Embed Size (px)
Citation preview

1

2
AREAS OF PILOT PROJECT

3
EXECUTIVE SUMMARY
A beautiful quote of Swami Vivekananda encapsulates the spirit of Ekal movement’s
eventful journey-“Arise, awake and stop not till the goal is reached.”
Ekal movement, with the vision and passion of few compassionate and patriotic people,
aimed to reach, uplift, nurture and empower the most unreachable, neglected and
impoverished tribal and rural areas, spread across the remote corners of our otherwise
progressive Bharat. This noble thought and mission led to the development of ‘One teacher
schools’ (Ekal Vidyalaya) to make primary education as the starting point of growth in
remotest villages. Gradually, as the movement gained momentum and support of society
at large, other vital development parameters became the focus areas of Ekal and the vision
got enlarged from just education to integrated rural development.
One such key focus area of Ekal is rural and tribal health through its wing- Arogya
Foundation. The niche knowledge and experience of the health conditions of the rural –
tribal Bharat led to the need of a health project or do something measurable, achievable,
having far reaching impact on the overall health scenario in villages of Bharat. This led to
the start of the flagship Anaemia Control Pilot project of Ekal in 2013.
Anaemia or lack of blood in human body, came to be recognized as a silent killer, having
a negative ripple effect on the overall health of an individual.
Iron deficiency is thought to be the most common cause of anaemia globally, although
other conditions, such as folate, vitamin B12, vitamin A deficiencies, chronic
inflammation, parasitic infections, and inherited disorders can all cause anaemia.
But, the most disastrous consequence of Anaemia is its role in maternal mortality and
infant mortality in India. The girl child would grow to an anaemic adolescent and due to
an early marriage would again give birth to an anaemia impacted generation. This would
result in not only a slowed productivity and economic progress of a nation, but also a black
mark in the human and social development of a country.
World Health Organization’s (WHO) global database on Anaemia estimated the
prevalence of anaemia worldwide at 25 per cent, with India, being, one of the countries
with very high prevalence of anaemia in the world. Almost 58 per cent of pregnant
women in India are anaemic and it is estimated that anaemia is the underlying cause
for 20–40 per cent of maternal deaths in India. The National Family health surveys of
Government of India have also pointed at this grim reality from time to time.
All the above factors made Ekal take up a pilot programme to combat Anaemia in 8 blocks
(sanch/block is a cluster of 30 villages) in four Indian states, namely, U.P, Rajasthan,
Odisha and Jharkhand under the leadership of qualified and dedicated team of doctors,
supported by a team of trained Arogya Sevikaas (health volunteers). The target population
was 10-45 yrs of females and 2-10 yrs of children. The remedies used were both, the
curative measures of medication and preventive measures such as diet counselling and
raising health awareness among rural folks for a sustainable solution to Anaemia. A

4
rigorous follow up of Hb levels after six months of intervention was done to compare the
results and judge the improvement from the baseline status.
The women tested for haemoglobin were classified into anaemic and non-anaemic.
Further, the Anaemic were classified into Mild anaemic, Moderate anaemic and severe
anaemic as per the reduced Hb levels respectively.
Through the intervention of Ekal under the pilot project, the no. of women in severe
and moderate category (<7% and upto 10% Hb) has reduced from 6,221 to 3,946
achieving reduction in anaemic patients by 37%. Improvement achieved in the no. of
women in the mild category (>10% and upto 12% Hb) is from 9,563 to 11,838 i.e. by
24%.
To understand the true impact of Ekal’s pilot project as shown above, not only one needs
to appreciate the successful increase in the Hb levels of women, health and development
of children in villages but also growth in the overall awareness towards their own health
and surroundings. The most noticeable and commendable change also is in the
empowerment of and immense respect for rural women who as health volunteers became
catalyst in the health revolution of their fellow sisters and children. This has been a big
achievement in a male dominated social structure of village.
But the very nature and characteristic of Anaemia is such that it cannot be just considered
as an isolated health problem. Without ensuring better nutrition and environmental
conditions to the villagers, mere medication, no matter how good and effectively
administered, is unlikely to solve the problem.
In fact a permanent cure of Anaemia lies in making it a part of a holistic health awareness
programme, encompassing personal hygiene, rural sanitation, balanced diet, behavioural
change communication through lifestyle and food style changes ,emphasis of health
regulation through traditional home remedies/therapies and even empowerment of women
to end the gender inequality and discrimination.
And, this is a uphill but very much possible task which needs constant drive and motivation
of not only Ekal, but the society at large in form of medical fraternity, students, corporates
and the biggest contributor can be the Government which needs to be partnered for a
common objective of a better, healthier and capable Bharat.
As quoted in the words of Mahatma Gandhi- “The difference between what we do
and what we are capable of doing would suffice to solve most of the world’s
problems.”

5
INDEX
Chapters Pg. no. /s
1. Introduction 6
2. Meaning, Causes & Effects of Anaemia 6-9
3. Rationale of Ekal’s focus on Anaemia Control 9-10
4. Impact of Anaemia on Maternal/infant mortality & development 10-12
5. Prevalence of Anaemia in India 12-14
6. Government’s initiatives for Anaemia control and the gaps therein 15-16
7. Ekal’s pilot programme on anaemia control 17-23
• Objective & Scope
• Areas under Pilot
• Methodology of intervention
8. Baseline and final Hb testing: comparative data & highlights 24-29
9. Financials of the Pilot project 30
10. Challenges, award of certificate by RIMS and future strategies 30-32
11. Conclusion 32
12. Acknowledgement 33
13. Annexures 34-40
Annexure 1 - States Wise IMR & MMR targeted under 12th Five year plan
Annexure 2 - Key personnel involved in Anaemia Pilot project
Annexure 3 - Specimen Block (Sanch) Survey Report
Annexure 4 - Health Volunteer (Arogya Sevika) training cum feedback form
Annexure 5- Certificate of Ethics Committee of RIMS
14. Appendices 41-42
Appendix A- Photographs and names of Iron rich foods
Appendix B- Additional photographs of Anaemia control programme
15. References 43

6
1. INTRODUCTION
1.1 Ekal, in its spirit to make the most vulnerable and neglected segments of rural and tribal
India, become both a beneficiary of and a catalyst in Bharat’s progress , started its journey
with providing basic, non- formal education through its one teacher schools. Basic health
and hygiene awareness was already an integral part of the curriculum but, having
recognized the widespread impact of diseases on both children and other villagers, Ekal
formed a specialized health-wing called as Arogya Foundation of India in the year 2003.
1.2 Arogya Foundation is a dedicated step to provide cost effective quality health care
services to all the Ekal Vidyalaya villages, in an attempt to bridge the gap between remote
areas and modern health facilities. It stands as a significant milestone in Ekal’s journey
from school development to integrated village development.
1.3 It was noticed during the regular Arogya village camps that majority of females across
age groups complained common symptoms of weakness, body ache and loss of appetite.
Also the children were found to be suffering from malnutrition, parasitic infections and
impaired growth. The underlying cause was identified as Anaemia- a silent but grave killer
with a ripple negative effect on the human body and a flagship pilot programme of
Anaemia control was undertaken. A project well in time, much in lines with the Persian
proverb, “A stone thrown at the right time is better than gold given at the wrong time.”
2. WHAT IS ANAEMIA
2.1 Anaemia, in simple terms means lack of blood in the body. It is a condition in which
the number of red blood cells (RBCs), and consequently their oxygen-carrying capacity, is
insufficient to meet the body’s physiological needs. Not only oxygen, blood is a carrier of
all vital nutrients in the body so lack of blood means lack of nutrition in the body. Anaemia
can result from defective red cell production, increased red cell destruction or blood
loss.The function of the RBCs is to deliver oxygen from the lungs to the tissues and carbon
dioxide from the tissues to the lungs. This is accomplished by haemoglobin.
2.2 Symptoms of anaemia include numbness, dryness of skin, lack of interest, loss of
appetite and low blood pressure due to lack of oxygen. In its severe form, it is associated
with fatigue, weakness, dizziness, drowsiness and menstrual pain in women.
2.3 Reduced levels of haemoglobin in the blood evidence the presence of anaemia.
World Health Organization (WHO) has given standardized estimates of haemoglobin
for detection of Anaemia as in the table below:

