Embed Size (px)
Citation preview

SYMPOSIUM
Architecture of the LungMorphology and Function
Harumi Itoh, MD, PhD,* Mizuki Nishino, MD,† and Hiroto Hatabu, MD, PhD†
Abstract: The architecture of the lung is discussed with special fo-cus on lung parenchyma. The lung parenchyma is mainly comprisedof numerous air-containing passages and intervening fine structures,corresponding to alveolar ductal lumens and alveoli, as well as alveo-lar septa and small pulmonary vessels occupying 10% of total paren-chymal volume. The shapes and relative arrangements of alveolarducts and alveoli are discussed in detail, which is followed by a briefdescription of bronchial circulation and pulmonary lymphatics.
(J Thorac Imaging 2004;19:221–227)
The purpose of this article is to demonstrate the architectureof the lung with special focus on lung parenchyma. The
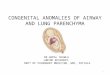
term “architecture” simply describes the notion of morpho-logic and functional correlation.1,2 There are two kinds of lungstructures, parenchymal and non-parenchymal structures. Thelung parenchyma resembles a sponge, and occupies 90% oftotal lung volume. Non-parenchymal structures consist of thebronchial tree, pulmonary vessels, and interlobular septa (Fig.1). As shown in Figure 1B, the bronchi and pulmonary arteriesrun together, alternated by pulmonary veins.
LUNG PARENCHYMAA closer look at the lung parenchyma reveals numerous
air-containing passages and intervening fine structures. Bothare distributed evenly as seen in the 0.5 mm thick lung sliceshown in Figure 2. The passage and intervening structures cor-respond to alveolar ductal lumens and alveoli, respectively.Alveolar septa and small pulmonary vessels occupy 10% of thetotal parenchymal volume, that is, the mean density of lungparenchyma is 0.1g/ml, which corresponds to −900HU of CTattenuation.3
ALVEOLAR DUCT AND ALVEOLIAn alveolar duct is best viewed in the short axis diam-
eter. Seven or 8 alveoli surround the alveolar ductal lumen.
The interalveolar septum is a thin membrane, and the overallshape of the alveolus is polyhedral (Fig. 3A). When we look atthe alveolar duct on histology, every alveolar septal membraneappears as a line (Fig. 3B). The 2-dimensional histologic im-age shown in Figure 3B is more frequently referenced than the3-dimensional view shown in Figure 3A, which leads to a lackof 3-dimensional understanding of lung parenchyma. It is pos-sible to distinguish alveolar ductal lumen, alveolar entrance,lateral wall of alveolus, and dome of alveolus on both Figures3A and 3B. The diameter of the ductal lumen is 0.3 mm, andthe mean size of the alveolus is 0.2 mm. The alveolar ductlength is about 1 mm in the long axis. The inner surface of thealveolar duct is covered by a sheet of alveoli. The shape of eachalveolar entrance is not round but polygonal, like a honey-comb. At higher magnification, a small hole in the alveolardome can be seen, which is Kohn pore (Fig. 4).
The photographs of a real honeycomb show the entranceof each cell as hexagonal in shape (Fig. 5). Mathematically, theoverall shape is ideal for maximum cell volume in a limitedspace. The honeycomb structure is composed of a single layerof alveoli but in the lung parenchyma, the alveoli walls aredouble-layered.
When we look at a model of a honeycomb (Fig. 6A),each cell is derived from a rhombic dodecahedron originallydescribed by the German astronomer, Johannes Kepler. Notethe imaginary alveolar entrance, lateral wall, and alveolardome. Each dome is composed of 3 planes. The important geo-metric feature of this honeycomb model is that exactly thesame sheet of cells can be formed on the other side holding thedome in common. The red line in each dome indicates wherethe lateral wall stands and extends toward the other side. Whenwe compare the model with the magnified view of the alveoli,white lines corresponding to our red lines are seen in the domeof alveoli (Fig. 6B).
A double-layered alveolar sheet can be demonstrated ina lateral view, as shown in Figure 7A. Every lateral wall of thealveolus joins to the apex of the alveolar dome. On histology,it is emphasized that the double-layered alveolar sheets holdalveolar domes in common (Fig. 7B). This common histologicimage defines the 2-dimensional architectural unit of lung pa-renchyma. Now we take a histologic look at the architecturalunit forming a network in the parenchymal space and sur-
From the *Department of Radiology, University of Fukui Faculty of MedicalSciences, Matsuoka-cho, Yoshida-gun, Fukui, Japan; and †Department ofRadiology, Beth Israel Deaconess Medical Center, Boston, MA.
Reprints: Hiroto Hatabu MD, PhD, Department of Radiology, Beth Israel Dea-coness Medical Center, 330 Brookline Ave., Boston, MA 02215 (e-mail:[email protected]).
Copyright © 2004 by Lippincott Williams & Wilkins
J Thorac Imaging • Volume 19, Number 4, October 2004 221

