Embed Size (px)
DESCRIPTION
Management of periarticular fractures
Citation preview
Articular fractures
Principles of management
Ram K Shah
Fractures Around Knee Joint:
Femur, Tibia, Patella.
Aims & objectives
- Pathophysiology of articular healing after fracture
- Indications for treatment
- Treatment principles
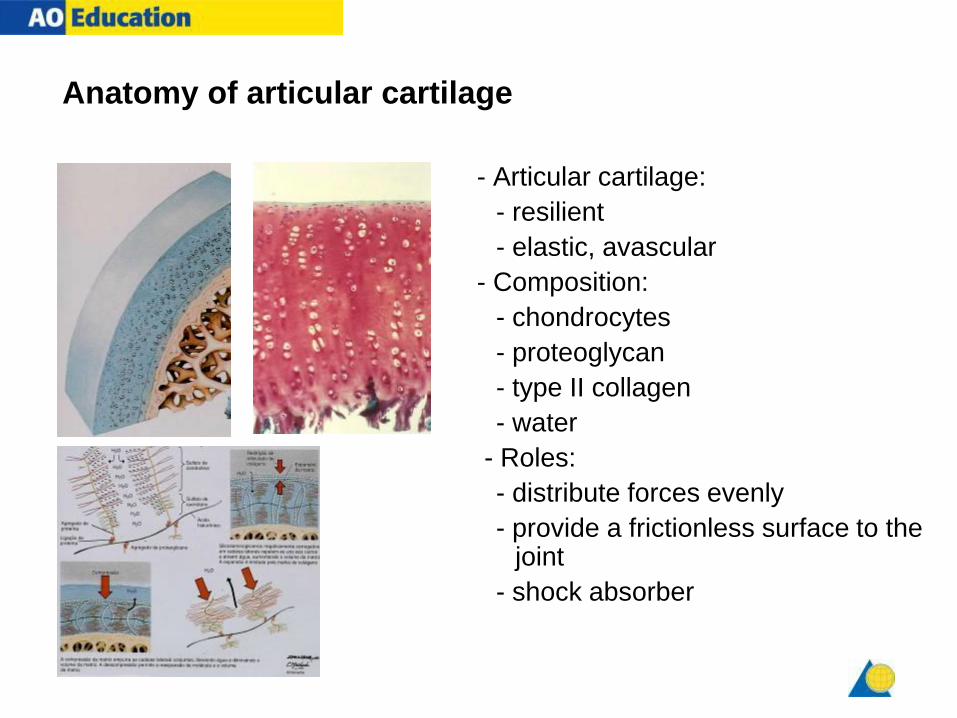
Anatomy of articular cartilage
- Articular cartilage:
- resilient
- elastic, avascular
- Composition:
- chondrocytes
- proteoglycan
- type II collagen
- water
- Roles:
- distribute forces evenly
- provide a frictionless surface to the joint
- shock absorber
Nutrition of articular cartilage
- Nutrition comes from synovial fluid
- Flow of synovial fluid requires motion and load
- To preserve injured articular cartilage: early motion and some load
Articular cartilage response to trauma
