Embed Size (px)
Citation preview

APPROACH TO THE MEDICAL CARDIOGENIC
SHOCK PATIENT
CASE STUDIES
Amynah Welji, PA-C

Cardiogenic Shock spectrum
THE ISCHEMIC PATIENT THE VHD PATIENT WITH
POOR FORWARD FLOW
THE MECHANICAL PUMP
FAILURE

Cardiogenic Decompensation Spectrum…Shock
• Does the pt describe any Low Cardiac Output symptoms?
• Do they c/o CP/pressure, dyspnea, decreased tolerance, fatigue N/V, loss of appetite, increased abdominal girth, LE edema and/or FTT
History
• Is the patient cold, clammy, gray or cyanotic, lethargic, A&O, profoundly tachycardic or bradycardic?
• How’s their breathing? Are they dry or wet, cold or warm?
• Are they making urine?
Physical Exam
• What are the filling pressures or response to straight leg raise?
• What are the Hemodynamics if SGC present: CVP, PAP, PAOP, CO/CI. If LHC available: what is RV pressure, LVEDP, AV or MV gradient, Ao pressure
Central Pressure Monitoring
• Echo: What’s the LVEF? Which structural & functional abnormalities exist? Is there an pericardial effusion?
• EKG / LHC: Is there ischemic disease?
Cardiac Imaging
• Labs: evaluate for End-organ function and oxygen consumption / delivery: CMP, LA, SvO2/ScVO2, CBC, Mag, iCa, TSH, BNP, Trop and ABG
Others Diagnostics

Frank Starling Curve
◦ Describes relationship between preload
and cardiac function. Principles include:
◦ As preload increases, SV also increases
◦ As cardiac muscle fibers become
maximally stretched, the proportional
increase in SV decreases and curve
flattens
◦ Preload + Contractility of the cardiac
muscles + afterload influence the
shape of the curve

How bad is it?
DRY WET
WARM Compensated
Tx: Continue GDMT
Decompensated / Volume overloaded
Tx: Diurese & resume GDMT as tolerated.
Return to Frank-Starling curve hemodynamics
COLD Low Output
Tx: Support Frank-Starling curve
hemodynamics
• May not tolerate GDMT or need
more afterload reduction
• Consider inotropic support based
on severity / clinical symptoms.
• Refer for Advance HF therapies)
Cardiogenic shock
Tx: Resuscitate & Recover first
• Inotropes
• Vasopressors
• MCS
• anti-arrhythmics
• End-organ support

Shock ManifestationsCardiogenic (CO = HR x SV) Distributive Hypovolemic
Primary
Abnormality
Low HR Low SV Low SVR Low PCWP & CVP
Other
Abnormalities
High-normal SV
High PCWP
High PCWP High CO
Normal SV
Normal PCWP
Low CO
Low SV
Compensatory
Changes
High SVR High SVR
High HR
High HR High SVR
High HR
Treatment
Inotropes: Milrinone > Dobutamine or Epinephrine
Vasopressors: Norepinephrine > Vasopressin +/- Epinephrine
Diureses
Beta-agonists / Pacing (low HR)
MCS: IABP, Impella, ECMO
ASO: OHT vs LVAD
Usually sepsis: Volume resuscitation + vasopresors
Vasopressors
Steroids for refractory cases
Volume resuscitation with Crystalloids > colloids
Correct anemia if present

Other Cardiac Shock Manifestations
Condition Clinical Manifestation
Acute Chord Tendinae
Rupture
Low CO
Low BP
Massive Pulmonary
Embolus
Low CO
Low LV preload → Low BP
Pericardial Tamponade Low RV preload → Low BP
Tension Pneumothorax Low RV preload → Low BP
Speed of resuscitation is crucial as prolonged hypoperfusion from any cause →
increased inflammation and ultimately distributive shock

Normal Hemodynamic Values

Hemodynamic Calculations
CALCULATION
Systemic Vascular
Resistance
SVR = 80 x [mean artery pressure – CVP]/CO
Pulmonary Vascular
Resistance
PVR = 80 x [mean PAp – PAOP]/CO
Cardiac Index (CI) CI = CO/body surface area
Stroke Volume Index SVI = CI/heart rate
Left Ventricular Stroke
Work Index
LVSWI = [mean systemic artery pressure – PAOP] x SVI x 0.136)
Right Ventricular Stroke
Work Index
RVSWI = [mean PAp – CVP] x SVI x 0.136
Oxygen Delivery DO2 = CI x 13.4 x hemoglobin concentration x arterial oxygen
saturation
Oxygen Uptake VO2 = CI x 13.4 x hemoglobin concentration x [arterial oxygen
saturation – venous oxygen saturation