7
2.4 CAUSES OF ANAEMIA
Iron is necessary for synthesis of haemoglobin. Iron deficiency is thought to be the most
common cause of anaemia globally, although other conditions, such as folate, vitamin B12,
vitamin A deficiencies, chronic inflammation, parasitic infections, and inherited disorders
can all cause anaemia.
Causes of Anaemia in Women:
Insufficient quantity of iron-rich foods and iron enhancers”in the diet (foods rich
In vitamin C such as citrus fruits), and low bioavailability of dietary iron (e.g. foods
containing only non-haem iron)
Excessive quantity of “iron inhibitors” in diet, especially during mealtimes (e.g.
tea, coffee, calcium-rich foods)
• Iron loss during menstruation
• Poor iron stores from infancy, childhood deficiencies and adolescent anaemia
• Iron loss from post-partum haemorrhage
• Increased iron requirement due to tissue, blood and energy requirements during
pregnancy
• Teenage pregnancy
• Repeated pregnancies with less than 2 years’interval
• Iron loss due to parasite load (e.g., malaria, intestinal worms)
• Poor environmental sanitation and unsafe drinking water
Causes of Nutritional Anaemia in children:
• Low iron stores at birth due to anaemia in mother
• Non-exclusive breastfeeding
• Too early introduction of inappropriate complementary food (resulting in
diminished breast milk intake, insufficient iron intake, and heightened risk of
intestinal infections)
• Late introduction of appropriate (iron-rich) complementary foods

8
• Insufficient quantity of iron and iron enhancers in diet, and low bioavailability
of
dietary iron (e.g. non-haem iron)
• Increased iron requirements related to rapid growth and development during
infancy and childhood
• Iron loss due to parasite load (e.g. malaria, intestinal worms)
• Poor environmental sanitation, unsafe drinking water and inadequate personal
hygiene
Anaemic/ malnutritioned infants
Anaemia is an indicator of both poor nutrition and poor health. Infectious diseases – in
particular malaria, helminth infections and other infections such as tuberculosis and
HIV/AIDS – are important factors contributing to the high prevalence of anaemia in many
populations. Anaemia is not only caused by imbalanced and insufficient nutrient intake but
is also a result of cultural and social factors like gender discrimination, child marriage,
female foeticide, illiteracy, low wages and domestic violence.
Early marriage & Neglected rural woman Gender Discrimination
early pregnancy
2.5 EFFECTS OF ANAEMIA
Pregnant women and children are particularly vulnerable to Anaemia.
Among women, iron deficiency prevalence is higher than in men due to menstrual iron
losses and the extreme iron demands of growing foetus during pregnancies, which are
approximately two times the demands in thenon-pregnant state. First, anaemia reduces
9
women’s energy and capacity for work and can therefore threaten household food security
and income. Second, severe anaemia in pregnancy impairs oxygen delivery to the foetus
and interferes with normal intra-uterine growth, resulting in intrauterine growth
retardation, stillbirth, lower birth weight and neonatal deaths. Therefore, anaemia is a
major contributor to poor pregnancy and birth outcomes in developing countries as it
predisposes to premature delivery, increased perinatal mortality and increased risk of death
during delivery and postpartum.
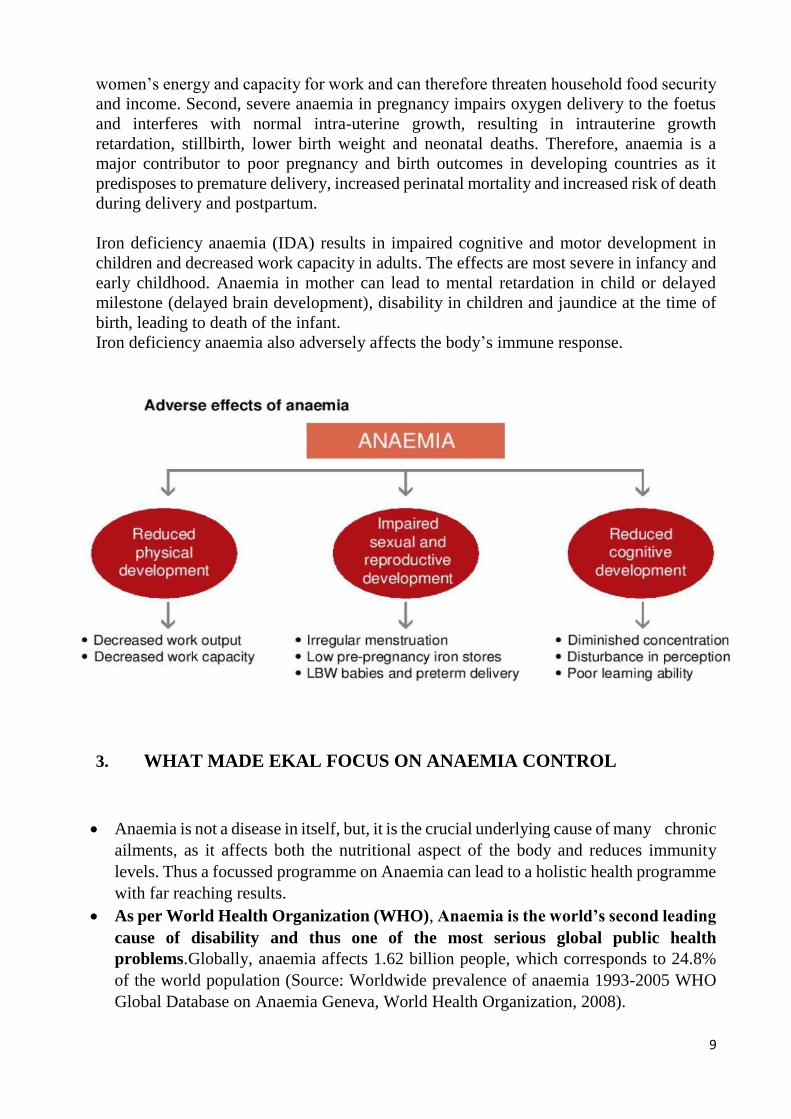
Iron deficiency anaemia (IDA) results in impaired cognitive and motor development in
children and decreased work capacity in adults. The effects are most severe in infancy and
early childhood. Anaemia in mother can lead to mental retardation in child or delayed
milestone (delayed brain development), disability in children and jaundice at the time of
birth, leading to death of the infant.
Iron deficiency anaemia also adversely affects the body’s immune response.
3. WHAT MADE EKAL FOCUS ON ANAEMIA CONTROL
Anaemia is not a disease in itself, but, it is the crucial underlying cause of many chronic
ailments, as it affects both the nutritional aspect of the body and reduces immunity
levels. Thus a focussed programme on Anaemia can lead to a holistic health programme
with far reaching results.
As per World Health Organization (WHO), Anaemia is the world’s second leading
cause of disability and thus one of the most serious global public health
problems.Globally, anaemia affects 1.62 billion people, which corresponds to 24.8%
of the world population (Source: Worldwide prevalence of anaemia 1993-2005 WHO
Global Database on Anaemia Geneva, World Health Organization, 2008).

