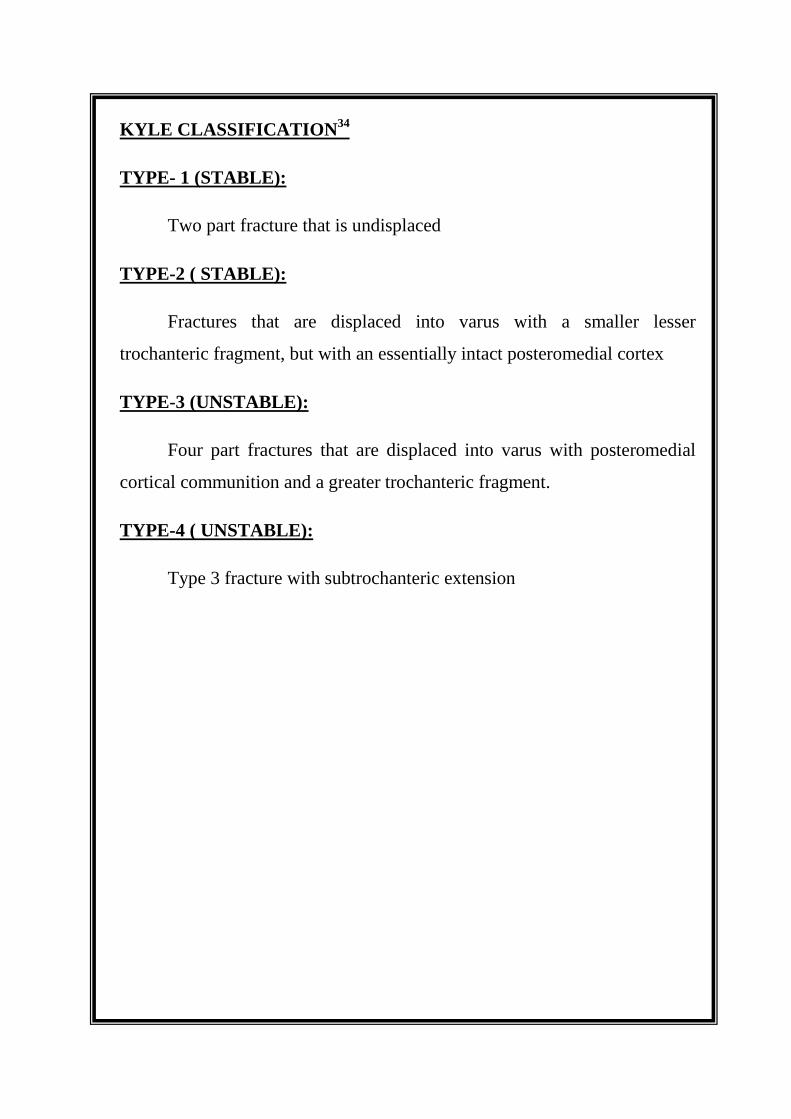
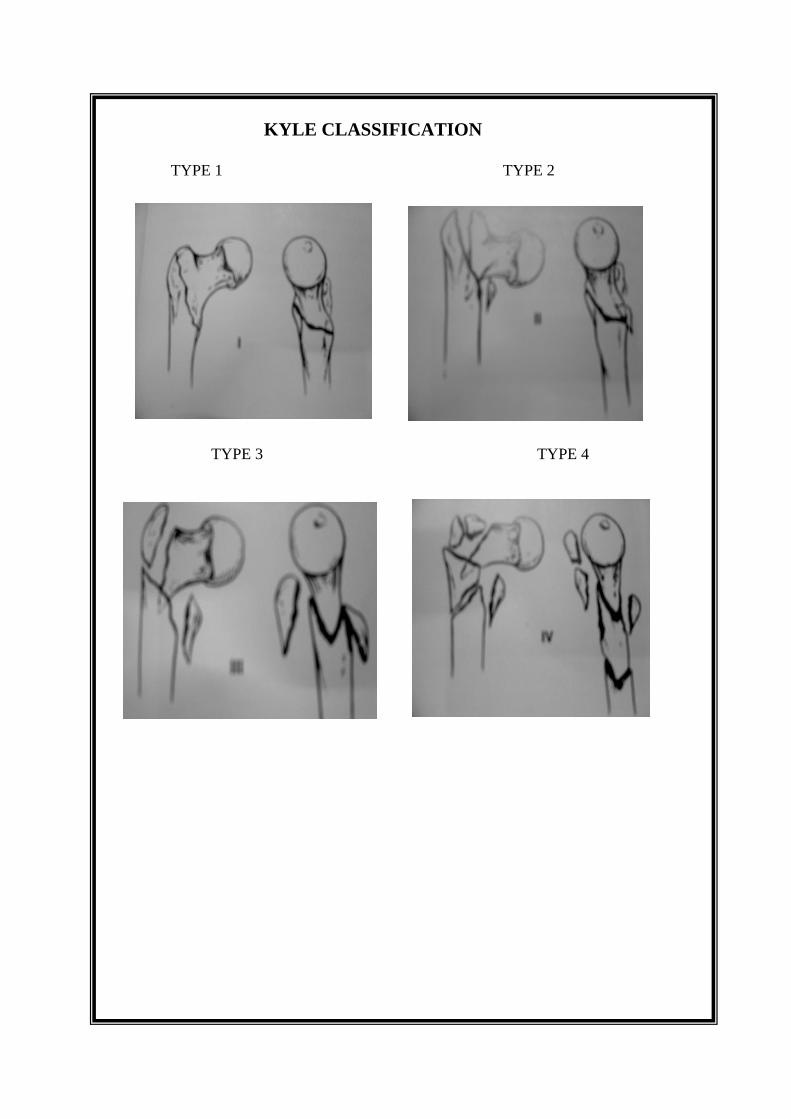
KYLE CLASSIFICATION
34
TYPE- 1 (STABLE):
Two part fracture that is undisplaced
TYPE-2 ( STABLE):
Fractures that are displaced into varus with a smaller lesser
trochanteric fragment, but with an essentially intact posteromedial cortex
TYPE-3 (UNSTABLE):
Four part fractures that are displaced into varus with posteromedial
cortical communition and a greater trochanteric fragment.
TYPE-4 ( UNSTABLE):
Type 3 fracture with subtrochanteric extension

TRONZO
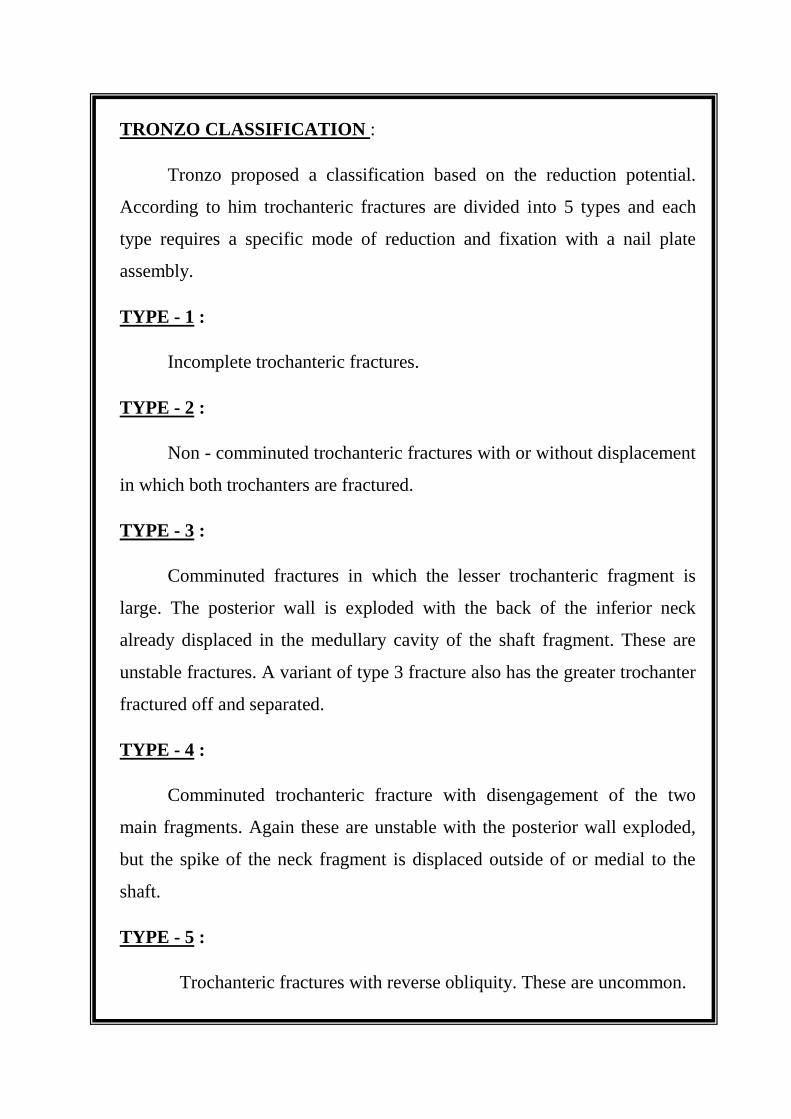
TRONZO CLASSIFICATION :
Tronzo proposed a classification based on the reduction potential.
According to him trochanteric fractures are divided into 5 types and each
type requires a specific mode of reduction and fixation with a nail plate
assembly.
TYPE - 1 :
Incomplete trochanteric fractures.
TYPE - 2 :
Non - comminuted trochanteric fractures with or without displacement
in which both trochanters are fractured.
TYPE - 3 :
Comminuted fractures in which the lesser trochanteric fragment is
large. The posterior wall is exploded with the back of the inferior neck
already displaced in the medullary cavity of the shaft fragment. These are
unstable fractures. A variant of type 3 fracture also has the greater trochanter
fractured off and separated.
TYPE - 4 :
Comminuted trochanteric fracture with disengagement of the two
main fragments. Again these are unstable with the posterior wall exploded,
but the spike of the neck fragment is displaced outside of or medial to the
shaft.
TYPE - 5 :
Trochanteric fractures with reverse obliquity. These are uncommon.

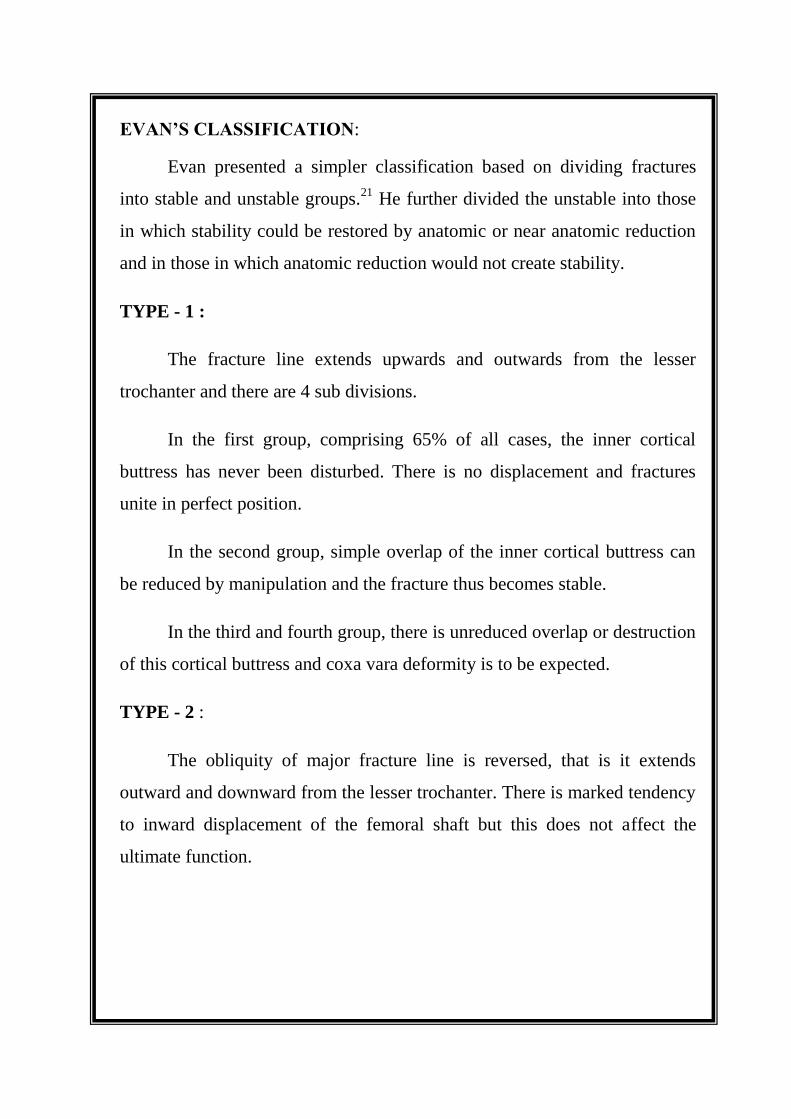
AO CLASSIFICATION
Type 1
A1.1 A1.2 A1.3
Type 2
A2.1 A2.2 A2.3
Type 3
A3.1 A3.2 A3.3
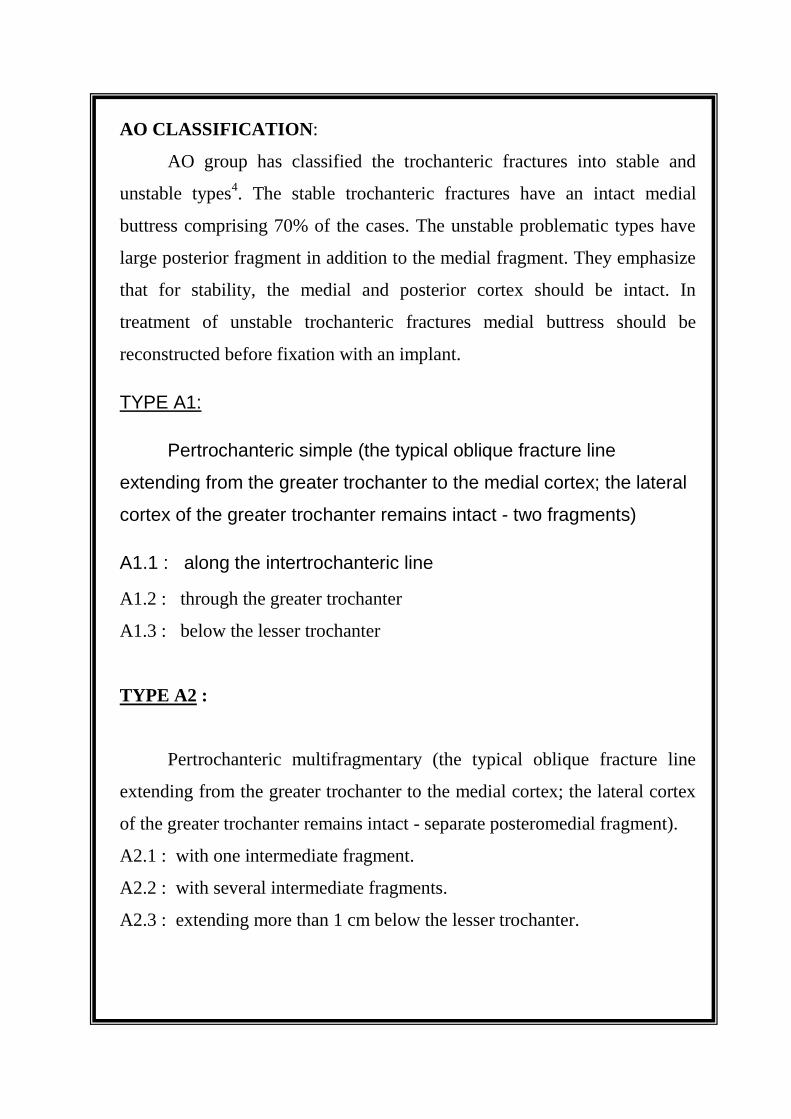
AO CLASSIFICATION:
AO group has classified the trochanteric fractures into stable and
unstable types4. The stable trochanteric fractures have an intact medial
buttress comprising 70% of the cases. The unstable problematic types have
large posterior fragment in addition to the medial fragment. They emphasize
that for stability, the medial and posterior cortex should be intact. In
treatment of unstable trochanteric fractures medial buttress should be
reconstructed before fixation with an implant.
TYPE A1:
Pertrochanteric simple (the typical oblique fracture line
extending from the greater trochanter to the medial cortex; the lateral
cortex of the greater trochanter remains intact - two fragments)
A1.1 : along the intertrochanteric line
A1.2 : through the greater trochanter
A1.3 : below the lesser trochanter
TYPE A2 :
Pertrochanteric multifragmentary (the typical oblique fracture line
extending from the greater trochanter to the medial cortex; the lateral cortex
of the greater trochanter remains intact - separate posteromedial fragment).
A2.1 : with one intermediate fragment.
A2.2 : with several intermediate fragments.
A2.3 : extending more than 1 cm below the lesser trochanter.
TYPE A3 :
Intertrochanteric fracture line extends across both the medial and
lateral cortices.
A3.1 : simple oblique ( reverse obliquity pattern ).
A3.2 : simple transverse.
A3.3 : multifragmentary.
STABLE INTERTROCHANTERIC FRACTURES:
A) The fracture runs from the greater trochanter obliquely downwards
and medially to exit just above the lesser trochanter. A good portion of
the calcar is attached to the proximal fragment anteromedially. Quite
commonly there is an avulsion fracture of the lesser trochanter. As a
rule the distal fragment is in external rotation. Rarely, the inferomedial
spike of the proximal fragment is impacted into the metaphysis of
proximal fragment.
B) An avulsion does not result in instability because it does not weaken
the medial buttress.
AUNSTABLE INTERTROCHANTERIC FRACTURES:
A) The medial fragment varies in size and reaches distally to a varying
degree. As a rule it contains the lesser trochanter. If the lateral wall
remains intact then the distal fragment migrates proximally because of
muscle pull. Commonly there is in addition quite a large posterior
fragment. Occasionally, the proximal fragment contains a long medial
spike made up of calcar and lesser trochanter. This makes it into a
long oblique or spiral fracture.
B) If the greater trochanter is fractured then the distal fragment is not
pulled upwards.
C) A badly comminuted intertrochanteric fracture has in addition to the
fractures of the lesser and greater trochanters further comminution
posteriorly and medially.
D) The intertrochanteric fracture is almost horizontal. Often one finds this
fracture associated laterally with a further anterior or posterior
fragment and occasionally both.
E) Occasionally the fracture has a reverse course beginning laterally and
distally and running upwards and medially. Medially it exits above the
lesser trochanter. Commonly it is associated with a fracture of the
greater trochanter.
HISTORICAL REVIEW
HISTORICAL REVIEW
Internal fixation in treatment of intertrochanteric fractures has gained
world wide acceptance.
From antiquity, the general apporach to these fractures consisted of
various methods of closed reduction and immobilisation.
Although, Von Langenbeck first reported an open reduction and
internal fixation of a fractured hip in 1878,28
it was only Smith Peterson's
refinement of the surgical approach and introduction of the Triflanged nail
some 40 years later that operative treatment became a practical alternative47
.
The problems and disadvantages of fixation by wires, threaded wires pins
and screw apparatuses rapidly forced it into the discard. Additions, deletions
and modifications to this armamentarium followed clinical trails in an
attempt to correct evident shortcomings in fixation.
In 1937, Thornton devised a plate attachment for the
S.P. Triflanged nail so that trochanteric fractures could be suitably fixed. 39
In 1941, Jewett developed a welded, single piece, angled nail. The Jewett
nail with a few minor structural changes has proven acceptable.31
A
simplification in design in the form of a "V" nail was introduced in 1944 by
Neufeld.
In the same year Austin Moore designed his blade plate for
trochanteric fractures but its use was short lived, for this fracture at least,
because of the superiority of other nails. In 1947, McLaughlin engineered a
variable angle nail plate, the advantage of which was the ease of adaptation
of the plate to the femoral shaft after the nail has been driven in.