rounding the alveolar ductal lumen (Fig. 8A). Every alveolarduct appears isolated in this image. However, on a 3-dimen-sional photograph of the lung specimen, the alveolar ducts arecharacterized by frequent branching (Fig. 8B). The pattern of
branching is different from that of a bronchiole, as there is nospur.
Next, we discuss the overall shape of the alveolar duct.In Figure 9A, the contact radiograph shows alveolar ductscoated with barium sulfate demonstrating a round radiolucentarea, which corresponds to alveolar ductal lumen, as comparedwith the magnified view of the lung specimen. The lumen issurrounded by polygonal alveoli. Note the characteristic zig-zag shaped domes of alveoli and that the overall shape of thealveolar duct is polygonal. The contact radiograph shows theoverall shape of the similarly sized bronchiole and alveolarducts (Fig. 9B). The bronchiole is cylindrical in shape, but thealveolar duct is polygonal. This implies that the alveolar ducthas an ideal overall shape for peak lung function. In fact, thehistologic image shows the number of alveolar ducts is muchgreater than that of the bronchioles (Fig. 9C).
RESPIRATORY BRONCHIOLEThe respiratory bronchiole is called the transitional zone
because part of the bronchiolar wall is replaced by alveoli. Thenumber of alveoli increases as the respiratory bronchiolesbranch out (Fig. 10A). The distance from the respiratory bron-chiole to the nearest septal structures of the secondary lobule isconstant. For example, in the case shown in Figure 10B, therespiratory bronchiole is separated from the pulmonary vein bylung parenchyma. The distance between the two is maintainedat 2 mm. On histologic examination of the respiratory bronchi-ole, the bronchiolar wall, which is remote from the pulmonaryartery, is replaced by a sheet of alveoli (Fig. 10C). A close-upimage reveals these alveoli form a double sheet of alveoliwhere they abut the recurrent branch of the alveolar duct (Fig.10D).
ALVEOLAR CAPILLARY BEDS AND VENULESThe important structural component of the interalveolar
septum is the alveolar capillary. The capillary beds are calcu-lated to comprise 50% of the volume of alveolar septum, asdemonstrated in Figure 11A. The alveolar capillary is a densenetwork consisting of a number of irregular polygons. Accord-ing to Weibel, 10% of alveoli come into contact with non-parenchymal structures, such as pulmonary vessels.4 A num-ber of alveoli abut the pulmonary vein (Figs. 11B and 11C).Such alveoli do not form the usual double-layered sheets ofalveoli. The alveolar dome contiguous to the vessel is a single-faced alveolar wall because gas diffusion does not occur to-ward the pulmonary vessel. In contrast, the interalveolar sep-tum is a double-faced alveolar wall. Gas exchange is possiblein both sides of the double-faced alveolar wall. Alveolar cap-illaries are connected to post- or pre-capillary small vessels(Fig. 12A). Such small pulmonary vessels occupy part of thelimited interstitial space between the alveolar ducts (Fig. 12B).
FIGURE 1. A, Inflated and fixed lung specimens show bron-chial tree, pulmonary vessels, and interlobular septa, which areknown as non-parenchymal structures. Lung parenchyma oc-cupies 90% of total lung volume. B, A schematic drawing ofthe lung based on a contact radiograph of the specimen isshown. Note that pulmonary artery and vein run alternativelyin the lung.
Itoh et al J Thorac Imaging • Volume 19, Number 4, October 2004
222 © 2004 Lippincott Williams & Wilkins

