Embed Size (px)
Citation preview

Integrated Systems and Technologies
Antiangiogenic Agent Sunitinib Transiently Increases TumorOxygenation and Suppresses Cycling Hypoxia
Shingo Matsumoto1, Sonny Batra1,3, Keita Saito1, Hironobu Yasui1,4, Rajani Choudhuri1,Chandramouli Gadisetti1,5, Sankaran Subramanian1, Nallathamby Devasahayam1,Jeeva P. Munasinghe2, James B. Mitchell1, and Murali C. Krishna1
AbstractStructural and functional abnormalities in tumor blood vessels impact the delivery of oxygen and nutrients to
solid tumors, resulting in chronic and cycling hypoxia. Although chronically hypoxic regions exhibit treatmentresistance, more recently it has been shown that cycling hypoxic regions acquire prosurvival pathways.Angiogenesis inhibitors have been shown to transiently normalize the tumor vasculatures and enhance tumorresponse to treatments. However, the effect of antiangiogenic therapy on cycling tumor hypoxia remainsunknown. Using electron paramagnetic resonance imaging and MRI in tumor-bearing mice, we have examinedthe vascular renormalization process by longitudinally mapping tumor partial pressure of oxygen (pO2) andmicrovessel density during treatments with a multi-tyrosine kinase inhibitor sunitinib. Transient improvementin tumor oxygenation was visualized by electron paramagnetic resonance imaging 2 to 4 days followingantiangiogenic treatments, accompanied by a 45% decrease in microvessel density. Radiation treatment duringthis time period of improved oxygenation by antiangiogenic therapy resulted in a synergistic delay in tumorgrowth. In addition, dynamic oxygen imaging obtained every 3 minutes was conducted to distinguish tumorregions with chronic and cycling hypoxia. Sunitinib treatment suppressed the extent of temporal fluctuations intumor pO2 during the vascular normalization window, resulting in the decrease of cycling tumor hypoxia.Overall, the findings suggest that longitudinal and noninvasive monitoring of tumor pO2 makes it possible toidentify a window of vascular renormalization to maximize the effects of combination therapy with anti-angiogenic drugs. Cancer Res; 71(20); 6350–9. �2011 AACR.
Introduction
Tumors can grow up to 2 to 3 mm3 in size by relying onpassive supplies of nutrients and oxygen. For further growth,tumors activate angiogenesis pathways to develop newvascular networks (1). In normal processes such as woundhealing, angiogenesis is tightly regulated and creates abalance between pro- and antiangiogenic factors. However
in tumors, the balance is tilted toward promoting angio-genesis, causing the development of architecturally andfunctionally abnormal vasculature (2, 3). The aberrant tumorblood vessel is neither as efficient nor well organized indelivering oxygen and nutrients (4–6). The consequent hyp-oxic and acidotic microenvironment diminishes tumorresponsiveness to treatments (7).
Tumor hypoxia can be categorized into 2 types: chronic orcycling hypoxia. Chronic hypoxia exists in tumor regionsbeyond the diffusion distance of oxygen. Longitudinal oxy-gen gradient, where the vascular oxygen concentrationremains low, in tumor blood vessels makes the radial oxygendiffusion distance shortened, leading to chronic hypoxia (8).Cycling hypoxia, also known as acute or intermittent hyp-oxia, has been attributed to fluctuations in tumor perfusionand erythrocyte flux (9, 10). Chaplin and colleagues reportedin preclinical studies that at least 20% of solid tumor cellsexperience cycling hypoxia (11). One consequence of cyclinghypoxia is increased resistance to treatments by conferringtumor cells and endothelial cells of tumor blood vessels withenhanced prosurvival pathways (12, 13). These observationsmake cycling hypoxia a common hallmark existing in atumor microenvironment. Baudelet and colleagues havenoninvasively observed the characteristic fluctuations oftransversal relaxation time (T2*)-weighted MRI signal insolid tumors attributed to physiologic noise that in turn
Authors' Affiliations: 1Radiation Biology Branch, Center for Cancer Re-search, National Cancer Institute; 2National Institute of Neurological Dis-order and Stroke, NIH; 3Howard Hughes Medical Institute-–NIH,Bethesda, Maryland; 4Laboratory of Radiation Biology, Department ofEnvironmental Veterinary Sciences, Graduate School of Veterinary Med-icine, Hokkaido University, Sapporo, Japan; and 5Department of Obstet-rics/Gynecology & Reproductive Biology, Michigan State University,Grand Rapids, Michigan
Note: Supplementary data for this article are available at Cancer ResearchOnline (http://cancerres.aacrjournals.org/).
S. Matsumoto and S. Batra contributed equally to this work.
S. Batra is a Howard Hughes Medical Institute-NIH research scholar
Corresponding Author: Murali C. Krishna, Radiation Biology Branch,Center for Cancer Research, National Cancer Institute, NIH, Building10, Room B3B69, 9000 Rockville Pike, Bethesda, MD 20892. Phone:1-301-496-7511; Fax: 1-301-480-2238; E-mail: [email protected]
doi: 10.1158/0008-5472.CAN-11-2025
�2011 American Association for Cancer Research.
