Embed Size (px)
Citation preview
Antibiotic Treatment of Tuberculosis:Old Problems, New SolutionsWith tuberculosis and drug resistance surging, the search is onfor new drugs along with better and faster ways of evaluating them
Sanjay K. Jain, Gyanu Lamichhane, Sridhar Nimmagadda,
Martin G. Pomper, and William R. Bishai
The German physician and scientistRobert Koch presented his discoveryof Mycobacterium tuberculosis onMarch 24, 1882, noting:
“If the importance of a disease for man-kind is measured by the number of fatali-ties it causes, then tuberculosis must beconsidered much more important thanthose most feared infectious diseases,plague, cholera and the like. One in seven
of all human beings dies from tuberculosis.If one only considers the productive mid-dle-age groups, tuberculosis carries awayone-third, and often more.”
More than 125 years later, tuberculosis (TB) issurging, leading to more deaths in 2006 thanany previous year in the last few decades. Dam-age from this disease continues to grow despiteeffective therapies for drug-susceptible TB thatkeep the incidence of TB in Western countries atrecord lows. The reasons for this shocking fail-
ure to control TB globally pivot on thedifficulty of providing sustained, properlydosed, multiantibiotic therapy in develop-ing countries. Worse, this failure has led todevelopment of drug-resistant TB, includ-ing the recent recognition of extensivelydrug-resistant (XDR) TB in precisely thoseregions that are least equipped to deal withit. The result, though predictable, is no lessdisturbing: high rates of rapidly fatal TBwith an estimated 1.7 million deaths world-wide annually, 9.2 million new cases of TBdisease, and more than 2 billion people in-fected with “latent” TB.
“Short-Course” Therapy
To Treat TB: a Paradox
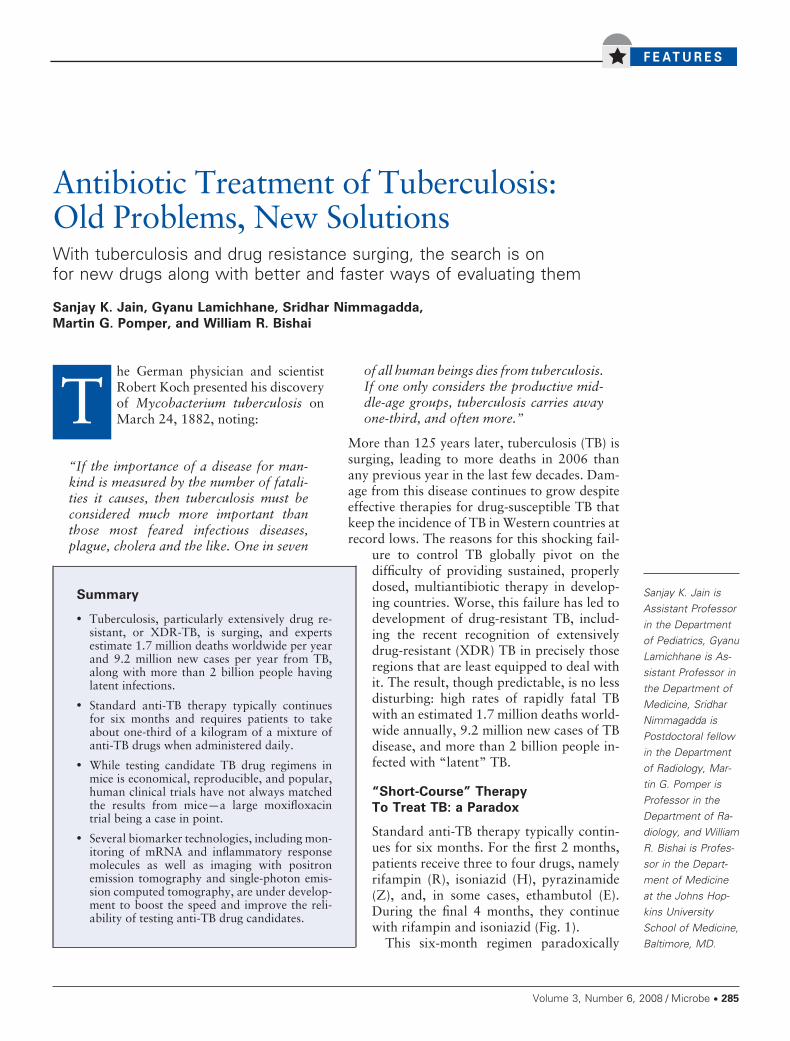
Standard anti-TB therapy typically contin-ues for six months. For the first 2 months,patients receive three to four drugs, namelyrifampin (R), isoniazid (H), pyrazinamide(Z), and, in some cases, ethambutol (E).During the final 4 months, they continuewith rifampin and isoniazid (Fig. 1).
This six-month regimen paradoxically
Summary
• Tuberculosis, particularly extensively drug re-sistant, or XDR-TB, is surging, and expertsestimate 1.7 million deaths worldwide per yearand 9.2 million new cases per year from TB,along with more than 2 billion people havinglatent infections.
• Standard anti-TB therapy typically continuesfor six months and requires patients to takeabout one-third of a kilogram of a mixture ofanti-TB drugs when administered daily.
• While testing candidate TB drug regimens inmice is economical, reproducible, and popular,human clinical trials have not always matchedthe results from mice—a large moxifloxacintrial being a case in point.
