Embed Size (px)
Citation preview
Anticoagulation and the Pregnant Patient
AC Forum Master Class Nathan Clark, Pharm D, FCCP, BCPS
Kaiser Permanente Colorado
Conflicts of Interest
• I have no relevant financial conflicts of interest to disclose.
Overview
1. Pathophysiology of thromboembolism in pregnancy
2. Pharmacology of preferred anticoagulants 3. Pregnancy planning in chronically
anticoagulated women 4. Anticoagulation for pregnant women with acute
deep vein thrombosis (DVT) or pulmonary embolism (PE)
5. Prevention of DVT/PE during pregnancy and postpartum
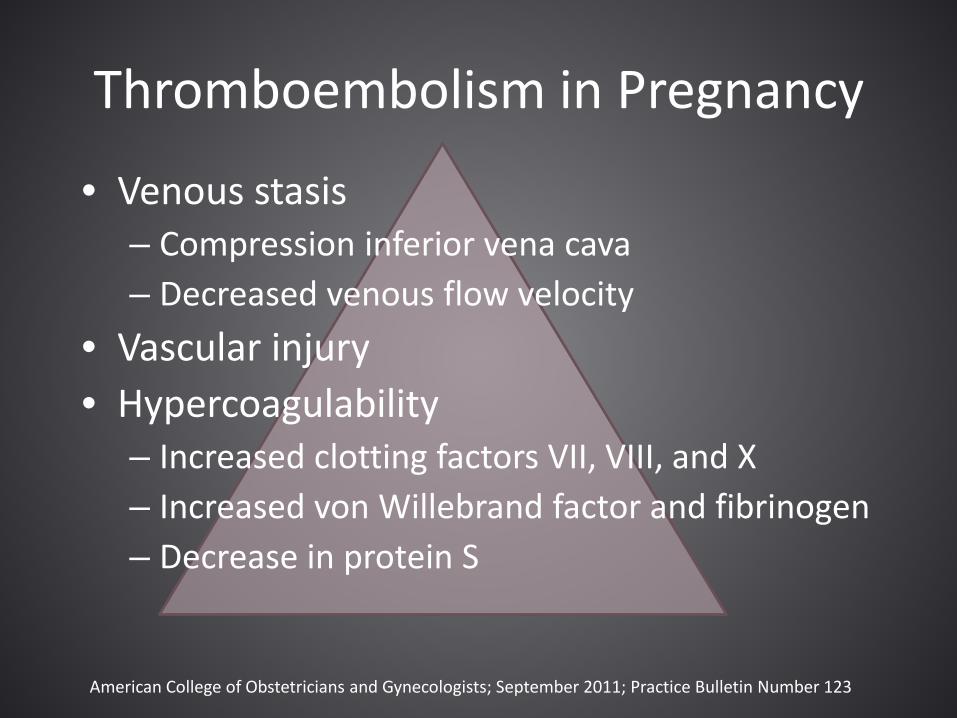
Thromboembolism in Pregnancy
• Venous stasis – Compression inferior vena cava – Decreased venous flow velocity
• Vascular injury • Hypercoagulability
– Increased clotting factors VII, VIII, and X – Increased von Willebrand factor and fibrinogen – Decrease in protein S
American College of Obstetricians and Gynecologists; September 2011; Practice Bulletin Number 123
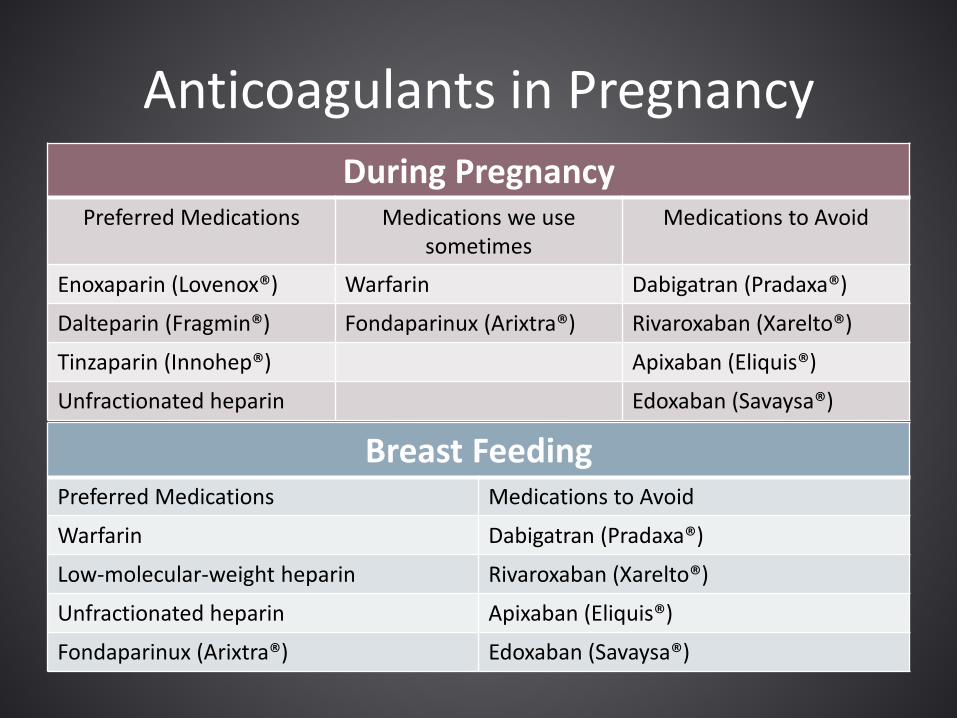
Anticoagulants in Pregnancy During Pregnancy
Preferred Medications Medications we use sometimes
Medications to Avoid
Enoxaparin (Lovenox®) Warfarin Dabigatran (Pradaxa®)
Dalteparin (Fragmin®) Fondaparinux (Arixtra®) Rivaroxaban (Xarelto®)
Tinzaparin (Innohep®) Apixaban (Eliquis®)