CancerResearch
Cancer Res; 71(20) October 15, 20116350
Cancer Research. on September 17, 2020. © 2011 American Association forcancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 30, 2011; DOI: 10.1158/0008-5472.CAN-11-2025

may correlate with instability of tumor oxygenation (14).These fluctuations were suppressed by treatments includingcarbogen combined with nicotinamide and flunarizine. Al-though the signal interpretation of T2*-weighted MRI iscomplex with regard to the absolute value of partial pressureof oxygen (pO2), such noninvasive and longitudinal imagingapproaches to study the temporal dynamics of pO2 would beuseful to identify effective treatments targeting cyclingtumor hypoxia.Antiangiogenic drugs have been shown to exhibit efficacy in
selectively destroying tumor blood vessels in experimentalanimals and in humans (1). Although as a monotherapy,antiangiogenic agents yielded modest success in human trials,they are being explored in combination therapies with cyto-toxic cancer therapies (15, 16). Although decrease in deliveryof oxygen and therapeutics to the tumor should be expectedon antiangiogenic treatments, numerous reports point to thesignificant benefit in patient survival when used with chemo-therapy or radiotherapy, suggesting an improvement of tumoroxygenation and perfusion (17–19). To explain this paradox,Jain and colleagues put forward a hypothesis that tumorvasculature transiently normalizes during the course of anti-angiogenic treatments, where the immature and ineffectivevessels get pruned, making the residual vessels structurallycompetent with improved function (20). Further researchwas carried out to serially monitor changes in the vascularnormalization process that identify a window, in whichchemotherapy or radiotherapy was delivered with maximaltherapeutic gain (17, 21, 22). A major challenge identified inthis effort is the development of noninvasive imaging biomar-kers of the vascular normalization process in tumors (20).Optimization of antiangiogenic therapies is complicated bythe fact that these agents are not directly cytotoxic to malig-nant cells, making tumor growth kinetics an unreliable ap-proach to identify the vascular normalization window (23).Useful criteria for an imaging modality would be noninvasiveand capable of longitudinally monitoring tumor physiologyand would provide a surrogate quantitative biomarker fortumor blood flow/perfusion (18, 20, 22).Electron paramagnetic resonance (EPR) is a spectroscopic
technique similar to nuclear MRI but detects paramagneticspecies. Recent availability of triarylmethyl (TAM) radicalderivatives as in vivo compatible paramagnetic tracers madeEPR imaging (EPRI) capable of mapping tissue pO2 (24, 25).The sequential imaging with EPRI for tissue oxygen andconventional MRI for anatomy in a system operating at acommon resonance frequency provides anatomically over-laid pO2 maps with tumor microvessel density maps (25). Inthe present study, we report the results from the imagingexperiments monitoring tumor pO2 to identify the tumorvascular renormalization window and optimize sequence ofcombination therapy of antiangiogenic drugs and radiation.The normalization window in tumor oxygenation inresponse to antiangiogenic treatment was noninvasivelyvisualized, and radiation treatment during this narrow timeperiod resulted in synergistic tumor growth delay. Further-more, the temporal resolution of EPRI made it feasible toobtain 3-dimensional (3D) pO2 maps every 2to 3 minutes
and enabled to distinguish the phenomenon of cyclinghypoxia (12, 26). The results show that the consequenceof sunitinib treatment is a decrease in the extent of cyclinghypoxia in tumors.
Materials and Methods
Tumor implantationWe established SCCVII tumors (obtained from Dr. T.
Phillips, UCSF, San Francisco, CA, and was tested in 2011by RADIL using a panel of microsatellite markers) in mousehind leg as described previously (25). Tumor-bearing femaleC3H mice were treated daily with oral administration of 50-mg sunitinib (LC Laboratories) per kg body weight 6 or10 days after tumor implantation. X-ray irradiation (10 Gy)was delivered 6 or 10 days after tumor implantation using anX-RAD 320 (Precision X-ray Inc.) with or without pretreat-ment of sunitinib. We carried out all our procedures incompliance with the Guide for the Care and Use of LaboratoryAnimal Resources (27), and experimental protocols wereapproved by the National Cancer Institute Animal Careand Use Committee.
EPRI for pO2
Technical details of the EPR scanner and oxygen imagereconstruction were described in Supplementary Data S1.Parallel coil resonators tuned to 300 MHz were used for EPRIand MRI. After the animal was placed in the resonator, TAM(1.125 mmol/kg bolus) was injected intravenously under iso-flurane anesthesia. The repetition time was 6.0 microseconds.The free induction decay (FID) signals were collected follow-ing the radiofrequency excitation pulses under a nested loop-ing of the x, y, and z gradients and each time point in the FIDunderwent phase modulation enabling 3D spatial encoding.Because FIDs last for 1 to 5 microseconds, it is possible togenerate a sequence of T2* maps, that is, EPR line width maps,which linearly correlate with local concentration of oxygenand allows pixel-wise estimation of pO2.
MRI for anatomy and blood volumeMRI scans were conducted using a 7T scanner (Bruker
BioSpin MRI GmbH). T2*-weighted anatomic images wereobtained using a fast spin echo sequence (RARE) with anecho time of 13 milliseconds, repetition time of 2,500 milli-seconds, RARE factor 8, and resolution of 0.125 � 0.125 mm.For convenience of coregistration with EPRI, all MRI imageshad the same slice thickness of 2 mm and field of view of3.2 cm with 16 slices or 2.8 cm field of view with 14 slices. Forblood volume calculation, spoiled gradient echo sequenceimages were collected before and 5 minutes after ultrasmallsuperparamagnetic iron oxide (USPIO; BioPAL Inc., colloidalsize of 30 nanoseconds) injection (1.2 mL/g body weight) withthe following parameters: matrix¼ 256� 256; echo time¼ 5.4milliseconds; and repetition time ¼ 250 milliseconds. Thepercentage of tumor blood volume was estimated as describedpreviously (28). Coregistration of EPRI and MRI images wasaccomplished using code written in MATLAB (MathWorks) asdescribed previously (25).