- Very sensitive to injury
- Poor healing potential
- Early mobilization enhances healing (Salter et al 1980)
- Anatomical reduction + interfragmentary compression + movement
= healing with hyaline cartilage
(Mitchell and Shepard 1980)
Clinical and experimental evidence—I
- Immobilization results in joint stiffness
- Immobilization of the articular fractures treated by ORIF (open
reduction and internal fixation) results in much greater stiffness
- Depressed osteochondral fragments which do not reduce by
closed manipulation and traction are impacted and will not reduce
by closed means
- Major depressions don’t fill with fibrocartilage, the
resulting instability is permanent
- Anatomical reduction and stable fixation of articular
fragments is necessary to restore joint congruency
- Metaphyseal defects must be filled with bone graft to
prevent articular redisplacement
Clinical and experimental evidence—II
- Metaphyseal and diaphyseal displacement must be reduced to
prevent joint overload
- Immediate motion is necessary to prevent joint stiffness and to
ensure articular cartilage healing and recovery, this requires stable
internal fixation
Clinical and experimental evidence—III
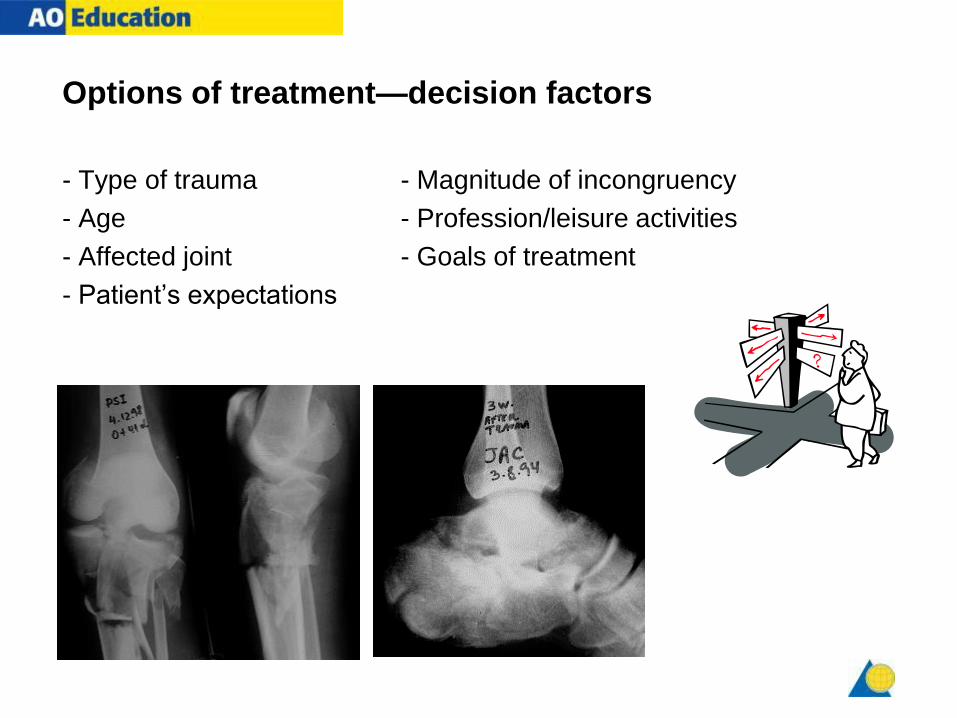
Options of treatment—decision factors
- Type of trauma - Magnitude of incongruency
- Age - Profession/leisure activities
- Affected joint - Goals of treatment
- Patient’s expectations
Principles of treatment
- Understand the injury
- Preoperative planning
- Timing
- Surgical approach
- Articular reduction
- Buttress of the metaphysis
- Postoperative care
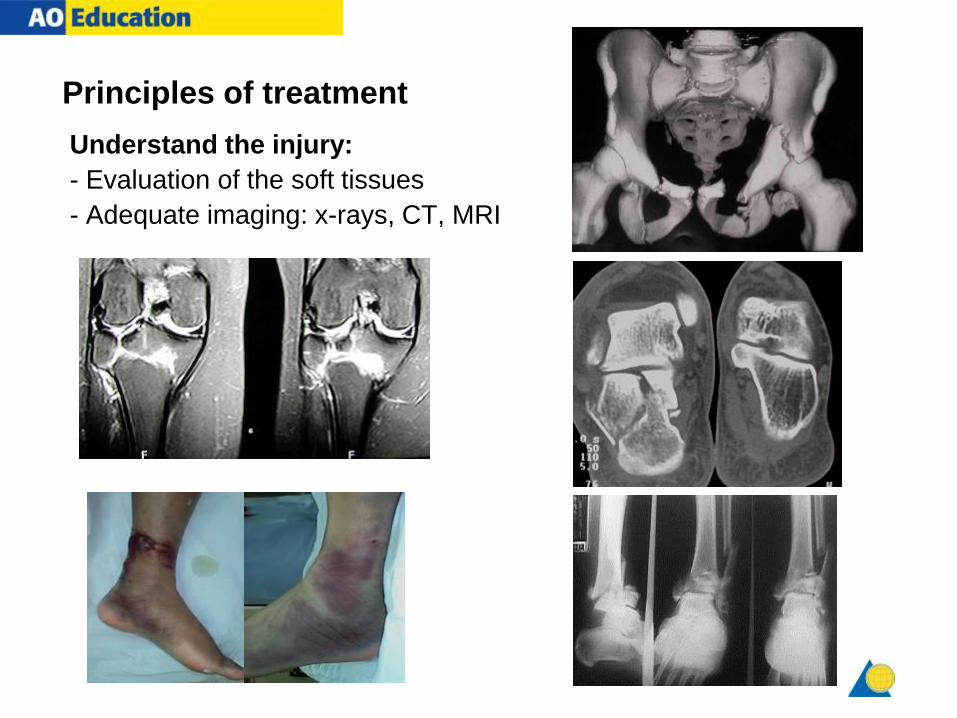