Unfractionated heparin Edoxaban (Savaysa®)
Breast Feeding Preferred Medications Medications to Avoid
Warfarin Dabigatran (Pradaxa®)
Low-molecular-weight heparin Rivaroxaban (Xarelto®)
Unfractionated heparin Apixaban (Eliquis®)
Fondaparinux (Arixtra®) Edoxaban (Savaysa®)
Anticoagulants to Avoid (usually) • Warfarin is teratogenic (category X)
– Exposure 6 to 12 weeks gestation: collagen malformation (nasal hypoplasia, stippled epiphyses)
– 3rd trimester exposure: fetal bleeding, CNS development – Miscarriage and spontaneous abortion (doses > 5mg/day ↑risk)
• Fondaparinux (category B)
– Long half-life (19 hours) – Found in umbilical chord blood samples
• Direct-acting oral anticoagulants (category B/C)
– Not known teratogens but cross placenta – Rivaroxaban and apixaban in breast milk
Obstet Gynecol. 2014 Jun;123(6):1256-61 Am J Obstet Gynecol. 2015 Nov;213(5):710 J Thromb Haemost. 2016 Jul;14(7):1436-41
N Engl J Med. 2004 Apr 29;350(18):1914-5.
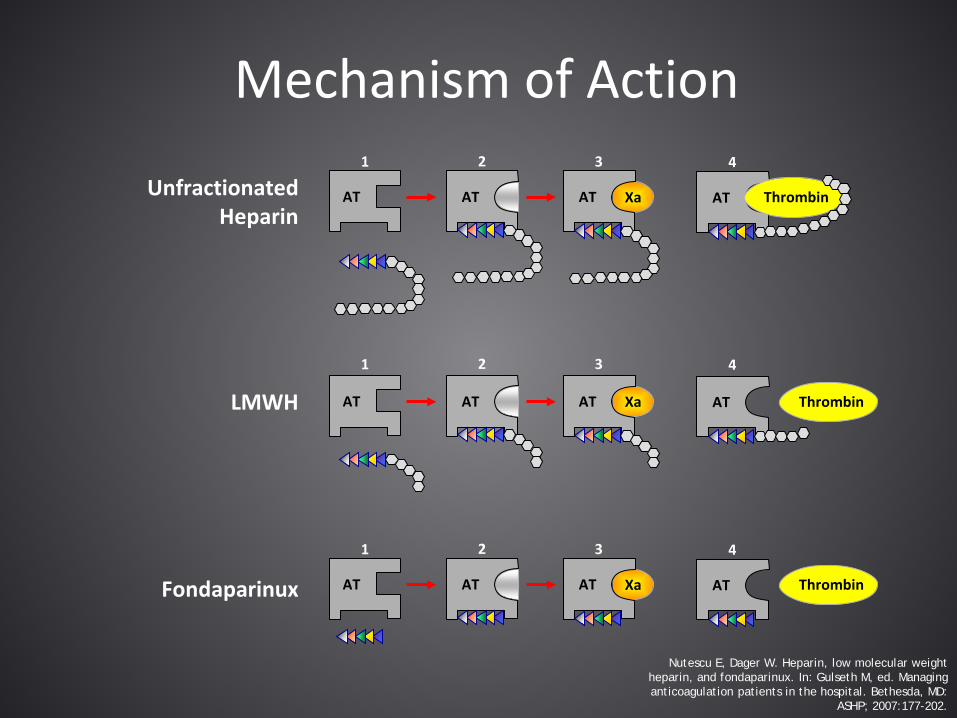
Mechanism of Action
LMWH
Fondaparinux
Xa
1
AT AT
2 3
AT
4
AT Thrombin
Xa
1
AT AT
2 3
AT
4
AT Thrombin
Xa
1
AT AT
2 3
AT
4
AT Thrombin
Unfractionated Heparin
Nutescu E, Dager W. Heparin, low molecular weight heparin, and fondaparinux. In: Gulseth M, ed. Managing anticoagulation patients in the hospital. Bethesda, MD:
ASHP; 2007:177-202.