Sunitinib Suppresses Cycling Tumor Hypoxia
www.aacrjournals.org Cancer Res; 71(20) October 15, 2011 6351
Cancer Research. on September 17, 2020. © 2011 American Association forcancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 30, 2011; DOI: 10.1158/0008-5472.CAN-11-2025

Immunohistochemical analysisTumor tissues were excised on hour after intravenous
injection of a pimonidazole (60 mg/kg). Tumor tissues werefixed with 4% paraformaldehyde and frozen, and 10 mm thicksections were obtained. After blocking nonspecific bindingsites, the slides were covered by CD31 antibody (BD Bios-ciences; 1:250) combined with aSMA antibody (Abcam Inc.;1:250) or rabbit anti-pimonidazole antisera (Natural Pharma-cia International, Inc.; 1:250) overnight at 4�C. The sectionswere incubated with Alexa Fluor 488 anti-rat and Alexa Fluor555 anti-rabbit secondary antibody (Invitrogen; 1:500).
Statistical analysisAll results were expressed as the mean � SEM. The differ-
ences in means of groups were determined by the Student ttest. The minimum level of significance was set at P < 0.05.
Results
Tumor pO2 can be noninvasively and longitudinallymonitored by EPRI
The collisional interaction between molecular oxygen andthe paramagnetic TAM leads to broadening of the EPR
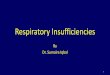
Figure 1. Longitudinal andnoninvasive monitoring of tumorpO2 by EPRI and effects ofantiangiogenic drug. A, MRIanatomic images (top) and EPRoxygen images (bottom) of a C3Hmouse, bearing a SCC VII tumor atthe right leg, show an increasinghypoxic region (pO2 < 10 mm Hg,blue color) along with its growth.Blood volume image by MRI withUSPIO revealed promotedangiogenesis in this tumor(top right). Immunohistochemicalanalysis (bottom right) confirmed ahigh density of microvasculature(CD31, green), which is poorlycovered with perivascular cells(aSMA, red). B, antiangiogenictreatment with sunitinib, initiatedat the early stage of tumor,delayed SCC tumor growth.Tumor pO2 levels were transientlyhigher than the day-matchedcontrol tumors during the 2 to6 days after daily sunitinibtreatment despite theapproximately 40% reduction intumor blood volume (third row).Histology (bottom left) showed asignificant reduction inmicrovascular density withoutchanging the number ofperivascular cells. C, pO2 changesin tumors in sunitinib-treated(red circles) and -untreated(blue circles) mice. *, P < 0.05;**, P < 0.01. D, blood volume inSCC tumors in control andsunitinib-treated mice. Sunit,sunitinib. Sunit 6-4, 4th day aftertreatment of a tumor 6 days afterimplantation.
Matsumoto et al.
Cancer Res; 71(20) October 15, 2011 Cancer Research6352
Cancer Research. on September 17, 2020. © 2011 American Association forcancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 30, 2011; DOI: 10.1158/0008-5472.CAN-11-2025

spectral line widths of TAM. By extracting the pO2-dependentEPR line width distribution of TAM, an in vivo pO2 map can begenerated where TAM is present at detectable levels (25).Figure 1A (top) shows anatomic images taken on days 8, 10,and 12 and an image representing the microvessel density(MRI) taken on day 12 of a squamous cell carcinoma (SCC)tumor–bearing control (untreated) mouse. The correspondingpO2 maps from the same time points are shown in Fig. 1A(bottom), along with an independent immunohistochemicalanalysis of microvessel density (CD31, green) and pericytes(aSMA, red). Longitudinal pO2 imaging showed that theextent of hypoxia increased with tumor size. The hypoxicfraction (pO2 <10 mmHg) was 24.2% � 6.8% on day 8 andincreased to 40.9% � 6.1% and 47.4% � 8.3% on days 10 and12, respectively. Blood volume images obtained by MRI usingthe blood pool contrast agent USPIO as an in vivo marker of
microvessel density (28) showed substantial vascularization inthis tumor. However, immunohistochemical analyses indicat-ed that the tumor blood vessels had inadequate pericytecoverage, suggesting inefficient oxygen delivery by these ves-sels (4, 6), consistent with the hypoxic nature of this tumor.
Early treatment with an antiangiogenic drug delaysprogression of tumor hypoxia
In earlier preclinical studies with antiangiogenic drugs, arenormalization of tumor vasculature along with a transientimprovement in oxygen status was observed (17, 22). Wehypothesized that if the vascular normalization is occurredby sunitinib treatment, tumor oxygenation improves simulta-neously with reduced vascular microvessel density underthe assumption of unchanged cellular oxygen consumption.To noninvasively study this phenomenon, daily sunitinib
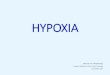
Figure 2. Tumor pO2 and blood volume imaging before and after antiangiogenic treatment initiated at the later stage of tumor. A, initiation of antiangiogenictreatment at the later stage of tumor improved tumor oxygenation (top) and reduced tumor blood volume (bottom) without a significant change intumor size. B and C, frequency histograms (percentage of voxels with a given pO2 and blood volume) before and 4 days after antiangiogenic treatmentshowed a clear right shift in pO2 but a shift in blood volume. D, quantitation of pO2 changes in sunitinib-treated and control mice. *, P < 0.05. E, tumorblood volume decreased approximately 45% 4 days after treatment initiated at the later stage of tumor. Sunit, sunitinib. Sunit 10-4, 4th day after treatment of atumor 10 days after implantation.
