Embed Size (px)
Citation preview

APDSF Executive Committee Meeting
8th Sept.2017 The Taj Mahal Hotel
New Delhi
( Rtd.Br. Gen.)Dr Lalita Joshi
President DSAN
Vice President APDSF

Introduction
Nepal is landlocked country between north in China and India in south, west and east.
Population 29,033,914 (July 2016 est.) Kathmandu 1.183 million
2015 est.
2/3 of the country is covered by hills and mountains More than
84% of population live in rural area.
Literacy rate: 53.7% (male:65, female: 43)

Birth rate 19.9 / 1,000 population 2016
Mother’s mean age at birth 1st child 20.1 years in 25-29 years group
Dialects 123
Religion Hindu 81% Buddhist 9%
Mt. Everest 8848 meters World’s most unique Living Goddess KUMARI

Situation of Disability in Nepal
Different types of disabilities:
o Physical disability: 36.3 percent of the
disabled population
o Blindness/Low vision: 18.5 percent
o Deaf/Hard of hearing: 15.4 percent
o Speech problem: 11.5 percent
o Multiple disabilities: 7.5 percent
o Mental disability: 6 percent
o Intellectual disability: 2.9 percent
o Deaf-Blind: 1.8%
Earthquakes 2015, the number of disabled persons in Nepal has increased.
Thousands of “temporarily or permanently disabled through crush or other injuries.”
Worldwide 20,000 ID

Disability situation
National Census held in 2011 :- 7-10 % of total population disabled
Still disability taken as penance to past sins and object of pity.
68.2% PWDs are illiterate compared to without disability
No comprehensive data on Developmental disabilities
Skill training negligible for DD
Research showed 69.3% depend on family support .
PWDs posed problems in 90.5 % of the households
Health, accessibility, education, economy, and employment opportunities for Developmental disabilities in particular almost nil
Never got any treatment of disabilities or co-morbid conditions (as in DS) though curable due to lack of knowledge , poverty , poor health facilities
DD face Discrimination / restriction from achieving their fundamental rights by Government, family and society

Human ambulance
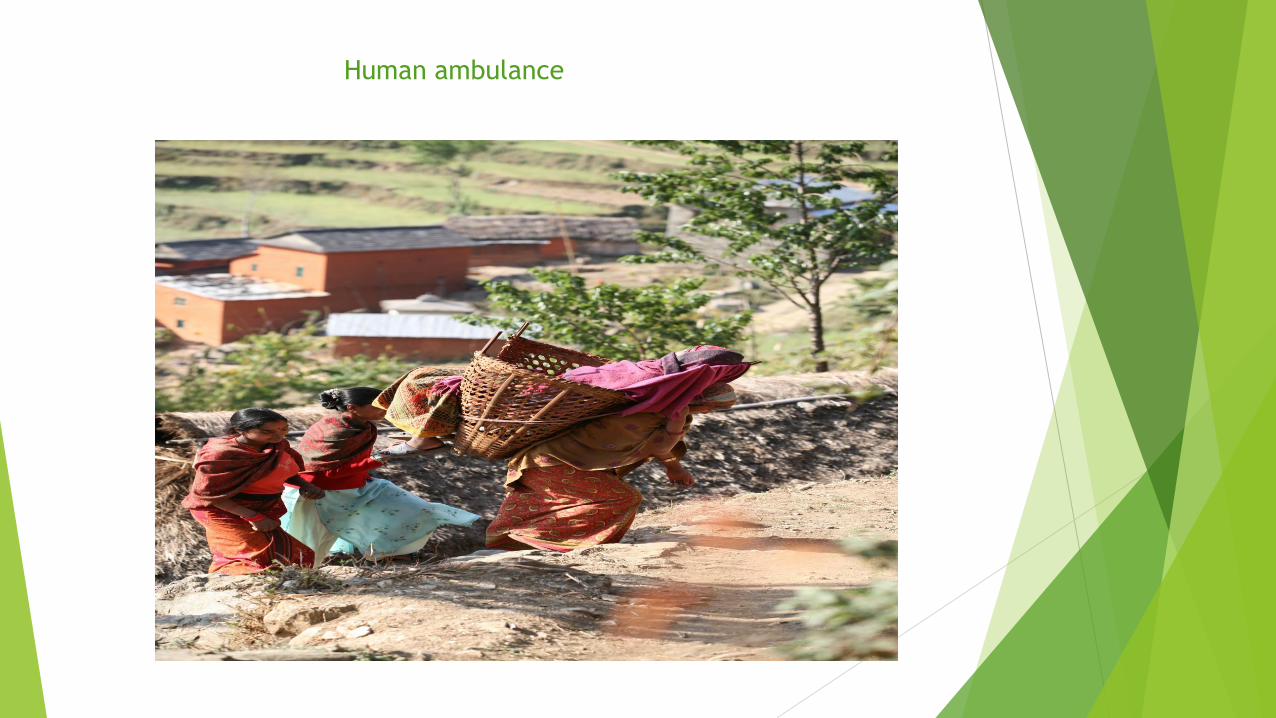
Human ambulance
Need of Data on disability
Assist policymakers to make decisions about the type of preventive programs appropriate for the country.
Increase access to services by removing physical and social barriers
Thematic disability curriculum adaptations for ease /success in education
Skill training for livelihood opportunities
Encourage governments to construct better facilities or provide tax incentives to schools or firms that accept persons with disabilities
Global Scenario
The increasing risk of chromosomal abnormalities , particularly Down syndrome, with advancing maternal age . Middle- and low income countries have a high birth prevalence of Down syndrome for a number of reasons, including a high frequency of older women becoming pregnant, limited access to family planning, and absent prenatal screening, diagnosis and associated services. Birth prevalence may be as high as2-3 per 1,000 live births in middle- and low-income countries and as low as 1.2 per 1,000 live births in high-income countries (Modell et al., 1992; WHO, 1996). An estimated 217,300 infants with Down syndrome are born each year. Early infant or childhood death from congenital heart disease and infection is common among infants and children with Down syndrome in middle- and low-income countries. In South America, 55 percent of infants with Down syndrome die prior to their first birthday, approximately 60 percent of them having congenital heart defects (Castilla et al., 1998).