• Several biomarker technologies, including mon-itoring of mRNA and inflammatory responsemolecules as well as imaging with positronemission tomography and single-photon emis-sion computed tomography, are under develop-ment to boost the speed and improve the reli-ability of testing anti-TB drug candidates.
Sanjay K. Jain isAssistant Professorin the Departmentof Pediatrics, GyanuLamichhane is As-sistant Professor inthe Department ofMedicine, SridharNimmagadda isPostdoctoral fellowin the Departmentof Radiology, Mar-tin G. Pomper isProfessor in theDepartment of Ra-diology, and WilliamR. Bishai is Profes-sor in the Depart-ment of Medicineat the Johns Hop-kins UniversitySchool of Medicine,Baltimore, MD.
Volume 3, Number 6, 2008 / Microbe Y 285
also is called “short-course” anti-TB therapy.When administered daily, a typical adult patient isrequired to consume more than one-third of akilogram of anti-TB drugs in a series of 182 dailydoses—in contrast to 2–5 grams in 5–7 doses forcuring an uncomplicated, community-acquiredbacterial pneumonia or similar infection.
So why does it take so long to treat TB diseasein humans when cultures of M. tuberculosis maybe killed in a matter of mere hours to days?According to current models, several popula-tions of bacilli have to be dealt with in infectedindividuals: those that are growing rapidly,those growing slowly, and those that sporadi-
cally replicate. Cells falling intothese separate populations arekilled biphasically, with the rapidmultipliers being cleared duringthe earlier bactericidal phase, andthe slowly and sporadically multi-plying organisms killed during thelater sterilizing phase (Fig. 1).
Isoniazid and streptomycin (S)have good early bactericidal activ-ity when tested in animals, reduc-ing infection burdens initially byfour to five orders of magnitude.However, these agents do not clearthe infections. Thus, despite theearly rapid kill, the slowly andsporadically multiplying popula-tions of M. tuberculosis remain as“persisters,” and these may onlybe cleared by antibiotics possess-ing “sterilizing” activity.
Such persister cells are moreslowly cleared and may be tolerant(phenotypically resistant) to anti-TB therapy. Treatment with ri-fampin, a sterilizing antibiotic,gradually reduces bacillary countsto zero during the latter phase oftherapy in humans. When pyrazin-amide is administered during thefirst two months of treatment, itshortens the overall length of ther-apy, albeit without showing muchbactericidal activity when used onits own. Ethambutol, superfluousin treating drug-susceptible M. tu-berculosis, is a drug that is rou-tinely included in the regimenwhen particular populations are
believed to harbor drug-resistant TB.
Candidate Drugs For Treating TB
While prospects for new broad-spectrum anti-bacterials are limited, several promising nar-row-spectrum anti-TB drugs are under develop-ment (Table 1). Among those new agents aretwo nitroimidazoles, PA-824 (Pa) being devel-oped by the TB Alliance and Chiron, OPC-67683 (O) by Otsuka, a diarylquinoline TMC-207 by Tibotec, an ethambutol derivativeSQ-109 by Sequella, and a pyrrole LL-3858 by
F I G U R E 1
Standard anti-TB therapy. Current model of short-course therapy for tuberculosis showing theintensive (bactericidal) phase in the first 2 months during which rapid killing is observed andthe inclusion of pyrazinamide is necessary for long-term treatment shortening. Typically,optimal regimens in this phase require four drugs: isoniazid (H), rifampin (R), pyrazinamide (Z),and ethambutol (E). The continuation (sterilizing) phase during the remaining 4 months isshown where the rate of killing is lower due to persister bacteria which are slowly orsporadically multiplying. If the isolate is susceptible, Z and E are dropped in the continuationphase. In abbreviated form, standard therapy in humans is HRZE2-HR4. (Adapted from J.Grosset, Clin. Chest Med. 1:231–241, 1980).
286 Y Microbe / Volume 3, Number 6, 2008
Lupin. Several of them are enteringphase II/III clinical trials.
Concerned over our vulnerability tomultidrug-resistant (MDR) and XDRTB, experts also are reexamining ap-proved antibacterials that might be usedto treat patients with TB. This list in-cludes the fluoroquinolone antibioticsmoxifloxacin (M) and gatifloxacin (G),the oxazolidinone antibiotic linezolid,the nitroimidazole antibiotic metronida-zole, and the long-acting rifamycin rifa-pentine (P), which is licensed for TB.One near-term research priority is todetermine whether agents such as fluo-roquinolones and rifapentine may beused in combinations that offer advan-tages over standard anti-TB therapy.
Considerable preclinical testing is re-quired to identify the multidrug regi-mens that best exploit the activities ofnew agents. While in vitro studies help,assessing bactericidal and sterilizingactivities in infected animals that re-ceive doses equivalent to what humanscould expect is an essential part ofthese evaluations.
Insights from Evaluating Novel
TB Drug Combinations
Evaluating new agents combined withestablished anti-TB drugs in mice oftenbrings surprises. For example, addingone of several newer agents, includingmoxifloxacin, PA-824, and OPC-67683,to standard anti-TB drug regimens onlymarginally reduced TB organ burdens.Thus, the new agent plus the standardregime of HRZ is little better than thanHRZ without the new agent.