Sunitinib Suppresses Cycling Tumor Hypoxia
www.aacrjournals.org Cancer Res; 71(20) October 15, 2011 6353
Cancer Research. on September 17, 2020. © 2011 American Association forcancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 30, 2011; DOI: 10.1158/0008-5472.CAN-11-2025

treatmentwas initiated at an early stage before tumors becamehypoxic (6 days after SCC tumor implantation, hypoxic fraction<3%). In mice receiving early antiangiogenic treatment initi-ation, sunitinib significantly delayed the SCC tumor growth(Fig. 1B). When the pO2 status and microvessel density wereevaluated by consecutive EPRI and MRI scans, a differentpattern emerged. The pO2 levels in treated tumors weretransiently higher than in untreated mice (P < 0.01) followedby a monotonous decrease (Fig. 1C), whereas approximately40% reduction in the microvessel density as assessed by MRI(Fig. 1D) and immunohistochemistry (Fig. 1B, bottom) wasobserved after 2 to 6 days of sunitinib treatment. The increasein tumor pO2, which was accompanied by a decrease inmicrovascular density, after sunitinib treatment comparedwith untreated controls may be attributed to a phenomenonknown as transient vascular renormalization, where the de-livery of nutrients including oxygen improves as a result ofpruning immature blood vessels and the subsequent recruit-ment of pericytes (19, 22). Further continuation of sunitinibtreatment resulted in hypovascularity for up to 2 weeks afterinitiating treatment, at which time the tumors became severelyhypoxic compared with the size-matched control tumors.
Antiangiogenic treatment at a later stage improvestumor oxygenation by vascular normalization
In addition to vascular normalization, sunitinib-inducedsuppression of tumor growthmight contribute to the improved
tumor oxygenation. To investigate this, sunitinib treatmentwas initiated at a later stage (SCC day 10), when the tumorsbecame significantly hypoxic (hypoxic fraction�35%). Figure 2shows images of tumor pO2 and microvessel density from SCCtumors treated with sunitinib 10 days after tumor implanta-tion. day 0 corresponds to images before treatment. The otherimages were taken on days 2 and 4 after initiating sunitinibtreatment. Even in this tumor, which had significant hypoxicregions, tumor oxygen levels increased 2 and 4 days aftersunitinib treatment compared with oxygen level before treat-ment (Fig. 2A, top). It should be noted that no significantchange in tumor size occurred during these time points (835�44 mm3 before treatment and 822 � 89.5 mm3 4 days aftertreatment), despite a 45% reduction in tumor blood volume[Fig. 2A (bottom) andE]. In frequency histograms of this tumor,a right shift of tumor pO2 was observed (Fig. 2B) with aconcomitant left shift of the blood vessel density (Fig. 2C).The transient increase in tumor pO2was quantified (Fig. 2D), aswas the loss in microvessel density (Fig. 2E).
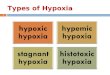
In 2 instances (Figs. 2A and 3A), the tumor size and shapedifference between before and 4 days after sunitinib treatmentwere less than 3%. This permitted monitoring individualvoxel-based changes in pO2 (Fig. 3A) and blood volume(Fig. 3B) before and after sunitinib treatment. In the scatterplot of data from these 2 experiments (Fig. 3C), a left shift ofthe data in each row from the untreated (left column) tothe treated (right column) indicates a decrease in tumor
Figure 3. Voxel-based trace of changes in tumor pO2 (A) and blood volume (B) of representative 2 mice, where the tumor size and shape were the samebefore and 4 days after sunitinib treatment initiated 10 days after tumor implantation. C, scatter plots of pO2 versus blood volume in before (left column)and after sunitinib-treated (right column) mice. The data were classified into 4 groups as follows: (i) pO2 more than 10 mm Hg before and after 4 dayssunitinib treatment (black circles); (ii) pO2 less than 10 mm Hg before and after treatment (red circles); (iii) pO2 less than 10 mm Hg before and pO2 more than10 mm Hg after treatment (blue circles); and (iv) pO2 more than 10 mm Hg before and pO2 less than 10 mm Hg after treatment (green circles).
Matsumoto et al.
Cancer Res; 71(20) October 15, 2011 Cancer Research6354
Cancer Research. on September 17, 2020. © 2011 American Association forcancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 30, 2011; DOI: 10.1158/0008-5472.CAN-11-2025

microvessel density and an upward shift of the data from theleft column to the right column in each row would indicate animprovement in tumor pO2. The analyzed data were classifiedinto 4 groups on the basis of pO2 levels before and aftersunitinib treatment as follows: (i) pO2 levels more than 10 mmHg before and after treatment (black circles), which mayrepresent tumor regions that are normoxic and covered withfunctional vessels; (ii) pO2 levels less than 10 mm Hg beforeand after sunitinib treatment, which may represent hypoxicregions whose vasculature was not responsive to sunitinibtreatment (red circles); (iii) pO2 levels less than 10 mm Hgbefore and more than 10 mm Hg after sunitinib treatment(blue circles), which may represent regions with normalizedvasculature after sunitinib treatment; and (iv) pO2 levels morethan 10 mm Hg before and less than 10 mm Hg after sunitinibtreatment (green circles), regions where sunitinib may havedestroyed the vasculature substantially such that the effect ofthe hypovasculature may have overwhelmed the beneficialeffect of vascular normalization. The results frommouse 1 (thesamemouse shown in Fig. 2) showed that a significant fractionof pixels in the tumor that was hypoxic before sunitinib
treatment (blue circles) displayed pO2 increase to a level morethan 10 mm Hg with a concomitant decrease in blood vesseldensity. In addition, the average pO2 values of all groupsshowed an increase, suggesting a global vascular normaliza-tion in the tumor (Supplementary Data S2). Similar resultswere observed in mouse 2 (Fig. 3C), but the improvement intumor pO2 was relatively limited and also some regions ofsignificant hypoxia were established after treatment (greencircles).
