Embed Size (px)
Citation preview

Extra-articular Proximal Tibial Fractures: Nail or Plate?
John C. Kurylo, MDPaul Tornetta III, MD
Proximal tibial fractures are challeng-ing to treat because of the frequency ofsubstantial soft-tissue injury, thestrong deforming forces involved, and
the need for accurate alignment. Thischapter will focus primarily on extra-articular proximal tibial fractures andthose with minimally displaced intra-
articular extension that can be treatedwith intramedullary (IM) nailing orplate fixation.
Proximal tibial fractures make up5% to 11% of all tibial injuries andtypically are caused by a high-energymechanism.1 Because of the locationof these fractures in the highly vascularand muscular area of the lower extrem-ity, there is a higher incidence of arte-rial injury, muscle damage, and com-partment syndrome than in diaphysealfractures.2,3 Burgess et al4 reportedthat the most proximal tibial fracturesresult from pedestrians being struck byautomobiles; the extent of the soft-tissue injury is often grossly underesti-mated.
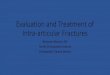
The AO/Orthopaedic Trauma As-sociation (OTA) system is the mostwidely used system for classifyingproximal tibial fractures. Type A frac-tures are extra-articular, type B frac-tures are partially articular, and type Cfractures are articular with a metaphys-eal component. Both IM nails andplates are appropriate for treatingtype A and simple intra-articular typeC1 fracture patterns5 (Figure 1).
Regardless of the fixation methodchosen, traditional fracture care princi-ples should be followed. Open frac-tures are treated with urgent irrigationand débridement of the devitalized tis-
Dr. Tornetta or an immediate family member serves as a board member, owner, officer, or committee member ofthe American Orthopaedic Association and the Orthopaedic Trauma Association; has received royalties fromSmith & Nephew; and serves as a paid consultant to or is an employee of Smith & Nephew. Neither Dr. Kurylonor any immediate family member has received anything of value from or owns stock in a commercial companyor institution related directly or indirectly to the subject of this chapter.
AbstractThe surgical goals for treating proximal tibial fractures are to restore articular con-gruity, the mechanical axis, and knee motion while avoiding soft-tissue complica-tions. The fracture pattern should be correctly identified and understood. For frac-tures with minimal intra-articular extension, fracture fixation with anintramedullary nail can decrease the risk of infection because it uses a small inci-sion that is not placed directly over the injured soft tissue, and it provides better ax-ial load sharing than a plate. Using the semiextended technique, choosing the cor-rect starting portal, incorporating blocking screws or stability screws into thefixation construct, and using mini-open reduction and internal fixation of thefracture will help achieve the goals of fracture fixation with an intramedullarynail.
All proximal tibial fractures can be treated successfully with a plate or multipleplates. When a plate is used, the surgical approach and technique should minimizesoft-tissue damage and account for future surgical procedures that may be needed.Fractures with intra-articular involvement and/or comminution of the medialmetaphyseal region are appropriately treated with dual plating. Extra-articularfractures without major medial comminution may be treated with a locked lateralplate. Final union rates for patients treated with either intramedullary nail orplate fixation are reported at 96% and 97%, respectively. A prospective, random-ized, multicenter study is currently in progress to further clarify and advance thetreatment of proximal tibial fractures.
Instr Course Lect 2013;62:61-77.
6
© 2013 AAOS Instructional Course Lectures, Volume 62 61
sue. Temporary external fixation maybe used, particularly if initial definitivesoft-tissue coverage cannot be obtainedor if the surgeon chooses to performthe definitive reduction and fixationunder more ideal conditions. Thesefractures should be closely monitoredbecause of the substantial risk for com-partment syndrome.
ImagingThe surgical goals for treating proxi-mal tibial fractures are to restore artic-ular congruity, the mechanical axis,and knee motion while avoiding soft-tissue complications. To accomplishthese goals, correct identification ofthe fracture pattern is necessary. APand lateral radiographs may not pro-vide adequate information on fracture
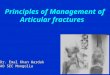
comminution, displacement, planes,and, especially, intra-articular displace-ment. A caudad plateau view, with thex-ray beam directed 10° caudal on theAP orientation, will provide a betterunderstanding of the articular exten-sion. Oblique internal and external ro-tation views may provide additionalinformation about the fracture. CTwill provide the best informationabout intra-articular extension, if pres-ent. This is particularly helpful in de-termining if a fracture extends into thearea of portal placement for nailing(Figure 2). This chapter’s authors typ-ically obtain a CT scan if an intra-articular fracture is seen on radio-graphic studies.
Closed TreatmentAlthough closed treatment of proximaltibial fractures is beyond the scope ofthis chapter, it is an option that shouldbe considered. Sarmiento et al6 cham-pioned the nonsurgical management
Figure 1 Illustration of the AO classification system of proximal tibial frac-tures. Type A fractures are extra-articular, type B fractures are partially artic-ular, and type C fractures are articular with a metaphyseal component. (Re-produced from Hiesterman TG, Shafiq BX, Cole PA: Intramedullary nailing ofextra-articular proximal tibia fractures. J Am Acad Orthop Surg 2011;19(10):690-700.)
Figure 2 AP tibia (A), lateral tibia (B), and lateral knee (C) radiographs and CT scan (D) of a proximal tibial fractureshowing fracture extension into the nail portal (circle). Postoperative AP (E) and lateral (F) radiographs show joint reduc-tion with two anterior-to-posterior screws after IM nailing.
Trauma
62 © 2013 AAOS Instructional Course Lectures, Volume 62
of proximal tibial fractures. The au-thors reported on 68 patients withnonarticular proximal tibial fractureswho were treated with a long leg cast.In patients with proximal tibial andfibular fractures, 84% had acceptableoutcomes (less than 5° of angulation inany plane) at union. Based on these re-sults, nonsurgical treatment can beconsidered for patients with goodalignment in the initial cast or those
who present without fracture displace-ment.
Treatment With an IM NailIn early reports, proximal tibial frac-ture treatment with IM nailing was as-sociated with high rates of malalign-ment and loss of proximal fragmentfixation. In 1995, Lang et al1 reportedthat 84% of their patients treated withIM nailing had sagittal malunion, and25% had loss of reduction. Freedmanand Johnson7 reported that 58% ofproximal tibial fractures treated withIM nailing resulted in malalignment,and 83% of these fractures were seg-mental or comminuted. It is importantto note that unlocked transverse screwswere used in these early series; thesescrews provided only uniaxial stabilityand may have contributed to the lossof reduction.
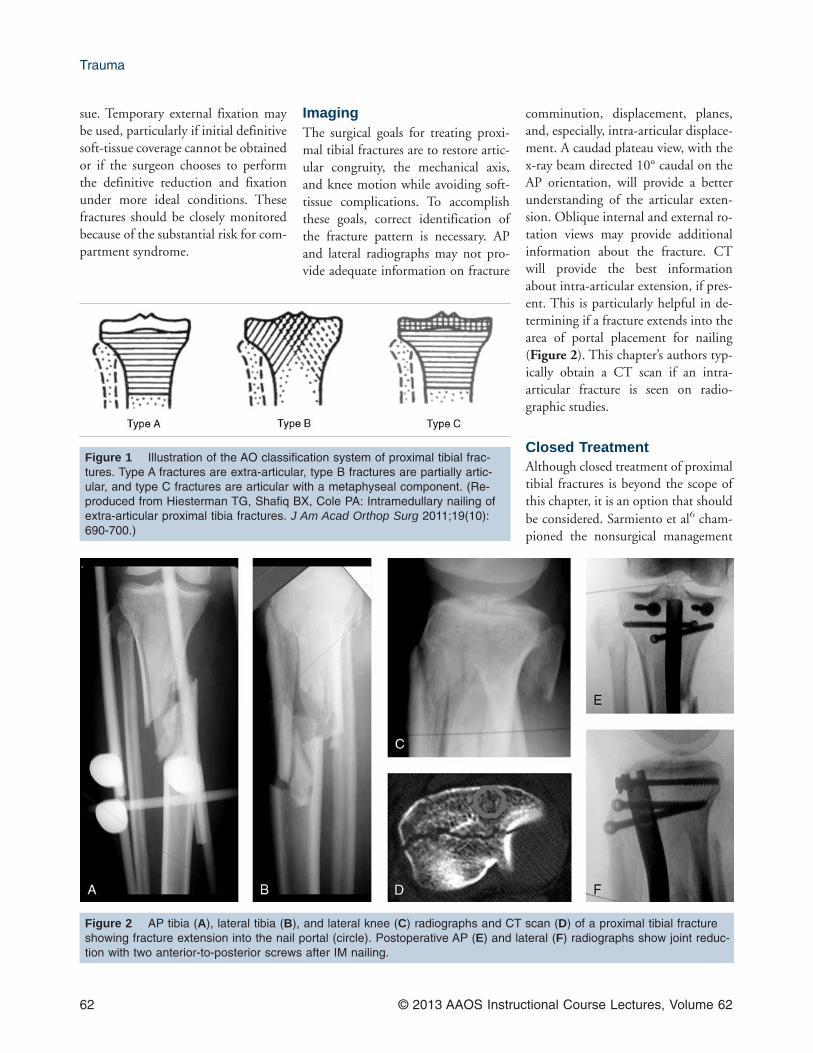
Malreductions are mainly caused byerrant portal placement. The mostcommon error is a starting portal thatis too medial. When nailing a proximaltibial fracture, the nail tends to lieagainst the lateral portion of the proxi-mal tibia. If the portal is medial, thiswill result in a valgus deformity (Fig-ure 3). A more lateral starting portalwill prevent a valgus deformity. Flex-ion and posterior translation at thefracture site is the second most com-mon deformity. Early IM nail designsexacerbated the posterior translational
deformity of the proximal tibial frac-ture when the proximal bend of thetibial nail was distal to the fracturesite.8
The relative contraindications forusing IM nailing for proximal tibialfractures include a narrow IM canal,inability to pass a nail because of an ex-isting canal deformity, or the presenceof a tibial base plate in a total knee ar-throplasty or knee fusion. IM nailingfor tibial fractures in pediatric patientsshould be approached with caution.Court-Brown et al9 reported on 52 ad-olescent patients between the ages of13 and 16 years who had a tibial frac-ture treated with IM nailing. Partialgrowth arrest of the proximal tibialphysis did not develop in any of thepatients.