Conditions with elevated RA (CVP)
◦ Elevated RA pressures can be seen in a number of conditions including
the following: ▪ Diseases of the right ventricle (eg, right ventricular infarction or cardiomyopathy)
▪ Pulmonary hypertension
▪ Pulmonic stenosis
▪ Left-to-right shunts
▪ Tricuspid valvular disease
▪ Cardiac tamponade
▪ Constrictive pericardial disease
▪ Restrictive cardiomyopathies
▪ Left ventricle systolic heart failure
▪ Hypervolemia

Conditions with elevated PAP
❑The mean PA pressure can be elevated (eg, mPAp, >22 mmHg) by diverse conditions
❑Etiologies associated with PH will also result in mild elevations of the PAP’s. Causes of PH include:
❑Pulmonary arterial hypertension (eg, idiopathic, connective tissue disease, congenital heart disease; Group 1)
❑PH due to left heart disease (eg, left heart failure, mitral valvular disease; Group 2)
❑PH due to chronic lung disease and/or hypoxemia (eg, emphysema, interstitial lung disease; Group 3)
❑PH due to chronic pulmonary thromboembolism (Group 4)
❑PH due to multifactorial mechanisms (eg, sickle cell disease; Group 5
Acute Acute on Chronic Chronic
Venous Thromboembolism Hypoxemic-induced
vasoconstriction in a
patient with underlying
cardiopulmonary disease
Pulmonary
Hypertension (mPAP >
25mmHg).Hypoxemic-induced
pulmonary vasoconstriction

Conditions with Abnormal PCWP (PAOP)
◦ Abnormally HIGH PAOP — Any condition
that raises left ventricular end diastolic
pressure results in an elevated occlusion
pressure including the following:
❑Left ventricular systolic heart failure
❑Left ventricular diastolic heart failure
❑Mitral and aortic valve disease
❑Hypertrophic cardiomyopathy
❑Hypervolemia
❑Large right-to-left shunts
❑Cardiac tamponade, constrictive and
restrictive cardiomyopathies
Abnormally LOW PAOP – Any condition that cause a low wedge pressure includes the following:
❑ Hypovolemia (eg, hemorrhagic shock, severe intravascular volume depletion)
❑ Pulmonary venoocclusive disease (variably normal or low)
❑ Obstructive shock due to large pulmonary embolism

Interpreting Mixed Venous

MECHANICAL CARDIAC SUPPORT IN
THE CARDIAC ICU

NTERMACS profile descriptions.61
Abbreviations: INTERMACS, Interagency Registry for Mechanically Assisted Circulatory Support;
NYHA, New York Heart Association.
INTERMACS
PROFILE
CRITERIA
I Critical Cardiogenic Shock (“Crash & Burn”)
2 Progressive decline (“Sliding on Inotropes”)
3 Stable but inotrope dependent (“Dependent stability”)
4 Resting symptoms
5 Exertion intolerant
6 Exertion limited
7 Advanced NYHA III

Goals of MCS
Types of support
❑LV Support
❑RV Support
❑Biventricular Support Organ
Perfusion & Oxygen Delivery
Decrease preload
Decrease Afterload
Bridge to more
durable device
Support through high-risk
procedure
Increase Cardiac Output

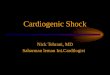
Mechanical Cardiac Support Devices
◦ Intraaortic Balloon Pump (IABP): Diastolic augmentation &
counterpulsation
◦ Extracorporeal Membrane Oxygenation (ECMO) & its
multiple configurations: Ability to oxygenate in hypoxemic states and
unload RV & LV simultaneously
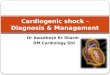
◦ Percutaneous LVAD’s:
◦ Impella: impeller-driven, axial-flow pump placed via a pigtail catheter with inlet that sits in LV and pumps blood out in the ascending aorta. Can provide from 2.5 –5.0L/min of CO per catheter selection
◦ TandemHeart: LA to FA bypass system that can deliver up to 4L/min CO
◦ CentriMag blood pump
◦ Extracorporeal surgically implanted centrifugal pump that can provide up to 10L/min of CO. NOTE: pump can be placed centrally or peripherally in the ECMO circuit
◦ FDA Approved for up to 6hrs or for acute RV support up to 30days
A: IABP B: Impella C: TandemHeart