Vascular normalization with sunitinib increases oxygendiffusion distance and reduces hypoxic fraction intumors
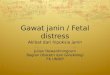
The noninvasive observation of transiently improved tumoroxygenation by EPRI after antiangiogenic treatment wasfurther validated by histologic analysis. Immunohistochemicalevaluation of pimonidazole (Fig. 4A), a hypoxia marker, showsthat the hypoxic fraction of SCC tumors decreased by 9% and7% after 4 days of sunitinib treatment initiated at days 6 and10, respectively. Microvascular density (CD31 staining, Fig. 4B)decreased 40% 4 days after sunitinib treatment, whereas no
Figure 4. Vascular normalizationwith sunitinib increases oxygendiffusion distance and reduceshypoxic fraction in tumors. A,immunostaining of hypoxiamarker pimonidazole ofrepresentative tumors. Left,untreated control (SCC day 10);middle, 4 days after sunitinibtreatment initiated on SCCday 6; and right, 4 days aftersunitinib treatment initiated onSCC day 10. B, double staining ofendothelial cell (CD31, green) andhypoxia (pimonidazole, red) showelongated oxygen gradients after4 days sunitinib treatment.C, summary ofimmunohistochemical analysis.*, P < 0.05; **, P < 0.01. Sunit,sunitinib; pimonidazole, pimo.
Sunitinib Suppresses Cycling Tumor Hypoxia
www.aacrjournals.org Cancer Res; 71(20) October 15, 2011 6355
Cancer Research. on September 17, 2020. © 2011 American Association forcancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 30, 2011; DOI: 10.1158/0008-5472.CAN-11-2025

significant change was observed in the number of pericytes(aSMA, Fig. 4C). The average distance between microvessels(CD31) and the edge of hypoxic regions (pimonidazole) wasmeasured to represent oxygen gradient distance and wasdetermined to be 75 mm in untreated control tumors, whichincreased to 110 mm 4 days after sunitinib treatment (Fig. 4Band C). These histologic results are consistent with previousobservations and support noninvasive assessment of transientvascular normalization and resultant improvement of tumoroxygenation after antiangiogenic treatment.
Transient increase in tumor oxygenation byantiangiogenic treatment enhances outcome ofradiotherapy
As hypoxic cells show resistance to radiation, a transientincrease in tumor oxygenation has a potential to improvetreatment effect of radiation. A combination of 10 Gy radiationat the end of 4 days sunitinib treatment synergistically delayedthe tumor growth (8 days) compared with monotherapy ofradiation (2-day delay) or 4 days of sunitinib treatment (2-daydelay, Fig. 5). Collectively, microenvironmental changes result-ing from normalization of tumor blood vessels by antiangio-genic treatment contributed to the augmented efficacy ofradiotherapy during the window of improved tumor oxygen-ation that can be directly monitored with EPRI.
Vascular normalization with sunitinib suppressescycling hypoxia
In recent studies (12, 26), the temporal fluctuations oftumor pO2 in the various tumor subregions were examinedto distinguish chronically hypoxic tumor regions from tran-siently hypoxic regions, a phenomenon known as cyclinghypoxia. It was found that there was a significant spatiotem-poral heterogeneity in the dynamics of tumor pO2. To examinethe effect of antiangiogenic agents in modifying these spatio-temporal fluctuations in tumor pO2, dynamic oxygen imagingexperiments were carried out in treated and untreated mice.Figure 6A shows a series of snapshot EPRI images taken every3 minutes over a period of 30 minutes in untreated animals.For the 4 regions of interest (ROI), marked ROI-1 to ROI-4, thetemporal pO2 changes are displayed in Fig. 6B. The resultsshow that there were no significant temporal fluctuations in
ROI-2, typical of chronically hypoxic regions, whereas ROIs 1, 3,and 4 displayed features characteristic of cycling hypoxia, withpO2 fluctuations of approximately 20 mm Hg were noticed.When similar experiments were carried out on sunitinib-treated animals and the various ROIs examined (Fig. 6C), itcan be seen that in addition to the chronically hypoxic region,ROI-2, which displays steady levels of pO2 less than 10 mmHg,ROIs 1, 3, and 4 show an improved and more stable pO2 levels(Fig. 6D). Similar results were obtained in 4 independent micefor both untreated and sunitinib-treated groups. Figure 6Eshows SDs of tumor pO2 (pO2 SD) maps of the treated anduntreated mice calculated from the 10 images taken in the 30-minute time window. This parametric image can visualize thelocations and extent of temporal pO2 fluctuations, and regionswith high pO2 SD (>6 mmHg) were observed in the largemajority of untreated tumors whereas limited area of highpO2 SD in sunitinib-treated tumors. Averaged pO2 SD values intumor regions decreased by 25% 4 days after sunitinib treat-ment compared with size-matched untreated control tumors(Fig. 6E, right). This observation from EPRI experiments pro-vides new information that the vascular normalization byantiangiogenic treatment minimizes cycling hypoxia resultingfrom temporal pO2 instability.
