Embed Size (px)
Citation preview
769© Springer Science+Business Media, LLC 2016E.I. Traboulsi, V. Miraldi Utz (eds.), Practical Management of Pediatric Ocular Disorders and Strabismus, DOI 10.1007/978-1-4939-2745-6
Appendix 1: Prescribing Practices for Refractive Errors in Pediatric Patients
Virginia Miraldi Utz
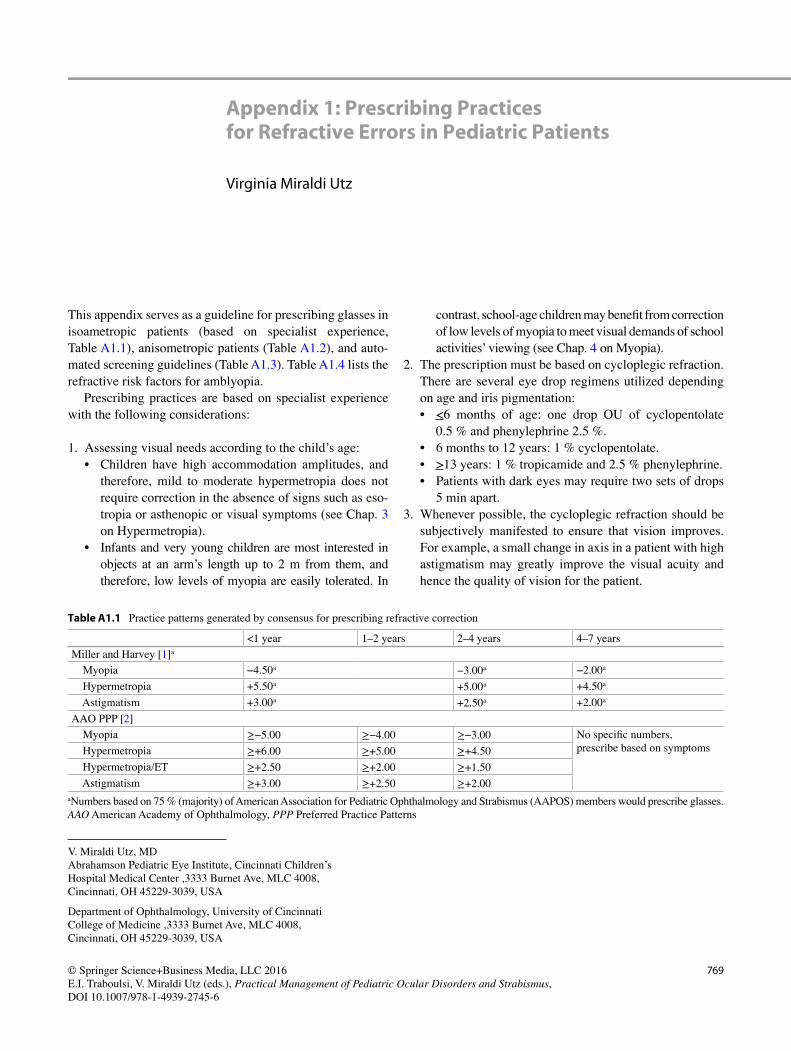
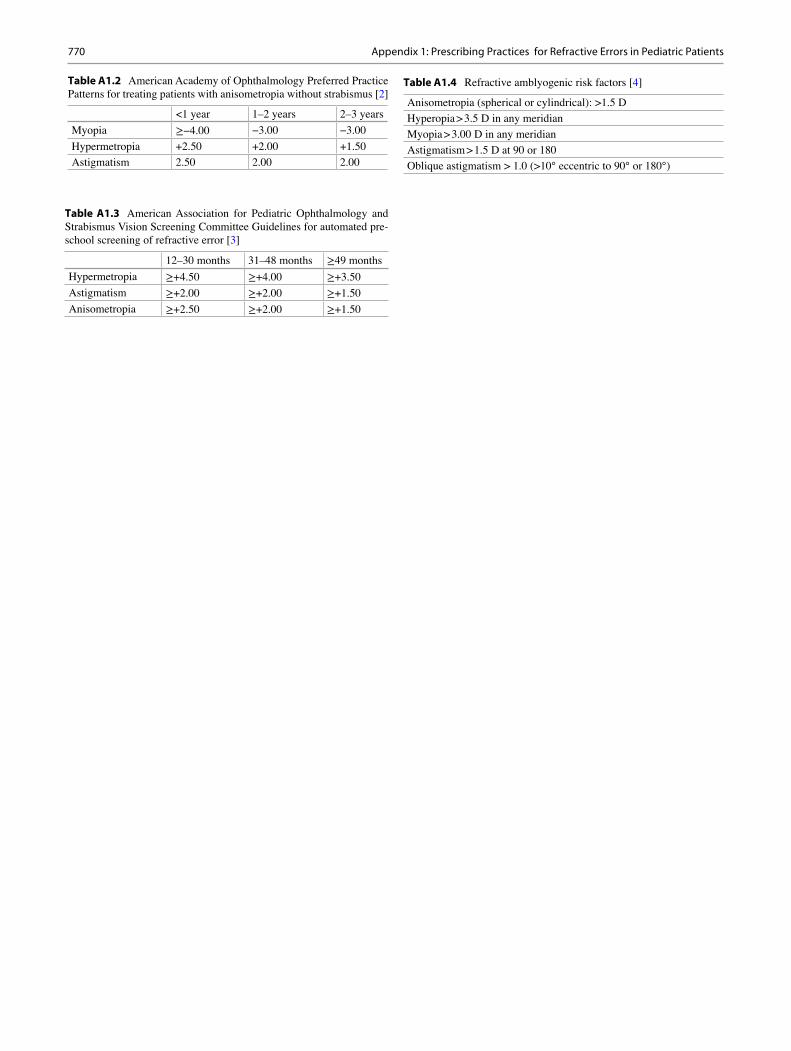
This appendix serves as a guideline for prescribing glasses in isoametropic patients (based on specialist experience, Table A1.1 ), anisometropic patients (Table A1.2 ), and auto-mated screening guidelines (Table A1.3 ). Table A1.4 lists the refractive risk factors for amblyopia.
Prescribing practices are based on specialist experience with the following considerations:
1. Assessing visual needs according to the child’s age:• Children have high accommodation amplitudes, and
therefore, mild to moderate hypermetropia does not require correction in the absence of signs such as eso-tropia or asthenopic or visual symptoms (see Chap. 3 on Hypermetropia).
• Infants and very young children are most interested in objects at an arm’s length up to 2 m from them, and therefore, low levels of myopia are easily tolerated. In
contrast, school-age children may benefi t from correction of low levels of myopia to meet visual demands of school activities’ viewing (see Chap. 4 on Myopia).
2. The prescription must be based on cycloplegic refraction. There are several eye drop regimens utilized depending on age and iris pigmentation:• < 6 months of age: one drop OU of cyclopentolate
0.5 % and phenylephrine 2.5 %. • 6 months to 12 years: 1 % cyclopentolate. • > 13 years: 1 % tropicamide and 2.5 % phenylephrine. • Patients with dark eyes may require two sets of drops
5 min apart. 3. Whenever possible, the cycloplegic refraction should be
subjectively manifested to ensure that vision improves. For example, a small change in axis in a patient with high astigmatism may greatly improve the visual acuity and hence the quality of vision for the patient.
V. Miraldi Utz, MD Abrahamson Pediatric Eye Institute, Cincinnati Children’s Hospital Medical Center , 3333 Burnet Ave, MLC 4008 , Cincinnati , OH 45229-3039 , USA
Department of Ophthalmology , University of Cincinnati College of Medicine , 3333 Burnet Ave, MLC 4008 , Cincinnati , OH 45229-3039 , USA
Table A1.1 Practice patterns generated by consensus for prescribing refractive correction
<1 year 1–2 years 2–4 years 4–7 years
Miller and Harvey [ 1 ] a
Myopia −4.50 a −3.00 a −2.00 a
Hypermetropia +5.50 a +5.00 a +4.50 a
Astigmatism +3.00 a +2.50 a +2.00 a
AAO PPP [ 2 ]
Myopia ≥−5.00 ≥−4.00 ≥−3.00 No specifi c numbers, prescribe based on symptoms Hypermetropia ≥+6.00 ≥+5.00 ≥+4.50
Hypermetropia/ET ≥+2.50 ≥+2.00 ≥+1.50
Astigmatism ≥+3.00 ≥+2.50 ≥+2.00
a Numbers based on 75 % (majority) of American Association for Pediatric Ophthalmology and Strabismus (AAPOS) members would prescribe glasses. AAO American Academy of Ophthalmology, PPP Preferred Practice Patterns
770
Table A1.2 American Academy of Ophthalmology Preferred Practice Patterns for treating patients with anisometropia without strabismus [ 2 ]
<1 year 1–2 years 2–3 years
Myopia ≥−4.00 −3.00 −3.00
Hypermetropia +2.50 +2.00 +1.50
Astigmatism 2.50 2.00 2.00
Table A1.3 American Association for Pediatric Ophthalmology and Strabismus Vision Screening Committee Guidelines for automated pre-school screening of refractive error [ 3 ]
12–30 months 31–48 months ≥49 months
Hypermetropia ≥+4.50 ≥+4.00 ≥+3.50
Astigmatism ≥+2.00 ≥+2.00 ≥+1.50
Anisometropia ≥+2.50 ≥+2.00 ≥+1.50
Table A1.4 Refractive amblyogenic risk factors [ 4 ]
Anisometropia (spherical or cylindrical): >1.5 D
Hyperopia > 3.5 D in any meridian
Myopia > 3.00 D in any meridian
Astigmatism > 1.5 D at 90 or 180
Oblique astigmatism > 1.0 (>10° eccentric to 90° or 180°)
Appendix 1: Prescribing Practices for Refractive Errors in Pediatric Patients

771© Springer Science+Business Media, LLC 2016E.I. Traboulsi, V. Miraldi Utz (eds.), Practical Management of Pediatric Ocular Disorders and Strabismus, DOI 10.1007/978-1-4939-2745-6
Appendix 2: Strategies for the Child Who Would Not Wear Glasses
Sarah L. Lopper
In this appendix, we explore possible causes of intolerance to glasses. We will look for possible errors related to the pre-scription, the manufacturing of the lenses, or the fi t of the frame. We will also consider issues related to behavior or intolerance to foreign objects on the child’s face. Finally we will explore errors related to the initial examination and orig-inal prescription.
I. The Prescription Is Not Accurate or There Is an Optical Problem with the Lenses
1. Step 1: Examine the optics of the glasses.• Verify that the lenses were made as prescribed: Optical
labs grind lenses in minus cylinder format, and it is possible that the glasses prescription was transposed incorrectly if it was written in plus cylinder format.
• Use a lensometer to measure the glasses prescription and confi rm it was made as prescribed.
Clinical Skill: Nonautomated Lensometry • Step 1. Place the lens on the lensometer. Secure after fi nd-
ing the intersection of both sets of lines, and place this in the center of the lensometer eyepiece view.
• Step 2. Turn the power wheel back and forth to focus each set of lines. If both sets of lines are in focus at the same time (the single thicker lines and the set of three striped lines), then there is no cylinder present and the lens is spherical power only.
• Step 3. If each set of lines is best focused at a different posi-tion on the power wheel, then there is cylinder present to correct for astigmatism. Focus each set separately, and adjust/determine the axis so the lines are exactly straight.
• Step 4. Note power of best focus; the least plus/most- minus set of lines is the sphere and the difference in power strength until the next set of lines is in focus is the amount of cylinder (astigmatism) in the lens if you are document-ing in plus-cylinder format.
Clinical Skill: Lens Transposition from Plus to Minus Cylinder • Step 1. Add the sphere and cylinder together to get the
new spherical power. • Step 2. Change the sign of the cylinder (+ becomes − and
− becomes +); do not change the amount of the cylinder. • Step 3. Change the axis by 90°. • Example 1: +3.25 + 2.50 × 135 in plus cylinder format
becomes +5.75−2.50 × 045 in minus cylinder format. • Example 2: +3.25−2.50 × 135 in minus cylinder format
becomes +0.75 + 2.50 × 045 in plus cylinder format.
2. Step 2: Verify that the lens is well centered in front of the child’s visual axis.• The optical center of the lens is the point on the principle
axis of the lens through which light passes undeviated, and this should be aligned with the patient’s visual axis.
• The optical center of the lens can be measured and marked with a lensometer. Find the intersection of the two sets of lines in the center of the lensometer eye-piece view, and use the self-recoiling lens marker to make a dot on the lens center.
• Place the glasses on the patient and determine if the mark matches the center of their pupils. If there is sig-nifi cant horizontal or vertical displacement, the child may not be seeing well because of an induced pris-matic effect, especially in higher prescriptions. – Prentice’s law applies to the amount of induced
prism: P = dF where P is the prism power in Δ, d is dis-
placement in centimeters, and F is the refracting power of the lens
S. L. Lopper, O.D. Department of Ophthalmology, University of Cincinnati College of Medicine , 3333 Burnet Ave , Cincinnati , OH , USA
772
3. Step 3: Consider distortions related to polycarbonate material:• The Abbe value (range 20–60) describes the amount of
chromatic aberration of lens materials and is intrinsic to the specifi c refractive index of the lens material [ 5 ]. Lower Abbe values have more aberrations (spherical aberration, coma, marginal astigmatism, curvature of fi eld, and distortion) and are most pronounced with increasing distances from the center of the lens. Aberrations are more signifi cant in higher plus or minus lenses. – Polycarbonate has an Abbe value of 30. – CR-39 and Crown glass have Abbe values of 58.
4. Step 4: Consider a defect in or an inappropriate base curve of the lens.• Measure base curve of the lenses with a lens clock.
They should be no steeper than 7 diopters or fl atter than 4 diopters in two primary meridians 90° apart.
• Lower number = fl atter base curve and higher num-ber = steeper base curve.
• Patients may prefer their “old” glasses with a different base curve than the “new” glasses. Matching previous base curve can help.
5. Step 5: Consider aniseikonia in patients with signifi cant anisometropia.• This can be corrected with base curve adjustments or
contact lenses.
II. The Glasses Are Not Manufactured Well or Are Not Fitting Well
• When glasses are fi tted, several measurements are taken to ensure a proper fi t. If there are deviations from these initial fi tting measurements, the effective power of the lenses may change and affect visual acuity, or the child may complain of asthenopia. – Vertex distance : The posterior surface of lenses should
generally be 12–15 mm from the corneal plane. This becomes especially signifi cant when lens power is above 5–6 diopters.
Increasing vertex distance
Makes a “plus” lens more “plus”
Makes a “minus” lens less “minus”
Decreasing vertex distance
Makes a “plus” lens less “plus”
Makes a “minus” lens more “minus”
– Pantoscopic tilt: The angle of tilt of the lower rim of the glasses frame toward the cheek. A normal amount of
pantoscopic tilt is approximately 10° (±5°). This is taken into account when the frame is fi tted. For every 2° of pantoscopic tilt, the optical center is lowered 1 mm [ 6 ]. Companies make tools to measure pantoscopic tilt, or
you can simply use a protractor. Place the vertical straight edge of the protractor parallel to the fl oor. The pantoscopic tilt is the angle that is made between the lens and the temple when the 90° mark is aligned with the temple.
– Face form : the wrap of the frame around the face. If there is too much face form or unequal face form for the right and left lenses, the patient will not be looking through the optical center of the lens and the vertex distance is affected.
• Poorly fi tting frames: – Frames that are too tight on a child’s cheeks or those
that pinch behind their ears will not be comfortable. – Nose pads that are not adjusted appropriately or miss-
ing will be uncomfortable.
III. Behavioral Issues
• Behavioral problems of the child may limit success with glasses.
• Sometimes children just do not like the color or style of their frames anymore or they do not want to wear them anymore due to peer pressure from classmates.
• In addition, some patients with Down syndrome or pedi-atric patients with sensory integration disorders such as autism spectrum disorder may have diffi culty adjusting to glasses.
• Discuss with a co-managing occupational therapist to see if the glasses can be integrated into their therapy session or look for additional strategies that might increase compliance.
IV. There Is a Change in the Child’s Refraction, a Binocular Vision Disorder, or a New or Previously Undetected Eye Problem
• Repeat the cycloplegic refraction and subjectively mani-fest if the patient is able.
• Consider cycloplegic eye drops to help the child adjust/accept the hyperopic correction.
• Rule out a binocular vision disorder or accommodative dysfunction.
• Perform a dilated eye exam to rule out ocular health changes.
Appendix 2: Strategies for the Child Who Would Not Wear Glasses

773© Springer Science+Business Media, LLC 2016E.I. Traboulsi, V. Miraldi Utz (eds.), Practical Management of Pediatric Ocular Disorders and Strabismus, DOI 10.1007/978-1-4939-2745-6
Appendix 3: Prescribing Prisms for Pediatric Patients
Sarah L. Lopper
Goals of Prismatic Correction
• Restore binocularity and/or fusion • Relieve or eliminate diplopia • Alleviate abnormal head position • Relieve asthenopic symptoms
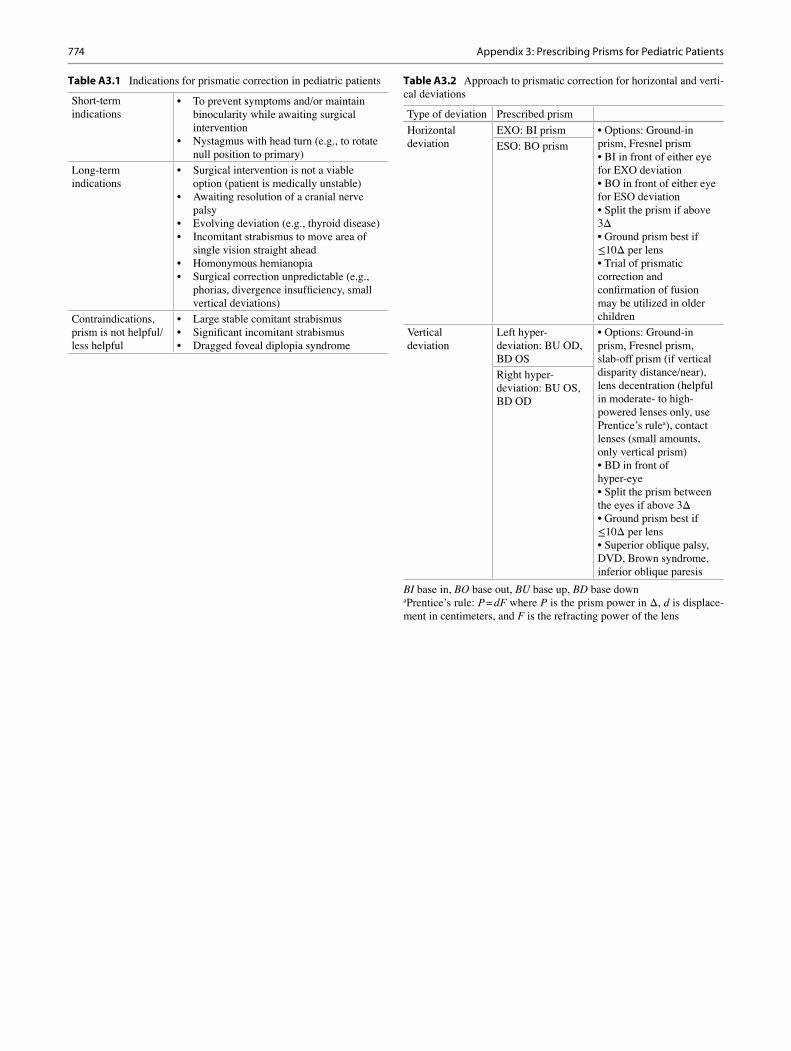
Steps for Determining and Prescribing Prismatic Correction (Table A3.2 )
(1) Always correct refractive error fi rst. Perform a cyclople-gic refraction with subjective manifest whenever possible.
(2) Prismatic correction is best tolerated with smaller angle and comitant strabismus.
(3) Perform a prism adaptation trial for 20–30 min. (4) Demonstrate effectiveness fi rst with Fresnel prism prior
to grinding into the lens. (5) If there is both a vertical and a horizontal deviation,
determine fi rst if the vertical deviation is the primary or secondary deviation. If it is the primary deviation, address the vertical deviation fi rst.
(6) Larger amounts of prism add to lens thickness and weight, cause image distortions, and give the lens a poor appearance. Smaller lens, eye size, high index lens mate-rial, antirefl ective coating, and lens edge treatments can all improve prism lens appearance [ 8 ]. As a general guideline, 1Δ adds 1 mm of lens thickness [ 9 ].
(7) Fresnel prism is available up to 40Δ, but prisms larger than 8–10Δ start having a poorer optical quality and will cause increased refl ections and a decrease in visual acu-ity and contrast sensitivity. Use on the non-dominant eye, Fresnel lenses change color over time.
(8) Sector Fresnel prism can be applied to just a portion of the lens (e.g., “A” or “V” pattern deviations, non- comitant strabismus, hemianopic visual fi eld loss).
