Embed Size (px)
Citation preview

Jan W. Casselman, MD, PhD . F. Erwin Offeciers, MD, PhD . Paul J. Govaerts, MDRudolf Kuhweide, MD . Hugo Geldoí MD . Thomas Somers, MD . Guido D'Hont, MD
Aplasia and Hypoplasia of the VestibulocochlearNerue: Diagnosis with MR Imaging'
PUWOSE: To introduce aplasia orhypoplasia of the vestibulocochlearnerve (VCN) as a possible cause oÍhearing loss and to identify the mag-netic resonance (MR) imaging char-acteristics of this entity.
MATERIALS AND METHODS: Inseven patients with congenital deaf-ness oÍ unexplained sensorineuralhearing loss, MR imaging enableddiagnosis of aplasia or hypoplasia ofthe VCN. Axial (0.7-mm) three-di-mensional Fourier transformation-constructive interference in steadystate (3DFT-CISS) images and para-sagittal reconstruction images per-pendicular on the course of the VCNwere obtained. Twenty normal innerears weÍe also studied; their findingswere compared with those of thepatients.
RESULTS: The facial nerve and infe-rior and superior vestibular and co-chlear branches of the VCN wereidentified on the MR images in the20 normal inner ears. Aplasia of theVCN was detected in two patientswith normal labyrinths but with asevere stenosis of the internal audi-tory canal. A common VCN with ab-sence of the cochlear branch wasfound bilaterally in two patients witha congenital malformation oÍ thelabyrinth. A common VCN with ab-sence oÍ hypoplasia of the cochlearbranch was found in three patientswith normal internal auditory canalsand labyrinths.
CONCLUSION: Submillimetric gra-dient-echo images (eg, 3DFT-CISS)should always be used to excludeaplasia or hypoplasia of the cochlearbranch of the VCN in all cochlearimplant candidates and patients withcongenital deafness. This entity, whichcan occur with or without associatedlabyrinthine malÍormatiory should beconfirmed in two planes.
ll rÍecNrrIc resonance (MR) imag-IVI ing is accepted as the methodof choice to look for abnormalities inpatients with sensorineural hearingloss andlor vertigo (1-5). Moreover,gradient-echo MR imaging proved itsvalue in patients with congenital in-ner ear malformations (6) and espe-cially in candidates for cochlear im-plantation (7-9). The MR demonstrationof a normal cochlea, with a fluid-filledscala $rmpani and vestibuli, indicatesthat these patients are ideal candidatesfor implantation. Nevertheless, in someof these patients the cochlear implantdid not result in auditory perception,although the implant iisètt wórteaand was not causing the problem(O'Donoghue GM, personal commu-nication, 1996). A possible explanationcould be an absent or abnormal co-chlear branch of the vestibulocochlearnerve (VCN). With the advent of sub-millimetric T2-weighted gradient-echo images, these nerves and nervebranches can be visualized in a reli-able way inside the internal auditorycanal and cerebellopontine angle (10).In the internal auditory canal, the fa-cial nerve and the cochlear branch,inferior vestibular branch, and supe-rior vestibular branch of the VCN arebest recognized on axial three-dimen-sional Fourier transformation-<onstruc-tive interference in steadv state (3DFT-
CISS) images and can be confirmed onparasagittal reconstruction images (5).
The purpose of our study was tointroduce aplasia or hypoplasia of theVCN as a possible cause of sensori-neural hearing loss or congenital deaf-ness and to identify the MR imagingcharacteristics of this entity with useof the 3DFT-CISS sequence.
MATERIALS AND METHODS
Subjects
During a period of 24 months (fromFebruary L994toJanluary 1996), the diag-nosis of aplasia or hypoplasia of the co-chlear branch of the VCN was made at MRimaging in seven patients (six male pa-tients, one Íemale patient; age range,242years; average age, 11 years). The commonclinical finding that led to computed to-mography (CT; and MR imaging was sen-sorineural hearing loss. The sensorineuralhearing loss was congenital and bilateralin three patients (who were part of a co-chlear implantation selection program)and congenital and unilateral in three pa-tients, and sudden hearing loss occurredin one patient. More details oÍ the clinicalpreseniation oÍ these patients are listed inthe Table.
Imaging Protocol
All patients underwent MR imagingperformed with a 1-T, active-shielded su-
Indexterms: Ear,abnormalities,l'2b1419,l251,429.Ear,anatomy,l2\gz.EaIMR"12S121.4I2.Magnetic resonance (MR), pulse sequences, 1,251,21412 . Magnetic resonance (MR), thin section,125.12'1,412 . Nerves, abnormalities, 1,25 1,41,9, 1,25 1.429
Abbreviations: 3DFT-CISS : three-dimensional Fourier transÍormation-constructive interferencein steady state, VCN = vestibulocochlear nerve.