Discussion
The transient vascular normalization resulting fromantiangiogenic cancer treatments presents a window of op-portunity to augment treatment with radiation and/or che-motherapy to realize additive or synergistic responses intreatment (20–22). Noninvasive imaging biomarkers thatcan quantitatively and longitudinally monitor physiologicchanges in tumor microenvironment in response to antian-giogenic therapies will be of significant value where the classicendpoints in cancer treatment such as tumor shrinkage maynot apply (23, 29). Such capabilities will be especially usefulwhen planning combination therapies (1, 22). By using theimage contrast provided by molecular oxygen to a paramag-netic tracer such as TAM, EPRI can provide quantitative mapsof tissue pO2, a key determinant of radiotherapy. Anatomicguidance with MRI allows the spatial coregistration of tissue/tumor oxygenation in a straight forward manner (25).
Figure 5. Transient increase intumor oxygenation byantiangiogenic treatmentenhances outcome ofradiotherapy. Tumor growthkinetic study was carried out ongroups of tumor-bearing mice thatinclude untreated control (blackcircles), single 10 Gy radiation atSCC day 10 (blue circles), 4 dayssunitinib treatment during 6 to10 days after SCC implantation(red circles), and 4 days sunitinibfollowed by single 10 Gy radiation(green circles). Sunit, sunitinib. p.o., per os.
Matsumoto et al.
Cancer Res; 71(20) October 15, 2011 Cancer Research6356
Cancer Research. on September 17, 2020. © 2011 American Association forcancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 30, 2011; DOI: 10.1158/0008-5472.CAN-11-2025

The results from the present imaging and histologic studiesshow that, after starting sunitinib treatment, there is a timewindowwhen tumor oxygenation in treatedmice is significantlyhigher than in the untreated controls. The improved oxygen-ation, which is accompanied by a decrease in blood vesseldensity, suggests that the residual blood vessels had improvedfunction in terms of delivering oxygen and nutrients, in agree-ment with earlier reports (17, 22, 30). Interestingly, Ansiaux andcolleagues reported that antiangiogenic drugs SU5416 andvandetanib increased tumor oxygenation by a decrease inoxygen consumption (31, 32). Such other mechanism of tran-sient increase in tumor oxygenationmay be also involved in thecase of sunitinib and further investigations remain required.Evenwhen sunitinib treatmentwas started at a later stage in thetumor growth where there is already significant hypoxia, asimilar profile of improved oxygenation was observed. The largeproportion of hypoxic tumor regions that became oxygenatedafter sunitinib treatment (blue circles in Fig. 3C) representtumor regions that can be expected to be responsive to radio-therapy. In addition, a synergistic delay in tumor growth wasobserved when radiation was delivered during the improvedtumor oxygenation after 4 days of sunitinib administration
(Fig. 5). These results support the capability of EPRI to longi-tudinally and noninvasively visualize tumor pO2, allowing us tomonitor and adjust the impact of antiangiogenic drugs onindividual tumors and optimize benefit of combined therapyof antiangiogenesis and other treatments.
Cycling hypoxia is now a well-recognized hallmark of solidtumors (9, 12). The cycle of hypoxia/normoxia induces accu-mulation of hypoxia-inducible transcription factor-1 in bothtumor cells as well as supporting endothelial cells, promotescancer cell phenotypes with enhanced prosurvival pathways,and acquires resistance to therapy with increased malignantpotential (13, 33, 34). However, until now, treatments currentlydid not consider the existence of cycling hypoxia, nor examinethe consequence of antiangiogenic agents on cycling tumorhypoxia. The phenomenon of cycling hypoxia has been orig-inally observed as a consequence of radiobiological experi-ments and investigated in detail using histologic approachesand subsequent window-chamber experiments (9, 33). Be-cause a priori knowledge of location and frequency of cyclinghypoxia may help plan the treatment regimens, noninvasiveimaging techniques are being actively explored to monitor thisphenomenon with required spatial and temporal resolutions
Figure 6. Vascular normalizationwith sunitinib improves cyclinghypoxia in SCC tumors. A,dynamic 3D EPRI imagesobtained every 3 minutesnoninvasively visualizedfluctuating pO2 in an untreatedcontrol SCC tumor. B, four ROIs, 1to 4, were selected and the pO2
fluctuations were plotted. C, inindependent experiment, 4 daysof sunitinib treatment reducedextent of temporal fluctuations intumor pO2. D, temporal pO2
fluctuations in ROIs 1 to 4 wereplotted. E, SD of pO2 fluctuation intumor calculated from sequential10 scans for 30-minutemeasurement time. Sunit,sunitinib.