(9) Consider prism in the following cases (Table A3.1 ):• Blow out fracture (Fresnel) • Nystagmus (place null point in primary position) • After retinal surgery (if small-angle strabismus and/
or anisometropia with diplopia) • Sixth nerve palsy (adjusting Fresnel prism as angle
changes) • Thyroid disease [ 10 ] (Table A3.2 )
S. L. Lopper, O.D. Department of Ophthalmology , University of Cincinnati College of Medicine , 3333 Burnet Ave , Cincinnati , OH 45299 , USA
774
Table A3.1 Indications for prismatic correction in pediatric patients
Short-term indications
• To prevent symptoms and/or maintain binocularity while awaiting surgical intervention
• Nystagmus with head turn (e.g., to rotate null position to primary)
Long-term indications
• Surgical intervention is not a viable option (patient is medically unstable)
• Awaiting resolution of a cranial nerve palsy
• Evolving deviation (e.g., thyroid disease) • Incomitant strabismus to move area of
single vision straight ahead • Homonymous hemianopia • Surgical correction unpredictable (e.g.,
phorias, divergence insuffi ciency, small vertical deviations)
Contraindications, prism is not helpful/less helpful
• Large stable comitant strabismus • Signifi cant incomitant strabismus • Dragged foveal diplopia syndrome
Table A3.2 Approach to prismatic correction for horizontal and verti-cal deviations
Type of deviation Prescribed prism
Horizontal deviation
EXO: BI prism • Options: Ground-in prism, Fresnel prism • BI in front of either eye for EXO deviation • BO in front of either eye for ESO deviation • Split the prism if above 3Δ • Ground prism best if ≤10Δ per lens • Trial of prismatic correction and confi rmation of fusion may be utilized in older children
ESO: BO prism
Vertical deviation
Left hyper-deviation: BU OD, BD OS
• Options: Ground-in prism, Fresnel prism, slab-off prism (if vertical disparity distance/near), lens decentration (helpful in moderate- to high-powered lenses only, use Prentice’s rule a ), contact lenses (small amounts, only vertical prism) • BD in front of hyper-eye • Split the prism between the eyes if above 3Δ • Ground prism best if ≤10Δ per lens • Superior oblique palsy, DVD, Brown syndrome, inferior oblique paresis
Right hyper-deviation: BU OS, BD OD
BI base in, BO base out, BU base up, BD base down a Prentice’s rule: P = dF where P is the prism power in Δ, d is displace-ment in centimeters, and F is the refracting power of the lens
Appendix 3: Prescribing Prisms for Pediatric Patients
775© Springer Science+Business Media, LLC 2016E.I. Traboulsi, V. Miraldi Utz (eds.), Practical Management of Pediatric Ocular Disorders and Strabismus, DOI 10.1007/978-1-4939-2745-6
Appendix 4: Pathogens and Medications for Infectious Conjunctivitis in Children
Alison E. Smith
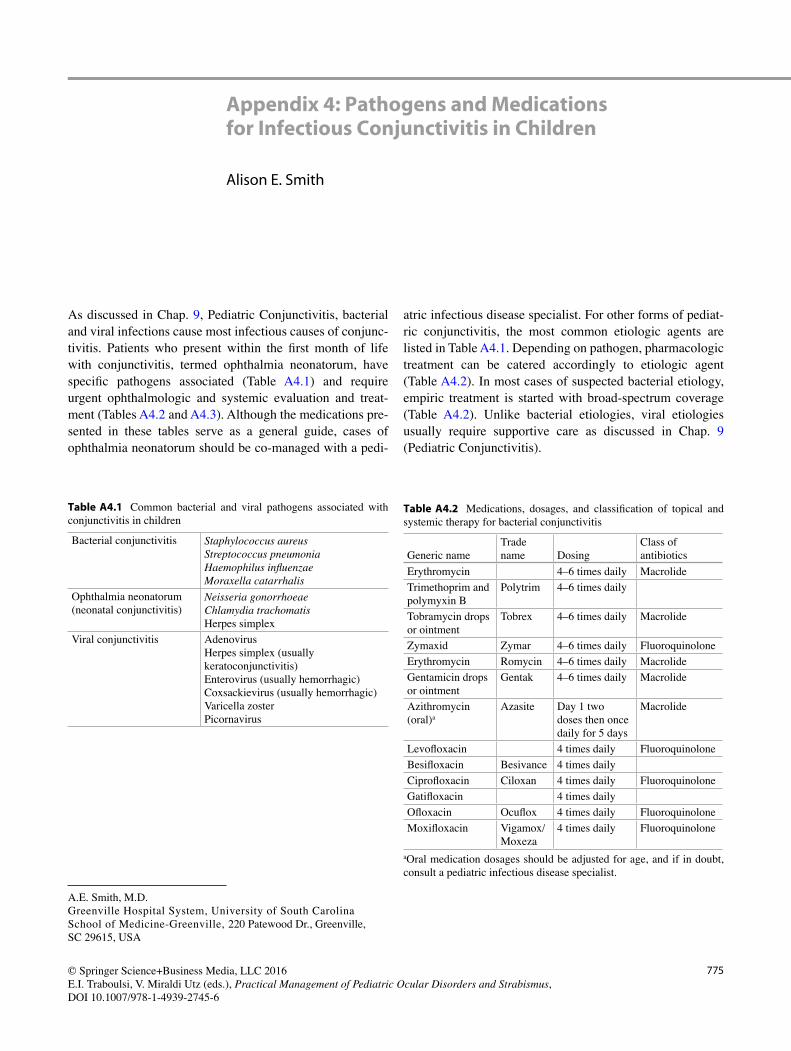
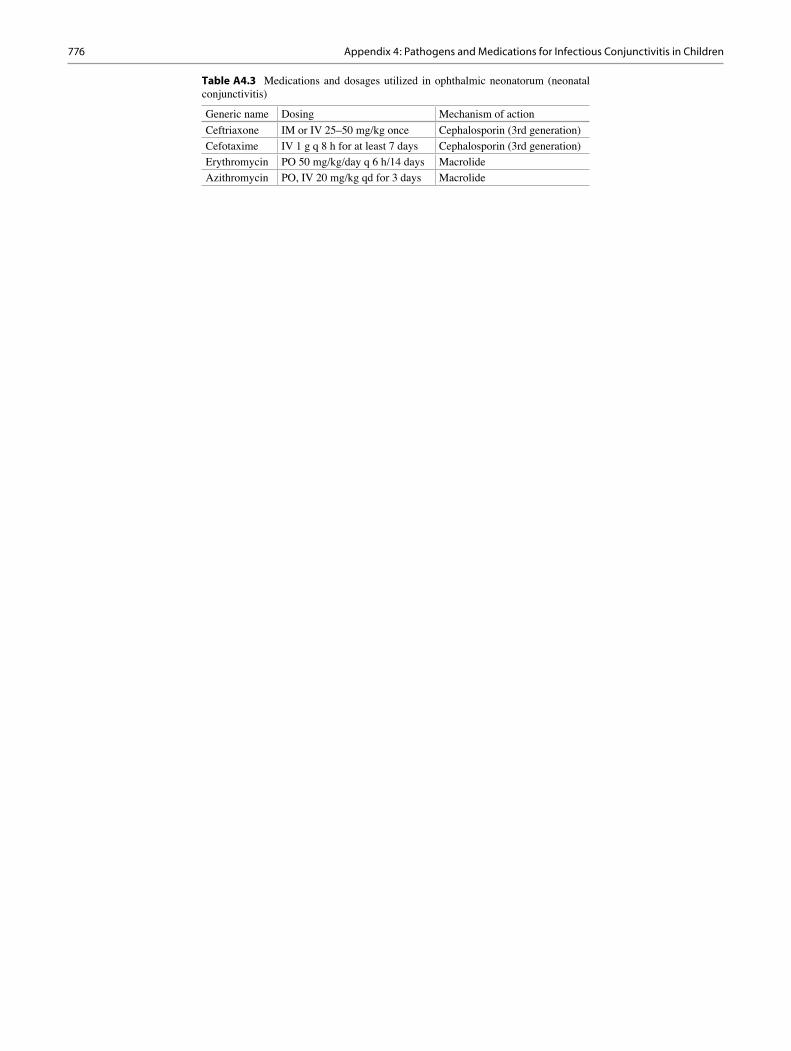
As discussed in Chap. 9 , Pediatric Conjunctivitis, bacterial and viral infections cause most infectious causes of conjunc-tivitis. Patients who present within the fi rst month of life with conjunctivitis, termed ophthalmia neonatorum, have specifi c pathogens associated (Table A4.1 ) and require urgent ophthalmologic and systemic evaluation and treat-ment (Tables A4.2 and A4.3 ). Although the medications pre-sented in these tables serve as a general guide, cases of ophthalmia neonatorum should be co-managed with a pedi-
atric infectious disease specialist. For other forms of pediat-ric conjunctivitis, the most common etiologic agents are listed in Table A4.1 . Depending on pathogen, pharmacologic treatment can be catered accordingly to etiologic agent (Table A4.2 ). In most cases of suspected bacterial etiology, empiric treatment is started with broad-spectrum coverage (Table A4.2 ). Unlike bacterial etiologies, viral etiologies usually require supportive care as discussed in Chap. 9 (Pediatric Conjunctivitis).
A. E. Smith, M.D. Greenville Hospital System, University of South Carolina School of Medicine-Greenville , 220 Patewood Dr. , Greenville , SC 29615 , USA
Table A4.1 Common bacterial and viral pathogens associated with conjunctivitis in children
Bacterial conjunctivitis Staphylococcus aureus Streptococcus pneumonia Haemophilus infl uenzae Moraxella catarrhalis
Ophthalmia neonatorum (neonatal conjunctivitis)
Neisseria gonorrhoeae Chlamydia trachomatis Herpes simplex
Viral conjunctivitis Adenovirus Herpes simplex (usually keratoconjunctivitis) Enterovirus (usually hemorrhagic) Coxsackievirus (usually hemorrhagic) Varicella zoster Picornavirus
Table A4.2 Medications, dosages, and classifi cation of topical and systemic therapy for bacterial conjunctivitis
Generic name Trade name Dosing
Class of antibiotics
Erythromycin 4–6 times daily Macrolide
Trimethoprim and polymyxin B
Polytrim 4–6 times daily
Tobramycin drops or ointment
Tobrex 4–6 times daily Macrolide
Zymaxid Zymar 4–6 times daily Fluoroquinolone
Erythromycin Romycin 4–6 times daily Macrolide
Gentamicin drops or ointment
Gentak 4–6 times daily Macrolide
Azithromycin (oral) a
Azasite Day 1 two doses then once daily for 5 days
Macrolide
Levofl oxacin 4 times daily Fluoroquinolone
Besifl oxacin Besivance 4 times daily
Ciprofl oxacin Ciloxan 4 times daily Fluoroquinolone
Gatifl oxacin 4 times daily
Ofl oxacin Ocufl ox 4 times daily Fluoroquinolone
Moxifl oxacin Vigamox/Moxeza
4 times daily Fluoroquinolone
a Oral medication dosages should be adjusted for age, and if in doubt, consult a pediatric infectious disease specialist.
776
Table A4.3 Medications and dosages utilized in ophthalmic neonatorum (neonatal conjunctivitis)
Generic name Dosing Mechanism of action
Ceftriaxone IM or IV 25–50 mg/kg once Cephalosporin (3rd generation)
Cefotaxime IV 1 g q 8 h for at least 7 days Cephalosporin (3rd generation)
Erythromycin PO 50 mg/kg/day q 6 h/14 days Macrolide
Azithromycin PO, IV 20 mg/kg qd for 3 days Macrolide
Appendix 4: Pathogens and Medications for Infectious Conjunctivitis in Children
777© Springer Science+Business Media, LLC 2016E.I. Traboulsi, V. Miraldi Utz (eds.), Practical Management of Pediatric Ocular Disorders and Strabismus, DOI 10.1007/978-1-4939-2745-6
Appendix 5: Medications Commonly Used in Allergic Conjunctivitis Treatment
Alison E. Smith
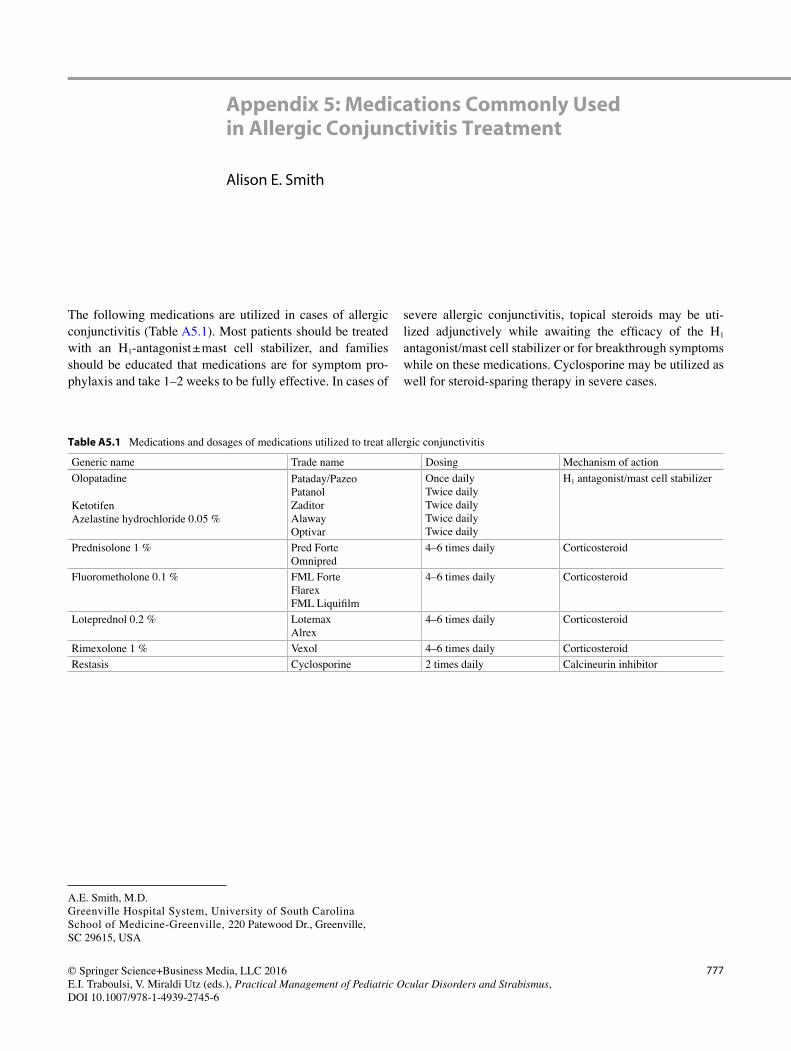
The following medications are utilized in cases of allergic conjunctivitis (Table A5.1 ). Most patients should be treated with an H 1 -antagonist ± mast cell stabilizer, and families should be educated that medications are for symptom pro-phylaxis and take 1–2 weeks to be fully effective. In cases of
severe allergic conjunctivitis, topical steroids may be uti-lized adjunctively while awaiting the effi cacy of the H 1 antagonist/mast cell stabilizer or for breakthrough symptoms while on these medications. Cyclosporine may be utilized as well for steroid-sparing therapy in severe cases.
A. E. Smith, M.D. Greenville Hospital System, University of South Carolina School of Medicine-Greenville , 220 Patewood Dr. , Greenville , SC 29615 , USA
Table A5.1 Medications and dosages of medications utilized to treat allergic conjunctivitis
Generic name Trade name Dosing Mechanism of action
Olopatadine
Ketotifen Azelastine hydrochloride 0.05 %
Pataday/Pazeo Patanol Zaditor Alaway Optivar
Once daily Twice daily Twice daily Twice daily Twice daily
H 1 antagonist/mast cell stabilizer
Prednisolone 1 % Pred Forte Omnipred
4–6 times daily Corticosteroid
Fluorometholone 0.1 % FML Forte Flarex FML Liquifi lm
4–6 times daily Corticosteroid
Loteprednol 0.2 % Lotemax Alrex
4–6 times daily Corticosteroid
Rimexolone 1 % Vexol 4–6 times daily Corticosteroid
Restasis Cyclosporine 2 times daily Calcineurin inhibitor

779© Springer Science+Business Media, LLC 2016E.I. Traboulsi, V. Miraldi Utz (eds.), Practical Management of Pediatric Ocular Disorders and Strabismus, DOI 10.1007/978-1-4939-2745-6
Appendix 6: IOL Power Selection for Children
Rupal H. Trivedi and M. Edward Wilson
R. H. Trivedi, M.D. • M. E. Wilson, M.D. Department of Ophthalmology , Miles Center for Pediatric Ophthalmology, Storm Eye Institute, Medical University of South Carolina , 167 Ashley Avenue, MSC 676 , Charleston , SC 29425-6760 , USA
780
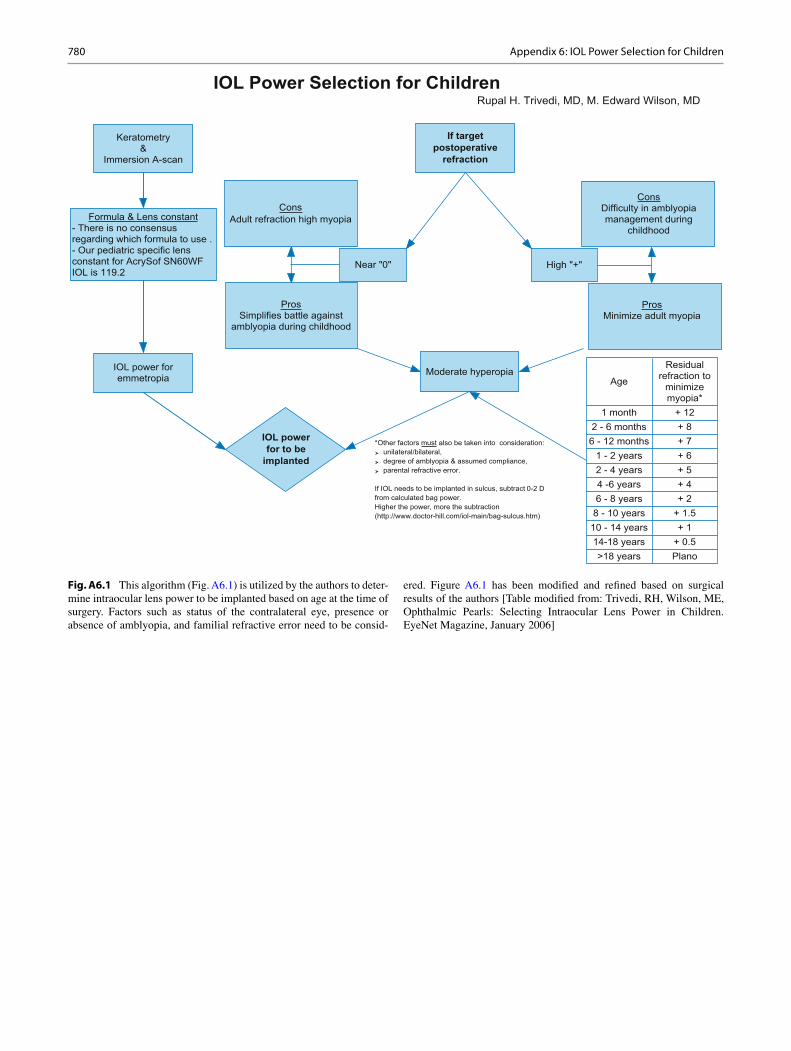
Fig. A6.1 This algorithm (Fig. A6.1 ) is utilized by the authors to deter-mine intraocular lens power to be implanted based on age at the time of surgery. Factors such as status of the contralateral eye, presence or absence of amblyopia, and familial refractive error need to be consid-
ered. Figure A6.1 has been modifi ed and refi ned based on surgical results of the authors [Table modifi ed from: Trivedi, RH, Wilson, ME, Ophthalmic Pearls: Selecting Intraocular Lens Power in Children. EyeNet Magazine, January 2006]
Appendix 6: IOL Power Selection for Children

781© Springer Science+Business Media, LLC 2016E.I. Traboulsi, V. Miraldi Utz (eds.), Practical Management of Pediatric Ocular Disorders and Strabismus, DOI 10.1007/978-1-4939-2745-6
Appendix 7: Measuring Axial Eye Length in Children
Fadia AlKhawaldeh
In order to determine the correct power for an intraocular lens implant, it is necessary to obtain axial eye length (AEL) and keratometric measurements on the patient. The tech-nique for obtaining these measurements varies depending on the age of the child and his or her physical ability to cooper-ate during testing.
For most children under the age of 6 or 7 years, a sedated immersion technique performed in the operating room prior to surgery or during a sedated eye exam is best. For children over the age of 7, the ultrasonographer is able to use his/her best judgment to assess the child’s ability to cooperate and to follow instructions. If the child is cooperative and able to follow directions, the instrument of choice is the IOL Master ® for accurate AEL and keratometric readings. If the child is uncooperative, combative, or unable to comprehend or fol-low verbal instructions, a sedated immersion technique is preferred.
Using IOL Master ® for Axial Eye Length Measurements
When attempting to measure AEL on a child, it’s important to ensure that the child understands fully what is about to take place. This will help alleviate any anxiety they may be experiencing due to the impending test, in addition to ensur-ing their best cooperation and efforts are put forth. To begin with, the ultrasonographer should explain to the patient and his or her parent/guardian what they are about to do in simple
terms so the child understands. Then instruct the patient to place his or her chin in the chin rest and focus on the central light. Playing games such as “statue” and staring contests help the child focus and make the test less intimidating. This not only ensures a more a more accurate measurement but the full cooperation of the child as well.
Sedated Immersion A-Scan
For infants, children under 7 years of age, and those who are combative or unable to follow directions, a sedated immer-sion A-scan is necessary in order to obtain the axial eye length and keratometric measurements required for IOL cal-culations. This procedure is typically performed under full anesthesia in an operating room environment.
Once the child has been fully inducted and sedated, the ultrasonographer begins by using a handheld keratometer to obtain corneal keratometric measurements for each eye. In order to ensure consistency and accuracy, three separate readings should be taken. Once the keratometric readings are obtained, a plastic scleral shell measuring between 16 and 20 mm is placed directly on the eye and fi lled with sterile saline solution. The saline solution acts as a medium for the A-scan sound waves to travel through. Next, the ultrasonog-rapher engages the machine using the foot pedal and obtains the requisite axial eye length measurements. Again, a mini-mum of three should be obtained to ensure accuracy. The procedure is repeated for the fellow eye, thus ensuring all measurements and calculations are complete for future sur-gical procedures when necessary. Additionally, this allows the ultrasonographer and surgeon to assess for any anatomi-cal differences between the eyes and adjust the calculations and treatments accordingly.
F. AlKhawaldeh, M.B.A., C.O.T., R.O.U.B. Department of Refractive Surgery , Cole Eye Institute, Cleveland Clinic , 9500 Euclid Avenue, Suite i-21 , Cleveland , OH 44195 , USA
782
At this point, the axial eye length measurements are com-plete, and the physician is able to determine the necessary lens power needed for the IOL implant (see Appendix 6).
If the surgeon’s view of the retina is obstructed due to the density of the cataract, he or she may request a B-scan to be performed at the same time. If a B-scan is required, the ultra-sonographer will then switch from the A-scan probe to the larger B-scan probe. A gel is used as a coupling agent on the
eye to allow for better sound wave penetration, and the ultra-sonographer will conduct a full sweep of the eye in all four quadrants and at the cardinal positions of 12, 3, 6, and 9 o’clock. If any abnormal fi ndings are observed, they are reported and their location is documented and addressed by the surgeon accordingly.
Appendix 7: Measuring Axial Eye Length in Children
783© Springer Science+Business Media, LLC 2016E.I. Traboulsi, V. Miraldi Utz (eds.), Practical Management of Pediatric Ocular Disorders and Strabismus, DOI 10.1007/978-1-4939-2745-6
Appendix 8: Surgical Instrumentation in Strabismus Surgery
Elias I. Traboulsi
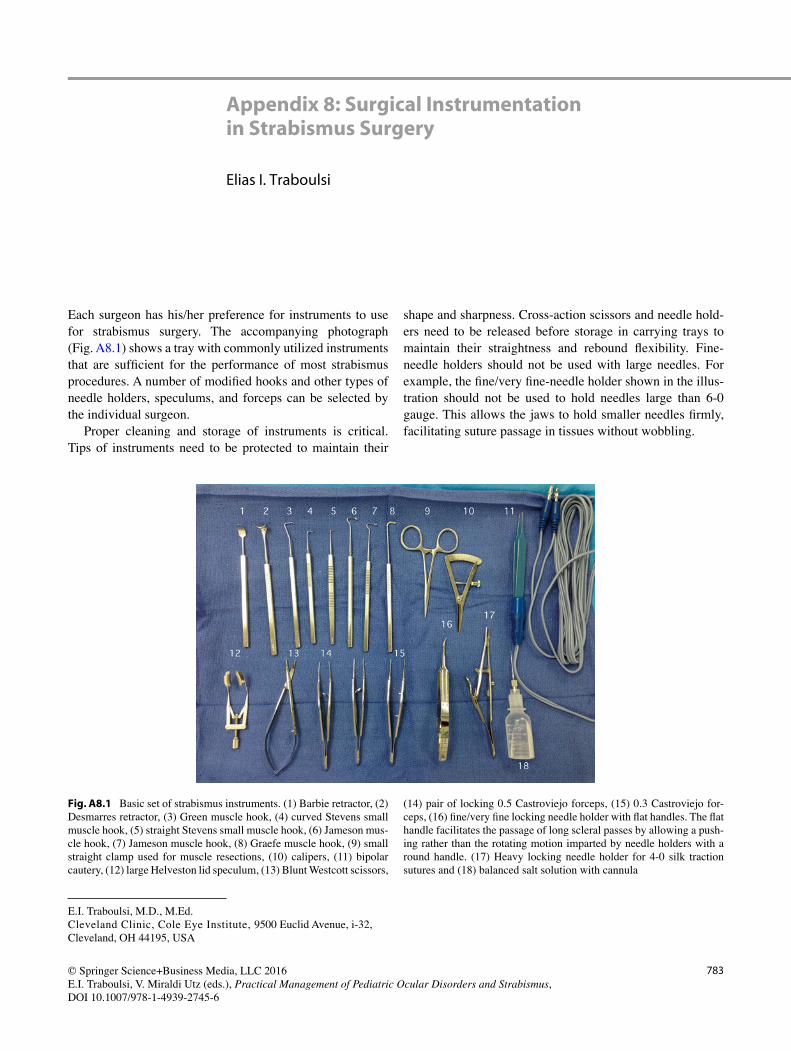
Each surgeon has his/her preference for instruments to use for strabismus surgery. The accompanying photograph (Fig. A8.1 ) shows a tray with commonly utilized instruments that are suffi cient for the performance of most strabismus procedures. A number of modifi ed hooks and other types of needle holders, speculums, and forceps can be selected by the individual surgeon.