In 1940, Godey - Moreira reported 10 fractures treated with a
cannulated "stut bolt screw" which impacted the fragments. Perfect results
were obtained in 7 of the 8 patients followed.
In 1955, Schumpelich and Jantzen described the use of a Sliding
Screw, the design of which they attributed to Ernst Pohl. Callender modified
the device further and it was used by Harrington and Johnson in a series of
unstable intertrochanteric fractures.47
In 1964, Clawson reported on the treatment of trochanteric fractures
using a Sliding Screw and plate.16
The device was developed independently
by the Richards' manufacturing company. Clawson made several further
modifications and in its current form the device is known as Richards'
Compression Hip Screw. 18
In recent years, the Sliding Hip Compression Screw system (Richards,
Zimmer, etc.) has become a widely used method of internal fixation for
trochanteric fractures.
This stabilisation of trochanteric fractures by remotely introduced
medullary implants was first recommended by Lezius, Kuentscher and later
Simon Weidner and especially Ender advanced in this direction and refined
this method.50
Since the development of AO Osteosynthesis technique many
orthopaedic units have added this versatile system to their armamentarium.
The Percutaneous compression plating system 33,52
is a new method in
managing trochanteric fractures which is composed of a plate, two
telescoping neck screws and three shaft screws. The plate is specially
designed to allow it to pass through soft tissue and to glide along the femoral
shaft. The system permits percutaneous screw fixation and fracture
compression.
In 2000 Elder S, Frankenburg E20
has introduced calcium phosphate
cement augumented fixation of osteoporotic unstable intertrochanteric
fractures
In 2002 Janzing HM,30
Huben B,J stated that percutaneous compression
plating system in peritrochanteric fractures of hip is a minimal invasive
technique with reduced operative time and postoperative pain than fixation
of sliding hip screw
In 2003 Hardy DC26
stated that sloted intramedullary hip screw nail
reduces proximal mechanical unlodindg on the femur
In 2006 N K Karn,44
G K singh proposed that external fixator in the
treatment of intertrochanrtic fracture needs less amout of operative time,
blood loss is minimal with mimal amount of shortening when compared to
sliding hip screw
In 200751
Yechiel Gotfried proposed that integrity of lateral femoral
wall in intertrochanteric hip fractures is predictor for reoperation in
peritrochanteric hip fractures
In 2008 Ricci46
, William M proposed that new implant designs for
intramedullary nails and for external fixation have recently challenged
compression hip screw as a best metyhod of treatment for intertrochanteric
fractures. External fixator as a result of new advances in its desigs like
reduced pintract infections and improved pin fixation strength has recently
shown to be reasonable alternative treatment option
The long list of devices that have been used to stabilize these fractures
is a testimonial to the fact that many did not work well. Thus there are
continuing attempts to improve both the design and materials of fixation
devices.
BIOMECHANICS OF INTERTROCHANTERICFRECTURES
BIOMECHANICS OF
INTER TROCHANTERIC FRACTURES
Operative treatment of intertrochanteric hip fractures with
internal fixation creates a fracture fragment – implant assembly
intended to withstand the forces acting on the fracture site. Since
avoiding recumbency is often the goal of internal fixation and
since many patients with trochanteric hip fractures lack the
balance, co- ordination and ability to avoid weight bearing upon
the fractured femur, it is often necessary that the fracture
fragment implant assembly be strong enough to withstand the
body weight and the very considerable muscle forces which act
on the trochanteric region of femur. These forces have been
shown to be equivalent to as much as three times the body
weight acting upon the femoral head.
Creating a fracture fragment – implant assembly capable of
withstanding loads of this magnitude is the bio - mechanical goal of the
surgeon who elects upon the operative treatments of intertrochanteric
fractures. Strength of the fracture fragment implant is determined by 5
independent variables. (Kaufer et al)
1 . Bone quality
2 . Fragment geometry
3 . Reduction
4 . Implant
5 . Implant placement.
BONE QUALITY:
The mechanical properties of bone (hardness, elasticity, strength,
etc) vary considerably depending upon age, sex, race, general state of
health, muscle mass, and level of activity. Bone strength varies in
different bones in same individual as well as in different areas in the
same bone.
Most of the unstable intertrochanteric fractures are relatively low
trauma injuries occurring in atrophic, osteoporotic or osteomalacic
bones. Singh has developed a roentgenographic method for determining
bone strength which is based upon the trabacular pattern of the proximal
femur.
FRAGMENT GEOMETRY:
Much clinical attention is focussed upon the number, size,
location and displacement of trochanteric fracture fragment.
Comminution, especially if it involves the posterior and medial portion
of the trochanteric region is recognized as a major factor contributing to
the complications of fixation. Multiple fragment fracture with
comminution extending into the medial and posterior femoral cortex is
far more likely to displace into varus and retro version. Fractures with
posterior and medial cortical comminution are therefore considered
unstable, while two parts trochanteric fractures are far more likely to be
stable.
Although reduction and inter fragmentary fixation of the lesser
fragment of a comminuted unstable intertrochanteric fractures can
contribute to the stability of the post fixation assembly , in practice ,
inter fragmentary fixation is time consuming, frequently disappointing
and may contribute to infection and other biological complications of
operative treatment. It is therefore generally agreed that one should
ignore the lesser fragments and concentrate on gaining stable fixation of
the major proximal fragment to the major distal fragment attaining
postero - medial cortical contact.
REDUCTION:
An unstable reduction is one in which there is insufficient contact
between the fragment to contribute to the post reduction integrity of the
proximal femur. Post fixation strength of an unstable fracture reduction
depends entirely upon the mechanical characteristics of the implant.
Stable reduction of a unstable intertrochantic fracture provides
sufficient medial and posterior cortical contact between the major
proximal fracture fragment and the major distal fragment to resist the
varus and the posterior distilling forces which predominate in these
fracture. Stable reduction contributes significantly to the strength of the
post fixation assembly.
Restoration of normal anatomy is the goal of all fracture
treatment. Cadaveric studies of unstable intertrochanteric fractures
stabilized with anatomic reduction, showed optimal stress distribution
(highest compression strain in the medial cortex and lowest strain on the
side plate).
Reduction and fixation of the postero medial fragment depends on
the size of the fragment. Anatomic reduction of a large postero medial
fragment increase the load resistance by 57 % whereas fixation of a
small postero medial fragment increase the stability only by 17%.
(Apel et al)

However, anatomic reduction of unstable intertrochanteric
fracture can be difficulty to achieve and is associated with a prohibitive
frequency of complication of fixation. Recognition of this problem has
stimulated recent interest in non – anatomical stable reduction. Of these,
the medial displacement reduction advocated by Dimon and Hughston
first described Rowe was most popular.
There is however no evidence to suggest that medial displacement
is mechanically superior to a perfect anatomic reduction. Non
anatomical reduction should therefore be reserved for those fractures in
which perfect anatomic reduction cannot be achieved.
Valgus reduction markedly decreases joint reaction force
moment arm and can markedly increase the fracture to varus deformity.
However, severe degrees valgus should be avoided because it demands
increased abductor muscle power to stabilize the pelvis during single leg
stance and increase the joint reaction force. Valgus reduction may
therefore contribute to an abductor limp or post traumatic arthiritis.
IMPLANTS:
Sliding hip screw includes traditional compression hip screw that
provide compression in the intertrochanteric plane and compression
plate that provide additional compression axially.
Sliding hip screws are available with plate angles from 1250 -
1550. 135
0 and 150
0 devices are more commonly used.

Even though the 1500 plates are preferable because the angle of
the lag screw more closely parallel with the compression forces within
the femoral neck and hence less chances of failure of implant due to
bending force, in clinical studies there is no difference in the
compression ability between 1350 hip compression screws and 150
0
devices.
Considering the problem of insertion of 1500 devices into the
center of the femoral head with more distal entry point below the lesser
trochanter, the higher angled plates are only rarely indicated for
extremely valgus femoral neck fractures and more distal fractures.
Moreover, 1350 devices are easily placed and their clinical results are
similar to those for the 1500 plates. Hence 135
0 devices are more
frequently used.
Depending upon the length of the measured sliding hip screw,
either short or long barrelled plate devices are used. Long barrelled
plates are used when the length of the measured sliding hip screw is
more than 85 mm.
NAIL PLACEMENT:
Optimal implant placement is determined by the distribution of
good bone within the proximal fragment as well as the net sum of force
vectors acting upon it. Telescoping implants are least likely to penetrate
into the joint and may therefore be inserted more deeply into the
proximal fragment, thus affording maximal proximal fragment control.

The center of pressure acting upon the femoral head lies within
the head’s antero-superior quadrant. It is therefore best to place the
fixation device in the postero-inferior quadrant of the head of the femur
so that the device must plough through the maximal quality of bone
before it cuts out.
Depth of screw insertion is always a compromise. Based upon a
consensus of laboratory and clinical data, the ideal position of screw
must be within 10 mm. from the subchondral cortex and in the postero-
inferior quadrant of the head of the femur.36
This position places the tip
of the implant into bone formed by the decussation of the tension and
compression trabaculae, thus assuming maximal proximal fragment
control. One of the major advantages of a telescoping device with a
blunt end is the ability to insert it close to the subchondral cortex of the
femoral head with minimal risk of joint penetration within the limits of
technical skill, implant placement is the surgeon’s choice.
Of the 5 determinants of trochanteric fracture fixation stability,
bone quality and fragment geometry are of great importance but are
entirely the product of the patient and the trauma which cannot be
modified by the treating Surgeon. Reduction, implant placement and
implant selection represent the Surgeon’s choice. The implant selection
and placement are of relatively greater importance than reduction.
MATERIALS AND METHODS

MATERIALS AND METHODS
Study has been conducted at VIJAYA HOSPITAL AND
ST.JOSEPH’s HOSPITAL, NELLORE during the period from June
2008 to December 2010. 30 patients with intertrochanteric fractures
treated with DHS fixation were selected for the study, of which
2 patients expired after the 6th month post operatively due to age factor
and other co-morbid conditions.
Hence the total number of patients included in the study was 28 patients.
The follow up period ranges from 6 months to 2 1/2 years.
INCLUSSION CRITERIA
. Intertrochanteric fractures in adults
. Stable intertrochanteric fractures
.Unstable intertrochanteric fractures
EXCLUSION CRITERIA
. Compound fractures
.pathological fracture
.Fractures in children
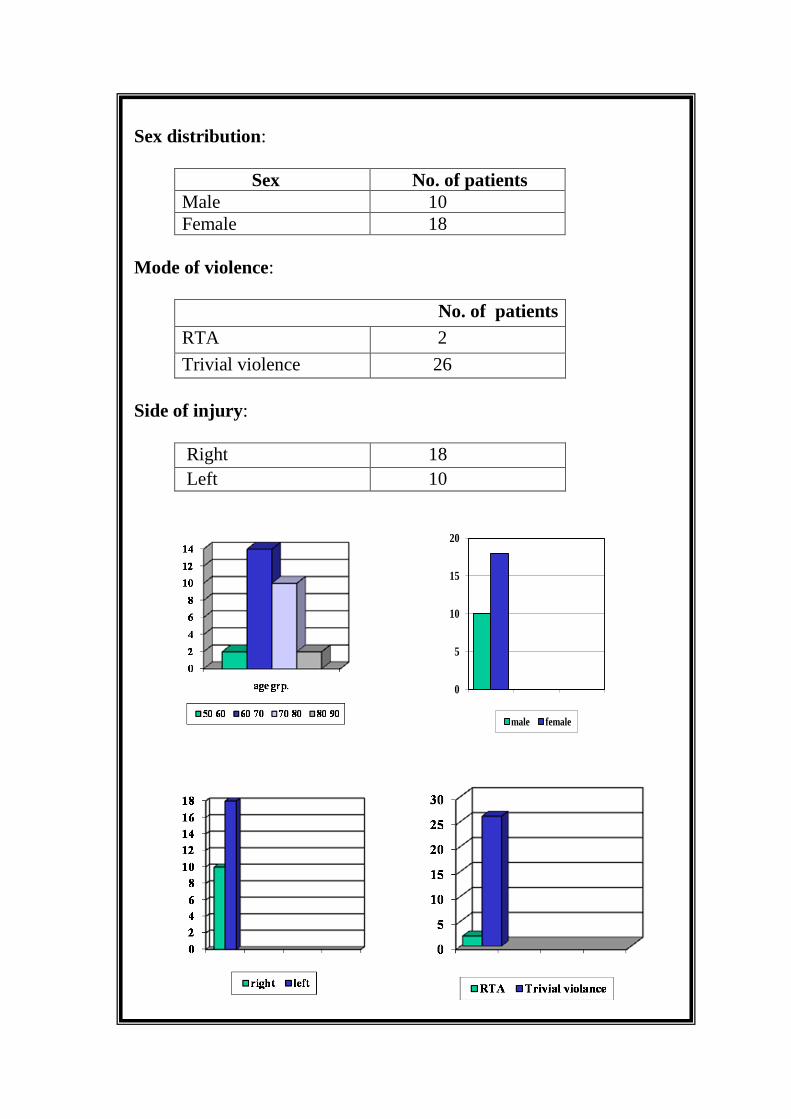
Age distribution:
Majority of the patients were in the 7th and 8
th decade of life.
Age No. of Patients
< 60 2
60 –70 14
70 –80 10
80 –90 2
0
5
10
15
20
male female
Sex distribution:
Sex No. of patients
Male 10
Female 18
Mode of violence:
No. of patients
RTA 2
Trivial violence 26
Side of injury:
Right 18
Left 10