Bangla Desh Total population (‘000) 148 692 Estimated annual births (‘000) 3 038 5442 annual births with Down syndrome, March of Dimes 2006 Bhutan The March of Dimes Report on Birth Defects estimated that 876 children were born with birth defects annually in Bhutan (Christianson, Howson and Modell, 2006). 32 with Down syndrome India Total population (‘000) 1 224 614 Estimated annual births (‘000) 27 165 Down syndrome frequency of 1 in 916 (82 cases of Down syndrome in 75 103 births) (Verma et al., 1998). In the more recent three-centre study that specifically investigated Down syndrome, 1 per 1150 births was affected. Indonesia Total population (‘000) 239 871 Estimated annual births (‘000) 4 372 The Down Syndrome Association of Indonesia estimates that there are almost 300 000 cases in the country Down syndrome, 0.12%; (MoH Republic of Indonesia, 2010). Sri Lanka Total population (‘000) 20 860 Estimated annual births (‘000) 378 The March of Dimes Report on Birth Defects estimated that 22 641 children were born with birth defects annually in Sri Lanka(Christianson, Howson and Modell, 2006). 692 with Down syndrome
Regional scenario

Country scenario - NEPAL Total population (‘000) 29 959 Estimated annual births (‘000) 72
Sources: 1. United Nations Children’s Fund. State of the world’s children 2012: children in an urban world. New York:
UNICEF, 2012
2. The UN Inter-agency Group for Child Mortality Estimation (IGME). Levels & Trends in Child Mortality: Report 2012. 2012
3. Ministry of Health and Population (MOHP) Nepal, New ERA, and ICF International Inc. Nepal Demographic and Health
Survey2011. Kathmandu, Nepal: Ministry of Health and Population, New ERA, and ICF International, Calverton, Maryland,
2012.
Why have DS not received the attention they deserve to date from policy-makers, funding organizations and health-care providers? 1 This is probably due to the misperception that these disorders are rare. 2 Another myth is that DS require expensive and high technology interventions for their care and prevention that are beyond the health budgets of low- and middle-income countries (LMIC). On the contrary, it has become apparent that simple technologies and strategies are at hand for prevention
The March of Dimes Report on Birth Defects estimated that 43 727 children were born with birth defects annually in Nepal (Christianson, Howson and Modell, 2006). They comprise of 1533h with Down syndrome. 2016 WHO reports show Down syndrome being 3rd in the Birth defects list in Southeast Asia region including Nepal.

Challenges
a. Surveillance program
No database of DS deliveries ( Hospitals/home).
b. Genetic services
No Dept. of Medical genetics, Genetic counsellors
C. Prevention program
No preconception genetic counselling in high risk group for DS
d. Services for DS
Health needs / Early interventions
Quality education/ employment Key obstacles unwillingness to creating a more accessible environment at schools or workstations Transition from adolescence to adulthood – programs for self sufficiency
Old age issues (physical, psychosocial welling being) now lifespan increased
nearly to 70 years

Opportunities
Education - DOE is doing curriculum development , adaptations on need based assessments / teachers training program on specific disability types along with general disabilities
Health - free heart operation for children below 15 yrs for all depending on budget allocations from Govt.
Genetic lab started in Bir Hospital
BD Surveillance, Prevention & Control being formulated by FHD
Record of birth defects HMIS started
Ten hospitals identified for initiating birth defects surveillance, needs consensus and commitments
Early detection/referral training started (2 districts Jajarkot –FCHV ,MO, Stakeholders Rukum - Health facility incharge ,MO )
10 years disability action plan /policy for prevention, treatment ,rehabilitation formulated 2016 -2025

Way forward
Family planning- small family size, less babies in advanced maternal age
Preconception/Antenatal screening – genetic screening/counseling
Newborn screening- inexpensive clinical examination and karyotyping on suspicion
Equal/easy access to diagnostic facilities
Training and awareness programs for primary health care providers ,doctors, nurses,female health workers, birth attendants
Database of DS in hospitals /home in HMIS
MEDIA messages in public interest for detection / awareness
Prenatal diagnosis at to be added to ANC protocol
Can provide endorsement, resources and support.
To carry out activities which could not be accomplished alone
A better pool of experts and experience
Shared apprenticeship and exchange of know-how
An increased brand/public awareness
Legality of pursued action
APDSF






























