Embed Size (px)
Citation preview
THE MANY USES OF STEROIDS:
FROM BODYBUILDERS
TO CRITICAL ILLNESS
April Merrill, MS, APRN, CCNS
OBJECTIVES Identify the different categories of
steroid medications
Identify the uses for steroid medications
Identify side-effects and precautions for steroid medications
WHAT ARE HORMONES? Hormones- secreted by cells to regulate the
activity of other cells. Growth Development Behavior Reproduction
Coordinates the production, use and storage of energy.
Homeostasis Nutrition Metabolism Excretion Water and salt balance
WHAT ARE STEROIDS? The term steroid refers to any synthetic
(man made) or naturally occurring fat (lipid) soluble compound that has a physiological response.
Steroids are hormones derived from cholesterol and differ only in the ring structure and side chains attached to it.
STEROID HORMONES Adrenalcortical steroids Progesterone & related steroids Androgens Estrogens Bile acids & bile salts Cholesterol
PROGESTERONE & RELATED STEROIDS Progestogens (also known a progestins) such
as progesterone Produced from the corpus luteum in normal
menstrual cycle Estrogens, including estradiol and estrone
produced primarily by developing follicles in the ovaries, the corpus luteum, and the placenta
promote the development of female secondary sexual characteristics, such as breasts
involved in the thickening of the endometrium and other aspects of regulating the menstrual cycle.
ANDROGENS Testosterone
primarily secreted in the testes of males and the ovaries of females
plays a key role in the development of male reproductive tissues such as the testis and prostate
promotes secondary sexual characteristics such as increased muscle, bone mass and the growth of body
Prevents osteoporosis
ANABOLIC STEROIDS
Roids
Juice
Sauce
Sloop
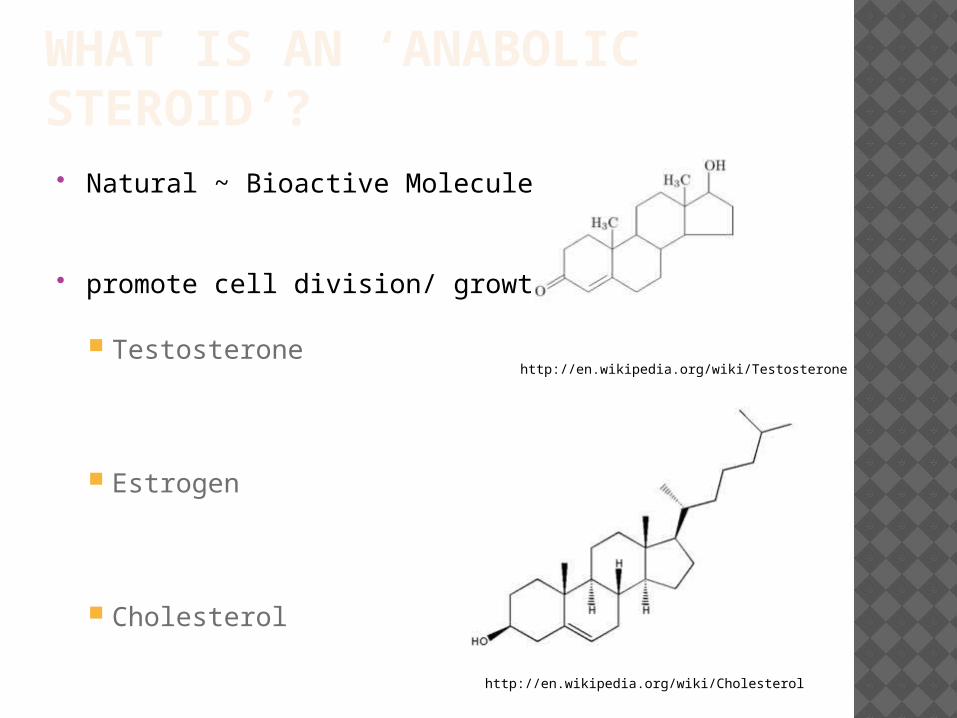
WHAT IS AN ‘ANABOLIC STEROID’? Natural ~ Bioactive Molecules
promote cell division/ growth
Testosterone
Estrogen
Cholesterol
http://en.wikipedia.org/wiki/Testosterone
http://en.wikipedia.org/wiki/Cholesterol
WHAT IS A ‘SYNTHETIC’ ANABOLIC? Structural Definition
Not found in nature. How they are prepared.