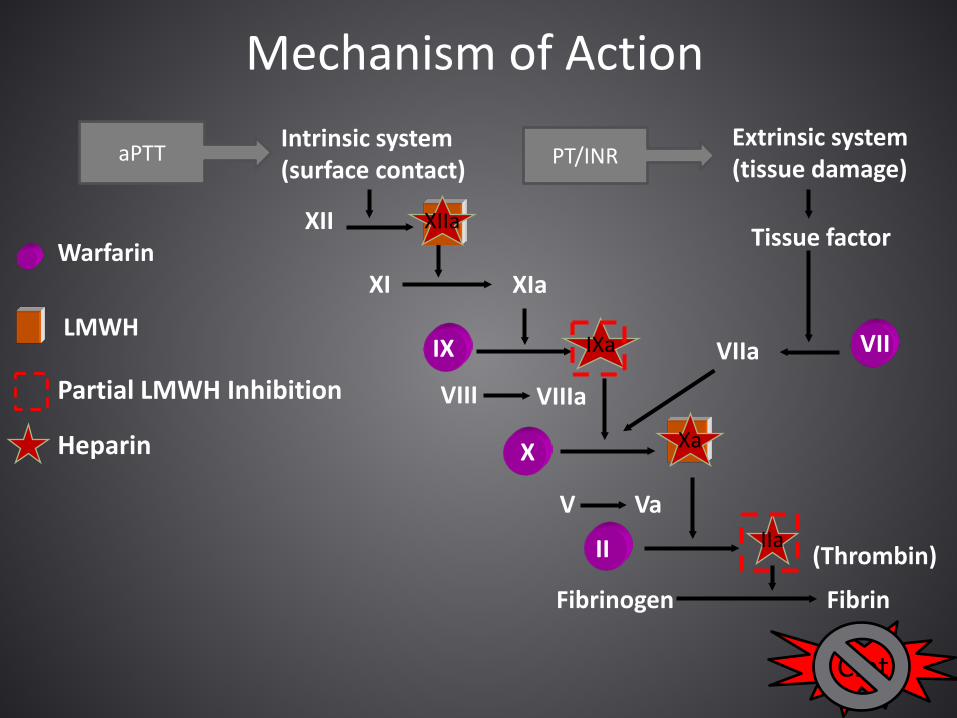
Mechanism of Action
Intrinsic system (surface contact)
XII
XI
Tissue factor
VIII VIIIa
Extrinsic system (tissue damage)
V Va
IX VII
X
II
Fibrinogen Fibrin
(Thrombin)
XIa
VIIa
aPTT PT/INR
Warfarin
LMWH Partial LMWH Inhibition Heparin
Clot
IXa
XIIa
Xa
IIa
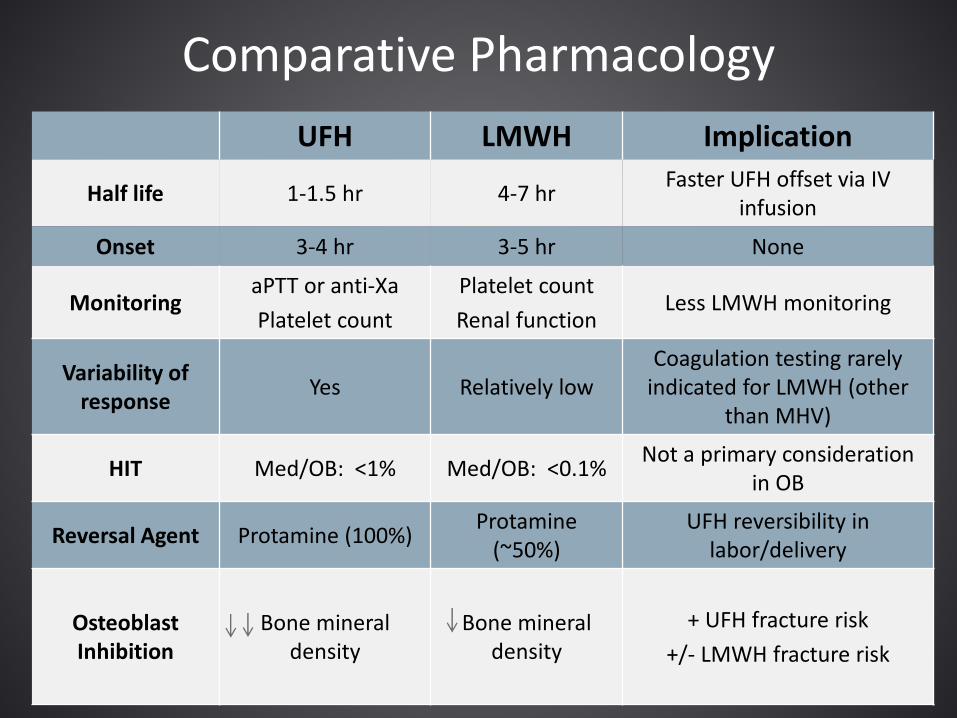
Comparative Pharmacology UFH LMWH Implication
Half life 1-1.5 hr 4-7 hr Faster UFH offset via IV infusion
Onset 3-4 hr 3-5 hr None
Monitoring aPTT or anti-Xa Platelet count
Platelet count Renal function
Less LMWH monitoring
Variability of response Yes Relatively low
Coagulation testing rarely indicated for LMWH (other
than MHV)
HIT Med/OB: <1% Med/OB: <0.1% Not a primary consideration in OB
Reversal Agent Protamine (100%) Protamine (~50%)