Many techniques have been shownto be helpful with complex proximaltibial nailing (Table 1). In general, IMnailing is an attractive method fortreating proximal tibial fractures. Itmay decrease the risk of infection be-cause it uses a small incision that is notplaced directly over the injured soft tis-sue, and it provides better axial loadsharing than a plate. To achieve ade-quate reduction with IM nailing, it isnecessary to understand the character-istics of the fracture and the deformingmechanical forces acting on theproximal tibia.7 The patella tendon,
Figure 3 A, A medial startingportal for nail placement will create avalgus deformity at the fracture site.The short arrow represents a startingportal that is too medial. The dashedline represents the nail trajectory ifthe nail were to follow the originaltrajectory. However, with a startingportal that is too medial, the fracturegaps medially, a valgus deformity re-sults, and the nail’s final position isdifferent than originally planned(large curved arrow). B, A more lat-eral starting portal aids in proper an-gulation. The short arrow representsthe correct starting portal. The nail isintroduced and follows the correcttrajectory without causing a varus ora valgus deformity. (Reproducedfrom Tornetta P III: Technical consid-erations in the surgical managementof tibial fractures. Instr Course Lect1997;46:271-280.)
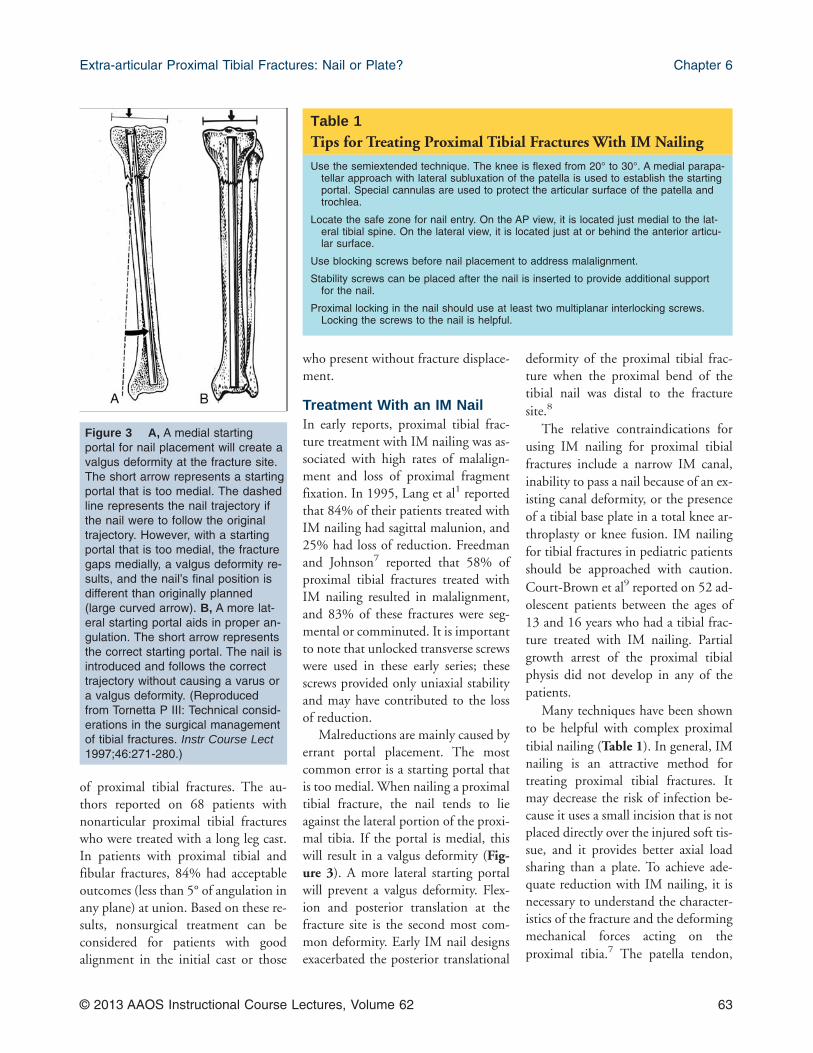
Table 1Tips for Treating Proximal Tibial Fractures With IM Nailing
Use the semiextended technique. The knee is flexed from 20° to 30°. A medial parapa-tellar approach with lateral subluxation of the patella is used to establish the startingportal. Special cannulas are used to protect the articular surface of the patella andtrochlea.
Locate the safe zone for nail entry. On the AP view, it is located just medial to the lat-eral tibial spine. On the lateral view, it is located just at or behind the anterior articu-lar surface.
Use blocking screws before nail placement to address malalignment.
Stability screws can be placed after the nail is inserted to provide additional supportfor the nail.
Proximal locking in the nail should use at least two multiplanar interlocking screws.Locking the screws to the nail is helpful.
Extra-articular Proximal Tibial Fractures: Nail or Plate? Chapter 6
© 2013 AAOS Instructional Course Lectures, Volume 62 63
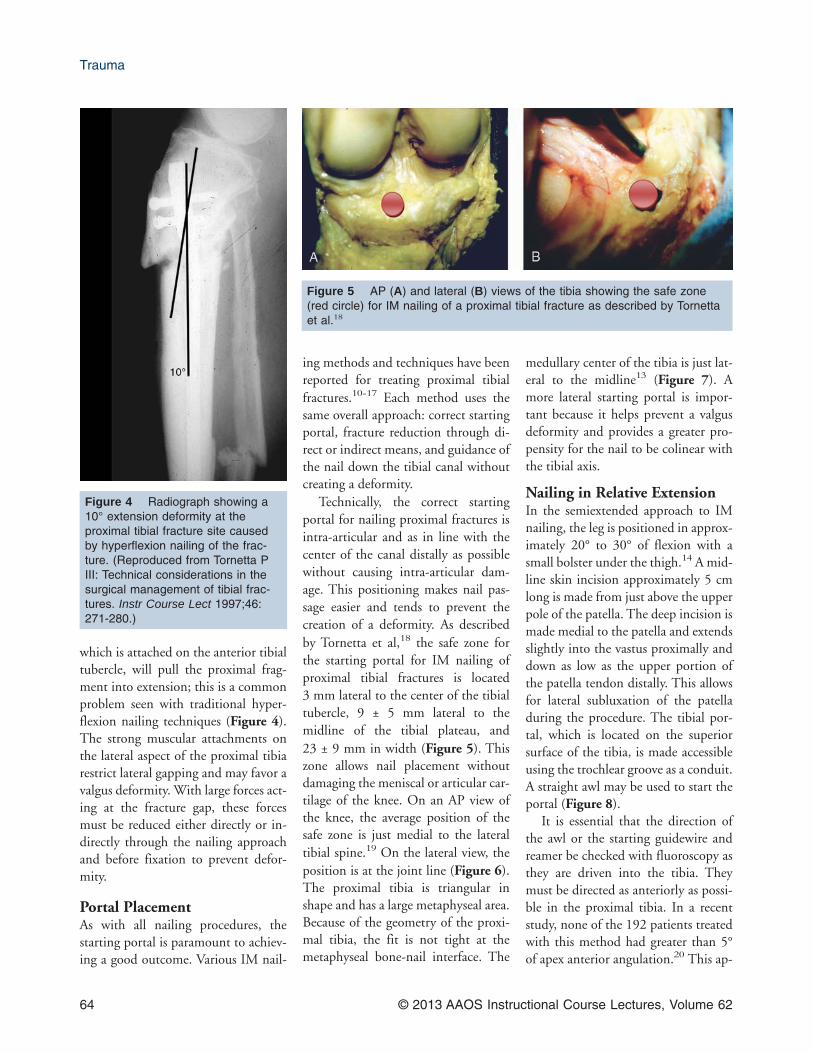
which is attached on the anterior tibialtubercle, will pull the proximal frag-ment into extension; this is a commonproblem seen with traditional hyper-flexion nailing techniques (Figure 4).The strong muscular attachments onthe lateral aspect of the proximal tibiarestrict lateral gapping and may favor avalgus deformity. With large forces act-ing at the fracture gap, these forcesmust be reduced either directly or in-directly through the nailing approachand before fixation to prevent defor-mity.
Portal PlacementAs with all nailing procedures, thestarting portal is paramount to achiev-ing a good outcome. Various IM nail-
ing methods and techniques have beenreported for treating proximal tibialfractures.10-17 Each method uses thesame overall approach: correct startingportal, fracture reduction through di-rect or indirect means, and guidance ofthe nail down the tibial canal withoutcreating a deformity.