Semi-syntheticNatural Source MaterialsSynthetic Chemistry Derivation
AdvantagesCostHighly variable structure
USES Anabolic steroids are synthetic versions of
testosterone, the body’s natural sex hormone. They assist athletes by facilitating efforts to gain strength and muscle mass for increased muscular endurance, power and speed.
Stimulation of: Sexual development Growth Puberty Bone marrow Appetite Muscle Mass Stamina
http://www.steroidabuse.com/how-anabolic-steroids-work.html
SIDE EFFECTS Hormonal System
Men
Infertility
Breast development
Shrinking of the testicles
Women
Enlargement of the clitoris
Excessive growth of body hair
Both Sexes
Male-pattern baldness
Muscoloskeletal System
Short stature
Tendon rupture
Cardiovascular System
Heart attacks
Enlargement of the left ventricle
Liver
Cancer
Peliosis hepatis
Skin
Acne and cysts
Oily scalp
ROID RAGE Altered hormone levels
Inability to control behavior
Severe mood swings
Irritability
Violent aggression
Depression
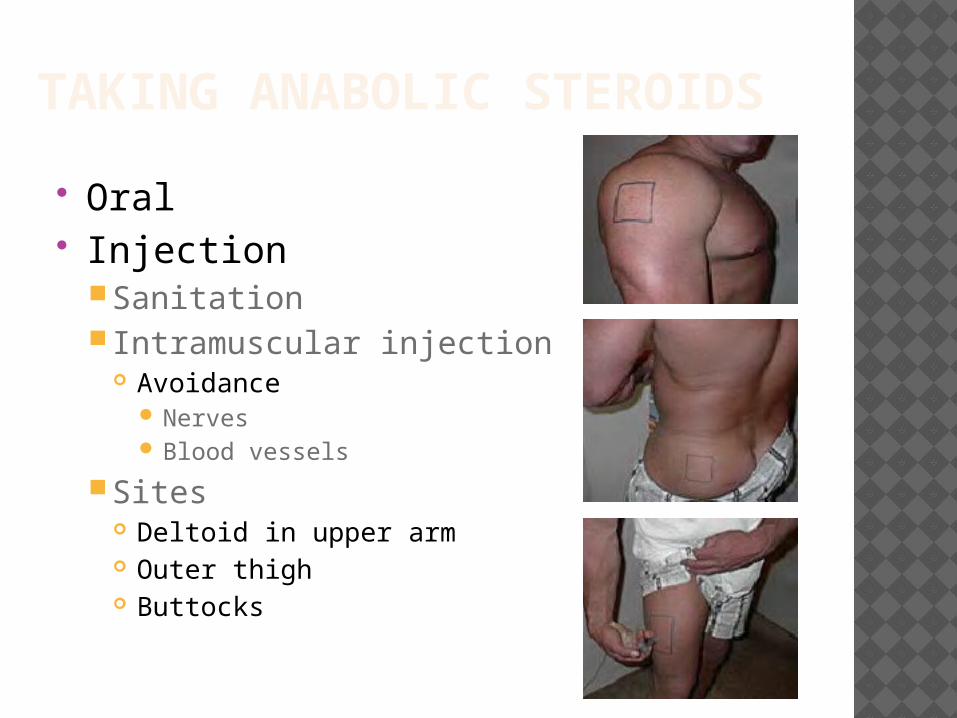
TAKING ANABOLIC STEROIDS
Oral Injection
Sanitation Intramuscular injection
Avoidance Nerves Blood vessels
Sites Deltoid in upper arm Outer thigh Buttocks
LEGAL AND MORAL ISSUES
Is it cheating?
Is it legal?
Is it worth it?
DETECTION TIMES Nandrolone decanoate- 18 mos.
Depo-testosterone- 3 mos.