UFH reversibility in labor/delivery
Osteoblast Inhibition
Bone mineral density
Bone mineral density
+ UFH fracture risk +/- LMWH fracture risk
Managing Mechanical Heart Valves in Pregnancy
• Women with mechanical heart valves (MHVs) are very high risk for thrombosis and pregnancy complication
• Preconception planning is mandatory • The optimal anticoagulant strategy has not
been defined
BMJ. 2002 Nov 23; 325(7374): 1228–1231
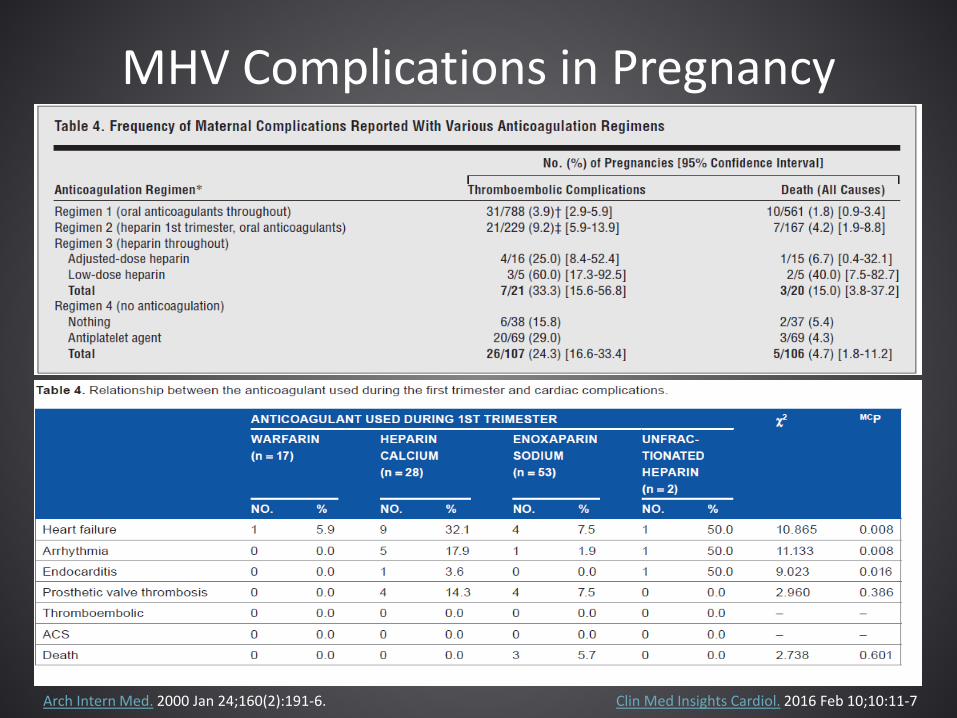
MHV Complications in Pregnancy
Arch Intern Med. 2000 Jan 24;160(2):191-6. Clin Med Insights Cardiol. 2016 Feb 10;10:11-7
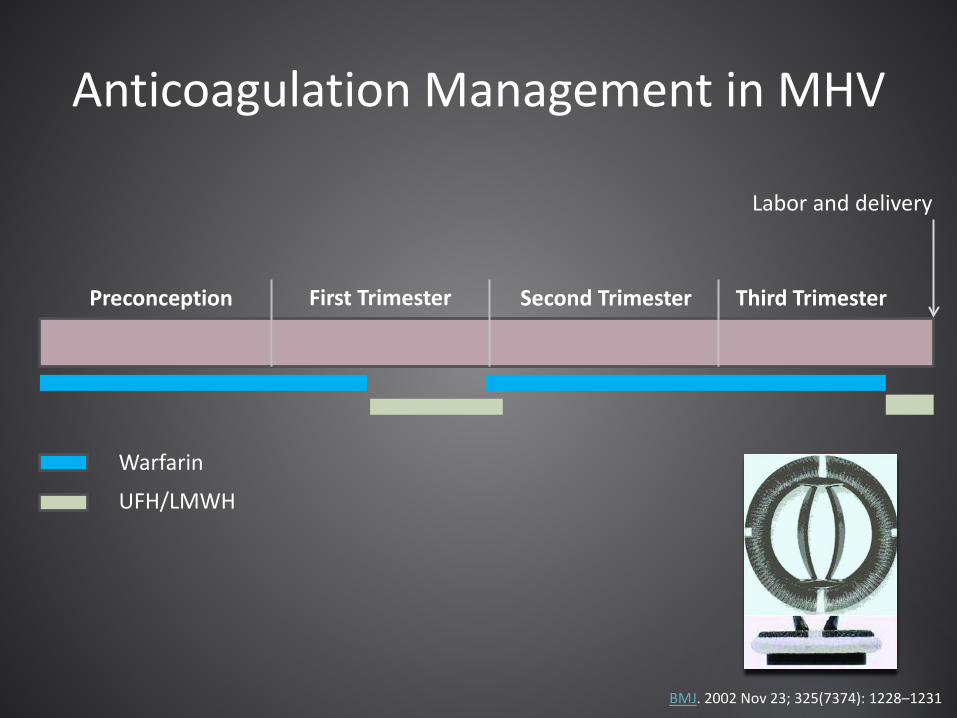
Anticoagulation Management in MHV
Preconception First Trimester Second Trimester Third Trimester
Labor and delivery
Warfarin
UFH/LMWH
BMJ. 2002 Nov 23; 325(7374): 1228–1231
