Embed Size (px)
Citation preview

Dr. Dev PahlajaniDr. Dev PahlajaniMD,FACC,FSCAIMD,FACC,FSCAI
ANTICOAGULATION IN COMPLEX PCI
Chief of Interventional cardiology
Breach Candy Hospital and Consultant Cardiologist
Nanavati Heart Institute,Mumbai

Anticoagulation in complex PCI
STEMI,NSTEMI COMPLEX ANATOMY CTO,BIF.MULTIPLE STENTS NEED FOR DAPT+OAC PROSTHETIC VALVE AFIB,LV THROMBUS +TIA

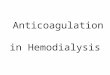
Major Bleeding is Associated with an Increased Risk of Hospital Death in ACS Patients
Moscucci et al. Moscucci et al. Eur Heart JEur Heart J 2003;24:1815-23 2003;24:1815-23
GRACE Registry in 24,045 ACS patientsGRACE Registry in 24,045 ACS patients
*After adjustment for comorbidities, clinical presentation and hospital therapies*After adjustment for comorbidities, clinical presentation and hospital therapies**p<0.001 for differences in unadjusted death rates**p<0.001 for differences in unadjusted death rates
OR (95% CI) OR (95% CI) 1.64 (1.18 to 2.28*)1.64 (1.18 to 2.28*)
00
Overall ACSOverall ACS UAUA NSTEMI NSTEMI STEMISTEMI
1010
2020
3030
4040
****
**** ****
****
5.15.1
18.618.6
3.03.0
16.116.1
5.35.3
15.315.3
7.07.0
22.822.8
Inho
spita
l dea
th (%
)In
hosp
ital d
eath
(%)
In hospital major bleedingIn hospital major bleeding YesYes
NoNo

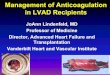
Blood Transfusion is Associated with an Increased 30-Day Mortality in NSTEMI
Rao et al. Rao et al. JAMAJAMA 2004;292:1555-62 2004;292:1555-62
N=24,112 ACS patients from GUSTO IIb, PURSUIT and PARAGONN=24,112 ACS patients from GUSTO IIb, PURSUIT and PARAGON
*Adjusted for baseline characteristics, bleeding and transfusion propensity and nadir hematocrit*Adjusted for baseline characteristics, bleeding and transfusion propensity and nadir hematocrit
HR=3.94*; HR=3.94*; 95%CI: 3.26 to 4.7595%CI: 3.26 to 4.75
30-day 30-day death ratedeath rate
TransfusionTransfusion
No TransfusionNo Transfusion
Log-rank Log-rank p<0.001p<0.001
00
0.020.02
0.040.04
0.060.06
0.080.08
0.100.10
55 1010 1515 2020 2525 3030DayDay
8.00%8.00%
3.08%3.08%
Cum
ulati
ve m
orta
lity
Cum
ulati
ve m
orta
lity

Potential Mechanisms for the Higher Morbidity/Mortality Associated with Bleeding
1. Cessation of antithrombotic therapies after bleeding may increase subsequent ischemic events
2. Patients who bleed may have an heightened inflammatory state
3. Adverse effects of hypotension
4. Adverse effects of transfusion
5. Common risk factors for bleeding and adverse outcome
1. Gibbons & Fuster. N Engl J Med 2006;354:1524-7 2. Califf. JAMA 2006;295:1579-803. Jozic J. AJC 2006;98:36M

Sweet spot for P2Y12 inhibition
M.Valgimigli, EUROPCR, 2013

Plethora of choices for Antithrombotic therapy
• Anticoagulants: UFH LMWH Fonda Bival
• Antiplatelets: ASA Clopidogrel (dose) Prasugrel (dose) Ticagrelor
• IV antiplatelets : None AbcixEpt/ Tiro (timing)
• Oral anticoagulant None Rivaroraban

Anticoagulation strategies in complex PCI
OAC WITH ?DAPT? TOAT? SAPT
PPCI BIVALURIDIN,LMWH