Parabolan- 5 weeks
Andriol- 1 week
Clenbuterol- 4 days
SCIENTIFIC NAMES
Oral
Oxymetholone
Oxandrolone
Methandrostenolone
Stanozolol
Injectable
Nandrolone decanoate
Nandrolone phenpropionateTestosterone cypionate
Boldenone undecyclenate

ANDRIOL
Dosage- 8-16 40 mg caps daily
Street price- $1 for 40 mg
Half-life: 3-5 hrs
DANATROL
Dose- 200-400 mg daily
$2-3 per 200 mg cap
Lack of popularity Slightly androgenic Expensive
METHYLTESTOSTERONE Dosage: 25-50 mg/ day Price: 2 50 mg tablets for $1 First oral steroid Works well; bad side effects and high
cost Potent androgen
Prone to ‘roid rage’
SUSTANON 250
Dosage: 250-1000 mg/ week Price: $10-30/ ml Stacks well with any compound Extreme anabolic tendencies
Good and bad Injectables

ANABOLIC REFERENCES www.steroid.com www.bodybuilding.com www.steroidworld.com www.wikipedia.com www.wrestlingusa.com www.anabolicsmall.com www.steroids.com www.pharmaeurope.com
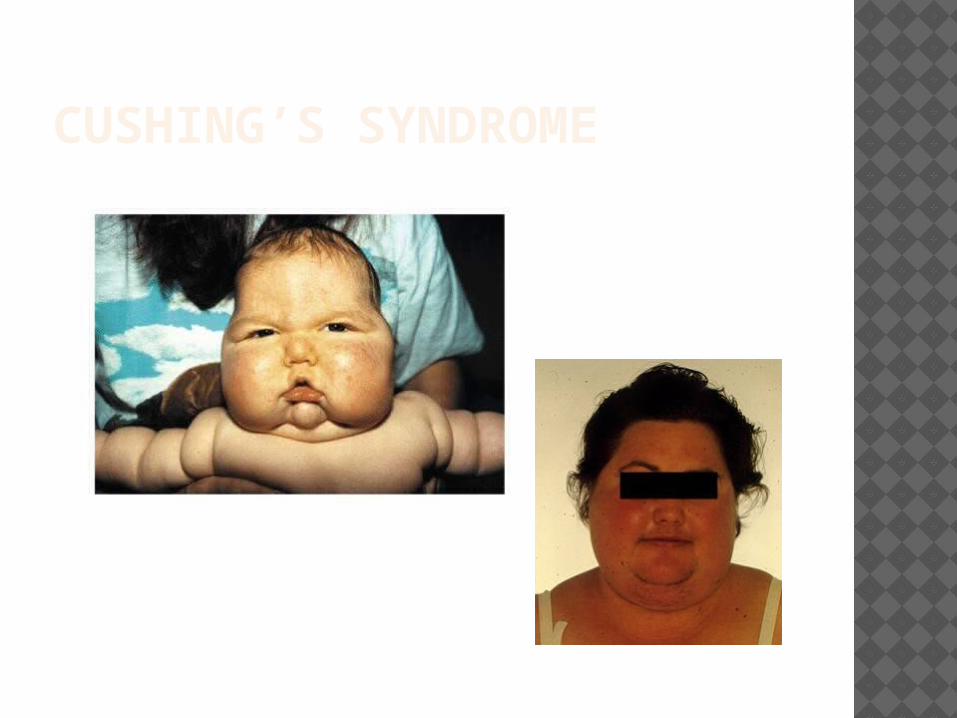
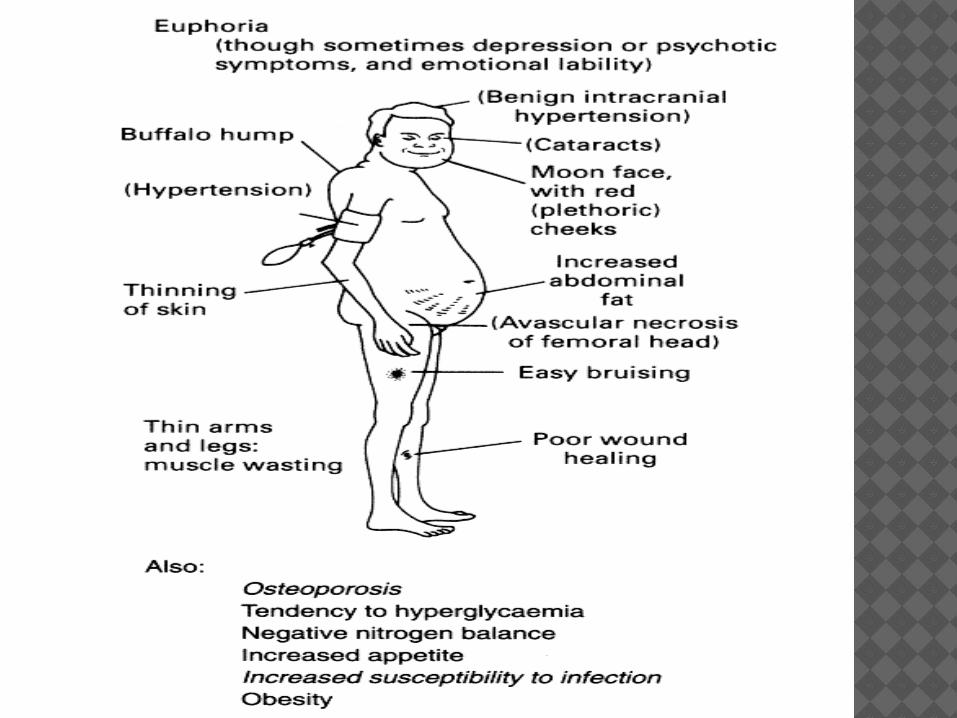
CUSHING’S SYNDROME

ADDISON’S DISEASE
ADRENALCORTICAL STEROIDS