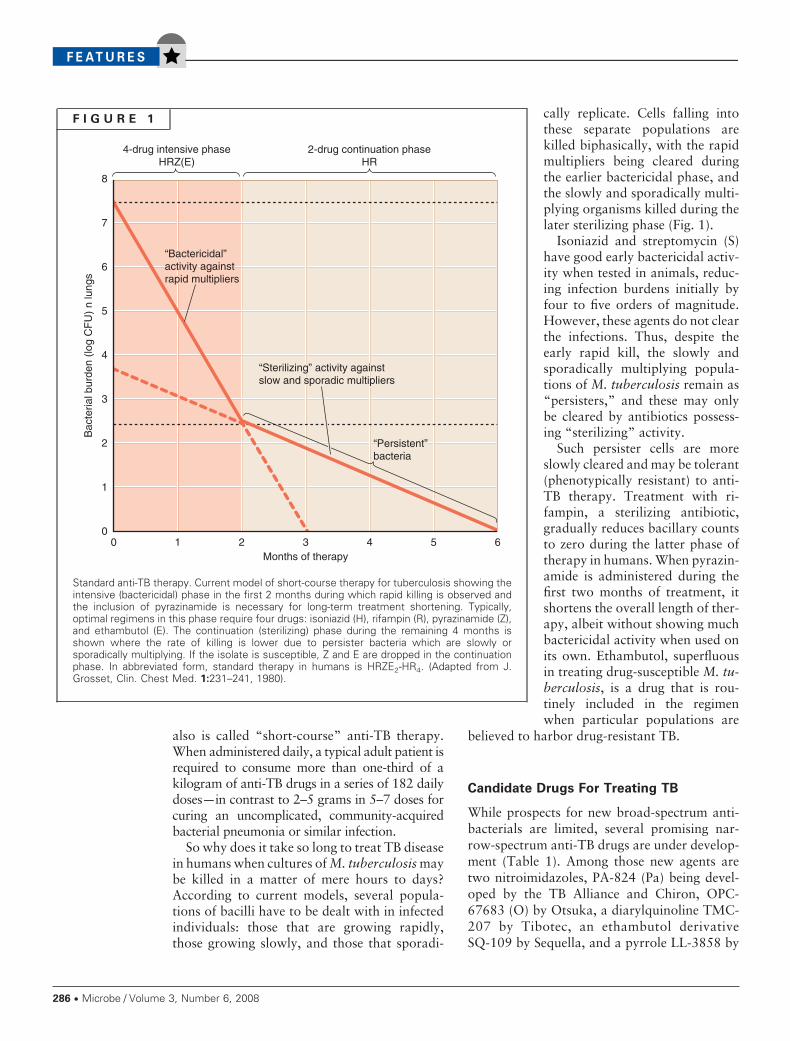
One drug in the standard mix, isoniazid, com-plicates these tests in mice. Remarkably, omit-ting it from such studies sometimes allows otherantibacterial drugs—for example, moxifloxa-cin—to stand out in terms of reducing M. tuber-culosis organ burdens and the time it takes tocure the animals being tested (Fig. 2). Thus,although isoniazid is a potent bactericidal agent,it appears to antagonize the actions of otheranti-TB drugs such as rifampin and pyrazin-amide that are being administered simulta-
neously (consistent with Fig 2A-C). Replacingisoniazid—and thus avoiding antagonism that itcauses—with similarly acting drugs such asmoxifloxacin, PA-824, or OPC-67683 revealsthe possibility of shortening treatments. In par-ticular, substituting moxifloxacin for isoniazidproduces a sustained cure in mice after only 4months of treatment, with no relapses 90 daysafter anti-TB therapy ends. Clinical trials areunder way to address whether these results inmice hold true for humans.
F I G U R E 2
Addition of new agents (M, O, or PA [in red]) to standard therapy is less effective thanreplacement of isoniazid (H) by the new agent in the mouse TB model. Mouse lung CFUcounts in untreated mice (blue curves), mice treated with standard therapy for 6 monthsHRZ(E)2-HR4 (purple curve) versus the addition of a new drug to standard therapy(orange curves) versus the replacement of isoniazid (H) by the new drug (green curves),also indicated by the red arrow. Ethambutol (E) is used in the continuation phase ofhuman TB as a safety agent in case the infecting strain turns out to be drug resistant,hence it is sometimes omitted in mouse studies. (A) Moxifloxacin (M) as the new drug(from Nuermberger et al., Am. J. Respir. Crit. Care Med. 169:421–426, 2004). (B)OPC67683 (O) as the new drug (Matsumoto et al., PLoS Med. 3:e466, 2006). (C) PA-824(Pa) as the new drug (from Nuermberger et al., Antimicrob. Agents Chemother.50:2621–2625, 2006).