Sunitinib Suppresses Cycling Tumor Hypoxia
www.aacrjournals.org Cancer Res; 71(20) October 15, 2011 6357
Cancer Research. on September 17, 2020. © 2011 American Association forcancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 30, 2011; DOI: 10.1158/0008-5472.CAN-11-2025

(12). EPRI provided a noninvasive capability to obtain 3D pO2
maps within 3 minutes. Serial oxygen mapping with EPRI in atime window of 30 minutes enabled to spatially distinguishcycling hypoxic regions from chronically hypoxia regions in thetumors (26). To quantitatively visualize the extent of cyclinghypoxia, the parametric image (SD of pO2 map) was calculatedfrom 10 individual images in 30-minute time window. Theresults in this study show, for the first time, that cycling hypoxiain tumors can be suppressed by sunitinib. Thus antiangiogenictreatmentmight, in addition to its well-knownmodes of actionalone or in combination therapy, prevent prosurvival pathwaysthat can be acquired by cycling hypoxia.
Jain and colleagues reported that the combination of MRI-based parameters with circulating collagen IV can predictsurvival of glioblastoma patients after anti-VEGF treatment(30). Combination of such blood markers with the pO2 andblood vessel density values may improve the accuracy ofthese types of predictions. The present study showed thatthe methodology developed here has the capability to non-invasively and longitudinally monitor spatial and temporalchanges in tumor pO2 before and after antiangiogenesistreatment and to successfully visualize the improvement in
cycling hypoxia during the vascular normalization window,which results in enhanced efficacy of combined radiationtherapy. EPRI can use the experience from MRI to scale upfor human use, making it a promising modality for integrationinto clinical settings.
Disclosure of Potential Conflicts of Interest
No potential conflicts of interest were disclosed.
Acknowledgments
The authors thank Melissa Stauffer, PhD, of Scientific Editing Solutions forproviding editorial assistance.
Grant Support
This research was supported by the Intramural Research Program, Center forCancer Research, National Cancer Institute, NIH.
The costs of publication of this article were defrayed in part by the paymentof page charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Received June 14, 2011; revised July 29, 2011; accepted August 11, 2011;published OnlineFirst August 30, 2011.
References1. Folkman J. Tumor angiogenesis: therapeutic implications. N Engl J
Med 1971;285:1182–6.2. Jain RK. A new target for tumor therapy. N Engl J Med 2009;360:
2669–71.3. Naumov GN, Akslen LA, Folkman J. Role of angiogenesis in human
tumor dormancy: animal models of the angiogenic switch. Cell Cycle2006;5:1779–87.
4. Carmeliet P, Jain RK. Angiogenesis in cancer and other diseases.Nature 2000;407:249–57.
5. Jain RK. Molecular regulation of vessel maturation. Nat Med 2003;9:685–93.
6. Matsumoto S, Yasui H, Batra S, Kinoshita Y, BernardoM,MunasingheJP, et al. Simultaneous imaging of tumor oxygenation and microvas-cular permeability using Overhauser enhanced MRI. Proc Natl AcadSci USA 2009;106:17898–903.
7. Gatenby RA, Gillies RJ. Why do cancers have high aerobic glycolysis?Nat Rev Cancer 2004;4:891–9.
8. DewhirstMW,OngET, BraunRD, SmithB, KlitzmanB, Evans SM, et al.Quantification of longitudinal tissue pO2 gradients in window chambertumours: impact on tumour hypoxia. Br J Cancer 1999;79:1717–22.
9. Dewhirst MW. Relationships between cycling hypoxia, HIF-1, angio-genesis and oxidative stress. Radiat Res 2009;172:653–65.
10. Kimura H, Braun RD, Ong ET, Hsu R, Secomb TW, PapahadjopoulosD, et al. Fluctuations in red cell flux in tumor microvessels can lead totransient hypoxia and reoxygenation in tumor parenchyma. CancerRes 1996;56:5522–8.
11. Chaplin DJ, Olive PL, Durand RE. Intermittent blood flow in a murinetumor: radiobiological effects. Cancer Res 1987;47:597–601.
12. Matsumoto S, Yasui H, Mitchell JB, Krishna MC. Imaging cyclingtumor hypoxia. Cancer Res 2010;70:10019–23.
13. Martinive P, Defresne F, Bouzin C, Saliez J, Lair F, Gregoire V, et al.Preconditioning of the tumor vasculature and tumor cells by intermit-tent hypoxia: implications for anticancer therapies. Cancer Res2006;66:11736–44.
14. Baudelet C, Ansiaux R, Jordan BF, Havaux X, Macq B, Gallez B.Physiological noise in murine solid tumours using T2*-weighted gra-dient-echo imaging: a marker of tumour acute hypoxia? Phys MedBiol 2004;49:3389–411.
15. Bergers G, Hanahan D. Modes of resistance to anti-angiogenictherapy. Nat Rev Cancer 2008;8:592–603.
16. Senan S, Smit EF. Design of clinical trials of radiation combined withantiangiogenic therapy. Oncologist 2007;12:465–77.
17. Ansiaux R, Baudelet C, Jordan BF, Beghein N, Sonveaux P, DeWever J, et al. Thalidomide radiosensitizes tumors through earlychanges in the tumor microenvironment. Clin Cancer Res 2005;11:743–50.
18. Cerniglia GJ, Pore N, Tsai JH, Schultz S, Mick R, Choe R, et al.Epidermal growth factor receptor inhibition modulates the microen-vironment by vascular normalization to improve chemotherapy andradiotherapy efficacy. PLoS One 2009;4:e6539.
19. Zhou Q, Guo P, Gallo JM. Impact of angiogenesis inhibition bysunitinib on tumor distribution of temozolomide. Clin Cancer Res2008;14:1540–9.