Proper cleaning and storage of instruments is critical. Tips of instruments need to be protected to maintain their
shape and sharpness. Cross-action scissors and needle hold-ers need to be released before storage in carrying trays to maintain their straightness and rebound fl exibility. Fine- needle holders should not be used with large needles. For example, the fi ne/very fi ne-needle holder shown in the illus-tration should not be used to hold needles large than 6-0 gauge. This allows the jaws to hold smaller needles fi rmly, facilitating suture passage in tissues without wobbling.
E. I. Traboulsi, M.D., M.Ed. Cleveland Clinic, Cole Eye Institute , 9500 Euclid Avenue, i-32 , Cleveland , OH 44195 , USA
Fig. A8.1 Basic set of strabismus instruments. (1) Barbie retractor, (2) Desmarres retractor, (3) Green muscle hook, (4) curved Stevens small muscle hook, (5) straight Stevens small muscle hook, (6) Jameson mus-cle hook, (7) Jameson muscle hook, (8) Graefe muscle hook, (9) small straight clamp used for muscle resections, (10) calipers, (11) bipolar cautery, (12) large Helveston lid speculum, (13) Blunt Westcott scissors,
(14) pair of locking 0.5 Castroviejo forceps, (15) 0.3 Castroviejo for-ceps, (16) fi ne/very fi ne locking needle holder with fl at handles. The fl at handle facilitates the passage of long scleral passes by allowing a push-ing rather than the rotating motion imparted by needle holders with a round handle. (17) Heavy locking needle holder for 4-0 silk traction sutures and (18) balanced salt solution with cannula
785© Springer Science+Business Media, LLC 2016E.I. Traboulsi, V. Miraldi Utz (eds.), Practical Management of Pediatric Ocular Disorders and Strabismus, DOI 10.1007/978-1-4939-2745-6
Appendix 9: Surgical Planning and Numbers
Virginia Miraldi Utz and Elias I. Traboulsi
The following tables are based on the numbers recommended by Marshall M. Parks, M.D., and modifi ed by many [ 11 , 12 ]. While they have been used to plan pediatric and adult cases, it is unclear if they have been derived from cases performed in either or both groups. We do not address the issue of oper-ating on three horizontal muscles to treat large- angle devia-tions. We prefer operating on two muscles and addressing the residual deviation, if any, afterward using the two unop-erated horizontal muscles. We do not address the topic of adjustable suture use in this appendix.
Horizontal Strabismus Surgery
Esotropia
1. Binocular Surgery
Medial rectus recession Lateral rectus resection a
15 PD = 3.0 mm 20 PD = 3.5 mm 25 PD = 4.0 mm 30 PD = 4.5 mm 35 PD = 5.0 mm 40 PD = 5.5 mm 50 PD = 6.0 mm 60 PD = 6.5 mm 70 PD = 7.0 mm
15 PD = 3.5 mm 20 PD = 4.5 mm 25 PD = 5.5 mm 30 PD = 6.0 mm 35 PD = 6.5 mm 40 PD = 7.0 mm 50 PD = 8.0 mm
a If a large medial rectus recession has been performed (>6.0 mm) and bilateral lateral rectus resection is planned for residual esotropia, the numbers for the resection of the lateral recti need to be reduced
2. Monocular Surgery
Medial rectus recession Lateral rectus resection
15 PD = 20 PD = 25 PD = 30 PD = 35 PD = 40 PD = 50 PD = 60 PD = 70 PD =
3.0 mm 3.5 mm 4.0 mm 4.5 mm 5.0 mm 5.5 mm 6.0 mm 6.5 mm 7.0 mm
3.5 mm 4.0 mm 5.0 mm 5.5 mm 6.0 mm 6.5 mm 7.0 mm 7.5 mm 8.0 mm
Exotropia
1. Binocular Surgery
Lateral rectus recession Medial rectus resection a
15 PD = 4.0 mm 20 PD = 5.0 mm 25 PD = 6.0 mm 30 PD = 7.0 mm 35 PD = 7.5 mm 40 PD = 8.0 mm b 50 PD = 9.0 mm b
15 PD = 3.0 mm 20 PD = 4.0 mm 25 PD = 5.0 mm 30 PD = 5.5 mm 35 PD = 6.0 mm 40 PD = 6.5 mm
a If a large lateral rectus recession has been performed (≥9.0 mm) and bilateral medial rectus resection is planned for residual exotropia, the amount of resection may need to be reduced. b Recessions greater than 9.0 mm may result in an abduction defi cit. In these cases, the surgeon might consider a staged approach (bilateral lateral rectus recession followed by bilateral medial resection if resid-ual exotropia is still present).
V. Miraldi Utz, M.D. Abrahamson Pediatric Eye Institute, Cincinnati Children’s Hospital Medical Center , 3333 Burnet Ave, MLC 4008 , Cincinnati , OH 45229-3039 , USA
Department of Ophthalmology , University of Cincinnati College of Medicine , 3333 Burnet Ave, MLC 4008 , Cincinnati , OH 45229-3039 , USA
E. I. Traboulsi, M.D. Cleveland Clinic, Cole Eye Institute , 9500 Euclid Avenue, i-32 , Cleveland , OH 44195 , USA
786
2. Monocular Surgery
Lateral rectus recession Medial rectus resection
15 PD = 20 PD = 25 PD = 30 PD = 35 PD = 40 PD = 50 PD =
4.0 mm 5.0 mm 6.0 mm 6.5 mm 7.0 mm 7.5 mm 8.5 mm
3.0 mm 4.0 mm 4.5 mm 5.0 mm 5.5 mm 6.0 mm 6.5 mm
Vertical Rectus Muscle Surgery
Nystagmus Surgery for Face Turn
Face Turn to the RIGHT (Left Gaze Preference)
1. Goal: Move eyes to the RIGHT
Degrees of face turn <20° 30° 45°
Left eye: recess LR 7 mm 9 mm 10 mm
Left eye: resect MR 6 mm 8 mm 8.5 mm
Right eye: recess MR 5 mm 6.5 mm 7.0 mm
Right eye: resect LR 8 mm 10 mm 11 mm
Face Turn to the LEFT (Right Gaze Preference)
1. Goal: To move eyes to the LEFT
Degrees of face turn <20° 30° 45°
Right eye: recess LR 7 mm 9 mm 10 mm
Right eye: resect MR 6 mm 8 mm 8.5 mm
Left eye: recess MR 5 mm 6.5 mm 7.0 mm
Left eye: resect LR 8 mm 10 mm 11 mm
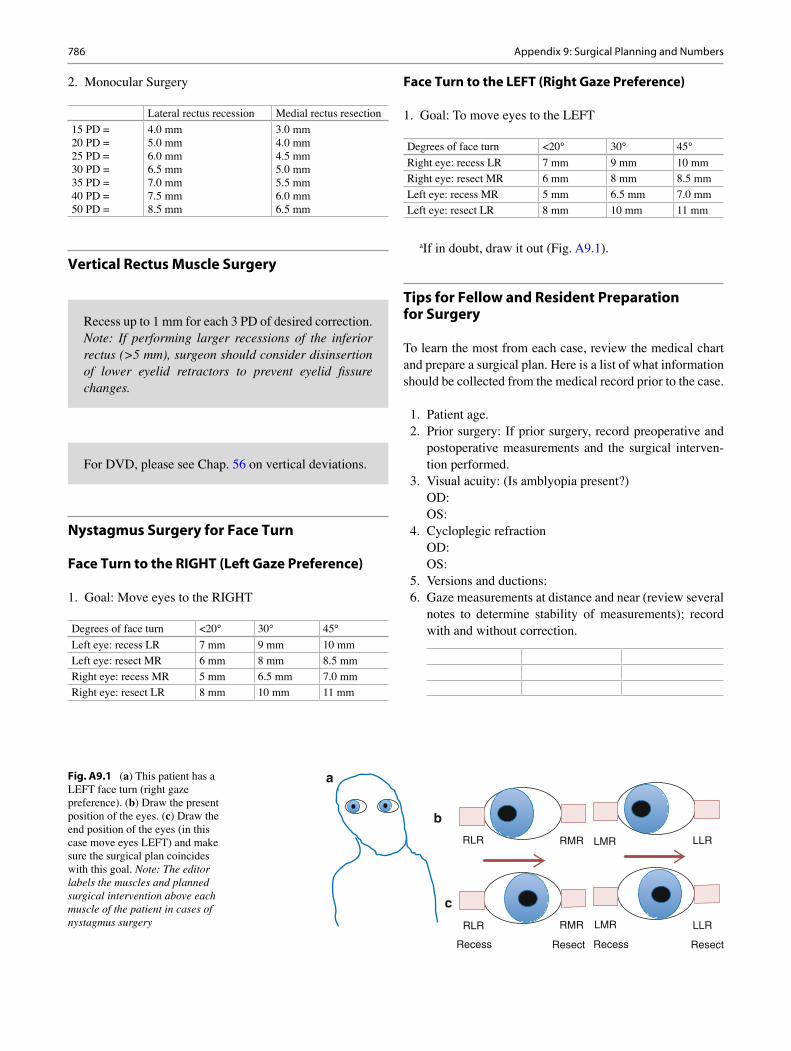
a If in doubt, draw it out (Fig. A9.1 ).
Tips for Fellow and Resident Preparation for Surgery
To learn the most from each case, review the medical chart and prepare a surgical plan. Here is a list of what information should be collected from the medical record prior to the case.
1. Patient age. 2. Prior surgery: If prior surgery, record preoperative and
postoperative measurements and the surgical interven-tion performed.
3. Visual acuity: (Is amblyopia present?) OD: OS:
4. Cycloplegic refraction OD: OS:
5. Versions and ductions: 6. Gaze measurements at distance and near (review several
notes to determine stability of measurements); record with and without correction.
Recess up to 1 mm for each 3 PD of desired correction. Note: If performing larger recessions of the inferior rectus (>5 mm), surgeon should consider disinsertion of lower eyelid retractors to prevent eyelid fi ssure changes.
For DVD, please see Chap. 56 on vertical deviations.
Fig. A9.1 ( a ) This patient has a LEFT face turn (right gaze preference). ( b ) Draw the present position of the eyes. ( c ) Draw the end position of the eyes (in this case move eyes LEFT) and make sure the surgical plan coincides with this goal. Note: The editor labels the muscles and planned surgical intervention above each muscle of the patient in cases of nystagmus surgery
a
b
c
RLR
RLR
Recess Resect Recess Resect
RMR
RMR
LMR
LMR LLR
LLR
Appendix 9: Surgical Planning and Numbers
787
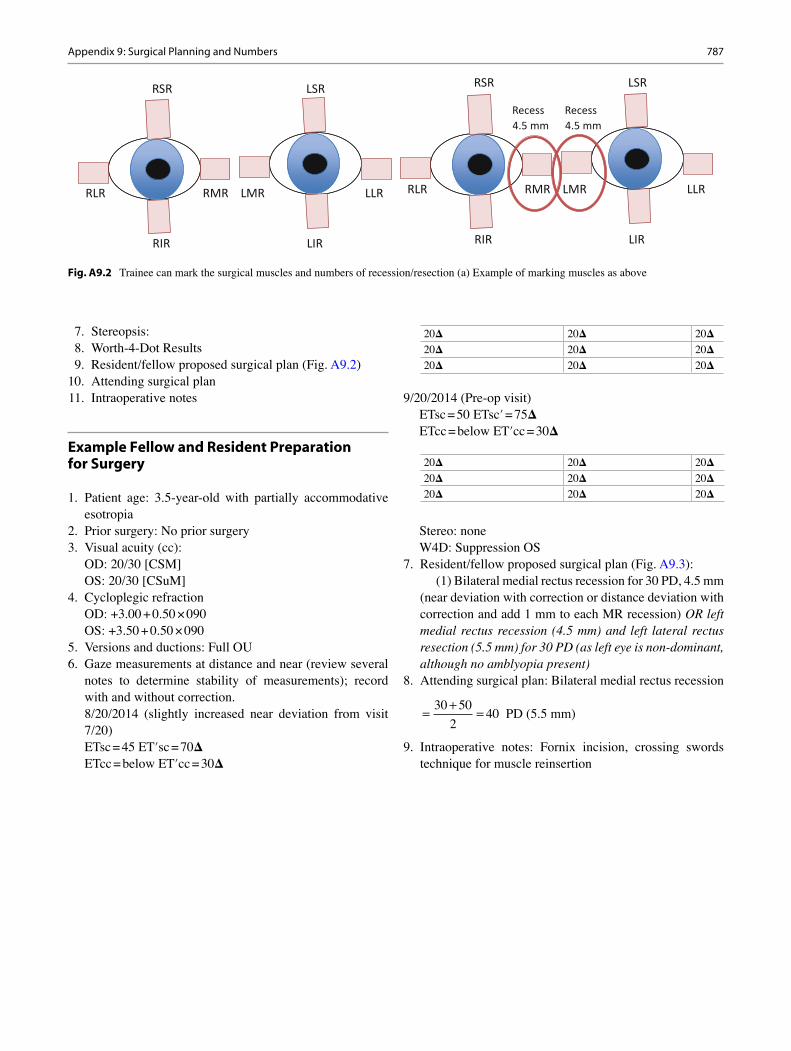
7. Stereopsis: 8. Worth-4-Dot Results 9. Resident/fellow proposed surgical plan (Fig. A9.2 ) 10. Attending surgical plan 11. Intraoperative notes
Example Fellow and Resident Preparation for Surgery
1. Patient age: 3.5-year-old with partially accommodative esotropia
2. Prior surgery: No prior surgery 3. Visual acuity (cc):
OD: 20/30 [CSM] OS: 20/30 [CSuM]
4. Cycloplegic refraction OD: +3.00 + 0.50 × 090 OS: +3.50 + 0.50 × 090
5. Versions and ductions: Full OU 6. Gaze measurements at distance and near (review several
notes to determine stability of measurements); record with and without correction. 8/20/2014 (slightly increased near deviation from visit 7/20) ETsc = 45 ET′sc = 70 Δ ETcc = below ET′cc = 30 Δ
20 Δ 20 Δ 20 Δ
20 Δ 20 Δ 20 Δ
20 Δ 20 Δ 20 Δ
9/20/2014 (Pre-op visit) ETsc = 50 ETsc′ = 75 Δ ETcc = below ET′cc = 30 Δ
20 Δ 20 Δ 20 Δ
20 Δ 20 Δ 20 Δ
20 Δ 20 Δ 20 Δ
Stereo: none W4D: Suppression OS
7. Resident/fellow proposed surgical plan (Fig. A9.3 ): (1) Bilateral medial rectus recession for 30 PD, 4.5 mm
(near deviation with correction or distance deviation with correction and add 1 mm to each MR recession) OR left medial rectus recession (4.5 mm) and left lateral rectus resection (5.5 mm) for 30 PD (as left eye is non-dominant, although no amblyopia present)
8. Attending surgical plan: Bilateral medial rectus recession
=+
=30 50
240
PD (5.5 mm)
9. Intraoperative notes: Fornix incision, crossing swords technique for muscle reinsertion
Fig. A9.2 Trainee can mark the surgical muscles and numbers of recession/resection (a) Example of marking muscles as above
RLR RMR LMR LLR
RIR LIR
RSR LSR
RLR RMR LMR LLR
RIR LIR
RSR LSR
Recess4.5 mm
Recess4.5 mm
Appendix 9: Surgical Planning and Numbers

789© Springer Science+Business Media, LLC 2016E.I. Traboulsi, V. Miraldi Utz (eds.), Practical Management of Pediatric Ocular Disorders and Strabismus, DOI 10.1007/978-1-4939-2745-6
Appendix 10: ROP Examination and Treatment Pearls
Michael B. Yang
Order of Examination One recommended sequence of examination outlined below (pupil, optic nerve, then tempo-ral, nasal, superior/inferior retina) is based on the likelihood of detecting examination fi ndings that impact the decision for treatment or follow-up should an abbreviated examina-tion become necessary due to physiologic instability in the infant [ 1 ]. (1) Check the pupil for iris neovascularization. (2) Check the optic nerve and posterior pole vessels to evaluate for the presence of plus disease. The diagnosis of plus dis-ease may be subjective. Thus, recalibration of one’s mental image of plus disease periodically by comparison with stan-dard photographs from ICROP is recommended [ 2 ]. (3) Check the temporal 4 clock hours of retina to determine if the ROP is in zone I or close to the macula, as disease sever-ity is usually greatest in the temporal retina followed by the nasal retina and then the superior/inferior retina. (4) Check the nasal 4 clock hours of retina to determine whether the nasal retina is vascularized to the ora serrata for 2 clock hours. If so, then by defi nition retinal vascularization has proceeded into zone III temporally. (5) Check the superior and inferior retina last as these areas are unlikely to have a higher stage of ROP than the temporal or nasal retina.
Examination Equipment An Alfonso lid speculum (Storz E4112) effectively retracts the eyelids. The sclera can be indented by using a calcium alginate swab with a thin alumi-num shaft or by using a Flynn scleral depressor (Storz E5107). The latter can create a line of white with pressure
that mimics the appearance of stage 1 or 2 ROP or that hides potential ROP on the downslope of the indented retina away from the examiner’s view. A 28-diopter condensing lens is useful for determining the location of disease because if the nasal border of the optic nerve is placed at one edge of the afforded view during binocular indirect ophthalmoscopy, the other edge of the view marks the temporal boundary of zone I [ 2 ]. A 20-diopter lens allows the visualization of the details of plus disease and stage 3 ROP.
Laser Photocoagulation Surgery may be performed under general anesthesia in the operating room or sedation in the nursery. Typical initial settings for a portable diode laser used in ROP treatment (Oculight XLS, Iridex, Mountain View, CA) are 100 mW power, 300 ms duration, and 300 ms repeat interval. The power is gradually increased until a gray-white burn is achieved with the spots set about one-half burn width apart. Applying a row of laser spots to the avas-cular retina just peripheral to the vascular-avascular junction 360° serves to mark off the posterior extent of the planned treatment. If the view becomes blurry during treatment, one can more safely complete the laser procedure by ablating the avascular retina peripheral to the fi rst row of laser.
Bevacizumab Injection A different drug lot can be used for each eye if bilateral therapy is planned. Slightly more than the standard dose of 0.625 mg of bevacizumab in 0.025 ml should be drawn by the pharmacist directly from the manufacturer supplied vial in a 1-ml tuberculin syringe which is then fi tted with a 30-gauge needle without a safety guard that can impede injection. The treating physician can waste the excess just before injection. Povidone-iodine 5 % solution for endophthalmitis prophylaxis is instilled in the eye for a few minutes before injection. Then cotton applica-tors soaked with topical anesthetic are applied to the injec-tion site. Pretreatment with systemic pain medication
M. B. Yang, M.D. Abrahamson Pediatric Eye Institute, Cincinnati Children’s Hospital Medical Center , 3333 Burnet Ave, MLC 4008 , Cincinnati , OH 45229- 3039 , USA
Department of Ophthalmology , University of Cincinnati College of Medicine , 3333 Burnet Ave, MLC 4008 , Cincinnati , OH 45229-3039 , USA

790
should be considered. The treating physician’s fi nger should not touch the plunger until the needle has been inserted through the sclera as the minutest pressure will cause a small amount of drug to escape at the needle tip. The injec-tion site should be measured at 0.5–1.0 mm from the cor-neal limbus since the pars plana is narrow in the premature infant [ 3 ]. The eye should be immobilized with forceps or a cotton tip applicator, while the sclera is penetrated with the needle aimed toward the optic nerve to avoid injuring the lens. As the needle is withdrawn, the injection site is blotted with a cotton tip applicator.
References
1. Chiang MF, Melia M. Buffenn AN, et al. Detection of clinically signifi cant retinopathy of prematurity using wide-angle digital pho-tography: a report by the American Academy of Ophthalmology. Ophthalmology 2012; 119: 1272–80.
2. Cryotherapy for Retinopathy of Prematurity Cooperative Group. 15-year outcomes following threshold retinopathy of prematurity : fi nal results from the multicenter trial of cryotherapy of retinopathy of prematurity. Arch Ophthalmol. 2005; 123: 311–8.
3. Simpson JL, Melia M, Yang MB, et al. Current role of cryotherapy in retinopathy of prematurity: a report by the American Academy of Ophthalmology. Ophthalmology. 2012; 119:873–7.
Appendix 10: ROP Examination and Treatment Pearls

791© Springer Science+Business Media, LLC 2016E.I. Traboulsi, V. Miraldi Utz (eds.), Practical Management of Pediatric Ocular Disorders and Strabismus, DOI 10.1007/978-1-4939-2745-6
Appendix 11: ROP Follow-Up Schedule
Michael B. Yang
The policy statement of the pediatric and ophthalmology specialty organizations in the United States recommends an initial ROP examination at 31 weeks postmenstrual age (PMA) or 4 weeks chronological age, whichever is later, for premature infants ≤1500 g birth weight or ≤30 weeks esti-mated gestational age at birth.
The recommended intervals for follow-up examinations based on retinal fi ndings using the revised International Classifi cation of ROP [ 14 ] (Table 29.2) are as follows: 1 week or less for immature vascularization in zone I or in the posterior aspect of zone II near the zone I border, stage 1 or 2 ROP in zone I, stage 3 ROP in zone II, or the presence or suspected presence of aggressive posterior ROP; 1 to 2 week(s) for immature vascularization in posterior zone II, stage 2 ROP in zone II, or unequivocally regressing ROP in zone I; 2 weeks for stage 1 ROP in zone II, immature vascu-larization in zone II, or unequivocally regressing ROP in zone II; and 2 to 3 weeks for stage 1 or 2 ROP in zone III or regressing ROP in zone III.
The suggested criteria for termination of screening examinations include (1) full retinal vascularization (mature), (2) retinal vascularization into zone III without
previous ROP in zone I or II and in an infant ≥35 weeks PMA, (3) the attainment of 50-week PMA in an infant with-out the presence of prethreshold ROP or worse disease, or (4) absence of vascular tissue that can reactivate after previ-ous regression of ROP in zone II or III.