Radiology 7997 ; 202:77 3-7 81
l From the Departments of Diagnostic Radiology (J.W.C.) and Otorhinolaryngology (R.K., G.D.),AZ St-Jan Brugge, Ruddershove 10, B-8000 Brugge, Belgium; the University Department of Ear, Noseand Throat, Sint-Augustinus Hospital, University of Antwerp, Belgium (F.E.O., P.I.G., T.S.); and theDepartment of Otorhinolaryngology, AZ St-Lucas, Brugge, Belgium (H.G.) Received June 1,4,'1,996;revision requested July 29; revision received October 10; accepted October 14. Address reprint re-quests to I W.C
O RSNA,1997
773

Clinical and Imaging Data of the Affected Inner Ears of the Seven Patients with Aplasia oÍ HyPoPlasia of the VCN
Pati€ntNo./SexlAge (v)
MR Findings
Clinicai Presentation Side CT Findings Labyrinth IAC Nerues
7/F/2 Until age 9 months, parents thorrghtfhe child had nonnat hearing; at 14months, bilateral congenital deafnesswas conÍirmed with audiogram(vibration deafness) and AB&nóïmàl facial nerve function; poten-tial cochlear implant candidate
2/M/42 Bilateral aplasia of external ear and theEAC, ncrmal Íacial nerve functron,plastíc and otologic surgery(approximately 30 interventions),BAHA on the right side andbilateralepitheses, sudden SNHL on the rightside (at àge 42 years) with com-pletely deaf ear on the left {peraudiogram)
\IM/Z Congenital deaÍness, noted by parentsat age 6 months; at 18 months. deaf-ness confirmed with ABR and audio-gr:am (corner audiogram); presum-ably autoscmal or X-linked tecessive;electric promontory sfimula tion:response on }eft eaÍ; potentialcochlear implant candidate
4/M110 Bilateral congenital deafness conÍirmedwith audiogÍam; electric promontorystimulation is planned; potentialcochlear implant candidate
5lM/6 Congenital hearing loss an the left sidesince birth; at 6 y€aÍs, total con-genital deafness on the left side con-Íjrmed with audiogram (phantomcurve), normal hearing on the rightsíde
Right Common cavity,abnormal semicir-cular canals
Lefi Common cavity,abnormal semicir-cular canals
Right Common cavity, IACstenosis, partialdeveloPment ofSSC
LeÍt Common cavity, IACstenosis, PartialdevèloPment ofS5C
Left Normál
Right IACstenosisLeft IAC stenosis
LeÍt Stenosis,separatecanál for faciàlnerve
Stenosis,separate AplasiaoÍVCNcanal for Íacialnerve
Aplasia of VCNAplasia of VCN
Common VCN
CommonVCN
Common VCN
Common VCN
Rudimentary ves-tibuiar nerve,absent cochlearbranch
Rudimentary ves-tibular nerve,absent cochlearbranch
Hypoplasia of thecochlear branch
NormalNormal
Normal
StenosisStenosis
Normal
Normal
Stenosis
Stenosis
Normal
Normal
Normal
Common cavity,atrnormal semicir-cular canals
Common cavi$r,abnormal semicir-cular canals
Common cavity. pàr-tial development ofSSC
Common cavity, par-tial development ofSSC
Normal
6/M/5
7lM/1.2
Congenital deafness on the right sidesince birth, only míld hearing loss onthe }eft; completely deaf ear on theright confirmed with audiogram
Child turns head to the left to hearwith nomal right ear; ccngenitalhigh Írequency heaïing loss on theIeft side conÍirmed with audiogram;normal hearing on the right
Right Not applicable Norrnal
Left Normal Normal
Note,-ABR - auditory brain'stem Íespónses/ BÀHA : bone'anchored hearing aid, EAC = externai auditóly canal, IAC : internal auditory canal, SNHL :
sensoíineural hearing loss, SSC : supedor semiciïcular canal.
peÍconductive system (Magnetom SP 42;Siemens, Erlangen, Germany) A standardcircular oolarized head coil was used toallow simultaneous imaging oÍ both innerears. All Datients underwent a routine in-ner eaÍ siudy with an axial,7-mm-thick,T2-weighted spin-echo sequence (2,000/16,90 [repetition time msec/echo timemsecl, one signal acquired) of the brainand a selective, axial,3-mm-thick, contigu-ous, T1-weighted spin-echo sequence(500/14, four signals acquired) with andwithout administration of an intravenousgadolinium chelate. Their temporal boneswere also examined with a coronal gado-linium-enhanced T1 -weighted sequence.A dose of 0 1 mmol/kg gadoterate meglu-mine (Dotarem; Guerbet Laboratories,Aulnay-sous-Bois, France) or gadopen-tetate dimeglumine (Magnevist; Schering,Berlin, Germany) was used. The Patients
774. R.adiology
were also examined with a 3DFT-CISS gra-dient-echo sequence. The details of thisgradient-echo sequence have been pub-lished previously (4,10) The most impor-tant parameters of this sequence are theÍollowing: 15/21,65" flip angle, one axialslab oÍ 22.4-mm thickness, 32 partitions,256 x 256 matrix, 170-mm field of view,two signals acqufued This results in0.7-mm axial sections with an in-planeresolution oÍ 0.66 x 0 66 mm and a totalacouisiton time oÍ 8 minutes 6 secondsThè absence oÍ nerves oÍ nerve brancheswas always checked on Parasagittal 3DFT-CISS reconstruction images. These recon-struction images were made through thecerebellopontine angle and middle andlateral thirds of the internal auditory canaland were angled perpendicular on thecourse oÍ the nerves (Figs 1, 2a,2b).
In six of the patients, 1.S-mm-thick axial
CT sections also were obtained every 1mm, and in two patients (patients 2 and 4)additional coronal CT scans were acqufued.
Control Group
Twenty normal inner ears were alsostudied with 0.7-mm-thick 3DFT-CISS im-ages The selected 3DFT-CISS examina-tions were Íree oÍ movement or flow arti-facts and therefore allowed adequateevaluation of the nerves in the cèrebello-pontine angle and internal auditory canal.The reliability to distinguish the facialnerve and the inferior vestibular, superiorvestibular, and cochlear branches of theVCN in the cerebellopontine angle andinternal auditory canal was checked onthese axial images and on the parasagittal3DFT-CISS reconstruction images, made
March7997

\ \
perpendicular on the course oÍ the nervesin the cerebellopontine angle and in themiddle and lateral thirds oÍ the internalauditory canal. The thickness of the nerves inrelation to one another was evaluated on theparasagittal reconstruction images. Espe-cially, the thicknesses oÍ the VCN (in thecerebellopontine angle) and its cochlearbranch (in the intemal auditory canal) werecompared with the thickness of the facial
RESUTTS
Control Group
The facial nerve and the cochlearbranch, inf erior vestibular branch,and superior vestibular branch of theVCN (Fig 1) could be visualized onthe axial3DFT-CISS images in all20normal inner ears (Fig2a,2b). On theparasagittal reconstruction imagesmade at the level of the cerebellopon-tine angle, both the facial nerve andVCN were always visible. At this loca-tion, the VCN was 11/z-2 timeslargerin diameter than the facial nerve in19 of the 20 normal inner ears (Fig 2c).In one inner ear, they were the samesize. In 19 inner ears, the facial nerveand the cochlear branch of the VCNand the common vestibular nerve (thevestibular branch of the VCN, not yetbifurcating into a superior and infe-rior branch) could be distinguishedon the parasagittal reconstruction im-ages made through the middle thirdoÍ the internal auditory canal. Thethree branches of the VCN and thefacial nerve could be separated fromone another on the parasagittal recon-struction images made near the fun-dus of the internal auditory canal. Inonlv one patient was it difficult to vi-suaiize thè facial nerve because this
Volume 202 o Number 3
nerve probably was small and adja-cent to the wall of the internal audi-tory canal; the three branches of theVCN were clearly visible. On theseimages made through the internalauditorv canal. the cochlear branchof the VCN was larger than the Ía-cial nerve in 12 inner ears, was aslarge as the Íacial nerve in five innerears, and was smaller than the facialnerve in only three inner ears (Fig2d,2e).