FIGURE 2. A, Details of lung paren-chyma consisting of numerous air-containing passages and interveningfine structures, corresponding to al-veolar ducts and alveoli. B, A magni-fied view of Fig. 2A.
FIGURE 3. A, Short axis view of al-veolar duct surrounded by 7–8 al-veoli. Note a thin membranous in-teralveolar septum and polyhedron-shaped alveolus. B, Histologic imageof alveolar duct showing alveolarseptal membrane as a line.
FIGURE 4. An enlarged view of the alveolar dome shows Kohnpore as small hole (arrow).
FIGURE 5. Photograph of a real honeycomb. Note the hex-agonal shape of the entrance of each cell.
FIGURE 6. A, Model of a honey-comb. Note the exact same sheet ofcells formed on the other side hold-ing the dome in common. B, A mag-nified view of alveoli showing whitelines similar to the red lines in thehoneycomb model.
J Thorac Imaging • Volume 19, Number 4, October 2004 Architecture of the Lung
© 2004 Lippincott Williams & Wilkins 223

FIGURE 7. A, A lateral view of adouble-layered alveolar sheet. Noteevery lateral wall of the alveolus ad-joins the apex of the alveolar dome.B, Histology confirms that the double-layered alveolar sheets hold alveolardomes in common.
FIGURE 8. A, Histologic specimenshows a network in the parenchymalspace that surrounds the alveolarductal lumen. Note that every alveo-lar duct appears isolated. B, Magni-fied view of the inflated and fixedlung specimen showing frequentbranching of the alveolar duct.
FIGURE 9. A, Contact radiograph ofalveolar ducts with barium sulfate.Note the round radiolucent area cor-responding to alveolar ductal lumensurrounded by polygonal alveoli. B,Note the cylindrically-shaped bron-chioles and polygonal shape of thealveolar duct. C, On histology, agreater number of alveolar ducts areshown compared with those seen ina bronchiole.
Itoh et al J Thorac Imaging • Volume 19, Number 4, October 2004
224 © 2004 Lippincott Williams & Wilkins

Typically, small pulmonary vessels are located in the cornerwhere 4 alveolar ducts gather (Fig. 12C). This corner is calleda ridge in solid geometry and is ideal for blood vessel distribu-tion. However, we do not know the specific details of how thearteriole and venule are arranged in lung parenchyma. For this
purpose, radiologic analysis combined with 3-dimensional re-constructions may be necessary. The rough arrangement of thearteriole and venule within the secondary lobule is shown inFigure 12D. However, the size of these vessels is still too largeto study at an alveolar ductal level.
FIGURE 10. A, Contact radiographof respiratory bronchiole withbarium sulfate, showing an increasein the number of alveoli as the respi-ratory bronchiole branches out. B,Note the constant distance from re-spiratory bronchiole to the nearestseptal structures of the secondarylobule. C, Histology of the respirato-ry bronchiole. D, Magnified view ofthe respiratory bronchiole demon-strating the double sheet of alveoliabutting the recurrent branch of al-veolar duct.
FIGURE 11. A, Micrograph demon-strating a dense network of alveolarcapillaries consisting of a number ofirregular polygons. B, Magnifiedview of the lung parenchyma showsa number of alveoli abutting the pul-monary vein (arrow). C, Histologicspecimen shows contact between al-veoli and pulmonary vein.
J Thorac Imaging • Volume 19, Number 4, October 2004 Architecture of the Lung
© 2004 Lippincott Williams & Wilkins 225