20. Jain RK. Normalizing tumor vasculature with anti-angiogenic therapy:a new paradigm for combination therapy. Nat Med 2001;7:987–9.
21. Cuneo KC, Geng L, Fu A, Orton D, Hallahan DE, Chakravarthy AB.SU11248 (sunitinib) sensitizes pancreatic cancer to the cytotoxiceffects of ionizing radiation. Int J Radiat Oncol Biol Phys 2008;71:873–9.
22. Winkler F, Kozin SV, Tong RT, Chae SS, Booth MF, Garkavtsev I, et al.Kinetics of vascular normalization by VEGFR2 blockade governs braintumor response to radiation: role of oxygenation, angiopoietin-1, andmatrix metalloproteinases. Cancer Cell 2004;6:553–63.
23. Miller JC, Pien HH, Sahani D, Sorensen AG, Thrall JH. Imagingangiogenesis: applications and potential for drug development. J NatlCancer Inst 2005;97:172–87.
24. Elas M, Bell R, Hleihel D, Barth ED, McFaul C, Haney CR, et al.Electron paramagnetic resonance oxygen image hypoxic fraction plusradiation dose strongly correlates with tumor cure in FSa fibrosarco-mas. Int J Radiat Oncol Biol Phys 2008;71:542–9.
25. Matsumoto S, Hyodo F, Subramanian S, Devasahayam N, Muna-singhe J, Hyodo E, et al. Low-field paramagnetic resonance imagingof tumor oxygenation and glycolytic activity in mice. J Clin Invest2008;118:1965–73.
26. Yasui H, Matsumoto S, Devasahayam N, Munasinghe JP, ChoudhuriR, Saito K, et al. Low-field magnetic resonance imaging to visualizechronic and cycling hypoxia in tumor-bearing mice. Cancer Res2010;70:6427–36.
27. National Research Council. Guide for the care and use of laboratoryanimals. Washington, DC: National Academy Press; 1996.
Matsumoto et al.
Cancer Res; 71(20) October 15, 2011 Cancer Research6358
Cancer Research. on September 17, 2020. © 2011 American Association forcancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 30, 2011; DOI: 10.1158/0008-5472.CAN-11-2025

28. Hyodo F, Chandramouli GV, Matsumoto S, Matsumoto K, MitchellJB, Krishna MC, et al. Estimation of tumor microvessel density byMRI using a blood pool contrast agent. Int J Oncol 2009;35:797–804.
29. Brindle K. New approaches for imaging tumour responses to treat-ment. Nat Rev Cancer 2008;8:94–107.
30. Sorensen AG, Batchelor TT, Zhang WT, Chen PJ, Yeo P, Wang M,et al. A "vascular normalization index" as potential mechanisticbiomarker to predict survival after a single dose of cediranib inrecurrent glioblastoma patients. Cancer Res 2009;69:5296–300.
31. Ansiaux R, Baudelet C, Jordan BF, Crokart N, Martinive P, DeWever J,et al. Mechanism of reoxygenation after antiangiogenic therapy using
SU5416 and its importance for guiding combined antitumor therapy.Cancer Res 2006;66:9698–704.
32. Ansiaux R, Dewever J, Gregoire V, Feron O, Jordan BF, Gallez B.Decrease in tumor cell oxygen consumption after treatment withvandetanib (ZACTIMA; ZD6474) and its effect on response to radio-therapy. Radiat Res 2009;172:584–91.
33. Dewhirst MW, Cao Y, Moeller B. Cycling hypoxia and free radicalsregulate angiogenesis and radiotherapy response. Nat Rev Cancer2008;8:425–37.
34. Moeller BJ, Cao Y, Li CY, Dewhirst MW. Radiation activates HIF-1 toregulate vascular radiosensitivity in tumors: role of reoxygenation, freeradicals, and stress granules. Cancer Cell 2004;5:429–41.
Sunitinib Suppresses Cycling Tumor Hypoxia
www.aacrjournals.org Cancer Res; 71(20) October 15, 2011 6359
Cancer Research. on September 17, 2020. © 2011 American Association forcancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 30, 2011; DOI: 10.1158/0008-5472.CAN-11-2025

2011;71:6350-6359. Published OnlineFirst August 30, 2011.Cancer Res Shingo Matsumoto, Sonny Batra, Keita Saito, et al. Oxygenation and Suppresses Cycling HypoxiaAntiangiogenic Agent Sunitinib Transiently Increases Tumor
Updated version
10.1158/0008-5472.CAN-11-2025doi:
Access the most recent version of this article at:
Material
Supplementary
http://cancerres.aacrjournals.org/content/suppl/2011/08/30/0008-5472.CAN-11-2025.DC2
Access the most recent supplemental material at:
Cited articles
http://cancerres.aacrjournals.org/content/71/20/6350.full#ref-list-1
This article cites 33 articles, 11 of which you can access for free at:
Citing articles
http://cancerres.aacrjournals.org/content/71/20/6350.full#related-urls
This article has been cited by 12 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
SubscriptionsReprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. (CCC)Click on "Request Permissions" which will take you to the Copyright Clearance Center's
.http://cancerres.aacrjournals.org/content/71/20/6350To request permission to re-use all or part of this article, use this link
Cancer Research. on September 17, 2020. © 2011 American Association forcancerres.aacrjournals.org Downloaded from
Published OnlineFirst August 30, 2011; DOI: 10.1158/0008-5472.CAN-11-2025