Patients
In all patients, the T2-weightedspin-echo images of the brain werenormal, and the unenhanced andgadolinium-enhanced T1 -weightedimages of the inner ear helped con-firm only the stenosis of the internalauditory canal (five inner ears [threepatientsl) and the malformations ofthe osseous and membranous laby-rinths (four inner ears [two patients]).However, these inner ear malforma-tions were far easier to visualize onthe 3DFT-CISS images. The absence ofgadolinium enhancement in the cer-ebellopontine angle, internal auditorycanal, and membranous labyrinth ruledout an acoustic neuroma or acute laby-rinthitis as the cause of the deafness orhearing loss. Chronic labyrinthitis wasruled out on CT scans (no calcifications)and on the 3DFT-CISS images (nofibrous obliteration of the intralaby-rinthine fluid spaces). Both inner earswere involved in three oÍ the sevenpatients.
Two patients (three inner ears) hadnormal osseous and membranouslabyrinths but had very narrow inter-nal auditory canals. One of them (pa-
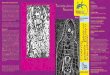
Figure 1. Diagram shows the nerves in the internal auditory canal.The posterior wall of the internal auditory canal is removed, and crosssections (top) through the cerebellopontine angle-porus region (left),middle third of the internal auditory canal (middle), and lateral thirdof the internal auditory canal (right) were rnade. Facial nerve (smallthick arrow), VCN (large arrow), common vestibular nerve (large ar-rowhead), inferior vestibular branch (small arrowhead), superior ves-tibular branch (curved arrow), and cochlear branch (thin arrow) of theVCN are indicated. Á : anterior, P : posteÍior, f : jugular Íoramen,open arrow = petro-occipital fissure
tient 2) even had a separate bony ca-nal for the facial nerve/ parallel to theinternal auditory canal. In these twopatients, the VCN was completelyabsent, and onlv a facial nerve wasvisualized on tÉe gradient-echo im-ages (Fig 3).
Associated malformations of theosseous and membranous labyrinthswere seen in only two patients (fourinner ears [patients 3 and 4]), and inone of them, the internal auditorycanal was also stenotic on both sides.These patients had a common VCN,without trifurcation into cochlear,inÍerior vestibular, and superior ves-tibular branches (Fig ).
Three other patients (three innerears) had normal internal auditorycanals and labyrinthine structures.Two of them (patients 5 and 6), how-ever, had a common VCN runningtoward the vestibular labvrinth. andin both patients the cochlear branchof the VCN was absent (Fig 5). In theother patient (patient 7), hypoplasiaof the cochlear branch of the VCNwas found (Fig 6). All MR and CTfindings are listed in the Table.
DISCUSSION
For years, CT was the best tech-nique to look for congenital malfor-mations of the inner ear in patientswith congenital deafness. With theadvent of MR imaging, it became pos-sible to exclude abnormality along theacoustic pathway and in the auditorycortex on T2-weighted spin-echo im-ages. Later on, gadolinium-enhancedTl-weighted spin-echo images wereused in these patients to exclude acous-tic neuromas; labyrinthitis, and otherpossible pathologic conditions in thecerebellopontine angle, internal audi-tory canal, and membranous labyrinth(1-5). In recent years, T2weighted gra-dient-echo techniques have beenused more and more to study the in-ner ear. These gradient-echo imagesare needed to evaluate the very smallstructures of the inner ear and to de-tect some of the abnormalities in thecerebellopontine angle, internal audi-tory canal, and membranous laby-
Radiology . 775

rinth (4-6,8). Good gradient-echo im-ages must provide high contrastbetween the cerebrospinal fluid-in-tralabyrinthine fluid, nerves, andbone, and the sections must be verythin. In this study, axial 0.7-mm-thin3DFT-CISS images were used becausethey provide excellent contrast be-tween the different inner ear struc-tures, and even the cerebrospinalfluid around the brain stem remainscompletely white on these images(10). Similar results were reportedwith other gradient-echo techniques,including 3D gradient-recalled acqui-sition in the steady state (11), contrastmaterial-enhanced fast acquisition inthe steady state (12), and 3tt fast im-aging with steady-state precession(13), and even a fast spin-echo (14)sequence proved to be beneficial inthe study oÍ the inner ear. The con-genital malformations, detectablewith CT, could now also be recog-nized on these gradient-echo images.The big advantage, however, was thatit now became possible to detect un-expected inner ear malformations inpatients with sensorineural hearingloss and/or vertigo by using MRalone, obviating an additional CTstudy (6).
CT and MR imaging could now beused to confirm the presence of a nor-mal cochlea in candidates for cochlearimplantation and to exclude calcifica-tions in the cochlea (at CT) and/orfibrous obliteration in the membra-nous labyrinth (at MR imaging). Inthe absence of calcifications and fi-brous obliterations, it is possible tointroduce a cochlear implant into thecochlea. It is, however, obvious thatthe next important structure to bechecked in ihese patients is the co-chlear branch of the VCN. However,the MR technique must be fine-tunedto be useful fof detection of nerveaplasias or hypoplasias. These malfor-mations can be detected only on thin-section T2-weighted gradient-echoimages (eg, 3DFT-CISS, etc) or comPa-rable fast spin-echo images.