Type of fracture:
BOYD & GRIFFIN classification:
TYPE-1------------- 03
TYPE-2--------------12
TYPE-3-------------- 05
TYPE-4-------------- 08

Associated injuries:
One patient had fracture neck of femur on opposite side
previously for which Hemiarthroplasty was done.
2 patients had ipsilateral Colles’ fractures which were managed
conservatively.
Associated medical problems:
Diabetes mellitus - 13 patients
Hypertension - 11 patients
IHD - 04 patients
Initial management:
Initiall to start with all the patients were put on skin traction on
admission.
Average time interval between admission and surgery was 8.5
(range 7– 10) days during which period patients were evaluated for
medical problems.
Spinal anesthesia was given for all the patients.
C-arm and fracture table were used for all the patients.
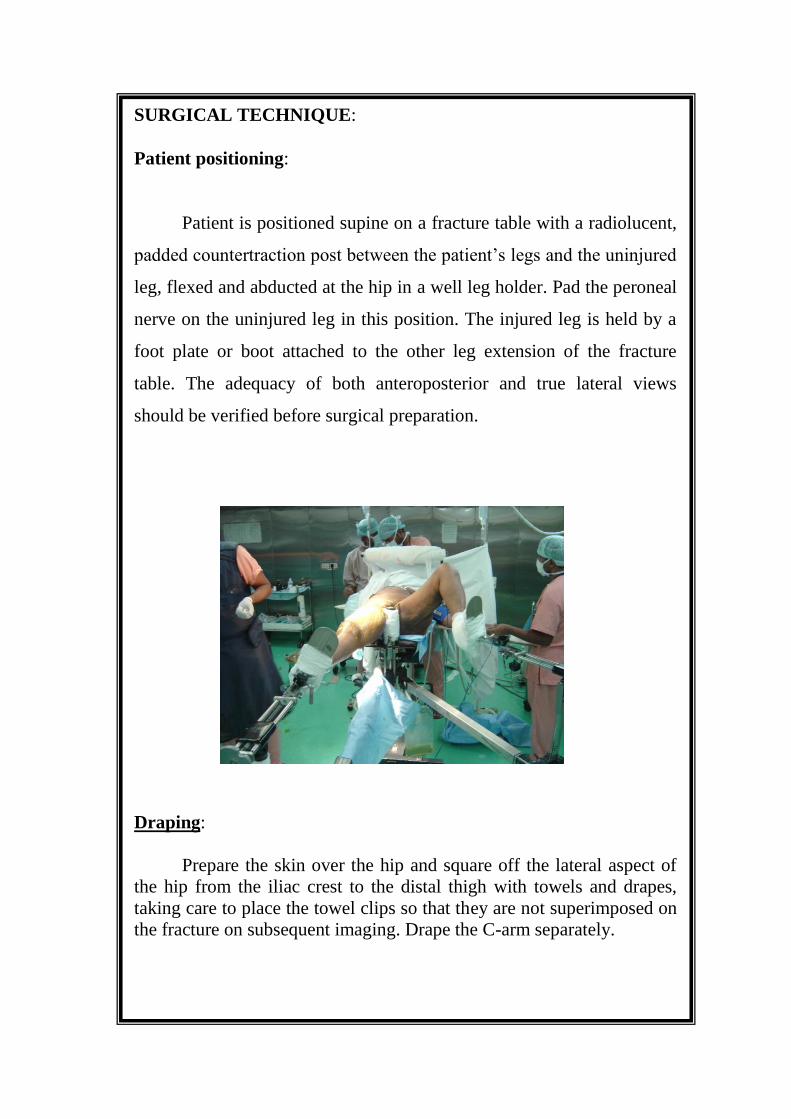
SURGICAL TECHNIQUE:
Patient positioning:
Patient is positioned supine on a fracture table with a radiolucent,
padded countertraction post between the patient’s legs and the uninjured
leg, flexed and abducted at the hip in a well leg holder. Pad the peroneal
nerve on the uninjured leg in this position. The injured leg is held by a
foot plate or boot attached to the other leg extension of the fracture
table. The adequacy of both anteroposterior and true lateral views
should be verified before surgical preparation.
Draping:
Prepare the skin over the hip and square off the lateral aspect of
the hip from the iliac crest to the distal thigh with towels and drapes,
taking care to place the towel clips so that they are not superimposed on
the fracture on subsequent imaging. Drape the C-arm separately.

Reduction technique:
Perform a closed reduction of the fracture. Generally, the fracture
can be reduced in neutral or slight internal rotation. Avoid too much
traction, which may cause valgus overreduction. Check for the reduction
by anterioposterior and lateral roentgenograms or by image intensifier,
paying special attention to cortical contact medially and posteriorly.
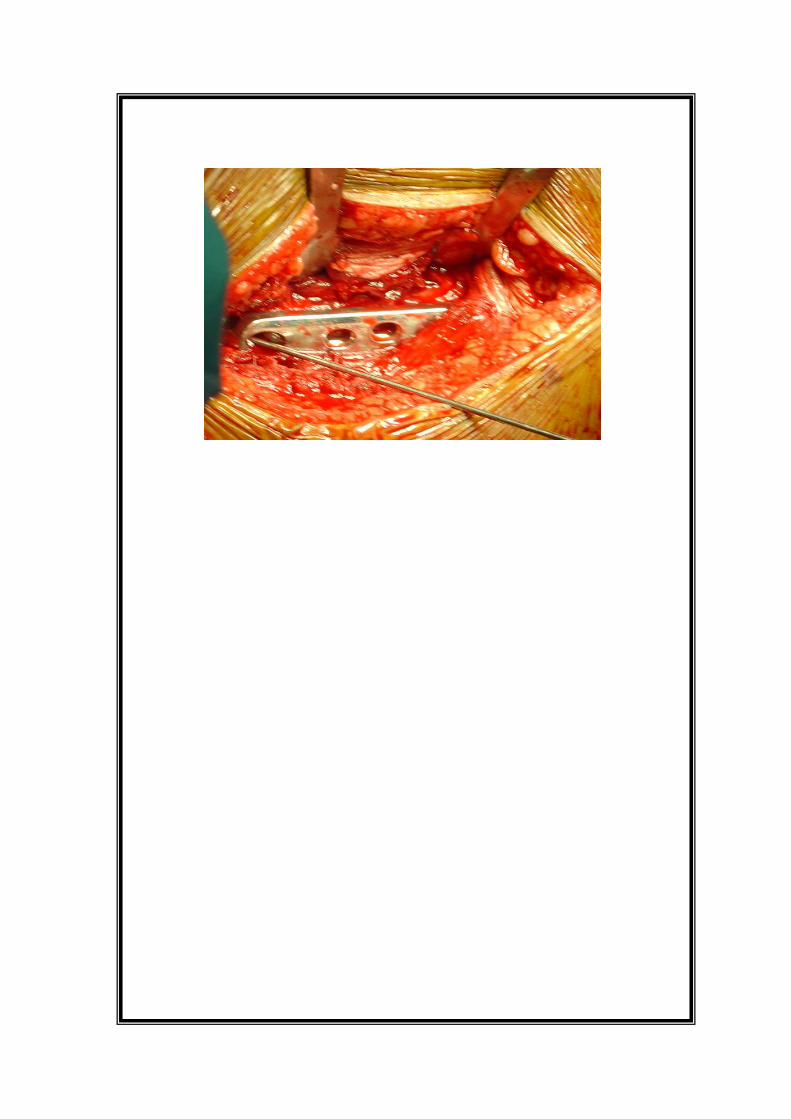
Exposure:
Skin incision is made from 5 cm above the tip of the greater
trochanter passing through center of tip of the greater trochanter and
extend down the line of shaft of the femur for approximately 8 cm.
Incise the fat and underlying deep fascia, retract the cut edges of the
fascia to pull the tensor fascia lata anteriorly. Split the fibres of vastus
lateralis along its line of fibres and elevate it from the lateral inter
muscular septum taking care to coagulate perforating branches of the
profunda femoris artery.
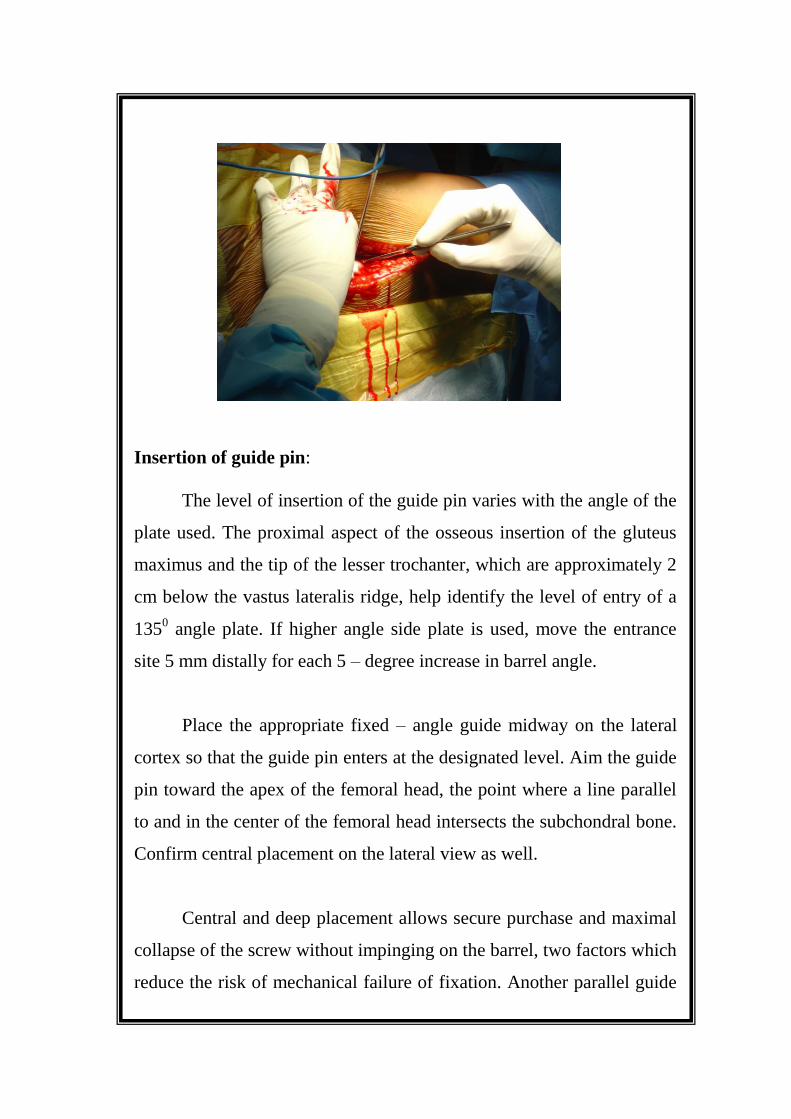
Insertion of guide pin:
The level of insertion of the guide pin varies with the angle of the
plate used. The proximal aspect of the osseous insertion of the gluteus
maximus and the tip of the lesser trochanter, which are approximately 2
cm below the vastus lateralis ridge, help identify the level of entry of a
1350 angle plate. If higher angle side plate is used, move the entrance
site 5 mm distally for each 5 – degree increase in barrel angle.
Place the appropriate fixed – angle guide midway on the lateral
cortex so that the guide pin enters at the designated level. Aim the guide
pin toward the apex of the femoral head, the point where a line parallel
to and in the center of the femoral head intersects the subchondral bone.
Confirm central placement on the lateral view as well.
Central and deep placement allows secure purchase and maximal
collapse of the screw without impinging on the barrel, two factors which
reduce the risk of mechanical failure of fixation. Another parallel guide

pin is inserted to provide temporary stability for unstable fractures, in
which the reduction can be lost if the guide pin backs out after reaming.
Reaming of femur:
Once the guide pin has been inserted and measured, advance it an
additional 5 mm into the subchondral bone, ream according to the exact
measurement of the lag screw length, and choose a lag screw that
matches the length measurement. As an alternative, insert the guide pin
into the subchondral bone, measure and set the reamer 5 mm shorter
than the length measured. Choose a lag screw that matches the length
reamed.
Set the power combination reamer to the lag screw length
indicated by the measuring gauge and ream until the distal aspect of the
positive stop reaches the lateral cortex.
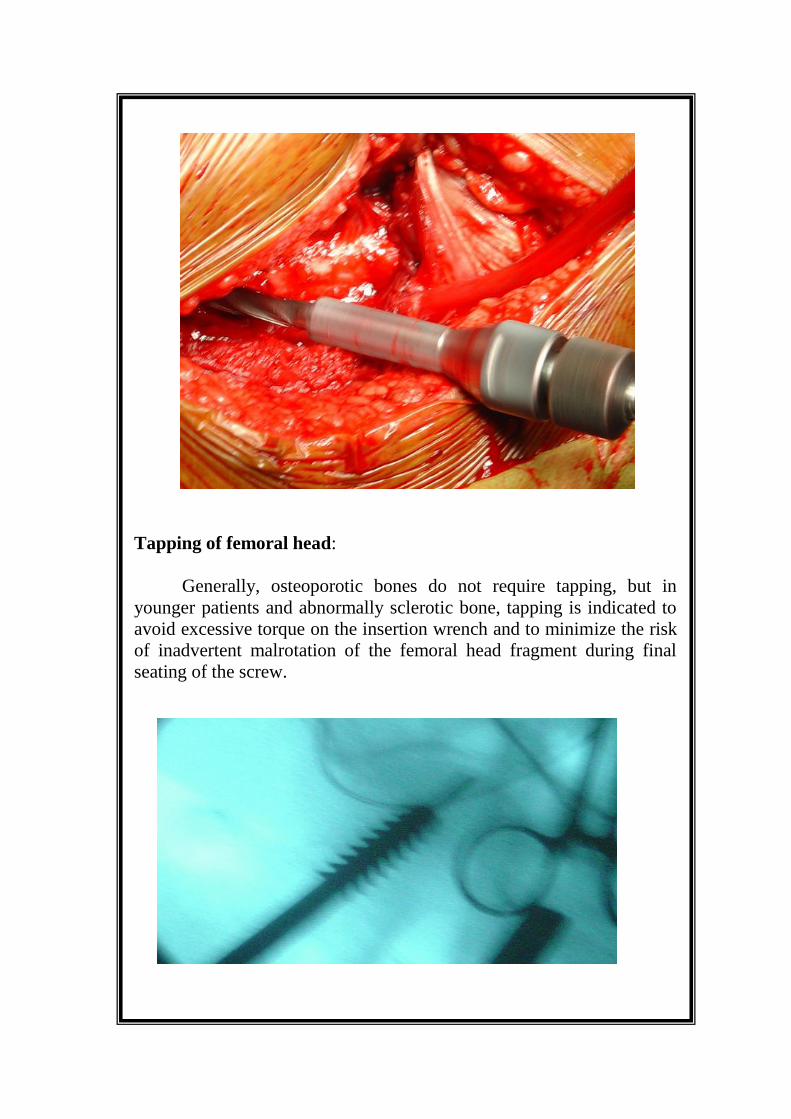
Tapping of femoral head:
Generally, osteoporotic bones do not require tapping, but in
younger patients and abnormally sclerotic bone, tapping is indicated to
avoid excessive torque on the insertion wrench and to minimize the risk
of inadvertent malrotation of the femoral head fragment during final
seating of the screw.

