Embed Size (px)
Citation preview

“Controversies in Hematology: Case-Based Discussion”
Catastrophic antiphospholipid syndrome
Pichika Chantrathammachart MD Division of Hematology, Department of Medicine
Ramathibodi Hospital

Introduction • Clinical syndrome
– Rapid onset of multifocal thrombosis associated with multi-organ failure
– Serological criteria for APS
• Rare – Prevalence of less than 1 in 2000 (app. 600
reported cases) – Mortality estimated at 50%.
• <1% of patients with the APS

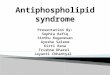
David Garcia, and Doruk Erkan, n engl j med 378;21 nejm.org May 24, 2018
Summary of the Proposed Pathogenesis of Antiphospholipid-Antibody–Mediated Clinical Problems.

Catastrophic antiphospholipid syndrome (CAPS) spectrum
• Definite or probable APS • CAPS-like disease • Microangiopathic APS • Thrombotic storm

Presentations
CAPS : thrombotic microangiopathic condition, characterized by a diffuse thrombotic microvasculopathy (a) Clinical evidence of multiple organ involvement
developing over a very short period of time
(b) Histopathological evidence of multiple small-vessel occlusions
(c) Laboratory confirmation of antiphospholipid (aPL) antibodies, usually in high titer

Preliminary Criteria for Classification of CAPS
1. Evidence of involvement of > 3 organs, systems and/or tissues 2. Development of manifestations simultaneously or in < 1 week 3. Confirmation by histopathology of small vessel occlusion in at least one organ or tissue 4. Laboratory confirmation of the presence of antiphospholipid antibodies (lupus anticoagulant and/or anticardiolipin antibodies)
Definite catastrophic APS : all 4 criteria Probable catastrophic APS : - All 4 criteria, except for only 2 organs, systems and/or tissues involved - All four criteria, except for the absence of laboratory confirmation at least 6 weeks apart - 1, 2 and 4 - 1, 3 and 4 and the development of a third event in more than a week but less than a month, despite anticoagulation
Asherson et al. 2003

Case 1 ชายไทยค 69 ป
CC : ปลายมอ-เทา เยน ปวด เปลยนส 1 วน
PI : 2 wk PTA ขาบวม ปสสาวะลดลง เหนอยงายขน
5 days PTA ปวดทอง ปวดบดๆตลอดทงวน ถายเหลว วนละ 1-2 ครง เหนอยมากขน อาการเปนมากขนเรอยๆ
1 day PTA ปวดเทามาก เทาเยนและสคลาขน จงมาโรงพยาบาล
PH : - CAD S/P CAG (2007)
- Smoking 50 pack-year

Physical examinations V/S T 36.8 C, BP 105/48 mmHg, PR 91 BPM, RR 20 /min RS : fine crepitation BLL, decreased BS RLL

Investigations
CBC Hb/Hct 8/25.1 WBC 6700 N86 L4 M9 Plt 174,000 Coag PTT 30.1 sec (22-33) PT 17.6 sec (10.5-13.5) TT 10.6 sec (10-13) D-dimer 21530 BUN/CR 120/7.71 K 5.7 UA prot 3+, blood marked+ WBC 0-1, RBC 0

Investigations & management - I
• Anti-GBM , • p-ANCA , c-ANCA • ANA homogeneous > 1:1280 nucleolar > 1:1280 • Antithrombin 45% • Protein S 63% • Protein C 43% • Cryoglobulin
DDx • RPGN vs RPGN mimics • Raynuad’s phenomenon
Treatment • Dexamethasone 5 mg IV q 6 hr • Nifedipine • Hemodialysis


MDCT Angiography of Aorta and Peripheral Run Off
- Severe stenosis at bilateral ATA, proximal right peroneal artery and proximal right PTA.

Investigations & management - II
• Pleural fluid ANA
homogeneous > 1:1280
nucleolar > 1:1280
speckle > 1:1280
• B2-GPI Ab 4 (0-20)
• aCL 24.0
(neg <12)
• Lupus anticoagulant
• Anti-Scl-70 3
DDx • SLE with CAPS * (SNAPS) • Scleroderma renal crisis • Other TMAs • Cancer-associated thrombosis
Treatment • Dexamethasone 5 mg IV q 6 hr • Enoxaparin 0.4 ml SC OD • ASA (81) 1x1
Planned renal biopsy >> cancelled

Thrombotic microangipathy (TMA)
STEC-HUS and STEC-
like aHUS
(associated with complement
Secondary TMA
TTP
Shiga toxin-producing E. coli - Strain O157:H7 and other strains - Shigella disenteriae type I - Streptococcus pneumoniae (neuraminidase)
Complement abnormalities - Mutations in FH, MCP, FI, THBD, FB and C3 - Polymorphism risk in FH and MCP - Anti-FH antibodies
TTP (ADAMTS13 acitvity <5-10%) - Genetic cause - Antibodies

Causes of secondary TMA
Pregnancy • Pre-eclampsia, eclampsia • HELLP syndrome • Postpartum TMA Systemic disease • SLE • Scleroderma • Vasculitis • APS/CAPS
Glomerulonephritis • C3 glomerulopathies • Glomerulopathies ass with
MGUS • IgA nephropathy Malignant arterial hypertension Infections • HIV, HCV, H1N1, others Neoplasms