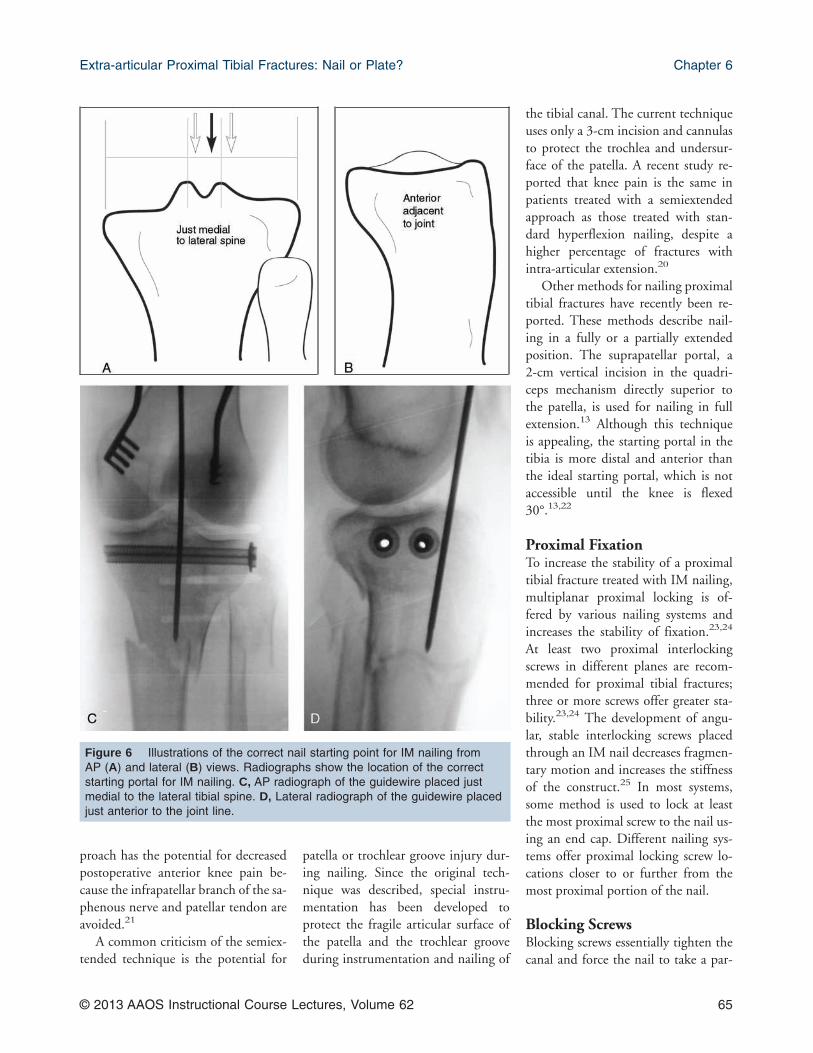
Technically, the correct startingportal for nailing proximal fractures isintra-articular and as in line with thecenter of the canal distally as possiblewithout causing intra-articular dam-age. This positioning makes nail pas-sage easier and tends to prevent thecreation of a deformity. As describedby Tornetta et al,18 the safe zone forthe starting portal for IM nailing ofproximal tibial fractures is located3 mm lateral to the center of the tibialtubercle, 9 ± 5 mm lateral to themidline of the tibial plateau, and23 ± 9 mm in width (Figure 5). Thiszone allows nail placement withoutdamaging the meniscal or articular car-tilage of the knee. On an AP view ofthe knee, the average position of thesafe zone is just medial to the lateraltibial spine.19 On the lateral view, theposition is at the joint line (Figure 6).The proximal tibia is triangular inshape and has a large metaphyseal area.Because of the geometry of the proxi-mal tibia, the fit is not tight at themetaphyseal bone-nail interface. The
medullary center of the tibia is just lat-eral to the midline13 (Figure 7). Amore lateral starting portal is impor-tant because it helps prevent a valgusdeformity and provides a greater pro-pensity for the nail to be colinear withthe tibial axis.
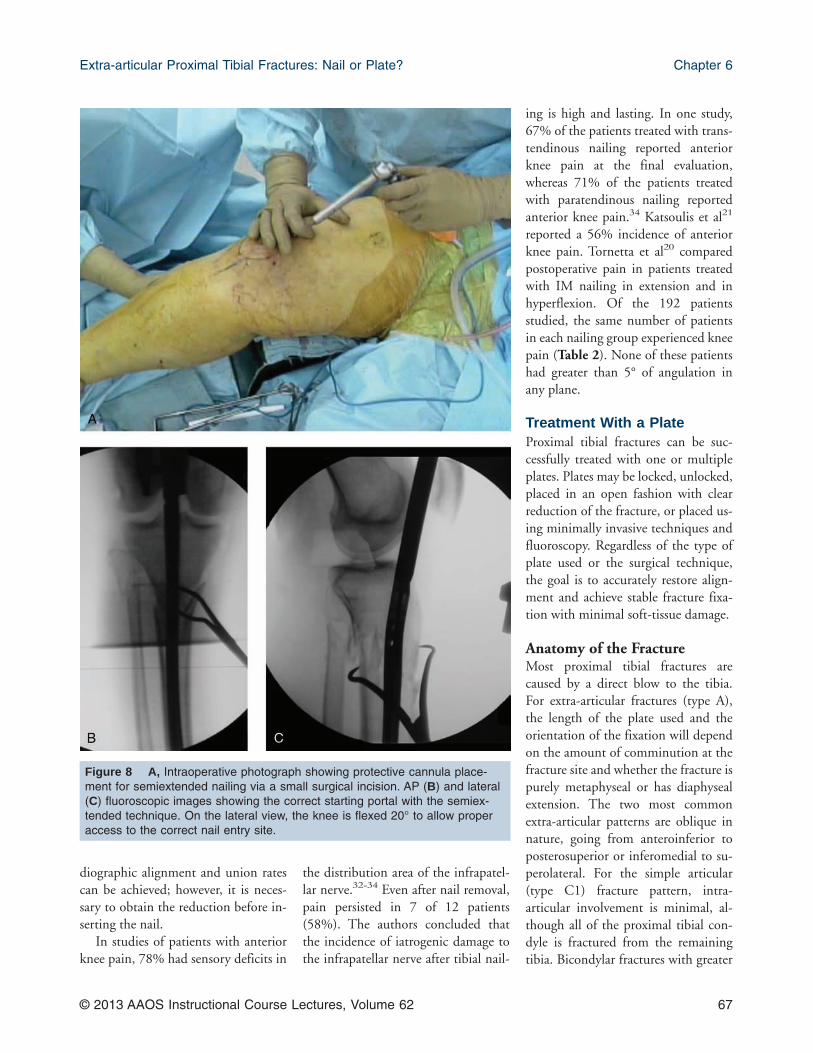
Nailing in Relative ExtensionIn the semiextended approach to IMnailing, the leg is positioned in approx-imately 20° to 30° of flexion with asmall bolster under the thigh.14 A mid-line skin incision approximately 5 cmlong is made from just above the upperpole of the patella. The deep incision ismade medial to the patella and extendsslightly into the vastus proximally anddown as low as the upper portion ofthe patella tendon distally. This allowsfor lateral subluxation of the patelladuring the procedure. The tibial por-tal, which is located on the superiorsurface of the tibia, is made accessibleusing the trochlear groove as a conduit.A straight awl may be used to start theportal (Figure 8).
It is essential that the direction ofthe awl or the starting guidewire andreamer be checked with fluoroscopy asthey are driven into the tibia. Theymust be directed as anteriorly as possi-ble in the proximal tibia. In a recentstudy, none of the 192 patients treatedwith this method had greater than 5°of apex anterior angulation.20 This ap-
Figure 4 Radiograph showing a10° extension deformity at theproximal tibial fracture site causedby hyperflexion nailing of the frac-ture. (Reproduced from Tornetta PIII: Technical considerations in thesurgical management of tibial frac-tures. Instr Course Lect 1997;46:271-280.)
Figure 5 AP (A) and lateral (B) views of the tibia showing the safe zone(red circle) for IM nailing of a proximal tibial fracture as described by Tornettaet al.18
Trauma
64 © 2013 AAOS Instructional Course Lectures, Volume 62
proach has the potential for decreasedpostoperative anterior knee pain be-cause the infrapatellar branch of the sa-phenous nerve and patellar tendon areavoided.21
A common criticism of the semiex-tended technique is the potential for
patella or trochlear groove injury dur-ing nailing. Since the original tech-nique was described, special instru-mentation has been developed toprotect the fragile articular surface ofthe patella and the trochlear grooveduring instrumentation and nailing of
the tibial canal. The current techniqueuses only a 3-cm incision and cannulasto protect the trochlea and undersur-face of the patella. A recent study re-ported that knee pain is the same inpatients treated with a semiextendedapproach as those treated with stan-dard hyperflexion nailing, despite ahigher percentage of fractures withintra-articular extension.20
Other methods for nailing proximaltibial fractures have recently been re-ported. These methods describe nail-ing in a fully or a partially extendedposition. The suprapatellar portal, a2-cm vertical incision in the quadri-ceps mechanism directly superior tothe patella, is used for nailing in fullextension.13 Although this techniqueis appealing, the starting portal in thetibia is more distal and anterior thanthe ideal starting portal, which is notaccessible until the knee is flexed30°.13,22
Proximal FixationTo increase the stability of a proximaltibial fracture treated with IM nailing,multiplanar proximal locking is of-fered by various nailing systems andincreases the stability of fixation.23,24
At least two proximal interlockingscrews in different planes are recom-mended for proximal tibial fractures;three or more screws offer greater sta-bility.23,24 The development of angu-lar, stable interlocking screws placedthrough an IM nail decreases fragmen-tary motion and increases the stiffnessof the construct.25 In most systems,some method is used to lock at leastthe most proximal screw to the nail us-ing an end cap. Different nailing sys-tems offer proximal locking screw lo-cations closer to or further from themost proximal portion of the nail.
Blocking ScrewsBlocking screws essentially tighten thecanal and force the nail to take a par-
Figure 6 Illustrations of the correct nail starting point for IM nailing fromAP (A) and lateral (B) views. Radiographs show the location of the correctstarting portal for IM nailing. C, AP radiograph of the guidewire placed justmedial to the lateral tibial spine. D, Lateral radiograph of the guidewire placedjust anterior to the joint line.
