-
7/27/2019 Anterior Interosseuos Nerve Transfer to the Motor
Branch of the Ulnar Nerve - Haase
1/6
Anterior Interosseous Nerve Transferto the Motor Branch of the
UlnarNerve for High Ulnar Nerve Injuries
Steven C. Haase, MD
Kevin C. Chung, MD
Primary repair of a high ulnar nerve injury results in a
uniformly
poor outcome as a result of the great distance between the site
of
injury and the innervated muscles. In this study the authors
present two cases of high ulnar nerve injuries in adults.
Recon-
struction was performed using the distal branch of the
anterior
interosseous nerve, which was transferred to the distal
motor
branch of the ulnar nerve. This resulted in timely return of
function to the ulnar-innervated intrinsic muscles of the
hand,
which was documented further by electromyography. For high
ulnar nerve injuries, this type of nerve transfer is a much
better
approach than the traditional primary neurorrhaphy.
Haase SC, Chung KC. Anterior interosseous nerve transfer to the
motor
branch of the ulnar nerve for high ulnar nerve injuries. Ann
Plast Surg2002;49:285290
From the Section of Plastic Surgery, Department of Surgery, The
University
of Michigan Medical Center, Ann Arbor, MI.
Received Nov 1, 2001, and in revised form Jan 25, 2002. Accepted
for
publication Jan 25, 2002.
Address correspondence and reprint requests to Dr Chung, Section
of
Plastic Surgery, The University of Michigan Health System, 1500
E.
Medical Center Drive, 2130 Taubman Center, Ann Arbor, MI
48109-0340.
In adults, repair of high ulnar nerve injuries
those near or above the elbowhas historically
yielded unsatisfactory results, with minimal re-
covery of intrinsic muscle function and resultant
claw hand deformity.1 This is true despite the
most meticulous techniques, whether the repair
is primary or secondary, and regardless of
whether a nerve graft is used.2,3 Although sensa-
tion is restored most of the time, recovery of
motor function in the intrinsic muscles of the
hand is almost uniformly poor, especially in the
adult patient. This is principally the result of the
considerable distance between the site of injury
and the muscle motor end plates to be reinner-
vated. During the several months required for the
regenerating axons to traverse this gap, the dener-
vated muscles undergo irreversible atrophy and
fibrosis.
We present 2 patients who illustrate an alterna-
tive method for reconstructing high ulnar nerve
lesions. Transfer of the terminal branch of the
anterior interosseous nerve to the motor branch of
the ulnar nerve at the wrist should reduce greatly
the delay in reinnervation of the intrinsic muscles
and lead to an improved outcome. Our objectives
were to demonstrate the usefulness of this innova-
tive technique and to present the outcomes we
observed, including electromyographic evaluation
of the reconstruction.
Patient Reports
Patient 1
Patient 1 is a 41-year-old right-hand-dominant
carpenter who was involved in a motor vehicle
accident in which he sustained a complex right
upper arm laceration. The ulnar nerve was di-
vided 8 cm above the elbow, as was the medial
head of the triceps muscle (Fig 1). The wound
was closed initially at the referring hospital, and
the patient was sent to our institution for defini-
tive repair of the nerve injury.Within a week of injury, the
patient was taken
to surgery, at which time the ulnar nerve was
transposed anteriorly and repaired. The anterior
interosseous nerve was divided at its most distal
point, where it entered the pronator quadratus
muscle (Fig 2). Guyons canal was opened and
the motor branch of the ulnar nerve was identi-
fied and traced proximally as far as possible,
where it was divided. This motor branch was
tunneled under the flexor tendons and was co-
apted to the transected anterior interosseous
nerve (Fig 3).
Six months after surgery there was evidence of
reinnervation of the intrinsic muscles of the hand
(Fig 4). Most notable was the return of function of
the interosseous (Fig 5), adductor pollicis, and
abductor digiti quinti muscles. Nerve conduction
studies were performed 11 months postopera-
tively. They revealed single motor unit recruit-
ment in the intrinsic muscles of the hand
Copyright 2002 by Lippincott Williams & Wilkins, Inc.
285DOI: 10.1097/01.SAP.0000015429.34256.34
-
7/27/2019 Anterior Interosseuos Nerve Transfer to the Motor
Branch of the Ulnar Nerve - Haase
2/6
innervated normally by the ulnar nerve, consis-tent with
proximal-to-distal regrowth.
Patient 2
Patient 2 is a 52-year-old man who was involved
in a motor vehicle accident, during which he
sustained partial degloving injury of the right
arm. This wound was covered initially with a
skin graft at another institution (Fig 6), and the
patient was referred to our center for definitive
reconstruction.