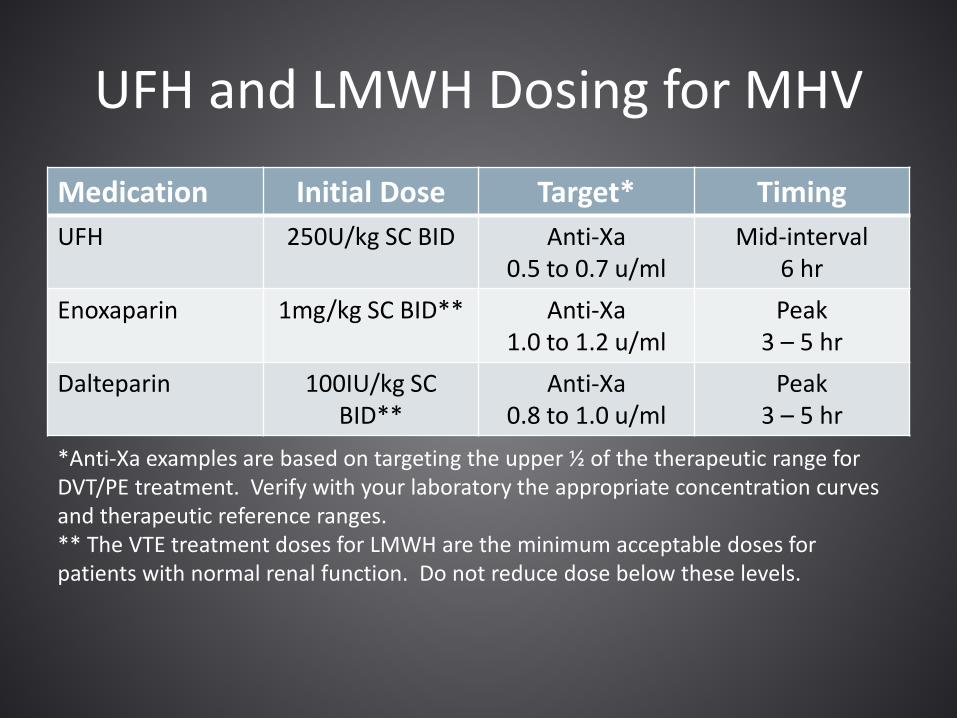
UFH and LMWH Dosing for MHV
Medication Initial Dose Target* Timing UFH 250U/kg SC BID Anti-Xa
0.5 to 0.7 u/ml Mid-interval
6 hr Enoxaparin 1mg/kg SC BID** Anti-Xa
1.0 to 1.2 u/ml Peak
3 – 5 hr Dalteparin 100IU/kg SC
BID** Anti-Xa
0.8 to 1.0 u/ml Peak
3 – 5 hr *Anti-Xa examples are based on targeting the upper ½ of the therapeutic range for DVT/PE treatment. Verify with your laboratory the appropriate concentration curves and therapeutic reference ranges. ** The VTE treatment doses for LMWH are the minimum acceptable doses for patients with normal renal function. Do not reduce dose below these levels.
Labor and Delivery for MHV
• Stop UFH/LMWH 24 hours prior to induction – IV UFH can be substituted in very high risk (e.g.