Extra-articular Proximal Tibial Fractures: Nail or Plate? Chapter 6
© 2013 AAOS Instructional Course Lectures, Volume 62 65

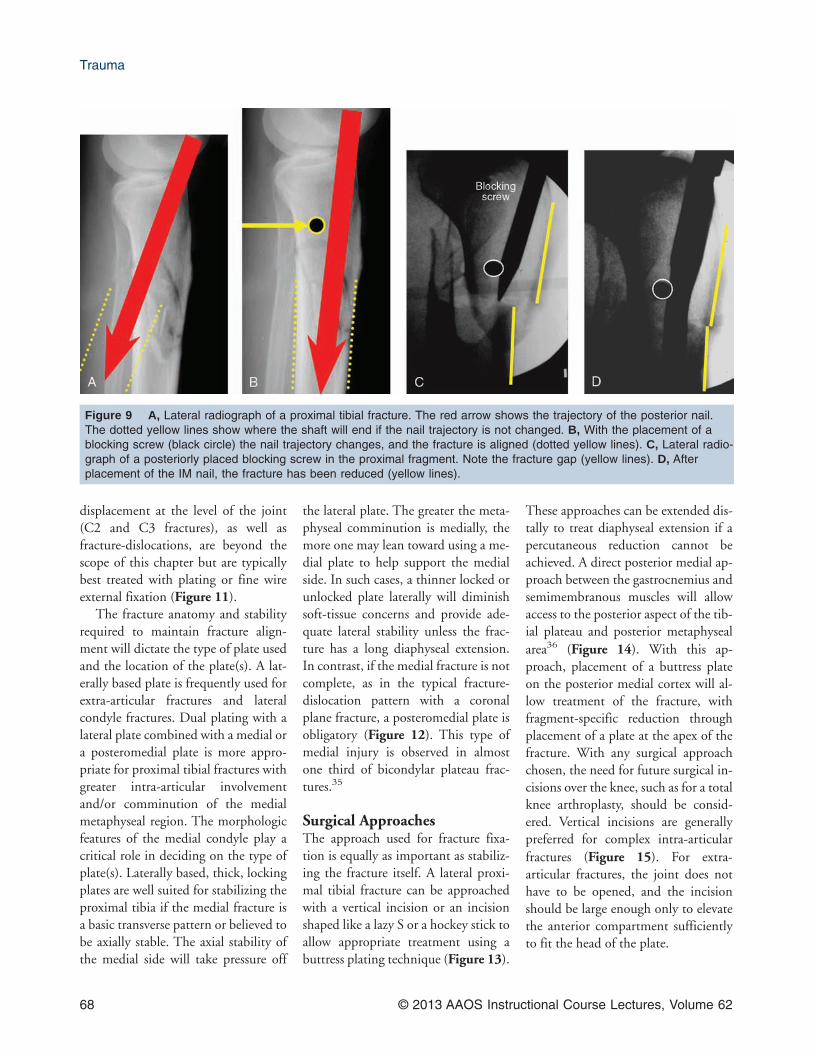
ticular path to avoid malalignment inthe sagittal and coronal planes. Thescrews are placed before nail insertionand reaming. Krettek et al15 andCole26 described their techniques forblocking screw placement to addressmalreduction. To prevent apex ante-rior angulation, a coronal blockingscrew can be placed in the posteriorhalf of the proximal fragment (Fig-ure 9). Valgus malalignment can be re-lated to a medial entry point and a lat-erally directed nailing insertion anglein the proximal fragment. To correctthis, a blocking screw can be placed onthe lateral side of the proximal frac-ture. If the portal is too medial, then itmust be widened, even when using alateral blocking screw. Both coronaland sagittal blocking screws can beused simultaneously to reduce multidi-
rectional forces. Krettek et al15 re-ported a mean loss of reduction be-tween placement of the initialblocking screw and follow-up as 0.5°in the frontal plane and 0.4° in the sag-ittal plane. No complications were re-lated to the use of blocking screws.When blocking screws are used appro-priately, reproducible results can be ex-pected for acceptable alignment, andthe biomechanical stability of thebone-implant construct is increased25%.12,27 If blocking screws are placedafter IM nailing to add stability to theconstruct, they are called stabilityscrews rather than blocking screws.12
Mini-Open Reduction andInternal FixationThe treatment of a proximal tibialfracture with an IM nail can be aided
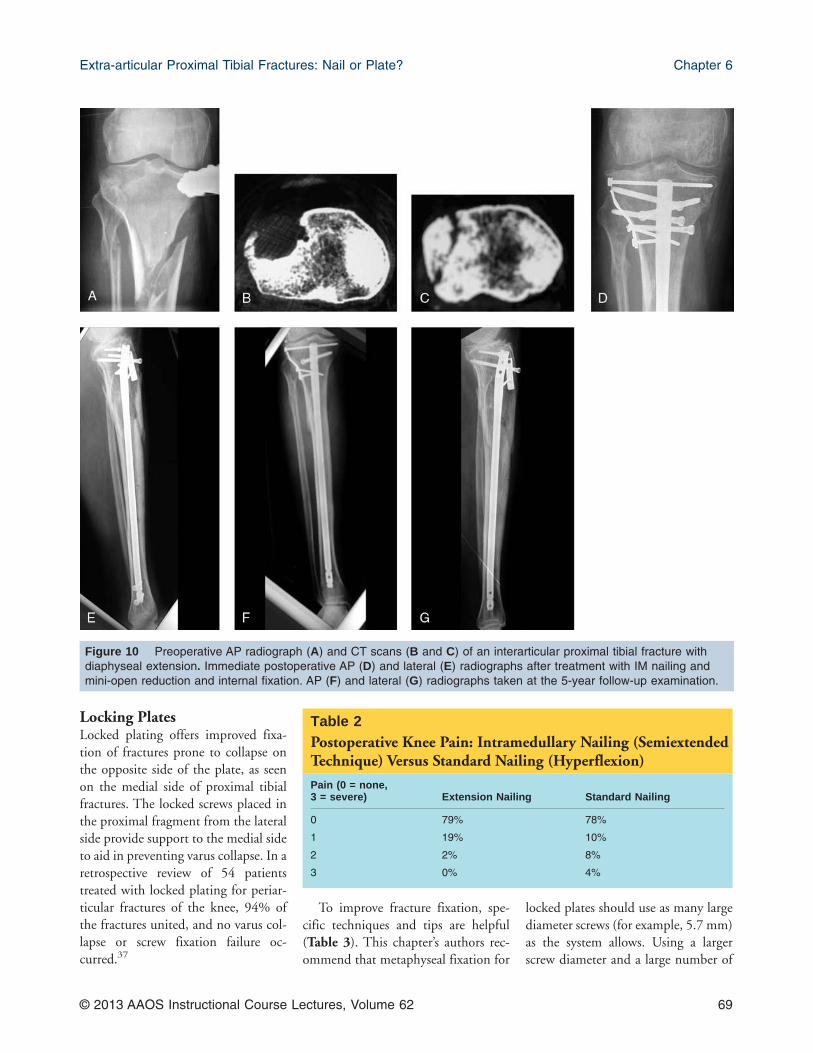
by using percutaneous clamps or smallplates, which can be placed to obtainand maintain the reduction before nailor lag screw placement. Percutaneousreduction clamps do not increase therate of infection.28 If clamp fixation isnot sufficient, unicortical plating is anoption.29,30 A small, four- or six-holeplate is placed over the fracture or frac-ture fragment and is held in place withat least two unicortical screws. Theplate can be placed percutaneously orvia a mini-open approach. If possible,the plate should lie anteriorly to avoidthe canal. Potential complicationsfrom this method include an addi-tional incision and dissection. How-ever, the plate may provide excellentstability for fracture reduction, and theunicortical screws can be replaced bybicortical screws after IM nailing toimprove overall stability17 (Figure 10).This technique is not needed for allproximal tibial fractures, but it offersanother method of providing stability.This is particularly helpful in open in-juries in which further soft-tissue dis-section is not necessary and can be det-rimental.
OutcomesMost complications seen with IM nail-ing of proximal tibial fractures involvemalreduction (greater than 5° in anyplane). The advent of the semiex-tended technique; angular, stable in-terlocking screws; and improved im-plant designs have resulted in averagemalreduction rates between 0% and8.2%.20,31 Nork et al17 evaluated456 patients with a tibial shaft frac-ture; 37 had a tibial fracture in theproximal quarter that was treated withIM nailing. Postoperative angulationwas less than 5° in any plane for 34 ofthe 37 fractures (92%). Two infectionswere reported in the 37 patientstreated with IM nailing, with both in-fections involving open fractures. Theauthors concluded that satisfactory ra-
Figure 7 A, Photograph of the proximal tibia. Sectioning demonstrates thewide metaphyseal region that narrows distally to a well-defined cortical tube.B, Enface view of the tibial sections arranged in order from proximal to distalshows the more lateral trajectory a nail will take within the medullary canal ofthe tibia. (Reproduced with permission from Buehler KC, Green J, Woll TS,Duwelius PJ: A technique for intramedullary nailing of proximal third tibia frac-tures. J Orthop Trauma 1997;11:218-223.)
Trauma
66 © 2013 AAOS Instructional Course Lectures, Volume 62
diographic alignment and union ratescan be achieved; however, it is neces-sary to obtain the reduction before in-serting the nail.
In studies of patients with anteriorknee pain, 78% had sensory deficits in
the distribution area of the infrapatel-lar nerve.32-34 Even after nail removal,pain persisted in 7 of 12 patients(58%). The authors concluded thatthe incidence of iatrogenic damage tothe infrapatellar nerve after tibial nail-
ing is high and lasting. In one study,67% of the patients treated with trans-tendinous nailing reported anteriorknee pain at the final evaluation,whereas 71% of the patients treatedwith paratendinous nailing reportedanterior knee pain.34 Katsoulis et al21
reported a 56% incidence of anteriorknee pain. Tornetta et al20 comparedpostoperative pain in patients treatedwith IM nailing in extension and inhyperflexion. Of the 192 patientsstudied, the same number of patientsin each nailing group experienced kneepain (Table 2). None of these patientshad greater than 5° of angulation inany plane.
Treatment With a PlateProximal tibial fractures can be suc-cessfully treated with one or multipleplates. Plates may be locked, unlocked,placed in an open fashion with clearreduction of the fracture, or placed us-ing minimally invasive techniques andfluoroscopy. Regardless of the type ofplate used or the surgical technique,the goal is to accurately restore align-ment and achieve stable fracture fixa-tion with minimal soft-tissue damage.
Anatomy of the FractureMost proximal tibial fractures arecaused by a direct blow to the tibia.For extra-articular fractures (type A),the length of the plate used and theorientation of the fixation will dependon the amount of comminution at thefracture site and whether the fracture ispurely metaphyseal or has diaphysealextension. The two most commonextra-articular patterns are oblique innature, going from anteroinferior toposterosuperior or inferomedial to su-perolateral. For the simple articular(type C1) fracture pattern, intra-articular involvement is minimal, al-though all of the proximal tibial con-dyle is fractured from the remainingtibia. Bicondylar fractures with greater
Figure 8 A, Intraoperative photograph showing protective cannula place-ment for semiextended nailing via a small surgical incision. AP (B) and lateral(C) fluoroscopic images showing the correct starting portal with the semiex-tended technique. On the lateral view, the knee is flexed 20° to allow properaccess to the correct nail entry site.