Glucocorticoids- cortisol controls carbohydrate, fat and protein
metabolism anti-inflammatory by preventing
phospholipid release, decreasing eosinophil action
Mineralocorticoids-aldosterone controls electrolyte and water levels, mainly
by promoting sodium retention in the kidney.
SPECIFIC DRUGS Prednisone (Deltasone) Methylprednisolone (Solumedrol IM/IV) Cortisone Betamethasone (Diprolene) Dexamethasone (Decadron) Hydrocortisone (Solucortef IM/IV) Prednisolone Triamcinolone (Azmacort, Nasacort,
Kenalog) Fluticasone (Flovent, Flonase, Advair*) Budesonide (Pulmicort, Rhinocort,
Symbicort*)
* Combination product
INDICATIONS Replacement; Addison’s disease (low dose) Non-endocrine (high dose)
Rheumatoid arthritis / SLE / other inflammation (po, intra-articular injection)
Asthma (oral, inhaled, IV) Inflammatory bowel diseaseAllergic responsesDermatologic (topical, oral)CancersOrgan transplant (immune system suppression) Respiratory support in preterm infantsDecrease cerebral edema (suppress
inflammation)
ACTIONS Background/overview Metabolism Mineralocorticoid effect (sodium
retention) Anti-inflammatory Immunosuppressant
ADVERSE EFFECTS Adrenal insufficiency Osteoporosis Infection Glucose intolerance Muscle wasting Fluid and electrolyte imbalance
Edema, HTN, muscle weakness, dysrhythmias
Growth suppression Depression/suicide
“roid rage” Cataracts, glaucoma Peptic ulcer Iatrogenic Cushing’s syndrome Thin skin
DRUG INTERACTIONS Digoxin, thiazide / loop diuretics due to
hypokalemia NSAIDs due to GI bleeding Insulin and oral hypoglycemics due to
hyperglycemia Vaccines due to immunosuppression
No live vaccines
ADRENAL SUPPRESSION Need for additional doses during stress
if replacement Tapering if not replacement
DO NOT ABRUPTLY STOP (with exceptions) Alternate day dosing
Theoretically there is less endogenous corticosteroid suppression (via feedback)
POTENCY OF TOPICAL CORTICOSTEROIDS Potency can vary greatly between
various drugs, preparations (cream vs. ointment), and routes of administration
Systemic absorption also varies based on routeEx. Topical cream/ointment will have greater
systemic effect if skin broken vs. intact
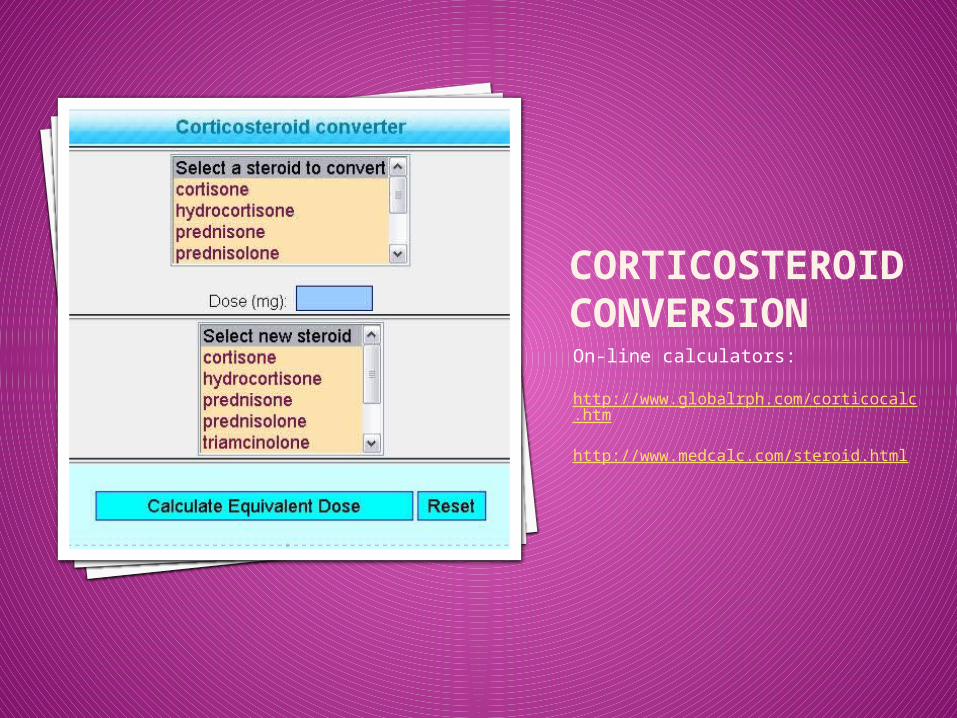