The responsibilities for educating the family of premature infants at risk for ROP and ensuring timely follow-up exami-nations (whether inpatient or after hospital discharge) should be carefully delineated between the neonatal intensive care unit (NICU) staff and the examining ophthalmologist [ 16 ]. It may be prudent for the ophthalmologist to also indepen-dently keep track of the infants who warrant follow-up examinations rather than rely solely upon the NICU to schedule them correctly. 1
1 Many of these recommendations are based on evidence from multi-center studies, but they do not account for center-specifi c differences or infant characteristics that may modify the risk of individual infants. Ophthalmologists who wish to deviate from the recommended ROP screening guidelines may benefi t from developing institutional consen-sus after a careful review of center-specifi c evidence. However, some insurance companies may not provide liability coverage, if examiners deviate from the guidelines.
M. B. Yang, M.D. Abrahamson Pediatric Eye Institute, Cincinnati Children’s Hospital Medical Center , 3333 Burnet Ave, MLC 4008 , Cincinnati , OH 45229-3039 , USA
Department of Ophthalmology , University of Cincinnati College of Medicine , 3333 Burnet Ave, MLC 4008 , Cincinnati , OH 45229-3039 , USA

793© Springer Science+Business Media, LLC 2016E.I. Traboulsi, V. Miraldi Utz (eds.), Practical Management of Pediatric Ocular Disorders and Strabismus, DOI 10.1007/978-1-4939-2745-6
Appendix 12: Pseudotumor Cerebri Diagnostic Criteria
Grant T. Liu
G. T. Liu, M.D. Department of Ophthalmology , Children’s Hospital of Philadelphia , 34th and Civic Center Blvd. , Philadelphia , PA 19104 , USA
794
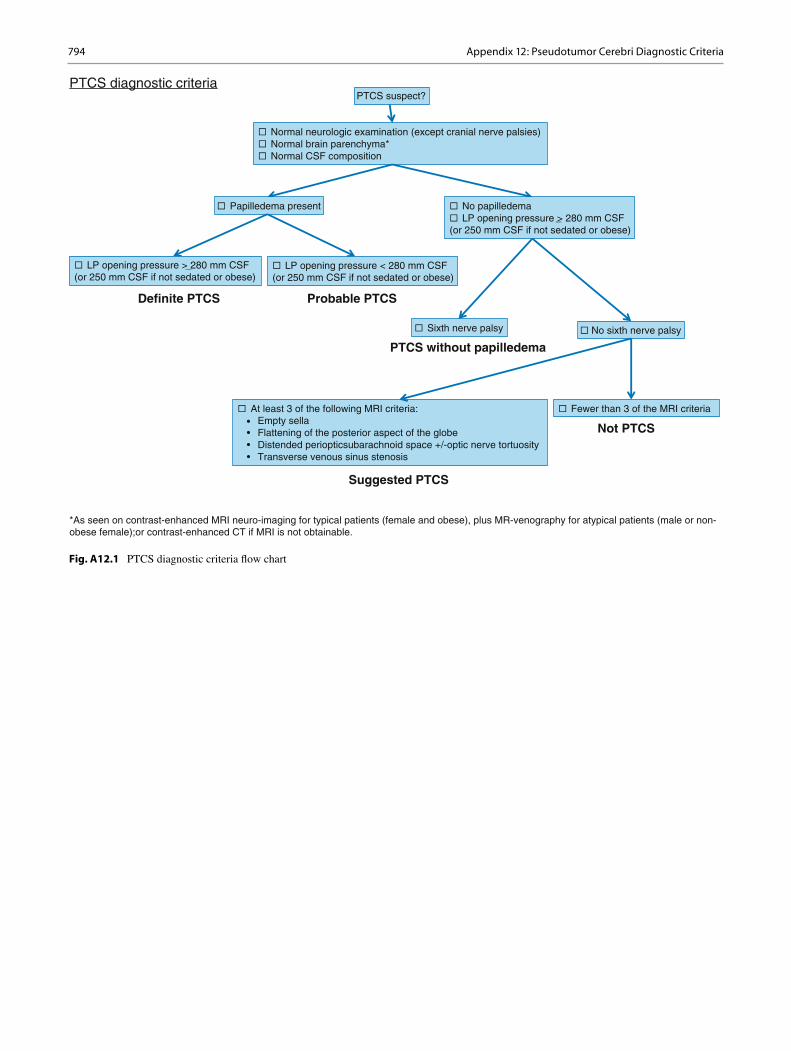
Fig. A12.1 PTCS diagnostic criteria fl ow chart
Normal neurologic examination (except cranial nerve palsies)Normal brain parenchyma*Normal CSF composition
PTCS suspect?PTCS diagnostic criteria
Papilledema present No papilledemaLP opening pressure > 280 mm CSF
(or 250 mm CSF if not sedated or obese)
LP opening pressure > 280 mm CSF (or 250 mm CSF if not sedated or obese)
LP opening pressure < 280 mm CSF(or 250 mm CSF if not sedated or obese)
*As seen on contrast-enhanced MRI neuro-imaging for typical patients (female and obese), plus MR-venography for atypical patients (male or non-obese female);or contrast-enhanced CT if MRI is not obtainable.
Sixth nerve palsy No sixth nerve palsy
At least 3 of the following MRI criteria:• Empty sella• Flattening of the posterior aspect of the globe• Distended periopticsubarachnoid space +/-optic nerve tortuosity• Transverse venous sinus stenosis
Fewer than 3 of the MRI criteria
Definite PTCS Probable PTCS
PTCS without papilledema
Not PTCS
Suggested PTCS
Appendix 12: Pseudotumor Cerebri Diagnostic Criteria
795© Springer Science+Business Media, LLC 2016E.I. Traboulsi, V. Miraldi Utz (eds.), Practical Management of Pediatric Ocular Disorders and Strabismus, DOI 10.1007/978-1-4939-2745-6
Appendix 13: Anisocoria
Greg Kosmorsky
Figure A13.1
1. The diagnosis of physiologic anisocoria is based on a brisk reaction with no dilation lag (e.g., the anisocoria is equal in both dim and light conditions). Physiologic anisocoria is usually ≤1 mm.
2. If there is brisk reaction to light , but dilation lag (e.g., anisocoria is greater under dim conditions), the differential diagnosis includes Horner syndrome as well as mechani-cal or pharmacologic miosis. Both apraclonidine and cocaine testing can be used to determine if a Horner syn-drome is present, but do not distinguish between pregangli-onic and postganglionic lesions. Hydroxyamphetamine is used to distinguish between preganglionic and postgangli-onic involvement.• Apraclonidine 1 % testing:
– Mechanism: Apraclonidine inhibits the alpha-2 receptor on the presynaptic nerve terminal inhibit-ing norepinephrine release.
– Testing: Normal eye constricts. Abnormal (smaller) pupil dilates because there is adrenergic supersensitivity (increased alpha-1 receptors) on the iris dilator muscle. Apraclonidine has weak alpha-1 activity leading to the dilation observed.
**Use caution in young children as it may cause seda-tion because of CNS affects**
• Cocaine: Blocks reuptake of norepinephrine (NE) at presynaptic nerve terminal – Testing: Normal pupil will dilate. Abnormal
(smaller) pupil will not dilate because little or no NE is released into the synapse.
• Hydroxyamphetamine (instill 24 h after cocaine): – Mechanism: Releases NE from presynaptic nerve
terminal – Testing:
Postganglionic : Abnormal (smaller) pupil does not respond and remains miotic with testing (nerve terminal has degenerated).
Preganglionic: Abnormal (smaller) pupil dilates as much (if not more) than the normal pupil (postganglionic neuron is intact).
– Acquired Horner syndrome requires further diagnostic workup in the pediatric population as the differential includes trauma, malignancy, and neuroblastoma of the sympathetic chain. Diagnostic workup should include imaging of the brain, neck, and chest. Urine catecholamines could also be considered.
3. If there is a poor reaction to light (anisocoria greater in dim illumination), the following etiologies must be care-fully distinguished:• Mechanical etiology: Evaluate at slit lamp for transil-
lumination defects, sphincter tears, synechiae, or post-surgical abnormalities of the pupil
• Adie’s tonic pupil: An Adie’s pupil is caused by post-ganglionic parasympathetic denervation and is usually unilateral. A tonic pupil is usually poorly reactive, and occasionally sectoral segments of sphincter paralysis can be observed at the slit lamp. Diagnostic testing can be performed with dilute 0.1 % pilocarpine: – Mechanism: Pilocarpine is a direct-acting choliner-
gic agonist. – Testing:
0.1 % Pilocarpine: The denervated iris sphincter is supersensitive to dilute 0.1 % pilocarpine and will constrict. The normal pupil will have mini-mal reaction at this dilute concentration.
*** Note: An early Adie’s pupil may not be supra-sensitized and yield a false-negative test. It is prob-
G. Kosmorsky, D.O. Department of Ophthalmology , Cleveland Clinic, Cole Eye Institute I-30 , 9500 Euclid Ave , Cleveland , OH 44195 , USA
796
ably better to assume a possible pupil-involving third nerve palsy and image accordingly for aneu-rysm. ***
1 % Pilocarpine: Both normal and abnormal pupils should constrict. If the abnormal (dilated) pupil fails to con-strict to 1 % pilocarpine, then it is likely pharmaco-logically dilated . If the abnormal pupil (dilated) pupil constricts appropriately , a third nerve palsy must be evaluated by neuroimaging for vascular mal-formation, aneurysm, and malignancy compressing the pupillary fi bers. Other clinical signs of a partial or full third nerve palsy may be present (ptosis, adduc-tion, supraduction, or infraduction defi cit).
References
1. Miller JM, Harvey EM. Spectacle prescribing recommendations of AAPOS members. J Pediatr Ophthalmol Strabismus. 1998;35(1):51–2.
2. American Academy of Ophthalmology. Pediatric eye evaluations, preferred practice pattern. San Francisco, CA: American Academy of Ophthalmology; 2012.
3. Donahue SP, Arthur B, Neely DE, Arnold RW, Silbert D, Ruben JB, Committee POSVS. Guidelines for automated preschool vision screening: a 10-year, evidence-based update. J AAPOS. 2013;17(1):4–8.
4. Donahue SP, Arnold RW, Ruben JB, Committee AVS. Preschool vision screening: what should we be detecting and how should we report it? Uniform guidelines for reporting results of preschool vision screening studies. J AAPOS. 2003;7(5):314–6.
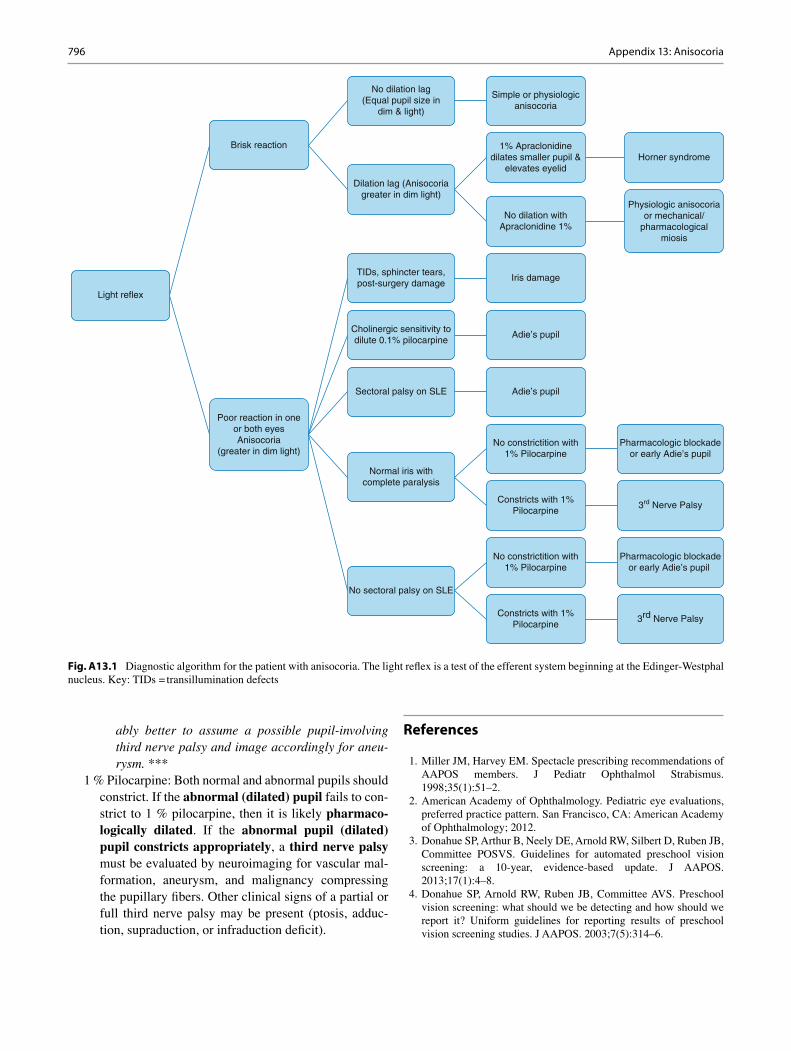
Fig. A13.1 Diagnostic algorithm for the patient with anisocoria. The light refl ex is a test of the efferent system beginning at the Edinger-Westphal nucleus. Key: TIDs = transillumination defects
Light reflex
Brisk reaction
No dilation lag(Equal pupil size in
dim & light)
Simple or physiologicanisocoria
Dilation lag (Anisocoriagreater in dim light)
1% Apraclonidinedilates smaller pupil &
elevates eyelidHorner syndrome
No dilation withApraclonidine 1%
Physiologic anisocoriaor mechanical/
pharmacologicalmiosis
Poor reaction in oneor both eyesAnisocoria
(greater in dim light)
TIDs, sphincter tears,post-surgery damage
Iris damage
Cholinergic sensitivity todilute 0.1% pilocarpine
Adie’s pupil
Sectoral palsy on SLE Adie’s pupil
Normal iris withcomplete paralysis
No constrictition with1% Pilocarpine
Pharmacologic blockadeor early Adie’s pupil
Constricts with 1%Pilocarpine
No sectoral palsy on SLE
No constrictition with1% Pilocarpine
Pharmacologic blockadeor early Adie’s pupil
Constricts with 1%Pilocarpine
3rd Nerve Palsy
3rd Nerve Palsy
Appendix 13: Anisocoria

797
5. Schramm KD. Dispensing pediatric eyewear. Oxford: Butterworth- Heinemann; 2000.
6. Meister D, Sheedy JE. Introduction to ophthalmic optics. San Diego, CA: Carl Zeiss Vision; 1999–2000. p. 69.
7. Cotter SA. Clinical uses of prism. A spectrum of applications. St. Louis, MO: Mosby; 1995.
8. Meister D, Sheedy JE. Introduction to ophthalmic optics. San Diego, CA: Carl Zeiss Vision; 1999–2000. p. 57.
9. Jabs DA, Nussenblatt RB, Rosenbaum JT. Standardization of Uveitis Nomenclature Working G. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol. 2005;140(3):509–16.
10. Good WV, Hoyt CS. Strabismus management. Boston, MA: Butterworth-Heinemann; 1996. pp. 217, 234, 362, 280, 323.
11. Mitchell PR, Wheeler MB, Parks MM. Kestenbaum surgical proce-dure for torticollis secondary to congenital nystagmus. J Pediatr Ophthalmol Strabismus. 1987;24:87–93.
12. Parks MM. Ocular motility and strabismus. New York, NY: Harper and Row; 1975. pp. 108, 120, 121.
13. Paysee EA, Coats DK, Sprunger DT. Predictive value of temporal retinal disease in retinopathy of prematurity. J Pediatr Ophthalmol Strabismus. 1997;34:177–81.
14. International Committee for the Classifi cation of Retinopathy of Prematurity. The international classifi cation of retinopathy of pre-maturity revisited. Arch Ophthalmol. 2005;123:991–9.
15. Hairston RJ, Maquire AM, Vitale S, Green WR. Morphometric analy-sis of pars plana development in humans. Retina. 1997;17:135–8.
16. Section on Ophthalmology, American Academy of Pediatrics, American Academy of Ophthalmology, and American Association for Pediatric Ophthalmology and Strabismus, and American Association of Certifi ed Orthoptists. Screening examinations of premature infants for retinopathy of prematurity. Pediatrics. 2013;131:189–95.
Appendix 13: Anisocoria
799© Springer Science+Business Media, LLC 2016E.I. Traboulsi, V. Miraldi Utz (eds.), Practical Management of Pediatric Ocular Disorders and Strabismus, DOI 10.1007/978-1-4939-2745-6
Index
A A- and V-pattern strabismus , 586–589
bilateral superior oblique overaction , 591 craniosynostosis syndromes , 584 horizontal rectus muscle dysfunction , 584 oblique muscle overaction , 584 ocular misalignment , 590 treatment
oblique muscle surgery , 589 rectus muscle surgery , 586–589
upgaze and downgaze , 583 vertical rectus muscle dysfunction , 584
AAO . See American Academy of Ophthalmology (AAO) AAP . See American Academy of Pediatrics (AAP) Abraham, A. , 547 , 548 , 550–554 Abusive head trauma , 314–318
bilateral thin-fi lm subdural hemorrhages , 317 brain injury , 317 child abuse , 313 Child Abuse Pediatrics Team , 317 child maltreatment , 313 CPS , 313 diagnosis
abusive injuries , 314 acceleration-deceleration injuries , 314 cataracts and lens subluxation , 315 child’s developmental abilities , 314 color fundus photograph , 314 , 315 deprivation amblyopia , 318 endocarditis , 314 fundus photography , 316 hemorrhages , 316 hemorrhagic macular schisis cavities , 314 hemosiderin , 314 international classifi cation system , 316 interobserver differences , 316 macular schisis cavity , 318 non-accidental trauma , 314 ophthalmology consultation , 314 retinal hemorrhages , 314–316 retinal photography , 314 retinal/visual sequelae , 317 retinopathy , 316 subconjunctival hemorrhage , 314 subdural hemorrhage , 314 subhyaloid hemorrhage , 314 traumatic retinoschisis , 314 vitreous hemorrhage , 314
dilated indirect ophthalmoscopy , 317 hemorrhagic macular schisis cavities , 317 optimal visual function , 317
Shaken baby syndrome , 313 skeletal survey , 317
Accommodative convergence to accommodation (AC/A) ratio , 496 Accommodative esotropia , 37 , 39 , 41
AC/A ratio , 496 , 499 , 500 atropine relaxation , 496 augmentation , 497 augmented and slanted recessions , 500 binocular development , 500 binocular function , 496 binocular vision and stereopsis , 496 characteristics vs . results , 500 , 501 diagnosis and treatment , 496 dosage calculation , 497 , 498 , 500 ET and hyperopia , 498 glasses/contact lenses , 497 hyperopia , 495–497 , 502 infantile esotropia syndrome , 496 medial rectus recessions , 500 , 501 refractive correction , 500 single and double vision , 496 spectacle bifocal and hyperopic correction , 502 spectacle correction , 497 spectacle weaning technique , 502 strabismus surgery , 497 surgical treatment , 501–502 visual system , 497 weaning , 502
Accommodative non-refractive esotropia , 496 ACE . See Angiotensin-converting enzyme (ACE) Achromatopsia , 295 , 339–341 Acids , 159 ACMG . See American College of Medical Genetics (ACMG) Acquired immunodefi ciency syndrome (AIDS) , 244 Acquired sixth nerve palsy , 507–508 Acquired traumatic cataract
CPC , 465 GDD , 465 glaucoma , 465 history , 464 , 465 interval history (6 months) , 465 management , 465
Acute acquired comitant esotropia , 489 Acute demyelinating encephalomyelitis (ADEM)
description , 430 infl ammatory demyelinating disease , 431 lumbar puncture , 431 monophasic illness , 433
Acute infl ammatory DON . See Demyelinating optic neuritis (DON) Acute posterior multifocal placoid pigment epitheliopathy
(APMPPE) , 230
800
Acute retinal necrosis (ARN) , 242 , 243 Acute strabismus
adult patients , 635 clinical evaluation , 636–637 clinical features , 635–636 etiology , 636 management , 637
Adamantiades–Behcet’s disease (ABD) , 230 Adamopoulou, C. , 81–97 ADEM . See Acute demyelinating encephalomyelitis (ADEM) Adjustable suture technique , 569 Afferent pupillary defect (APD) , 83 Aggressive posterior ROP (AP-ROP) , 301 Akar, S. , 500 , 509 Alkali injury , 159 Allergic conjunctivitis
AKC , 106 chronic red eyes , 105 eczema and allergies , 105 itching and eye rubbing , 105 VKC , 106
Al-Nammari, S. , 669 Amaro-Quireza, L. , 291 , 293 , 295 Amblyopia , 48 , 137 , 138 , 175 , 177 , 181 , 660 , 662 , 719 Amblyopia management , 83–85 , 94 , 95
BCVA , 81 binocular treatments , 96 children >7 years of age , 94 clinical examination , 83 defi nition, amblyopia , 82 deprivation amblyopia , 82 , 83 diagnostic and therapeutic algorithm , 97 moderate amblyopia , 89 moderate to severe amblyopia , 85 , 93 , 94 occlusion therapy , 85 , 86 ocular dominance columns , 82 PEDIG trials , 89–92 refractive amblyopia , 82 residual amblyopia
levodopa , 94 occlusive and pharmacologic , 94 refractive surgery , 95
risk factors , 81 deprivation amblyopia , 83 refractive amblyopia , 83 refractive and deprivation amblyopia , 83
screening guidelines , 83 strabismic amblyopia , 82 from strabismus
occlusive penalization , 84 patching , 85 Surgical correction , 84
treatment strategies , 82 visual acuity , 86 , 87
Amblyopia Treatment Study 2C (ATS2C) , 85 American Academy of Ophthalmology (AAO) , 331 , 560 American Academy of Pediatrics (AAP) , 214 , 215 , 331 American Association for Pediatric Ophthalmology and Strabismus
(AAPOS) , 39 , 84 American College of Medical Genetics (ACMG) , 331 Amyloid precursor protein (APP) , 737 Amyloid-β peptide (Aβ) , 737 Ancillary ophthalmic testing
automated visual fi elds , 430 HVF 24-2 SITA fast visual fi elds , 431 , 432 lumbar puncture , 431
macular edema and submacular fl uid OCT , 431 , 433 MRI , 431 , 435 , 436 NMO and MOG antibodies , 431 OCT , 430 spectral domain OCT with acute DON , 431 , 434 VEP signal , 431
Angiotensin-converting enzyme (ACE) , 431 Angle kappa
esotropia , 14 strabismus assessment , 13
Anisometropia , 75 , 77 Anisometropic amblyopia , 88 , 92 , 93
bangerter fi lter , 93 BCVA
atropine , 88 , 92 , 93 patching , 88
contact lens , 93 prescribed glasses , 87 refractive correction , 88
Anisometropic or strabismic or combined mechanism , 89 , 91 Anomalous retinal correspondence (ARC)
binocular conditions , 30 eye misalignment , 29 harmonious/nonharmonious , 29 NRC , 30 paradoxical diplopia , 29
Anterior segment dysgenesis syndromes Axenfeld–Rieger syndrome , 141 clinical fi ndings , 142 diagnosis , 144–145 genetics , 144 glaucoma , 143–144 management and Prognosis , 145–146 posterior embryotoxon , 142 spectrum , 143
Anterior segment herpetic disease amblyopia , 126 anterior segment , 120 anterior segment herpetic eye disease , 127 drug management , 127 epithelial keratitis , 120 evidence-based oral antiviral treatment protocols , 120 herpes virus infections , 119 herpetic keratitis , 126 HSV-1 and HSV-2 , 120 mobility and photophobia , 127 ocular herpes , 120 oral acyclovir , 127 pediatric herpes infection , 126 polymerase chain reaction (PCR) , 120 trigeminal nerve (CN V) , 120 VZV , 125–126 VZV and CMV , 119
Anterior segment ischemia , 645–646 Anterior segment OCT (AS-OCT) , 285 Apert syndrome , 130 , 710 , 721 Aphakic infant fi t with GP lens , 69 , 70 Aphakic infant fi t with Silsoft lens , 69 Aphakic/pseudophakic glaucoma
cataract , 457 childhood cataract surgery , 458 CPC , 458 cyclodestructive procedures , 459 diagnosis , 457 EUAs , 458 GDD , 458
Index
801
Goldmann applanation tonometry , 458 IATS , 458 IOP and glaucoma , 457 medical therapy , 458 micro-catheter , 458 risk factors , 458 trabeculectomy, mitomycin C , 459 WGA Consensus , 457
Apputukan , 550 ARC . See Anomalous retinal correspondence (ARC) Archer, S.M. , 552 Ariss, M.M. , 103–107 , 150–152 , 313–318 , 547 , 548 , 550–554 , 635 ,
637–639 Arnold–Chiari malformation , 751 Aronow, M.E. , 370 Astigmatism , 51
amblyopia , 52 correction , 52 correction, refractive errors , 52 cycloplegic retinoscopy , 52 guidelines , 52 irregular (see Irregular astigmatism ) preferred practice pattern , 52 preferred practice patterns , 52 regular (see Regular astigmatism ) survey , 52
Atopic keratoconjunctivitis (AKC) , 106 Atrophic nerves , 274–275 Atropine , 92 , 93 Avery, R.A. , 411 Axenfeld–Rieger syndrome , 141–145 , 332
B Babiuch, A.E. , 25–34 , 469–472 , 474 Bacterial conjunctivitis
aminoglycoside , 104 antibiotics , 104 azithromycin , 104 contact lens , 104 discharge , 104 Neisseria and chlamydia , 104 pathogens , 104 placebo vs . antibiotics , 104 polymyxin and bacitracin ointment , 104 polymyxin B-trimethoprim , 104
Bacterial keratitis , 112 , 113 corneal ulcers , 113 diagnosis , 112 pathogenesis , 112 risk factors , 112 treatment
antimicrobials , 112 corticosteroids , 113 drop vs . ointment formulations , 112 monotherapy , 113
Bagolini striated lenses , 32 Bahl, R.S. , 513 , 514 , 516 , 517 , 521 , 525–527 , 531 , 583 , 584 , 586 , 588 ,