slide 18
Impella

Mechanical Cardiac Support Devices
IABP ECMO TANDEM-HEART IMPELLA
Afterload Reduced Increased Increased Neutral
LV stroke volume Slight increase Reduced Reduced Reduced
Coronary
perfusion
Slight increase Unknown Unknown Unknown
LV preload Slightly reduced Reduced Reduced Slightly reduced
PCWP Slightly reduced Reduced Reduced Slightly reduced
Peripheral tissue
perfusion
No significant
increase
Improved Improved Improved
Table 2
Hemodynamic effects of mechanical circulatory support devices.
Note: Adapted from Werdan K, Gielen S, Ebelt H and Hochman JS, “Mechanical circulatory support in cardiogenic shock,”
European Heart Journal (2014) 35, 156–67, by permission from Oxford University Press and European Society of Cardiology.

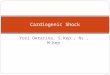
IABP : Impella Comparison
PROS
o Least resource intensive MCS to place quickly
o Smallest catheter size compared to other (Impella and ECMO @ PAH)
o Can be used for prolonged duration
o Thought to indirectly improve RV support due to increased coronary perfusion
o Offers LV relaxation and unloading
CONS:
o Offers the least amount of IABP CO support
o May not be sufficient cardiac support
PROS
o Offers better LV relaxation & unloading compared to IABP & ECMO
o Impella RP can directly support the failing RV
o Different catheters for differing LV support need: 2.5L/min (Impella 2.5) vs 3.5L/min (Impella CP) or 5L/min (Impella 5.0 surgically placed)
CONS:
o Cannot be used with mural thrombus
o Anecdotally, have seen increased bleeding complications
o Decreased duration of use per manufacturer recommendation
IABP Impella

Cardiogenic Shock – Case Studies
THE ISCHEMIC PATIENT THE VHD PATIENT WITH
POOR FORWARD FLOW
THE MECHANICAL PUMP
FAILURE

Case Scenario 1 – CGS-VHD
◦ 67yo WM w/ a PMH of AS s/p bioprosthetic AVR, OSA, HLD, prostate CA s/p prostatectomy,
bladder surgery, obesity, and DM presented for elective R/LHC for TAVR eval. Procedure aborted
d/t pulmonary edema & admitted to CCU on NRB for optimization. Pt recently admitted for ADHF
@ OSH. Overnight, developed increase FiO2 requirements with ^^BP, requiring Cardene.
◦ Recent Echo: EF 55-60%, moderate LVH, severe bioprosthetic AS with mild MR/TR. Mildly dilated
Ao root & asc Ao, mild PHTN
◦ New Echo: Severe AS, MG 100mmHg
◦ What are your next steps:
◦ Diuresis with guided hemodynamic monitoring?
◦ IABP?
◦ BAV?
◦ Pharmacological: Cardene / NTG for BP mgt

Case Scenario 1 – CGS-VHD
◦ Next steps:
◦ Diureses with guided hemodynamic monitoring: failed tx overnight with clinical decompensation
◦ IABP: unable to lay flat, would need to intubate, which may in itself be deleterious
◦ BAV: Not a candidate due to bioprosthetic AV
◦ Veno-V asodilators: will not fully address MG of 100mmHg
◦ PLAN → emergent TAVR
◦ Discussion:
◦ Given underlying LVH and likely poor LV compliance, despite normal LVEF, a hypertensive response further worsened LVEDP and LVEDV → LV overload → LA overload → pulmonary edema → worsening respiratory failure on 15L Salter by first night
◦ ADHF in setting of severe AS → CGS with limited forward flow → unresponsive to diuretics d/t renal hypoperfusion
◦ In order to safely place SGC or MCS, would need to intubate pt, which could have resulted in cardiac arrest given MG 100mmHg.
◦ Mechanical problem = mechanical fix → GOAL: restore forward flow
◦ Hence, emergent TAVR was the only option to restore flow

Case Scenario 2 (same patient)Patient received post TAVR in CCU: hypotensive with new LBBB and CP → symptomatic CHB. SGC with chandler probe placed. Patient noted to be in CGS requiring high dose Epi 0.15mcg/kg/min, Norepi, Milrinone with MSOF, requiring CRRT initiation. He had received Lopressor 100mg (home dose) post TAVR.
◦ HD’s: CI 1.57, CVP 20’s on moderate doses of Epi / Norepi / Vasopressin
◦ STAT Echo: LVEF 25-30% with anterior wall & anterior septum are akinetic, RV mild to moderately dilated with RVSF moderately to severely reduced, severe BAE, Valve-in-valve well seated w/o PVL and normal gradient. NO pericardial effusion noted
◦ Labs: Trop 23, LA 11
Pt noted to have refractory CGS despite above measures, requiring multiple amps of bicarb. He was cannulated for VA ECMO / intubated by anesthesia.
Why refractory Shock in patient with prior normal LVEF and no evidence of RV failure who now has LV & RV dysfunction? What changed?
◦ Symptomatic CHB / asynchronous pacing?
◦ Ischemia?
◦ TAVR related?