Selection of Lag Screw:
A fully inserted Lag screw that equals the measured length will
allow 5 mm of compression when the compression screw is used or 5
mm of fracture collapse. A 5 mm shorter Lag screw will allow an
additional 5 mm of compression. Do not use a screw that is more than
10 mm shorter than indicated by the measuring gauge or the screw may
be insufficiently covered within the barrel. This may inhibit the screw
from sliding within the barrel.
Insertion of plate and lag screw:
Assemble the appropriate plate and Lag screw onto the insertion
wrench. Screw the Lag screw retaining rod into the distal end of the Lag
screw until a firm connection is obtained. Place the entire assembly over
he guide pin and introduce it into the reamed hole. Advance the Lag
screw into the proximal femur to the predetermined level and verify its
position with image intensification.
A 1800
turn represents a 1.5 mm advancement of the Lag screw.
Verify the position and depth of the screw with image intensification in
both planes. Remove the centering sleeve and advance the side plate
onto the Lag screw shaft. Use the plate tamper to fully seat the plate.
Unscrew the Lag screw retaining rod and remove the insertion wrench
from the back of the Lag screw. Then remove the threaded guide pin.
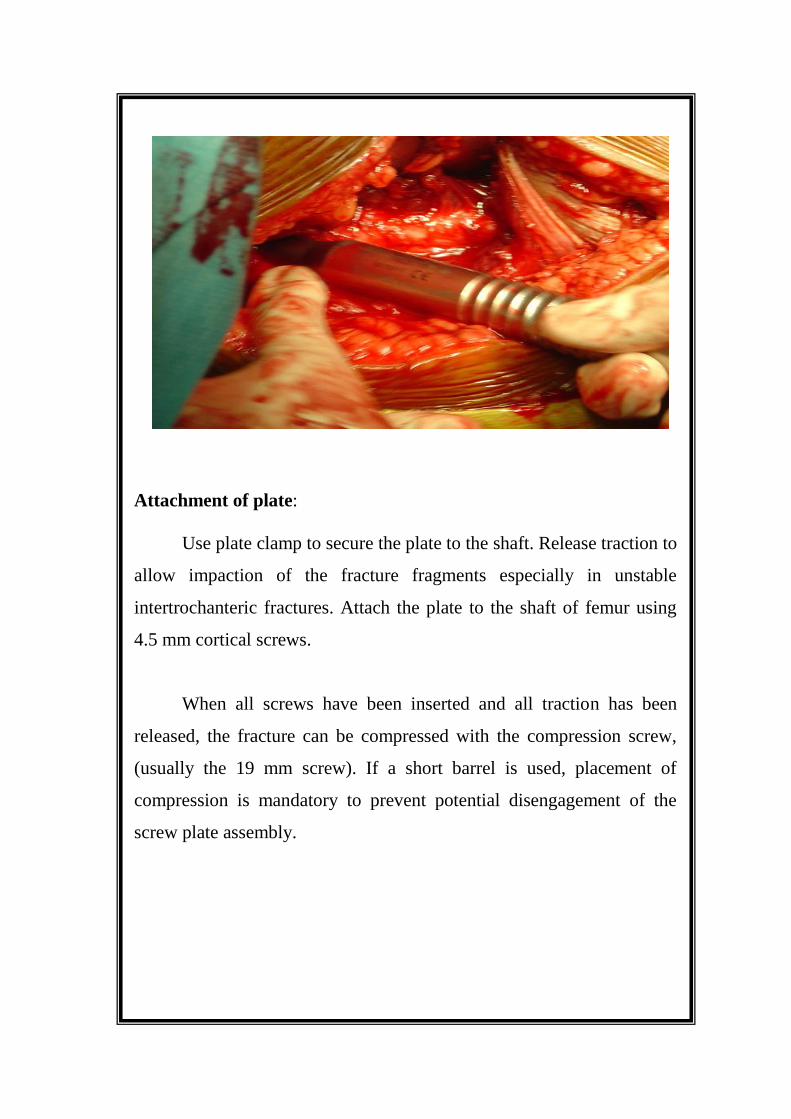
Attachment of plate:
Use plate clamp to secure the plate to the shaft. Release traction to
allow impaction of the fracture fragments especially in unstable
intertrochanteric fractures. Attach the plate to the shaft of femur using
4.5 mm cortical screws.
When all screws have been inserted and all traction has been
released, the fracture can be compressed with the compression screw,
(usually the 19 mm screw). If a short barrel is used, placement of
compression is mandatory to prevent potential disengagement of the
screw plate assembly.
PROFORMA
CASE NO:1
Name :R.Saradha IP. No.:41972
Age / Sex : 55\F DOA :2\11\2008
Occupation : House wife DOS :6\11\2008
Address: bujibuji nellore DOD :14\11\2008
nellore
Time between Injury and Admission: Same day
Nature of Injury: Trivial
Side of Injury : Left femur
Associated injuries: Nil
Associated Medical Problems: Nil
RADIOGRAHY : X-ray No. 76 Date:2\11\2008
Boyd-Griffin Classification: Type 2
Pre-Operative Traction: Skin traction for 4 days
Time between Admission and Surgery: 4 days
Operative Treatment
Anesthesia SA
Reduction Method. Closed
Approach Lateral approach
Implant DHS
Post Operative Treatment
Antibiotics yes
Analgesics yes
Blood transfusion No
Drain removal date 8\11\2008
Suture removal on 10.th
post operative day
Ambulation in Bed started 3 post operative day
Walking without support 6 months
Post operative complications: -Nil
Follow up of patients:
One Month : Radiologically implant insitu, Clinically looked
for tenderness . Adviced partial weight bearing with walker
Three Months : Radiologically implant insitu with compression at
the fracture site is seen. Clinically hip movements are near normal
no tenderness Adviced full weight bearing with walker
Six Months : Rdiologically healed fracture, Clinically hip
movements are near normal, shortening of 1cm. Adviced unaided
walking
One year : Patient was assessed by Harris Hip Score
Shortening by 1cm
Fracture united at 6 months
Score -92

CASE 1 Pre-op Imm Post op
3 Months Post - Op
1 Month Post - Op
6months Post - Op
1 year Post - Op
3 Months Post -Op
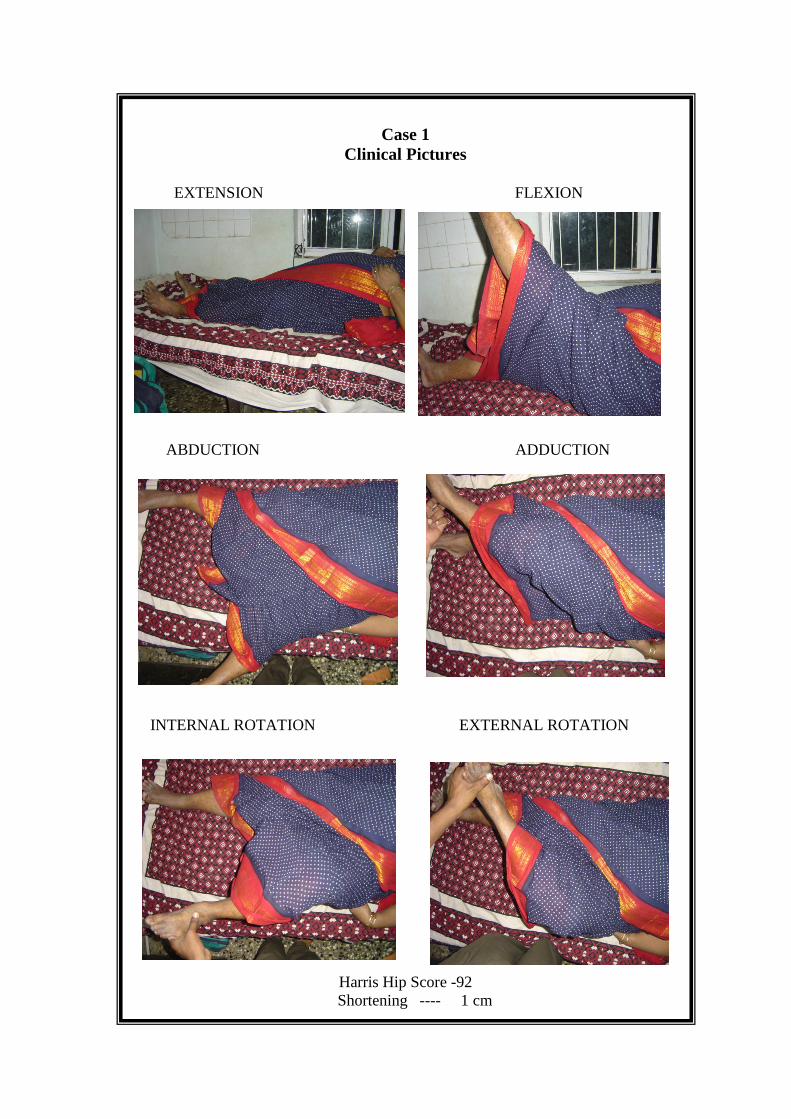
Case 1
Clinical Pictures
EXTENSION FLEXION
ABDUCTION ADDUCTION
INTERNAL ROTATION EXTERNAL ROTATION
Harris Hip Score -92
Shortening ---- 1 cm

CASE NO: 2
Name : S.Ram mohan IP. No.:38833
Age / Sex : 75\M DOA :7\6\2008
Occupation: Farmer DOS :13\6\2008
Address: Chithareddy palem DOD :21\6\2008
nellore
Time between Injury and Admission: One day
Nature of Injury : Trivial
Side of Injury : Right femur
Associated Injuries : Nil
Associated Medical Problems : Hypertensive
RADIOGRAHY : X-ray No.1 Date:7\6\2008
Boyd-Griffin Classification : Type 3
Pre-Operative Traction : Skin traction one day
Time between Admission and Surgery: 6 days
Operative Treatment:
1. Anesthesia : SA
2. Reduction Method : CLOSED
3. Approach : LATERAL APROACH
4. Implant : DHS
Post Operative Treatment
5. Antibiotics Yes
6. Analgesics Yes
7. Blood transfusion Nil
8. Drain removal date 15\6\2008
9. Suture removal on 10 Post operative day
10. Ambulation in Bed started 2 Post operative day
11. Walking without support 6 M0NTHS
Post Operative Complications -Nil Follow up of patients:
One Month : Radiologically Implant insitu . Clinically no
tenderness . Partial weight bearing is adviced with help of a
walker after 2 wks
Three Months : Radiologically implant insitu with
compression at the fracture site is seen . Clinically hip
movements are near normal, no tenderness . Adviced Full weight
bearing with the help of a walker
Six Months :Radiologically Healed fracture . Clinically
Hip movements are normal, shortening of 0.5 cm. Adviced
unaided walking
One Year : Normal range of hip movements
Union occured by 5 months
Shortening of 0.5 cm
Harris hip score - 94
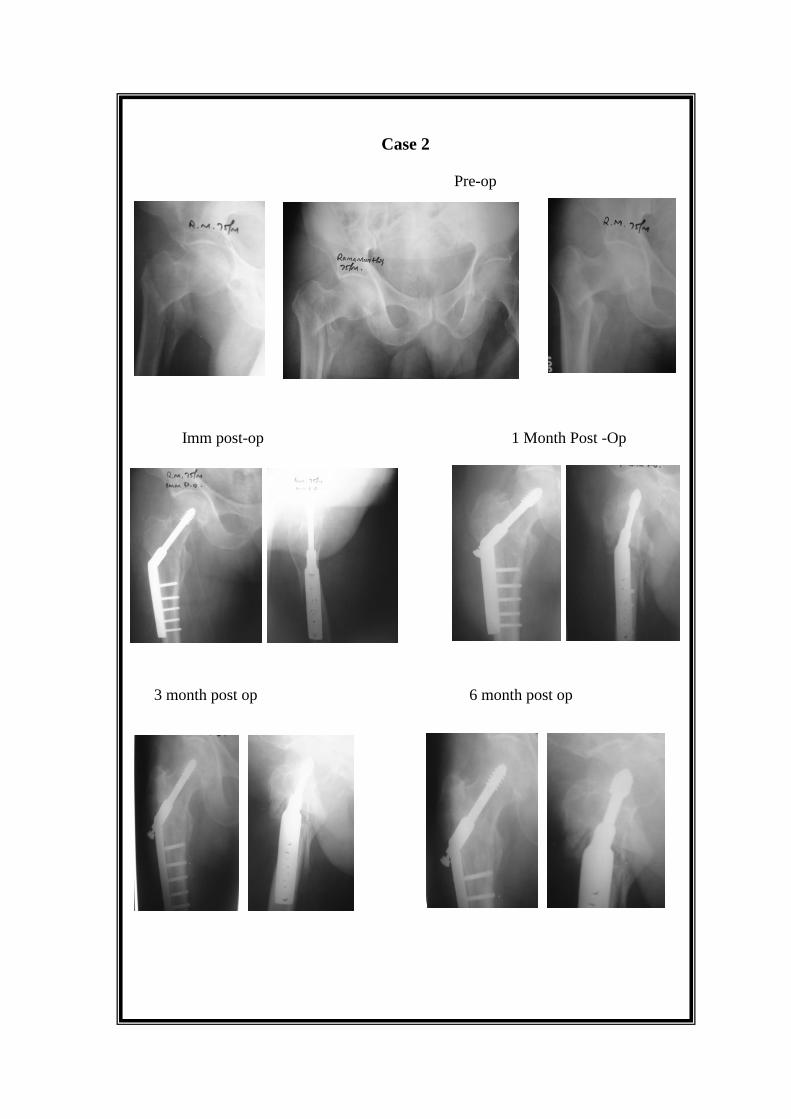
Case 2
Pre-op
Imm post-op 1 Month Post -Op
3 month post op 6 month post op