Volume 3, Number 6, 2008 / Microbe Y 287
Meanwhile, recent studies suggest that cur-rent rifamycin dosing for patients with TB maybe too low. However, the development of rifa-mycin derivatives with long half-lives, includingrifapentine, rifabutin, and rifalazil, makes itpossible to raise the effective dosing. Of thisgroup, rifapentine has a 10–15 hour half-life,
which is about fivefold longer than that of ri-fampin, and it has a two- to fourfold increase inin vitro activity against M. tuberculosis. There isnow considerable interest in using it daily orincreasing the twice-weekly dose as a means ofboosting rifamycin exposure. For example, sub-stituting daily rifapentine for rifampin signifi-
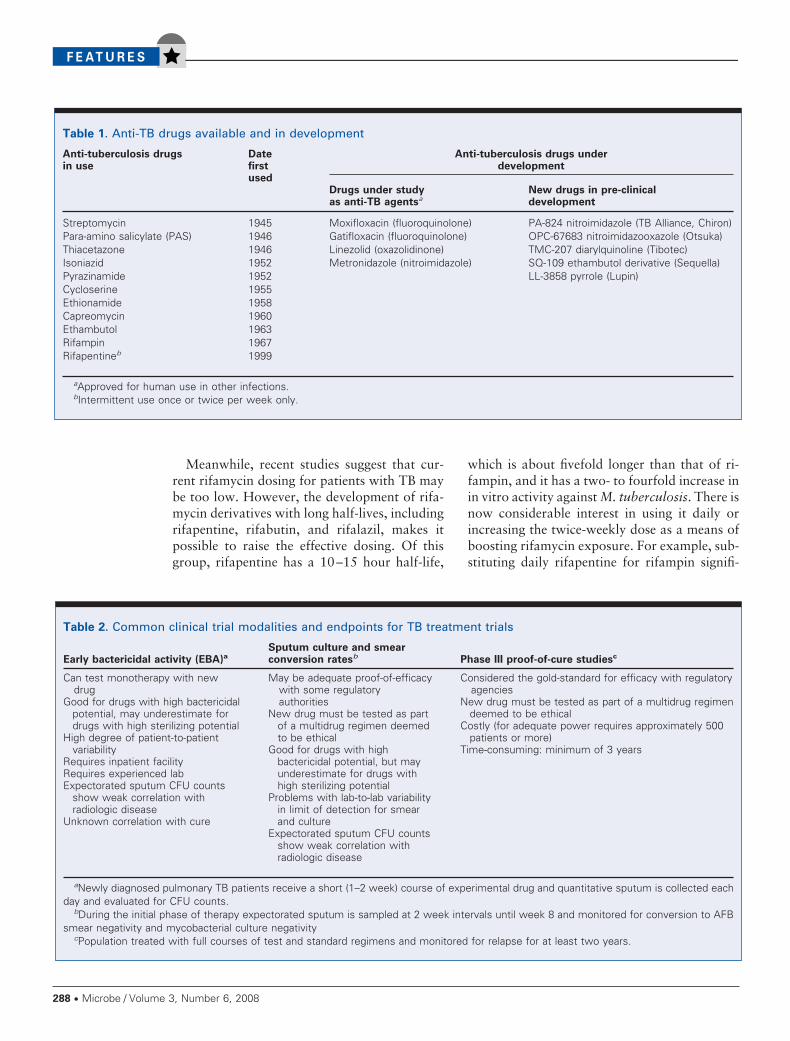
Table 1. Anti-TB drugs available and in development
Anti-tuberculosis drugsin use
Datefirstused
Anti-tuberculosis drugs underdevelopment
Drugs under studyas anti-TB agentsa
New drugs in pre-clinicaldevelopment
Streptomycin 1945 Moxifloxacin (fluoroquinolone) PA-824 nitroimidazole (TB Alliance, Chiron)Para-amino salicylate (PAS) 1946 Gatifloxacin (fluoroquinolone) OPC-67683 nitroimidazooxazole (Otsuka)Thiacetazone 1946 Linezolid (oxazolidinone) TMC-207 diarylquinoline (Tibotec)Isoniazid 1952 Metronidazole (nitroimidazole) SQ-109 ethambutol derivative (Sequella)Pyrazinamide 1952 LL-3858 pyrrole (Lupin)Cycloserine 1955Ethionamide 1958Capreomycin 1960Ethambutol 1963Rifampin 1967Rifapentineb 1999
aApproved for human use in other infections.bIntermittent use once or twice per week only.
Table 2. Common clinical trial modalities and endpoints for TB treatment trials
Early bactericidal activity (EBA)a
Sputum culture and smearconversion ratesb Phase III proof-of-cure studiesc
Can test monotherapy with newdrug
Good for drugs with high bactericidalpotential, may underestimate fordrugs with high sterilizing potential
High degree of patient-to-patientvariability
Requires inpatient facilityRequires experienced labExpectorated sputum CFU counts
show weak correlation withradiologic disease
Unknown correlation with cure
May be adequate proof-of-efficacywith some regulatoryauthorities
New drug must be tested as partof a multidrug regimen deemedto be ethical
Good for drugs with highbactericidal potential, but mayunderestimate for drugs withhigh sterilizing potential
Problems with lab-to-lab variabilityin limit of detection for smearand culture
Expectorated sputum CFU countsshow weak correlation withradiologic disease
Considered the gold-standard for efficacy with regulatoryagencies
New drug must be tested as part of a multidrug regimendeemed to be ethical
Costly (for adequate power requires approximately 500patients or more)
Time-consuming: minimum of 3 years
aNewly diagnosed pulmonary TB patients receive a short (1–2 week) course of experimental drug and quantitative sputum is collected eachday and evaluated for CFU counts.
bDuring the initial phase of therapy expectorated sputum is sampled at 2 week intervals until week 8 and monitored for conversion to AFBsmear negativity and mycobacterial culture negativity
cPopulation treated with full courses of test and standard regimens and monitored for relapse for at least two years.
288 Y Microbe / Volume 3, Number 6, 2008
cantly shortens anti-TB therapy neededfor relapse-free cures of mice.