589 , 591 Bain, K.E. , 759 Balloon catheter dilation , 655–657 Bangerter Filter Treatment Study , 93 Bardet-Biedl syndrome (BBS) , 342–344 Barry, J. , 625 Batten disease (Jansky-Bielschowsky disease) , 283 Baumal, C.R. , 244 BCVA . See Best-corrected visual acuity (BCVA)
Beck, A.D. , 442 Best-corrected visual acuity (BCVA) , 81 , 88 , 90 , 92 , 93 Bevacizumab Eliminates the Angiogenic Threat of ROP (BEAT-ROP) ,
302–303 Bhandari, R. , 138 Bhardwaj, G. , 316 Bhatti, M.T. , 427–431 , 433 , 435–437 Bielschowsky Head Tilt test , 627 Bilateral congenital cataracts
aphakic glaucoma , 460 , 462 history , 459 , 461 , 462 interval history (1 year) , 460 interval history (2 months) , 462 interval history (4 months) , 463 interval history (5 months) , 462 interval history (6 weeks) , 460 IOP , 460 management , 459 , 462 pseudophakic glaucoma , 463
Bilateral Group E retinoblastoma , 389 Bilateral isoametropic amblyopia , 91 Bilateral keratitis , 239 Bilateral sixth nerve palsy , 508 Binocular vision
diplopia , 27 fusion , 26–27 fusional vergence amplitudes , 27 horror fusionis , 28 monofi xation syndrome , 26 , 27 sensory and motor fusion , 27 stereopsis , 27 visual confusion , 27
Blau syndrome , 226 Blepharophimosis, ptosis, and epicanthus inversus syndrome
(BPES) , 660 Blepharoptosis
blepharophimosis syndrome , 663 BPES , 660 and chronic progressive external ophthalmoplegia , 661 complications , 664 congenital ptosis , 664 cranial nerve III paresis , 660 craniofacial and genetic syndromes , 660 diagnostic evaluation , 661–662 double elevator palsy , 660–661 Fasanella–Servat procedures , 664 frontalis suspension procedure , 664 Horner syndrome , 661 , 663 Kearns–Sayre syndrome , 661 levator muscle , 659 Müller’s Muscle resection , 664 myasthenia gravis , 660 myotonic dystrophy , 661 ptosis , 660–662 superior tarsal muscle , 659 surgical management , 662 Synkinetic syndromes , 661
Boente, C.S. , 135–138 , 141–145 Bosch, M.M. , 366 Boston Children’s Hospital (BCH) , 410 , 411 Bourneville disease , 370–372 Bowsher, J.D. , 605 , 606 , 608 , 610 BPES . See Blepharophimosis, ptosis, and epicanthus inversus
syndrome (BPES) Brachytherapy , 390 , 391 Bradfi eld, Y.S. , 469–472 , 474 Brodie, S.E. , 321–324
Index
802
Brodsky, M.C. , 606 Brown syndrome , 628 , 630 , 631
alternate cover test , 627 anomalous head posture , 630 diagnosis , 624 E.O.M. , 624 left brown syndrome
F.D.T. , 627 , 629 , 630 head turn status , 630 , 631
management , 624 oblique surgery , 630 right eye , 624 , 625
alternate cover test , 628 ocular motility profi le , 628
silicone expander , 630 Y-pattern exotropia , 626 , 627
Brown, H.W. , 623 Broxterman, E. , 635 , 637–639 Brugha, R.E. , 669 B-scan ultrasonography , 400 , 402 , 563 B-scan ultrasound , 402 Buck, D. , 538
C CAIs . See Carbonic anhydrase inhibitors (CAIs) Calhoun, J.H. , 750 Campagna, M. , 412 Capillary hemangioma , 689 Carbonic anhydrase inhibitors (CAIs) , 442 Carrai, P. , 213–217 , 219 , 220 , 251 , 253–256 Cataracts , 366 , 737 Cat-scratch disease (CSD)
antibiotic therapy , 239 diagnosis , 239 immunocompetent patients , 239 neuroretinitis , 239 ocular complication , 239 transmission , 239
Cavernous hemangioma , 691 Cavuoto, K.M. , 641–646 CBC . See Complete blood count (CBC) CCDD . See Congenital cranial dysinnervation disorders (CCDD) Centers for Medicare and Medicaid Services (CMS) , 329 Central corneal thickness (CCT) , 203 Central, steady, and maintained (CSM) , 445 Central, steady, and unmaintained (CSuM) , 445 CGRN . See Childhood Glaucoma Research Network (CGRN) Chandler, J.R. , 668 Chemotherapy , 388–390
retinoblastoma intra-arterial , 388–390 intravenous , 388 , 389 intravitreal , 390 periocular , 390
Child physical abuse , 317 Child Protective Services (CPS) , 313 Childhood glaucoma , 448–454
acetylcholine , 454 Ahmed valve chamber , 455 angle surgery , 454 anterior chamber , 454 classifi cation , 439–440 corneal abrasion
anterior segment examination , 450 Axenfeld-Rieger (AR) spectrum disorder , 450 genetics evaluation , 450
glaucoma-fi ltering surgery , 450 gonioscopy , 450 management , 450 optic nerves , 450 prominent posterior embryotoxon , 450
cycloablation , 455 esotropia
anterior segment examination , 453 B-scan ultrasound , 453 dome-shaped hyperechoic mass , 453 enucleation vs . intra-arterial chemotherapy , 454 Icare ® , 453 posterior segment examination , 453 retinoblastomas , 454 vitreous cavity , 453
eye pain acetazolamide , 452 anterior chamber , 451 , 452 anterior segment examination , 450–452 apraclonidine , 452 B-scan , 451 fi brinous membrane , 451 fl at retina and choroid , 451 goniotomy , 452 juvenile idiopathic arthritis (JIA) , 451 keratic precipitates (KP) , 451 medical and surgical therapies , 452 palpation , 450 posterior segment examination , 451 scleral depression , 451 Tonopen ® , 451 , 452 ultrasound biomicroscopy , 451 uveitis , 451 , 452
fi ltering surgery , 454 glaucoma drainage devices , 455 juvenile open-angle glaucoma , 448 pediatric glaucoma , 439 pediatric glaucoma surgery , 454 right eye pain
anterior segment examination , 452 , 453 B-scan , 452 C/D ratio measure , 453 carbonic anhydrase inhibitors (CAIs) , 453 ciliary body band , 453 gonioscopy , 453 hand motion (HM) , 452 hyphema , 453 Icare ® , 452 intact posterior segment , 452 management , 453 Tonopen ® , 452 , 453
Schlemm canal , 454 scleral fl ap , 454 secondary amblyopia and strabismus , 439 strabismus , 455 Sturge–Weber Syndrome
anterior segment examination , 448 antiepileptics and stroke , 448 bimodal distribution , 449 C/D ratio , 449 choroidal hemangioma , 449 glaucoma drainage device (GDD) , 449 glaucoma drainage valve , 449 gonioscopy , 449 medical and surgical management , 449 posterior segment examination , 449 Prominent superior and inferior arcuate defects , 449
Index
803
trabeculotomy , 454 viscoelastic device , 454
Childhood Glaucoma Research Network (CGRN) , 439 Children’s Hospital of Philadelphia (CHOP) ROP algorithm , 301 Chorioretinitis , 238 Choroidal neovascularization (CNV) , 402 Choroideremia , 283 Choudhary, M. , 593–596 , 598–602 Chromosomal microarray (CMA) , 331 Clefting syndromes , 712–713 CLIA . See Clinical Laboratory Improvement Amendments (CLIA) Clinical activity score (CAS) system , 562 Clinical assessment score (CAS) system , 562 Clinical Laboratory Improvement Amendments (CLIA) , 329 Cloquet canal , 193 CMA . See Chromosomal microarray (CMA) CMS . See Centers for Medicare and Medicaid Services (CMS) CMV . See Cytomegalovirus (CMV) CNV . See Copy number variation (CNV) Coats’ disease , 194 , 354 Cohen syndrome , 205–206 Colobomatous microphthalmia
classifi cation , 398 , 400 Combined hamartomas of the retina and RPE (CHRRPE) , 366 Comparative genomic hybridization (CGH) , 335 , 336 Complete blood count (CBC) , 451 Compound heterozygous , 335 Computed tomographic (CT) , 564 Cone dysfunction , 295 Cone rod dystrophy , 278–281 Confocal scanning laser ophthalmoscope (cSLO , 263 Congenital cataract, right eye
history , 463 interval history (1 year) , 463 management , 463 pseudophakic glaucoma , 463
Congenital cranial dysinnervation disorders (CCDD) , 526 follow-up examination , 602 impression , 601 management , 601 ocular motility , 593 rationale , 601–602
Congenital esotropia . See Infantile esotropia Congenital Esotropia Observational Study (CEOS) , 484 Congenital fi brosis of the extraocular muscles (CFEOM)
amblyopia , 598 A-pattern strabismus , 599 exotropic fi brosis cases , 599 extraocular muscles , 600 head posture and ocular deviation , 600 horizontal rectus transposition , 600 hypertropia , 599 hypotropia , 599 inferior rectus , 600 inferior rectus recession , 599 , 600 Möbius syndrome , 600 nasal transposition, inferior rectus , 600 paralytic and fi brotic muscle , 600 planning surgery , 600 plication , 600 ptosis , 598 stay sutures , 599 strabismus and abnormal head posture , 598–600 strabismus surgery , 599 superior rectus resection , 599 synergistic horizontal divergence , 600 vertical and horizontal overcorrections , 600
Congenital glaucoma , 144 , 145 Congenital orbital cystic lesions
dermoid cysts , 684 microphthalmia with cyst , 682–683 teratoma , 684–685
Congenital sixth nerve palsy , 506–507 Congenital stationary night blindness (CSNB) , 293 Conjunctivitis , 103
characteristics , 103 childhood , 103 infectious viral and bacterial , 103 noninfectious , 103 serotypes , 103
Copy number variation (CNV) , 335 Corneal anesthesia
amniotic membranes act , 133 anesthetic corneas , 133 anti-infl ammatory agents , 133 antimicrobial therapy , 132 Apert syndrome , 130 autologous serum , 133 categories , 129 classifi cation, congenital corneal anesthesia , 130 craniosynostoses , 130 cyanoacrylate , 132 epithelial keratopathy , 129 eyelid-altering diseases , 130 familial congenital corneal anesthesia and familial trigeminal
anesthesia , 131 fungal cultures , 132 history and exam elements , 132 interpalpebral distance , 131 lagophthalmos , 129–132 nerve growth factors and neurotransmitters , 129 orbicularis oculi muscle dysfunction , 130 palpebral insuffi ciency , 130 pediatric corneal anesthesia and exposure keratopathy , 133 punctal occlusion , 133 treatment , 132
Corneal leukoma , 135 Corticosteroids , 560 Costenbader, F.D. , 480 Costin, B.R. , 675–679 Cotter, S.A. , 83 , 88 Cover testing
cycle mode and distance fi xation , 9 occluder , 9 strabismus and motor fusion state , 9
Cover-uncover test , 9 CPS . See Child Protective Services (CPS) Cranial nerve III palsy
amblyopia , 528 aneurysms , 526 bilateral congenital , 526 cranial surgery/neurosurgery , 526 diagnosis , 526–527 infectious and infl ammatory etiologies , 526 levator palpebrae muscles , 525 management , 527 medical records , 526 muscles , 525 neoplastic causes , 526 oculomotor palsy , 525 orthotropia , 528 population-based study , 526 spontaneous resolution , 531 vascular abnormalities , 526
Index
804
Cranial nerve palsies , 240 , 635 , 637 , 639 Cranial Nerve VI (CN VI) , 506 Craniofacial disorders
amblyopia , 719 craniosynostosis , 719 , 720 cycloplegic refraction , 719 diplopia , 719 horizontal rectus muscle surgery , 720 ocular torticollis , 720 strabismus , 719
Craniosynostosis , 719 Apert syndrome , 710 bone growth , 707 brain and cerebral spinal fl uid (CSF) , 707 branchial arches , 706 calvarium , 707 clefting anomalies , 706 clefting syndromes , 712–713 craniofacial deformities , 705 Crouzon syndrome , 709–710 , 716 fetal development, facial prominences , 706 hemifacial microsomia , 715 hypertelorism , 707 maxillary and mandibular prominences , 706 nasolacrimal groove forms , 706 neonatal calvarium , 707 nonsyndromic , 707–708 ophthalmic sequelae , 705 pediatric skull and cranial sutures , 707 Pfeiffer syndrome , 712 Saethre–Chotzen syndrome , 710 , 711 skull/neurocranium , 707 syndromic craniosynostosis and ophthalmic considerations , 708 transgenic animal models , 707 Virchow’s law , 707
Craniosynostosis syndromes , 584 Crouzon syndrome , 709–710 , 716 , 720 Cruz, O.A. , 570 , 573 Cryotherapy
retinoblastoma , 390 Cryotherapy for retinopathy of prematurity (CRYO-ROP) , 302 CSD . See Cat-scratch disease (CSD) CSM . See Central, steady, and maintained (CSM) CSNB . See Congenital stationary night blindness (CSNB) CSuM . See Central, steady, and unmaintained (CSuM) Cyclodialysis cleft , 307 , 309 Cycloplegia , 761 Cystoid macular edema (CME) , 216 , 224 Cytomegalovirus (CMV) , 119 , 244
D 4 Δ base-out prism test , 32 Dacryocystitis , 655 , 656 Dal Canto, A.J. , 563 , 571 , 575 Davitt, B.V. , 573 Dawson, E. , 625 de Haas, V. , 412 de Morsier syndrome , 396 De novo , 335 Deacon, B.S. , 183–189 Del Monte, M.A. , 495–497 , 499–502 , 613 , 614 , 616–621 Demyelinating optic neuritis (DON) , 431–436 , . See also Ancillary
ophthalmic testing with abnormal brain MRI , 437 diagnostic criteria , 430
diseases with ADEM , 431–433 MS , 433–436 NMO , 433
idiopathic monophasic/chronic/recurrent demyelinating condition , 430
long-term management , 436 with normal brain MRI , 436 with suspected NMO , 437 treatment , 436 unilateral/bilateral asymmetric cases , 430
Deprivation amblyopia , 82 , 83 , 95 Dermoid cysts , 684 Descemet stripping automated endothelial keratoplasty
(DSAEK) , 137 Devic disease . See Neuromyelitis optica (NMO) DHD . See Dissociated horizontal deviation (DHD) Dhoot, S.B. , 313–318 Diamond, G.R. , 720 Diffuse unilateral subacute neuroretinitis (DUSN)
electroretinographic changes , 237 unilateral vision loss , 238
Diode cyclophotocoagulation (CPC) , 458 Dissociated horizontal deviation (DHD) , 605 Dissociated strabismus complex (DSC) , 605 Dissociated torsional deviation (DTD) , 605 Dissociated vertical deviation (DVD) , 484 , 585
anti-elevation syndrome , 607 DHD and DTD , 605 elevation movement , 605 Hering’s Law , 605 high-grade fusional mechanisms , 606 hypertropia , 605 infantile esotropia , 606 inferior oblique , 606 latent nystagmus , 606 quantitative measurements , 606 refi xation movements , 606 surgical management , 606 treatment , 606 visual axis , 605
DON . See Demyelinating optic neuritis (DON) Dosso, A.A. , 105 Dosunmu, E.O. , 439–455 , 457–465 Double Maddox rod test
cyclodeviation , 20 excyclodeviation , 20 incyclodeviation , 20
Down syndrome (DS) , 501 accommodation insuffi ciency , 740 behavioral/tactile sensory , 741 brushfi eld spots , 735 , 736 cataracts , 737 , 738 cognitive disabilities , 735 cycloplegia , 741 esotropia , 737 excimer laser keratorefractive procedures , 741 eyelid and orbit , 739 genetics , 736 glasses , 741 glaucoma , 739 head-tilt esotropia , 736 intellectual disability , 735 keratoconus , 738–739 management , 741 Mohindra retinoscopy , 741
Index
805
myopia , 739 nasolacrimal system obstruction , 739 nystagmus , 737–738 palpebral fi ssure , 735 , 740 pediatric/general ophthalmologist , 742 person-fi rst language , 742 refractive correction , 741 refractive errors , 739–740 screening , 741–742 strabismus , 736–737 torticollis , 739
Down, J.L. , 735 , 739 DSAEK . See Descemet stripping automated endothelial keratoplasty
(DSAEK) DSC . See Dissociated strabismus complex (DSC) DTD . See Dissociated torsional deviation (DTD) Duane retraction syndrome , 507
amblyopia , 550 autopsy , 547 bilateral medial rectus recession , 552 concomitant recession, superior rectus muscles , 552 congenital cranial dysinnervation disorder , 548 diagnosis , 550 electromyography , 548 esodeviation , 553 esotropia , 548 examination , 550–551 exotropia , 548 genetics , 550 , 551 horizontal muscle resection , 552 ipsilateral recession, single rectus muscle , 551–552 management , 550–552 Marcus Gunn Jaw-Winking , 549 nonsurgical management , 551 occlusive penalization therapy , 554 orthophoria , 553 strabismus , 550 surgical management , 551–552 types , 548–550 unilateral recession, medial and lateral rectus muscles , 552 vertical muscle transpositions , 552
Duane syndrome , 484 Duction test
Brown syndrome , 17 limitations, movement , 17
Duncan, J.E. , 271–275 , 277 , 281 , 283–285 , 287 Dunn, W.J. , 567 Dupps, W.J. , 129–133 Durairaj, V.D. , 676 DUSN . See Diffuse unilateral subacute neuroretinitis (DUSN) DVD . See Dissociated vertical deviation (DVD) Dynamic retinoscopy
hypo-accommodative ability , 765 indications , 765 technique , 765–766
Dysinnervation , 659
E E.O.M. . See Extraocular muscles (E.O.M.) Early treatment for ROP (ETROP) , 302 Ectopia lentis , 200–201
ADAMTSL4 , 202 amblyopia , 202 axial myopia, cataract and retinal detachment , 202–203 craniofacial dysostosis , 205
diagnosis , 201 endocapsular/extracapsular techniques , 207 iridodonesis , 201 lens dislocation , 207 Marfan syndrome , 201 , 202 medical management , 206–207 molybdenum cofactor defects and sulfi te oxidase defi ciency , 205 OD>OS , 201 , 202 phakic and aphakic refraction , 207 pupils , 202 subluxated lenses , 199 , 207 subluxation lenses , 202 sulfate metabolism , 199 Traboulsi syndrome , 202 WMS , 199 zonule , 199
Ectopia Lentis et Pupillae , 202 Eisenberg, M.A. , 613 , 614 , 616–621 El-Dairi, M.A. , 271–275 , 277 , 281 , 283–285 , 287 , 427–431 , 433 ,
435–437 Electroretinography (ERG)
anesthesia , 293 Burian-Allen electrodes , 293 cone dysfunction , 295 Dawson-Trick-Litzkow (DTL) , 293 electrodes and light stimulus , 293 Ganzfeld stimulator , 291 Hawlina-Konec electrode (HK) , 293 indications , 291–293 LCA and RP , 295 photovoltaic effect , 293 protocol , 293 retinal dystrophies , 291 , 292 rod dysfunction , 293–295 skin corneal/skin electrodes , 291 waveform morphologies , 293
Ellis, F.D. , 569 Ellis, F.J. , 659–664 Ellis, G.S. Jr. , 3–15 , 17–23 , 500 Ellsworth, R. , 384 Embryology , 193–194 Encephalofacial angiomatosis , 372 Endogenous endophthalmitis , 245 Endophthalmitis , 642 , 644 Endophytic tumors , 369 Endotheliitis , 124 Enhanced depth imaging (EDI) , 272 Enophthalmos , 675 Enucleation
retinoblastoma , 387–388 Enzyme-linked immunoassay (ELISA) , 234 EOMs . See Extraocular muscles (EOMs) Epidemic keratoconjunctivitis (EKC)
adenovirus , 105 confocal microscopy , 105 punctate keratopathy , 105 steroids , 105 subepithelial infi ltrates , 105 symptoms , 105 viral conjunctivitis , 105
Epiretinal membranes (ERMs) , 224 , 366 , 367 Epithelial keratitis , 121–122 Escott, S.M. , 233–245 Esotropia , 548 Estimated gestational age (EGA) , 301 Exam under anesthesia (EUA) , 656
Index
806
Examinations under anesthesia (EUAs) , 458 Excimer laser treatment , 75 , 76 Exophthalmometry , 675 Exophytic lesions , 370 Exotropia , 526
clinical evaluation , 536–537 exophoria , 535 infantile exotropia , 535 , 536 intermittent , 537 intermittent exotropia , 536 lazy left eye infant , 542–544 minus lens therapy , 537–538 occasional drifting , 539 , 540 outward drifting , 540–542 part-time occlusion , 537 pseudoexotropia , 535 sensory , 536 surgical intervention , 538 , 539
Extraocular muscle entrapment , 676 , 678 Extraocular muscles (EOMs) , 526 , 624
CFEOM1 , 594 CFEOM2 , 594 CFEOM3 , 594–595 unilateral/bilateral involvement , 594
F FDT . See Forced duction testing (FDT) FAF . See Fundus autofl uorescence (FAF) Faivre, L. , 203 Familial adenomatous polyposis (FAP) , 372 Familial exudative vitreoretinopathy (FEVR) , 195 , 355 Farkas, L.G. , 713 Feldon, S.E. , 561 FEVR . See Familial exudative vitreoretinopathy (FEVR) FGFR . See Fibroblast growth factor receptors (FGFR) Fibroblast growth factor receptors (FGFR) , 707 Fibrosis of extra-ocular muscles , 632 Fisher, M.J. , 363 , 412 , 413 Fluorescein angiography , 382 Fluorescein angiography (FA) , 262 , 263 , 265 FMNS . See Fusion maldevelopment nystagmus syndrome (FMNS) Forced duction testing (F.D.T.) , 627 Foster, J. , 705–708 , 710 , 712–716 Foster, R.S. , 509 , 552 Foveal hypoplasia , 285 Freedman, S.F. , 271–275 , 277 , 281 , 283–285 , 287 , 439–455 , 457–465 Frontalis sling , 527 Fuchs heterochromic iridocyclitis (FHI) , 244 Fundus autofl uorescence (FAF) , 265 Fundus camera , 263 Fungal keratitis , 113 , 114
corneal perforation , 114 diagnosis , 113 pathogenesis , 113 risk factors , 113 treatment
amphotericin B , 113 epithelial toxicity , 114 polyenes , 113
Fusion maldevelopment nystagmus syndrome (FMNS) Alexander’s law , 748 blockage syndrome , 749 defi nition , 748 eye movements , 748 fogging technique , 749
neurologic/ocular causes , 748 Fusional vergence amplitude testing