Case -2
Clinical Pictures
Harris Hip Score – 94
Shortening --0.5 cm
CASE NO: 3
Name : G.Ranga samy IP. No.:42645
Age / Sex : 76\M DOA :5\3\2009
Occupation: Farmer DOS :10\3\2009
Address: venkateswara puram DOD :20\3\2009
nellore
Time between Injury and Admission: Same day
Nature of Injury : Trivial
Side of Injury : Left femur
Associated Injuries : Colles fracture rt
Associated Medical Problems : Diabetic
RADIOGRAHY : X-ray No.17 Date:5\3\2009
Boyd-Griffin Classification : Type 2
Pre-Operative Traction : Skin traction for 5 days
Time between Admission and Surgery: 5 days
Operative Treatment
Anaesthesia SA
Reduction Method. Closed
Approach Lateral Approach
Implant DHS
Post Operative Treatment
Antibiotics Yes
Analgesics Yes
Blood transfusion 1Unit
Drain removal date 2nd
post operative day
Suture removal on 10th
post operative day
Ambulation in Bed started 4th
post operative day
Walking without support 6 months
Post operative complications:- UTI
Follow up of patients:
One Month : Radiologically implant insitu . Clinically no
tenderness. Partial weight bearing is allowed after 2 wks with the
help of walker
Three Months : Radiologically Implant insitu with
compression at the fracture site .Clinically hip movements are
near normal and no tenderness. Full weight bearing is adviced
with the help of walker
Six Months : Radiologically Fracture healed . Clinically
hip movements are near normal, shortening of 1.5 cm . Adviced
unaided walking
One Year : Hip movements are near normal
Shortening of 1.5 cm
Fracture healed by 6 months
Harrishirscorre-87
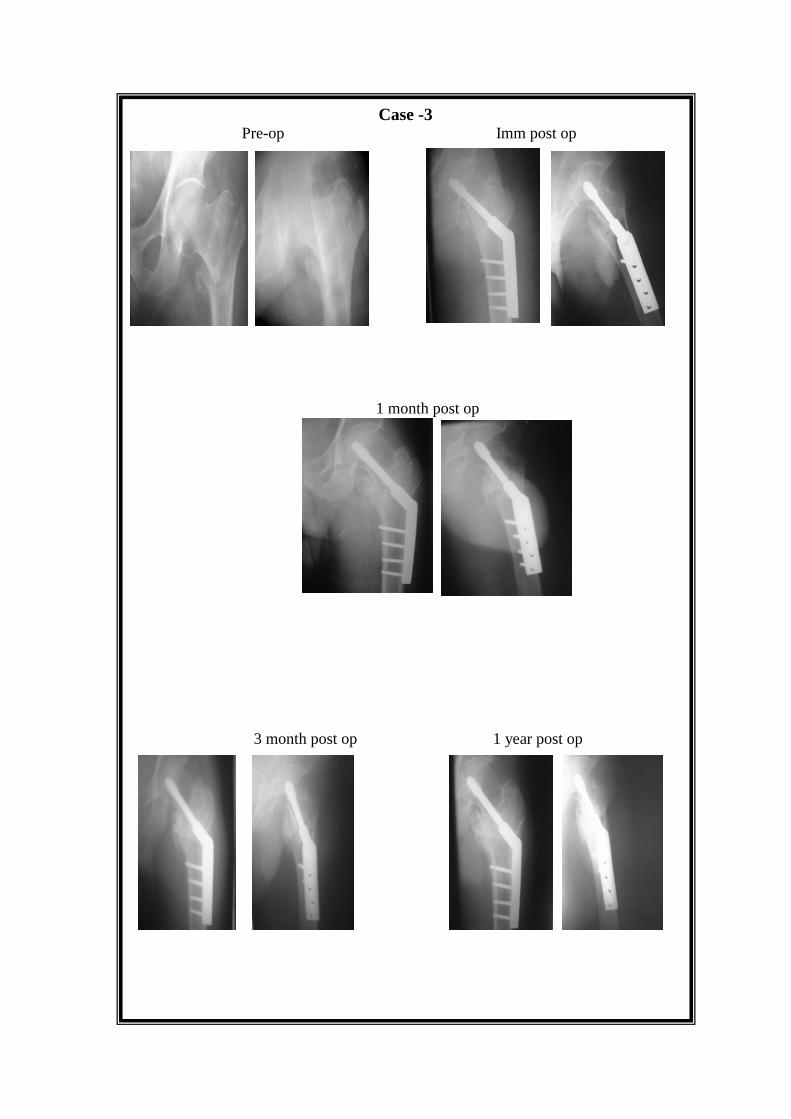
Case -3 Pre-op Imm post op
1 month post op
3 month post op 1 year post op
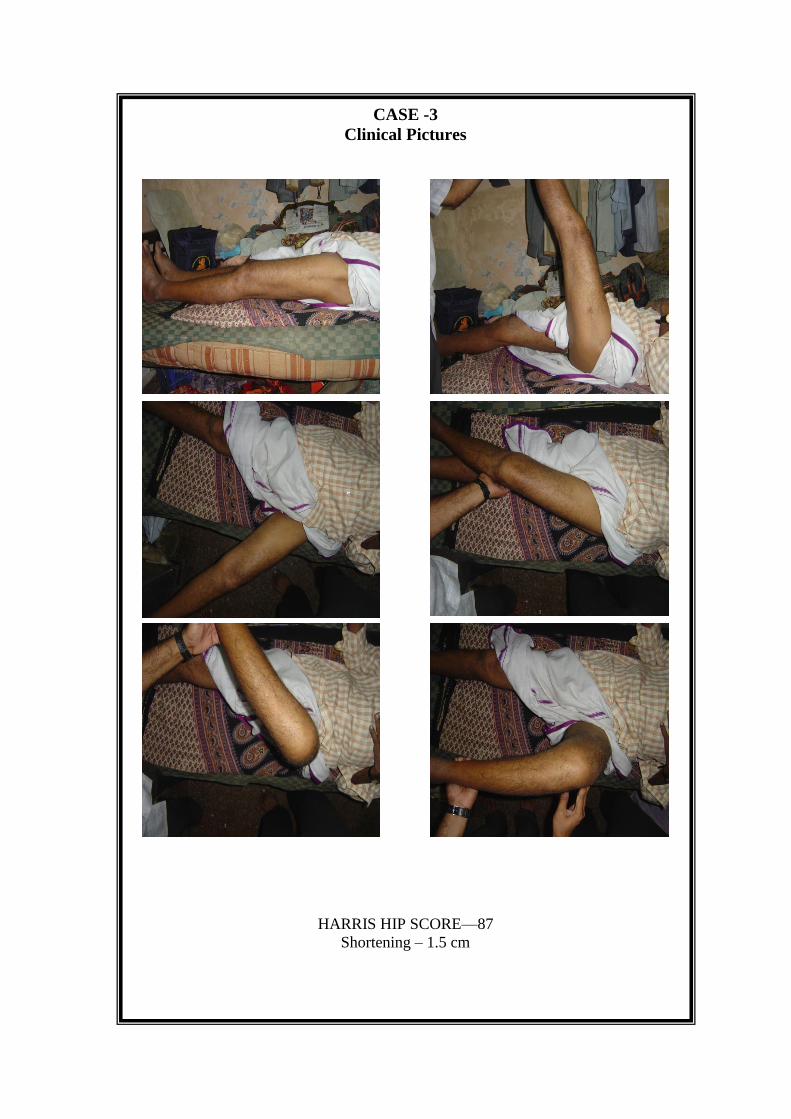
CASE -3
Clinical Pictures
HARRIS HIP SCORE—87
Shortening – 1.5 cm

CASE NO : 4
Name : P.Rama rao IP. No.:13246
Age / Sex :32\M DOA :3\10\2009
Occupation: Construction worker DOS : 8\10\2009
Address: Podhalakur road DOD :15\10\2009
Nellore
Time between Injury and Admission: 2 days
Nature of Injury: High velocity
Side of Injury: Left femur
Associated Injuries: Nil
Associated Medical Problems: Nil
RADIOGRAHY : X-ray No. 24 Date: 3\10\2009
Boyd-Griffin Classification Type 3
Pre-Operative Traction: Skin traction for 5 days
Time between Admission and Surgery: 5 days
Operative Treatment:
Anaesthesia SA
Reduction Method. Closed reduction
Approach Lateral approach
Implant DHS
Post Operative Treatment
Antibiotics Yes
Analgesics Yes
Blood transfusion No
Drain removal date 2nd
Post operative day
Suture removal on 10th
post operative day
Ambulation in Bed started 2nd
post operative day
Walking without support 6months
Post operative complication : Nil
Follow up of patients:
One Month : Radiologically Implant insitu. Clinically
mild tendrness present. Partial weight bearing is allowed with
help of walker after 4wks
Three Months : Radiologically Implant insitu with
compression at the fracture site. Clinically hip movements are
mildly restricted. moderate pain present
Adviced Full weight bearing with the help of a walker
Six Months : Radiologically headled fracture .Clinically
Mild restriction of hip movements . shortening of 1.5 cm present.
Adviced unaided walking
One Year : Moderate restriction of movements
Moderate pain and limp
Shortening of 1.5 cm with heterotrophic ossification
Harris hip score- 75

Case -4
Pre-op Imm post-op
3 Months Post -Op
6 Months Post -Op
1 Year Post –Op

Clinical Pictures-4 EXTENSION FLEXION
ABDUCTION EXTERNAL ROTATION
ADDUCTION INTERNAL ROTATION
Harris hip Score -75
Shortening—2.5 cm
CASE NO :5
Name : D.Venkata subbiah IP. No.:12426
Age / Sex : 78\M DOA :12\12\2009
Occupation: Labour DOS : 19\12\2009
Address: Venkatachalam DOD :27\12\2009
nellore
Time between Injury and Admission: On the day of injury
Nature of Injury: Trivial
Side of Injury: Left femur
Associated Injuries: Nil
Associated Medical Problems: Hypertensive and diabetic
RADIOGRAHY : X-ray No. 28 Date: 12\12\2009
Boyd-Griffin Classification Type 4
Pre-Operative Traction: Skin traction for 7 days
Time between Admission and Surgery: 7 days
Operative Treatment:
Anaesthesia S A
Reduction Method. Closed method
Approach Lateral approach
Implant DHS
Post Operative Treatment
Antibiotics Yes
Analgesics Yes
Blood transfusion One unit
Drain removal date 2nd
post operative day
Suture removal on 10th
post operative day
Ambulation in Bed started 7th
post operative day
Post operative complications: Decubitus ulcer
Follow up of patients:
One Month : Radiologically Implant insitu. Clinically
tenderness present. Partial weight bearing was adviced after 2wks
with help of a walker
Three Months : Radiologically implant insitu with
compression at fracture site Clinically Hip movemens are
moderately restricted with sever pain.
Six Months : Radiologically lag screw was cut through.
patient has undergone hemiarthoplasty. Walking with help of a
stick
One Year :Sever pain and limp
Hemiarthoplaty has been done
Harris hip score - 54

Complication
Case 5
Pre-op Immediate post-op
6 months post-op After bipolar arthroplasty
CASE NO:6
Name :S.Amanamma IP. No.:18647
Age / Sex :72\F DOA : 19\10\2009
Occupation: House wife DOS :25\10\2009
Address: Muthukuru DOD :2\11\2009
nellore
Time between Injury and Admission:10 days
Nature of Injury: Trivial
Side of Injury: Right femur
Associated Injuries: Nil
Associated Medical Problems: Hypertensive
RADIOGRAHY : X-ray No. 27 Date:19\10\2009
Boyd-Griffin Classification Type 3
Pre-Operative Traction: Skin traction for 6 days
Time between Admission and Surgery: 6 days
Operative Treatment:.
Anaesthesia SA
Reduction Method. Closed method
Approach Lateral approach
Implant DHS
Post Operative Treatment
Antibiotics Yes
Analgesics Yes
Blood transfusion 2 units
Drain removal date 2 post operative day
Suture removal on 12post operative day
Ambulation in Bed started 4 post operative day
Post operative complications:- Nil
Follow up of patients:
One Month : Radiologically Implant insitu. Clinically
Pain present. Adviced not to weight bear
Three Months : Radiologically implant insitu and fracture
site compression was not attained. Clinically Pain present and
movements are restricted . Adviced PWD with help of a walker
Six Months : Radiologically lag screw was cut through.
Clinically Sever pain and limp present. hip movements are
markedly restricted . Adviced surgery but pt refused for second
surgery
One Year : Sever pain with limp
Hip movements are restricted
Harris hip score - 60