AVR/MVR) – stop 4 hours prior to induction
• Normal aPTT prior to epidural (UFH) • Restart UFH/LMWH at previous dose
– 12 hours after vaginal delivery – 24 hours after cesarean birth
• Bridge back to warfarin
Management of Long Term Anticoagulation for DVT/PE History
• Anticoagulation options: – Continue oral anticoagulation (warfarin/DOAC)
with frequent pregnancy testing OR – Transition to LMWH (preferred to UFH)
• Initial dosing is the same as MHV:
– Twice daily dosing is still preferred during pregnancy due to enhanced renal clearance
Acute DVT/PE During Pregnancy
• Uncomplicated DVT can be treated as an outpatient
• PE should be monitored as inpatient for at least 24 hours
• Anticoagulation options remain UFH and LMWH – LMWH preferred over UFH as outpatient
Monitoring Therapeutic UFH/LMWH
• Therapeutic UFH always requires monitoring during long term use – Anti-Xa or aPTT every 3 days until therapeutic then every 1
to 4 weeks – Adjust dose by 2000 to 4000 units per day – Target anti-Xa 0.35-0.7u/ml
• Therapeutic LMWH anti-Xa monitoring is optional for VTE – Periodic anti-Xa monitoring every 4 weeks , or – Adjust LMWH dose according to weight gain, or – No LMHW dose adjustment is also an option
Labor and Delivery for DVT/PE
• Similar to MHV, but rarely a need for IV UFH – Possible exceptions:
• Very recent (within 4 weeks) acute DVT/PE • Profound thrombophilia and extensive VTE history
• Bridge back to warfarin, or • Restart DOAC if not breastfeeding • Duration of therapy for first, pregnancy-
related DVT/PE is 3 to 6 months AND at least 6 weeks postpartum
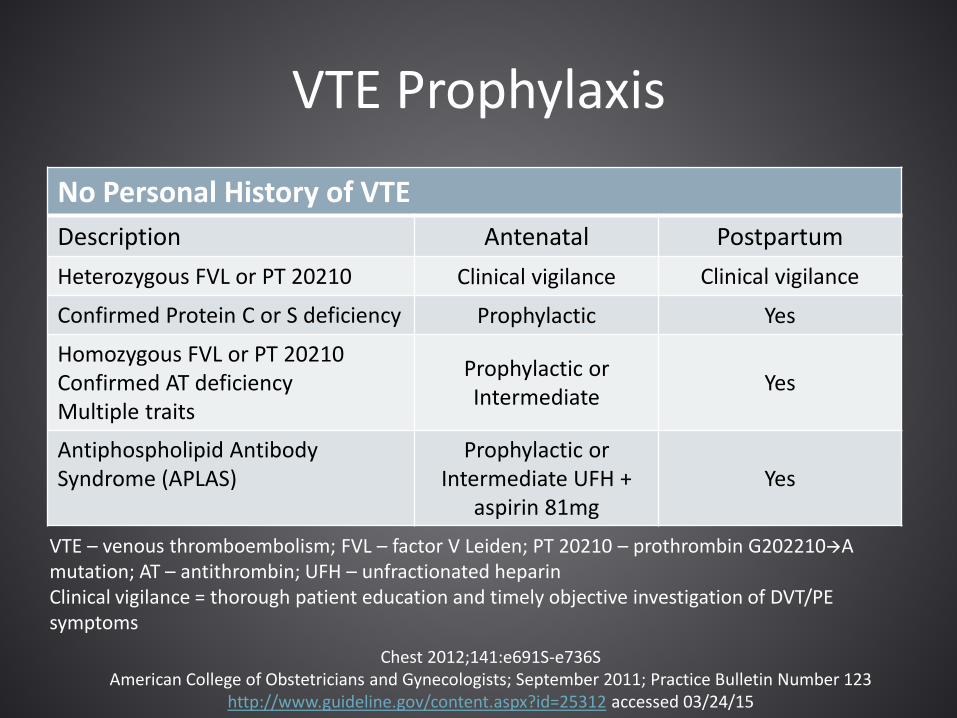
VTE Prophylaxis