Visualization of the Nervesin the Internal Auditory Canal
It is crucial to use images with athickness of 1 mm or less to visualizethe facial nerve and the three branchesof the VCN separately inside the in-ternal auditory canal. Nerve visualiza-tion becomes more accurate when, forinstance, 0.7-mm-thick sections areused instead oÍ 1.0-mm sections (10).The four nerves could be visualizedin the internal auditory canal on theaxial 0.7-mm-thick 3DFT-CISS images
776 . Radiology
e.
Figure 2. Normal facial nerve and VCN in the cerebellopontine angle and internal auditory
canal. (a) Axial O.7-mm-thick 3DFT-CISS image (15127,65" flip angle) obtained through the
superior part oÍ the left internai auditory canal shows the total course of the facial nerve
(black arrowheads) from the brain stem to the fundus of the internal auditory canal. At this
level, the facial nerve is always parallel to the VCN (black arrows), which becomes the supe-
rior vestibular branch (white arrows) of the VCN in the lateral part of the internal auditory
canal. F : flocculus, V : vestibule, white arrowheads = lateral semicircular canal (b) Axial
O.7-mm-thick 3DFT-CISS image (15/27,65'flip angle) obtained through the inferior part of
the left internal auditory canal. A typical biÍurcation of the VCN into the cochlear (thin white
arrow) and inferior vestibular (large white arrow) branches is always visible on the images
through the inferior half of the internal auditory canal. The VCN can be seen in the cerebello-
pontine angle and medial third oÍ the internal auditory canal (large black arrows). V : vesti-
Lule, thin black arÍows = cochlea. Lines C Ë represent the perpendicular lines along which
level of the middle third of the internal auditory canal (along line D in a and b). The VCN
has divided into a cochlear branch (thin white arrow) and a common vestibular branch (large
white arrow). The facial nerve (arrowhead) is visible in its normal high and anterior position
in the internal auditory canal Á = anterior, P : posteÍioÍ. (e) Parasagittal 3DFT-CISS recon-
struction image obtained perpendicular to the course of the nerves at the level oÍ the lateral
third of the internal auditory canal (along line E in a and b). Near the fundus of the internal
auditory canal, the Íacial nerve (arrowhead) and the cochlear branch of the VCN (thin white
arrow) are still visible in the anterior part of the internal auditory canal and have the same
size, which can be normal, but more frequently the cochlear nerve is the larger one. At this
level, the common VCN has split into superior (small white arrow) and inferior (large white
arrow) branches. Á : anterior, P : posterior.
in all 20 normal inner ears and on the nerve that is difficult to see on theparasagittal reconstruction images in axial images.19 of them. This proves that in the ab- The thickness of the nerves insidesence of movement artifacts, in coop- the internal auditory canal can beerative patients, this technique is re- measured, but these nerves are tooliable enough to demonstrate the small to be measured in a reliable wayfour nerves (Fig 2). Verification of on images with an in-plane resolutionthe nerves in a second plane makes oÍ 0.66 x 0.66 mm and a thickness of
March 1997

b. e.
Figure 3. Patient 1. Type 1 malformation of the VCN (aplasia). (a) Axial 0.7-mmthick 3DFT-CISS image (75/27,65" flip angle) obtained through the upper part of the right stenotic inter-nal auditory canal Only very little cerebrospinal fluid can be seen in the stenotic internal au-ditory canal (white arrows), and it is impossible to demonstrate the presence or absence oÍnerves in such a narrow canal Only one nerve, the facial nerve (black arrows), can be recog-nized in the cerebellopontine angle F = flocculus, arrowheads : intralabyrinthine fluid in thecomnon crus (b) Axial 0 7-mm-thick 3DFT-CISS image (15/27,65" flip angle) obtained through thelower part of the right stenotic intemal auditory canal. Again, little cerebrospinal fluid is visible inthe stenotic intemal auditory canal (thin white anows). High-signal-intensity inhalabyrinthine fluidis seen in the cochlea (large white arrow), posterior semicircular canal (small white arrow), and vesti-bule (arrowhead). F : flocculus. (c) Parasagittal 3DFT-CISS reconstruction image obtained perpen-dicular to the course of the intemal auditory canal and facial nerwe at the level oÍ the right cerebello-pontine angle. At the level of the cerebellopontine angle, only the facial nerve (arrow) can berecognized anterior to the flocculus (F) In normal eaÍs, two nerves are always present at thissite (Figs 1,2c) Therefore, parasagittal ÍeconstÍuction images through the cerebellopontineangle are very reliable to demonstrate the absence of the VCN in patients with congenitaldeafness and normal facial nerve function. á : anterior, p : posterior. (d) Parasagittal 3DFT-CISS reconstruction image obtained perpendicular to the course of the internal auditory canalat the level of the middle third of the internal auditory canal shows the very narrow internalauditory canal filled with cerebrospinal fluid (arrow) It is impossible to recognize nerves inthis narrow canal. Á : anterior, P : posterior (e) Parasagiital 3DFT-CISS reconstruction im-age obtained perpendicular to the course of the internal auditory canal at the level of the lat-eral third of the internal auditory canal. At the level of the fundus, the internal auditory canalis wider (white arrows), and this allows visualization of the facial nerve (black arrow); thethree branches of the VCN are absent Á : anterior, p : posterior
nerve and its superior and inferior cerebellopontine angle, where thevestibularbranches is difficult to evalu- facial nerve and the VCN are found,ate. Sometimes the bifurcation is seen and the latter was nearly always 1/z-2only near the fundus of the internal times larger than the facial nerve andauditory canal, and in the region just was never smaller. These findings canmedial to the bifurcation, the nerve be used as a reference when the nervesthen becomes shaped like a figure in the cerebellopontine angle and inter-eight and therefore has a large cÍanio- nal auditory canal have to be checked.caudal diameter. The diameters of the
:.::I": l^111' I ::1 il:, ?^'1{ :,"_':^"_ E mb ryo I o gic D evero p mentwere easler to cteDrct rnsrde tne rnter-nal auditory canal on the parasagittal Aplasia of the complete VCN andimages and were more constant in aplasia or hypoplasia of its cochlearsize. Most frequently, the cochlear branch were demonstrated on MRbranch of the VCN was larger than images in seven patients (10 innerthe facial nerve, although the latter ears). These abnormalities occurredcan be as large or even larger. The isolated or in association with a steno-findings were more constant in the sis of the internal auditory canal
Volume 202 r Number 3
and/or congenital malformation ofthe labyrinth. A possible explanationfor these isolated and associatednerve abnormalities can be sought inthe embryologic development of thelabyrinth and VCN.