COMPLICATION
CASE 6 Pre-op Immediate post-op
3 months post-op 6 months post-op
CASE NO:7
Name :J.Kasthuramma IP. No.:27785
Age / Sex :69\F DOA :6\9\2009
Occupation: House wife DOS :10\9\2009
Address: Lakshmipuram DOD : 20\9\2009
sangam
Time between Injury and Admission: 2 days
Nature of Injury: Trivial
Side of Injury: Right femur
Associated Injuries: Nil
Associated Medical Problems: Hypertension
RADIOGRAHY : X-ray No. 24 Date: 6\9\2008
Boyd-Griffin Classification Type 2
Pre-Operative Traction: Skin traction for 4 days
Time between Admission and Surgery: 4 days
Operative Treatment:
Anaesthesia SA
Reduction Method. Closed method
Approach Lateral approach
Implant DHS
Post Operative Treatment
Antibiotics Yes
Analgesics Yes
Blood transfusion Nil
Drain removal date 2 post operative day
Suture removal on 10 post operative day
Ambulation in Bed started 3 post operative day
Walking without support 6 months
Post operative complication: Nil
Follow up of patients:
One Month : Radiologically Implant insitu . Clinically
No tenderness. Partial weight bearing is adviced with the help of
walker after 3 wks
Three Months : Radiologically implant insitu with
compression at the fracture site. Clinically Hip movements are
mildly restricted with shortening . Adviced FWB with walker
after 4 wks
Six Months : Radiologically fracture healed. Clinically
moderate restriction of hip movements with moderate pain and
shortening. Adviced unaided walking
One Year : Mild limp with restricted range of movements
Harris hip score - 74
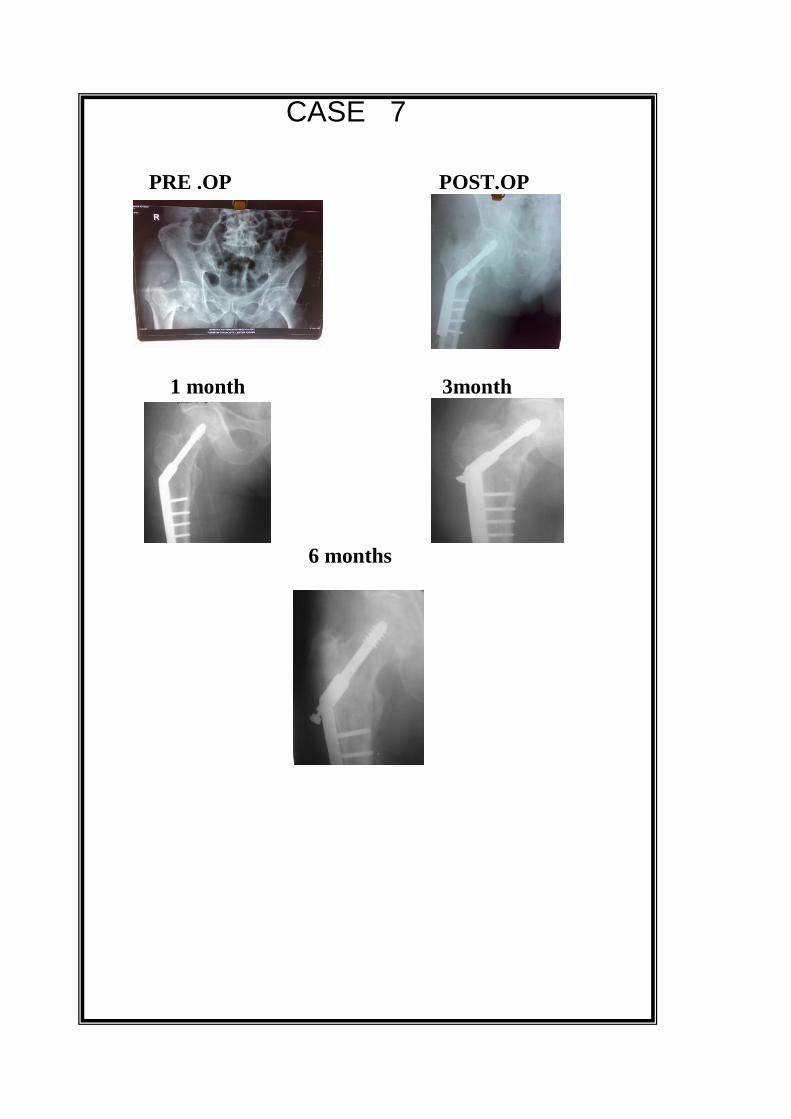
CASE 7
PRE .OP POST.OP
1 month 3month
6 months
CASE NO : 8
Name :K.Subbamma IP. No.:40878
Age / Sex :60\F DOA : 11\7\2008
Occupation: house wife DOS : 14\7\2008
Address: Vasili DOD :24\7\2008
athmakur
Time between Injury and Admission: On the day of injury
Nature of Injury: Trivial
Side of Injury: Left femur
Associated Injuries: Nil
Associated Medical Problems: Hypertensive
RADIOGRAHY : X-ray No. 4 Date:11\7\2008
Boyd-Griffin Classification Type 2
Pre-Operative Traction: Skin traction for 3 days
Time between Admission and Surgery: 3 days
Operative Treatment:
Anaesthesia SA
Reduction Method. Closed method
Approach Lateral approach
Implant DHS
Post Operative Treatment
Antibiotics Yes
Analgesics Yes
Blood transfusion One unit
Drain removal date 2 post operative day
Suture removal on 10 post operative day
Ambulation in Bed started 2 post operative day
Walking without support 6 months
Post operative complications: Nil
Follow up of patients:
One Month : Radiologically Implant insitu. Clinically
no tenderness. Adviced Partial weight bearing after 2 wks with
the help of a walker
Three Months : Radiologically implant insitu with
compression at the fracture site . Clinically Hip movements are
near normal. Adviced Full weight bearing after 4 wks with the
help of a walker
Six Months : Radiologically fracture heald. Clinically Hip
movements are normal with 1 cm shortening . Adviced unaided
walking
One Year : Hip movements are near normal
Moderate limp and fracture united by 7 months
Harris hip score - 92
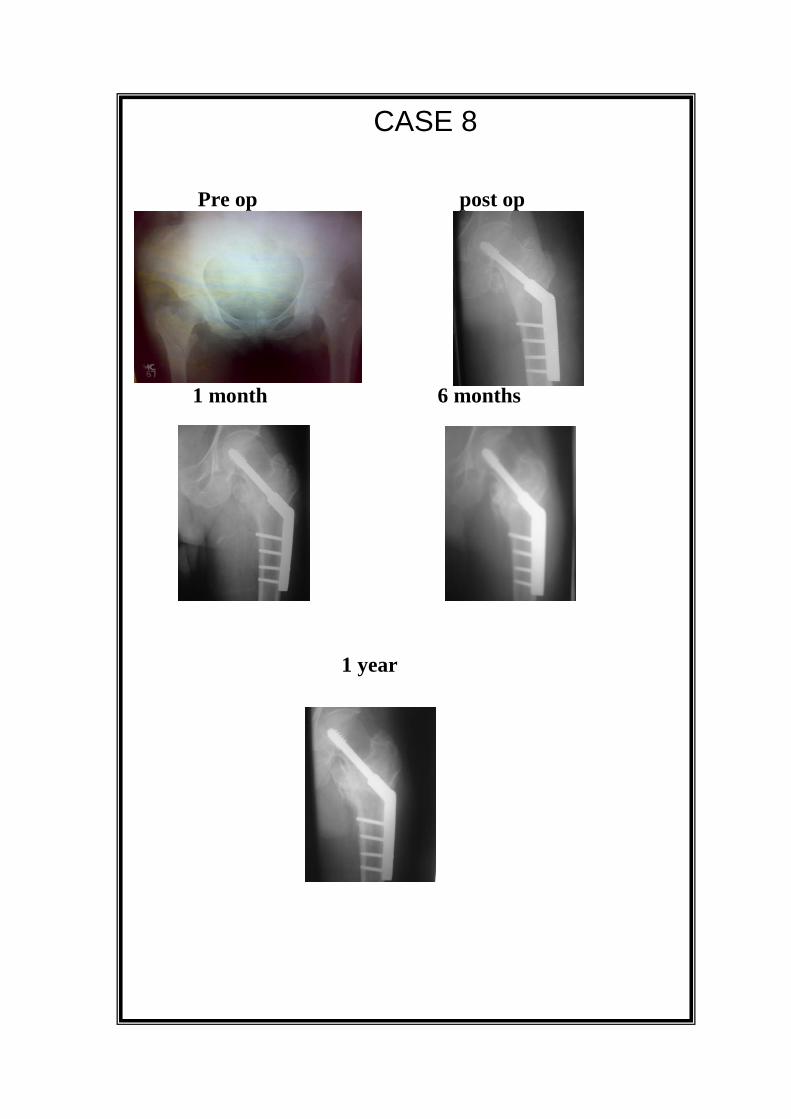
CASE 8
Pre op post op
1 month 6 months
1 year
CASE NO :9
Name :V.Lakshmi IP. No.:28038
Age / Sex :68\F DOA :16\9\2009
Occupation: House wife DOS :17\9\2009
Address: Totapalli guduru DOD :27\9\2009
nellore
Time between Injury and Admission: 2 days
Nature of Injury: Trivial
Side of Injury: Right femur
Associated Injuries: Nil
Associated Medical Problems: Nil
RADIOGRAHY : X-ray No. 22 Date:16\9\2009
Boyd-Griffin Classification Type 2
Pre-Operative Traction: Skin traction one day
Time between Admission and Surgery: 1 Day
Operative Treatment:
Anaesthesia SA
Reduction Method. Closed method
Approach Lateral approach
Implant DHS
Post Operative Treatment
Antibiotics Yes
Analgesics Yes
Blood transfusion 2 units
Drain removal date 2 post operative day
Suture removal on 10 post operative day
Ambulation in Bed started 2 post operative day
Walking without support 6 months
Post operative complication : Nil
Follow up of patients:
One Month : Radiologically implant insitu. Clinically mild
tenderness present. Partial weight bearing is adviced after 4wks
with the help of a walker
Three Months : Radiologically implant insitu with moderate
compression at the fracture site. Clinically Moderate restriction of
hip movement and pain. Adviced Full weight bearing with the
help of a walker
Six Months : Radiologically fracture healed. Clinically
restriction of hip movements with pain and shortening of 1.4 cm
One Year : Mild pain and limp
Moderate restriction of movements
Fracture healed by 5 months
Harris hip score 82
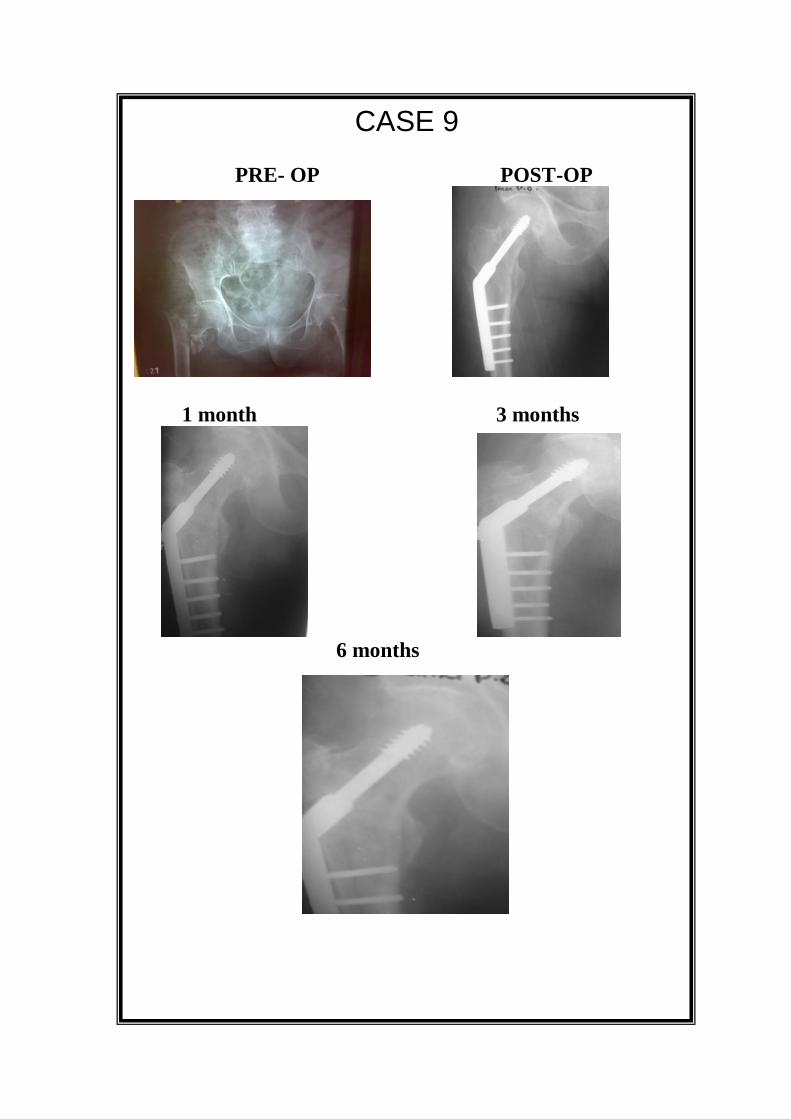
CASE 9
PRE- OP POST-OP
1 month 3 months
6 months

CASE NO :10
Name :V.Subramanyam IP. No.:45361
Age / Sex :52\M DOA :5\4\2009
Occupation: Farmer DOS :7\4\2009
Address: Maipadu DOD :17\4\2009
nellore
Time between Injury and Admission: 10 days
Nature of Injury: High velocity
Side of Injury: Right femur
Associated Injuries: NIL
Associated Medical Problems: HYPERTENSION
RADIOGRAHY : X-ray No. 18 Date:5\4\2009
Boyd-Griffin Classification TYPE 4
Pre-Operative Traction: Skeletal traction for 2 days
Time between Admission and Surgery: 2 days
Operative Treatment:
Anaesthesia SA
Reduction Method. Closed method
Approach Lateral approach
Implant DHS
Post Operative Treatment
Antibiotics Yes
Analgesics Yes
Blood transfusion Nil
Drain removal date 2 post operative day
Suture removal on 10 post operative day
Ambulation in Bed started 3 post operative day
Walking without support 6 months
Post operative complications:-- Nil
Follow up of patients:
One Month : Radiologically Implant insitu. Clinically
mild tenderness present. Partial weight bearing is adviced after 3
wks with the help of walker
Three Months : Radiologically implant insitu with
compression at the frcture site . Clinically marked restriction of
movments occasional pain. Adviced to Full weight bearing after
1 month with the help of a walker.
Six Months : Radiologically fracture united. Clinically
Moderate restriction of movements with flexion deformity,
occasional pain and shortening of 1.8 cm. Adviced to walk
unaided
One Year : Restriction of hip movements
Fixed flexion deformity
Harris hip score- 84
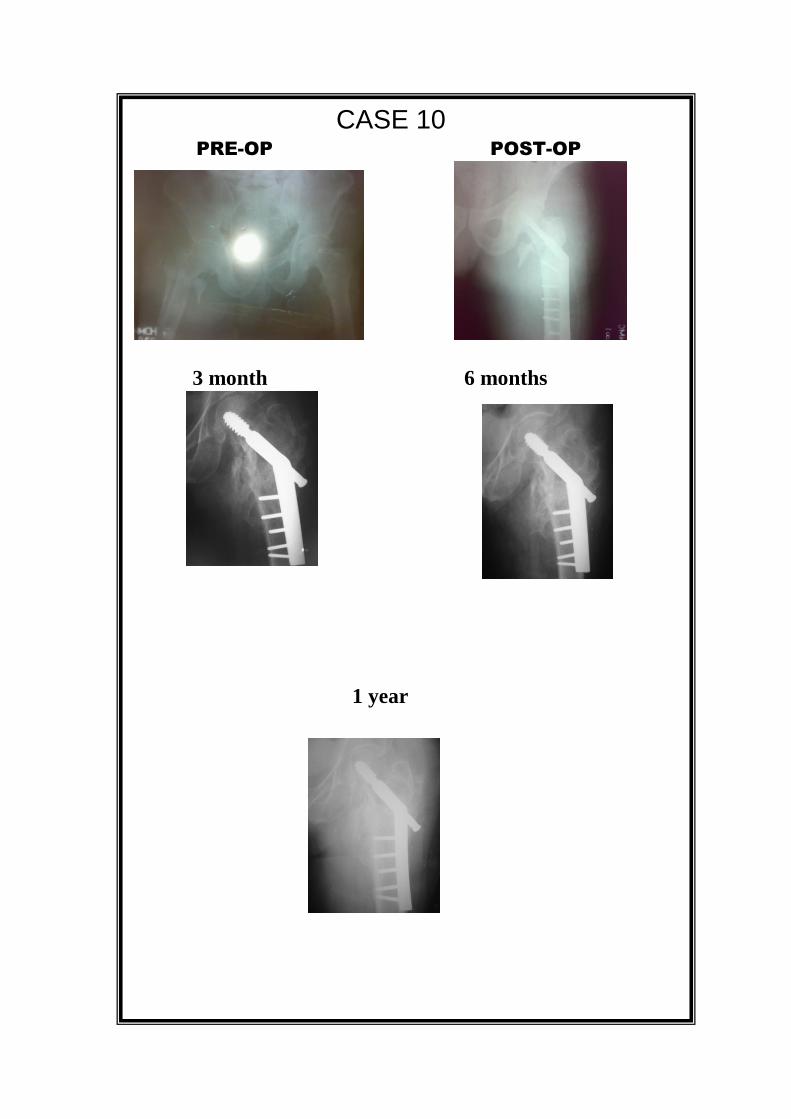
CASE 10 PRE-OP POST-OP
3 month 6 months
1 year
CASE NO :11
Name : T.Radhamma IP. No.:42645
Age / Sex :86\F DOA :3\1\2009
Occupation: House wife DOS :6\1\2009
Address: Mulapet DOD : 16\1\2009
nellore
Time between Injury and Admission: Day of injury
Nature of Injury: Trivial
Side of Injury: Left femur
Associated Injuries: Nil
Associated Medical Problems: Diabetic
RADIOGRAHY : X-ray No. 13 Date: 3\1\2009
Boyd-Griffin Classification Type 2
Pre-Operative Traction: Skin traction for 3 days
Time between Admission and Surgery: 3 days
Operative Treatment:
Anaesthesia SA
Reduction Method Closed method
Approach Lateral approach
Implant DHS
Post Operative Treatment
Antibiotics Yes
Analgesics Yes
Blood transfusion Nil
Drain removal date 2 post operative day
Suture removal on 10 post operative day
Ambulation in Bed started 2 post operative day
Walking without support 6 months
Post operative complications:- UTI
Follow up of patients:
One Month : Radiologically Implant insitu. Clinically
tenderness present. Advice Partial weight bearing after 3wks with
help of a walker
Three Months : Radiologically implant insitu with
compression at the fracture site . Clinically hip movements are
near normal with moderate pain. Adviced Full weight bearing
with help of a walker
Six Months : Radiologically fracture united. Clinically hip
movements are normal with moderate pain and shortening of
1 cm. Adviced walking un aided
One Year :Moderate limp and tenderness
Movements are normal
Fracture united by 5 months
Harris hip score - 90
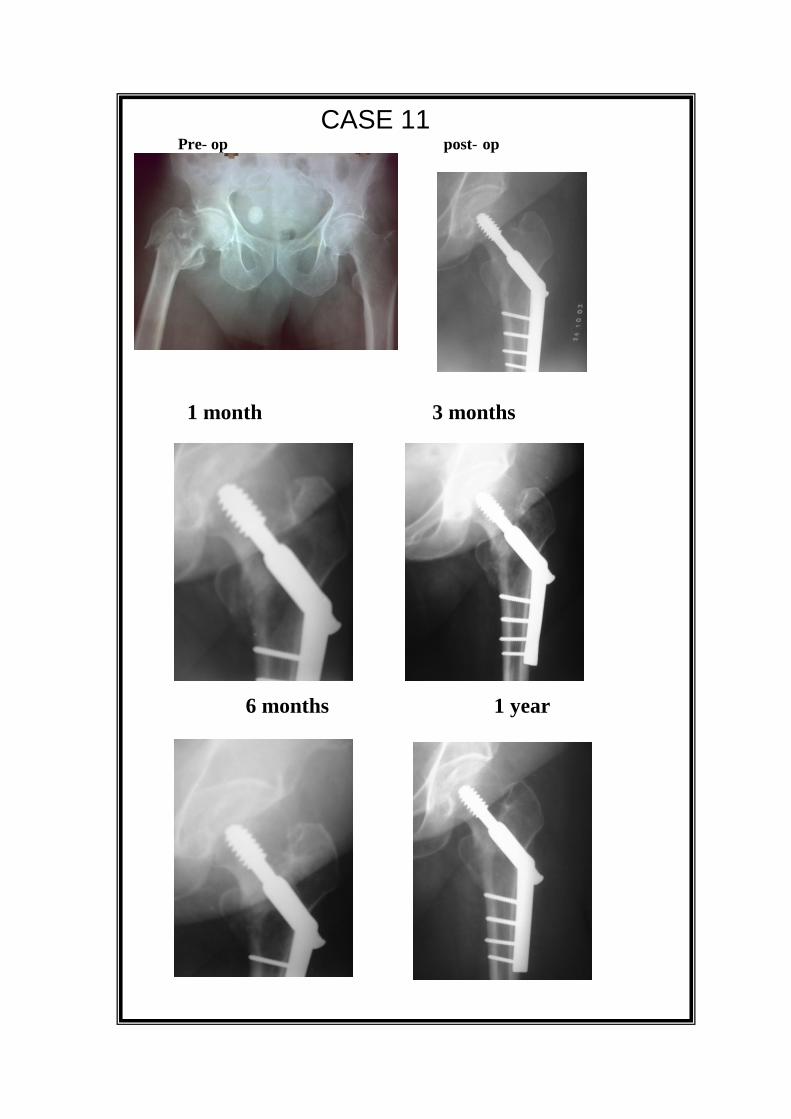
CASE 11 Pre- op post- op
1 month 3 months
6 months 1 year