Differential diagnosis of catastrophic APS
History & condition CAPS TTP-HUS HELLP
syndrome Sepsis DIC HIT SRC
History APS/SLE/malignancy/pregnancy
None Pregnancy Infection Infection Heparin exposure
Scleroderma
Thrombosis
Small/large vessels
Small vessels
Small vessels
Large/small vessels
Small vessels
Large/small vessels
Small vessels
Hemolysis -/+ ++ + -/+ -/+ - +
Schistocytes -/+ ++ -/+ -/+ -/+ - +
Fibrinogen Normal/high
Normal/high
Normal/high
Normal/low
Normal/low
Normal/high
Normal/high
Typical Abs aPL ADAMTS
13 None None None Anti-PF4 None
EXPERT REVIEW OF HEMATOLOGY, 2017, VOL. 10, NO. 4, 365–374

Clinical manifestations
• Thrombosis-related manifestations
– Intra-abdominal thrombotic complications
: kidneys, adrenal glands, splenic, intestinal, and mesenteric or pancreatic vasculature
• SIRS-related manifestations
– ARDS : cytokine storm
Severity of thrombosis Organ dysfunction

Clinical manifestations
CAPS: Descriptive analysis of 500 patients from the International CAPS Registry I. Rodríguez-Pinto et al. Autoimmunity Reviews 15 (2016) 1120–1124

Lab and serology features
CAPS: Descriptive analysis of 500 patients from the International CAPS Registry I. Rodríguez-Pinto et al. Autoimmunity Reviews 15 (2016) 1120–1124

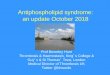
Triggers
• Infection : common • Anticoagulant withdraw, subtherpeutic INR • Other medications : OCPs • Obstetric complications • Malignancy • SLE flares • Others : trauma, surgery ~ 1/3 of cases - no obvious precipitating factors

Demographic characteristics and precipitating factors of patients with CAPS
(CAPS registry; 1992-2014)
CAPS: Descriptive analysis of 500 patients from the International CAPS Registry I. Rodríguez-Pinto et al. Autoimmunity Reviews 15 (2016) 1120–1124

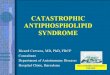
Histological characterization of APS-associated nephropathy
Sciascia, S. et al. Nat. Rev. Nephrol. (2014) 10, 279–289

Scleroderma renal crisis
Thrombotic microangiopathy changes in SRC
• Small vessel thrombi : 11/17 (65%) • Glomerular thrombi : 3/17 (18%), (P = 0.01)
Thrombotic microangiopathy
changes in HUS • Glomeruli : 11/12 (92%) • Small vessels : 4/12 (33%) (P = 0.009)
Prominent arterial onion skin lesion
Arterial thrombosis associated with prominent glomerular ischemic collapse

Seronegative CAPS
• First introduced to describe patients with clinical manifestations highly suggestive of APS but with persistently negative LA, aCL and anti-b2 glycoprotein I (anti-b2GPI)
Hughes GR, Khamashta MA. Ann Rheum Dis 2003;62:1127.
• Antiphospholipid antibodies
– Lupus anticoagulant
– aCL (IgG and/or IgM)
– Anti-b2GPI antibody (IgG and/or IgM)

Non-criteria aPLs • Antibodies to vimentin/cardiolipin complex
– Persistently positive in almost all APS patients and a large number of SNAPS patients.
• Anti-PT: aPT-A and aPS/PT
– Good specific tests to confirm APS; but standardization needed to be included in the diagnostic criteria.
– Anti-PT-A + other tests: good risk marker for thrombosis.
• The annexin A5 resistance assay
• IgA aCL and IgA anti-b2GPI antibodies
• Antibodies to negatively charged phospholipids : PE, PA, PS and PI

Treatments of CAPS
• Anticoagulant • Glucocorticoids • Plasmapheresis • IVIg • Cyclophosphamide • Rituximab • Eclulizumab • Others : Defibrotide, Prostacyclin


Summary of recommendations
Legault K, et al Thromb Haemost 2018; 16: 1–9

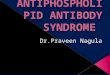
Treatment algorithm for CAPS
EXPERT REVIEW OF HEMATOLOGY, 2017, VOL. 10, NO. 4, 365–374

Treatments
CAPS: Descriptive analysis of 500 patients from the International CAPS Registry I. Rodríguez-Pinto et al. Autoimmunity Reviews 15 (2016) 1120–1124

Treatment outcome
Recovery rate
Anticoagulants + corticosteroids 63.8 %
AC+ CS+ therapeutic plasma exchange 77.8 %
AC + CS + TPE and/or IVIG 69 %
CAPS registry
AC+ CS+ therapeutic plasma exchange
16/21 full response
3/21 partial response
Uthman I, Transfus Apher Sci 2005;33(1):11–7

Therapeutic apheresis in the treatment of CAPS
• Response rate in combine with other treatments (AC+CS) ~ 76-78%
• FFP vs albumin – FFP provide natural anticoagulant, complement activation
products and cytokines.
• Volume – 2-5 L
• Start within first 12 hours and daily session in first 3 days,
• Duration of treatment 3-5 days

Final diagnosis • Disseminated CMV infection • HAP
– Acinetobacter baumannii - XDR
• IPA – Lung C/S : Aspergillus fumigatus
• Scleroderma : SRC
Treatment • Dexamethasone 5 mg IV q 6 hr • Enoxaparin 0.4 ml SC OD • ASA (81) 1x1 • Plasmapheresis, IVIg • ATB

Management of SRC
Autoimmunity Reviews 17 (2018) 882–889

Conclusions Catastrophic antiphospholipid syndrome (CAPS) • Disseminated thrombosis, mainly in small vessels • Leads to multi-organ failure • Many.. many mimic syndromes
1. Exclude condition that need specific treatment : TTP : HIT : SRC 2. Treatments should be started ASAP : Anticoagulant : Immunosuppressions e.g CS, PE, IVIg : Supportive care : RRT, infection etc.

THANK YOU FOR YOUR ATTENTION