10
But, it is the intergenerational, self-perpetuating vicious cycle of Anaemia
characterised by maternal mortality and infant mortality that is most serious and root
cause of Ekal’s special focus on Anaemia. Control of anaemia is not just a control of a
disorder but a major step in ensuring the health of both present and the future generation.
3.1 Maternal iron deficiency and anaemia render the offspring vulnerable for developing
iron deficiency and anaemia right from infancy. Poor iron content of complementary food
and family food consumed by the young child results in further increase in prevalence of
anaemia in childhood. With the onset of menstruation and associated blood loss, there is a
further rise in prevalence and severity of anaemia in adolescent girls. Early marriage and
adolescent pregnancy aggravate anaemia and result in poor iron stores in the offspring.
4. MATERNAL MORTALITY AND ROLE OF ANAEMIA IN MMR
4.1 MATERNAL MORTALITY RATIO (MMR) is defined as the number of maternal
deaths per 100,000 live births due to causes related to pregnancy or within 42 days of
termination of pregnancy, regardless of the site or duration of pregnancy.
4.2 In India, Anaemia is directly or indirectly responsible for 40 per cent of maternal
deaths. There is 8 to 10-fold increase in MMR when the Hb falls below 5 g/dl. (Source:
Prevalence & consequences of anaemia in pregnancy, a report by National Institute of
Health & Family Welfare, April 24, 2009)
4.3 As can be seen from the figure below-haemorrhage accounts for more than one- third
of all deaths followed by puerperal sepsis and abortion. Besides these, anaemia which has
been included in “other conditions” is a major contributory factor.

11
Note: SRS is Sample Registration System of India
MMR IN INDIA declined from 560 deaths
per 100,000 live births in
1990 to 190.
4.4 CHILD MORTALITY LINKED TO MATERNAL MORTALITY
Infant mortality rate (IMR) is the number of deaths of children less than one year of age
per 1000 live births. IMR, according to SRS 2010 at national level was 47 per 1000 live
births in 2010 as compared to 50 in 2009. The IMR is higher in respect of Female (49) as
compared to Male (46). IMR was also higher in rural areas (51 per 1000 live births) as
compared to urban areas (31 per 1000 live births) during 2010.One in every21 infants, one
in every 20 infants in rural areas and one in every 32 infants in urban areas still dies, within
one year of life in our country (SRS, 2010).

12
4.5 ANAEMIA- AN OBSTACLE TO NATIONAL DEVELOPMENT-POOR HDI
Anaemia reduces the work capacity of individuals, bringing serious economic
consequences.
UNITED NATIONS HUMAN DEVELOPMENT INDEX (HDI) is a summary measure
of average achievement in key dimensions of human development, including a long and
healthy life. India ranks 135th position among 187 countries as in 2014 in the UN Human
Development Index (HDI). (Source: YouTube video link
https://www.youtube.com/watch?v=Ur4pvqXKCDs)
5. PREVALENCE OF ANAEMIA IN INDIA
5.1 The WHO Global Database on Anaemia for 1993–2005, covering almost half the
world’s population, estimated the prevalence of anaemia worldwide at 25 per cent. India
is one of the countries with very high prevalence of anaemia in the world. Almost 58 per
cent of pregnant women in India are anaemic and it is estimated that anaemia is the
underlying cause for 20–40 per cent of maternal deaths in India. India contributes to
about80 per cent of the maternal deaths due to anaemia in South Asia, as depicted below:
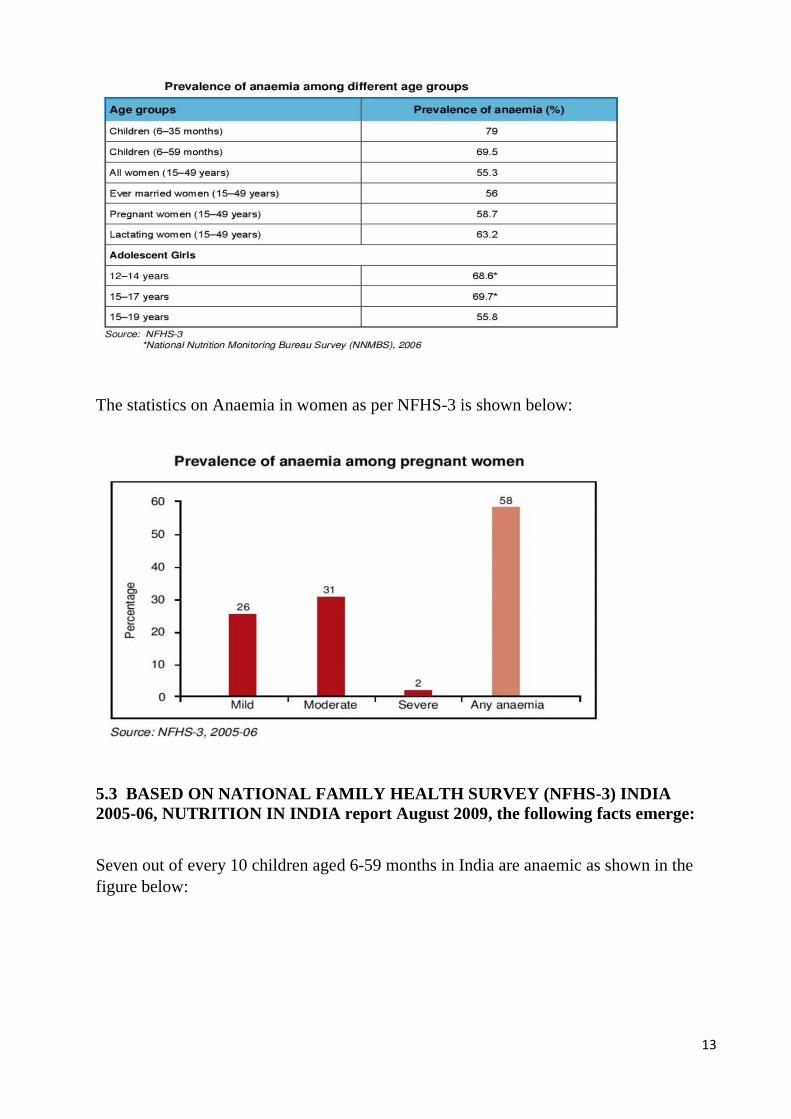
5.2 The National Family Health Survey-3 (NFHS-3),carried out in 2005-2006 by the
Ministry of Health And Family welfare, Government Of India ,suggests that anaemia
is widely prevalent among all age groups, and is particularly high among the most
vulnerable – nearly 58 per cent among pregnant women, 50 per cent among non-pregnant
non-lactating women, 56 per cent among adolescent girls (15–19 years), 30 per cent among
adolescent boys and around 80 per cent among children under 3 years of age – as shown
below:
13
The statistics on Anaemia in women as per NFHS-3 is shown below:
5.3 BASED ON NATIONAL FAMILY HEALTH SURVEY (NFHS-3) INDIA
2005-06, NUTRITION IN INDIA report August 2009, the following facts emerge:
Seven out of every 10 children aged 6-59 months in India are anaemic as shown in the
figure below:

14
An intergenerational examination of anaemia shows that the likelihood of a child being
anaemic is strongly related to the mother’s anaemia status.
The prevalence of anaemia in children age 6-59 months increases steadily with the
mother’s level of anaemia, reaching 83 percent for children of mothers who are severely
anaemic, as shown below:
In 2014-15, India will implement the fourth National family Health survey-4.