amblyoscope , 18 deviations , 19 prism amount , 19 single binocular vision , 18
G Gair, E.J. , 567 Ganglion cell layer-inner plexiform thickness (GCL-IPL) , 363 Gappy, C. , 479 , 480 , 484–486 Garcia, G. , 669 Gardner Syndrome , 372 GCS . See Glasgow Coma Score (GCS) Gene Tests , 380 Genetic counseling
Axenfeld–Rieger syndrome , 332 bilateral Legg–Calve–Perthes disease vs . multiple epiphyseal
dysplasia , 332 comparative genomic hybridization (CGH) , 332 dysplasia , 332 fundus and optic nerve , 332 healthcare professionals , 331 process , 331
Genetic testing AAO , 331 AAP and ACMG , 331 achromatopsia , 333 , 334 amblyopia , 333 CLIA , 329 CMA , 331 CMS , 329 cost , 329–330 EFEMP3 causes , 330 family history , 330–331 fundus images , 334 , 335 juvenile X-linked retinoschisis , 333 laboratory reputation , 330 microarray , 330 NGS , 330 nystagmus , 333 predictive genetic testing , 331 PS and KSS , 334 retinal dystrophy , 333 turnaround time , 330 WES , 330
Ghasia, F.F. , 81–97 , 747–752 Gigliotti, F. , 104 Glasgow Coma Score (GCS) , 316 Glaucoma , 151 , 273–274 , 739 Goldberg, M.F. , 191 Goldenhar syndrome , 713 Goldman, R. , 669 Goldmann visual fi eld testing , 431 Goldstein, D.A. , 233–245 Goniotomy , 441 , 444 , 452 , 454 Gonococcal conjunctivitis , 107 Gradenigo’s syndrome , 508 Graves disease , 687 Gray, M.E. , 167–171 Greenberg, M.F. , 552 Greenstick fracture . See Trapdoor fractures Gregg, F.M. , 95 Group A retinoblastoma , 390 Group C retinoblastoma , 391
Index
807
Group D retinoblastoma , 389 Gu, S. , 363 Gupta, N. , 161 Guyton, D.L. , 614
H Hanson, L L. , 175–181 Haploscopic tests , 33 Harada , 229 Harley, R.D. , 750 Harris, G. , 669 Harrison, D.A. , 207 Harvey, E.M. , 38 Hatt, S.R. , 537 HEDS . See Herpetic Eye Disease Study Group (HEDS) Heidary, G. , 407–413 Hemangioblastomas
retinal and optic nerve head , 369–370 Hematologic tumors
histiocytic , 694–695 leukemia and lymphoma , 694 xanthogranuloma , 695
Hemifacial microsomia , 713 , 715–716 Hemizygous , 335 Herpes simplex keratouveitis , 240–241 Herpes simplex virus (HSV)
anterior segment , 120 blepharoconjunctivitis and periocular disease , 120–121 endotheliitis , 124 epithelial keratitis , 121–122 herpetic disease , 120 iritis , 124–125 neonatal ocular , 125 stromal keratitis , 122–124
Herpes simplex virus-1 (HSV-1) , 114 Herpes zoster ophthalmicus (HZO) , 242 Herpetic Eye Disease Study Group (HEDS) , 120 Herring’s Law , 8–9 Hertle, R.W. , 710 Hess, R.F. , 96 Heterochromia , 254 Heterozygous , 335 Hirschberg method , 14 Histoplasmosis , 244–245 Homocystinuria , 204–205 Homozygous , 335 Hood, C.T. , 109–116 Horizontal muscle displacement/transposition , 588 Horner syndrome , 661 Hubel, D.H. , 82 Human Adenovirus Working Group , 104 Humphrey visual fi eld (HVF) , 431 Humphrey Visual Field 24-2 SITA Standard , 473 , 474 Hung-up syndrome , 628 , 630 Hutcheson, K.A. , 502 HVF . See Humphrey visual fi eld (HVF) Hyperdeviations
hypertropia , 610 incyclotorsion , 610 inferior oblique overaction , 608 skew deviation , 610 superior oblique muscle , 610
Hyperlysinemia , 205 Hypermetropia in infancy , 39 , 41 , 42
AAPOS , 39 AAPOS survey , 38
algorithm, evaluation and management , 40 amblyopia and strabismus , 39 combination , 37 correction , 42 cycloplegic refraction , 39 cycloplegic refractive errors , 38 esodeviation , 37 esotropia , 37 moderate levels , 38 outcomes , 38 , 42 PEDIG , 39 prescribing practices and screening guidelines , 38 prescription , 39 refractive correction , 38 retinoscopy , 39 strabismus and amblyopia , 37 visual acuity
amblyopia , 41 central, steady and maintained (CSM) , 39 CSM OU , 39 high hypermetropia with pseudoesotropia , 41 isolated bracketed HOTV , 41 , 42 management options , 39 , 41 single optotype , 41
Hyphema , 242 , 254 clinical features , 150 complications , 149 , 151 examination , 152 injury , 150 management , 152 medical management , 150 , 151 pathophysiology , 150 sickle cell trait , 152 surgical management , 151 trauma , 149
Hypotropia , 526 HZO . See Herpes zoster ophthalmicus (HZO)
I Iannaccone, A. , 411 ICGA . See Indocyanine green angiography (ICGA) Idiopathic intermediate uveitis , 224 Idiopathic intracranial hypertension . See Pediatric pseudotumor
cerebri syndrome (PTCS) Immunomodulatory therapies (IMT) , 223 Incomitant strabismus , 636 , 639 Incontinentia pigmenti , 356 Indocyanine green angiography (ICGA) , 265 Infant Aphakia Treatment Study (IATS) , 96 , 458 Infantile cataracts , 183 , 186–188
evaluation , 175 , 177 , 178 familial bilateral congenital cataracts , 179 , 180 informed consent , 189 inherited causes , 175–177 parental counseling , 189 pediatric (see Pediatric cataracts ) post-surgical issues
age and surgical timing , 187 posterior capsule opacifi cation , 188 surgical technique , 187 , 188
surgery morphology , 187 surgical intervention , 186 , 187
systemic disorders , 180–181 systemic evaluation , 177 unilateral congenital cataract , 178 , 179
Index
808
Infantile esotropia , 485 , 486 algorithm , 486 amblyopia , 485 binocular vision , 479 , 480 CEOS , 484 Chavasse’s theory , 480 cross fi xation , 479 DVD , 484 eye fi xating and left eye deviating , 481 IOOA , 484 Krimsky method , 484 , 485 latent nystagmus , 484 management , 485 monofi xation syndrome , 480 ophthalmic examination , 484 refractive errors , 484 right esodeviation and hypertropia , 483 , 484 smooth pursuit asymmetry , 484 strabismus , 479 treatment
bilateral medial rectus recessions/unilateral recess–resect procedure , 485
botulinum toxin , 485 CEOS , 485 orthotropia , 485 strabismus , 486
Worth’s sensory theory , 479 Infantile hemangioma , 689 Infantile nystagmus syndrome (INS)
defi nition , 749 eye positions , 750 foveal morphology , 750 FRMD7 gene , 751 head oscillations , 750 Kestenbaum procedure , 750 , 751 OCT , 751 structural eye abnormalities , 751 vertical rectus muscles , 751
Infectious endophthalmitis , 245 Infectious uveitis , 233–245
bacterial CSD , 239 intraocular tuberculosis , 240 Lyme disease , 239 , 240 syphilis , 238–239
fungal endogenous endophthalmitis , 245 histoplasmosis , 244–245
parasitic DUSN , 237 toxocariasis , 236–237 toxoplasmosis , 233–235
viral CMV , 243 , 244 herpes simplex keratouveitis , 240–241 necrotizing retinitis , 242–243 Rubella , 244 VZV , 241 , 242
Inferior oblique overaction (IOOA) , 484 , 606 hypertropia , 608 infantile esotropia , 607 superior oblique muscle , 608 superior oblique palsy , 608
Inferior Oblique Palsy , 627 Inferior orbital wall fractures
enophthalmos , 675 entrapped and non-entrapped , 676
history and examination , 675 ophthalmic examination , 675 ( see also Pediatric orbital fl oor
fractures ) surgical intervention , 676 trauma , 675
Infl ammatory lesions nonspecifi c orbital infl ammation , 685–686 ruptured dermoid cyst , 687–688 thyroid eye disease , 686–687
Informed consent advantages , 189 amblyopia therapy , 189 cataract surgery , 189 implantation , 189 optical rehabilitation , 189 pediatric cataract surgery , 189 unilateral infantile cataracts , 189
Infrared imaging , 265 Ingram, R.V. , 37 INS . See Infantile nystagmus syndrome (INS) Insulin-like growth factor 1 (IGF-1) , 300 Intermittent exotropia , 535–537 , 539 Intermittent exotropia control scale (IXTCS) , 537 International Classifi cation for ROP (ICROP) , 300 International League of Associations for Rheumatology (ILAR) , 213 International Society for Clinical Electrophysiology of Vision
(ISCEV) , 293 Intraocular foreign body (IOFB) , 308 Intraocular lens (IOL) , 216 Intraocular pressure (IOP) , 457
corneal blood staining , 151 elevation , 151 injury , 150 traumatic hyphema , 150
Intraoperative relaxed muscle technique , 570 Intraoperative relaxed muscle technique (IRMT)
contralateral eye , 570 cross-swords technique , 570 diplopia , 571 distal rectus tendon , 570 inferior rectus recession , 571 Westcott scissors , 570
IOFB . See Intraocular foreign body (IOFB) IOOA . See Inferior oblique overaction (IOOA) IOP . See Intraocular pressure (IOP) Iridodonesis , 201 Iris hamartomas (Sakurai-Lisch nodules) , 360 , 363 Iritis , 124–125 Irregular astigmatism
conditions , 51 corneal or lenticular , 51 corneal scarring , 55 , 56 corneal topography , 51 diagnosis , 51 Keratoconus suspect , 54 , 55 Marfan syndrome , 57
ISCEV . See International Society for Clinical Electrophysiology of Vision (ISCEV)
Isenberg, S.J. , 500 IXTCS . See Intermittent exotropia control scale (IXTCS)
J Jain, A. , 668 Janse, A.J. , 366 Joseph, D.P. , 169 Jotterand, V.H. , 500
Index
809
Juthani, V. , 129–133 Juvenile (psammomatoid) ossifying fi broma , 697 Juvenile idiopathic arthritis (JIA) , 216 , 217
abatacept , 220 adalimumab , 219 adherence , 216 biologic agents , 219 cataract , 217 children and adolescents , 215 classifi cation , 213 , 214 complications , 214 etanercept , 219 eye infl ammation , 214 folinic acid , 219 golimumab , 219 IL-1 inhibitors , 219 IL-6 inhibitors , 220 ILAR , 213 immunomodulators , 219 infl iximab , 219 methotrexate and adalimumab , 217 methotrexate therapy , 217 MTX , 217 multidisciplinary approach , 216 OCT , 217 ocular complications
band keratopathy , 216 cataracts , 216 CME , 216 cystoid macular edema , 217 IOL , 216 macular edema , 216 microvascular factors , 217 viscoelastic , 216
pathogenesis , 214 pediatric age group , 213 pediatric rheumatology and ophthalmology community , 220 rituximab , 220 SD-OCT , 218 short-term and long-term functional outcomes , 215 sustained-release dexamethasone implant , 217 , 218 TNF-α , 219 tocilizumab , 220 treatments , 215 uveitis , 214–216
Juvenile open-angle glaucoma (JOAG) anterior segment , 471 automated visual fi eld testing , 470 cycloplegic refraction , 472 diagnosis , 472 diagnosis and management algorithm , 470 , 471 follow-up examination , 472 genetic testing , 470 glaucoma , 469 GLC1 , 469 gonioscopy , 469 IOP , 470 myopia , 469 OCT , 470 optic nerve cupping OU , 470 pachymetry , 471 pertinent examination , 472 planning , 472 posterior segment , 471 postoperative follow-up appointment (2 months) , 472–474 postoperative follow-up appointment (one-week) , 472
sensorimotor , 470 Tono-Pen ® , 470 treatment , 470
Juvenile ossifying fi broma , 698 Juvenile xanthogranuloma (JXG) , 253–255 Juvenile X-linked retinoschisis , 278
K Kasabach–Merritt syndrome , 690 Kaufman, A.H. , 119–127 Kaufman, A.R. , 119–127 Kazim, M. , 560 Kearns–Sayre syndrome (KSS) , 334 Kekunnaya, R. , 552 Kelly, J.P. , 412 Keratoconus , 738–739 Kerr, N.C. , 559–564 , 566–571 , 573 , 575 , 577 Kestenbaum procedure , 750 , 751 Kestenbaum, A. , 750 Khan, A.O. , 202 , 507 Kim, S.H. , 400 Kim, T. , 155–165 Kivlin–Krause syndrome , 135 Knapp procedure , 527 Knox, D.L. , 507 Knudson, A.G. , 379 , 380 Kovarik, J.J. , 605 , 606 , 608 , 610 Koyanagi , 229 Kraft, S.P. , 552 Kraus, C.L. , 183–189 Krimsky method , 14 , 485 Kuhn, F. , 167 Kumar, P. , 191 , 193–197 , 379–391 Kushner, B.J. , 500
L Laithier, V. , 412 Lam, G.C. , 86 Langerhans cell histiocytosis (LCH)
classifi cation , 694 histiocytic vascular infi ltrate , 694
LaRoche, G.R. , 489–493 Laser therapy
retinoblastoma , 390 LASIK , 75 Latent deviations
detection , 10–11 vs . manifest deviations , 11–12 measurement , 11
Latent nystagmus , 748–749 LCA . See Leber congenital amaurosis (LCA) Leber congenital amaurosis (LCA) , 281–283 , 295 , 345–348 Leber’s hereditary optic neuropathy (LHON) , 760 Lee, J. , 507 , 625 Leigh, R.J.Z.D. , 752 Lens opacity , 177 Leukemia , 253 Leukocoria , 381 , 386 Levodopa , 94 LHON . See Leber’s hereditary optic neuropathy (LHON) Lim, S.A. , 760 Limbal stem cell defi ciency (LSCD)
corneal scarring , 164 fi lamentary keratitis , 164
Index
810
Lin, J. , 291 , 293 , 295 Lindquist, T.P. , 505–510 Liu, G.T. , 418–424 Logarithm of minimal angle of resolution (logMAR) , 5 logMAR . See Logarithm of minimal angle of resolution (logMAR) Longmuir, S.Q. , 316 Loose lenses vs . phoropter , 761 Lowder, C. , 213–217 , 219 , 220 , 251 , 253–256 Low-fl ow malformations (LFMs)
distensible , 693 lymphatic dominant LVMs (LD-LVMs) , 692 nondistensible , 691 , 693 venous dominant LVMs (VD-LVMs) , 692
LSCD . See Limbal stem cell defi ciency (LSCD) Lueder, G.T. , 569 , 577 Lusk, K. , 725 , 726 , 731–733 Lyme disease
bilateral keratitis , 239 diagnosis , 239 , 240 mild conjunctivitis , 240 retinal vasculitis , 239 stages , 239
Lymphoma , 253 Lyons, S.A. , 38
M Maddox rod test
advantage , 13 prim bar/rotary prism , 13 strabismus , 12
Mahoney, N.R. , 507 Malalis, J.F. , 233–245 Malformations , 395
optic nerve (see Optic nerve malformations ) Malingering
after eye trauma , 759 vision loss , 757
Manifest deviation detection , 9–10 vs . latent deviation , 11–12 measurement , 10
Mantyjarvi, M.I. , 758 Marcotty, A. , 535–537 , 539–543 , 651 , 652 , 654–656 Marfan syndrome
amblyopia , 203 beta-blocking agents , 204 corneal curvature , 203 FBN1 molecular testing , 203 fi brillin 1 , 203 fi brillin fi bers , 203 infants and children , 204 keratometry and CCT values , 203 kyphoscoliosis , 203 lens extraction , 204 Losartan ® , 203 microspherophakia , 203 open angle glaucoma , 204 stretched and rarifi ed zonules , 203 , 204 subluxation lens , 203 transforming growth factor-beta neutralizing antibodies/losartan ,
203 Marfan, A. , 203 Marino, M.J. , 329–336 Masquerade syndromes , 251–255
diagnostic algorithm , 257 malignant
leukemia , 253 lymphoma , 253 retinoblastoma , 251 , 252
nonmalignant JXG , 253 , 254 occult intraocular foreign bodies , 255 orbital pseudotumor , 255 retinal detachment , 255
Mazow, M.L. , 569 McCormack, S.E. , 418–424 McGregor, M.L. , 719 , 720 , 722 McKeown, C.A. , 641–646 Medina, C.A. , 379–391 Meghpara, B. , 243 Mehendale, R.A. , 552 Mesenchymal tumors
fi bro-osseous tumors , 697 , 698 leiomyoma , 698 orbital rhabdomyosarcoma , 695 , 697
Metabolic disorders , 175 , 180 Microcephaly , 353 , 356 Microphthalmos , 381 Microspherophakia , 203 Mikaeloff, Y. , 433 Miller, J.E. , 568 Miller, J.M. , 38 Miller, N. , 526 , 527 Miyake, N. , 550 Möbius syndrome , 506 , 507 , 600 Moffatt, M.E. , 313–318 MOG . See Myelin-oligodendrocyte glycoprotein (MOG) antibodies Mondok, L. , 757–760 Moreno, L. , 413 Morning glory disc anomaly (MGDA) , 396–399 Mosaic Down syndrome (MDS) , 736 Motley, W.W. , 179 , 181 , 735–737 , 739–742 Motor fusion test
fusional vergence amplitude testing , 18–19 NPC , 19
Mourits, M.P. , 563 Multiple evanescent white dot syndrome (MEWDS) , 268 Multiple sclerosis (MS)
CIS study , 433 diagnosis , 433 MRI , 431 pediatric DON studies , 433 risk of , 433
Myasthenia gravis globe retraction , 638 hospital course , 638–639 myasthenia gravis (MG) , 638
Myelinated nerve fi bers , 404–405 Myelin-oligodendrocyte glycoprotein (MOG) antibodies , 431 Myopia , 47 , 48
axial , 45 , 46 control groups , 48 growth and development, human eye , 46 management
cycloplegic refraction , 48 differential diagnosis , 47 low-grade , 48 progression , 48 retinoscopy , 48 surgical refractive procedures , 48 symmetrical and uncorrected , 48 young children , 48
mild , 47
Index
811
myopic correction , 45 ocular and systemic conditions , 46–47 prevalence , 45 prevention , 48 refractive , 45 , 46 retinopathy, moderate , 47 school-aged , 48 Stickler syndrome , 47 , 48 uncorrected myopic eye’s focal point , 45
Myotonic dystrophy , 661
N Nabavi, C. , 705–708 , 710 , 712–716 Nasolacrimal duct obstruction (NLDO) , 652–655 , 712
amblyopia , 651 congenital glaucoma , 651 , 652 , 656 congenital tear duct obstruction , 651 , 652 , 656 corneal abrasion , 651 , 652 dacryocystitis , 655 , 656 epiphora , 651 , 652 , 657 management
congenital dacryocystocele , 654 , 655 epiphora , 654 NLD compression , 652 , 653 ocular adnexa , 652 offi ce vs . operating room , 654 surgical outcomes , 654–655
Pediatric Eye Disease Investigator Group , 652 tearing , 651
Nasolacrimal system obstruction , 739 Natan, K. , 551 National Center for Biotechnology Information (NCBI) , 330 National Child Abuse and Neglect Data System (NCANDS) , 313 National Society of Genetic Counselors , 380 NCANDS . See National Child Abuse and Neglect Data System
(NCANDS) NCBI . See National Center for Biotechnology Information (NCBI) NCS . See Newcastle control score (NCS) Near point of convergence (NPC)
diplopia , 19 fusional convergence amplitude testing , 19
Necrotizing retinitis , 242–243 ARN , 242
Neonatal conjunctivitis , 103 chemicals , 107 chlamydia , 107 erythromycin , 107 gonorrhea , 107 N. gonorrheae , 107 Neisseria , 107 ophthalmia neonatorum , 107 pathogens , 107 perinatal transmission , 107 prophylaxis , 107
Nerve palsy, children amblyopia , 515 bilateral palsy , 517 Brown syndrome , 516 congenital cases , 513 diplopia , 517 esodeviation , 516 excyclotorsion , 514 , 517 , 519 facial asymmetry , 514 fundus torsion , 516 hypertropia , 513 , 516 hypertropias , 517
intracranial mass/stroke , 517 ipsilateral inferior oblique recession , 517 Knapp classifi cation , 515 motor nerve , 513 muscle surgery , 516 ocular movements , 516 physical therapy , 514 sports-related head injury , 521 superior oblique , 516 superior oblique traction test , 515 Surgical management , 516 three-step Parks-Bielschowsky test , 514 torsion , 521 torticollis , 514 , 517 trauma , 517 , 519 trochlear nerve , 513 vertical fusional amplitudes , 517
Neural tumors optic nerve glioma , 688–689 optic nerve sheath meningioma , 689 orbital schwannomas , 689
Neurofi bromatosis type 1 (NF1) , 407 characterization , 359 diagnosis , 411 features , 410 iris hamartomas (Sakurai-Lisch nodules) , 360 , 363 OPG , 360–364 , ( see also Optic pathway gliomas (OPG) ) orbitotemporal neurofi bromas (plexiform neurofi bromas) , 360 , 364 pVEPs , 411 tissue defi nitions , 360
Neurofi bromatosis type 2 (NF2) case study , 365 cataracts , 366 characterization , 364 diagnostic criteria , 364 mild [Gardner] subtype , 364 ophthalmologic fi ndings , 365 severe [Wishart] subtype , 364
Neurogenic esotropia afferent defects and strabismus , 490–491 children , 489 , 490 descriptions , 489 dilation and cycloplegic refraction , 493 diplopia , 490 , 493 efferent defects and strabismus , 491 hyperopia , 490 MRI , 490 myopia , 492 neuroimaging investigations , 489 neuromotility assessment , 491 nystagmus , 492 ophthalmoscopy , 492 PD , 492 posterior fossa medulloblastoma , 493 sensory adaptation testing and neurologic examination , 493 strabismus , 489 , 493 suppression , 492 , 493
Neuromyelitis optica (NMO) antibodies , 431 description , 430 diagnostic criteria , 433 DON with suspected , 437 in females , 433 MOG antibodies , 433 neurologic symptoms , 433
Neuro-ophthalmologic fi ndings , 366 Neuroretinitis , 239 , 274
Index
812
Newcastle control score (NCS) , 537 Next-generation sequencing (NGS) , 330 , 335 NGS . See Next-generation sequencing (NGS) Nguyen, V.T. , 570 Nicholson, B.P. , 563 , 570 , 571 , 573 Nicolin, G. , 412 NLDO . See Nasolacrimal duct obstruction (NLDO) NMO . See Neuromyelitis optica (NMO) Non-entrapped fractures , 676 Non-ocular tumors
retinoblastoma , 383 Nonorganic visual loss (NOVL)