Principles of treatment
Understand the injury:
- Evaluation of the soft tissues
- Adequate imaging: x-rays, CT, MRI
Principles of treatment
Preoperative planning:
- Positioning
- Approach
- Implant selection
- Reduction tactics
- Sequence of fixation
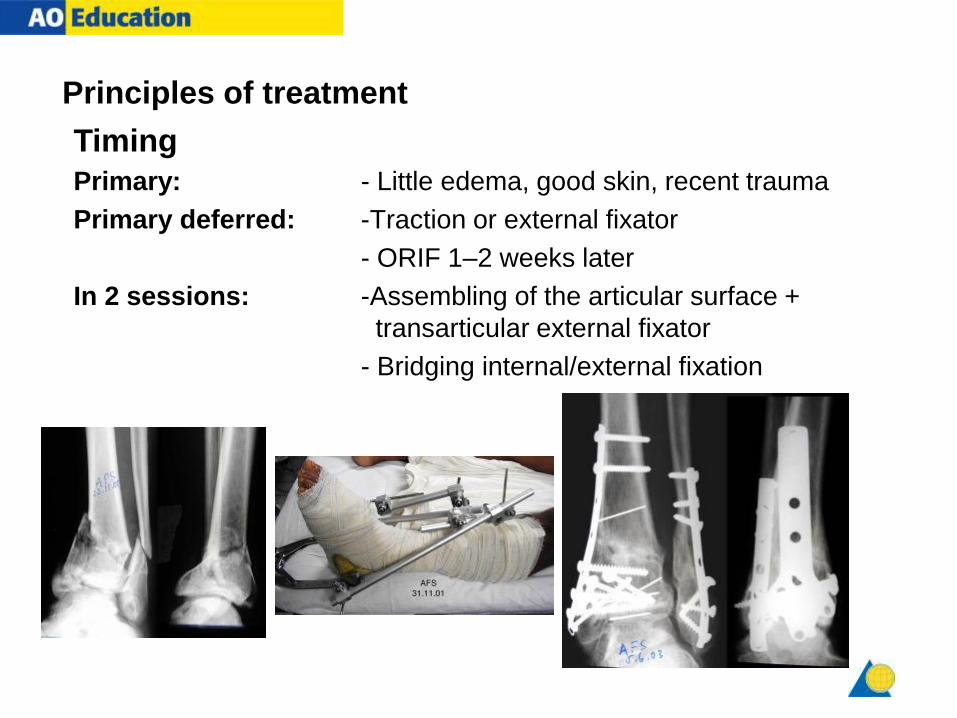
Principles of treatment
Primary: - Little edema, good skin, recent trauma
Primary deferred: -Traction or external fixator
- ORIF 1–2 weeks later
In 2 sessions: -Assembling of the articular surface +
transarticular external fixator
- Bridging internal/external fixation
Timing
Principles of treatment
Surgical approach:
- Soft- tissue condition
- The least traumatic possible
- Indirect reduction
- Arthroscopy, C-arm, percutaneous

1 year follow-up
C-arm Indirect reduction
Percutaneous fixation
Principles of treatment