Studying Drugs in Mice
with TB: Useful, Not Perfect
While testing new TB drug therapies inmice is economical, reproducible, andpopular, the key question is how well itpredicts performance in humans. Overseveral decades, this approach oftenproved successful in predicting humanefficacy. For example, pyrazinamide be-came an essential component of mod-ern multidrug therapy after beingscreened in mice. More recently, thesterilizing activity of RZ combinationregimens in mice led to tests in humansshowing RZ efficacious as 2-month,short-course preventive therapy for la-tent TB. However, this regimen is nolonger used because it induces idiosyn-cratic hepatitis in humans.
Some TB clinical trials are focused ondrug combinations to shorten the treat-ment period. For example, Study 27 inthe Centers for Disease Control andPrevention (CDC)-sponsored TB TrialsConsortium (TBTC) evaluated moxi-floxacin as a substitute for ethambutol(E) during the initial phase of therapy.Patients were randomized to receiveHRZE or HRZM during the first 8 weeks oftherapy. Those patients who received moxi-floxacin progressed more quickly to negativesputum cultures, although the overall percent-age of patients who achieved culture-negativityby 8 weeks was nearly the same. The clinicaltrial results closely resembled those in mice,where HRZM was marginally better than HRZ(Fig. 2A). However, in a more recent clinicalstudy in Brazil, HRZM not only accelerated butalso increased the proportion of patients withnegative sputum cultures at 8 weeks comparedto HRZE.
Another regimen that looked more excitingwhen tested in mice, replacing isoniazid withmoxifloxacin, was also tested in humans asTBTC Study 28: initial phase MRZE versusHRZE. However, the human results did notresemble those in mice in this trial, and therewas no statistically significant difference be-tween the two at 8 weeks. Why?
One possibility is that that the divergencebetween results of MRZ(E) versus HRZ(E)stems from the fact that human sputum cultureconversion rates may not be directly comparableto the parameters measured in mice—namely,total bacterial organ burdens over time. Second,isoniazid antagonism of other drugs could be ofmuch smaller magnitude in humans than mice.Third, TB-inflicted tissue damage may be lesssevere in mice than in humans, monkeys, orrabbits, thereby giving faster CFU clearances insome regimens. Fourth, mice are more suscepti-ble to TB than humans, developing chronicmultibacillary infection even after small inocula,whereas humans tend to contain the initial inoc-ula and develop latent infections. Fifth, miceclear some antibiotics very quickly compared tohumans and these human pharmacokinetics/pharmacodynamics parameters of antibioticsare difficult to emulate in some instances.Hence, despite increased costs and biohazard
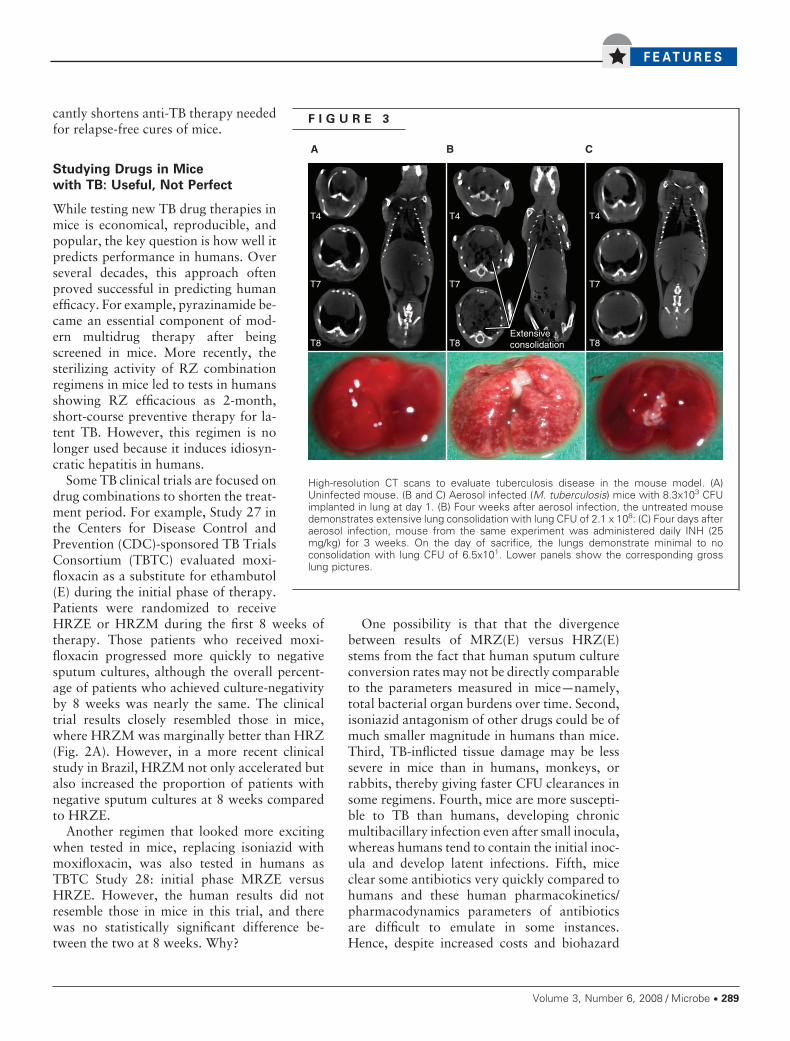
F I G U R E 3
High-resolution CT scans to evaluate tuberculosis disease in the mouse model. (A)Uninfected mouse. (B and C) Aerosol infected (M. tuberculosis) mice with 8.3x103 CFUimplanted in lung at day 1. (B) Four weeks after aerosol infection, the untreated mousedemonstrates extensive lung consolidation with lung CFU of 2.1 x 108: (C) Four days afteraerosol infection, mouse from the same experiment was administered daily INH (25mg/kg) for 3 weeks. On the day of sacrifice, the lungs demonstrate minimal to noconsolidation with lung CFU of 6.5x101. Lower panels show the corresponding grosslung pictures.