anxiety-inducing factors , 758 binocular and monocular , 759 clinicians , 760 diagnostic testing , 759 fogging test , 759 functional visual loss , 758 groups , 757 hysterical amblyopia , 758 management , 760 psychogenic amblyopia , 758 Titmus stereo test , 759 visual conversion disorder , 758 visual disturbance , 758 visual fi eld testing , 759
Nonspecifi c orbital infl ammation (NSOI) , 685 biopsy , 686 differential diagnosis , 685 pediatric , 685 , 686
Nonsteroidal anti-infl ammatory drug (NSAID) , 217 Non-treponemal tests , 238 Normal retinal correspondence (NRC)
exotropia , 32 fusional vergence , 27
Norrie disease , 195 , 355 NOVL . See Nonorganic visual loss (NOVL) NPC . See Remote near point of convergence (NPC) Nucci, P. , 251 , 253–256 Nystagmus , 737–738 , 748–751
and eye movement abnormalities , 747 , 749 classifi cation , 748 conjugate/disconjugate , 747 corrective/abnormal eye movement , 747 esotropia , 23 eye movement recordings , 22 eye positions , 748 , 749 INS (see Infantile nystagmus syndrome (INS) ) latent nystagmus (see Fusion maldevelopment nystagmus
syndrome (FMNS) ) ocular and neurologic conditions , 23 ocular fl utter , 752 oculomotor apraxia , 23 opsoclonus , 752–753 pediatric ophthalmology practice , 747 retinal electrophysiologic testing , 748 spasmus nutans , 751 vertical nystagmus in infancy , 751–752 voluntary , 753
Nystagmus blockage syndrome , 749
O Oblique muscle overaction , 584 Oblique muscle surgery
anterior and posterior borders , 584 , 585 anteriorization/anterior transposition , 585
inferior oblique muscle , 584 , 587 inferior rectus muscle , 584 , 588 inferotemporal fornix incision , 584 , 585 intermuscular septum , 584 , 586 superior oblique muscle , 585 , 586
Occult intraocular foreign body , 255 OCT . See Optical coherence tomography (OCT) Octopus visual fi eld analyzer (Haag-Streit AG) , 431 Ocular chemical injury , 161–163
acids , 159 acute management , 155 , 156 alkali , 159 classifi cation , 156 , 157 , 160 , 161 corneal opacifi cation , 164 corneal opacity , 156 cycloplegic refraction , 156 early management , 156 , 157 emergency department , 156 epidemiology , 158 , 159 limbal stem cell defi ciency , 164 long-term management , 157 , 158 medical treatment
acetazolamide , 163 amniotic membrane grafting , 162 beta-adrenergic antagonists , 163 carbonic anhydrase inhibitors , 163 corneal epithelium , 161 corticosteroids , 161 cyclomydril , 163 cycloplegic agents , 163 epithelial defect , 162 infl ammatory reaction , 161 liquid formulations , 162 management , 162 punctal occlusion , 163 safety and effi cacy , 161 stages, corneal wound healing , 162 systemic ascorbate , 162 tetracyclines , 163
phone call , 155 sequelae and surgery , 163–165 signs and symptoms , 159 , 160
Ocular dominance columns , 82 Ocular fl utter , 752 Ocular rosacea , 115 Ocular toxocariasis , 195 , 236 , 237 Ocular toxoplasmosis , 234 , 235 Ocular trauma scores (OTS) , 167 , 168 , 307 O'Doherty, M. , 356 Olitsky, S.E. , 505–510 Open globe injury , 167–169 Ophthalmic abnormalities
amblyogenic ametropia/anisometropia , 713 amblyopia , 713 amblyopia and strabismus , 713 chronic corneal exposure , 714 craniofacial deformity , 713 craniofacial disorders , 713 craniofacial surgeries , 715 craniosynostosis/clefting syndrome , 713 dacryocystitis , 714 dye disappearance test , 714 exophthalmometry , 714 lacrimal outfl ow system , 715 measurement , 713 nasolacrimal duct stenosis , 714 oculoplastic , 715
Index
813
Opremcak, E.M. , 223 , 224 , 226–230 Opsoclonus , 752–753 Optic disc drusen , 402–404 Optic nerve , 472–474 Optic nerve coloboma , 398–400 Optic nerve edema
neuroretinitis , 274 , 277 optic neuritis , 274 , 277 papilledema , 274 , 276
Optic nerve head drusen , 274 Optic nerve hypoplasia (ONH) , 275–277
de Morsier syndrome , 396 defi nition , 395 different pathways and timing in eye development , 396 , 398 double-ring sign , 395 , 396 genetic and environmental associations , 395 , 396 , 398 hypopituitarism , 396 OCT , 395 , 397 prevalence , 395 septo-optic dysplasia , 396 tortuosity of retinal veins , 395 , 396
Optic nerve malformations clinical associations , 404 , 405 MGDA , 396–399 myelinated nerve fi bers , 404–405 ONH , 395 , 396 optic disc drusen , 402–404 optic nerve coloboma , 398–400 optic pit , 399–401 papillorenal syndrome , 399 peripapillary staphyloma , 400–402 tilted disc syndrome , 401–402
Optic neuritis , 274 Optic neuritis in children , 430
differential diagnosis , 427 , 428 DON (see Demyelinating optic neuritis (DON) ) fl uorescein angiogram , 429 grade 2 swelling, optic nerve , 427 , 428 history, case study , 427 neuroretinitis with , 429
Optic neuropathy , 561 Optic pathway gliomas (OPG) , 751
BCH , 410 classifi cation , 410 clinical synopsis , 407–410 diagnosis , 410 , 411 , 413 differentiate NF1-associated and non-NF1-associated , 410 GCL-IPL , 363 guidelines , 363 low-grade designation , 410 low-grade neoplasms , 407 low-grade pilocytic astrocytomas , 360 management and treatment , 412 neurocutaneous disorder , 407 neuroimaging , 363 NF1 , 407 ophthalmic screening , 411–412 ophthalmologic progression , 363 radiographic progression , 363 screening and monitoring , 360 , 364 SD-OCT , 360 symptomatic , 360 VEPs , 360 visual Outcomes , 412–413
Optic pit , 399–401
Optical coherence tomography (OCT) , 217 , 272 , 274 , 275 , 277–286 , 441 AS-OCT , 285 atrophic nerves
compressive lesions , 275 papilledema , 275 RNFL , 274 , 278
bioptigen , 285 chiasmal glioma , 279 genetic retinopathies
batten disease , 283–285 choroideremia , 283 , 284 cone rod dystrophy , 278–282 foveal hypoplasia , 285 , 286 juvenile X-linked retinoschisis , 278 , 281 leber congenital amaurosis , 281–283 pseudohypopyon , 283 rod cone dystrophy , 283 RPE/photoreceptor changes , 277 Stargardt disease , 277–278 , 281 vitelliform dystrophy , 283
glaucoma , 273–274 noninvasive imaging technology , 271 optic nerve edema , 274 optic nerve head drusen , 273 , 274 optic nerve head map , 273 optic nerve head scan , 274 optic nerve hypoplasia , 275–277 , 280 optical waves , 271 retinal nerve fi ber layer , 275 retinal scans
EDI , 272 high-resolution scans , 272 macular maps , 272
retinitis pigmentosa , 284 retinopathy , 285 , 287 RNFL , 273 vitelliform dystrophy , 283
Orbital abscess imaging, role of , 668 with/without intracranial complications , 668
Orbital cellulitis defi nition , 667 ethmoid and maxillary sinuses , 668 ( see also Periocular infections ) polymicrobial , 668 symptoms , 667 treatment of , 669
Orbital pseudotumor , 255 Orbital retinoblastoma , 699 Orbital rhabdomyosarcoma
grouping of , 697 Orbitotemporal neurofi bromas (plexiform neurofi bromas) , 360 , 364 Örge, F.H. , 135–138 , 141–145 Osteoporosis , 354 OTS . See Ocular trauma scores (OTS)
P Paley, G.L. , 418–424 Panuveitis syndromes , 230 Papilledema , 274
diagnostic requirements , 418 dilated fundus examination , 418
Papillorenal syndrome , 399 Para-arteriolar retinal pigment epithelium (PPRPE) , 345 Parental counseling , 189
Index
814
Parinaud oculoglandular syndrome , 239 Park, K.A. , 402 Parks, M.M. , 95 , 480 , 500 , 750 Parrozzani, R. , 360 Pars planitis
active infl ammatory cells , 226 aphakia , 226 biomicroscopic examination , 224 chronic cyclitis and peripheral uveitis , 224 cystoid macular edema , 226 fl uorescein angiography , 226 inactive and old cells , 226 lensectomy , 226 periocular steroid injections , 226 retinal vasculitis and granulomatous infl ammation , 224 snowbanking and collagen band formation , 225 “step ladder” treatment approach , 226
Patel, C.K. , 513 , 514 , 516 , 517 , 521 Pattern reversal VEPs (pVEPs) , 411 Pearson syndrome (PS) , 334 Pediatric cataract surgery , 188 , 189 Pediatric cataracts
additional tests , 184 , 185 classifi cation , 185 , 186 examination , 184 presentation , 183 , 184
Pediatric contact lens , 60–64 , 66 , 67 aphakia , 69 aphakia treatment , 59 aphakic , 69 binocular vision and stereopsis , 59 cataract surgery , 59 component , 68 consultation
aphakia , 60 corneal health , 60 fi tting process , 60 , 61 IOL formula , 61 parameters , 61 traumatic cataract , 60
cornea without the lens , 68 fi tting process
determination, base curve , 62–63 diameter , 66 , 67 Refraction determination , 63 , 64 , 66
fl uorescein pattern , 68 glasses , 59 GP lens, corneal scar , 70 GP lenses , 68 insertion and removal process , 68 material , 67–68 microbial keratitis , 68 off-eye evaluation of the contact lens , 68 on-eye evaluation of the fi t with white light , 68 power , 68 replacement , 68 selection
GP lens , 62 materials/designs , 61 RGP , 62 Silsoft ® lens , 61
training, caregivers , 68 Pediatric corneal ulcers
amblyopia , 116 and microbial keratitis , 116 anterior stromal infi ltrate , 110 astigmatism , 109
children , 109 HSV epithelial keratitis , 111 HSV immune stromal keratitis , 111 ophthalmic examination , 109 rosacea blepharoconjunctivitis , 111 tree branch injury , 110
Pediatric Eye Disease Investigator Group , 652 Pediatric Eye Disease Investigator Group (PEDIG) , 97 Pediatric glaucoma , 439 , 442 , 454 Pediatric Intensive Care Unit (PICU) , 316 Pediatric masquerade uveitis . See Masquerade syndrome Pediatric ocular trauma
ancillary tests , 169 antibiotic prophylaxis , 170 conjunctival peritomy , 170 materials , 169 medication concentrations , 170 open globe injury , 167 , 168 OTS , 167 , 168 post-operative care , 170 prognostic information , 167 steak knife injury , 170 , 171
Pediatric orbital fl oor fractures clinical synopsis , 677–679 long-term follow up , 676–677 surgical management , 677
Pediatric patients , 8–15 accommodative convergence/accommodation (AC/A) ratio , 20 , 21 amblyogenic condition , 4 double Maddox rod test , 20 examination process , 3 gradient method , 20–21 heterophoria method , 20 motor fusion testing , 18–20 nystagmus , 22–23 nystagmus/strabismus , 4 pediatric eye conditions , 3 Prince Rule , 21 prism neutralization , 18 ptosis , 22 retinoscopy , 22 sensory testing , 18 strabismus , 8–15 strabismus measurement and detection (see Strabismus ) vestibular system , 4 visual acuity , 4–8 visual attention , 4
Pediatric pseudotumor cerebri syndrome (PTCS) , 418–420 CSF opening pressure , 424 diagnosis
fl owchart , 418 , 419 normal brain parenchyma , 418 papilledema , 418 venous imaging , 418
ICP, unclear etiology , 418 primary , 418–421 secondary , 418 , 423 treatment
acetazolamide vs . placebo , 418 lower ICP and weight loss , 419 OCT measurements , 420 patient’s specifi c clinical presentation , 419 side effects , 419
young, prepubertal population , 422 Pediatric refractive surgery , 74–76
case studies , 73 , 74 corneal changes , 76
Index
815
indications , 74 LASIK and PRK procedures , 75 post-operative correction , 77 refractive error, ranges , 75 surgical candidates
amblyopia , 74 craniofacial/musculoskeletal disorders , 75
treatment options anisometropia , 75 hyperopic patients , 76 PIOL , 75 , 76
Periocular infections CBC testing , 668 classifi cation , 668 clinical decision-making process , 668 description , 667 intracranial involvement , 668 masquerade-type conditions , 668 MRSA , 669 oral vs . intravenous antibiotics , 668 orbits imaging , 668 subperiosteal abscess , 669 subperiosteal elevation along lamina papyracea , 670 , 671 subtle post-septal infl ammatory changes without abscess , 672 , 673
Peripapillary staphyloma , 400–402 Perry, J.D. , 561 , 675–679 Persistent fetal vasculature (PFV)
amblyopia therapy , 196 Bergmeister papilla , 192 cataract , 197 clinical genetics , 194 Coats’ disease , 194 coloboma , 192 , 193 corneal opacifi cation , 193 deformations and malformations , 191 diagnosis , 195 embryology , 193–194 etiology , 191 FEVR , 195 heritable systemic diseases , 193 intraocular cautery , 196 intraocular scissors , 196 lensectomy and limbal approach , 196 Mittendorf dot , 192 molecular genetics , 194 Norrie disease , 195 ocular toxocariasis , 195 patients , 191 PHPV , 192 posterior stalks , 193 pupillary membrane , 191 , 192 retinal detachment , 195 retinoblastoma , 194 ROP , 195 surgery , 196 , 197 treatment , 195–196 tripartite classifi cation system , 192
Persistent hyperplastic primary vitreous (PHPV) , 191 , 332 Peters anomaly
beta 1,3-galactosyltransferase-like ( B3GALTL ) , 135 bilateral corneal leukomas , 139 corneal opacifi cation , 136 corneal opacity , 137–138 diagnosis , 136 glaucoma , 136 , 138 heterogeneous chromosomal abnormalities , 135 homeobox genes , 135
Kivlin–Krause syndrome , 135 Krause–Kivlin syndrome , 136 lens vesicle , 135 management , 137 ocular abnormalities , 136 ocular malformations , 135 ophthalmology evaluation fi ndings , 139 penetrating keratoplasty (PK) , 136 Peters plus syndrome , 136 prenatal alcohol exposure , 135 sclerocornea , 136 ultrasound biomicroscopy , 139 , 140
Pfaffenbach, D. , 550 Pfeiffer syndrome , 712 Phakic IOL (PIOL) implantation , 75 Phakomatoses , 359
encephalofacial angiomatosis (Sturge-Weber syndrome) , 372 familial adenomatous polyposis (Gardner Syndrome) , 372 gene, protein and diagnostic criteria , 361–362 genetic and pathophysiologic criteria , 359 NF1 (see Neurofi bromatosis type I (NF1) ) NF2 (see Neurofi bromatosis type 2 (NF2) ) retinal abnormalities , 366 retinal angiomatosis (von Hippel-Lindau) , 366–370 TSC , 370–372
Pharyngoconjunctival fever , 105 PHPV . See Persistent hyperplastic primary vitreous (PHPV) Pichi, F. , 213–217 , 219 , 220 , 251–256 PICU . See Pediatric Intensive Care Unit (PICU) Pierce, J.B. , 313–318 Pigmented ocular fundus lesions (POFLs) , 372–374 PIOL . See Phakic IOL (PIOL) implantation Plaque radiation therapy (Brachytherapy) , 390 , 391 Ple-plakon, P.A. , 109–116 Plexiform neurofi bromas , 360 , 364 Pollard, Z.F. , 552 Polyarteritis nodosa (PAN) , 230 Portable fundus cameras , 263 , 264 , 267 , 268 Posterior segment
abusive head trauma , 309 amphotericin B , 308 anterior segment exam , 310 blunt trauma , 307 chalcosis , 308 cornea and limbus , 307 dense vitreous hemorrhage , 309 diffuse intracerebral hemorrhage , 311 dilated fundus exam , 310 endophthalmitis , 308 fl uorescein angiography , 311 fundus photographs , 310 , 311 intraocular wire , 310 IOFB , 308 laser indirect ophthalmoscopy , 311 metallosis bulbi , 308 monocular blindness , 307 non-accidental trauma , 309 OTS , 307 pediatric ocular trauma score , 307 , 308 penetrating and perforating injuries , 308 premacular hemorrhage , 309 preretinal and nerve fi ber layer hemorrhage , 309 RAPD , 307 retinal heme , 311 seizures , 311 ultrasound biomicroscopy , 309 vitreous cavity , 308
Index
816
Posterior uveitis anterior uveitis , 224 basic laboratory investigation , 224 cataract, glaucoma and band keratopathy , 224 CME and ERM , 224 diagnosis , 224 eye and fundus , 223 IMT , 223 initial evaluation , 224 macular edema/dense vitreous haze , 224 medical management , 223 oral corticosteroids , 223 sarcoidosis/polyarteritis nodosa , 224
Postnatal growth in ROP studies (G-ROP) , 301 Post-traumatic endophthalmitis , 170 PPRPE . See Para-arteriolar retinal pigment epithelium (PPRPE) Prematurity , 46 , 47
myopia retionpathy , 46 , 47
Prendiville, P. , 569 Preseptal cellulitis
eyelid trauma , 667 oral vs . intravenous antibiotics , 668 pediatric population , 667 ( see also Periocular infections )
Presumed ocular histoplasmosis syndrome (POHS) , 244 , 245 Primary congenital glaucoma (PCG) , 443–448
anterior segment , 441 automated visual fi eld testing , 441 axial length , 441 buphthalmos and corneal edema
angle surgery , 445 anterior segment examination , 444 anterior segment photograph , 445 axial length , 444 blepharospasm, epiphora, and photophobia , 445 central corneal thickness , 444 cycloplegic refraction , 445 gonioscopy , 445 goniotomy , 445 management , 445 surgical treatment , 445 Tonopen ® , 444 , 445 trabeculotomy , 445 visual acuity , 445 within normal limits (WNL) , 444
cloudy eyes angle surgery , 443 anterior segment examination , 443 central corneal thickness (CCT) , 443 cup-to-disk (C/D) ratio , 443 cycloplegic retinoscopy , 443 intraocular pressure (IOP) , 443 management plan , 443 metabolic acidosis and tachypnea , 443 myopic refl ex , 443 retinoscopy , 443 visual acuity , 443 wince to light (WTL) , 443
corneal haze anterior segment examination , 443 , 444 axial lengths , 444 C/D ratio , 444 central cornea thickness (CCT) , 444 diagnosis , 444 examination under anesthesia (EUA) , 443 gonioscopy , 444
goniotomy , 444 management , 444 optic nerve examination , 444 primary corneal disease , 444 Tonopen ® , 443 , 444
cycloplegic refraction , 441 diagnosis , 440 dilated fundus examination , 441 genetic basis , 441 , 442 glaucoma
anterior segment examination , 446 , 447 automated visual fi eld (AVF) , 446 band keratopathy and posterior capsular opacifi cation , 446 bleb-related endophthalmitis , 446 B-scan ultrasound image , 447 C/D ratio , 447 central corneal thickness (CCT) , 446 conjunctiva , 446 cycloablation , 447 , 448 cycloplegic retinoscopy , 446 defi nitive plan , 446 diode cyclophotocoagulation , 447 endophthalmitis , 447 goldmann applanation tonometry (GAT) , 446 gonioscopy , 446 inferonasal quadrant , 447 light perception (LP) , 446 macula , 446 management , 446–448 optic nerve examination , 446 optical coherence tomography (OCT) , 446 surgical history , 446 Tonopen ® , 446 trabecular meshwork (TM) , 446 ultrasound , 447 visual acuity , 446 , 447
glaucomas , 440 gonioscopy , 441 intraocular pressure (IOP) , 440 latanoprost and brimonidine
glasses , 445 gonioscopy , 445 management , 445 trabeculectomy , 446 visual acuity , 445
medical treatment , 442 OCT , 441 surgical treatment , 441–442 trabecular meshwork , 441
Primary pediatric optic nerve sheath meningioma (PPONSM) , 689 Prism dioptre (PD) , 492 Pritchard, C. , 3–15 , 17–23 Pritchard, C.H. , 500 PRK , 75 Proptosis, children , 682–699
congenital orbital cystic lesions dermoid cysts , 684 , 685 microphthalmia with cyst , 682–683
diagnostic testing and imaging , 682 differential diagnosis , 682 , 683 hematologic tumors (see Hematologic tumors ) infl ammatory lesions
nonspecifi c , 685–686 ruptured dermoid cyst , 687–688 thyroid eye disease , 686–687
medical history , 681
Index
817
mesenchymal tumors leiomyoma , 698 orbital rhabdomyosarcoma , 695–698
metastatic tumors orbital retinoblastoma , 699 secondary cystic lesions , 699
neural tumors ONG , 688 optic nerve sheath , 689 orbital schwannomas , 689
orbit examination , 681–682 vascular lesions
capillary hemangioma , 689–691 malformations , 691–694
PS . See Pearson syndrome (PS) Pseudo-Brown syndrome , 632 Pseudopapilledema , 402 , 403 Ptosis , 526–528
astigmatic changes , 22 marginal refl ex distances and levator , 22 skeletal and muscular changes , 22
Pushker, N. , 669
Q Qian, Y. , 652
R Radiation therapy
retinoblastoma , 391 Ramaesh, K. , 130 Random dot stereoacuity test , 34 RAPD . See Relative afferent pupillary defect (RAPD) RB1 gene , 380 , 381 , 383 RBCs . See Red blood cells (RBCs) Red blood cells (RBCs) , 452 Red eye fl ow chart , 107 , 108 Red -glass test
diplopia , 31 exotropia , 31
Reem, R.E. , 667–673 , 719 , 720 , 722 Reese, A. , 384 Refractive amblyopia , 52 , 53 , 82 Refractive error , 46 , 52 , 57 , 662
astigmatism guidelines , 52 Marfan syndrome , 57
myopia (see Myopia ) Regular astigmatism