FIGURE 12. A, Micrograph showsconnection between alveolar capil-laries and post- or pre- capillarysmall vessels. B, Magnified view ofthe lung shows small pulmonaryvessels occupying part of the limitedinterstitial space between alveolarducts. C, Histology shows typical lo-cation of small pulmonary vessel. D,The contact radiograph showsrough arrangement of arteriole andvenule within the secondary lobule.
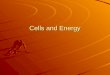
FIGURE 13. A, Macroscopic speci-men of the left lower lobe inflatedwith air. B, 3D CT of the specimen.Note the rich network pattern espe-cially in the lower portion. C, HRCTshows subpleural structure as thinlines along visceral pleura. D, Histol-ogy confirms subpleural lymphatics.
Itoh et al J Thorac Imaging • Volume 19, Number 4, October 2004

BRONCHIAL CIRCULATIONThere is a rich blood supply from bronchial arteries in
the bronchi and hilar lymph nodes as well as communicatingvessels between the pulmonary vein and the bronchial venousplexus.5 Bronchial veins are located around a bronchoarterialsheath, which communicates directly with the adjacent pulmo-nary vein. The pulmonary vein gives off a small branch to theneighboring airways. This special route may be responsible forperibronchial cuffing seen in the abnormal condition wherepulmonary venous pressure elevates.
PULMONARY LYMPHATICSSubpleural lymphatic structures are sandwiched be-
tween air and lung parenchyma. As shown in Figure 13, 3-di-mensional CT shows these structures to be a rich network, es-pecially in the lower portion of the specimen. On HRCT, theyappear as thin lines along the visceral pleura (Fig. 13C). Fi-nally, these subpleural lymphatics were proved on histology(Fig. 13D).
CONCLUSIONSKnowledge of the architecture of lung parenchyma is es-
sential for understanding the morphologic-functional relation-
ship of the lung to elucidate the gas exchange process. Thelung parenchyma is mainly comprised of numerous air-containing passages and intervening fine structures, corre-sponding to alveolar ductal lumens and alveoli, whose shapesand relative arrangements in 3 dimensions were discussed indetail.
ACKNOWLEDGMENTThe authors thank Ms. Donna Wolfe, Mr. Michael Lar-
son, and Mr. Ronald J. Kukla for their assistance in manuscriptpreparation.
REFERENCES1. Itoh H, Nakatsu M, Yoxtheimer LM, et al. Structural basis for pulmonary
functional imaging. Eur J Radiol. 2001;37:143–154.2. Itoh H, Murata K, Konishi J, et al. Diffuse lung disease: pathologic basis
for the high-resolution computed tomography findings. J Thorac Imag-ing. 1993;8:176–188.
3. Schneider W, Bortfeld T, Schlegel W. Correlation between CT numbersand tissue parameters needed for Monte Carlo simulations of clinical dosedistributions. Phys Med Biol. 2000;45:459–478.
4. Weibel ER. Looking into the lung: what can it tell us? Am J Roentgenol.1979;133:1021–1031.
5. Murata K, Itoh H, Todo G, et al. Bronchial venous plexus and its commu-nication with pulmonary circulation. Invest Radiol. 1986;21:24–30.
J Thorac Imaging • Volume 19, Number 4, October 2004 Architecture of the Lung
© 2004 Lippincott Williams & Wilkins 227









![Biochemical and Biophysical Research Communicationssourcedb.shanghaipasteur.cas.cn/yw/pa/201206/P... · 2013-12-05 · infection [1]. Once inside the lung parenchyma, the basidiospores](https://img.pdfslide.net/doc/110x75/5f49a9cebbfd856d0f6ff5c3/biochemical-and-biophysical-research-co-2013-12-05-infection-1-once-inside.jpg)







![Iron in Lung Pathology - pdfs.semanticscholar.org€¦ · and mediate damage and repair of the lung parenchyma [7]. However, the specific roles of these cell types in basal iron](https://img.pdfslide.net/doc/110x75/601d4454cb152e487712e511/iron-in-lung-pathology-pdfs-and-mediate-damage-and-repair-of-the-lung-parenchyma.jpg)