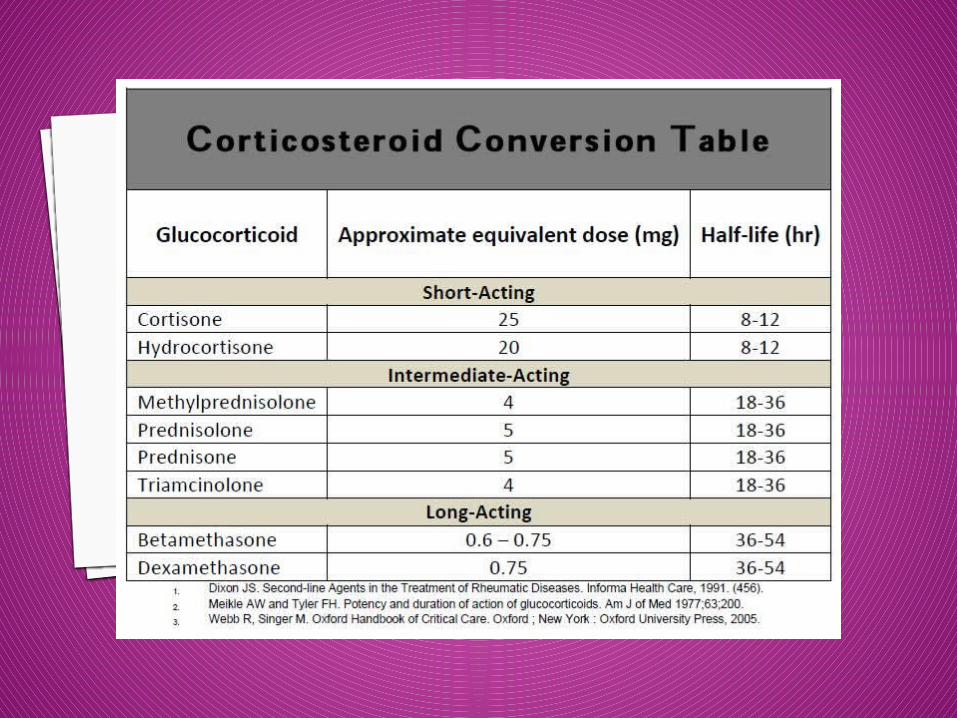
CORTICOSTEROID CONVERSIONOn-line calculators:
http://www.globalrph.com/corticocalc.htm
http://www.medcalc.com/steroid.html
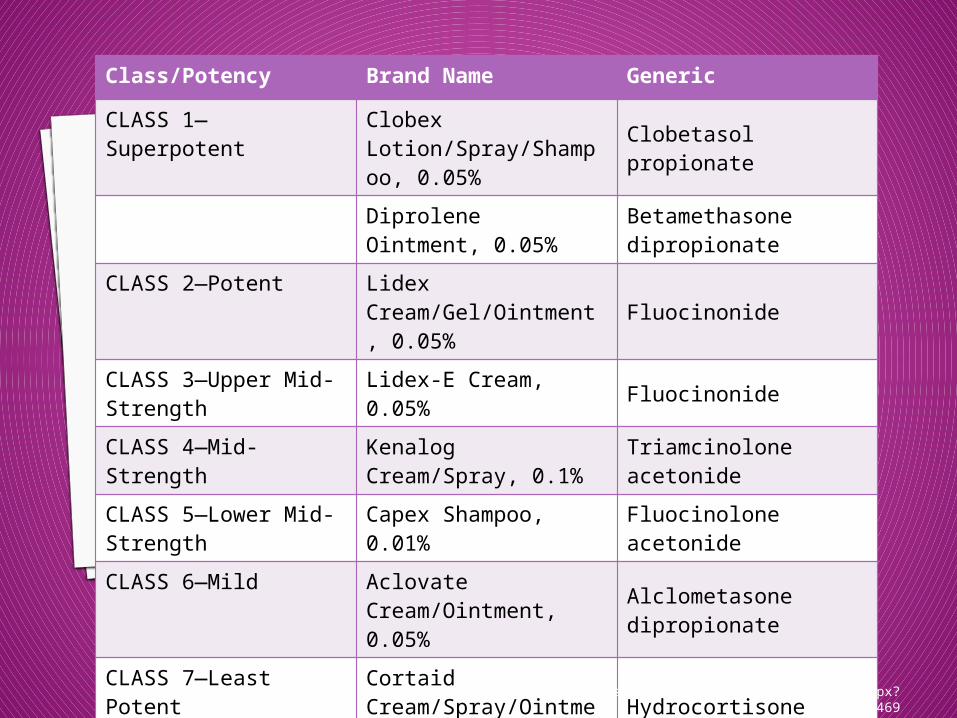
Class/Potency Brand Name Generic
CLASS 1—Superpotent Clobex Lotion/Spray/Shampoo, 0.05%
Clobetasol propionate
Diprolene Ointment, 0.05%
Betamethasone dipropionate
CLASS 2—Potent Lidex Cream/Gel/Ointment, 0.05%
Fluocinonide
CLASS 3—Upper Mid-Strength Lidex-E Cream, 0.05% Fluocinonide
CLASS 4—Mid-Strength
Kenalog Cream/Spray, 0.1%
Triamcinolone acetonide
CLASS 5—Lower Mid-Strength
Capex Shampoo, 0.01%
Fluocinolone acetonide
CLASS 6—Mild Aclovate Cream/Ointment, 0.05%
Alclometasone dipropionate
CLASS 7—Least Potent
Cortaid Cream/Spray/Ointment
Hydrocortisone
http://www.psoriasis.org/NetCommunity/Page.aspx?pid=469
NURSING IMPLICATIONS Give with food Give before 9 am to mimic circadian
rhythm Contraindicated if systemic fungal
infection Caution with pregnancy or lactation,
HTN, heart disease, renal failure, GI irritation, DM
THE END Questions????