Extra-articular Proximal Tibial Fractures: Nail or Plate? Chapter 6
© 2013 AAOS Instructional Course Lectures, Volume 62 67
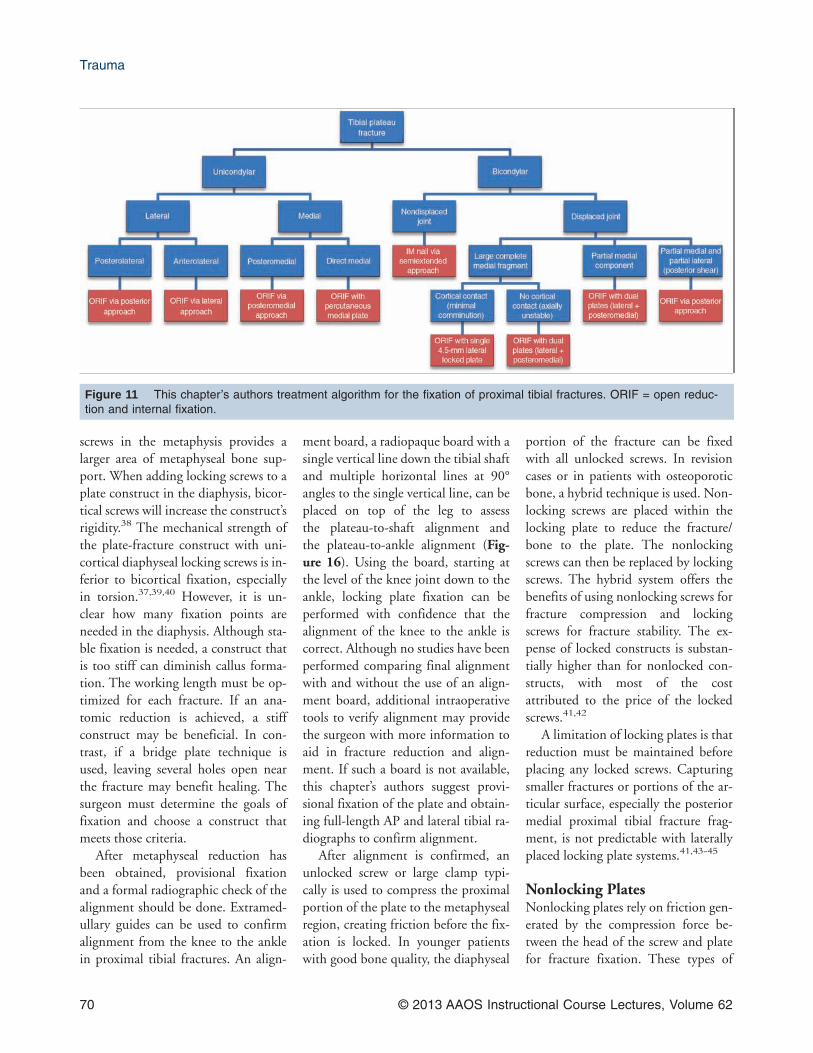
displacement at the level of the joint(C2 and C3 fractures), as well asfracture-dislocations, are beyond thescope of this chapter but are typicallybest treated with plating or fine wireexternal fixation (Figure 11).
The fracture anatomy and stabilityrequired to maintain fracture align-ment will dictate the type of plate usedand the location of the plate(s). A lat-erally based plate is frequently used forextra-articular fractures and lateralcondyle fractures. Dual plating with alateral plate combined with a medial ora posteromedial plate is more appro-priate for proximal tibial fractures withgreater intra-articular involvementand/or comminution of the medialmetaphyseal region. The morphologicfeatures of the medial condyle play acritical role in deciding on the type ofplate(s). Laterally based, thick, lockingplates are well suited for stabilizing theproximal tibia if the medial fracture isa basic transverse pattern or believed tobe axially stable. The axial stability ofthe medial side will take pressure off
the lateral plate. The greater the meta-physeal comminution is medially, themore one may lean toward using a me-dial plate to help support the medialside. In such cases, a thinner locked orunlocked plate laterally will diminishsoft-tissue concerns and provide ade-quate lateral stability unless the frac-ture has a long diaphyseal extension.In contrast, if the medial fracture is notcomplete, as in the typical fracture-dislocation pattern with a coronalplane fracture, a posteromedial plate isobligatory (Figure 12). This type ofmedial injury is observed in almostone third of bicondylar plateau frac-tures.35
Surgical ApproachesThe approach used for fracture fixa-tion is equally as important as stabiliz-ing the fracture itself. A lateral proxi-mal tibial fracture can be approachedwith a vertical incision or an incisionshaped like a lazy S or a hockey stick toallow appropriate treatment using abuttress plating technique (Figure 13).
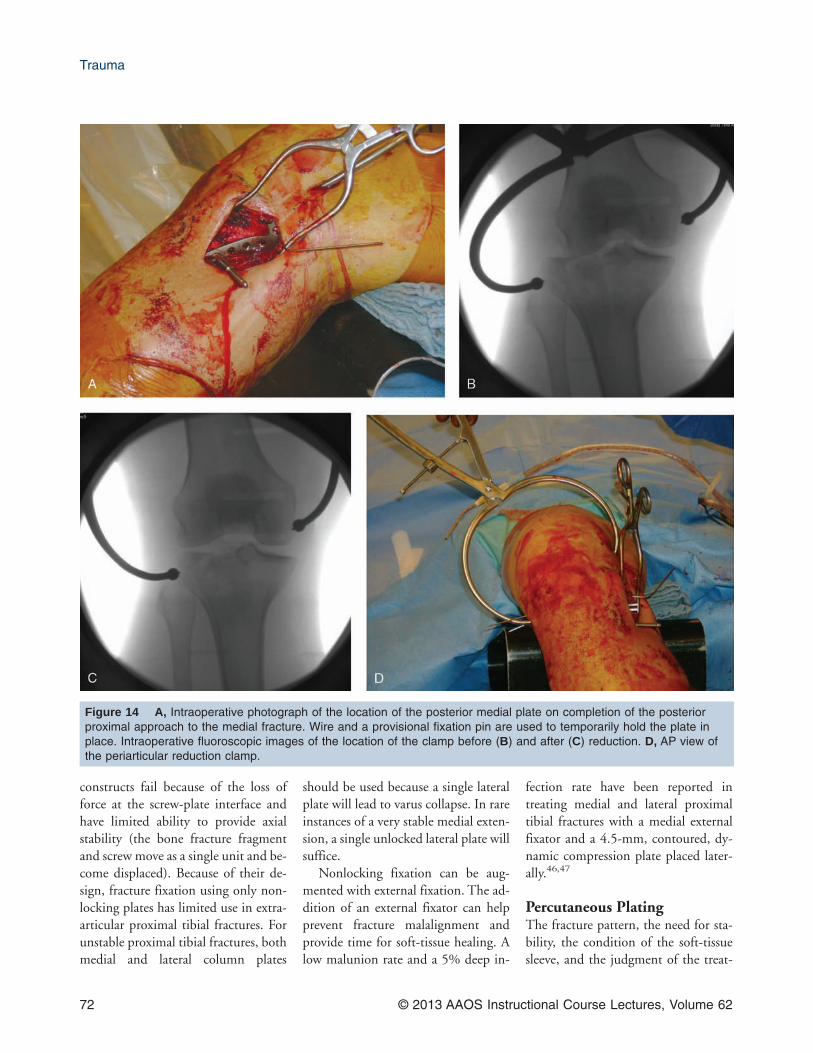
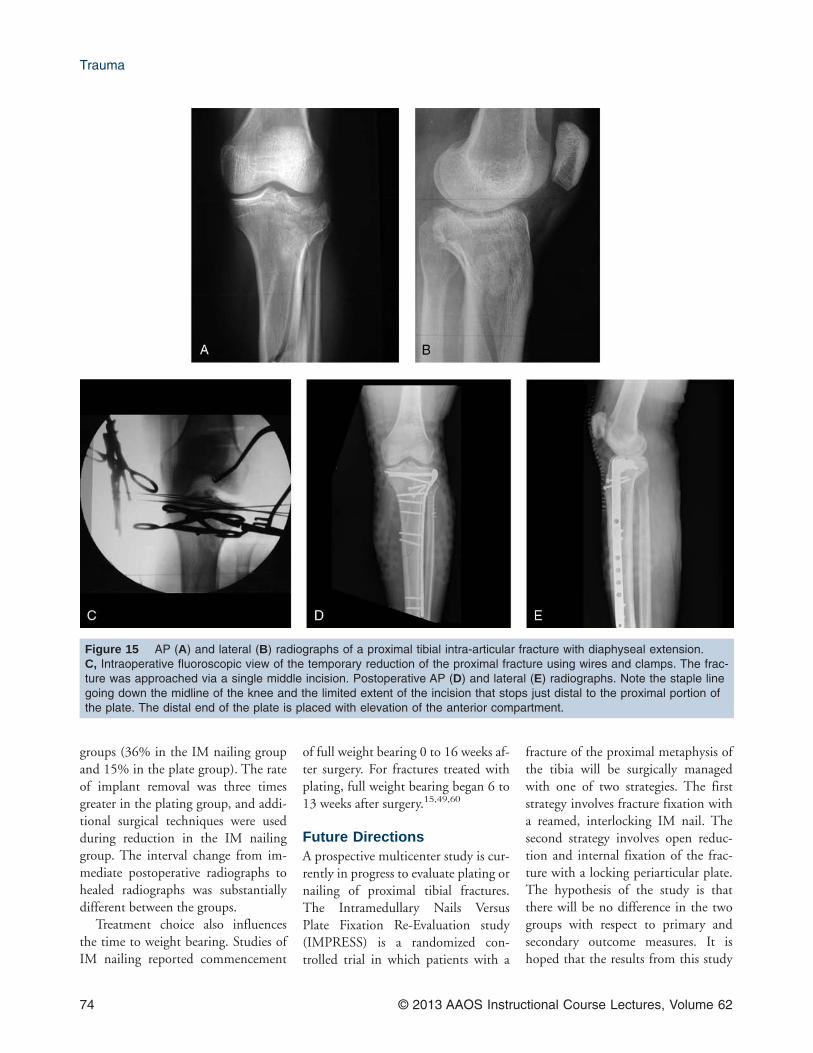
These approaches can be extended dis-tally to treat diaphyseal extension if apercutaneous reduction cannot beachieved. A direct posterior medial ap-proach between the gastrocnemius andsemimembranous muscles will allowaccess to the posterior aspect of the tib-ial plateau and posterior metaphysealarea36 (Figure 14). With this ap-proach, placement of a buttress plateon the posterior medial cortex will al-low treatment of the fracture, withfragment-specific reduction throughplacement of a plate at the apex of thefracture. With any surgical approachchosen, the need for future surgical in-cisions over the knee, such as for a totalknee arthroplasty, should be consid-ered. Vertical incisions are generallypreferred for complex intra-articularfractures (Figure 15). For extra-articular fractures, the joint does nothave to be opened, and the incisionshould be large enough only to elevatethe anterior compartment sufficientlyto fit the head of the plate.