CASE NO:12
Name :P.Rajyalakshmi IP. No.:53421
Age / Sex :69\F DOA :9\8\2009
Occupation: Housewife DOS : 15\8\2009
Address: Venkatagiri DOD : 25\8\2009
Time between Injury and Admission 3days
Nature of Injury: Trivial
Side of Injury: Left femur
Associated Injuries: Nil
Associated Medical Problems: Hypertension and diabetes
RADIOGRAHY : X-ray No.5 Date: 9\8\2009
Boyd-Griffin Classification Type 2
Pre-Operative Traction: Skin traction for 6 days
Time between Admission and Surgery: 6 days
Operative Treatment:
Anaesthesia SA
Reduction Method. Closed reduction
Approach Lateral approach
Implant DHS

Post Operative Treatment
Antibiotics yes
Analgesics yes
Blood transfusion Nil
Drain removal date 2 post operative day
Suture removal on 10 post operative day
Ambulation in Bed started 2 post operative day
Walking without support 6 months
Post operative complications : Nil
Follow up of patients:
One Month : Radiologically Implant insitu. Clinically
tenderness present. Adviced Partial weight bearing after 4 wks
with help of walker
Three Months : Radiologically implant insitu with
compression at the fracture site . Clinically Near normal hip
movements. Adviced FWB with the help of a walker.
Six Months : Radiologically fracture heald. Clinically
normal movements of hip with occasional pain . Adviced to walk
unaided
One Year : Hip movements are near normal
Mild limp
Fracture united by 5 months
Harris hip score - 92
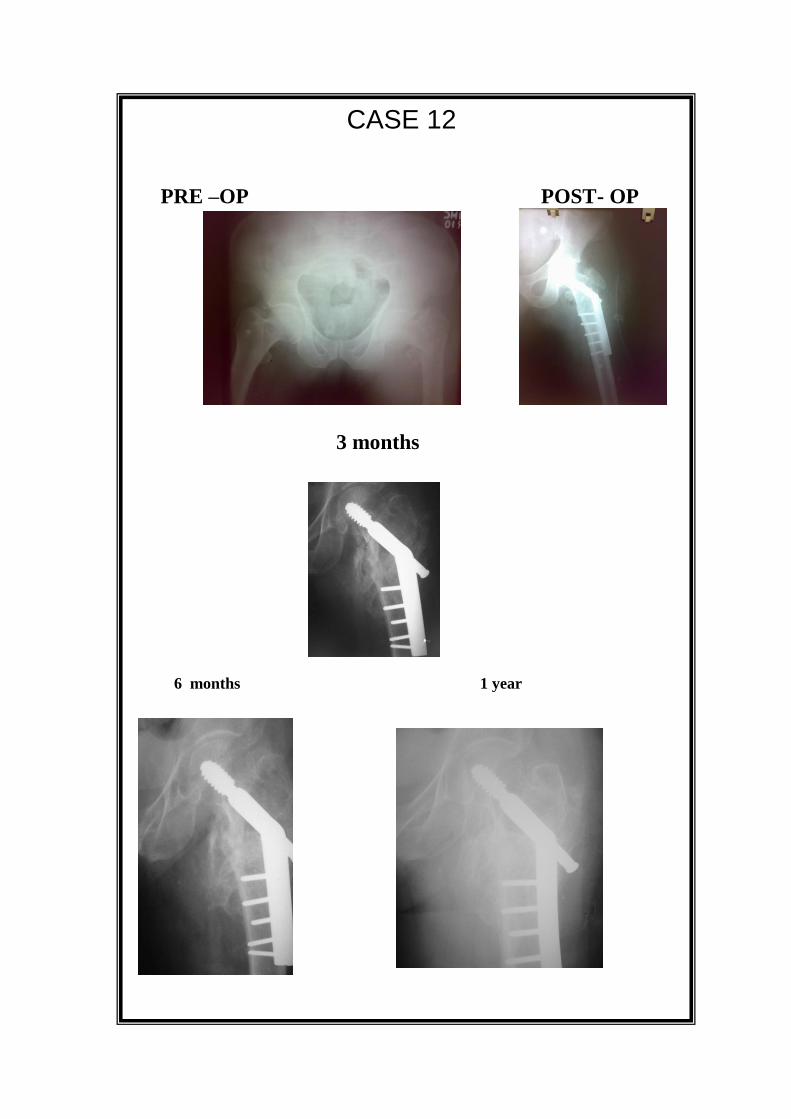
CASE 12
PRE –OP POST- OP
3 months
6 months 1 year

POST OPERATIVE PROTOCOL
POST OPERATIVE PROTOCOL
All patients were allowed to flex the knee from 2nd
Post operative
day and physical ambulation was started on 8th Post operative day on an
average.
All the patients were covered with appropriate antibiotics.
All the patients were checked both clinically and radiologically
for the first 6 wks partial weight bearing was allowed with the help of a
walker.all patients were reviewed at 3 months both clinically and
radiological assement were done for placement of implant , compression
at the fracture site, examined for range of movements, tenderness and
shortening . All patients were adviced to weight bear with the help of
walker
At 6 months both clinical and radiological assessment were done,
check x-ray is taken to see weather fracture has heald. Clinically
examined for range of movements and tenderness ,shortening and any
fixed deformities. All Patients were adviced to walk with full weight
bearing.
All Patient were assessed between 9month or 1year for harris hip score
by DHS fixation for the analysis of results of intretrochanteric
fractures.
RESULTS
RESULTS
Finally, 28 patients in my study an average age group of 70 years,
with intertrochanteric fractures were analysed with an average follow-up
period of 09 months and average duration of stay in the hospital of 13
days.
The results were analysed using the Harris Hip Scoring System.
Union occurred in 26 fractures and 2 non-unions with screw
cut through. All the patients had some amount of shortening with
majority of the patients (16 patients) having a shortening of 0-1 cm, 9
patients with 1-2 cm of shortening and 3 patients with >2 cm shortening.
12 patients had short limb gait and 6 patients were using a cane on
ipsilateral side for walking. 2 of the patients in our study were squatting
and sitting on the floor cross - legged in spite of the advice that they
should not squat or sit on the floor cross-legged following surgery.
2 of the patients with non-union with coxa - vara had screw
cut – through.
The results were analysed based on the Harris Hip Scoring
System and the patients were categorized according to the scores they
attained as follows:
Excellent : 100 - 90
Good : 89 - 80
Fair : 79 - 70
Poor : < 70

RATE OF UNION
NO.OF
CASES STUDIED
UNION
NON-UNION
28 26 2
AMOUNTOFSHORTENING
NO.OF
CASES
STUDIEd
0-1cm 1-2 cm >2 cm
28 patients 16 pts 9 pts 3 pts
Harris hip score: 23
Pain:
None or ignores it - 44.
Slight, occasional, no compromise in activities - 40.
Mild pain, no effect on average activities, rarely moderate pain with
unusual activity; may take aspirin - 30.
Moderate pain, tolerable but makes concessions to pain; some limitation
of ordinary activity or work; may require occasional pain medicine
stronger than aspirin - 20.
Marked pain, serious limitation of activities - 10
Totally disabled, crippled, pain in bed, bedridden -0
Limp:
None - 11
Slight - 8
Moderate - 5
Severe - 0
Support:
None - 11
Cane for long walks - 7
Cane most of the time - 5
One crutch - 3
Two canes - 2
Two crutches - 0
Not able to walk - 0
Distance walked:
Unlimited - 11
Six blocks - 8
Two or three blocks - 5
Indoors only - 2
Bed and chair - 0
Stairs:
Normally without using a railing - 4
Normally using a railing - 2
In any manner - 1
Unable to do stairs - 0
Put on shoes and socks:
With ease - 4
With difficulty - 2
Unable - 0
Sitting:
Comfortably in ordinary chair one hour - 5
On a high chair for one-half hour - 3
Unable to sit comfortably in any chair - 0
Enter public transportation (1):
Yes.
No.
Flexion contracture : …… (degrees ).
Limb length discrepancy : …… ( cm ).
Absence of deformity: (All Yes - 4; Less Than 4-0)
Less than 300 fixed flexion contracture: Yes - No
Less than 100 fixed adduction: Yes - No
Less than 100 fixed internal rotation
in extension : Yes - No
Limb length discrepancy less than 3.2 cm : Yes - No

Range of motion:
Flexion ( 1400 ) : ……
Abduction ( 400 ) : ……
Adduction ( 400 ) : ……
External rotation (400 ) : ……
Internal rotation ( 400 ) : …
Range of motion score :
2110 - 300
0 : 5
1610 - 210
0 : 4
1010 - 160
0 : 3
610 - 100
0 : 2
310 - 60
0 : 1
00 - 30
0 : 0
Range of Motion Score: ……
Total Harris Hip Score: ……
Readmission to Hospital: Yes / NO
Date of Readmission: ….\….\….
Implant Removal Date: ….\….\….
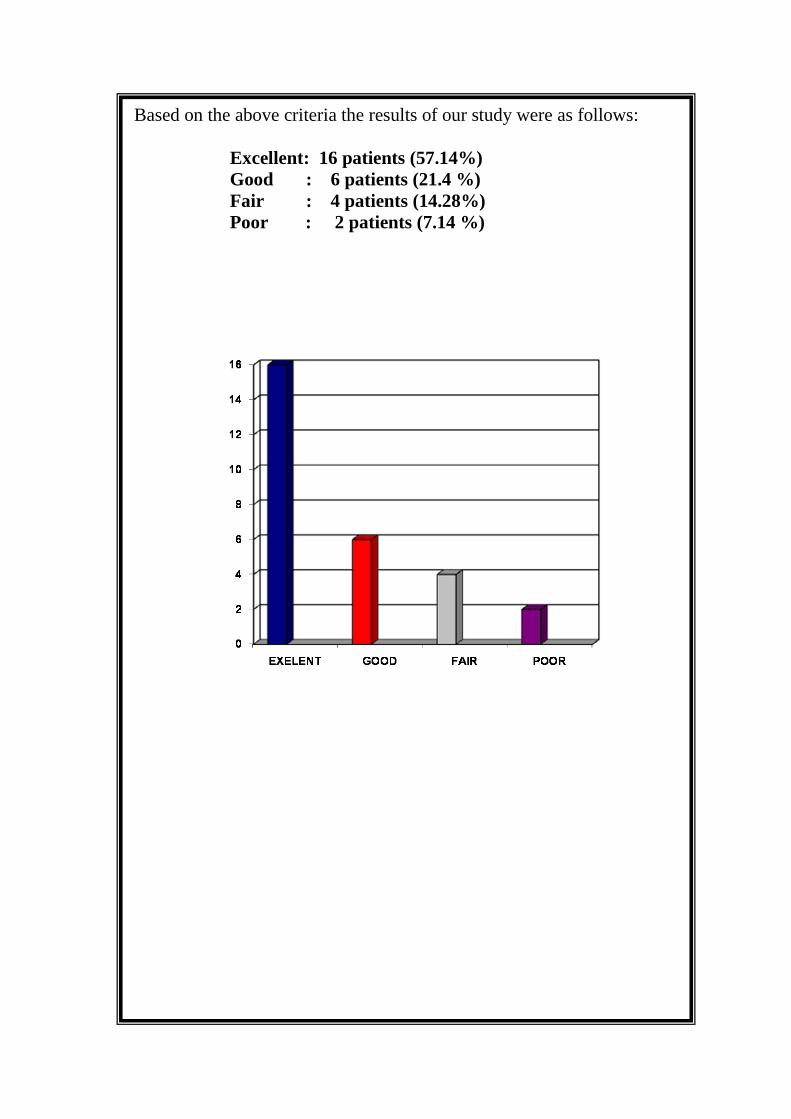
Based on the above criteria the results of our study were as follows:
Excellent: 16 patients (57.14%)
Good : 6 patients (21.4 %)
Fair : 4 patients (14.28%)
Poor : 2 patients (7.14 %)
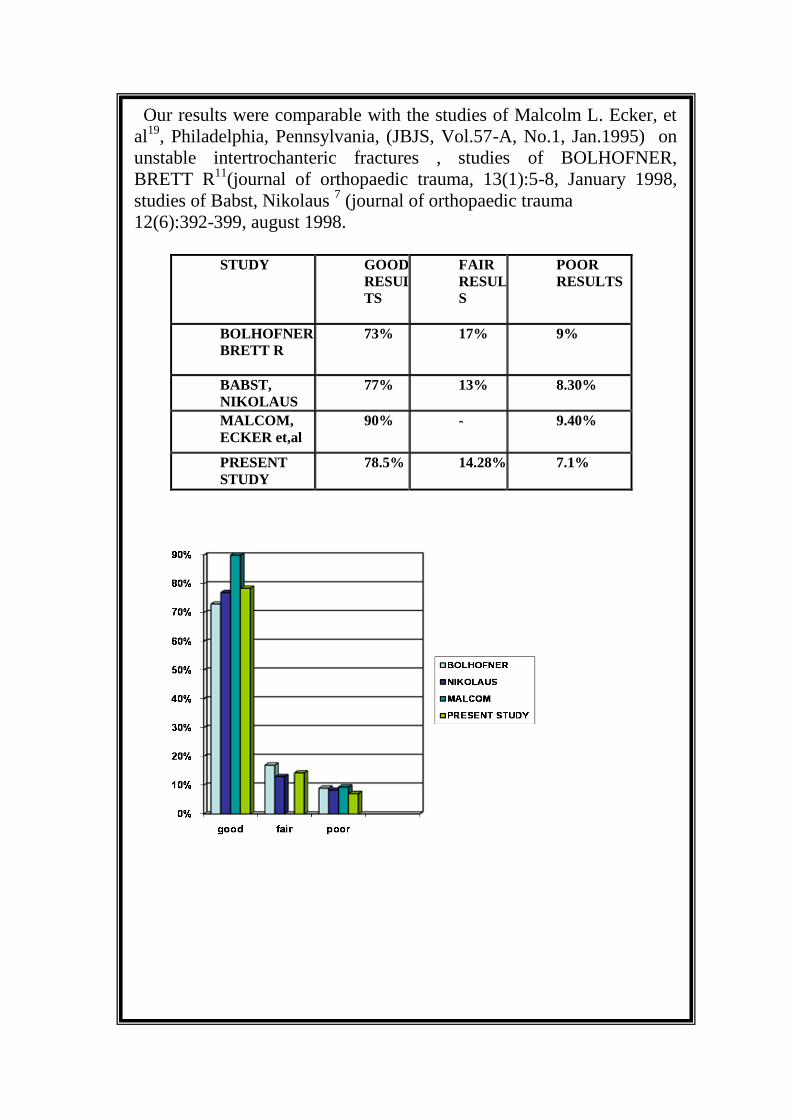
Our results were comparable with the studies of Malcolm L. Ecker, et
al19
, Philadelphia, Pennsylvania, (JBJS, Vol.57-A, No.1, Jan.1995) on
unstable intertrochanteric fractures , studies of BOLHOFNER,
BRETT R11
(journal of orthopaedic trauma, 13(1):5-8, January 1998,
studies of Babst, Nikolaus 7 (journal of orthopaedic trauma
12(6):392-399, august 1998.
STUDY GOOD
RESUL
TS
FAIR
RESULT
S
POOR
RESULTS
BOLHOFNER
BRETT R
73% 17% 9%
BABST,
NIKOLAUS
77% 13% 8.30%
MALCOM,
ECKER et,al
90% - 9.40%
PRESENT
STUDY
78.5% 14.28% 7.1%