15
6. GOVERNMENT’S INITIATIVES FOR ANAEMIA CONTROL
6.1 GOI has started National Iron+ Initiative to prevent and control iron deficiency
Anaemia, a grave public health challenge in India. Besides pregnant women and lactating
mothers, it aims to provide IFA supplementation for children, adolescents and women in
reproductive age group.
National Iron+ Initiative reaches the following age groups:
• Bi-weekly iron supplementation for preschool children 6 months to 5 years
• Weekly supplementation for children from 1st to 5th grade in Govt. & Govt. Aided
schools
• Weekly supplementation for out of school children (5–10 years) at Anganwadi Centres
• Weekly supplementation for adolescents (10–19 years)
• Pregnant and lactating women
• Weekly supplementation for women in reproductive age
6.2 As per ADOLESCENT GIRLS ANAEMIA CONTROL PROGRAMME –UNICEF
report 2011, India is home to nearly 113 million adolescent girls and the prevalence of
anaemia in adolescent girls is estimated at 56 per cent. In view of the scale of the problem,
the Government of India and state governments with technical support by UNICEF and
partners have been implementing for over a decade the Adolescent Girls Anaemia Control
Programme. The main objective of the programme is to reduce the prevalence and severity
of anaemia in school-going adolescent girls using schools as the delivery channel and in
out-of-school adolescent girls using the community anganwadi centre of India’s Integrated
Child Development Services (ICDS) programme as the delivery platform.
6.3 The programme strategy for the initial phase was built around three essential
interventions: 1) weekly iron and folic acid supplementation (WIFS) comprising 100 mg
of elemental iron and 500 μg of folic acid; 2) bi-annual deworming prophylaxis (400 μg of
albendazole) six months apart for the prevention of helminth infestations; and 3)
information, counselling and support to adolescent girls on how to improve their diets and
how to prevent anaemia.
6.4 The coverage of the programme doubled as the number of adolescent girls benefiting
from the Adolescent Girls Anaemia Control Programme increased from 8.8 million by the
end of 2005 to 14.5 million by the end of 2010.
6.5 One of the goals for the 12th Five Year Plan 2012-17 is to reduce anaemia in girls
and women by 50 per cent.
Current figures of IMR & MMR and the targeted estimates under twelfth plan are available
in Annexure 1

16
6.6 WHY STILL A GAP?
Even after decades of implementing the national nutritional anaemia control programmes
by the Government of India, it is astonishing to see that 50% of pregnant women are still
anaemic, as per WHO norms.
IMP REASONS WHY GOVERNMENT AID NOT REACHING TRIBAL POPULATION AS
PER MINISTRY OF HEALTH & FAMILY WELFARE:
Difficult terrain and sparsely distributed tribal population in forests and hilly
regions.
Locational disadvantage of sub-centres, PHCs (Public Health centres), CHCs
(community health centres).
Non availability of service providers due to vacant posts and lack of residential
facilities.
Lack of suitable transport facility for quick referral of emergency cases.
Lack of appropriate HRD policy to encourage/motivate the service providers to
work in tribal areas.
Inadequate mobilization of NGOs.
Lack of integration with other health programs and other development sectors.
Activities not tuned to the tribal idioms, beliefs and practices.
Services not being client friendly in terms of timing, cultural barriers inhibiting
utilization.
Weak monitoring and supervision systems.
Besides the above listed reasons, The Government health workers are more engaged in
distribution of IFA medicines for Anaemia, they are not focussed on increasing the
villagers awareness about this disease .The doctors and other medical practitioners lack in
the very motivation to reach those, who are suffering the most.
Corruption is another major reason which is quoted as to why the benefit of Government’s
efforts does not reach the grassroots as medicines get expired even before they reach the
health centres.
But in a country like India with world’s second largest population and widespread diversity
in geographical, demographical and cultural terms, is it right to just blame the
Government for not coming up to the expectations of its people?
Or is it better to initiate steps in that direction and in fact become a partner with the
Government towards a more healthy and capable India?
Ekal’s Anaemia Control programme aims to do just that.

17
7. EKAL’s PILOT PROGRAMME ON ANAEMIA CONTROL
7.1 Initially the focussed programme on Anaemia started in 2010 through medical camps,
but experiencing the high dropout rate of women, a pilot programme was launched in 2013
where the focus got shifted to door to door evaluation and treatment of Anaemia in order
to reach all concerned.
Ekal’s Pilot programme on Anaemia control aimed for the following transition in the life
of every woman and child in the village:
PRESENT SCENARIO EKAL’S ANAEMIA CONTROL PROGRAM
TO HELP MOVE TO
TARGET SCENARIO
You tube video link of Ekal’s Arogya Anaemia control programme
https://youtu.be/ToAH_zXor8U

18
7.2 OBJECTIVES OF EKAL’s ANAEMIA PILOT PROJECT
To make Anaemia control its flagship health programme and eradicate the
moderate to severe levels of Anaemia completely in target group of women and
children in all Ekal villages in next 5-10 years.
To replicate the pilot model in rest of the country.
To make the most vulnerable rural girls/women and children healthy and contribute
in reducing the mortality rates such as MMR &IMR, due to Anaemia, thereby
ensuring the health of both the present and future generation.
To capitalize on its strength in terms of strong manpower, Ekal started a pilot
programme on Anaemia, on the basis of which a holistic health programme can be
launched.
To focus on a person centric programme by way of tracking the improvement in
health on the basis of follow up and comparative analysis.
To do something measurable in health, having far reaching favourable effect on the
village community to encourage our generous donors to contribute in our health
initiatives.
To create awareness among the community to utilize the locally available resources
to combat problems like Anaemia through food &life style changes.
7.3 SCOPE OF PILOT PROJECT
Total eight blocks, (each comprising of 30 villages), were selected in four states of
U.P (3 blocks), Rajasthan (1 block), Odisha (2 blocks) and Jharkhand (2 blocks).
Pilot areas selected based on the high anaemia prevalence, as per national statistics.
The process would include both curative health service in terms of Allopathic
treatment and preventive services in terms of counselling and awareness
programmes.
Target population is girls/women of reproductive age of 10-45 years age group and
children of 2-10 years age group (most affected set of people).
Availability of workers (karyakartaas), area coordinators and doctors to monitor
and train them on a regular basis was duly considered.

19
7.4 AREAS OF PILOT PROJECT
SAMBHAG(state) BHAG(division) ANCHAL(district) SANCH(block)
JHARKHAND Ranchi Ramgarh Gola
Lohardaga Lohardaga Bhandra
ODISHA East Odisha Keonjhar(kendujhar) Telkoi
West Odisha Rourkela Jarangloi
EAST U.P Vindhyachal Mirzapur Rajgarh
Sonbhadra Gurmura
Renukoot Myorpur
RAJASTHAN Udaipur Udaipur Jhadol
7.5 METHODOLOGY OF INTERVENTION
Arogya Samitis at Sambhag, Bhag, Anchal and Sanch (State, division, district and block
respectively) were constituted to guide and control the program. These Samitis comprised
of personnel related to medical field viz. doctors, paramedics, pharmacist and some
socially oriented persons. These Samitis with the help of CTO(central team members),
Bhag and Anchal Arogya Pramukh selected 6 heath volunteers in a block. Each was to
deliver the planned services in a group of nearly 5 villages. Most of these volunteers were
12th standard pass.
Detailed list of key personnel involved in pilot project is available at Annexure 2.
A standard set of procedures were followed in all the pilot areas, as follows:
A. TRAINING- It had two components:
Training of CTOs (Central team members), Bhag and Anchal Arogya Pramukhs:
delivered at two levels, namely Naishnatya Varg (training of trainers) and Naipunya
Varg (skill development), prevalent in Ekal Movement. In these camps (besides
other topics) the participants were taught the whole methodology, documentation
and reporting systems of Anaemia Control Programme.