Approximately 6 weeks after the initial injury,the patient was
taken to surgery for repair of a
15-cm ulnar nerve gap with two strands of sural
nerve graft (Fig 7). Distally, the anterior interosse-
ous nerve was coapted to the motor branch of the
ulnar nerve at the wrist, using a 7-cm sural nerve
graft (Fig 8). The nerve graft was used because of
a substantial amount of tension at the nerve
coaptation site with primary repair. Because flex-
ion of the small finger was already noticeably
weak, transfer of the flexor digitorum profundus
tendon of the small finger to the flexor digitorum
profundus tendon of the middle finger was per-
formed. The elbow wound was covered with a
gracilis muscle free flap.
One year postoperatively, the patients function
of his intrinsic muscles had returned almost
completely. He was able to abduct and adduct the
fingers of his right hand (Fig 9). He has regained
protective sensation along the ulnar side of his
hand. His elbow range of motion is normal (Fig
10).
Discussion
Ulnar nerve injuries at or above the level of the
elbow generally have a poor functional outcome
with traditional repair. Children with similar
injuries have better outcomes, most likely be-
cause of the increased plasticity of their nervous
systems.4
Regardless of age, muscle atrophy begins at the
moment of denervation, and if the elapsed time toreinnervation
is long, the atrophic changes in the
muscle become irreversible. This explains why
functional recovery gets worse as the delay be-
tween the time of injury and the time of recon-
struction increases. Likewise, the more proximal
the nerve lesion, the less likely that adequate
recovery can occur once nerve regeneration
traverses the increased distance to the end organ
targets. Several investigators have sought to slow
down or to stop this muscle atrophy by external
or internal muscle stimulation during the dener-
vated period.5 These kinds of muscle stimulators
are largely experimental at this time.
To obtain a more satisfactory outcome, tendon
transfers have been considered an integral part of
reconstructing high ulnar nerve lesions.6 Without
tendon reconstruction, most patients are left with
clawed, weak hands. We have undertaken an
alternative method of reconstruction in isolated
high ulnar nerve injuries. The terminal branch of
the anterior interosseous nerve is a predominant
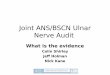
Fig 2. The arrow points to the anterior interosseousnerve at its
entrance into the pronator quadratusmuscle. Note the accompanying
anterior interosseousvessels.
Fig 1. The end of the proximally divided ulnar nervewas held by
a pickup.
Annals of Plastic Surgery Volume 49 / Number 3 / September
2002
286
-
7/27/2019 Anterior Interosseuos Nerve Transfer to the Motor
Branch of the Ulnar Nerve - Haase
3/6
motor nerve that innervates the pronator quadra-
tus muscle and sends a few sensory branches to
the wrist joint. This nerve can be transferred to
the distal motor branch of the ulnar nerve,
thereby greatly reducing the necessary distance
for axonal regeneration to the intrinsic muscles.
This type of nerve transfer was brought to our
attention by Mackinnon and Novak.7 A report
also exists in the Chinese literature that used
cadaveric analyses to demonstrate the feasibility
of this approach.8 Several features of this transfer
are attractive. The donor defect is essentially
negligible. The intact pronator teres muscle is
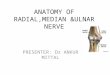
Fig 3. (A) The arrow points to therepair between the
anteriorinterosseous nerve and the motorbranch of the ulnar nerve.
(B)Diagram illustrating the anteriorinterosseous nerve transfer to
the
motor branch of the ulnar nerve. N nerve; M muscle.
Fig 4. The right reconstructed hand hasrecovered intrinsic
muscle function.
Fig 5. The patient is able to abduct and adduct the fingers.
Haase and Chung: Anterior Interosseous Nerve Transfer
287
-
7/27/2019 Anterior Interosseuos Nerve Transfer to the Motor
Branch of the Ulnar Nerve - Haase
4/6
sufficient to pronate the forearm. Because the
transferred nerve is a pure motor nerve, there
should be no competition by sensory fibers for
motor pathways during reinnervation.
Reconstruction of this injury should provide
for sensation in the ulnar nerve distribution as
well. Fortunately, return of sensation is some-
what less problematic, because the sensory recep-
tors do not depreciate to the extent that muscle
atrophy occurs in motor units. Therefore, repair
of the ulnar nerve by primary repair or nerve graft
at the site of injury is still required to direct the
sensory axons to their destination in the hand.
Some groups have sought to shorten the recovery
time for these nerve pathways as well, proposing
a transfer of the median nerve sensory branch to
the ulnar sensory nerve at the wrist.9 This ap-
proach may leave the patient with an insensate
palm. We think that return of sensation down the
native pathways of the ulnar nerve, despite the
delay, should suffice to provide at least protective
sensation in most cases.
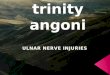
Fig 6. Skin graft over the elbow wound.
Fig 7. Proximal ulnar nerve repair using two strands ofsural
nerve graft.
Fig 8. (A) The arrow points to the motor branch of the ulnar
nerve. (B) The anterior interosseous to motor branch ofthe ulnar
nerve was repaired using sural nerve graft (arrow).