No Personal History of VTE Description Antenatal Postpartum Heterozygous FVL or PT 20210 Clinical vigilance Clinical vigilance
Confirmed Protein C or S deficiency Prophylactic Yes
Homozygous FVL or PT 20210 Confirmed AT deficiency Multiple traits
Prophylactic or Intermediate Yes
Antiphospholipid Antibody Syndrome (APLAS)
Prophylactic or Intermediate UFH +
aspirin 81mg Yes
VTE – venous thromboembolism; FVL – factor V Leiden; PT 20210 – prothrombin G202210A mutation; AT – antithrombin; UFH – unfractionated heparin Clinical vigilance = thorough patient education and timely objective investigation of DVT/PE symptoms
Chest 2012;141:e691S-e736S American College of Obstetricians and Gynecologists; September 2011; Practice Bulletin Number 123
http://www.guideline.gov/content.aspx?id=25312 accessed 03/24/15
Why UFH for APLAS?
• Meta-analysis of women with APLAS found the combination of UFH and aspirin reduced the risk of pregnancy loss by 54%
• Quality of the evidence was not high, but this remains the only data to support an anticoagulant for prevention of miscarriage in any thrombophilia population
Cochrane Database Syst Rev. 2005 Apr 18;(2):CD002859
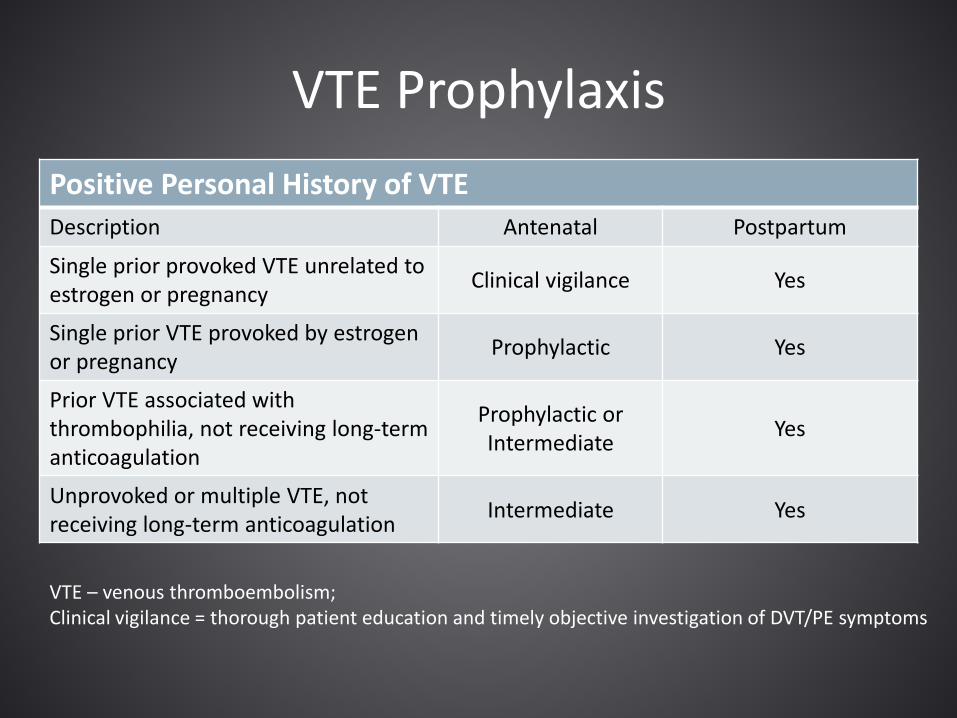
VTE Prophylaxis Positive Personal History of VTE Description Antenatal Postpartum
Single prior provoked VTE unrelated to estrogen or pregnancy Clinical vigilance Yes
Single prior VTE provoked by estrogen or pregnancy Prophylactic Yes
Prior VTE associated with thrombophilia, not receiving long-term anticoagulation
Prophylactic or Intermediate Yes
Unprovoked or multiple VTE, not receiving long-term anticoagulation Intermediate Yes
VTE – venous thromboembolism; Clinical vigilance = thorough patient education and timely objective investigation of DVT/PE symptoms