20
Training in Session –Udaipur
Training of health volunteers: the health volunteer was a female from a village
(preferably married) who commits to volunteer for taking care of the health of her
village and the training she receives from Arogya Foundation. Initially 2 day
training of these health volunteers was conducted at block of district headquarters.
They were trained
- To test the blood of women for Hb gm%,
- To diagnose Anaemic women with the help of digital haemoglobinometer.
- To deliver medicines to women and children
- To visit the women at home and counsel them about diet and other
precautions to protect and treat anaemia, also to advise them to grow
nutritional garden comprising of green leafy vegetables
- To conduct group meetings in village to arouse awareness about anaemia
and its related social reasons.
- To document the whole activity.
Health volunteers training at Lohardaga
B. Survey:-
In these blocks (cluster of 30 villages), where the program was initiated, first a survey was
conducted to register all women of child bearing age (10-45 yrs.) residing in Ekal village
which usually comprises of less than 100 homes. All the children (2-10 yrs.) were also
registered. The survey was conducted by Anchal Arogya Pramukhs with the help of
Acharyas of Ekal Vidyalaya. Documentation of survey report was done in a particular
format.

21
Target Population- woman and children
Sample report of block(sanch) survey is available in Annexure 3
C. Blood Testing of Women and delivery of medicines:-
- The registered women were tested for Hb gm%
- Those found to be anaemic were delivered Iron, folic acid and B12 capsules-
Once a day for 100 days.
- All the registered Women irrespective of anaemia and all the registered
children were given tablet or Syrup of Albendazole (wormicide) on the spot.
The women found to be anaemic were
divided into three groups as follows:
• Mild - 10 to 12 gm/dl
• Moderate - 7 to 10gm/dl
• Severe - below 7gm/dl
Haemoglobinometer- Hb testing machine
Deviation from the standard in testing:
In Gola Sanch in Jharkhand, after initial survey the medicine distribution was initiated
without estimating the Hb% of women as the understanding at that time was that, it is a
known fact that anaemia in India is stated to be between 60 – 80% in women, testing is not
needed initially and will be done after 6 months.

22
Health Volunteer Haemoglobin testing by health volunteer
Telkoi block Hb testing: Adolescent girls Distribution of Iron folic acid tablets
D. COUNSELLING AND AWARENESS
Counselling was given to villagers both in respect of the dangers of Anaemia, the changes
that they should do in their diet and lifestyle to have a balanced, nutritional food.
Also, the awareness aspect covered the socio –cultural aspect to combat gender
discrimination and similar evils.
Diet counselling was customized as per the needs of that area, to make the villagers aware
of the locally available resources and efficiently use them to combat Anaemia. Stress was
laid on eating green leafy vegetables like bathua, palak, moonga saag etc. and Gur
(jaggery)-Chanaa, rich in iron content. Where even these were not available, cooking in
utensils made of iron was popularised.
Good sources of Iron:
Chana Sag Palak Daals Gur- Chana diet

23
Jhadol block diet awareness programme Anaemia awareness Camp
Also , as a health awareness initiative to improve the
overall nutrition of the villagers, they were taught to
cultivate nutritional gardens or ‘Poshan Vatikaas’, as
popularly called under Gramothan Yojana of Ekal, in
the areas surrounding their homes. In Telkoi Sanch
alone, as reported in Ekal Parinaam Kumbh, March
2015, by Bhag Arogya Yojana Pramukh- Jharna, 464
Poshan Vatikaas were planted.
Anaemia Counselling
Follow up and evaluation
The follow up was done by regular visits of health volunteers to each village, for observing
the diet pattern and correcting the same, checking the medicine consumption, awareness
talk and gaining knowledge of any major illnesses in this period. After six months the Hb%
of the women was to be retested. All target children and women were delivered
Albendazole again and only those women, who were still anaemic, were given iron folic
acid. The same regime was to be followed with counselling until all are brought out of the
clutches of anaemia.
A sample health volunteer training cum feedback form is available at Annexure 4

24
8. BASELINE AND FINAL Hb TESTING: COMPARATIVE DATA & HIGHLIGHTS
8.1 Area wise baseline survey of total no. of women registered
15,784 women were thus covered under baseline survey with their Hb tests.
8.2 Block wise Final Evaluation : The comparative number of women under
anaemic categories based on Hb levels before (Test 1) and after intervention
(Test 2):
Odisha
Sanch- Telkoi
Sambhag(state) Bhag(division) Anchal(district) Sanch(block)
No. of
Registered
Women
Odisha E.Odisha Keonjhar Telkoi 1487
Odisha W.Odisha Raurkela Jarangloi 2702
Rajasthan Udaipur Udaipur Jhadol 2004
East UP
Vindhyachal
Mirjapur Rajgarh 1736
Renukut Myorpur 1077
Sonebhadra Gurmura 1361
Jharkhand Lohardaga Lohardaga Bhandra 2567
Jharkhand Ranchi Ramgarh Gola 2850
Total Women - 15784
138
485
721
143
11
267
1039
170
Severe Moderate Mild non anemic
<7 7 to 10 10 to 12 >12
Keonjhar, TelkoiTEST 1 TEST 2

25
The no. of women in severe and moderate categories reduced to 278 which was 623 in the
beginning showing reduction by 55.3%. Improvement in the no. of women above 10gm%
is from 864 to 1209 i.e. 39.9%.
Sanch- Jarangloi
The no. of women in severe and moderate categories reduced from 1226 to 888 achieving
reduction by 27.5%. Improvement in the no. of women above 10gm% was from 1476
earlier to 1864 i.e. by 26.2%. In this Sanch one important reason of Hb% improvement
was that due to special effort of GRC Jarangloi, nutritional gardens had been developed
by most of the families.
RAJASTHAN Sanch- Jhadol
90
11361277
1995
883
1569
295
Severe Moderate Mild non anemic
<7 7 to <10 10 to< 12 >=12
Rourkela, Jarangloi
TEST 1 TEST 2
215
793
636
360
29
408
950
617
Severe Moderate Mild non anemic
<7 7 to 10 10 to 12 >12
Udaipur,Jhadol
TEST 1 TEST 2

26
The no. of women in severe and moderate categories reduced to 437 from 1008 in the
beginning, amounting to a reduction in anaemic patients by 56.6%. Improvement in the
no. of women above 10gm% was from 996 to 1567 i.e. 57.3%.
UTTAR PRADESH
Sanch- Rajgarh
The no. of women in severe and moderate categories reduced to 358 from 596 in the
beginning, amounting to a reduction in anaemic patients by 33.9%. Improvement in the
no. of women above 10gm% was from 1140 to 1378 i.e. 20.87%.
Sanch- Myorpur
59
537
863
277
13
345
894
484
Severe Moderate Mild non anemic
<7 7 to 10 10 to 12 >12
Mirzapur,Rajgarh
TEST 1 TEST 2
45
428
498
106
32
419
497
129
Severe Moderate Mild non anemic
<7 7 to 10 10 to 12 >12
Renukoot,Myorpur
TEST 1 TEST 2