Volume 3, Number 6, 2008 / Microbe Y 289
inconveniences, there may be value in testingcertain aspects of anti-TB drug performance inlarger animals such as guinea pigs, rabbits, andnonhuman primates.
Surrogate Markers Would Help in
Evaluating Anti-TB Therapies
Tools for evaluating TB treatments, especially inclinical trials, are painfully primitive, expensive,and time-consuming. For instance, multidrugcocktail phase III trials entail treating hundredsof patients with full courses of standard and testregimens and monitoring them for at least twoyears for relapses (Table 2). Another option,phase IIB studies monitoring patients for 8
weeks for sputum culture conver-sion rates, is of limited value be-cause sputum bacterial burdendoes not always correlate closelywith overall disease.
Contrast TB clinical trials op-tions with those for testing antivi-ral drugs against HIV, where thereare well-validated markers of dis-ease burden, namely quantitativeviral loads, and progression of dis-ease that is measured in decliningCD4 cell counts.
In recognizing this need, offi-cials at CDC and other experts callfor urgent development of newmarkers and endpoints for TB.However, such biomarkers will beuseful only if they refine and sim-plify efforts to evaluate candidatedrugs or reduce time for measuringresponses to them. Further, bio-marker technology needs to bevalidated before surrogate mark-ers can be used to measure end-points. Biomarker technologiesthat are validated in animals andeasily scalable to humans may laythe groundwork for evaluatingcandidate anti-TB therapies in pa-tients.
Several biomarker technologiesare under development for TB. Forinstance, specific mRNA mole-cules are being used to monitormycobacterial viability. In one se-ries of studies, investigators used
antigen 85B mRNA, which was lost rapidlywhen anti-TB therapy was started. Thus,changes in levels of this mRNA species corre-lated with culture clearance of the pathogen.Moreover, for one patient who subsequentlyrelapsed, that mRNA remained persistently de-tectable. Other approaches measure nonspecificmarkers of inflammation such as erythrocytesedimentation rate, C-reactive protein, �2-mi-croglobin, and pro-calcitonin, to follow TB andother bacterial diseases in humans. In principle,following any of these markers would be usefulfor assessing responses to anti-TB therapy be-cause host immunity is essential for controllingTB and for suppressing reactivation.
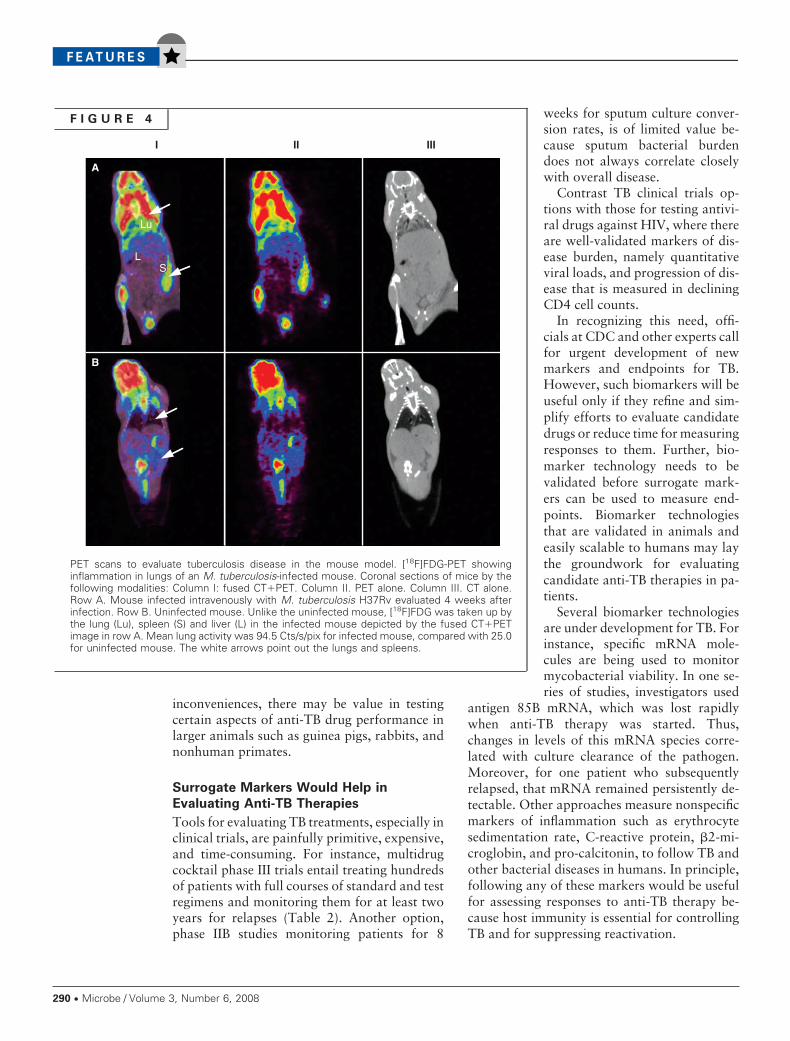
F I G U R E 4
PET scans to evaluate tuberculosis disease in the mouse model. [18F]FDG-PET showinginflammation in lungs of an M. tuberculosis-infected mouse. Coronal sections of mice by thefollowing modalities: Column I: fused CT�PET. Column II. PET alone. Column III. CT alone.Row A. Mouse infected intravenously with M. tuberculosis H37Rv evaluated 4 weeks afterinfection. Row B. Uninfected mouse. Unlike the uninfected mouse, [18F]FDG was taken up bythe lung (Lu), spleen (S) and liver (L) in the infected mouse depicted by the fused CT�PETimage in row A. Mean lung activity was 94.5 Cts/s/pix for infected mouse, compared with 25.0for uninfected mouse. The white arrows point out the lungs and spleens.