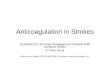
Primary Outcome Measures (ITT)Primary Outcome Measures (ITT)
12.1
8.3
5.5
9.2
4.9 5.4
0
5
10
15
20
Net adverse clinicalevents
Major bleeding* MACE**
30 d
ay e
vent
rate
s (%
)
Heparin + GPIIb/IIIa inhibitor (N=1802) Bivalirudin monotherapy (N=1800)
RR = 0.99 [0.76, 1.30] RR = 0.99 [0.76, 1.30] PPsupsup = 0.95 = 0.95
RR = 0.60 [0.46, 0.77]RR = 0.60 [0.46, 0.77]PPsupsup ≤ 0.0001 ≤ 0.0001
RR = 0.76 [0.63, 0.92] RR = 0.76 [0.63, 0.92] PPsupsup = 0.005 = 0.005
1 endpoint 1 endpoint
*Not related to CABG*Not related to CABG**MACE = All cause death, reinfarction,**MACE = All cause death, reinfarction,
ischemic TVR or strokeischemic TVR or strokeStone GW, et al. Stone GW, et al. N Engl J MedN Engl J Med. 2008 May 22;358(21):2218-30. 2008 May 22;358(21):2218-30

HORIZONS AMI—30-Day Stent Thrombosis (N=3,124)
UFH + GP IIb/IIIaUFH + GP IIb/IIIa(N=1553)(N=1553)
BivalirudinBivalirudin(N=1571)(N=1571)
PPValueValue
ARC definite or ARC definite or probable*probable* 1.9%1.9% 2.5%2.5% 0.330.33
DefiniteDefinite 1.4%1.4% 2.2%2.2% 0.110.11
ProbableProbable 0.5%0.5% 0.3%0.3% 0.260.26
Acute Acute (≤24 hrs)(≤24 hrs) 0.3%0.3% 1.3%1.3% 0.00090.0009
Subacute Subacute (>24 hrs – 30d)(>24 hrs – 30d) 1.7%1.7% 1.2%1.2% 0.300.30
Stone GW, et al. N Engl J Med. 2008 May 22;358(21):2218-30

WHY IS THERE AN EXCESS OF EARLY STENT THROMBOSIS IN HORIZONS AMI ?
Clopidogrel
BIVALIRUDIN
ASPIRIN
PPCI 24hrs

Bivalirudin plasma levels in PCI
• Plasma concentrations vs time(25 min elimination half life)• Bolus plus infusion (for the duration of the procedure) is
required dosing

HORIZONS: Impact of pre-randomized heparin on Acute Stent
Thrombosis


Enrolment7962 consecutive patients enrolled for elective or primary PCI in
144 hospitals across 23 countries

ENOXAPARIN ALL COMERS BCH ( N = 1111)
NON PAMI ( N = 1038)
PAMI ( N = 73)
NO GP IIb (578)ANGIOSEAL
105
GP II b (312 )ANGIOSEAL 45
NO GP II b 43NO MAJOR
BLEED
GP II b (30)1 DIED OF GI
BLEED
NO GP II b 43NO MAJOR
BLEED

Independent predictors of bleeding

Antiplatelet strategy in patients on OAC
• Should we stop or continue OAC pre PCI?• Should we bridge with heparin?• Post PCI triple drug therapy or dual drug ?

Peri procedural management
P. Karjalainen, EUROPCR, 2013
Current guidelines recommend that in AF-patients with ine or
more stroke factors (CHA2DS2-VASc score), OAC is recommended.
During elective angiography and PCI?
1)Discontinue OAC 5-7 days prior + Bridging heparin
2)Discontinue OAC (5-7 D) + no additional/ Briding heparin
3)Uninterrupted OAC with therapeutic INR level (2.0-3.0) .No
additional heparins

Wide variability in Practice on oral anticoagulation therapy pts undergoing
coronary stenting
M.Valgimigli, EUROPCR, 2013
Tx at discharge in the CRUSADE registry among 1,247 pts with AF

A. Rubboli, EUROPCR, 2013


WOEST: Primary Endpoint: Total number of TIMI bleeding events

WOEST: Secondary Endpoint( Death, MI, TVR, Stroke, ST

Take home messageBleeding is as important as preventing ischaemic
complications• Revisit bivalirudin with new protocol• Consider enoxaparin - has less bleeding• Continue OAC prior to PCI or cor.Angio-inr
around 2• OAC And the inopyridine safer than OAC And
DAPT