Articular reduction:
- Interfragmentary compression
- Step-by-step K-wires
- Bone graft into the defects
- Gaps forgiving, step-offs dangerous
Principles of treatment
- Articular reduction
- Buttress of the metaphysis:
- Usually with a bridging or a buttress plate

Principles of treatment
Postoperative care:
- Pain-free active mobilization
- Isometrics in day 1
- Physiotherapist
- Limited weight bearing (15–20 K)
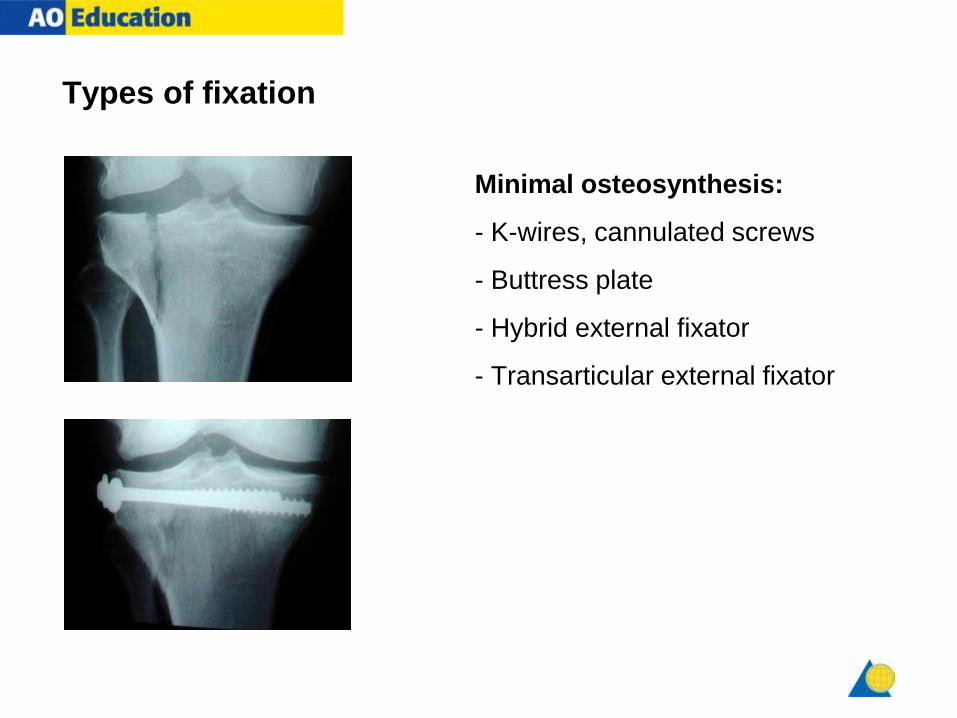
Types of fixation
Minimal osteosynthesis:
- K-wires, cannulated screws
- Buttress plate
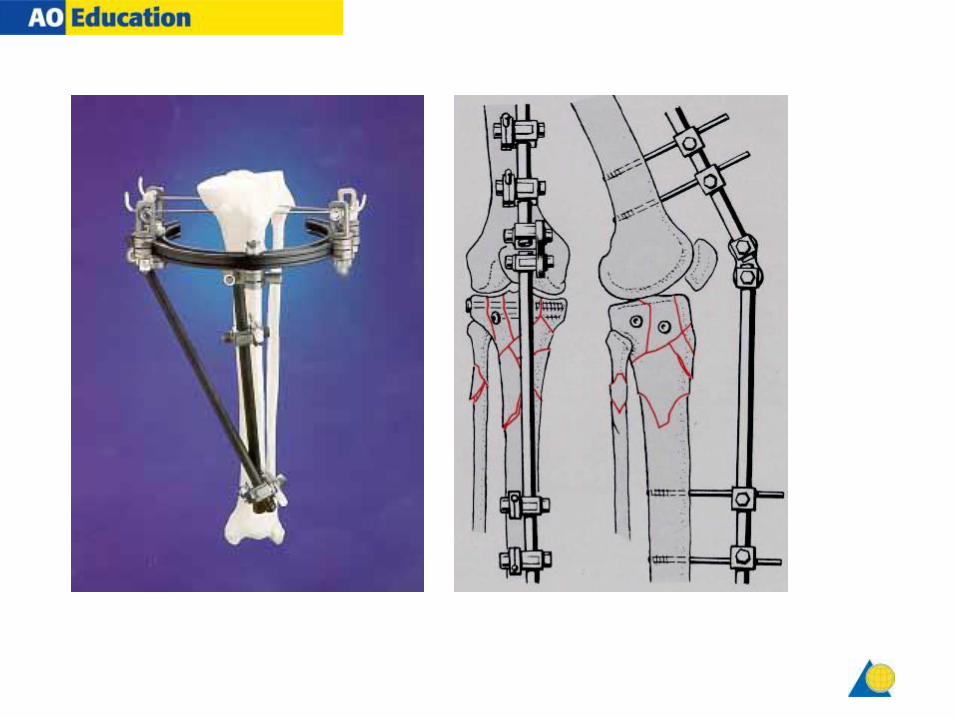
- Hybrid external fixator
- Transarticular external fixator

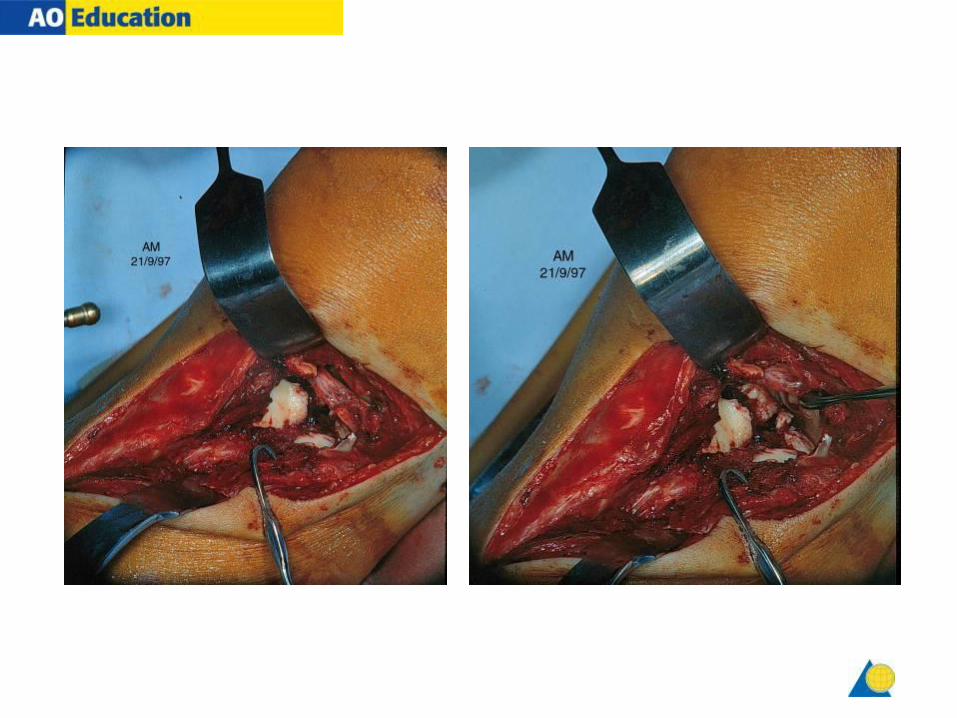
32-year-old male
41-B3
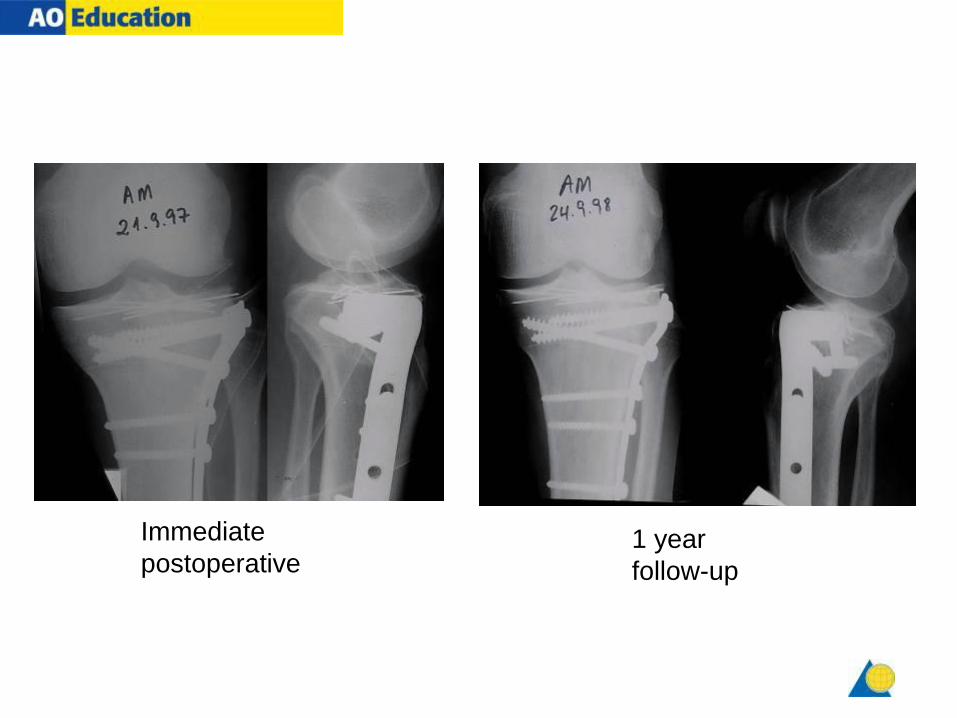
Immediate
postoperative 1 year
follow-up

33-C2
33-year-old female, polytrauma, multiple fractures