290 Y Microbe / Volume 3, Number 6, 2008
In terms of immunological biomark-ers, the T cell-based interferon �(IFN-�) release assays (IGRAs) are per-haps the most developed. These assaysmeasure IFN-�-release by T cells in re-sponse to two M. tuberculosis antigens,early secretory antigenic target-6(ESAT-6) and culture filtrate protein-10(CFP-10), both of which are strong tar-gets of T helper type 1 cells in TB pa-tients. Commercial kits, such as theQuantiFERON-TB Gold In Tube byCellestis that measures IFN-� levels inwhole blood and the T-SPOT.TB byOxford Immunotec that is an ex vivoenzyme-linked immunospot assay forcounting antigen-specific T-cells, areavailable.
These assays provide reliable rapidresults even when performed on ex-trapulmonary specimens. However,IGRA findings can vary among differ-ent populations and regions. Also, howlong T-cell responses remain elevated inpatients who are treated for latent dis-ease is not known. Positive results fromIGRAs, which were developed for diag-nosing latent infections, show delayswhen patients convert to active disease.They also cannot measure cases ofcured disease. Also, even though avail-able in kits, these assays remain re-source intensive, particularly for use inresource-poor countries. Nonetheless,these assays may provide useful bio-markers for evaluating novel anti-TB therapies.
Imaging Biomarkers
Traditional radiographic tools, including chestradiography and computed tomography (CT),lack sensitivity and specificity for monitoringresponses to anti-TB therapies. However,positron emission tomography (PET) withradiolabeled [18F]-2-fluoro-deoxy-D-glucose(FDG), which is being used for diagnosing sev-eral types of cancer, may also be used to produceimages of tuberculous lesions in humans.
Our preliminary data suggest that serial com-puted tomography (CT) and FDG-PET are use-ful for evaluating anti-TB therapy in animals(Fig. 3 and 4). Coregistering high-resolution (50
�m) CT and PET scans may also help in evalu-ating host tissue inflammatory indices in granu-lomas. However, neither of these technologies isyet validated for making preclinical or clinicalassessments. Further, because they measure in-flammation in host tissues, these lagging indica-tors may prove slow for detecting bacteriologi-cal responses to novel therapies.
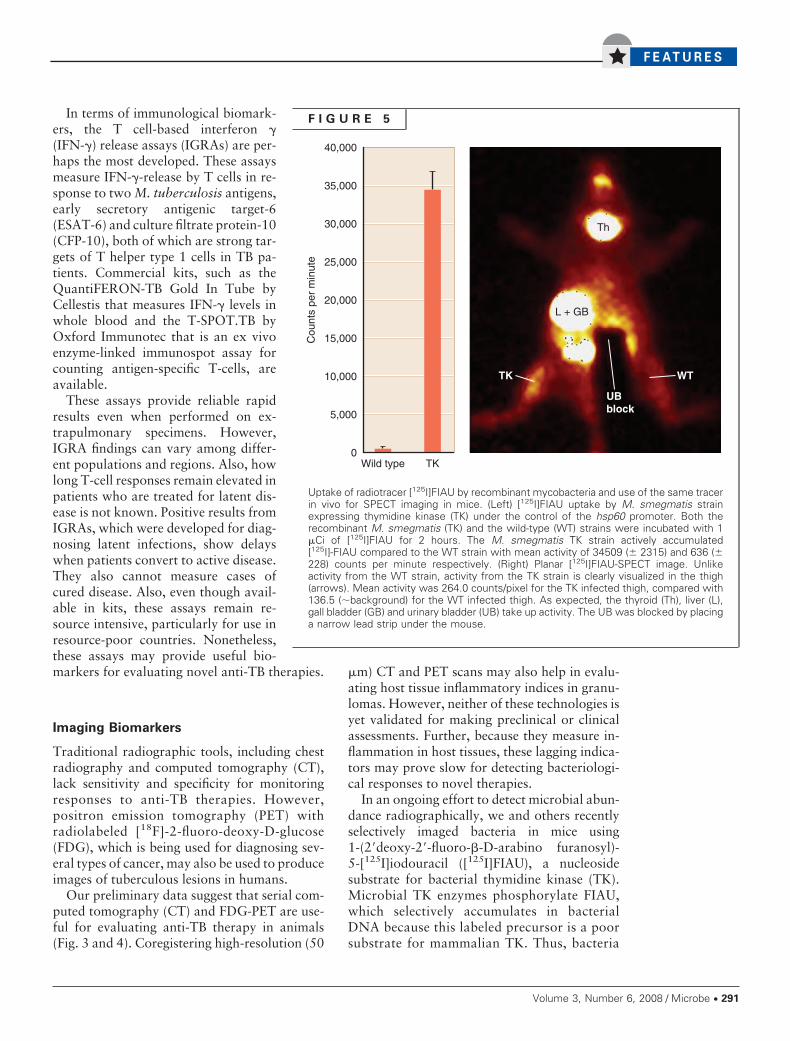
In an ongoing effort to detect microbial abun-dance radiographically, we and others recentlyselectively imaged bacteria in mice using1-(2�deoxy-2�-fluoro-�-D-arabino furanosyl)-5-[125I]iodouracil ([125I]FIAU), a nucleosidesubstrate for bacterial thymidine kinase (TK).Microbial TK enzymes phosphorylate FIAU,which selectively accumulates in bacterialDNA because this labeled precursor is a poorsubstrate for mammalian TK. Thus, bacteria
F I G U R E 5
Uptake of radiotracer [125I]FIAU by recombinant mycobacteria and use of the same tracerin vivo for SPECT imaging in mice. (Left) [125I]FIAU uptake by M. smegmatis strainexpressing thymidine kinase (TK) under the control of the hsp60 promoter. Both therecombinant M. smegmatis (TK) and the wild-type (WT) strains were incubated with 1�Ci of [125I]FIAU for 2 hours. The M. smegmatis TK strain actively accumulated[125I]-FIAU compared to the WT strain with mean activity of 34509 (� 2315) and 636 (�228) counts per minute respectively. (Right) Planar [125I]FIAU-SPECT image. Unlikeactivity from the WT strain, activity from the TK strain is clearly visualized in the thigh(arrows). Mean activity was 264.0 counts/pixel for the TK infected thigh, compared with136.5 (�background) for the WT infected thigh. As expected, the thyroid (Th), liver (L),gall bladder (GB) and urinary bladder (UB) take up activity. The UB was blocked by placinga narrow lead strip under the mouse.