27
The no. of women in severe and moderate categories reduced to 451 from 473 in the
beginning amounting to reduction in anaemic patients by 4.6%. Improvement in the no.
of women above 10gm% was from 604 to 626 i.e. 3.6%.
Sanch- Gurmura
The no. of women in severe and moderate categories reduced to 200 from 449 in the
beginning amounting to a reduction in anaemic patients by 55.4%. Improvement in the no.
of women above 10gm% was from 912 to 1161 i.e. 27.3%.
JHARKHAND
Sanch- Bhandra
46
403
647
265
9
191
742
419
Severe Moderate Mild non anemic
<7 7 to 10 10 to 12 >12
Sonebhadra, Gurmura
TEST 1 TEST 2
112
1005 1039
411
35
725
1275
532
< 7 7 - 10 10 to 12 12<
Lohardaga,Bhandra
TEST 1 RETEST

28
Bhandra in Jharkhand is 80% tribal block. The no. of women in severe and moderate
category reduced to 760 from 1117 in the beginning amounting to a reduction in anaemic
patients by 35.52%. Improvement in the no. of women above 10gm% was from 1450 to
1807 i.e. 24.62%.
Sanch- Gola
The no. of women in severe and moderate category reduced to 624 from 729 in the
beginning amounting to a reduction in anaemic patients by 14.8%. Improvement in the no.
of women above 10gm% was from 2121 to 2225 i.e. 4.9%.
In Gola Sanch, the intervention was designed with slight variation. Here, initially after
wormicide Albandazole, 100 days of Iron+Folic Acid+B12 regimen was administrated
without testing Hb%. 3 months after the last day of the above regimen first test for Hb%
was performed followed by diet counselling associated with administering herbal
preparations which were prepared from plants found in vicinity to the villages. The health
volunteers were specially trained for this.
20
709
1744
377
14
610
1785
440
< 7 7 - 10 10 to 12 12<
Ramgarh,Gola
TEST 1 RETEST

29
8.3 Combined Impact in all blocks by comparison of no. of women under different
Hb levels before (Test 1) and after intervention (Test 2):
The no. of women in severe and moderate categories reduced from 6221 to 3946 achieving
reduction in anaemic patients by 37%. Improvement in the no. of women above 10gm%
was from 9563 to 11838 i.e. by 24%.
8.4 Highlights of Hb Test Results
86.5% of rural women initially suffered from anaemia, of which 47% women were
suffering from mild anaemia (Hb gm% between 10-12) who can be brought out of
anaemia by diet counselling associated with control of other factors like, hygiene,
sanitation, gender discrimination etc.
Only 4.5% women were found severely anaemic (below 7gm%Hb), who improved
considerably as after second test only 0.9% are left in this category.
Majority of women having 7-10gm% Hb improved considerably. Those improved
in this category were 89.1%.
The experience in Gola block gives us an extra scope of improving anaemia without
medicines in most of the anaemic women except those having very severe anaemia.
The results fortify the theory that lower is the haemoglobin better is the
improvement ratio in Hb gm %. In below 7% category the women showing
improvement were 97% while it reduced gradually viz. in 7-10gm% category the
same was 89% and in 10-12gm% category it was still lower-71%.
725
5496
7425
2138
148
3798
8751
3087
Severe Moderate Mild non anemic
<7 7 to 10 10 to 12 >12
All blocks compiled no. of women as per Hb%
Test 1 Retest

30
9. FINANCIALS OF PILOT PROJECT ON ANAEMIA
9.1 COST PER BLOCK(SANCH)
(total villages-30, total women-5000, total children-2000 approx)
Sr. No. Cost Rs.
1 Survey 4,000
2 Medicines:
Albendazole & Iron/folic acid 8,49,000
3 Hb Testing 2,50,000
4 Travelling 72,000
5 Training 60,000
Total Cost per block(for 30 villages) 12,35,000
Total Cost per village 41,167
Note: Owing to wide variation in number of targeted persons in each village, it was not
appropriate to work out cost per person separately for each block. However, based on
total number of women and children covered, the average cost per person per year came
in range of Rs. 200 per annum.
9.2 SOURCE OF FUNDS FOR PILOT PROJECT
Out of the total cost on Anaemia Control under the pilot project, the funding was available
from two sources, 24% arranged from within Bharat and 76% from USA, as donations.
10.1 Challenges/Problems in the Execution of Pilot Project
• Availability of educated manpower in terms of minimum qualification of at least
10th standard pass female workers in village on a continuous basis.
• Continuous training requirements of health volunteers due to their marriage and
migration from villages.
• Due to cultural factors like ghoonghat /pardaa(veil) system, especially in Rajasthan,
availability and mobility of females was a challenge.
• Availability of abundant and dedicated team of doctors to supervise, monitor and
train the team of karyakartaas was the most critical part of a successful health
programme on Anaemia.

31
• Slow progress in areas where karyakartaas were ineffective .In this respect, an
active role of Anchal Arogya Pramukh was very crucial for effective functioning of
health volunteers.
• Underutilization of funds allocated for Anaemia due to an over- frugal attitude to
save on cost of project e.g. buying less Hb testing machines.
• Scepticism about Government support and absence of liasioning with the
Government.
• Initial resistance from male members or families of the health volunteers and of the
beneficiaries.
• Initial resistance and lack of awareness of rural women to take medicines.
• Systematic and detailed record and compilation of essential information/facts by
karyakartaas at various levels e.g. training data, expenditure data, necessary to
analyse crucial aspects of pilot programme.
10.2 Certificate of Ethics Committee of RIMS
In spite of the above challenges, the project was appraised and has been awarded a
certificate by Rajendra Institute Of Medical Sciences (RIMS), Ranchi for the scientific
research project on Anaemia Control entitled “Evaluation of the effectiveness of the
preventive measure of iron deficiency anaemia control programme of Arogya Foundation
Of India, Jharkhand branch.”
The certificate of RIMS is available at annexure 5
10.3 Future Strategies on Anaemia Control Programme:
• Tie ups with Local Government bodies /similar NGOs to collaborate towards a
common health goal.
• Involvement and partnership of ASHA workers of Government and health
volunteers in Ekal’s Anaemia awareness programmes.
• Tie ups with government schools/aanganwaadi centres for spreading Anaemia
awareness, especially in children and adolescent girls.
• Increasing awareness of villagers by participation in village haats (melas) through
announcements about our medical camps/awareness camps for Anaemia.
• Screening specially designed short videos on Anaemia awareness and control on
projectors in villages during trainings of sevikaas and counselling camps in villages.
• Inclusion of medical students and social work students in Ekal’s Anaemia
programme, as part of their internship or research projects.
• Increasing the role of NMO- National Medicos Organization- a voluntary
organisation of doctors and students for social service, presently only active in
medical camps but not involved in Anaemia control project.