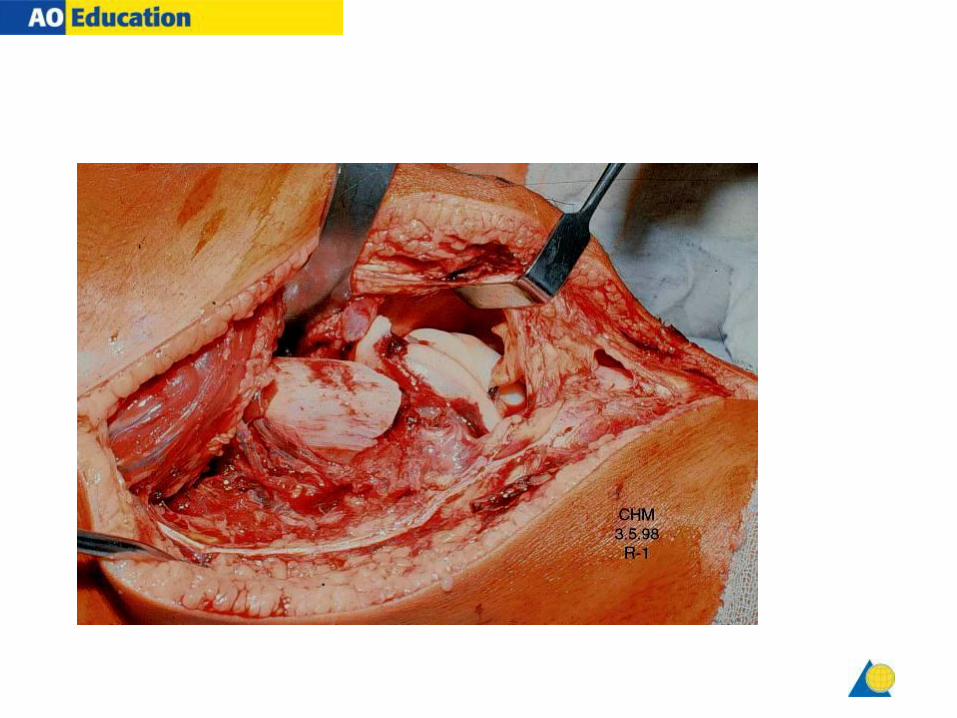
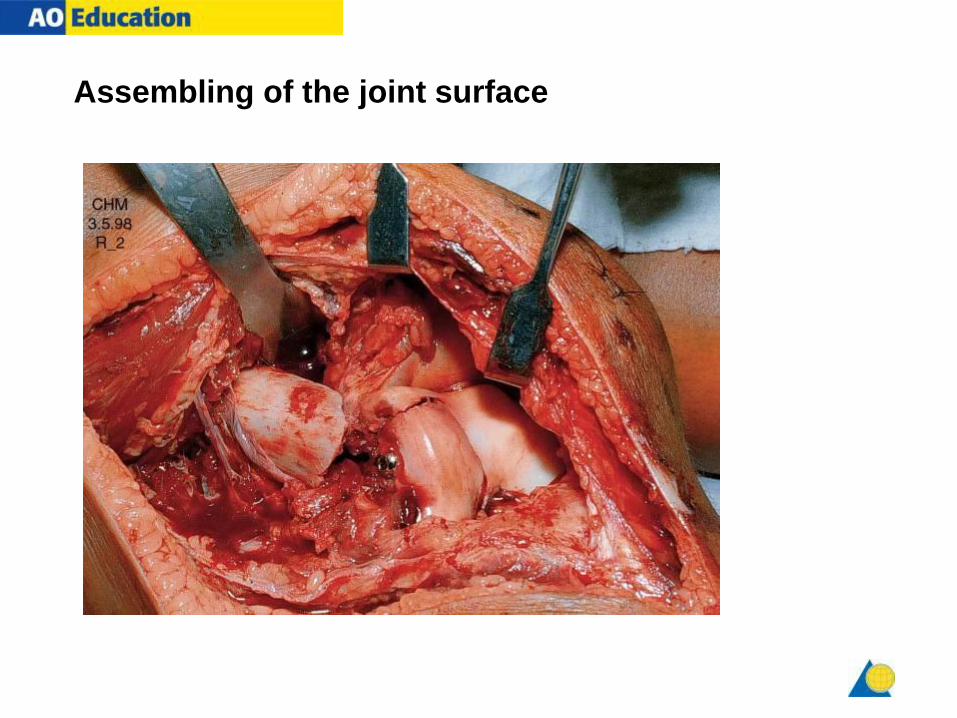
Assembling of the joint surface

Bridging plate joining the condyles and diaphysis


7 months

31-year-old, male
41-C3
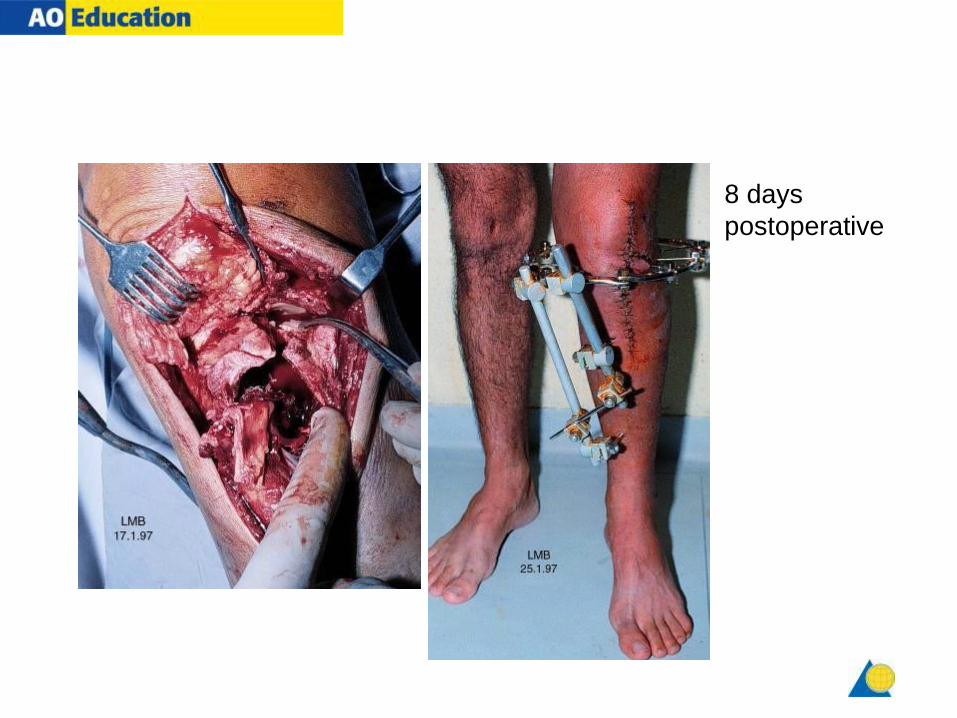
8 days
postoperative

First xRays

Tibial Condylar Fracture Treated by TRACTION

After Treatment
Evidence:
• Tibia: Conservative treatment is a valid option for fractures with minimal
displacement and surgical treatment is justified for severely displaced or
depressed fractures. Attention must be paid to the recognition and
restoration of joint stability and articular surface congruency for a
satisfactory outcome. (Med J Malaysia. 2005 Jul;60 Suppl C:83-90 )
• Femur: Regardless of treatment method, goals include restoration of
articular congruity, anatomical length, rotation, and axial alignment while
establishing adequate fixation to initiate early and unrestricted range of
motion.(J Knee Surg. 2007 Jan;20(1):56-66. )
• Calcaneum: The results of this 15-year follow-up of displaced intra-
articular calcaneal fracture randomised controlled trial were equivalent
between conservative and operative treatment and demonstrate similar
findings to those at one year follow-up. (Injury. 2007 Jul;38(7):848-55. Epub 2007
Apr 18. )
Take Home Message
- Intra-articular Condylar Fracture of Tibia & Femur requires accurate reduction and early joint motion for good anatomical and functional recovery.
- Conservative treatment with Traction or Hinged Brace is applied in selected patients for useful functional recovery.
- Undisplaced Burst Fracture Patella is treated conservatively.