ATR , 53 high WTR , 53 mild degree of oblique , 53 shape, cornea, and lens , 51 subtypes , 51 with the rule (WTR) , 53
Relative afferent pupillary defect (RAPD) , 307 Remote near point of convergence (NPC) , 19 Repka, M.X. , 500 Residual amblyopia , 92 Retcam 3 ® , 264 RetCam ® , 303 Retina , 308 , 310 , 311 Retinal abnormalities
CHRRPE , 366 neuro-ophthalmologic fi ndings , 366 vitreoretinal interface abnormalities , 366 , 367
Retinal and optic nerve head hemangioblastomas , 369–370 Retinal angiomatosis , 366–370 Retinal detachment , 195 , 255 , 256 Retinal dystrophies , 748
achromatopsia , 339–341 algorithm , 337 , 338 ancillary tests , 339 BSS , 342–344 children and infants , 337 cone disorders , 339 inherited conditions , 337 isolated ophthalmic disease , 337 LCA , 345 medical and vision history , 337 , 339 medical/surgical history and ROS , 339
Retinal hemorrhages abusive head trauma , 315 acceleration-deceleration injuries , 314 brain injury , 317 epidural hematoma , 315 hemorrhagic retinopathy , 316 optic nerve injury/retinal detachment , 318 optimal visual function , 317 traumatic brain injury , 314
Retinal imaging, pediatric patients , 262–268 considerations
examination setting , 262 medicolegal risk , 262 patient age , 262 physical or intellectual disability , 262
diagnosis , 261–262 imaging modalities , 263–268
FA , 263–265 FAF , 265 fundus camera , 263 ICGA , 265 infrared imaging , 265 SDOCT , 265–267 ultrasonography , 267–268
monitoring, progression and prognosis , 262 utility , 268–269
Retinal nerve fi ber layer (RNFL) , 273 Retinal toxicity , 321 , 322 Retinal vasculitis , 239 , 240 Retinitis pigmentosa (RP) , 295 Retinoblastoma , 194 , 252 , 253 , 379–385 , 387–391
classifi cation , 384 , 387 clinical features , 381 description , 379 diagnostic imaging , 382–383 , 386 differential diagnosis , 381–382 genetics
bilateral and multifocal tumors , 380 counseling , 380 development , 379 germline mutation , 380 patients diagnosed , 380 pinealoblastoma , 380 RB1 gene , 380 tumor suppressor gene , 379
management chemotherapy , 388–390 cryotherapy , 390 enucleation , 387–388 laser therapy , 390 patient-related factors/physician-related factors , 385 plaque radiation therapy (Brachytherapy) , 390 , 391
Index
818
Retinoblastoma ( cont .) radiation therapy , 391 treatment selection , 385
non-ocular tumors , 383 stepwise evaluation
diffuse infi ltrating type , 381 , 384 endophytic growing beneath , 381 , 383 exophytic growing beneath , 381 , 383 ophthalmic ultrasonography and examination , 381 , 382 ophthalmoscopy , 381 orbital cellulitis , 381 , 385 vitreous seeding , 381
Retinocytoma , 381 Retinoma , 381 Retinopathy of prematurity (ROP) , 195
abnormal proliferative process , 300 BEAT-ROP , 303 ETROP , 303 hypoxia , 300 ICROP , 300 IGF-1 and VEGF , 300 laser photocoagulation , 304 neovascularization , 304 pathogenesis , 300 retinal vessels , 300 right eye , 303 , 304 screening , 301–302 stages , 300 , 301 subgroups , 301 venous dilation and arteriolar tortuosity , 301 zones , 300 , 301
Retinoscopy cycloplegia , 761 examiner positioning and technique , 762 , 763 loose lenses vs . phoropter , 761 nonverbal/preverbal patients , 761 refraction , 761 sleeve position , 761 , 762
Rhabdomyosarcoma CT and MR imaging features , 696 histological types of , 696 orbital , 695–697 pathological features , 696 signs and symptoms , 696 subacute painless proptosis , 681
Richards, B.W. , 506 Rigid gas permeable , 62 Risk models for ROP version 2 (RM-ROP2) , 302 Robitaille, J. , 353–357 Rod cone dystrophy (retinitis pigmentosa) , 283 Rod monochromatism , 339–341 Rosacea keratoconjunctivitis
diagnosis , 115 doxycycline/erythromycin , 116 pathogenesis , 115 risk factors , 115 treatment , 115–116
RP . See Retinitis pigmentosa (RP) Rubella , 244 Rubin, P. , 668 Rungger-Brandle, E. , 105 Rutar, T. , 669
S Saccadic oscillations , 747 , 752 Saethre-Chotzen syndrome , 710 , 711
Sakurai-Lisch nodules , 360 , 363 Sanger sequencing , 336 Sanger, F. , 330 Sarcoidosis , 226–227 Saunders, R.A. , 552 SBS . See Shaken baby syndrome (SBS) Schmitt, M.A. , 337 , 339 , 341 , 342 , 344 , 346 , 349–351 Schwartz, T.L. , 725 , 726 , 731–733 Scleral perforation , 642–643 Scobee, R.G. , 500 Scott, A.B. , 567 Scott, J.A. , 759 SD-OCT . See Spectral domain optical coherence tomography
(SD-OCT) Sears, J.E. , 307–311 Sears, N.C. , 307–311 Sejpal, K. , 165 Şekeroğlu, H.T. , 593–596 , 598–602 Sener, E.C. , 593–596 , 598–602 Sensorial adaptations
binocular vision , 25–27 neurodevelopmental changes , 25 random dot stereoacuity test , 34 stereopsis , 33 strabismus , 28–29 Titmus stereo test , 34
Septo-optic dysplasia , 396 Shaken baby syndrome (SBS) , 309 Sheldon, C.A. , 418–424 Sherrington’s laws , 8–9 Shieh, C. , 155–165 Shields, J.A. , 236 Shorr, N. , 563 Sickle cell disease , 150 , 151 Silicone expanders , 630 Silsoft ® lens , 61 , 62 Simultaneous prism and cover test (SPCT)
esotropia , 10 occluder , 10
Singh, A.D. , 379–391 Single nucleotide polymorphism (SNP) , 336 Sinusitis
orbital cellulitis , 668 preseptal cellulitis , 667
Sisk , R.A. , 261–265 , 268 SITA fast 24-2 protocol , 431 Sixth nerve palsy
amblyopia , 510 amblyopia and suppression , 508 anterior segment ischemia , 509 central nervous system , 506 CN VI abducens nerve , 506 cranial nerve , 506 diplopia , 509 distribution and etiology , 505 esotropia , 506 Hummelsheim procedure , 508 interval history (2 weeks) , 509 , 510 interval history (4 weeks) , 510 interval history (4-8 weeks) , 510 intracranial pathology , 508 intraoperative botulinum injection , 509 Jensen procedure , 508 lumbar puncture , 510 management , 508 , 509 medial rectus recession and lateral rectus resection , 508 motility , 506
Index
819
muscle transposition , 508 neoplasm , 506 neuroimaging , 510 ophthalmoscopy , 506 paralytic strabismus , 505
Skew deviation , 610 Skov, C.M. , 569 Smith, A.E. , 103–107 Smooth pursuit asymmetry , 484 SNP . See Single nucleotide polymorphism (SNP) Spasmus nutans
amblyopia and strabismus , 751 in infants , 751 neuroimaging , 751 nystagmus, head nodding and torticollis , 751 retinal dystrophies , 751 suprasellar tumors , 751
SPCT . See Simultaneous prism and cover test (SPCT) Spectral domain OCT (SD-OCT) , 271 Spectral domain optical coherence tomography (SD-OCT) , 217 , 218 ,
262 , 265–267 , 360 Spierer, O. , 641–646 Sprunger, D.T. , 605 , 606 , 608 , 610 Stahl, E.D. , 73–77 Stair-case approach , 95 Stargardt disease , 277–278
adenosine triphosphate (ATP) , 351 ancillary tests , 350 autofl uorescence (AF) , 350 color fundus photo , 349 FAF , 349 fl uorescein angiography , 349 , 350 fundus autofl uorescence imaging , 349 fundus fl avimaculatus , 350 gene therapy trials , 351 genetic types , 351 multifocal ERG , 351 photoreceptor layer , 350 red blood cell lipids , 351 retinal dystrophy , 349 SD-OCT , 349 , 350 visual prognosis , 351 vitamin A supplementation , 351
Stereo tests , 18 Steroids for Corneal Ulcers Trial (SCUT) , 113 Stickler Syndrome , 47–48 Stilling–Türk–Duane’s syndrome
horizontal gaze palsy and progressive scoliosis , 596 Möbius syndrome , 595 synergistic horizontal divergence , 595–596
Stimulus deprivation amblyopia , 96 Strabismic amblyopia , 82 Strabismic or Combined Strabismic/Refractive Amblyopia , 86 Strabismus , 550 , 660–662
4 Δ base-out prism test , 32 afferent defects , 490–491 afterimage test , 32–33 amblyopia , 28 and amblyopia , 37 , 38 angle kappa , 13–14 ARC , 29 , 30 Bagolini striated lenses , 32 consistent glasses wear , 37 corneal light refl ex assessment , 13 cover testing , 9 development , 39
diplopia , 30–33 DS , 736–737 ductions test , 17 efferent defects , 491 fi xation (left/right eye) , 12 Gaze measurements , 12 haploscopic devices , 14 haploscopic tests , 33 Herring’s and Sherrington’s Laws , 8–9 Hirschberg method , 14 Krimsky method , 14 latent deviations , 10–11 Maddox rod test , 12–13 manifest deviation , 9–10 manifest/latent , 8 ocular rotations , 15–18 partial correction , 38 red glass test , 31 sensory adaptation , 492 suppression , 28–33 version testing , 15 , 17 W4D , 31
Strabismus age-based screening and referral criteria , 84 Strabismus reoperation , 616–619
cyclovertical deviation , 614 ductions and versions , 614 early childhood , 613 extraocular muscles , 613 eye muscle/periocular surgery/trauma , 613 , 614 eye/muscles , 613 fat adherence syndrome , 620 forced duction testing , 614 forced generation testing , 614–616 inferior rectus muscle , 620 medical records , 613 motor function , 614 nerve palsy , 620 ocular surgery , 613 operative fi ndings , 620 preoperative and intraoperative assessment , 621 restrictive or paralytic strabismus , 614 scleral buckle surgery , 620 slipped and lost muscles , 619 surgical approach
adjustable sutures , 618 anterior segment blood supply , 617 anterior/ posterior direction , 618 blebs , 617 conjunctival incision , 617 eye surgery , 617 fornix incision , 617 healing process , 619 limbal conjunctival approach , 617 limbal incision approaches , 617 limbal incisions , 618 optimal immediate postoperative alignment , 619 orbital anatomy and physical principles , 617 orthophoria , 619 physical exam and patient goals , 617 pseudotendon and actual tendon , 618 randomized control trials , 618 scar tissue , 618 scar tissue and Tenon’s capsule , 618 sclera , 618 scleral buckles/glaucoma drainage devices , 618 tendon or pink muscle fi bers , 618
Index
820
Strabismus reoperation ( cont .) Tenon’s capsule , 618 two-plane fornix incision , 618 two-plane incision , 617 Wescott scissors , 618
surgical planning , 620 binocular vision , 616 consecutive exotropia , 617 contralateral muscles , 616 goals and potential adverse outcomes , 616 limbus , 616 limitations , 616 loss of elasticity , 617 medial rectus muscles , 616 muscle placement , 617 patient’s expectations , 616 preoperative evaluation , 616 re-recessions , 617 specifi c professional or leisure activities , 616
visual acuity , 613 Strabismus surgery
anesthesia and surgical techniques , 641 anterior segment ischemia , 645–646 bradycardia , 642 exposed sutures , 646 eyelid position changes , 646 infection , 644 infl ammation , 644–645 intraoperative complications , 642–643 lost muscle , 643 malignant hyperthermia , 642 oculocardiac refl ex , 642 preoperative planning , 641–642 refractive changes , 646 sarcoplasmic reticulum membrane , 642 scleral perforation , 642–643 slipped muscle and stretched scar , 643–644 slipped muscle/orbital cellulitis , 641
Straight, S.M. , 583 , 584 , 586 , 588 , 589 , 591 Straka, D. , 705–708 , 710 , 712–716 Stromal keratitis , 122–124 Sturge–Weber Syndrome , 372 Subperiosteal abscess , 668–670 Sultan, G. , 203 Suprasellar tumors , 751 Swept-source OCT (SS-OCT) , 271 Sympathetic ophthalmia (SO) , 227–228 Synkinetic syndromes , 661 Syphilis
acquired ocular syphilis , 238 congenital , 238 , 239 diagnosis , 238 ocular , 239
Szperka, C. , 418–424
T Taich, A. , 759 Telemedicine Approaches to Evaluating Acute Phase ROP study
(e-ROP) , 302 Tendency Oriented Perimetry (TOP) protocol , 431 Teratomas , 684 , 685 The Intergroup Rhabdomyosarcoma Study (IRSG) , 695 Thiagalingam, S. , 412 Third nerve palsy , 525 Thomas, S.M. , 570
Thompson, H.S. , 759 Thyroid eye disease (TED) , 564 , 566 , 686–687
active and infl ammatory phase , 560 adjustable suture technique , 569 anesthesia , 568 bilateral inferior rectus surgery , 571–573 botulinum toxin , 567 classifi cation , 563 contralateral surgery , 571 corticosteroids and immunosuppressants , 560 CT , 564 duction-based surgery , 569–570 EOM fi brosis and optic neuropathy , 560 etiology, thyroid orbitopathy , 560 eye muscle surgery , 571 four-muscle surgery , 573 goals , 560 grading , 562 Graves’ disease , 559 , 564 hyperthyroidism , 559 imaging , 563 IRMT , 570–571 left hypotropia , 578 lubricants , 560 management , 568 oblique muscle surgery , 573 occlusion , 567 ophthalmic examination , 561–562 ophthalmic signs and symptoms , 561 orbital decompression , 560 , 563–564 pitfalls and complications , 575–577 planning strabismus surgery , 568 prisms , 567 QOL , 577 quantitating ductions , 562 radiation therapy , 560–561 reoperations , 573–575 resection , 575 right hypotropia , 565 stability , 575 and strabismus
cardinal gazes , 566 double Maddox rod testing , 566 ductions and versions , 564 exotropia , 566 Goldmann perimeter, binocular vision , 566 intraocular pressure measurements , 566 photographs , 566 prism and cover testing , 566
surgery , 568–569 surgical indications , 568 testing , 562–563 upgaze , 566 , 568
Thyroid orbitopathy , 560 , 561 Thyroid-stimulating hormone receptor (TSH-R) , 560 Thyroid-stimulating immunoglobulin (TSI) , 562 Tilted disc syndrome , 401–402 Time domain-OCT (TD-OCT) , 271 Titmus stereo test , 34 , 759 Todman, M.S. , 669 Toldo, I. , 759 TOP . See Tendency Oriented Perimetry (TOP) protocol Topical steroids , 216 Torticollis , 739 Toxocariasis
defi nition , 236
Index
821
ocular , 236 , 237 Toxoplasmosis
acquired , 235 congenital , 234 ocular , 234
Trabeculectomy , 470 Trabeculotomy , 441 , 445 , 454 Traboulsi syndrome , 205 Traboulsi, E.I. , 191 , 193–197 , 199 , 201–207 , 329–337 , 339 , 341 , 342 ,
344 , 346 , 349–351 , 359–374 , 395–405 , 547 , 548 , 550–554 , 559–564 , 566–571 , 573 , 575 , 577 , 652 , 757–760
Trapdoor fractures ischemia, extraocular muscle , 676 pediatric population , 676
Treacher-Collins syndrome , 712 Trisomy 21 , 736 Trivedi, R.H. , 61 , 183–189 Trochlear nerve palsy , 513 Tsang, S.H. , 291 , 293 , 295 Tuberculosis (TB)
intraocular , 240 ocular , 240 ocular involvement , 240 tuberculous choroidal granulomas , 240 tuberculous uveitis , 240
Tuberous sclerosis complex (TSC) adenoma sebaceum , 370 autosomal dominant multi-systemic disorder , 370 central nervous system , 370 diagnostic criteria , 370 hamartomas , 371 neuroimaging , 370 prevalence ranges , 370 retinal and optic nerve head astrocytic hamartomas , 370 visceral manifestations , 370
Tubulointerstitial nephritis and uveitis syndrome (TINU) , 228 Tychsen, L. , 480
U Ultrasonography , 267 Ultrasound biomicroscopy (UBM) , 253 Unilateral congenital cataract, left eye
aphakic glaucoma , 464 glaucoma , 461 history , 460 , 464 interval history (1 month) , 461 interval history (1 week) , 461 interval history (3 months) , 464 interval history (5 months) , 461 management , 460 , 464
Utz, V.M. , 81–97 , 175–181 , 359–374 , 535–537 , 539–543 Uveitis , 216 , 251 . See also Infectious uveitis
V Vajpayee, R. , 158 Van Mierlo, C. , 411 Varicella zoster virus (VZV) , 119 , 125–126 , 241 Vascular disorder
avascular retina , 354 bilateral congenital retinal , 356 bilateral vitreous bands , 356 diagnosis , 354–355 eye disease/blindness , 353
Genetic testing , 354 hemorrhages , 356 KIF11-related disease , 356 management approach , 356 ophthalmoscopy , 353 unilateral avascular retina , 354
Vascular endothelial growth factor (VEGF) , 300 Vascular lesions
capillary hemangioma , 689–691 malformations , 691–694
Velez, F.G. , 552 Venipuncture , 264 VEP . See Visual evoked potential (VEP) signal Vernal keratoconjunctivitis (VKC)
calcineurin inhibitors , 106 corneal ulcers , 106 Horner-Trantas dots , 106 neovascularization and scarring , 106 ocular surface allergy , 106 olopatadine , 106 papilla , 106 steroids , 106 symptoms , 106 tacrolimus (Protopic ® ) and cyclosporine (Restasis) , 106
Vertical nystagmus in infancy Arnold–Chiari malformations , 752 congenital downbeating nystagmus , 751 eye positions , 751 , 752 ophthalmologic examination , 751
Vicente, G.V. , 761–763 , 765 , 766 Vigabatrin (Sabril®)
age-based vigabatrin retinal toxicity monitoring guidelines , 322
benefi ts of screening , 323 drug , 321 electrophysiological testing , 322 γ-aminobutyric acid transaminase (GABA-T) , 321 Goldmann visual fi elds , 323 internal limiting membrane (ILM) and atrophy , 322 irreversible visual fi eld constriction , 321 ophthalmologic assessment , 322 peripheral retinal function , 321 photopic 30-Hz fl icker amplitudes , 323 photopic ERG 30-Hz fl icker response and Goldmann visual fi eld ,
324 , 325 retinal nerve fi ber layer , 321 , 322 standard of care , 322 visual dysfunction and dose , 321 visual fi eld constriction , 321 visual fi eld defects , 321 visual fi eld testing , 322
Viral conjunctivitis EKC , 105 pharyngoconjunctival fever , 105 prodrome , 104 red burning right eye , 104 serotypes , 104 visual acuity , 104
Viral keratitis corneal scaring , 115 diagnosis , 114 pathogenesis , 114 risk factors , 114 treatment , 115
VISA infl ammatory score , 562
Index
822
Vision impairment , 731–733 albinism and optic nerve atrophy , 726 binocular , 731 clinical low vision evaluations , 725 contrast sensitivity function , 731 craniopharyngioma , 728 devices and magnifi cation , 731 education services
assistive technology , 732 braille , 732 children and adolescents , 732–733 classroom setting , 732 learning media assessment , 732 medical and educational eligibility , 731 orientation and mobility (O&M) , 732 print, braille/dual media , 732
electronic and computer magnifi cation systems , 725–726 electronic magnifi cation , 728 learning , 725 literacy , 726 nystagmus and esotropia , 728 oculocutaneous albinism , 728 optical devices , 725 visual function assessment tools , 725 , 726
Vision loss clinical eye examination , 419 optic nerve compression , 421 treatment, PTCS , 419
Vision rehabilitation , 732 Visual acuity , 5–8 , 86 , 87
qualitative methods amblyopia , 6 base-down prism , 6 , 7 binocular conditions , 5 fi xation preference , 6 monocular testing , 5 nystagmus , 8 optotype monocular , 8 poor vision/visual attention , 7 preliterate vision , 7
quantitative methods logMAR , 5 Teller acuity card , 5
Visual evoked potential (VEP) signal , 431 Visual evoked potentials (VEPs) , 360 , 411 Visual rehabilitation , 187 Vitrectomy , 309 , 310 Vitreoretinal interface abnormalities , 366 , 367 Vogt , 229 Vogt–Koyanagi–Harada syndrome (VKH) , 229 Voluntary nystagmus , 753
Von Hippel-Lindau (VHL) 3p25-26 , 366 case study , 368 clinical manifestations , 366 retinal and optic nerve head hemangioblastomas , 369–370 surveillance guidelines , 368
VZV . See Varicella zoster virus (VZV)
W Waldman, A.T. , 433 Wall, P.B. , 395–405 Wei, L.A. , 676 Weight, Insulin-like growth factor I, Neonatal ROP algorithm
(WINROP ® ) , 301 Weill-Marchesani syndrome , 204 , 205 Weill-Marchesani syndrome (WMS) , 199 Weiss, A.H. , 412 WES . See Whole-exome sequencing (WES) West, C.E. , 500 WGA . See World Glaucoma Association (WGA) Whitaker, L. , 720 Whole-exome sequencing (WES) , 330 , 336 Wierda, S.B. , 150–152 Wiesel, T.N. , 82 Williams, W.T. , 104 Wilson, M.E. , 61 , 183–189 Winkler, K.P. , 525–527 , 531 World Glaucoma Association (WGA) , 439 , 457 World Health Organization (WHO) , 216 Worth 4- dot test
monofi xation syndrome , 31 Worth 4-dot test , 18 , 480 Wright, K.W. , 500 Wyburn-Mason syndrome , 692
X Xanthogranuloma , 695
Y Yang, M.B. , 300–304 Yousuf, S.J. , 507 Y-pattern exotropia , 624 , 626 , 627
Z Zamora, B.G. , 261–265 , 268 Zee, D.S. , 752 Zhang-Nunes, S. , 705–708 , 710 , 712–716
Index



