32
• Make short feedback videos /documentaries of villagers who are benefited by this
pilot project to bring about the impact generated. Dedicated funding for this purpose
is needed from donors.
• Raising dedicated funding from Corporates for Anaemia control under their CSR
funding schemes.
• Encouraging the use of RTI (Right to Information Act) through Ekal’s Jaagran
initiative, as a means to make the implementation of Government policies on
Anaemia Control more effective.
• To eradicate the socio-cultural causes of Anaemia, empowerment of rural women
is most essential .E.g. Ekal Mahila Samiti in Jharkhand is active in sensitizing the
villagers about gender discrimination. More such initiatives are needed.
• Anaemia control programme should be expanded not only in more Sanchs in
present four states of pilot but in all areas where there is presence and involvement
of Central Toli (CTO) of Karyakartaas.
• Ekal’s Anaemia programme, on the basis of successful pilot models, should reach
the most neglected and vulnerable pockets of tribal India, for e.g. the tea garden,
remote areas of Assam.
• Also needed is an operational surveillance system with reliable, affordable and
easy-to use methods for assessing and monitoring anaemia prevalence and the
effectiveness of interventions. Effective usage of information technology can be an
answer.
11. CONCLUSION
Anaemia is a major health problem which engulfs both mother and child and hence an
effective control and preventive strategy of Anaemia will ensure a healthy present and
future generation.
Anaemia cannot be considered in isolation but has to be viewed as a part of a
comprehensive health programme focusing on nutrition, hygiene, sanitation and
awareness. In the long run, only treatment with medicines is not a sustainable solution but
diet counselling and awareness in the villages, even empowerment of women to end the
gender inequality and discrimination is necessary. Knowledge and training of developing
PoshanVatika for growing green leafy vegetables and medicinal herbs is needed.
Health care education and BCC- behavioural change communication through lifestyle and
food style changes is the permanent cure of Anaemia. Traditional Home
remedies/therapies should also be popularised, especially in tribal areas, where local herbs
are readily available.
Such pilot projects like Anaemia control will play a pivotal role in making Ekal movement
move from an Ekal Vidyalya movement to an Integrated Village development model.
To be effective and sustainable, Anaemia control strategies must be led with firm political
commitment and strong partnerships involving all relevant sectors.

33
12. ACKNOWLEDGEMENT
We would like to express our sincerest gratitude to all those who have contributed
towards the successful completion of this Pilot project, with a special mention of:
Secretary, RIMS Ranchi
State health authorities of respective states
Local donors for various kinds of support
USA based donors
Senior karyakartaas of Ekal Abhiyaan at various levels including Arogya
karyakartaas at the field levels.

34

35
ANNEXURE 1 State wise IMR & MMR targeted under 12th Five year plan

36
Annexure 2- Key personnel involved in Anaemia Pilot project
Category Sr.
No.
Names Details
Patrons 1 Dr.Krishna Kumar Ayurvedic Medicine,Padmashree,
Coimbatore
2 Dr.(Prof.) Ghanshyam
Das
Retd.HOD. RIMS
3 Dr.(Prof.) Janardan
Sharma
HOD, RIMS
Guides 1 Dr.(Prof.) M.S.Bhatt Retd.HOD,RIMS
2 Dr.UmashankarKesari Asso. Prof., RIMS,Incharge Anaemia
Control Program
3 Dr.Vishwambhar Singh BHU, Varanasi
4 Dr.O.P.Agarwal Retd. Director,Bokaro and Rourkela
Hospitals
5 Dr.AK Agrawal Asso.Prof.RIMS
6 Dr.R.N.Chourasia Assit.Prof,BHU, Varanasi
7 Dr.Anjali Rani Assit.Prof,BHU, Varanasi
8 Dr.Debashish
Bhattacharya
HMBS, Secretary ,Arogya Foundation,
Keonjhar
9 Dr.Piyush Ranjan Sahu Odisha Health Services,Keonjhar
10 Dr. Debabrat Sahani Prof.Hitech Medical
College,Bhubaneswar
11 Dr.Arun Kumar Sahu MD Odisha Health Services, Keonjhar
12 Dr.Prabhas Ranjan Asso.Prof.Govt.Medical
College,Bhubaneswar
13 Dr.HK Mittal HOD, ESI Hospital, Delhi
14 Dr.Manoj Singh BHMS,UP State Health
Services,Mirzapur
15 Dr.(Vaidya)Shivnarayan
Pathak
BAMS, Udaipur
16 Dr.Kusum Chopra Retd. From National Institute of Health
and Family Welfare, Delhi
17 Dr. Harishanand BMS,Arogya Foundation of India
18 Dr.C.Satish BAMS, Joint Coordinator,
AFI,Coimbatore
19 Dr.O.P.Mahatma Retd. Civil Surgeon,State Health
Services,Udaipur
20 Dr. (Prof.) YN Verma HOD, RNT Medical College,Udaipur
21 Dr. (Prof.) Krishna
Prasad
BAMS, HOD, Ayurvedic
Medicine,RVS Medical
College,Coimbatore
22 Dr.Pradip BAMS ,Ooty, Tamilnadu

37
23 Dr.H.P.Singh MD ,Prakash Pali Clinic, Sonebhadra
24 Dr. M. Krithika MD, Ayurveda ,Prof. Ayurveda
College,Coimbatore
Trainers 1 Dr. Mukul Bhatia MS (Surgery),ArogyaYojana Pramukh,
Ekal Abhiyan
2 Dr. T.N. Satapathy BAMS,Sah-ArogyaYojana
Pramukh,Ekal Abhiyan
3 Dr. (Prof.) Vivek
Kashyap
Prof.PSM Dept.RIMS
4 Dr.Sandeep Agrawal Asst.Prof.Surgery,RIMS, Ranchi
5 Dr.Bhupendra Singh Asso.Prof, Forensic Medicine
&Toxicology, RIMS Ranchi
6 Dr.Sarita Mittal MOIC, Mother and Child Welfare
Centre, SDMC Hospital,Delhi
7 Dr.Suresh Agrawal MS, Surgery,Specialist in
AyurvedicMedicines,Ranchi
8 Dr.Vivek Sharma MD(Ayurvedic Medicine)
Associates 1 Dr.(Prof.) Omprakash HOD,OMF Surgery,Dental College,
Hazaribagh
2 Dr.(Prof.) Usha Rani Retd.HOD, obs. &Gynae RIMS
3 Dr.Jamuna MBBS, State Health
Services,Lohardaga
4 Dr.Ramesh Ranjan MD (Pathology), Ranchi
5 Dr.S.K.Jamuar MBBS,Ramgarh, Jharkhand
6 Dr.D.C.Ram Retd. Deputy Director,State Health
Services, Ramgarh, Jharkhand