Figure 9 A, Lateral radiograph of a proximal tibial fracture. The red arrow shows the trajectory of the posterior nail.The dotted yellow lines show where the shaft will end if the nail trajectory is not changed. B, With the placement of ablocking screw (black circle) the nail trajectory changes, and the fracture is aligned (dotted yellow lines). C, Lateral radio-graph of a posteriorly placed blocking screw in the proximal fragment. Note the fracture gap (yellow lines). D, Afterplacement of the IM nail, the fracture has been reduced (yellow lines).
Trauma
68 © 2013 AAOS Instructional Course Lectures, Volume 62
Locking PlatesLocked plating offers improved fixa-tion of fractures prone to collapse onthe opposite side of the plate, as seenon the medial side of proximal tibialfractures. The locked screws placed inthe proximal fragment from the lateralside provide support to the medial sideto aid in preventing varus collapse. In aretrospective review of 54 patientstreated with locked plating for periar-ticular fractures of the knee, 94% ofthe fractures united, and no varus col-lapse or screw fixation failure oc-curred.37
To improve fracture fixation, spe-cific techniques and tips are helpful(Table 3). This chapter’s authors rec-ommend that metaphyseal fixation for
locked plates should use as many largediameter screws (for example, 5.7 mm)as the system allows. Using a largerscrew diameter and a large number of
Figure 10 Preoperative AP radiograph (A) and CT scans (B and C) of an interarticular proximal tibial fracture withdiaphyseal extension. Immediate postoperative AP (D) and lateral (E) radiographs after treatment with IM nailing andmini-open reduction and internal fixation. AP (F) and lateral (G) radiographs taken at the 5-year follow-up examination.
Table 2Postoperative Knee Pain: Intramedullary Nailing (SemiextendedTechnique) Versus Standard Nailing (Hyperflexion)
Pain (0 = none,3 = severe) Extension Nailing Standard Nailing
0 79% 78%
1 19% 10%
2 2% 8%
3 0% 4%
Extra-articular Proximal Tibial Fractures: Nail or Plate? Chapter 6
© 2013 AAOS Instructional Course Lectures, Volume 62 69
screws in the metaphysis provides alarger area of metaphyseal bone sup-port. When adding locking screws to aplate construct in the diaphysis, bicor-tical screws will increase the construct’srigidity.38 The mechanical strength ofthe plate-fracture construct with uni-cortical diaphyseal locking screws is in-ferior to bicortical fixation, especiallyin torsion.37,39,40 However, it is un-clear how many fixation points areneeded in the diaphysis. Although sta-ble fixation is needed, a construct thatis too stiff can diminish callus forma-tion. The working length must be op-timized for each fracture. If an ana-tomic reduction is achieved, a stiffconstruct may be beneficial. In con-trast, if a bridge plate technique isused, leaving several holes open nearthe fracture may benefit healing. Thesurgeon must determine the goals offixation and choose a construct thatmeets those criteria.
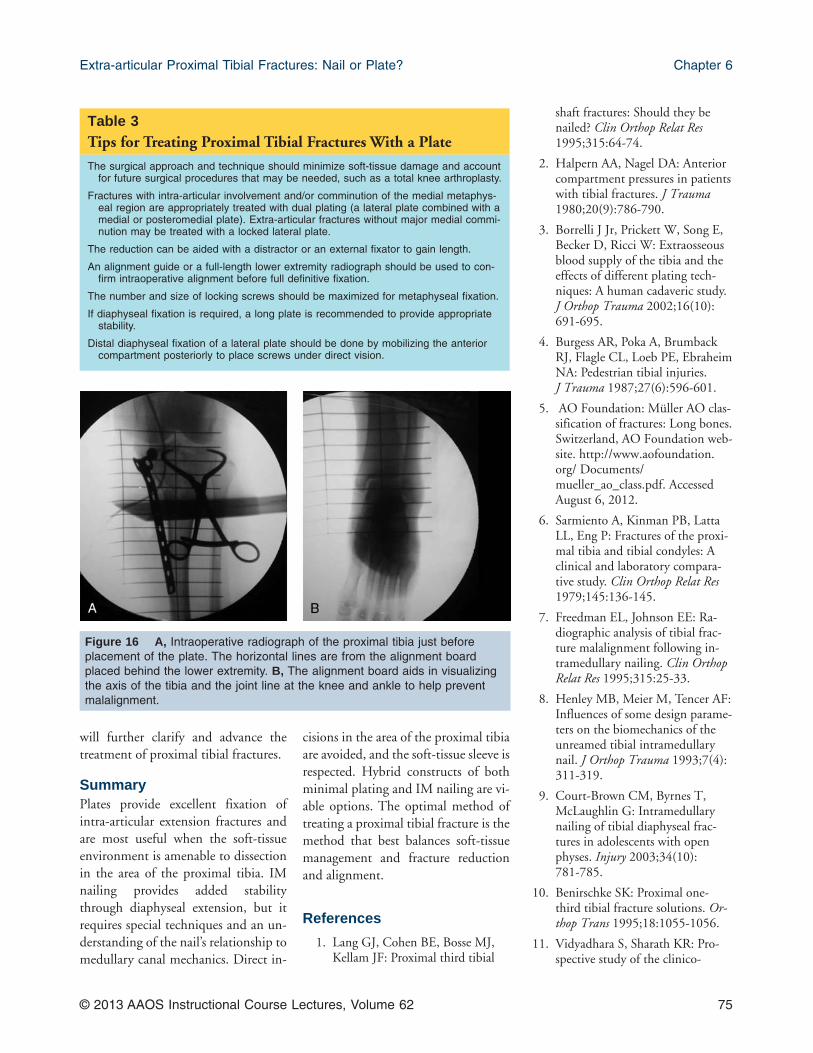
After metaphyseal reduction hasbeen obtained, provisional fixationand a formal radiographic check of thealignment should be done. Extramed-ullary guides can be used to confirmalignment from the knee to the anklein proximal tibial fractures. An align-
ment board, a radiopaque board with asingle vertical line down the tibial shaftand multiple horizontal lines at 90°angles to the single vertical line, can beplaced on top of the leg to assessthe plateau-to-shaft alignment andthe plateau-to-ankle alignment (Fig-ure 16). Using the board, starting atthe level of the knee joint down to theankle, locking plate fixation can beperformed with confidence that thealignment of the knee to the ankle iscorrect. Although no studies have beenperformed comparing final alignmentwith and without the use of an align-ment board, additional intraoperativetools to verify alignment may providethe surgeon with more information toaid in fracture reduction and align-ment. If such a board is not available,this chapter’s authors suggest provi-sional fixation of the plate and obtain-ing full-length AP and lateral tibial ra-diographs to confirm alignment.
After alignment is confirmed, anunlocked screw or large clamp typi-cally is used to compress the proximalportion of the plate to the metaphysealregion, creating friction before the fix-ation is locked. In younger patientswith good bone quality, the diaphyseal
portion of the fracture can be fixedwith all unlocked screws. In revisioncases or in patients with osteoporoticbone, a hybrid technique is used. Non-locking screws are placed within thelocking plate to reduce the fracture/bone to the plate. The nonlockingscrews can then be replaced by lockingscrews. The hybrid system offers thebenefits of using nonlocking screws forfracture compression and lockingscrews for fracture stability. The ex-pense of locked constructs is substan-tially higher than for nonlocked con-structs, with most of the costattributed to the price of the lockedscrews.41,42
A limitation of locking plates is thatreduction must be maintained beforeplacing any locked screws. Capturingsmaller fractures or portions of the ar-ticular surface, especially the posteriormedial proximal tibial fracture frag-ment, is not predictable with laterallyplaced locking plate systems.41,43-45
Nonlocking PlatesNonlocking plates rely on friction gen-erated by the compression force be-tween the head of the screw and platefor fracture fixation. These types of
Figure 11 This chapter’s authors treatment algorithm for the fixation of proximal tibial fractures. ORIF = open reduc-tion and internal fixation.
Trauma
70 © 2013 AAOS Instructional Course Lectures, Volume 62

Figure 12 Example of bicondylar tibial plateau fracture treated with dual plating. AP radiograph (A) and CT scans(B and C) of a bicondylar tibial plateau fracture treated initially with a spanning external fixator. AP (D) and lateral (E)postoperative radiographs after the fracture was treated with condylar plate fixation
Figure 13 Clinical photographs of the leg after healing of a proximal tibial fracture treated with a mini-open approach(A) and the lazy S approach (B).
Extra-articular Proximal Tibial Fractures: Nail or Plate? Chapter 6
© 2013 AAOS Instructional Course Lectures, Volume 62 71
constructs fail because of the loss offorce at the screw-plate interface andhave limited ability to provide axialstability (the bone fracture fragmentand screw move as a single unit and be-come displaced). Because of their de-sign, fracture fixation using only non-locking plates has limited use in extra-articular proximal tibial fractures. Forunstable proximal tibial fractures, bothmedial and lateral column plates
should be used because a single lateralplate will lead to varus collapse. In rareinstances of a very stable medial exten-sion, a single unlocked lateral plate willsuffice.
Nonlocking fixation can be aug-mented with external fixation. The ad-dition of an external fixator can helpprevent fracture malalignment andprovide time for soft-tissue healing. Alow malunion rate and a 5% deep in-
fection rate have been reported intreating medial and lateral proximaltibial fractures with a medial externalfixator and a 4.5-mm, contoured, dy-namic compression plate placed later-ally.46,47
Percutaneous PlatingThe fracture pattern, the need for sta-bility, the condition of the soft-tissuesleeve, and the judgment of the treat-
Figure 14 A, Intraoperative photograph of the location of the posterior medial plate on completion of the posteriorproximal approach to the medial fracture. Wire and a provisional fixation pin are used to temporarily hold the plate inplace. Intraoperative fluoroscopic images of the location of the clamp before (B) and after (C) reduction. D, AP view ofthe periarticular reduction clamp.