DISCUSSION
DISCUSSION
28 cases of intertrochanteric fractures were treated by Dynamic
hip screw implant system. The purpose of the study was to evaluate the
result of treatment in these patients.
In the present study two cases of implant cut through. N.D
Chatterjee et al 43
reported coxa vara in 3 cases due to cutting of
implants through head & neck of femur and also proximal migration of
DHS with avascular changes of femoral head in one case. Mattan et al40
in 2002 reported 10 patients with osteoporosis developed painful
avascular necrosis after DHS fixation.
Heyse-Moore et. al, retrospectively compared the results of 107
intertrochanteric fractures stabilized with a sliding hip screw to 103
fractures treated with a Jewett nail and concluded that those patients
treated with the sliding hip screw had shorter hospitalization stays and a
lower incidence of fixation failure.28
. In our study average hospital stay
was 13days with failure of fixation in 7.1%
Bannister et. al, in a prospective randomized study of 155
intertrochanteric fractures stabilized using sliding hip screw and Jewett
nail, found that fractures that fractures stabilized with sliding hip screw
had a significantly lower risk of mechanical failure and a lower
incidence of revision surgery.9 In our study 2 case got sliding hip
screw cut through the head and neck of femur and required revision
surgery

Jacobs et. al, reported on a series of 173 intertrochanteric
fractures treated with internal fixation, 72 with a Jewett nail and 101
with a Sliding Hip Screw.29
Treatment failure – defined as either loss of
fixation, symptomatic joint penetration, osteonecrosis, malunion or
nonunion – occurred in 25% of fractures stabilized with a Jewett nail
and in 6% of fractures stabilized using a Sliding Hip Screw. In our study
failure rate was 7.1% by using sliding hip screw
Sernbo et. al, compared use of Ender nails to use of a Sliding Hip
Screw for the treatment of unstable intertrochanteric fractures in a
prospective randomized trial.49
Butt et. al, reported on a prospective, randomized controlled trial
that compared results in 95 consecutive patients who sustained a
pertrochanteric fracture of the femur and were treated using a Sliding
Hip Screw ( no. = 48) or a Gamma nail (no. = 47).15
whereas clinical
and radiological outcomes were similar, the Gamma nail was associated
with a higher incidence of complications - in particular, femur fracture
distal to the implant. In our study implant cut through was seen in 2
cases and arthritis in 1 case
Aune et. al, reported on a series of 378 intertrochanteric and
subtrochanteric fractures prospectively randomized to treatment with
either a Gamma nail ( 177 fractures ) or a Sliding Hip screw ( 201
fractures ).6 At an average follow-up of 17 months, 15 patients needed
revision surgery: 13 in the Gamma nail group and 2 in the Sliding Hip
Screw group. In our study 2 patients required revision surgery due to
implant cut through
Leung et. al, reported on a prospective series of 186
peritrochanteric fractures stabilized with either a Gamma nail or Sliding
Hip Screw.37
Gamma nails were inserted in a significantly shorter
operative time using a smaller incision and were associated with a
smaller estimated blood loss. There was, however, no significant
difference between the two groups with regard to 6-month mortality
rate, post-operative mobility, or hip function at fo7low-up. A higher
number of intraoperative complications occurred in fractures stabilized
with a Gamma nail. In our study there was no intraoperative
complications by using sliding hip screw
Baumgaertner et. al, reported on a series of 131 patients ( 135
fractures ) who sustained an intertrochanteric fracture and were
randomly assigned to treatment with either a Sliding hip Screw or an
Intramedullary Hip Screw ( IMHS ).10
In patients with unstable
intertrochanteric fractures, the intramedullary device was associated
with significantly less surgical time and blood loss; however, use of the
Intramedullary Hip Screw in patients who had a stable fracture pattern
required significantly greater fluoroscopy time. Intraoperative
complications occurred exclusively in the Intramedullary Hip Screw
group. At latest follow-up, there was no difference in the percentage of
functional recovery between the two fixation groups.
Hardy et. al, performed a prospective, randomized study
comparing use of a Sliding Hip Screw to use of an Intramedullary Hip
Screw ( IMHS ) for stabilization of 100 intertrochanteric fractures in
patients age 60 years or older.22
The operative time was significantly
greater with use of the intramedullary device; however, estimated
intraoperative blood loss was significantly lower. One fracture stabilized
with a Sliding Hip Screw had loss of fixation. The in-hospital and 6-
month mortality rates were similar between the two treatment groups.
The Intramedullary Hip Screw was associated with significantly less
screw sliding and limb shortening than the Sliding Hip Screw,
particularly when used to stabilize unstable fracture patterns. Based on
the results of this study, the authors concluded that routine use of the
Intramedullary Hip Screw cannot be recommended for stabilization of
intertrochanteric hip fractures.
Based on the available literature sliding hip screw is the implant
of choice in Interttrochanteric fractures

CONCLUSION

CONCLUSION
From this study we conclude that DYNAMIC HIP SCREW is a
RELIABLE, VERSATILE and EFFECTIVE device for the treatment
of intertrochanteric fractures.
SUMMARY
Summary
This is a prospective study of 28 patients with
intertrochanteric fractures . All the patients were treated
with dyanamic hip screw fixation . Patients were followed
up for an average period of 9months and the results were
analyzed by using the harris hip scoring system. Among
these patients union occurred in 26 patients, non-union
occurred in 2 patients due to dynamic compression screw
cut out. The analized results with harris hip score system
are excellent in 16 patients, good in 6 patients, fair in 4
patients and poor in 2 patients and these results are almost
similar to other international studies done in the same
method . So from this study we have concluded that
dynamic hip screw fixation in an effective method of
fixation of intertrochanteric fractures
BIBILIOGRAPHY

B I B I L I O G R A P H Y
1. A Comparison between the medoff sliding plate and the compression hip
screw; JBJS (B) 2001, 74, 321-326
2. Adams C I, Robinson C M,Court-Brown C M et al; Prospective control
randomized trial of an intramedullary nail versus dynamic screw and plate
for intertrochanteric fracture of femur; J orthop trauma,2001 , 15:394
3. Atrengart L, Tornkvist H, Fornander P, Thorngren KG, Passanen L,
Lindgren V—A. Randomized study of the compression hip screws and
gamma nail in 426 fractures Clin. Orthop 2002; Aug 401: 209-211
4. A.O; Orthopedic trauma association committee for coding and classification
Fracture and dislocation Compendium; J Orthop trauma 1996; 10(1); 30-35.
5. Ahrengart L, Tornkvisk H, Fornander P, Thangren KG, Pasenen L, A
Randomised study of the compression hip screws and gamma nail in 426
fractures; Clin Orthop Aug 2002; (401); 209-22.
6. Aune et al; Gamma nail Vs Compression screw for trochanteric femoral
fractures; Acta Orthop Scand 1994; 65; 127-130.
7. Babst,Renner,Nikolaus, Bidermann;Clinical results using the trochanteric
stabilization plates along with DHS for internal fixation of unstable
intertrochanteric fractures; Journal of orthopaedic trauma, aug
1998,12(6):392-399
8. Barquet A, Francescoli L,Rienzi D, et al;Intratrochanteric and
subtrochanteric fractures treated with a long gamma nail; J orthop trauma;
2000 ,14:322
9. Barrister G; et al;The fixation and prognosis of throchanteric fractures ; A
Randomized prospective control trial; Clin orthop1990; 254, 242-46
10. Baungaertner M et al ; Intramedullary vs Extramedullary fixation for
treatment of intertrochantric hip fracture; Clin orthop 1998; 348;87-94
11. Bolhofer,Brett R, Russo, Paul R; Results of intertrochanteric fracture
treated with a 135 degree sliding screw with a 2 holed side plate; Journal of
orthopaedic trauma, jan 1999, 13(1): 5-8
12. Bong MR, Patel V, Lesaka K,et al; comparision of a sliding screw with a
trochanteric lateral support plate to an intramedullary hip screw for fixation
of unstable intertrochanteric hip fractures a cadaver study; Jtrauma,2004
56:791;
13. Boyd and griffin: Classification and treatment of trochanteric fractures;
Arch surg; 1949;58; 853-866
14. B.Tengre and J.Kjellander ; Antidiotic prophylaxis in operations on
trochanteric femoral fractures ; Scand j prim health care sep 2002;
20(3);188-92
15. Butt et al, Bryan d; Treatment of unstable trochanteric fractures ; Jbjs
1991; 73-A.
16. Clawson DK, Trochanteric fractures treated by the sliding screw plate
Fixation method. J trauma 1964, 732-752.
17. Docquiet PL, Manche E, Actrique JC, Genletb. B, Complications associated
with gamma nailing; A review of 439 cases; Acta Orthop Belg 2002 Jan
68(3): 251-7.
18. Doherty J.H Jr and Lyden J.P ; Intertrochanteric fractures of the hip treated
with compression screws ; Analysis of problems; Clin Ortho 1979; 141;
184-187.
19. Ecker, et al; JBJS Jan.1995; 57-A, No.1.
20. Elder S , Frankenburg E, Goulet J et al: Biomechanical
evolusion of calcium phosphate cement augumented fixation of
unstable intertrochanteric fracture; J orthop trauma 2000 ,
14:386.
21. Evans E ; The treatment of trochanteric fractures of femur J b j s 1949;
191;53-63
22. Hardy et al ; Use of an intramedullary hip screw compared with a
compression hip screw with a plate for intertrochanteric femoral fractures
JBJS 1998; 80-A ;618-30
23. Harris hip score; Harris WH; JBJS 1969; 51:1.
24. Haidukewych G J, Berry D J; Salvage of fluid internal fixation of
intertrochanteric hip fractures Clin orthop relat res,2003, 412:184
25. Haidukewych G J,Israel T A, Berry D J; Reverse obliquity fracture of the
intertrochanteric region of the femur J B J S,2001, 83A: 643
26. Hardy D C, Drossos K; Sloted intramedullary hip screw nail reduces
proximal mechanical unloading ,Clin orthop relat res,2003, 406:176
27. Herrera A, Domingo L J,Calvo A ,et al; A competitive study of trochanteric
fracture treatment with the gamma nail or the proximal femoral nail Int
orthop ,2002, 26:365
28. Heyse- moore et al; Treatment of intertrochanteric fractures of femur JBJS
1983; 65-B; 262-267.
29. Jacobs et al; Treatment of intertrochanteric hip fractures with a compression
hip screw and a nail plate; J Trauma 1976; 16; 599-603
30.. Janzing H M, Houben B T, Brandt S E, et al; the percutaneous
compressionPlate verses the dhs in the treatment of pertrochanteric hip
fracture. MinimalInvasive treatment reduces operative time and post
operative pain ; J trauma2002 , 52:293
31. . .Jewet et al; One piece angle nail for trochanteric fractures JBJ S1941; 23,
803
32. . Joseph et al;Unstable intertrochanteric fractures of the hip; Joseph H Dimon
Et al; columbus ,Georgia, J B J S apr 1967,49-a, no 3
33. . Kosygan KP, Mohan R Neuman RJ; The Gotfried percutaneous compression
plate compared with conventional classical hip screw fixation of
intertrochanteric fractures of hip JBJS Jan 2002; 84(1); 19-22
34. .. Kyle. RF; Right TM; Biomechanical analysis of the sliding characteristics of
compression screws; JBJS 1980; 62-A; 1308.
35. Larson.S; Freiberg.S; and Hansson L-1, Trochanteric fractures mobility,
complication and mortality in 60% cases treated with the sliding screw
technique Clin. Orthopedics; 1990; 260; 232-241.
36. . Larsson S ; Friberg S and Hansoon L ; Influence of reduction and implant
position on impaction and complications ; Clin orthop 1990; 256; 130-39
37. .Leung KS et al, Gamma nail and dynamic hip screws for pertrochanteric
fractures; A Randomised prospective study in elderly patients JBJS 1992;
74-B; 345-351
38. .Lorich DG, GellerDS,Nielsan JH; .Osteoporotic pertochanteric hip fracture
management and current controversies Instr.course.lect, 2004, 53:441
39. Massie WK: Extracapsular fractures of the hip treated by impaction using a
sliding Nail-plate fixation. Clin Orthop1962; 180-202.
40. .Matlan Y, Dimant A, Moshejee R, Peysee A ;- Avascular necrosis and
related complications following healed osteoporotic intertrochanteric
fractures; Isr Med Association J Jan 2002; 4 (6); 434-7.
41. Miedel R,Ponzer S,TornkvistH et al; The standard gamma nail or the medoff
sliding plate for un stable trochanteric or subtrochanteric fracture a
randamised control trial J B J S, 2005, 87B:681
42. Moroni A, Faldin C, Pegreffi F et al: Dynamic hip screw comparision with
external fixation for treatment of osteoporotic per trochanteric fractures; a
prospective randamised study; JBJS, 2005, 87A:753
43. N.D Chaterjee; Goutham Bhattacharya; Thirthankar Bhattacharya; Dynamic
hip screw and sliding plate for trochanteric fractures of femur; Review July
1991; 34; No:3.
44. .N K karn,G K sing,B shrestha, M P singh; comparission between external
Fixator and sliding hip screw in the management of trochanteric fracture of
Femur in Nepal ; J B J S 2006 (british) 88-b, 1347-1350
45. Parker. M.J; Cutting of dynamic hip screw related to its position; JBJS,
1992; 74-B(4); 625.
46. Ricci, William M: New implant for the treatment of intertrochanteric
Femur fracture ; Techniques in orthopaedics special issue: high usage
Articles, sep 2008 ,23(3): 222/231.
47. .. Schumpelick.W; Jantzen OM; A new principle in orthopaedic treatment of
trochanteric fractures of femur JBJS july 1995; 37-4
48. Schumplik.W and Jansten P.M; A new principle in the operative treatment of
trochnanteric fractures of the femur; JBJS; July 1995, 37-4, 693-69
49. ..Sernbo et al; Unstable intertrochanteric fractures of the hip, Treatment with
Ender`s pin compared with a compression hip screw JBJS Oct 1998; 70-A;
1297-1303.
50. The use of Ender’s pin in extra capsular fractures of hip JBJS 1981; 63;
14-28.
51. Yechiel gotfried ; integrity of the lateral femoral wall in intertrochanteric
Hip fracture an important predictor of a reoperation; J B J S 2007, 89;
2552-2553
52. ..Yeetriel Gotfried; Percutaneous compression plating of pertrochanteric hip
fractures MO; Dept Of Orthopedic surgery; Bnai Zion Medical center, Haifa
Israel.