38
Annexure 3 –Specimen Block (Sanch) Survey Report
Bhag-West Odisha Anchal-Rourkela Sanch-Jarongloi
Sl N
o.
village name To
tal M
em
ber
Mal
e
Fem
ale
0 to 2 Years
3 to 9 years
Tota
l
Women 10 to 20 Years 21 to 45 years
Tota
l
BP
L
Mal
e
Fem
ale
Mal
e.
Fem
ale
Mar
ried
(N
on
PG
)
Mar
ried
(P
G)
Un
mar
ried
Mar
ried
( N
on
PG
)
Mar
ried
(P
G)
Un
Mar
ried
1 Bhangamunda 422 211 211 9 4 29 20 62 0 0 54 69 0 17 140 54
2 Jarangloi 143 73 70 2 2 3 9 16 0 0 11 38 4 7 60 24
3 Jharmunda 308 162 146 2 5 26 1 34 0 0 25 55 2 10 92 48
4 Beheramal 365 182 183 8 5 23 21 57 4 3 36 45 11 15 114 54
5 Baliposh(goud para) 149 85 64 1 3 8 4 16 0 1 10 25 0 2 38 18
6 Kustuna 369 176 193 4 7 25 21 57 1 0 48 63 3 10 125 41
7 Beldihi 328 166 162 3 5 23 12 43 0 0 39 58 1 11 109 49
8 Bagbud 330 163 167 5 4 13 20 42 0 0 31 84 7 21 143 31
9 Banki 299 155 144 1 2 21 14 38 0 1 36 48 2 12 99 46
10 Bijadihi 273 124 149 4 8 18 13 43 0 0 33 38 0 19 90 31
11 Salbira 322 170 152 3 1 22 19 45 0 1 37 84 2 8 132 39
12 Nakti 245 121 124 8 5 10 9 32 0 1 34 71 1 1 108 46
13 Bhikhampur 241 118 123 10 4 8 16 38 0 0 25 46 1 8 80 30
14 Jharmunda (itma) 307 148 159 5 6 11 16 38 1 0 36 44 4 13 98 21
15 Tiklipara 251 134 117 6 5 14 9 34 0 0 30 53 2 1 86 42
16 Gariamal 198 105 93 5 1 4 6 16 2 1 22 42 1 8 76 25
17 Jambahal 273 137 136 6 7 12 16 41 1 0 24 43 5 6 79 46
18 Itma 377 190 187 12 9 15 21 57 1 1 30 53 2 4 91 42
19 Pandripali 289 147 142 4 8 16 12 40 0 0 19 69 3 2 93 44
20 Karla 236 120 116 3 4 18 13 38 0 2 15 71 1 9 98 42
21 Mundagaon 259 135 124 3 2 11 15 31 0 0 28 39 4 9 80 34
22 Tileimal 376 209 167 4 6 26 13 49 1 1 37 53 0 9 101 43
23 Jamudia (jamarla) 221 109 112 5 1 10 18 34 0 0 26 60 2 2 90 30
24 Patuabeda 347 177 170 5 7 23 19 54 2 2 26 48 26 5 109 54
25 Manharpur 282 145 137 9 6 13 10 38 1 0 32 42 3 15 93 29
26 Kulga (basti) 360 189 171 9 6 20 18 53 11 0 25 65 1 16 118 25
27 Kulga (Jamtola) 194 103 91 3 3 16 14 36 0 0 20 39 0 8 67 26
28 Talimunda 189 97 92 3 1 7 5 16 0 0 23 44 2 9 78 17
29 Veluabahal 314 152 162 8 0 14 21 43 0 0 40 50 0 13 103 18
30 Kusum Munda 212 104 108 4 5 20 22 51 0 0 32 35 1 1 69 32
Total 8479 4307 4172 154 132 479 427 1192 25 14 884 1574 91 271 2859 1081

39
Annexure 4 - Health Volunteer (Arogya Sevika) training cum feedback form
Sevika Abhyaas Varg-:Telkoi, Month-:February-2015
Sambhag-: Odisha Bhag- East Odisha
Date Of AbhyaasVarg
Name Of Sevika
Sevika Present
Total Women
Personal Contact
Awareness Pragram
Participant No
H.b% Testing
Anaemic Testing
IFA Supplied
Albendazole Supplied
26.02.15 PrakasiniSahu Yes 126 126 5 51 0 0 98 0
MeeraSahu Yes 175 175 5 36 0 0 112 0
RasmitaGiri Yes 140 140 5 48 0 0 87 0
TulamaniNayak Yes 115 115 5 45 0 0 76 0
Sumitra Nayak (B) No 120 120 5 51 0 66 68 0
TriveniSahu Yes 205 205 5 51 0 0 85 0
TOTAL 6 6 881 881 30 282 0 0 526 0
Given Tablets Total 0
Last Month Tablets receive 0
Remaining Tablets 50
Next month's Requirements 2063X100 IFA
Medicine received for next month
108000 IFA RECEIVED
Goura Ch. Jena
GourangaNayak Dr.Debashis Bhattacharya
Anchal Abhiyan Pramukh Anchal Arogya Yojana Pramukh Anchal Arogya samiti

40
Annexure 5- Certificate of Ethics Committee of RIMS
Certificate of Ethics Committee of RIMS, Ranchi for Research granted to Arogya
Foundation of India on Iron Deficiency Anaemia

41
Appendix A- Photographs and names of Iron rich foods
Iron rich foods
Kantewali Chaulai Sarson ka sag Methi Kala chana
Soyabean Til Seethaphal KucchaKela
Water Melon

42
Appendix B- Additional photographs of Anaemia control programme
Medical Camps
Hb Testing Awareness speech in Gola Jhadol block Hb testing
43
REFERENCES
1. Recent annual reports of Arogya Foundation of India
2. Presentations of Dr.Sarita Mittal and Dr.Mukul Bhatia
3. Medical Camp reports of Arogya Foundation
4. Compiled write ups/reports/data on Anaemia by Dr.Mukul Bhatia ji
5. Website of ministry of health and family welfare India –http://mohfw.nic.in/
6. Annual Report 2013-14, Maternal health programme
7. Annual report 2013-14 of National Health Mission
8. Journal of Obstetrics and Gynaecology, February 2010: Maternal risk factors and
anaemia in pregnancy
9. Report on prevalence & consequences of anaemia in pregnancy K. Kalaivani
Department of Reproductive Biomedicine, National Institute of Health & Family
Welfare, New Delhi, India April 24, 2009from the website of ICMR-
http://icmr.nic.in/ijmr/2009/november/1125.pdf (ICMR)
10. National family health survey (NFHS-3) INDIA 2005-06, NUTRITION IN
INDIA report August 2009, from the website www.nfhsindia.org
11. The national guidelines by Ministry of Health & Family Welfare for control of
iron deficiency anaemia, in January, 2013 from the website link
http://nrhm.gov.in/nrhm-components/rmnch-a/child-health-immunization/child-
health/guidelines.html
12. Excerpts from 12th five year plan : social sectors from the website
http://planningcommission.gov.in
13. Concept of Human Development Index and India’s ranking from website link-
http://hdr.undp.org/en/content/human-development-index-hdi
14. Human Development Report 2014: Sustaining Human Progress:Reducing
Vulnerabilities and Building Resilience from UNDP website
15. India factsheet :Economic and Human Development Indicators, from UNDP
website
16. Adolescent girls anaemia control programme –UNICEF report 2011
17. Concept of Millennium Development Goals from the website link
http://www.unicef.org/mdg/maternal.html
18. Trends in Maternal Mortality: 1990 to 2013 Estimates by WHO(World Health
Organization), UNICEF(United Nations Children’s Fund), UNFPA( United
Nations Population Fund) The World Bank and the United Nations Population
Division(UNPD) REPORT –from the website link:
http://www.unfpa.org/sites/default/files/pub-pdf/9789241507226_eng.pdf
19. World Health Organization(WHO) report from the website
http://www.who.int/topics/anaemia/en/
20. Joint statement by WHO and UNICEF
http://www.who.int/nutrition/publications/micronutrients/WHOandUNICEF_statemen
t_anaemia/en/
21. World bank 2014 report on health , nutrition and population, November 2014





























![[CLACKAMAS COUNTY ALTERNATE WORK WEEK PILOT PROJECT ... · [CLACKAMAS COUNTY ALTERNATE WORK WEEK PILOT PROJECT ] ... Clackamas County Alternate Work Week Pilot Project Final Report](https://img.pdfslide.net/doc/110x75/5b894f857f8b9a287e8bd8ee/clackamas-county-alternate-work-week-pilot-project-clackamas-county-alternate.jpg)