Trauma
72 © 2013 AAOS Instructional Course Lectures, Volume 62

ing surgeon regarding his or her abilityto reduce the fracture percutaneouslyshould be considered when choosingpercutaneous fixation versus an openapproach.48 Percutaneous placementand locked fixation are not synony-mous. Any plate may be placed withminimally invasive techniques. Thedecision to open the fracture is basedon the ability to reduce it closed orwith percutaneous clamps, externaldistractors, and plating as well as thedesired type of fixation (anatomic withcompression versus bridge plating).
The Less Invasive Stabilization Sys-tem (LISS; Synthes, Paoli, PA) was thefirst implant used in percutaneoustreatment of proximal tibial fractures.It is a precontoured lateral implantplaced in a submuscular manner. Thereported advantages of the LISS sys-tem, and percutaneous plating in gen-eral, are a smaller incision and lessmuscle dissection.49,50
Studies of percutaneous platinghave reported that malalignment oc-curs in 10% of patients, submuscularfixation of the tibia does not cause asubstantial rise in leg compartment
pressures, and the incidence of com-partment syndrome is not in-creased.50,51 Ricci et al52 confirmedthat percutaneous plating can be usedto successfully treat complex proximaltibial fractures without the need foradditional medial stabilization. How-ever, because the plate is placed with-out direct surgical visualization of itsentire length, the superficial peronealnerve is at substantial risk for injuryduring lateral percutaneous screwplacement.53 When the plate is in theregion of the neurovascular structures,a small 1- to 2-cm incision should bemade, and the anterior compartmentshould be retracted posteriorly to ex-pose the plate for safe screw place-ment.
ComplicationsInfection, malunion, nonunion, andpainful hardware necessitating removalare possible complications of plating.Postoperative infection rates rangefrom 1.6% with lateral fixation only to8.4% with dual plating.54 The infec-tion rate for percutaneous platingranges from 0% to 6%.51,53-57 Even
with open visualization and reductionof a proximal tibial fracture, malreduc-tion can occur. The rate of initial lossof fracture reduction using percutane-ous plating ranges from 0% to4%.51,53-57 Phisitkul et al58 reportedon 37 proximal tibial fractures treatedwith plate fixation. Complications in-cluded eight deep wound infections(22%), eight fracture malalignments(22%), and three fractures with loss ofreduction (8%). Fractures treated ini-tially with an external fixator followedby plating had a 5% deep wound in-fection rate and 4% nonunion rate.56
Cole et al49 reported a 5% incidence ofhardware removal after plate fixation.
OutcomesLindvall et al59 reported on 29 patientswith proximal tibial fractures treatedwith IM nailing and 42 treated withplating. There was no statistical differ-ence in the final union rate after anyadditional procedures, with 96%union in the IM nailing group and97% in the plate group. Apex anteriormalreduction was the most prevent-able form of malreduction in both
Figure 14 (continued) E, Lateral view of the periarticular reduction clamp. F, Lateral radiograph showing the finallocation of the plate on the posterior medial aspect of the tibia.
Extra-articular Proximal Tibial Fractures: Nail or Plate? Chapter 6
© 2013 AAOS Instructional Course Lectures, Volume 62 73
groups (36% in the IM nailing groupand 15% in the plate group). The rateof implant removal was three timesgreater in the plating group, and addi-tional surgical techniques were usedduring reduction in the IM nailinggroup. The interval change from im-mediate postoperative radiographs tohealed radiographs was substantiallydifferent between the groups.
Treatment choice also influencesthe time to weight bearing. Studies ofIM nailing reported commencement
of full weight bearing 0 to 16 weeks af-ter surgery. For fractures treated withplating, full weight bearing began 6 to13 weeks after surgery.15,49,60
Future DirectionsA prospective multicenter study is cur-rently in progress to evaluate plating ornailing of proximal tibial fractures.The Intramedullary Nails VersusPlate Fixation Re-Evaluation study(IMPRESS) is a randomized con-trolled trial in which patients with a
fracture of the proximal metaphysis ofthe tibia will be surgically managedwith one of two strategies. The firststrategy involves fracture fixation witha reamed, interlocking IM nail. Thesecond strategy involves open reduc-tion and internal fixation of the frac-ture with a locking periarticular plate.The hypothesis of the study is thatthere will be no difference in the twogroups with respect to primary andsecondary outcome measures. It ishoped that the results from this study
Figure 15 AP (A) and lateral (B) radiographs of a proximal tibial intra-articular fracture with diaphyseal extension.C, Intraoperative fluoroscopic view of the temporary reduction of the proximal fracture using wires and clamps. The frac-ture was approached via a single middle incision. Postoperative AP (D) and lateral (E) radiographs. Note the staple linegoing down the midline of the knee and the limited extent of the incision that stops just distal to the proximal portion ofthe plate. The distal end of the plate is placed with elevation of the anterior compartment.
Trauma
74 © 2013 AAOS Instructional Course Lectures, Volume 62
will further clarify and advance thetreatment of proximal tibial fractures.
SummaryPlates provide excellent fixation ofintra-articular extension fractures andare most useful when the soft-tissueenvironment is amenable to dissectionin the area of the proximal tibia. IMnailing provides added stabilitythrough diaphyseal extension, but itrequires special techniques and an un-derstanding of the nail’s relationship tomedullary canal mechanics. Direct in-
cisions in the area of the proximal tibiaare avoided, and the soft-tissue sleeve isrespected. Hybrid constructs of bothminimal plating and IM nailing are vi-able options. The optimal method oftreating a proximal tibial fracture is themethod that best balances soft-tissuemanagement and fracture reductionand alignment.
References
1. Lang GJ, Cohen BE, Bosse MJ,Kellam JF: Proximal third tibial
shaft fractures: Should they benailed? Clin Orthop Relat Res1995;315:64-74.
2. Halpern AA, Nagel DA: Anteriorcompartment pressures in patientswith tibial fractures. J Trauma1980;20(9):786-790.
3. Borrelli J Jr, Prickett W, Song E,Becker D, Ricci W: Extraosseousblood supply of the tibia and theeffects of different plating tech-niques: A human cadaveric study.J Orthop Trauma 2002;16(10):691-695.
4. Burgess AR, Poka A, BrumbackRJ, Flagle CL, Loeb PE, EbraheimNA: Pedestrian tibial injuries.J Trauma 1987;27(6):596-601.
5. AO Foundation: Müller AO clas-sification of fractures: Long bones.Switzerland, AO Foundation web-site. http://www.aofoundation.org/ Documents/mueller_ao_class.pdf. AccessedAugust 6, 2012.
6. Sarmiento A, Kinman PB, LattaLL, Eng P: Fractures of the proxi-mal tibia and tibial condyles: Aclinical and laboratory compara-tive study. Clin Orthop Relat Res1979;145:136-145.
7. Freedman EL, Johnson EE: Ra-diographic analysis of tibial frac-ture malalignment following in-tramedullary nailing. Clin OrthopRelat Res 1995;315:25-33.
8. Henley MB, Meier M, Tencer AF:Influences of some design parame-ters on the biomechanics of theunreamed tibial intramedullarynail. J Orthop Trauma 1993;7(4):311-319.
9. Court-Brown CM, Byrnes T,McLaughlin G: Intramedullarynailing of tibial diaphyseal frac-tures in adolescents with openphyses. Injury 2003;34(10):781-785.
10. Benirschke SK: Proximal one-third tibial fracture solutions. Or-thop Trans 1995;18:1055-1056.
11. Vidyadhara S, Sharath KR: Pro-spective study of the clinico-
Table 3Tips for Treating Proximal Tibial Fractures With a Plate
The surgical approach and technique should minimize soft-tissue damage and accountfor future surgical procedures that may be needed, such as a total knee arthroplasty.
Fractures with intra-articular involvement and/or comminution of the medial metaphys-eal region are appropriately treated with dual plating (a lateral plate combined with amedial or posteromedial plate). Extra-articular fractures without major medial commi-nution may be treated with a locked lateral plate.
The reduction can be aided with a distractor or an external fixator to gain length.
An alignment guide or a full-length lower extremity radiograph should be used to con-firm intraoperative alignment before full definitive fixation.
The number and size of locking screws should be maximized for metaphyseal fixation.
If diaphyseal fixation is required, a long plate is recommended to provide appropriatestability.
Distal diaphyseal fixation of a lateral plate should be done by mobilizing the anteriorcompartment posteriorly to place screws under direct vision.
Figure 16 A, Intraoperative radiograph of the proximal tibia just beforeplacement of the plate. The horizontal lines are from the alignment boardplaced behind the lower extremity. B, The alignment board aids in visualizingthe axis of the tibia and the joint line at the knee and ankle to help preventmalalignment.
Extra-articular Proximal Tibial Fractures: Nail or Plate? Chapter 6
© 2013 AAOS Instructional Course Lectures, Volume 62 75
radiological outcome of inter-locked nailing in proximal thirdtibial shaft fractures. Injury 2006;37(6):536-542.
12. Ricci WM, O’Boyle M, Borrelli J,Bellabarba C, Sanders R: Fracturesof the proximal third of the tibialshaft treated with intramedullarynails and blocking screws. J Or-thop Trauma 2001;15(4):264-270.
13. Buehler KC, Green J, Woll TS,Duwelius PJ: A technique for in-tramedullary nailing of proximalthird tibia fractures. J OrthopTrauma 1997;11(3):218-223.
14. Tornetta P III, Collins E: Semiex-tended position of intramedullarynailing of the proximal tibia. ClinOrthop Relat Res 1996;328:185-189.
15. Krettek C, Stephan C, Schandel-maier P, Richter M, Pape HC,Miclau T: The use of Poller screwsas blocking screws in stabilisingtibial fractures treated with smalldiameter intramedullary nails.J Bone Joint Surg Br 1999;81(6):963-968.