The development of the humancochlea starts with the appearance ofthe otic placode at the third embry-onic week. This placode transformsinto the otic vesicle that gives rise tothe endolymphatic duct, the utricu-lus, sacculus, semicircular canals, andcochlea. At 9 weeks, the cochlearwindings are fully developed and theappearance of the neural epitheliumhas started. Neuroblasts of the co-chlear ganglion separate from the oticepithelium. Fibers from these gan-glion cell bodies grow peripherallyback into the otic epithelium and cen-trally into the brain stem (15). Thefirst afferent fibers entering the undif-Íerentiated otic epithelium are seen at9-10 weeks (16). In the avian embryo,an abundant neuronal populationinvades the epithelium (77,78). This isfollowed by the disappearance ofmany redundant fibers, which maylead to a25% redsction in the num-ber of fibers. This reorganization iscalled "neural stabilization" (17\. Al-though it has been thought that thecochlear development or differentia-tion depends on the innervation, thishas been proved not to be the case.Explants of chicken otic vesicles thatlack neuronal fibers give rise to innerear sensory structures with normal mor-phologic features in vitro. This impliesthat the inner ear development is notdependent on any neuronal trigger orstimulus or trophic effect (19). Also, thedifferentiation of the hair cells is con-trolled by location-specific cues thatoriginate in the ear itselÍ. Conversely,the developing inner ear appears tohave an important trophic effect on thesurvival and the cytodifferentiation ofthe afferent neurones. The otic vesiclereleases a nerve growth factor-like sub-stance that is essential for the survivalof the neurones and for "neuronalstabilization" (18).
These data can explain why theVCN or its cochlear branch can beabsent in patients with an abnormalor absent cochlea. It is equally con-ceivable that a disturbance in the tro-phic effect that the cochlea exerts onthe cochlear neurones may result in awell-developed cochlea without asurviving cochlear nerve. The associa-tion of an absent VCN and a stenosisof the internal auditory canal is notexplained by these findings, but apossible hypothesis is that a normalinternal auditory canal is formed onlyin the presence of a normal nerve.
Radiology .777

Figure 4. Patient 3. Type 2A malformationof the VCN (common VCN with aplasia of itscochlear branch in the presence of a labyrin-thine malformation) (a) Axial 1.S-mm-thickCT scan of the left inner ear obtained throughthe upper part of the internal auditory canalshows only a single cavity (black arrows).The cochlea cannot be found at its normalsite (white arrow), and in this patient, thecochlea and the vestibule formed a single or"common caviïy." A partially developed andmalformed posterior semicircular canal (ar-rowhead) can be seen. IÁC = internal audi-tory canal. (b) Axial 1 S-mm-thick CT scan ofthe left inner ear obtained through the lowerpart of the internal auditory canal. The ab-sence of the cochlea (white arrow) and thepresence of a common cavity (black arrows)and a partially developed posterior semicir-cular canal íarrowhead) are confirmed at thislevel. IÁC : internal auditory canal. (c) Axial1.S-mm-thick CT scan of the left inner earobtained through the base of the abnormallabyrinth. At this level, an oval inferior exten-sion oÍ the common cavity can be recognized(arrows) and mimics a basal turn oÍ a cochlea.(d) Axial 0.7-mmthick 3DFT-CISS image (15/27,65" flip angle) obtained through the up-per part of the left internal auditory canal.The facial nerve (black arrow) and a vestibu-lar nerve (large white arrows) can be de-picted just under the roof of the internal au-ditory canal No fluid is seen at the sitewhere one normally finds the cochlea (thinwhite arrow), and a fluid-filled common cav-ity (small white arrows) and posterior semi-circular canal (arrowhead) are the only laby-rinthine structuÍes that can be visualized.The upper paÍt oÍ the posterior semicircularcanal was missing on the adjacent images(not shown) made higher through the innerear. (e) Axial 0 7-mm-thick 3DFT-CISS image(15/21,,65'flip angle) obtained through the middle part oÍ the left internal auditory canal.Both the facial nerve (black arrows) and the vestibular nerve (large white arrows) can be fol-lowed toward the porus oÍ the internal auditory canal where they come close together andtouch the posterior lip of the porus. No fluid is found in the cochlear region (thin white ar-row). A fluid-filled common cavity (small white arrows) and malÍormed posterior semicircularcanal (arrowhead) are noted. F = flocculus (f ) Axial 0 7-mm-thick 3DFT-CISS image (75/27,65'flip angle) obtained through the inÍerior part of the left internal auditory canal. The co-chlear and inferior vestibular branch of the VCN cannot be found. At this level, the Íacialnerve (black arrow) and a "common vestibular nerve" (large white arrow) can be recognizedin the cerebellopontine angle just anterior to the flocculus (F). The nerve is called a common i.
vestibular nerve because no separate superior and inferior branches of the VCN are present inthis patient. The absence oÍ fluid in the normal region of the cochlea (thin white arrow) and the presence oÍ a fluid-filled abnormal broad pos-terior semicircular canal (arrowhead) and "common cavity" (small white arrow) are confirmed. (g) Parasagittal 3DFT-CISS reconstruction im-age obtained at the level of the left cerebellopontine angle Two nerves can be seen in the cerebellopontine angle, and the VCN (white arrow)is larger than the Íacial nerve (black arrow), which is a normal finding Á : anterior, P = posterior. (h) Parasagittal 3DFT-CISS reconstructionimage obtained at the level of the middle third oÍ the leÍt internal auditory canal At this level, the cochlear branch of the VCN is missing, andonly a common VCN (white arrow) posteriorly and a facial nerve (black arrow) can be recognized A = anterior, p : posterior (i) Parasagittal3DFT-CISS reconstruction image obtained at the level of the lateral third of the left internal auditory canal Near the fundus oÍ the internal au-ditory canal, the common VCN (white arrow) is still seen instead of the three branches of the VCN that should be seen at this level. The fac'ial
nerve (black arrow), seen in the anterior part of the internal auditory canal, has an abnormal low position inside the internal auditory canal.Á : anter ior , P : poster ior .
oD'
Therefore, a disturbance in the tro-phic effect of the cochlea can result inloss of too many or all neuronal fibers,and in these patients, the internal au-ditory canal formed around the initialneuronal fibers will not develop fur-ther and eventually wil l be stenotic.