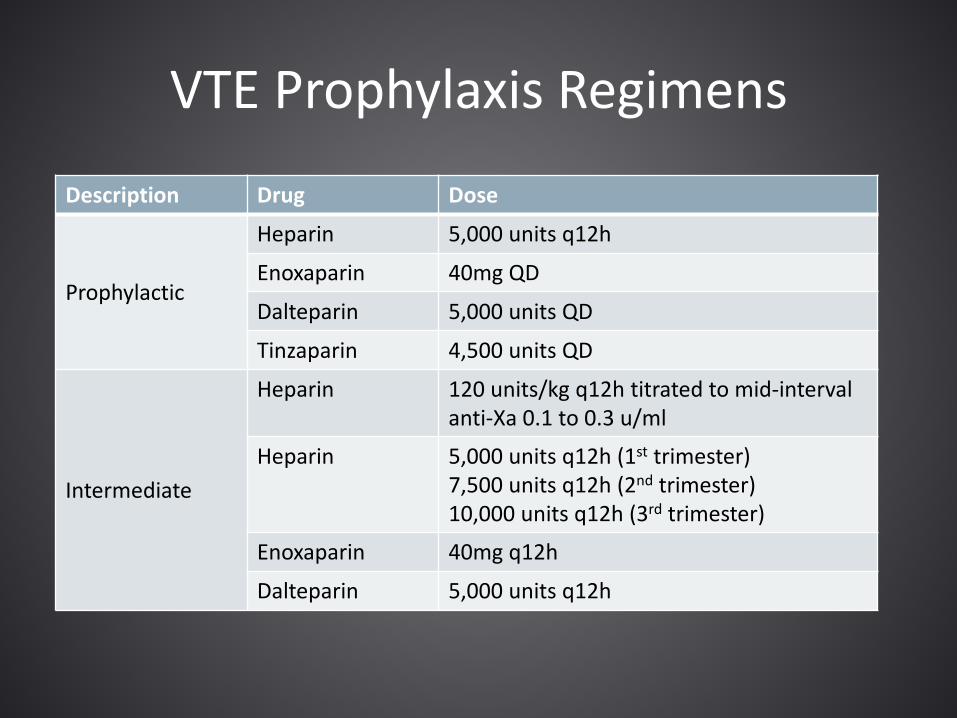
VTE Prophylaxis Regimens
Description Drug Dose
Prophylactic
Heparin 5,000 units q12h
Enoxaparin 40mg QD
Dalteparin 5,000 units QD
Tinzaparin 4,500 units QD
Intermediate
Heparin 120 units/kg q12h titrated to mid-interval anti-Xa 0.1 to 0.3 u/ml
Heparin 5,000 units q12h (1st trimester) 7,500 units q12h (2nd trimester) 10,000 units q12h (3rd trimester)
Enoxaparin 40mg q12h
Dalteparin 5,000 units q12h
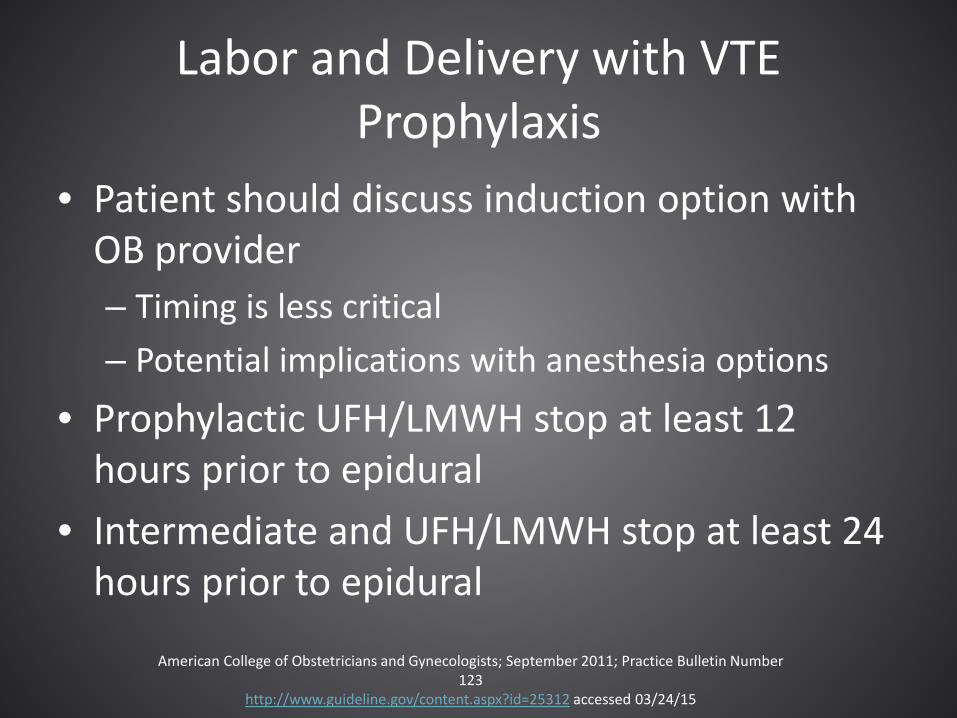
Labor and Delivery with VTE Prophylaxis
• Patient should discuss induction option with OB provider – Timing is less critical – Potential implications with anesthesia options
• Prophylactic UFH/LMWH stop at least 12 hours prior to epidural
• Intermediate and UFH/LMWH stop at least 24 hours prior to epidural
American College of Obstetricians and Gynecologists; September 2011; Practice Bulletin Number 123
http://www.guideline.gov/content.aspx?id=25312 accessed 03/24/15
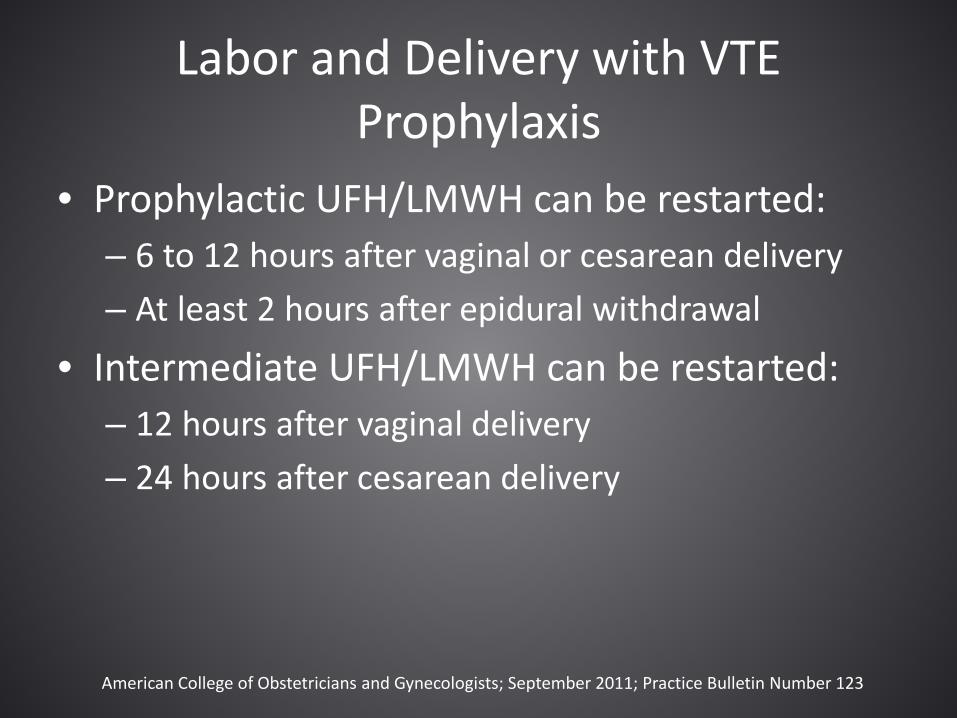
Labor and Delivery with VTE Prophylaxis
• Prophylactic UFH/LMWH can be restarted: – 6 to 12 hours after vaginal or cesarean delivery – At least 2 hours after epidural withdrawal
• Intermediate UFH/LMWH can be restarted: – 12 hours after vaginal delivery – 24 hours after cesarean delivery
American College of Obstetricians and Gynecologists; September 2011; Practice Bulletin Number 123
Postpartum VTE Prophylaxis Regimens
• Continue VTE prophylaxis 6 weeks postpartum – Resume the antenatal regimen, or – Transition to warfarin (INR 2-3)
Chest 2012;141:e691S-e736S
References you need to manage anticoagulation in pregnancy
https://www.asra.com/advisory-guidelines/article/1/anticoagulation-3rd-edition