Fig 9. The patient is able to abduct and adduct the fingers.
Annals of Plastic Surgery Volume 49 / Number 3 / September
2002
288
-
7/27/2019 Anterior Interosseuos Nerve Transfer to the Motor
Branch of the Ulnar Nerve - Haase
5/6
Helpful adjuncts to this procedure are also
illustrated in these patient reports. Transfer of the
flexor profundus tendon of the small finger
and/or ring finger to that of the middle finger
recovers function that is lost with denervation ofthe ulnar
portion of that muscle belly. Reinner-
vation of the more proximal ulnar-innervated
muscles (i.e., flexor carpi ulnaris) should occur in
a more traditional fashion after primary or sec-
ondary nerve repair at the elbow because the
connections to these more proximal muscles may
still be intact.
Reports of similar nerve transfer techniques
now exist in the literature. Transfer of a single
motor fascicle from the ulnar nerve to the biceps
muscle has restored elbow flexion in patients
with upper brachial plexus injuries.10 In an ani-
mal model, transfer of part of the ulnar nerve to a
transected median nerve has restored consider-
able function without substantial donor deficit.11
Certainly, the possibilities for future application
of this concept are not yet fully explored.
A valid criticism of this report is the inability to
rule out any MartinGruber connections in these
patients. However, anatomic studies have failed
to find these connections in the distal forearm; all
connections occurred more proximally.12 Al-
though no nerve conduction studies were ob-
tained preoperatively, our patients had no
clinical evidence of intrinsic muscle functionafter the initial
ulnar nerve transection. Even if
subclinical connections had been present, they
would be severed with the distal transection of
the ulnar nerve at Guyons canal. Any reinnerva-
tion observed must be the result of regeneration
through the nerve connection that we created.
We succeeded in restoring intrinsic muscle
function in 2 patients who would have had neg-
ligible recovery by traditional means. For high
ulnar nerve injuries, the anterior interosseous
nerve transfer to the deep motor branch of the
ulnar nerve should be the preferred method for
intrinsic muscle reinnervation.
References
1 Gaul JS. Intrinsic motor recoverya long-term study of
ulnar nerve repair. J Hand Surg [Am] 1982;7A:502508
2 Barrios C, Amillo S, de Pablos J, et al. Secondary repair
of
ulnar nerve injury. Acta Orthop Scand 1989;61:46 49
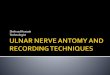
Fig 10. (A, B) Return of normal elbow flexion with a healed
gracilisfree flap muscle.
Haase and Chung: Anterior Interosseous Nerve Transfer
289
-
7/27/2019 Anterior Interosseuos Nerve Transfer to the Motor
Branch of the Ulnar Nerve - Haase
6/6
3 Vastamki M, Kallio PK, Solonen KA. The results ofsecondary
microsurgical repair of ulnar nerve injury.J Hand Surg [Br]
1993;18B:323326
4 Allan CH. Functional results of primary nerve repair.Hand Clin
2000;16:6772
5 Williams HB. A clinical pilot study to assess functionalreturn
following continuous muscle stimulation afternerve injury and
repair in the upper extremity using acompletely implantable
electrical system. Microsurgery1996;17:597 605
6 Trevett MC, Tuson C, de Jager LT, et al. The functionalresults
of ulnar nerve repair: defining the indications fortendon transfer.
J Hand Surg [Br] 1995;20B:444 446
7 Mackinnon SE, Novak CB. Nerve transfers: new optionsfor
reconstruction following nerve injury. Hand Clin 1999;15:643666
8 Wang Y, Zhu S, Zhang B. [Anatomical study and
clinicalapplication of transfer of pronator quadratus branch
ofanterior interosseous nerve in the repair of thenar branch
of median nerve and deep branch of ulnar nerve.] [In
Chinese.] Chung-Kuo Hsiu Fu Chung Chien Wai Ko Tsa
Chih 1997;11:335337
9 Battiston B, Lanzetta M. Reconstruction of high ulnar
nerve lesions by distal double median to ulnar nerve
transfer. J Hand Surg [Am] 1999;24A:11851191
10 Sungpet A, Suphachatwong C, Kawinwonggowit V, et al.
Transfer of a single fascicle from the ulnar nerve to the
biceps muscle after avulsions of upper roots of the bra-chial
plexus. J Hand Surg [Br] 2000;25B:325328
11 Lutz BS, Chuang DCC, Chuang SS, et al. Nerve transfers to
the median nerve using parts of the ulnar and radial
nerves in the rabbit effects on motor recovery of the
median nerve and donor nerve morbidity. J Hand Surg [Br]
2000;25B:329335
12 Shu HS, Chantelot C, Oberlin C, et al. MartinGruber
communicating branch: anatomical and histological
study. Surg Radiol Anat 1999;21:115118
Annals of Plastic Surgery Volume 49 / Number 3 / September
2002
290