Classification Proposal
The MR findings in the seven pa-tients with aplasia or hypoplasia of
778. Radiology
the cochlear branch of the VCN werein accordance with the clinical find-ings (Table) but as yet cannot be con-firmed with surgery or at pathologicexamination. The authors believe thatthe presented cases represent differ-ent stages or grades of developmentalanomalies oÍ the VCN. According tothe CT, MR imaging, and clinical find-ings and with respect to embryologicknowledge, we propose the followingclassification.
Tupe'l: Aplasia of the VCNËs'sociatrid with Stenosis of theInternal Auditory Canal
Bilateral stenotic internal auditorycanals (patient 1) and a left-sided ste-nosis (patient 2) were recognized onCT scans and on the axial 3DFT-CISSimages and parasagittal 3DFT-CISSreconstruction images. Both patientshad normal labyrinths. It was, how-ever/ impossible to look for nerves inthe extremely narrow internal audi-
N4arch7997

d. e. Í .
Figure 5. Patient 5. Type 28 malformation oÍ the VCN (common VCN with aplasia of its cochlear branch in the pÍesence of a normal laby-rinth) (a) Axial 0.7-mm-thick 3DFT-CISS image (15/21,65' flip angle) obtained through the upper part of the left internal auditory canal. Thefacial nerve (black arrowheads) and a common VCN (large white arrows) are seen high in the internal auditory canal; a vascular loop (blackarrow) is crossing the Íacial nerve deep in the internal auditory canal. Fluid is noted in the lateral (white arrowhead) and posterior (white ar-row) semicircular canals (b) Axial 0.7-mm-thick 3DFT-CISS image (75/21,,65" flip angle) obtained through the middle part oÍ the leÍt internalauditory canal. The Íacial nerve (black arrowheads) can be Íollowed toward the cerebellopontine angle, and part oÍ the "common VCN" (largewhite arrow) is depicted A cochlear branch of the VCN cannot be demonstrated High-signal-intensity intralabyrinthine fluid is noted in thecochlea (small white arrow) and lateral (white arrowheads) and posterior (thin white arrow) semicircular canals. F = flocculus, V = vestibule(c) Axial O.7-mmthick 3DFT-CISS image (75127,65'flip angle) obtained through the inferior part of the left internal auditory canal. Part of thecommon VCN (large white arrow) is still visible near the floor of the internal auditory canal. The cochlear branch of the VCN is again absent(black arrows). Fluid is noted inside the cochlea (small white arrow) and the posterior semicircular canal (thin white arrow). F : flocculus, V =
vestibule. (d) Parasagittal 3DFT-CISS reconstruction image obtained perpendicular to the course oÍ the nerves at the level oÍ the left cerebello-pontine angle The facial nerve (arrowhead) and the VCN (arrow) have the same size at the level of the cerebellopontine angle, which is a rarefinding in normal inner ears. Moreover, in this patient, the VCN was twice as large as the facial nerve on the opposite normal side (not shown),which supports the diagnosis oÍ hypoplasia of the VCN Á = anterior, F = flocculus, P : postedor. (e) Parasagittal 3DFT-CISS reconstÍuctionimage obtained perpendicular to the course of the nerves at the level of the middle third oÍ the left internal auditory canal. The cochlear branchof the VCN cannot be recognized, conÍirming the findings in b and c Therefore, the two nelves seen on this image must be the facial nerve(arrowhead) anteriorly and a common VCN (arrow) posterioÍly A: anterior, P : posterior. (Í) Parasagittal 3DFT-CISS reconstruction imageperpendicular to the course of the nerves at the level of the lateral third of the left internal auditory canal. Near the fundus of the internal audi-tory canal, the Íacial nerve (arrowhead) occupies its normal position. However, a separate superior and inÍerior vestibular branch oÍ the com-mon VCN and a cochlear branch cannot be demonstrated. Instead, a single common VCN continues deep in the internal auditory canal andgets larger in craniocaudal diameter (large arrow) near the fundus, expliining why this nerve could be identified on three contiguous 0.7-mm-thick axial images a-c Á : anterior, p : posterior, small arrow : high-signal-intensity intralabyrinthine fluid in the cochlea
tory canals in these two patients (Fig3). Nevertheless, the cerebellopontineangle could still be evaluated in thesepatients/ and both the axial and re-constructed parasagittal gradient-echoimages showed the presence of a singlenerve-the facial nerve. As alreadymentioned, the absence of the VCN inthe presence oÍ a normal cochlea canbe explained by a disturbance of thetrophic effect (nerve growth factor)that the cochlea exerts on the cochlearneurones (18). The hypothesis for theassociated stenosis of the internal au-ditory canal is that the absence of anormally developing VCN causes thestenosis of the internal auditory canal.The internal auditory canal is formedaround the neuronal fibers of the VCN,but these fibers can again disappearwhen there is a disturbance in thetrophic effect of the cochlea (nervegrowth factor) on these fibers. Thisexcessive loss of fibers or loss of allfibers orobablv results in an arrest ofthe development of the internal audi-tory canal. A separate canal for thefacial nerve was detected on CT scans
Volume 202 o Number 3
and gradient-echo MR images in pa-tient 2. This shows that abnormal de-velopment of the nerves can even beassociated with more severe and rareabnormalities of their canals.