Volume 3, Number 6, 2008 / Microbe Y 291

may be imaged and their burden in infectedhosts quantified using [125I]FIAU-single pho-ton emission computed tomography (SPECT).We applied this technology to image a M.smegmatis strain that was engineered to ex-press TK. This strain actively accumulates[125I]FIAU and may be imaged in mice (Fig. 5).We are continuing to evaluate M. tuberculosisstrains that are engineered to express TK. Weanticipate that [125I]FIAU-SPECT will behelpful for measuring mycobacterial loads in
M. tuberculosis-infected mice or other ani-mals. Coregistering such images with CT mayenable us to determine in which organs andtissue these bacteria accumulate and whetherthey localize to granulomas or other types ofspecific lesions. The development of radiolog-ical biomarkers is exciting, and this technol-ogy seems particularly well suited for trackinginfectious pulmonary diseases such as TB,where sampling microbial populations is no-toriously difficult.
ACKNOWLEDGMENTS
The support of NIH grants AI30036, AI43846, and CA92871 and Bill & Melinda Gates foundation TB Drug Acceleratorgrant 48793 is gratefully acknowledged.
SUGGESTED READING
Bettegowda, C., C. A. Foss, I. Cheong, et al. 2005. Imaging bacterial infections with radiolabeled 1-(2’-deoxy-2’-fluoro-beta-D-arabinofuranosyl)-5-iodouracil. Proc. Natl. Acad. Sci. USA 102:1145–1150.Dorman, S., J. Johnson, N. Padayatchi, et al. 2007. Moxifloxacin vs. isoniazid in the first 2 months of treatment for pulmonarytuberculosis. In: ICAAC. Chicago, 2007Efron, A., et al. A randomized, placebo-controlled trial of moxifloxacin vs. ethambutol in the initial phase of tuberculosistherapy in Brazil. In: ICAAC. Chicago, 2007Flynn, J. L. 2006. Lessons from experimental Mycobacterium tuberculosis infections. Microbes Infect. 8:1179–1188.Gandhi, N. R., A. Moll, A. W. Sturm, et al. 2006. Extensively drug-resistant tuberculosis as a cause of death in patientsco-infected with tuberculosis and HIV in a rural area of South Africa. Lancet 368:1575–1580.Nuermberger, E. L., T. Yoshimatsu, S. Tyagi, R. J. O’Brien, A. N. Vernon, R. E. Chaisson, W. R. Bishai, and J. H. Grosset.2004. Moxifloxacin-containing regimen greatly reduces time to culture conversion in murine tuberculosis. Am. Rev. Respir.Crit. Care Med. 69:421–426.Perrin, F. M., M. C. Lipman, T. D. McHugh, and S. H. Gillespie. 2007. Biomarkers of treatment response in clinical trials ofnovel anti-TB agents. Lancet Infect. Dis. 7:481–490.Rosenthal, I., M. Zhang, K. Williams, C. Peloquin, W. Bishai, R. Chaisson, J. Grosset, and E. Nuermberger. 2007. Dailydosing of rifapentine cures tuberculosis in three months or less in the murine model. PLoS Med. 4:e344.Spigelman, M., and S. Gillespie. 2006. Tuberculosis drug development pipeline: progress and hope. Lancet 367:945–947.World Health Organization. WHO report 2008: Global tuberculosis control—surveillance, planning, financing. Available athttp://www.who.int/tb/publications/global_report/2008/summary/en/index.html. Last accessed April 15, 2008.
292 Y Microbe / Volume 3, Number 6, 2008