16. Wysocki RW, Kapotas JS, VirkusWW: Intramedullary nailing ofproximal and distal one-thirdtibial shaft fractures with intraop-erative two-pin external fixation.J Trauma 2009;66(4):1135-1139.
17. Nork SE, Barei DP, SchildhauerTA, et al: Intramedullary nailingof proximal quarter tibial frac-tures. J Orthop Trauma 2006;20(8):523-528.
18. Tornetta P III, Riina J, Geller J,Purban W: Intraarticular ana-tomic risks of tibial nailing. J Or-thop Trauma 1999;13(4):247-251.
19. McConnell T, Tornetta P III,Tilzey J, Casey D: Tibial portalplacement: The radiographic cor-relate of the anatomic safe zone.J Orthop Trauma 2001;15(3):207-209.
20. Tornetta P III, Steen B, Ryan S:Tibial metaphyseal fractures:
Nailing in extension. OrthopaedicTrauma Association 2008 AnnualMeeting. Scientific Program Pa-pers: Session 2: Tibia/Polytrauma.http://www.hwbf.org/ota/am/ota08/otapa/OTA080207.htm.Accessed August 6, 2012.
21. Katsoulis E, Court-Brown C, Gi-annoudis PV: Incidence and aeti-ology of anterior knee pain afterintramedullary nailing of the fe-mur and tibia. J Bone Joint SurgBr 2006;88(5):576-580.
22. Eastman J, Tseng S, Lo E, Li CS,Yoo B, Lee M: Retropatellar tech-nique for intramedullary nailingof proximal tibia fractures: A ca-daveric assessment. J OrthopTrauma 2010;24(11):672-676.
23. Hansen M, Blum J, Mehler D,Hessmann MH, Rommens PM:Double or triple interlockingwhen nailing proximal tibial frac-tures? A biomechanical investiga-tion. Arch Orthop Trauma Surg2009;129(12):1715-1719.
24. Sayana MK, Davis BJ, Kapoor B,Rahmatalla A, Maffulli N: Frac-ture strain and stability with addi-tional locking screws in intramed-ullary nailing: A biomechanicalstudy. J Trauma 2006;60(5):1053-1057.
25. Horn J, Linke B, Höntzsch D,Gueorguiev B, Schwieger K: An-gle stable interlocking screws im-prove construct stability of in-tramedullary nailing of distal tibiafractures: A biomechanical study.Injury 2009;40(7):767-771.
26. Cole D: Intramedullary fixationof proximal tibia fractures. TechOrthop 1998;13(1).
27. Krettek C, Miclau T, Schandel-maier P, Stephan C, MöhlmannU, Tscherne H: The mechanicaleffect of blocking screws (“Pollerscrews”) in stabilizing tibia frac-tures with short proximal or distalfragments after insertion of small-diameter intramedullary nails.J Orthop Trauma 1999;13(8):550-553.
28. Tang P, Gates C, Hawes J, VogtM, Prayson MJ: Does open reduc-tion increase the chance of infec-tion during intramedullary nailingof closed tibial shaft fractures?J Orthop Trauma 2006;20(5):317-322.
29. Matthews DE, McGuire R, Free-land AE: Anterior unicortical but-tress plating in conjunction withan unreamed interlocking in-tramedullary nail for treatment ofvery proximal tibial diaphysealfractures. Orthopedics 1997;20(7):647-648.
30. Kim KC, Lee JK, Hwang DS,Yang JY, Kim YM: Provisionalunicortical plating with reamedintramedullary nailing in segmen-tal tibial fractures involving thehigh proximal metaphysis. Ortho-pedics 2007;30(3):189-192.
31. Hiesterman TG, Shafiq BX, ColePA: Intramedullary nailing ofextra-articular proximal tibia frac-tures. J Am Acad Orthop Surg2011;19(11):690-700.
32. Leliveld MS, Verhofstad MH:Injury to the infrapatellar branchof the saphenous nerve: A possiblecause for anterior knee pain aftertibial nailing? Injury 2012;43(6):779-783.
33. Keating JF, Orfaly R, O’Brien PJ:Knee pain after tibial nailing.J Orthop Trauma 1997;11(1):10-13.
34. Toivanen JA, Väistö O, Kannus P,Latvala K, Honkonen SE,Järvinen MJ: Anterior knee painafter intramedullary nailing offractures of the tibial shaft: A pro-spective, randomized study com-paring two different nail-insertiontechniques. J Bone Joint Surg Am2002;84(4):580-585.
35. Barei DP, O’Mara TJ, TaitsmanLA, Dunbar RP, Nork SE: Fre-quency and fracture morphologyof the posteromedial fragment inbicondylar tibial plateau fracturepatterns. J Orthop Trauma 2008;22(3):176-182.
Trauma
76 © 2013 AAOS Instructional Course Lectures, Volume 62
36. Medvecky MJ, Noyes FR: Surgicalapproaches to the posteromedialand posterolateral aspects of theknee. J Am Acad Orthop Surg2005;13(2):121-128.
37. Haidukewych G, Sems SA, Hueb-ner D, Horwitz D, Levy B: Re-sults of polyaxial locked-platefixation of periarticular fracturesof the knee. J Bone Joint Surg Am2007;89(3):614-620.
38. Dougherty PJ, Kim DG, Meister-ling S, Wybo C, Yeni Y: Biome-chanical comparison of bicorticalversus unicortical screw placementof proximal tibia locking plates: Acadaveric model. J Orthop Trauma2008;22(6):399-403.
39. Kregor PJ, Stannard J, ZlowodzkiM, Cole PA, Alonso J: Distal fem-oral fracture fixation utilizing theLess Invasive Stabilization System(L.I.S.S.): The technique and earlyresults. Injury 2001;32(suppl 3):SC32-SC47.
40. Egol KA, Kubiak EN, FulkersonE, Kummer FJ, Koval KJ: Biome-chanics of locked plates andscrews. J Orthop Trauma 2004;18(8):488-493.
41. Haidukewych GJ: Innovations inlocking plate technology. J AmAcad Orthop Surg 2004;12(4):205-212.
42. Gardner MJ, Helfet DL, LorichDG: Has locked plating com-pletely replaced conventional plat-ing? Am J Orthop (Belle Mead NJ)2004;33(9):439-446.
43. Althausen PL, Lee MA, Finke-meier CG, Meehan JP, RodrigoJJ: Operative stabilization of su-pracondylar femur fractures abovetotal knee arthroplasty: A compar-ison of four treatment methods.J Arthroplasty 2003;18(7):834-839.
44. Fulkerson E, Koval K, PrestonCF, Iesaka K, Kummer FJ, EgolKA: Fixation of periprostheticfemoral shaft fractures associated
with cemented femoral stems: Abiomechanical comparison oflocked plating and conventionalcable plates. J Orthop Trauma2006;20(2):89-93.
45. Raab GE, Davis CM III: Earlyhealing with locked condylar plat-ing of periprosthetic fracturesaround the knee. J Arthroplasty2005;20(8):984-989.
46. Bolhofner BR: Indirect reductionand compositie fixation of extraar-ticular proximal tibia fractures.Clin Orthop Relat Res 1995;315:75-83.
47. Gerber A, Ganz R: Combinedinternal and external osteosynthe-sis: A biological approach to thetreatment of complex fractures ofthe proximal tibia. Injury 1998;29(suppl):C22-C28.
48. Lowe JA, Tejwani N, Yoo BJ, Wo-linsky PR: Surgical techniques forcomplex proximal tibial fractures.Instr Course Lect 2012;61:39-51.
49. Cole PA, Zlowodzki M, KregorPJ: Treatment of proximal tibiafractures using the less invasivestabilization system: Surgical expe-rience and early clinical results in77 fractures. J Orthop Trauma2004;18(8):528-535.
50. Cole PA, Zlowodzki M, KregorPJ: Compartment pressures aftersubmuscular fixation of proximaltibia fractures. Injury 2003;34(suppl 1):A43-A46.
51. Boldin C, Fankhauser F, HoferHP, Szyszkowitz R: Three-yearresults of proximal tibia fracturestreated with the LISS. Clin OrthopRelat Res 2006;445:222-229.
52. Ricci WM, Rudzki JR, Borrelli JJr: Treatment of complex proxi-mal tibia fractures with the lessinvasive skeletal stabilization sys-tem. J Orthop Trauma 2004;18(8):521-527.
53. Deangelis JP, Deangelis NA, An-derson R: Anatomy of the superfi-cial peroneal nerve in relation to
fixation of tibia fractures with theless invasive stabilization system.J Orthop Trauma 2004;18(8):536-539.
54. Higgins TF, Klatt J, Bachus KN:Biomechanical analysis of bicon-dylar tibial plateau fixation: Howdoes lateral locking plate fixationcompare to dual plate fixation?J Orthop Trauma 2007;21(5):301-306.
55. Stannard JP, Wilson TC, VolgasDA, Alonso JE: Fracture stabiliza-tion of proximal tibial fractureswith the proximal tibial LISS:Early experience in Birmingham,Alabama (USA). Injury 2003;34(suppl 1):A36-A42.
56. Egol KA, Tejwani NC, Capla EL,Wolinsky PL, Koval KJ: Stagedmanagement of high-energy prox-imal tibia fractures (OTA types41): The results of a prospective,standardized protocol. J OrthopTrauma 2005;19(7):448-456.
57. Schütz M, Kääb MJ, Haas N:Stabilization of proximal tibialfractures with the LIS-System:Early clinical experience in Berlin.Injury 2003;34(suppl 1):A30-A35.
58. Phisitkul P, McKinley TO,Nepola JV, Marsh JL: Complica-tions of locking plate fixation incomplex proximal tibia injuries.J Orthop Trauma 2007;21(2):83-91.
59. Lindvall E, Sanders R, DipasqualeT, Herscovici D, HaidukewychG, Sagi C: Intramedullary nailingversus percutaneous locked plat-ing of extra-articular proximaltibial fractures: Comparison of 56cases. J Orthop Trauma 2009;23(7):485-492.
60. Gustilo RB, Simpson L, Nixon R,Ruiz A, Indeck W: Analysis of511 open fractures. Clin OrthopRelat Res 1969;66:148-154.
Extra-articular Proximal Tibial Fractures: Nail or Plate? Chapter 6
© 2013 AAOS Instructional Course Lectures, Volume 62 77