In these patients, the findings onthe parasagittal 3DFT-CISS recon-struction images made through thecerebellopontine angle are very reli-able in the exclusion or confirmationof aplasia of the VCN. Partial volumeeffects cannot explain the disappear-ance of a nerve in this plane, and innormal inner ears, both the facialnerve and VCN were always visibleanterior to the flocculus (Fig 2).Therefore, it is advisable to look foraplasia of the VCN at this level in pa-tients with congenital hearing lossand associated stenosis of one or bothinternal auditory canals.
The MR demonstration of the ab-sence of a VCN might predict that acochlear implant will not work. Nev-ertheless, it could be interesting toperform an electric promontorystimulation test and functional MRimaging of the auditory cortex to ex-
clude the presence of very thin co-chlear fibers, too thin to be detectedon MR images. However, it seems un-likely that a completely invisible VCNon MR images would possess enoughfibers to result in worthwhile hearing.
Type 2: Common VCN uith Aplasiaor Hypoplasia of lts Cochlear Branch
Type 2A: type 2 in the presence of alabyrinthine malformation -In two pa-tients (patients 3 and 4), the cochleaand vestibule formed a single, large,fluid-filled cavitv. known as a com-mon cavity (20).-They also had associ-ated malformations of the semicircu-lar canals (Table). In both patients, theaxial gradient-echo images and theparasagittal reconstruction imagesshowed that the cochlear branch ofthe VCN was absent (Fig a). As men-tioned above, the absence of a normaldeveloping cochlea can impede thesurvival or cytodifferentiation of theafferent neurons (cochlear branch)and can explain this combination ofmalformations. The absence of thecochlear branch was initially over-
Radiology . 779

d. e,
with hypoplasia of its cochlear branch in the presence oÍ a normal laby-tained through the upper part of the left internal auditory canal. The;een parallel to one another in the upper part of the internal auditoryd) and posterior (sma1l arrow) semicircular canals F : flocculus. (b) Axialte part of the left internal auditory canal The facial nerve can be Íol-
ls), and the common VCN (large white arrows) is still visible in the in-een in the cochlea (black arrow), the lateral semicircular canal (whitehe vestibule (y).F : flocculus (c) Axial 0.7-mm-thick 3DFT-CISS imagenal auditorv canal. The facial nerve (arrowhead) and the common VCN
'made iust above the f loor of the in iernal audi tory canal . A very th inr the internal auditory canal, compatible with a hypoplastic cochlear, posterior semicircular canal (small white arrow), and vestibule (V).F =
pendicular to the course of the nerves at the level of the left cerebello-rerve (arrowhead). This is a normal finding at this site, and therefore no= posterior (e) Parasagittal 3DFT-CISS reconstruction image obtainedI of the left internal auditory canal. Only two nerves, the facial nerverchlear branch, normally already visible at this site, is absent. Á : ante-rined perpendicular to the course of the nerves at the level of the lateralauditory canal, the facial nerve (arrowhead) is seen in its normal posi-lar nerve (thick white arrow) is seen instead of two separate branchesr branch (thin white arrow) is depicted. Deep in the internal auditoryze always remains close to the size of the facial nerve in normal inner
ears. This is not the case in this patient. Moreover, the diameter of the cochlear branch oÍ the opposite normal inner ear was larger than the
diameter of the facial nerve (noï shown). This finding suppoÍts the diagnosis of a hypoplastic cochlear branch of the VCN Á : anterior, P :
posterior, black al1,ow = high-signal-intensity intralabyrinthine fluid in the cochlea.
looked on the axial MR images of oneoÍ these patients (patient 3), and atthat time, parasagittal reconstructionimages were not made. The diagnosiswas made only several months laterwhen the images were reviewed for astudy on congenital malformations. Inthe meantime, electric stimulation ofthe left ear had elicited clear subjec-tive hearing sensation, and as a conse-quence, the ear surgeon (F.E.O.) placeda cochlear implant (LAURA; AntwerpBionic Systems, Antwerp, Belgium) intothe inferior part of the common cavlty,which looked like a basal tum oÍ thecochlea (Fig c). The postoperativeelectroaudiogram was within the nor-mal range and stable throughout the6-month postoperative period/ andthe child showed clear signs of audi-tory progress (voice control, auditorybehavior). The most probable expla-nation or hypothesis is that the singlecommon VCN probably carries somefibers projecting into the auditory cor-tex. These results make it, of course,
780. Radiology
difficult to make a decision in the sec-ond patient (patient 4), with similarmalformations on both sides and bi-lateral stenoses of the internal audi-tory canal. The results of the electricpromontory stimulation can guide thesurgeon, and in the future, functionalMR imaging of the auditory cortexmight become the technique of choice.Only this imaging modality has thepotential to demonstrate whether;'cochlear fibers" connect an abnormallabyrinth with the brain stem and au-ditory cortex, even in the absence of acochlear branch of the VCN.
Type 2B: type 2 in patients with a nor-mal labyrinth.-Three patients pre-sented with completely normal laby-rinths and internal auditory canals.The axial and parasagittal gradient-echo images showed an absent co-chlear branch oÍ the VCN in two pa-tients (patients 5 and 6), and in thesepatients, the common vestibularnerve could be followed to the fundusof the internal auditory canal without
a clear bifurcation or a very late (notvisible on MR images due to partialvolume effect with the fundus) bifur-cation in a superior and inferior ves-tibular nerve (Fig 5). In a third pa-tient (patientT), a very thin cochlearbranch could be seen on the axial andparasagittal gradient-echo images (Fig6). In these three patients, a distur-bance in the trophic effect (nervegrowth factor) that the cochlea exertson the cochlear neurones could onceagain explain the hypoplasia or com-plete absence of the cochlear branchof the VCN. Of course, these findingshad no clinical consequences as thesethree patients had a normal function-ing contralateral ear; nevertheless, theMR findings correlated well with theunilateral hearing loss. However, inpatients with normal labyrinths andbilateral aplasias oÍ the cochlearbranchoÍ the VCN, electric promontory stimu-lation and/or functional MR imagingshould be used as a selection tool forcochlear implant candidacy.