Case Scenario 2:CGS-VHD → CGS-acute ischemia
Why refractory Shock in patient with prior normal LVEF?
◦ Symptomatic CHB / asynchronous pacing: may have led to RV dysfunction but shouldn’t have caused
moderate to severe RV failure.
◦ Ischemia: trop up to 23, STAT echo reveals new WMA post TAVR raises concern for compromised coronary flow.
◦ Initial EKG with baseline artifact but wide QRS & LBBB.
◦ Post-ECMO EKG: anterior Q-waves with raised ST segments and lateral ischemic changes
◦ TAVR related: compromised coronary flow from TAVR placement → thrombus formation → infarct with acute
decompensation

Case Scenario 2:CGS-VHD → CGS-acute ischemia
Discussion:
Patient was infarcted post TAVR (trop peaked > 83). Taken back to CCL revealing thrombus at LM/LAD with TIMI 2 flow; started on Aggrastat.
Anterior ischemia → refractory CGS affecting MSOF and required quickly escalating therapies.
Previously low forward flow shock from CHRONIC severe AS was decompensating but patient had a higher threshold for decompensation
ACUTE ischemia accelerated the process and need for higher level MCS.
In this patient with active thrombus worsening ischemia, vasopressors / inotropes would increase cardiac demand → further worsening shock.

Case Scenarior 3: CGS – Pump Failure
◦ 41 y.o. Filipino male with NICM, EF 25% on home Milrinone @ 0.325mcg/kg/min is admitted with WCT and ADHF. He does
not have ICD and has been non-compliant with LifeVest in past. His PICC line has fallen out. He’s intubated/sedated for
DCCV in the ED w/o response. Treated with Amio boluses x 2 with conversion to SR. Started on Amio gtt.
◦ PE: Appears wet & warm, few basilar crackles. Normotensive
◦ Initial labs reveal fairly normal chemistries / CBC except LA 8
◦ SGC placed: HD profile includes – HR 110’s, CI 1.6L/min/M2, CVP 12, PAP 40/20’s, WP 22, SVR 1900 on Milrinone 0.375mcg
◦ Repeat Echo: EF down to 10%, severe TR, moderate MR. RV preserved size/function
What next steps are appropriate:
◦ Increase Milrinone?
◦ Add 2nd inotrope
◦ MCS?
◦ Diurese

Case Scenario 3: CGS – Pump Failure
Next Steps Taken:
◦ IABP placed:
◦ Adding Epinephrine could have worsened afterload
◦ Increasing Milrinone could’ve promoted WCT recurrence
◦ Repeat HD’s: similar to prior, now with hypotension due to increased sedation requirement → Epi added
with subsequent correction of CI and improvement in diureses.
◦ He failed multiple Epi and IABP weans due to drop in CI, tachycardia, tachypnea, but surprisingly
maintained normal end-organ function
◦ He self-extubated while on a SBT and suffered by severe agitation / delirium, later found to be from
alcohol withdrawal and now cerebral hypoperfusion

Case Scenario 3: CGS – Pump Failure
Discussion
He didn’t clinically appear to be in CGS on arrival, despite VT but LA high & SGC findings confirmed CGS. He was found to have urosepsis but no bacteremia. He required prolonged cardiac support with dual inotropes and MCS to allow him to recover from septic shock as well as severe alcohol withdrawal.
Note: without a SGC, he may have been treated as a septic shock patient with volume resuscitation instead.
Would an Impella or ECMO have offered better HD support than IABP and prevented 2nd inotrope / vasopressor, which ended up increasing further afterload once he was extubated?
Hospital course prolonged by significant fevers, ~105 degrees
Concern for worsening LV function and presenting VT can be related alcohol +/- lack of inotropic support. He was eventually weaned off Epi and then IABP with increased Milrinone dose as his new dose and will be worked up for advanced surgical options as OP. We tolerated lower SvO2 / Fick CI given no end-organ dysfunction noted on chem panel once his withdrawal improved.
He will need ICD protection vs better compliance with LifeVest if LVAD planned in < 3months