March 1997

The absence of the cochlear branchcan be recognized on thin-section gra-dient-echo images, although onceagain parasagittal reconstruction im-ages are mandatory to confirm thefindings seen on the axial images. Thedanger exists that the cochlear branchlies adiacent to the floor of the inter-nal auditory canal and is thereforenot seen on the axial gradient-echoimages due to partial volume effects.The parasagittal plane is better suitedto study this region and can be usedto exclude partial volume effects. Thediagnosis of hypoplasia of the co-chlear branch is more difficult. Inthree of the 20 normal inner ears, thecochlear branch of the VCN inside theinternal auditory canal was smallerthan the facial nerve. But even inthese cases, the diameters of bothnerves were nearly the same. In pa-tientT, the diameter of the cochlearbranch was much smaller than thediameter oÍ the facial nerve, whereason the opposite normal side the co-chlear branch was much larger thanthe facial nerve.
Tvpe 3?: Presence of a Common VCNuííth aplasia or Hypoplasia of theVestibular Branchks)
Theoretically, a third type of VCNaplasia or hypoplasia with only ab-sence of the vestibular branches butwith a normal cochlear branch couldbe conceived. To our knowledge,such a type of VCN malformation hasnot yet been detected on MR images.Since the vestibule develops at an ear-l ier stage than the cochlea, one mayexpect that a vestibular malformationwill always lead to an associated co-
chlear malformation. In such a case, atype 1 aplasia would be the result.Therefore, the authors speculate thatan isolated aplasia of the vestibularbranch or type 3 aplasia of the VCNmay not exist. I
References1 Mark AS, Seltzer S, Nelson-Drake J, Chap-
man JC, Fitzgerald DC, Gulya AJ Laby-rinthine enhancement on Gd-MRI in pa-
4.
tients with sudden deaÍness and vertiso:correlat ion wi th audiologic and electrónys-tagmographic studies Ann Otol RhinolLaryngol 1,992; 107 :459 464Mark AS, Fitzgerald D Segmental en-hancement of the cochlea on contrast-en-hanced MR: correlation with the frequencvof hear ing loss and possible s ign of p-er i -lymphatic fistula and autoimmune labyrin-thitis AJNR 1993;1.4:991. 996MarkAS Contrast-enhancedmagneticresonance imaging of the temporal boneNeuroimaging Clin North Am 1.994;4:1,17-1.31..Casselman IW, Kuhweide R, Dehaene I,Ampe W, Devlies F Magnetic resonanceexamination of the inner ear and cerebello-pontine angle in patients with vertigoand/or abnormal findings at vestibulartesting Acta Otolaryngol 1994; 513(suppl):1.5,27Casselman JW Temporal bone imaging.Neuroimaging Clin North Am 1.996;6:265-289Casselman JW, Kuhweide R, Ampe, et alInner ear malÍormations in patients withsensorineural hearins loss: detection withgradient-echo (3DFT-CISS) MRI Neurora-diolo gy 79 9 6 ; 38 :27 8-28 6Klein HM, Bohndorf K, Hermes H, et alComputed tomography and magnet icresonance imaging in the preoperativework-up for cochlear implantation Eur JRadiol 1992; 1,5:89-92Marsot-Dupuch kl, Meyer B. Imagerie desimplants cochléaires In: Bourjat P, VeillonF, eds Imagerie radiologique tête et cou.1st ed Paris, France: Editions Vigot,1995;L47-1.59.Harnsberger HR, Dart Dl, Parkin JL,Smoker WRK, Osborn AG Cochlear im-plant candidates: assessment with CT andMR imaging Radiology L987; L64:53-57Casselman JW, Kuhweide R, Deimling M,Ampe W, Dehaene I, Meeus L. Construc-tive interference in steady state-3DFT MRimaging of the inner ear and cerebellopon-tine angle. AJNR 1993; 14:47-57
Schmalbrock P, Brogan MA, Chakeres DW,Hacker VA, Ying K, Clymer BD. Optimi-zation of submillimeter-resolution MR im-aging methods for the inner ear JMRI1993;3:451459Tien RD, Felsberg GJ, MacÍall J Threedimensional MR gradient recalled echoimaging of the inner ear: cornparison ofFID and echo imaging techniques JMRI1993;1.1.:429435Tanioka H, Shirakawa T, Machida T, SasakiY Three-dimensionalreconstructedMRimaging of the inner ear Radiology 1991;178:1.41.-1.44Tien R, Felsberg GJ, Macfall J Fast spin-echo high-resolution MR imaging of theinner ear AIR 1992; 159:395-398Hemond SG, Delanty FJ Formation ofthe cochlea in the chicken embryo: se-quence of inneruation and localization ofbasal lamina-associated molecules BrainRes Dev Brain Res 1991; 61:87-90Pujol R, Lavigne-Rebillard M, Uziel ADevelopment of the cochlea Acta Oto-laryngól Suppl (Stockh) 199L; 482:7 -1'2Lefebvre PP, Weber T, Rigo JM, et al. In-teractions neuronotrophiques dans 1'oreilleinterne en développement Acta Otorhino-laryngol Belg 1989 ; 43 : 403409Lefebvre PP, Leprince P, Weber T, Rigo JM,Delree P, Moonen G. Neuronotrophiceffect of developing otic vesicle on cochleo-vestibular neurons: evidence for nervegrowth factor involvement, Brain Res 1990;507:254260Van De Water TR Effects of removal ofthe statoacoustic ganglion complex uponthe growing otocyst Ann Otol RhinolLaryngol 1976;85:L31.Jackler RK Luxford \AtrM, House \ÁIF.Consenital malÍormations of the inner ear:a c la is i f icat ion based on embryogenesisLaryngoscope 1.987 ; 97 :2-74
11.
13
t4
15z.
t2
t7
3I6
18
5t9
20.
10
Volume 202 . Number 3 Radiology . 781